Back to Journals » International Journal of Chronic Obstructive Pulmonary Disease » Volume 17
Low Peak Inspiratory Flow Rates are Common Among COPD Inpatients and are Associated with Increased Healthcare Resource Utilization: A Retrospective Cohort Study
Authors Clark B ![]() , Wells BJ
, Wells BJ ![]() , Saha AK, Franchino-Elder J, Shaikh A
, Saha AK, Franchino-Elder J, Shaikh A ![]() , Donato BMK
, Donato BMK ![]() , Ohar JA
, Ohar JA ![]()
Received 25 December 2021
Accepted for publication 2 June 2022
Published 29 June 2022 Volume 2022:17 Pages 1483—1494
DOI https://doi.org/10.2147/COPD.S355772
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Min Zhang
Brendan Clark,1 Brian J Wells,2 Amit K Saha,3 Jessica Franchino-Elder,1 Asif Shaikh,4 Bonnie MK Donato,1 Jill A Ohar5
1Health Economics and Outcomes Research, Boehringer Ingelheim Pharmaceuticals, Inc, Ridgefield, CT, USA; 2Department of Biostatistics and Data Science, Division of Public Health Sciences, Wake Forest School of Medicine, Winston-Salem, NC, USA; 3Department of Anesthesiology, Wake Forest School of Medicine, Winston-Salem, NC, USA; 4Clinical Development and Medical Affairs, Boehringer Ingelheim Pharmaceuticals, Inc, Ridgefield, CT, USA; 5Department of Medicine, Section of Pulmonary, Critical Care, Allergy and Immunology, Wake Forest School of Medicine, Winston-Salem, NC, USA
Correspondence: Jill A Ohar, Department of Medicine, Section of Pulmonary, Critical Care, Allergy and Immunology, Wake Forest School of Medicine, Winston-Salem, NC 27101, USA, Tel +1 336-406-6733, Fax +1 336-716-7277, Email [email protected]
Background: Patients with chronic obstructive pulmonary disease (COPD) can have low peak inspiratory flow (PIF), especially after hospitalization for acute exacerbation of COPD (AECOPD).
Purpose: To characterize patients hospitalized for AECOPD, and to assess the prevalence of low PIF, changes in PIF after hospitalization, and the association of low PIF with healthcare resource utilization (HRU) outcomes.
Patients and Methods: A retrospective cohort study was conducted using electronic health record data of hospitalized COPD patients in the Wake Forest Baptist Health system (01/01/2017 through 06/30/2020). Patients with a first eligible AECOPD hospitalization (index hospitalization) who were discharged before 05/31/2020 were included. PIF was measured using the In-Check DIAL™ at both medium-low resistance (R-2) and high resistance (R-5) during the index hospitalization. For R-2 and R-5, PIF was divided into low PIF (< 60 L/min; < 30 L/min) and high PIF (≥ 60 L/min; ≥ 30 L/min) groups. The primary outcome was the prevalence of low PIF. The stability of PIF after hospitalization was described. Adjusted regression models evaluated associations between low PIF and subsequent 30-day readmissions, 90-day readmissions, and HRU outcomes, including hospitalizations, emergency department visits, inpatient days, and intensive care unit (ICU) days.
Results: In total, 743 patients with PIF measured at R-2 and R-5 during a AECOPD hospitalization were included. The prevalence of low PIF was 56.9% at R-2 and 14.7% at R-5. PIF values were relatively stable after hospitalization. Adjusted analyses showed significant increases in HRU (all-cause hospitalizations [31%], COPD hospitalizations [33%], COPD inpatient days [46%], and COPD ICU days [24%]) during the follow-up period among patients with low PIF (< 60 L/min) at R-2. The 30- and 90-day readmission risks were similar between patients with low PIF and high PIF.
Conclusion: Low PIF is common among patients hospitalized for AECOPD, relatively stable after hospital discharge, and associated with increased HRU.
Keywords: AECOPD, electronic health records, healthcare utilization, PIF
Plain Language Summary
Patients with chronic obstructive pulmonary disease (COPD) have difficulty breathing, and worsening of symptoms can require hospitalization. They are often discharged from the hospital and provided with medications delivered by a dry powder inhaler, which is affected by peak inspiratory flow (PIF). This study examined the rates of airflow that patients with COPD could achieve while inhaling, using a device that measured PIF at different resistance levels, during hospitalization for an exacerbation of COPD. We aimed to identify the percentage of patients who could not achieve high PIF rates and assess their characteristics. We also observed the stability of PIF after hospitalization and evaluated associations between PIF and rates of healthcare visits after hospitalization.
This single-center study used electronic health record data from 743 patients hospitalized for COPD exacerbations between January 2017 and June 2020. Patients were categorized based on PIF measured at first hospitalization. PIF data collected after hospitalization during follow-up visits were also used for analysis. More than half (57%) of the patients had a low PIF of less than 60 liters per minute (L/min) when measured at medium-low resistance, and 15% had a low PIF of less than 30 L/min when measured at the high-resistance setting. Patients who could not achieve a PIF of at least 60 L/min at the medium-low resistance setting were found to have significantly more hospitalizations during the follow-up period, both all-cause hospitalizations (31%) and COPD hospitalizations (33%). These findings indicate that patients hospitalized for COPD often had low PIF, which was associated with higher rates of future hospitalization.
Introduction
Chronic lower respiratory diseases, including chronic obstructive pulmonary disease (COPD), were the fourth most common cause of death in the US in 2019 and are associated with significant morbidity, as well as substantial economic and social burdens.1,2 The main goals of treatment for COPD are reduction of symptoms and future risk of acute exacerbations of COPD (AECOPD), which the Global Initiative for Chronic Obstructive Lung Disease (GOLD) defines as an acute worsening of respiratory symptoms that result in additional therapy.3 One type of maintenance treatment modality for COPD is the use of dry powder inhalers (DPIs); while simpler to use than most other devices, DPIs are breath-actuated and require fast and hard inhalations to optimally release medication.4
Peak inspiratory flow (PIF) rate is defined as the maximal airflow (in liters per minute) achieved during a forced inspiratory maneuver.5,6 PIF rates required for the ideal delivery of medication from commonly used DPIs are published and have previously been termed “optimal PIF”.5,7 These depend upon the internal resistance of DPIs, thus varying among device brands. PIF rates below these thresholds have been defined as “suboptimal PIF”; however, the exact threshold values defining minimal effective PIFs remain under debate.5 In several reports, low PIF has been associated with poor drug delivery and inadequate drug de-aggregation.5,8–11 Two gamma scintillography trials further demonstrated that when using the Turbuhaler® powder inhaler, higher PIF was associated with improved lung deposition.12,13 Patients with COPD commonly have low PIF, especially during hospitalization for AECOPD.4,14 The prevalence of low PIF in COPD ranges from 32% to 52% in patients hospitalized for AECOPD,4 and low PIF is most prevalent among the elderly, women, and patients with a small stature or lung hyperinflation.6,15
Data on whether patients with COPD can achieve a clinical benefit using a DPI if they have low PIF are limited.4,14,16 In a randomized cross-over study in patients with low PIF (< 60 L/min), the use of a nebulized bronchodilator was associated with a higher forced expiratory volume in 1 second (FEV1) than the use of a DPI after 30 minutes, but not after 2 hours.17 In a phase 3b trial, use of a nebulized bronchodilator in patients with low PIF (< 60 L/min) produced numerically greater improvements from baseline in trough FEV1 compared with a DPI.18 One retrospective study of patients hospitalized for AECOPD showed that compared with patients with high PIF, those with low PIF had a significant increase in 90-day COPD readmissions and a shorter time to all-cause and COPD readmissions.14 However, a prospective observational study showed contrasting results.19 Thus, while it has been demonstrated that low PIF is associated with decreased drug delivery in vitro, there is a lack of clinical data showing whether low PIF is associated with poor patient outcomes and subsequent increases in healthcare resource utilization (HRU).
This study aimed to identify the prevalence of low PIF in a real-world population of patients hospitalized for AECOPD and to assess their demographic, clinical, and treatment characteristics, by PIF status. We also characterized the stability of PIF after hospitalization and evaluated potential associations between low PIF and HRU.
Patients and Methods
Study Design and Population
This retrospective, observational cohort study used electronic health record data from patients in the Wake Forest Baptist Health (WFBH) integrated health system between January 1, 2017, and June 30, 2020. In 2014, WFBH established a care plan for AECOPD hospitalizations that was found to reduce readmissions from occurring within 30 days of discharge; in 2018, it began measuring PIF using the In-Check DIAL™ at 2 different resistance settings (medium-low [R-2] and high [R-5]) as a component of the care plan.14,20 The In-Check DIAL™ imposes resistance to mimic different DPIs according to their internal resistance. R-2 DPIs include Accuhaler®, Diskhaler®, and Ellipta®, and R-5 DPIs include Easyhaler M® and Handihaler®. PIF was measured regardless of current inhaler use in patients hospitalized for AECOPD, as part of their outpatient post-discharge follow-up visit, as well as on initial assessment at pulmonary rehabilitation.20 Measurements were recorded by trained respiratory therapists at least once during hospital admission when patients were no longer in respiratory distress, able to complete a full sentence, and not using accessory muscles of respiration. Seated patients were told to inhale from functional residual capacity as fast and as hard as they could into the device; the best of 3 efforts was considered.
Eligible patients, aged ≥ 40 years, had ≥ 1 PIF measured using In-Check DIAL™ (Clement Clarke International Ltd, Harlow, UK and Alliance Tech Medical, Granbury, TX, USA) at both R-2 and R-5 during an AECOPD hospitalization. Patients were excluded if they had a diagnosis of cystic fibrosis or alpha-1 antitrypsin deficiency. Only the first eligible COPD hospitalization for each patient with a date of discharge prior to May 31, 2020, was included and used as the index hospitalization, defined as the first hospitalization in which PIF measurements by In-Check DIAL™ at the R-2 and R-5 levels of resistance were obtained. Patients were followed from the index hospitalization discharge date until 1 year, death, or study end (June 30, 2020), whichever occurred first.
Patient characteristics and COPD treatments were assessed on or before the index hospitalization discharge date. Relevant diagnoses and other clinical characteristics were identified using International Classification of Diseases 9th or 10th revision, clinical modification (ICD-9/10-CM) codes (Table S1). Baseline HRU was measured during the baseline period, defined as 1 year prior to the index hospitalization discharge date. eFrailty scores21 were available for patients aged ≥ 65 years who had the minimum number of elements necessary for score calculation. The Social Deprivation Index (SDI), a composite measure of area-level deprivation based on the demographic characteristics collected in the American Community Survey, was computed according to US census ZIP Code Tabulation Areas from 5-digit ZIP codes22 as a measure of the social determinants of health. Mortality data from the North Carolina (NC) State Center for Health Statistics were linked to the study database using a deterministic algorithm that utilizes name, sex, race, and date of birth and was used to censor patient follow-up.
Variables and Outcomes
The primary outcome was low PIF prevalence in the overall cohort. PIF measurements were dichotomized into low PIF and high PIF groups, separately for both R-2 and R-5, by PIF values obtained during the index hospitalization closest to the discharge date. Low PIF was defined as < 60 L/min and < 30 L/min for R-2 and R-5, respectively. High PIF was defined as ≥ 60 L/min and ≥ 30 L/min for R-2 and R-5, respectively.
PIF measurements after discharge from the index hospitalization, either in outpatient pulmonary clinics or during rehospitalizations, were available for subsets of patients and were used to explore the stability of PIF over time. Patients may have multiple PIF measurements on separate days during the post-discharge follow-up assessment period.
HRU outcomes during the follow-up period included 30-day all-cause readmissions, 90-day all-cause and disease-specific readmissions, and all-cause and disease-specific rates of inpatient hospitalizations, emergency department visits, inpatient days (length of stay [LOS]), and intensive care unit (ICU) days. Disease-specific outcomes included COPD and composite COPD or pneumonia events. COPD events were defined as the presence of a primary diagnosis of COPD or a primary diagnosis of acute respiratory failure plus a secondary diagnosis of COPD. Pneumonia events were defined as the presence of a primary diagnosis of pneumonia or a primary diagnosis of sepsis with a secondary diagnosis of pneumonia and no secondary diagnosis of severe sepsis present on admission (Table S1).
Statistical Analysis
Descriptive statistics summarized low PIF prevalence, patient demographics, and clinical characteristics. Student’s t-test and chi-square test were used to evaluate the differences in patient characteristics between PIF groups. Among subsets of patients with PIF measured after discharge from the index admission (eg, during readmission within 30 days), the proportion of patients who did not change PIF group (from low PIF to high PIF, or vice versa) was reported. Median (minimum, maximum) PIFs were plotted over time, according to PIF group at index (low PIF or high PIF), for the subsets of patients with PIF measured during specified time intervals over 1 year after discharge (eg, 30 to 60 days).
Poisson regression was used to assess the association between low PIF and incidence rates of HRU outcomes over the follow-up period. The offset term was the logarithm of person-years at risk. Person-years was used to accommodate the differences in at-risk time due to death or reaching the end of the study data. Multivariable logistic regression was used to assess the association between low PIF at index hospitalization and subsequent 30-day all-cause readmissions. Cox proportional hazards models were used to assess the association between low PIF and time to first readmission within 90 days of discharge from the index hospitalization. Separate models were developed for all-cause and disease-specific readmissions. Mortality data were used as a right censor for 90-day readmissions. Patients with ZIP codes outside of NC were excluded from the analysis of 30-day readmissions since any deaths occurring in this population would not be captured by the state death index, as were patients who died within 30 days of hospital discharge.
Regression models were adjusted for covariates including age, sex, race, Charlson Comorbidity Index score, number of all-cause admissions in the year prior to the index admission, body mass index, LOS for the index admission, and SDI. Due to small numbers of patients in the “other” race categories, it was necessary to simplify race as a binary variable (White vs other) for the regression models. Restricted cubic splines were included with each of the continuous variables to relax the linearity assumptions of the models. Splines were removed from variables in which the nonlinear components were not statistically significant. Missing data were reported for each variable. Body mass index was manually extracted from the electronic health record for a small number of patients where necessary. Variables with missing data were excluded from the regression analysis. All analyses were performed in R Studio (version 4.0.3).
Results
Patient Population
The study cohort included 743 patients with PIF measured at both R-2 and R-5 during the index hospitalization. Reasons for patient exclusion are given in Figure 1. Patient demographics and clinical characteristics are presented in Table 1. The median (interquartile range) age was 66.10 (59.65, 73.55) years, and 49.9% of patients were female. Compared with patients with high PIF, patients with low PIF had a higher median age, had a lower median body mass index, and were more often female. There was no significant difference between the low PIF and high PIF groups in eFrailty Index scores. GOLD status based on percent predicted FEV1 was only available in 46% of patients at baseline (Table 1). Maintenance COPD medications prescribed upon discharge from the index hospitalization were similar across PIF groups, with most patients prescribed triple therapy (long-acting muscarinic antagonist [LAMA] + long-acting beta2-agonist [LABA] + inhaled corticosteroid) (Table S2). Over 65% of patients were prescribed at least one DPI at discharge. In the year prior to the index hospitalization, the median number of hospital inpatient admissions and ICU days were similar between patients with low PIF and high PIF (all P > 0.05). During the index hospitalization, patients with low PIF had a significantly longer median LOS (R-2, P < 0.001; R-5, P < 0.001) than patients with high PIF, and significantly more patients with low PIF were admitted to the ICU (R-2, P = 0.001; R-5, P = 0.002) (Table 2).
 |
Table 1 Baseline Demographics and Clinical Characteristics by PIF Group |
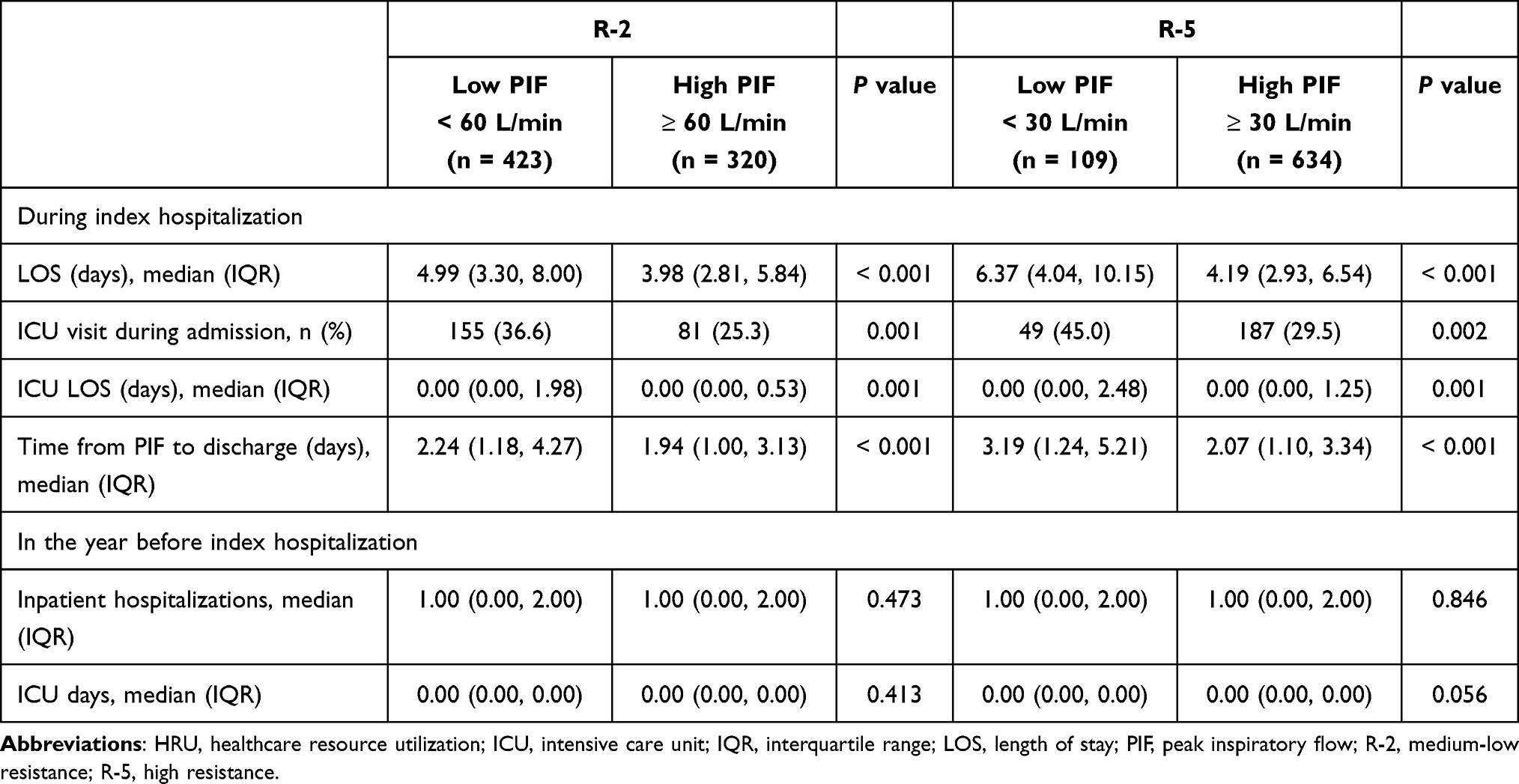 |
Table 2 Baseline and Index HRU by PIF Group |
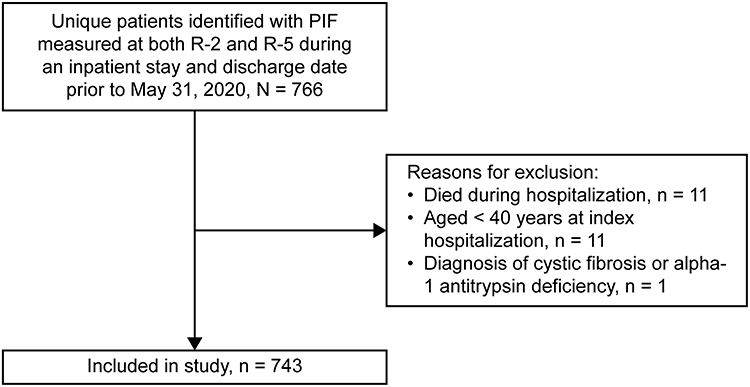 |
Figure 1 Patient flowchart. Abbreviations: PIF, peak inspiratory flow; R-2, medium-low resistance; R-5, high resistance. |
Prevalence of Low PIF
Approximately half of the patients (56.9%; n = 423) had low PIF (< 60 L/min) for R-2 and 14.7% (n = 109) had low PIF (< 30 L/min) for R-5 during their index hospitalization. The median (minimum–maximum) PIF was 50 (15–110) L/min for patients at R-2 and 40 (15–100) L/min for those at R-5 (Figure S1).
Healthcare Resource Utilization
The person-years of follow-up was 280.1 in the low PIF R-2 group and 225.0 in the high PIF R-2 group. Adjusted analyses showed low PIF at R-2 was associated with significant increases in rates of HRU outcomes, including all-cause hospitalizations (31%), COPD hospitalizations (33%), COPD inpatient days (46%), and COPD ICU days (24%) during the follow-up period (Table 3).
 |
Table 3 Incidence Rates and Unadjusted and Adjusted IRRs for HRU Outcomes During Follow-Upa |
A total of 686 patients had ZIP codes within NC and were eligible for the 30-day readmission analysis. The adjusted odds ratio (OR) showed numerically increased odds of 30-day all-cause readmissions for patients with low PIF at R-2 compared with patients with high PIF at R-2 (OR: 1.28; 95% confidence interval [CI]: 0.76–2.15), but the result was not statistically significant. The adjusted Cox proportional hazard ratio (HR) showed similar 90-day all-cause readmissions for patients with R-2 low PIF vs high PIF (adjusted HR: 1.22; 95% CI: 0.88–1.71). Adjusted HRs also showed similar 90-day COPD readmissions and 90-day COPD/pneumonia readmissions between groups (HR: 1.14; 95% CI: 0.75–1.73 and HR: 1.06; 95% CI: 0.70–1.59).
The HRU outcomes for R-5 PIF groups are generally consistent with those of the R-2 PIF groups (Table S3). Similarly, no statistically significant association was found between low PIF at R-5 and readmission outcomes.
Stability of PIF
PIF was measured in an outpatient pulmonary clinic within 30 days of index hospitalization discharge in 229 patients (30.8%). Of these, over 94% and 97% did not change R-2 and R-5 PIF groups from index, respectively. Similar patterns were seen in the 165 patients who had PIF measured during an all-cause readmission within 90 days of discharge from index hospitalization (Table S4). Median PIF, according to index PIF groups (low PIF and high PIF), was plotted for the subsets of patients with PIF remeasured during specified time intervals up to 1 year after index (Figure 2A and B).
 |
Figure 2 Median (minimum and maximum) PIFs in the year after the index admission by index PIF group. (A) PIFR R-2 measured over a year after the index admission; (B) PIFR R-5 measured over a year after the index admission. Abbreviations: PIF, peak inspiratory flow; PIFR, PIF rate; R-2, medium-low resistance; R-5, high resistance. Note: n denotes number of PIF measurements, N denotes total number of patients at each time point. |
Discussion
This retrospective observational study showed that low PIF is common during hospitalizations for AECOPD and that PIF status appeared relatively stable after hospital discharge. Compared with high PIF, low PIF was associated with increased subsequent HRU, including all-cause and COPD-related admissions, LOS, ICU days, and emergency department visits. Adjusted analyses showed that hospital readmissions in the 30 and 90 days after index, however, were statistically similar between the low PIF and high PIF groups. To the best of our knowledge, this is the first study showing an association between low PIF and increased HRU in real-world clinical practice. While low PIF has been shown to be associated with reduced drug delivery in vitro, decreased bronchodilator effect in vivo, and possible increased readmission after AECOPD, the impact of low PIF on outcomes such as LOS, ICU days, and other HRU measures has not been widely evaluated.5,8–10,12,14,17–19
PIF has been shown to affect drug delivery, drug de-aggregation, and particle size in vitro.4 The relationship between PIF and drug delivery is not linear but hyperbolic.23 This leads to greater differences in drug delivery per increment of PIF change at the lower end than at the upper end of the PIF spectrum. Therefore, even small decreases in the PIF below the minimal effective PIF, as published by device manufacturers, may lead to significant reductions in drug delivery.
In vivo, low PIF is associated with a decreased bronchodilator effect.18 Use of the nebulized LAMA revefenacin resulted in greater improvement in trough FEV1 compared with use of the dry powder LAMA tiotropium in patients with low PIF.18 Mahler et al showed similar results with the nebulized LABA arformoterol compared with the dry powder LABA salmeterol in patients with low PIF.17 Two studies have examined the effect of low PIF on hospital readmissions after AECOPD.14,19 The first, which measured PIF against no resistance (In-Check DIAL™ R-0), showed a significant association between low PIF and readmission.14 However, the second study, which measured PIF against the simulated resistance of the DISKUS® DPI (In-Check DIAL™ R-2), did not, which was aligned with the findings of our study.19 Compared with the study by Sharma et al,19 our study had a larger sample size and readmission analysis was adjusted for potential confounders. Our study did not show a statistically significant association between low PIF and 30- or 90-day readmissions; however, we observed an association between low PIF and several measures of HRU, including rates of hospitalizations, emergency department visits, and inpatient and ICU days. These findings are essential to clinical practice and health policy evaluations, as AECOPD is responsible for up to 70% of COPD-related healthcare costs, with hospital readmissions alone costing over $15 billion annually in direct costs.2
The association of low PIF with HRU is important. However, whether this relationship is causal and, if so, what the causal link could be is unknown. An important consideration of our study is that we did not define low PIF relative to patient’s current DPI use, because the lack of insurance claims data availability limited the assessment of medication/inhaler use during the follow-up period. However, over 65% of the patients in our study were prescribed at least one DPI at the time of discharge from the index admission, and low PIF was associated with increased HRU after discharge. Low PIF has been associated with age, female sex, small stature, and lung function impairment.6,15 Elderly women with a small stature and impaired lung function are more likely to have low PIF and to be considered frail,6,15 and frailty is linked with increased HRU.24 Although limited, our frailty data suggest that the link between low PIF and greater HRU may not be related to frailty.
In this study, 57% of patients had low PIF for an R-2 inhaler and 15% for an R-5 inhaler. These seemingly divergent values may be explained by the work of Barnes et al who showed that a PIF of 60 L/min against an R-2 resistance is roughly equivalent to a PIF of 40 L/min against an R-5 resistance.25 In exploring the distribution of PIF in this study, we found that 49% of patients had a PIF < 40 L/min against an R-5 resistance, thereby confirming the work of Barnes et al and aligning the low PIF threshold for R-2 and R-5 resistances.
For the subset of patients with PIF measured during a readmission within 90 days of index or at outpatient pulmonary clinic within 30 days, less than 6% changed their PIF group, indicating that PIF is relatively stable after hospitalization. However, it should be noted that in our study, the PIF for the index hospitalization was measured close to the discharge date when patients were no longer in respiratory distress. Although lung function deteriorates during AECOPD, PIF and inhalation volume increase during early recovery up to the stable stage.11,26
This study was conducted at a single health center; therefore, the generalizability of the results is limited. However, the prevalence of low PIF was consistent with that seen in other studies of PIF in COPD.14,15,27–30 Additionally, the retrospective and uncontrolled nature of this study is prone to inherent bias and limitations. We were unable to use SDI at the census block group level due to the inability to geocode some addresses, leading us to link SDI at the 5-digit ZIP code level instead. Although informative, the eFrailty Index was not included as a covariate since it is only designed for use in patients ≥ 65 years of age. Therefore, the authors relied on the less precise Charlson Comorbidity Index score as a measure of comorbidity. Loss to follow-up is also a concern for retrospective cohort studies, particularly in our study which used electronic medical record data alone. It is unknown if patients sought care elsewhere. However, our use of the NC state death registry should have reduced the potential bias introduced by loss to follow-up due to patient demise. The registry identifies deaths for NC residents regardless of where the deaths occur. Observational COPD studies are also potentially biased due to inaccurate COPD diagnoses based on ICD codes. One strength of this study is that all patients included were evaluated by respiratory therapists during index admission and deemed appropriate for inclusion in the COPD care pathway. A prospective design would be useful in validating these data and should be considered for further investigation.
DPIs require certain inspiratory force (flow, duration, and initiation of flow) to disperse, de-aggregate, and distribute the drug deep into distal airways.31 Therefore, future work exploring whether the association of low PIF with greater HRU is tied to DPI use would be of interest. This important question may best be answered with a prospective randomized trial assigning patients with low PIF to DPI devices or non-DPI devices, such as metered dose inhalers, nebulized medication, or soft mist devices.
Conclusions
We have shown that low PIF is common among patients hospitalized for COPD, relatively stable after hospital discharge, and associated with greater HRU. Our real-world evidence findings support clinical practice recommendations and health policy decisions considering the prevalence of low PIF and subsequent HRU among patients with AECOPD.
Abbreviations
AECOPD, acute exacerbation of chronic obstructive pulmonary disease; CI, confidence interval; COPD, chronic obstructive pulmonary disease; DPI, dry powder inhaler; FEV1, forced expiratory volume in 1 second; GOLD, Global Initiative for Chronic Obstructive Lung Disease; HR, hazard ratio; HRU, healthcare resource utilization; ICD9/10-CM, International Classification of Diseases 9th or 10th revision, clinical modification; ICU, intensive care unit; LABA, long-acting beta2-agonist; LAMA, long-acting muscarinic antagonist; LOS, length of stay; NC, North Carolina; OR, odds ratio; PIF, peak inspiratory flow; R-2, medium-low resistance; R-5, high resistance; SDI, Social Deprivation Index; WFBH, Wake Forest Baptist Health.
Data Sharing Statement
Due to the nature of this research, participants of this study did not agree for their data to be shared publicly, so supporting data is not available.
Ethics Approval and Informed Consent
The study was conducted in accordance with the Declaration of Helsinki and approved by the WFBH Institutional Review Board (approval number IRB00058893) with a waiver of informed consent according to 45 CFR 46.116 because the research involved no more than minimal risk to the subjects and could not practicably be carried out without the waiver. Protected Health Information was stored and analyzed within secure Wake Forest Servers and only available to the study team. No data at the patient level were shared outside of the institution.
Acknowledgments
Medical writing assistance was provided by Claire Line, Ph.D., of Cactus Life Sciences (part of Cactus Communications). We would also like to acknowledge the CTSI group at WFBH who supported the authors with the data collection: Brian Ostasiewski, Wendell Futrell, and Kobby Sekyere. We would like to acknowledge the use of services provided by the Informatics Program, supported by the National Center for Advancing Translational Sciences (NCATS), National Institutes of Health, through Grant Award Number UL1TR001420.
Author Contributions
All authors had full access to the data and take responsibility for the integrity of the data and the accuracy of the data analysis. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This study was funded by Boehringer Ingelheim. The study and the development of the manuscript was a collaboration between WFBH and Boehringer Ingelheim. The authors received no direct compensation related to the development of the manuscript. Boehringer Ingelheim was given the opportunity to review the manuscript for medical and scientific accuracy as well as intellectual property considerations. WFBH maintained ownership of the patient-level data.
Disclosure
Brendan Clark, Jessica Franchino-Elder, Asif Shaikh, and Bonnie MK Donato are employees of Boehringer Ingelheim Pharmaceuticals, Inc. Brian J Wells reports grants from Boehringer Ingelheim, during the conduct of the study. Jill A Ohar reports a research grant and publication assistance from Boehringer Ingelheim, during the conduct of the study; personal fees from and serving on the advisory board of Mylan, Sunovion, Boehringer Ingelheim, GlaxoSmithKline, Theravance, and Verona; and grants from Sunovion for a clinical study outside of the submitted work. The authors report no other potential conflicts of interest in relation to this work. This study was presented in part at the Virtual American Thoracic Society 2021 Conference, May 14–19 (Abstract A2165; available at: https://conference.thoracic.org/program/abstract-search.php?sid=P5762).
References
1. Kochanek KD, Xu J, Arias E. Mortality in the United States, 2019. NCHS Data Brief. 2020;(395):1–8.
2. Press VG, Konetzka RT, White SR. Insights about the economic impact of chronic obstructive pulmonary disease readmissions post implementation of the hospital readmission reduction program. Curr Opin Pulm Med. 2018;24(2):138–146. doi:10.1097/MCP.0000000000000454
3. Global Initiative for Chronic Obstructive Lung Disease. Global strategy for the diagnosis, management, and prevention of chronic obstructive lung disease. 2021 report; 2021. Available from: https://goldcopd.org/wp-content/uploads/2020/11/GOLD-REPORT-2021-v1.1-25Nov20_WMV.pdf.
4. Mahler DA. The role of inspiratory flow in selection and use of inhaled therapy for patients with chronic obstructive pulmonary disease. Respir Med. 2020;161:105857. doi:10.1016/j.rmed.2019.105857
5. Ghosh S, Ohar JA, Drummond MB. Peak inspiratory flow rate in chronic obstructive pulmonary disease: implications for dry powder inhalers. J Aerosol Med Pulm Drug Deliv. 2017;30(6):381–387. doi:10.1089/jamp.2017.1416
6. Mahler DA. Peak inspiratory flow rate: an emerging biomarker in chronic obstructive pulmonary disease. Am J Respir Crit Care Med. 2019;199(12):1577–1579. doi:10.1164/rccm.201901-0005LE
7. Dal Negro RW. Dry powder inhalers and the right things to remember: a concept review. Multidiscip Respir Med. 2015;10(1):13. doi:10.1186/s40248-015-0012-5
8. Grant AC, Walker R, Hamilton M, Garrill K. The ELLIPTA® dry powder inhaler: design, functionality, in vitro dosing performance and critical task compliance by patients and caregivers. J Aerosol Med Pulm Drug Deliv. 2015;28(6):474–485. doi:10.1089/jamp.2015.1223
9. Chodosh S, Flanders JS, Kesten S, Serby CW, Hochrainer D, Witek TJ. Effective delivery of particles with the HandiHaler dry powder inhalation system over a range of chronic obstructive pulmonary disease severity. J Aerosol Med. 2001;14(3):309–315. doi:10.1089/089426801316970268
10. Pavkov R, Mueller S, Fiebich K, et al. Characteristics of a capsule based dry powder inhaler for the delivery of indacaterol. Curr Med Res Opin. 2010;26(11):2527–2533. doi:10.1185/03007995.2010.518916
11. Chrystyn H, Niederlaender C. The Genuair® inhaler: a novel, multidose dry powder inhaler. Int J Clin Pract. 2012;66(3):309–317. doi:10.1111/j.1742-1241.2011.02832.x
12. Borgström L, Bondesson E, Morén F, Trofast E, Newman SP. Lung deposition of budesonide inhaled via Turbuhaler: a comparison with terbutaline sulphate in normal subjects. Eur Respir J. 1994;7(1):69–73. doi:10.1183/09031936.94.07010069
13. Newman SP, Moren F, Trofast E, Talaee N, Clarke SW. Terbutaline sulphate Turbuhaler: effect of inhaled flow rate on drug deposition and efficacy. Int J Pharm. 1991;74:209–213. doi:10.1016/0378-5173(91)90239-K
14. Loh CH, Peters SP, Lovings TM, Ohar JA. Suboptimal inspiratory flow rates are associated with chronic obstructive pulmonary disease and all-cause readmissions. Ann Am Thorac Soc. 2017;14(8):1305–1311. doi:10.1513/AnnalsATS.201611-903OC
15. Ghosh S, Pleasants RA, Ohar JA, Donohue JF, Drummond MB. Prevalence and factors associated with suboptimal peak inspiratory flow rates in COPD. Int J Chron Obstruct Pulmon Dis. 2019;14:585–595. doi:10.2147/COPD.S195438
16. Mahler DA. Peak inspiratory flow rate as a criterion for dry powder inhaler use in chronic obstructive pulmonary disease. Ann Am Thorac Soc. 2017;14(7):1103–1107. doi:10.1513/AnnalsATS.201702-156PS
17. Mahler DA, Waterman LA, Ward J, Gifford AH. Comparison of dry powder versus nebulized beta-agonist in patients with COPD who have suboptimal peak inspiratory flow rate. J Aerosol Med Pulm Drug Deliv. 2014;27(2):103–109. doi:10.1089/jamp.2013.1038
18. Mahler DA, Ohar JA, Barnes CN, Moran EJ, Pendyala S, Crater GD. Nebulized versus dry powder long-acting muscarinic antagonist bronchodilators in patients with COPD and suboptimal peak inspiratory flow rate. Chronic Obstr Pulm Dis. 2019;6(4):321–331. doi:10.15326/jcopdf.6.4.2019.0137
19. Sharma G, Mahler DA, Mayorga VM, Deering KL, Harshaw O, Ganapathy V. Prevalence of low peak inspiratory flow rate at discharge in patients hospitalized for COPD exacerbation. Chronic Obstr Pulm Dis. 2017;4(3):217–224. doi:10.15326/jcopdf.4.3.2017.0183
20. Ohar JA, Loh CH, Lenoir KM, Wells BJ, Peters SP. A comprehensive care plan that reduces readmissions after acute exacerbations of COPD. Respir Med. 2018;141:20–25. doi:10.1016/j.rmed.2018.06.014
21. Pajewski NM, Lenoir K, Wells BJ, Williamson JD, Callahan KE. Frailty screening using the electronic health record within a medicare accountable care organization. J Gerontol A Biol Sci Med Sci. 2019;74(11):1771–1777. doi:10.1093/gerona/glz017
22. Butler DC, Petterson S, Phillips RL, Bazemore AW. Measures of social deprivation that predict health care access and need within a rational area of primary care service delivery. Health Serv Res. 2013;48(2 Pt 1):539–559. doi:10.1111/j.1475-6773.2012.01449.x
23. Yokoyama H, Yamamura Y, Ozeki T, Iga T, Yamada Y. Analysis of relationship between peak inspiratory flow rate and amount of drug delivered to lungs following inhalation of fluticasone propionate with a Diskhaler. Biol Pharm Bull. 2007;30(1):162–164. doi:10.1248/bpb.30.162
24. Gilbert T, Neuburger J, Kraindler J, et al. Development and validation of a Hospital Frailty Risk Score focusing on older people in acute care settings using electronic hospital records: an observational study. Lancet. 2018;391(10132):1775–1782. doi:10.1016/S0140-6736(18)30668-8
25. Barnes CN, Mahler DA, Ohar JA, Lombardi DA, Crater GD. Peak inspiratory flows: defining repeatability limits and a predictive equation for different inhalers. Chest. 2020;158(4):1413–1419. doi:10.1016/j.chest.2020.03.072
26. Broeders ME, Molema J, Hop WC, Vermue NA, Folgering HT. The course of inhalation profiles during an exacerbation of obstructive lung disease. Respir Med. 2004;98(12):1173–1179. doi:10.1016/j.rmed.2004.04.010
27. Represas-Represas C, Aballe-Santos L, Fernández-García A, et al. Evaluation of suboptimal peak inspiratory flow in patients with stable COPD. J Clin Med. 2020;9(12):3949. doi:10.3390/jcm9123949
28. Ding N, Zhang W, Wang Z, et al. Prevalence and associated factors of suboptimal daily peak inspiratory flow and technique misuse of dry powder inhalers in outpatients with stable chronic airway diseases. Int J Chron Obstruct Pulmon Dis. 2021;16:1913–1924. doi:10.2147/COPD.S311178
29. Harb HS, Laz NI, Rabea H, Abdelrahim MEA. Prevalence and predictors of suboptimal peak inspiratory flow rate in COPD patients. Eur J Pharm Sci. 2020;147:105298. doi:10.1016/j.ejps.2020.105298
30. Duarte AG, Tung L, Zhang W, Hsu ES, Kuo YF, Sharma G. Spirometry measurement of peak inspiratory flow identifies suboptimal use of dry powder inhalers in ambulatory patients with COPD. Chronic Obstr Pulm Dis. 2019;6(3):246–255. doi:10.15326/jcopdf.6.3.2018.0163
31. Clark AR, Weers JG, Dhand R. The confusing world of dry powder inhalers: it is all about inspiratory pressures, not inspiratory flow rates. J Aerosol Med Pulm Drug Deliv. 2020;33(1):1–11. doi:10.1089/jamp.2019.1556
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.