")
Back to Journals » Open Access Rheumatology: Research and Reviews » Volume 10
Low mortality rate in Italian rheumatoid arthritis patients from a tertiary center: putative implication of a low anti-carbamylated protein antibodies prevalence
Authors Iacono D, Favoino E , Borgia A , Fasano S, Pantano I, D'Abrosca V, Picillo G , Grembiale RD, Perosa F , Valentini G
Received 25 January 2018
Accepted for publication 12 April 2018
Published 6 September 2018 Volume 2018:10 Pages 129—134
DOI https://doi.org/10.2147/OARRR.S163731
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Chuan-Ju Liu
Daniela Iacono,1 Elvira Favoino,2 Alessia Borgia,1 Serena Fasano,1 Ilenia Pantano,1 Virginia D’Abrosca,1 Giuseppe Picillo,1 Rosa Daniela Grembiale,3 Federico Perosa,2 Gabriele Valentini1
1Department of Clinical and Experimental Medicine, Rheumatology Section, University of Campania “Luigi Vanvitelli”, Naples, Italy; 2Department of Biomedical Sciences and Human Oncology (DIMO), Rheumatologic and Systemic Autoimmune Diseases Unit, University of Bari Medical School, Bari, Italy; 3Department of Medical and Surgical Sciences, University of Magna Graecia, Catanzaro, Italy
Background and objective: Anti-carbamylated protein antibodies (anti-CarP Ab) represent a novel kind of autoantibodies specificity detectable in the sera of patients with rheumatoid arthritis (RA). They have been recently reported to be associated with increased mortality in Spanish patients with RA. The aim of our study was to compare the incidence mortality rates (IMRs) detected in RA patients from a tertiary Italian center with those reported in other European tertiary centers and to evaluate the putative role of anti-CarP Ab in modulating the low IMR detected in our patients.
Methods: Clinical charts of patients consecutively admitted to our center, from January 1, 2008, to December 31, 2014, were retrospectively reviewed. The mortality rate (expressed as the number of deaths in the cohort divided by the number of years of IMR follow-up) and causes of death were assessed at December 31, 2015. Sera of 61 patients, representative of the whole cohort, collected at the time of admission to our center were investigated for the presence and the level of anti-CarP Ab. Demographic and clinical features, mortality rates and prevalence of anti-CarP Ab in our series were compared with those reported in other European cohorts.
Results: We observed 608 patients for a median of 3.51 years. All-cause and cause-specific IMRs in our cohort were significantly lower than the Better Anti-rheumatic Farmaco-therapy and the Spanish cohort, while only all-cause and cardiovascular IMRs were significantly lower in our series with respect to the Leiden Early Arthritis Clinic cohort. Anti-CarP Ab prevalence was significantly lower in our series than in any other European cohorts.
Conclusion: We confirm that the mortality rate is lower in our Italian RA cohort with respect to other European cohorts. Whether the low prevalence of anti-CarP Ab might be responsible for this result awaits to be furtherly investigated.
Keywords: rheumatoid arthritis, mortality, anti-carbamylated protein antibodies, death causes
Introduction
RA is a chronic systemic inflammatory disorder associated with increased mortality, in particular from CVD, infections and cancer.1–6 RA mortality has decreased over the past years, but it remained higher than in the general population with a standardized mortality rate (SMR) of 1.47, as derived by a recent meta-analysis of longitudinal studies.6 Nevertheless, RA mortality rate differs among series from distinct countries, ranging from 0.87 in Southern Sweden to 1.85 in Spain.7,8
We recently analyzed the mortality rate in 654 RA patients enrolled over a 6-year period in a South Italian tertiary rheumatology center, detecting an SMR of approximately 2, but pointing out an IMR lower than that reported in the NOAR. In particular, all-cause and neoplasm-related IMRs resulted to be significantly lower in our series than in patients from NOAR.9 Furthermore, unlike other series in which a number of factors including age, male sex, autoantibody positivity, disease activity and extra-articular manifestations are associated with an increased mortality, in our cohort, age at enrollment resulted to be the only independent predictor of earlier death.2,10
Anti-CarP Ab represent a novel kind of autoantibodies specificity detectable in the sera of patients with RA, with different prevalences in series from different countries.11–14 They have been recently reported to be associated with increased mortality in Spanish patients with RA.14
We undertook the present study to investigate the differences in IMR between our series and other tertiary center series from distinct countries. Moreover, we evaluated the anti-CarP Ab in the sera of a sample of patients representative of our series to investigate the putative role of these autoantibodies in modulating the low IMR detected in our patients.
Methods
Patients
Our cohort consisted of 654 patients consecutively admitted to the Rheumatology Unit of the Second University of Naples from January 1, 2008, to December 31, 2014, and satisfying at admission the American College of Rheumatology/European League Against Rheumatism (ACR/EULAR) 2010 criteria.15
Sex, age, disease duration, RF and ACPA positivity, disease activity and disability, as derived from medical records at baseline, were noticed. Disease duration (in years) was assessed from the first symptom ascribed to the disease. Serum RF (RF test, cut-off 20 units/mL) and ACPA (ELISA test, cut-off 25 units/mL) were also noticed. Disease activity was evaluated by Simplified Disease Activity Index. Disability was assessed by HAQ – Disability Index.16,17 The features of our cohort were compared with those reported in other European cohorts, that is, the BARFOT cohort, the LEIDEN EAC cohort and a Spanish cohort.13,14
On December 31, 2015, vital status and causes of death of the patients in our cohort were identified. In particular, deaths by CVD, cancer, respiratory disease, infections and other causes were considered. The mortality rate was expressed as the number of deaths in the cohort divided by the number of years of follow-up (deaths/person-years of IMR observation). It was compared with the IMR reported in the other European cohorts previously listed.
Sera of 61 patients, representative of our RA cohort, collected at the time of admission to our center were investigated for the presence and the level of anti-CarP Ab. Again, the proportion of patients positive for anti-CarP Ab in our cohort was compared with that reported in the other European cohorts.
Anti-CarP Ab assessment
Protein carbamylation
BSA was carbamylated by incubating 2 mg protein in 1 mL of 8 M urea (100 mM Tris-HCl pH 8.5) at 61°C for 15 h. The sample was then dialyzed against PBS at 4°C overnight. The efficiency of carbamylation was assessed by sodium dodecyl sulfate polyacrylamide gel electrophoresis to verify reduction in electrophoretic mobility.18
Detection of anti-CarP Ab
Levels of anti-CarP Ab in serum samples were assessed by indirect ELISA, as described with minor modifications.19 Briefly, polyvinylchloride 96-well microtiter plates were coated with modified and nonmodified BSA at 5 µg/mL. Wells were blocked with PBS containing 0.5% BSA (PBS-BSA), and then incubated for 4 h with serum samples diluted 100 times in PBS-BSA. Bound IgG was detected with HRP-conjugated anti-human IgG and o-phenylenediamine. Specific binding was determined by subtracting the reactivity to native BSA from the reactivity to carbamylated BSA. The levels of anti-CarP Ab were expressed as the percentage of binding relative to that of a positive RA patient serum. Values above the 95th percentile of healthy donors (n=41) were classified as positive.
Since we detected by the previously reported homemade assay that the prevalence of anti-CarP Ab is very low, we also investigated the same patients and 30 healthy subjects using the recently available commercial anti-CarP Ab kit (Novatein Biosciences, Woburn, MA, USA), an ELISA.20 This assay applied a technique called quantitative sandwich immunoassay. The microtiter plate was pre-coated with CarP. Standards and samples were then added to the microtiter plate wells. CarP Ab binded to the CarP in the coated wells. In order to quantify the amount of unbound CarP Ab in the sample, a HRP-conjugated anti-human secondary antibody was added to each well to bind the immobilized CarP. After incubation, plate was washed to remove all unbound components. Then, HRP substrate was added for a short incubation period. The enzyme–substrate reaction was stopped adding an acid stop solution. Only wells containing CarP Ab showed a change in color; this change was measured by a spectrophotometer at 450 nm. CarP Ab levels were expressed as concentration values (ng/mL). Values above the 95th percentile of healthy donors (n=30) were classified as positive.
Statistical analysis
Continuous variables were analyzed with the Mann–Whitney test, while chi-square test or Fisher’s exact test was applied for categorical variables, as appropriate. The comparison of mortality rates was conducted as comparison of IMRs. A p value <0.05 was considered significant. Analysis was performed with MedCalc, version 12.7.0.0.
Ethical approval and consent to participate
The study was approved by the Ethics Committee of the University of Campania “Luigi Vanvitelli” (protocol number 557). Written informed consent was obtained from all individual participants included in the study, according to the Declaration of Helsinki.
Results
Table 1 shows the epidemiological, serological and clinical features of the 654 patients of our cohort as compared to the 61 selected for anti-CarP Ab assessment. No difference was detected.
 | Table 1 Comparison of different features between our cohort and the sample tested for anti-CarP Ab Abbreviations: anti-CarP Ab, anti-carbamylated protein antibodies; SD, standard deviation; RF, rheumatoid factor; ACPA, anti-citrullinated cyclic peptides antibodies; HAQ-DI, Health Assessment Questionnaire – Disability Index; SDAI, Simplified Disease Activity Index. |
On December 31, 2015, 46 patients had been lost to follow-up (7%). The remaining 608 patients had been observed for a median of 3.51 years (range 0.21–7.96). Out of them, 19 had died: 11 (58%) for CV causes, 4 (21%) for malignancy, 3 (16%) for respiratory diseases, 1 for unknown causes (5.3%) and none for infections.
In our series, the overall IMR was 0.79 deaths/100 person-years; neoplasm-attributed IMR was 0.17; CV-attributed IMR was 0.46 and respiratory-attributed IMR was 0.13.
Anti-CarP Ab, as assessed by homemade technique, were found to exceed the 95th percentile of values detected in healthy donors in 2/61 patients (3.3%). Anti-CarP Ab, as assessed by commercial anti-CarP Ab kit, were found to exceed the 95th percentile of values detected in healthy donors in 6/61 patients (10%).
Table 2 lists the epidemiological, serological and clinical features, prevalence of anti-CarP Ab and the respective IMRs in distinct series.
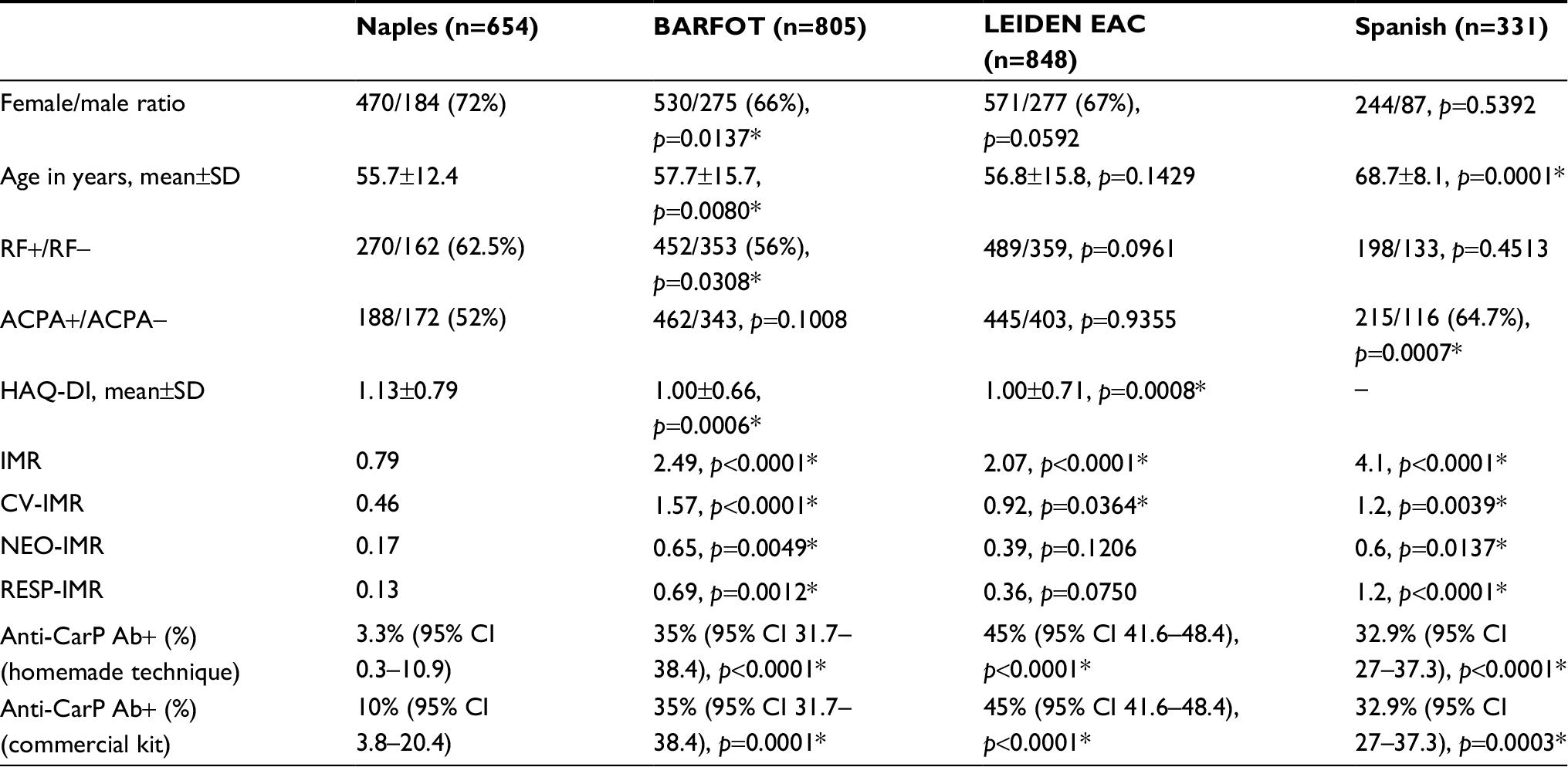 | Table 2 Comparison of different results between our cohort (Naples) and the other European cohorts Note: *A p value <0.05 was considered significant in the comparison between our cohort (Naples) and the other European cohorts. Abbreviations: BARFOT, Better Anti-rheumatic Farmaco-therapy; LEIDEN EAC, Leiden Early Arthritis Clinic; SD, standard deviation; CI, confidence interval; RF, rheumatoid factor; ACPA, anti-citrullinated cyclic peptides antibodies; HAQ-DI, Health Assessment Questionnaire – Disability Index; IMR, incidence mortality rate; CV, cardiovascular; NEO, neoplasm; RESP, respiratory; anti-CarP Ab, anticarbamylated protein antibodies. |
Despite a significantly higher proportion of negative prognostic factors (RF positivity and/or higher HAQ), all-cause IMRs were significantly lower in our cohort than in the North European BARFOT and LEIDEN EAC cohorts. These differences might depend on the significantly higher proportion of female patients and/or the earlier age characterizing our cohort with respect to the BARFOT and the LEIDEN EAC series.
As far as the Spanish cohort is concerned, we found that all-cause and cause-specific IMRs were significantly lower in our cohort. These results might be due to the significantly older age and higher proportion of ACPA positivity characterizing the Spanish series with respect to our series.
The proportion of patients resulted to be positive for anti-CarP Ab among those selected for anti-CarP Ab assay from our cohort was 3.3% (2/61 patients) as assessed by homemade technique and 10% (6/61 patients) as assessed by commercial anti-CarP Ab kit. This figure is significantly lower than that reported in the other European cohorts (Table 2).
Discussion
RA-increased mortality has long been known to be associated with high disease activity and severity and comorbidities, that is, CV and cerebrovascular diseases, infections, lymphoma and other neoplasms.21–24
Autoantibody positivity is recognized as a feature of more severe disease and has been associated with mortality with discordant results.12,13
We have recently investigated our RA cohort for all-cause and distinct-cause mortality. We found an increased all-cause mortality with respect to general population, mainly due to an increased risk of CV death.9
Intriguingly, we detected a death rate by cancer and infections lower than that reported in the Italian general population and in the British NOAR.9,13
We hypothesized that the detected differences might be ascribed either to the careful follow-up that RA patients undergo in tertiary centers, which may decrease mortality by cancer and infections, or to epidemiological differences among RA cohorts from different countries or both these aspects.25
We undertook the present study to investigate whether our mortality rate was also lower than that reported in other series and to look for the role, if any, of anti-CarP Ab prevalence in affecting the mortality rate of patients from different cohorts.
Comparing our results with those reported in other European tertiary center cohorts (BARFOT, LEIDEN EAC and Spanish cohorts), we confirmed the results obtained in our previous study in which we only compared our IMR with that reported in the NOAR, which is derived from primary and secondary care units.9,13
Actually, we found that all-cause and cause-specific IMRs were significantly lower in our cohort with respect to the BARFOT and the Spanish cohort, while only all-cause and CV IMRs were significantly higher in the LEIDEN EAC cohort than in our series, with no significant differences in terms of death due to neoplasm and respiratory diseases.13,14
These discrepancies might depend on demographic and clinical differences among the various cohorts. Nevertheless, we failed to find putative differences with respect to each North European cohort (Table 2).
Anti-CarP Ab have been recently identified in the sera of patients with RA and have been associated with increased mortality in Spanish RA patients, mainly by respiratory diseases.11,12,14
In order to investigate a further putative factor associated with the low mortality detected in our series, we analyzed anti-CarP Ab level in a sample of 61 patients representative of our RA cohort. We detected a prevalence as low as 3.3% by a homemade technique and 10% by the recently available commercial anti-CarP Ab kit. Both these figures are significantly lower than that reported in the other European cohorts.
Anti-CarP Ab have so far been investigated in another Italian series only in which a prevalence of anti-CarP Ab as high as 34% was detected. In that study, the features of the 309 patients enrolled are not addressed.26
Therefore, we cannot compare the 2 series and cannot make any hypothesis on these discrepancies. Nevertheless, the 95% CI of our anti-CarP Ab prevalence (0.3–10.9) does not overlap with any of those reported by other investigated cohorts.
Conclusion
We confirm that the mortality rate in our South Italian RA cohort is lower than that detected in patients from both North and South European countries and that this discrepancy cannot be ascribed to classical negative prognostic factors including RF and HAQ. We detected a very low prevalence of anti-CarP Ab in our sample representative of the entire cohort. Whether this is the aspect responsible for the low mortality rate detected awaits to be furtherly investigated.
Abbreviations
ACPA, anti-citrullinated cyclic peptides antibodies
anti-CarP Ab, anti-carbamylated protein antibodies
BARFOT, Better Anti-rheumatic Farmaco-therapy
BSA, bovine serum albumin
CarP, carbamylated protein
CV, cardiovascular
CVD, cardiovascular disease
ELISA, enzyme-linked immunoabsorbent assay
HAQ, Health Assessment Questionnaire
HRP, horseradish peroxidase
IMR, incidence mortality rate
LEIDEN EAC, Leiden Early Arthritis Clinic
NOAR, Norfolk Arthritis Registry
RA, rheumatoid arthritis
RF, rheumatoid factor
SMR, standardized mortality rate
Disclosure
The authors report no conflicts of interest in this work.
References
Pincus T, Callahan LF, Sale WG, Brooks AL, Payne LE, Vaughn WK. Severe functional declines, work disability, and increased mortality in seventy-five rheumatoid arthritis patients studied over nine years. Arthritis Rheum. 1984;27(8):864–872. | ||
Leigh JP, Fries JF. Arthritis and mortality in the epidemiological follow-up to the National Health and Nutrition Examination Survey I. Bull N Y Acad Med. 1994;71(1):69–86. | ||
Sokka T, Abelson B, Pincus T. Mortality in rheumatoid arthritis: 2008 update. Clin Exp Rheumatol. 2008;26(5 Suppl 51):S35–S61. | ||
Aviña-Zubieta JA, Choi HK, Sadatsafavi M, Etminan M, Esdaile JM, Lacaille D. Risk of cardiovascular mortality in patients with rheumatoid arthritis: a meta-analysis of observational studies. Arthritis Rheum. 2008;59(12):1690–1697. | ||
Meune C, Touzé E, Trinquart L, Allanore Y. Trends in cardiovascular mortality in patients with rheumatoid arthritis over 50 years: a systematic review and meta-analysis of cohort studies. Rheumatology (Oxford). 2009;48(10):1309–1313. | ||
Dadoun S, Zeboulon-Ktorza N, Combescure C, et al. Mortality in rheumatoid arthritis over the last fifty years: systematic review and meta-analysis. Joint Bone Spine. 2013;80(1):29–33. | ||
Lindqvist E, Eberhardt K. Mortality in rheumatoid arthritis patients with disease onset in the 1980s. Ann Rheum Dis. 1999;58(1):11–14. | ||
Martínez MS, García-Monforte A, Rivera J. Survival study of rheumatoid arthritis patients in Madrid (Spain). A 9-year prospective follow-up. Scand J Rheumatol. 2001;30(4):195–198. | ||
Iacono D, Fasano S, D’Abrosca V, Pantano I, Valentini G. Mortality in Italian patients with rheumatoid arthritis: evidence for a low mortality rate from cancer and infections in patients followed up at a tertiary center. Open Access Rheumatol. 2017;9:185–189. | ||
Symmons DP, Prior P, Scott DL, Brown R, Hawkins CF. Factors influencing mortality in rheumatoid arthritis. J Chronic Dis. 1986;39(2):137–145. | ||
Shi J, van de Stadt LA, Levarht EW, et al. Anti-carbamylated protein (anti-CarP) antibodies precede the onset of rheumatoid arthritis. Ann Rheum Dis. 2014;73(4):780–783. | ||
Humphreys JH, Verheul MK, Barton A, et al. Anticarbamylated protein antibodies are associated with long-term disability and increased disease activity in patients with early inflammatory arthritis: results from the Norfolk Arthritis Register. Ann Rheum Dis. 2016;75(6):1139–1144. | ||
Ajeganova S, Humphreys JH, Verheul MK, et al. Anticitrullinated protein antibodies and rheumatoid factor are associated with increased mortality but with different causes of death in patients with rheumatoid arthritis: a longitudinal study in three European cohorts. Ann Rheum Dis. 2016;75(11):1924–1932. | ||
Vidal-Bralo L, Perez-Pampin E, Regueiro C, et al. Anti-carbamylated protein autoantibodies associated with mortality in Spanish rheumatoid arthritis patients. PLoS One. 2017;12(7):e0180144. | ||
Aletaha D, Neogi T, Silman AJ, et al. 2010 rheumatoid arthritis classification criteria: an American College of Rheumatology/European League Against Rheumatism collaborative initiative. Ann Rheum Dis. 2010;69(9):1580–1588. | ||
Aletaha D, Smolen J. The Simplified Disease Activity Index (SDAI) and the Clinical Disease Activity Index (CDAI): a review of their usefulness and validity in rheumatoid arthritis. Clin Exp Rheumatol. 2005;23(5 Suppl 39):S100–S108. | ||
Wolfe F, Kleinheksel SM, Cathey MA, Hawley DJ, Spitz PW, Fries JF. The clinical value of the Stanford Health Assessment Questionnaire Functional Disability Index in patients with rheumatoid arthritis. J Rheumatol. 1988;15(10):1480–1488. | ||
Jaisson S, Lorimier S, Ricard-Blum S, et al. Impact of carbamylation on type I collagen conformational structure and its ability to activate human polymorphonuclear neutrophils. Chem Biol. 2006;13(2):149–159. | ||
Favoino E, Digiglio L, Cuomo G, et al. Autoantibodies recognizing the amino terminal 1-17 segment of CENP-A display unique specificities in systemic sclerosis. PLoS One. 2013;8(4):e61453. | ||
Ibrahim SE, Morshedy NA, Farouk N, Louka AL. Anti-carbamylated protein antibodies in psoriatic arthritis patients: relation to disease activity, severity and ultrasonographic scores. Egypt Rheumatol. 2018;40(1):17–21. | ||
Wolfe F, Mitchell DM, Sibley JT, et al. The mortality of rheumatoid arthritis. Arthritis Rheum. 1994;37(4):481–494. | ||
Myasoedova E, Davis JM 3rd, Crowson CS, Gabriel SE. Epidemiology of rheumatoid arthritis: rheumatoid arthritis and mortality. Curr Rheumatol Rep. 2010;12(5):379–385. | ||
Widdifield J, Bernatsky S, Paterson JM, et al. Trends in excess mortality among patients with rheumatoid arthritis in Ontario, Canada. Arthritis Care Res (Hoboken). 2015;67(8):1047–1053. | ||
Sparks JA, Chang SC, Liao KP, et al. Rheumatoid arthritis and mortality among women during 36 years of prospective follow-up: results from the Nurses’ Health Study. Arthritis Care Res (Hoboken). 2016;68(6):753–762. | ||
van Breukelen-van der Stoep DF, Zijlmans J, van Zeben D, et al. Adherence to cardiovascular prevention strategies in patients with rheumatoid arthritis. Scand J Rheumatol. 2015;44(6):443–448. | ||
Pecani A, Alessandri C, Spinelli FR, et al. Prevalence, sensitivity and specificity of antibodies against carbamylated proteins in a monocentric cohort of patients with rheumatoid arthritis and other autoimmune rheumatic diseases. Arthritis Res Ther. 2016;18(1):276. |
 © 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2018 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.