")
Back to Journals » International Journal of General Medicine » Volume 17
Low Estradiol Level and Endometrial Thickness on the Day of Endometrial Transformation Influence Clinical Pregnancy After Intrauterine Insemination
Authors Tang Q, Yi H, Chen S, Zheng Y, Wen Y, Yang M
Received 20 November 2023
Accepted for publication 11 April 2024
Published 15 April 2024 Volume 2024:17 Pages 1441—1449
DOI https://doi.org/10.2147/IJGM.S450912
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Woon-Man Kung
Qiaofei Tang,1,2 Honggan Yi,1,2 Siping Chen,1,2 Yantian Zheng,1,2 Yitao Wen,1,2 Man Yang1,2
1Reproductive Medicine Center, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China; 2Meizhou Municipal Engineering and Technology Research Center for Molecular Diagnostics of Major Genetic Disorders, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, Meizhou, People’s Republic of China
Correspondence: Man Yang, Reproductive Medicine Center, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences, No. 63 Huangtang Road, Meizhou, Meijiang District, People’s Republic of China, Email [email protected]
Background: The causes of pregnancy failure after intrauterine insemination (IUI) are controversial. The purpose of this study was to investigate the influencing factors on clinical pregnancy after IUI.
Methods: This study retrospectively analyzed 1464 cycles of IUI performed at the Meizhou People’s Hospital between March 2014 and June 2023. The χ2 test and logistic regression analysis was applied to assess the associations between the some factors (maternal age, paternal age, cycle type (natural cycle or ovulation induction cycle), hormone level on the day of endometrial transformation (estradiol (E2), luteinizing hormone (LH), and progesterone (P)), endometrial thickness on the day of endometrial transformation, and forward motile sperm concentration after treatment) and pregnancy failure.
Results: Among the 1464 IUI cycles in this study, 268 cycles of assisted reproduction resulted in clinical pregnancy, with a clinical pregnancy rate of 18.3%. During the cycles with clinical pregnancy, there were 25 (12.9%) preterm births and 169 (87.1%) full-term births. The E2 level on the day of endometrial transformation in clinical pregnancy group was higher than that in the pregnancy failure group (658.79± 656.02 vs 561.21± 558.83 pg/mL)(P=0.025). The clinical pregnancy group had a higher percentage of endometrial thickness between 8 and 13mm on the day of endometrial transformation than the pregnancy failure group (83.2% vs 75.0%)(P=0.002). The results of regressions analysis showed that low E2 level on the day of endometrial transformation (< 238.3 pg/mL vs ≥ 238.3 pg/mL: OR 1.493, 95% CI: 1.086– 2.052, P=0.014), and endometrial thickness < 8mm on the day of endometrial transformation (< 8mm vs 8– 13mm: OR 1.886, 95% CI: 1.284– 2.771, P=0.001) may increase risk of pregnancy failure performed IUI.
Conclusion: Low estradiol level, and endometrial thickness on the day of endometrial transformation may increase risk of pregnancy failure performed intrauterine insemination.
Keywords: intrauterine insemination, pregnancy failure, estradiol, endometrial thickness
Introduction
Infertility is defined by the World Health Organization (WHO) as a couple who is unable to conceive after having regular sexual intercourse for 12 months without using any form of contraception.1 It is estimated that 8% to 12% of couples with reproductive age worldwide are affected by infertility.2 Recently, the WHO issued new estimates that about one in six people worldwide experience infertility at some point in their lives.3 And the global burden of infertility disease has been increasing.4 The prevalence of infertility among couples of childbearing age in China is about 25%.5 Although infertility is not life-threatening, for patients with infertility, increased psychological stress and deteriorating relationships between family members can greatly affect their quality of life. Therefore, the harmful effects of infertility on patients, their families and society cannot be underestimated.6,7 Assisted reproductive technology (ART) is one of the main methods of assisted pregnancy for infertility patients.8
Intrauterine insemination (IUI) is an assisted reproductive technology in which sperm is artificially injected into the uterine cavity after a series of optimization treatments, and then naturally combined with the egg to form a fertilized egg and implantation.9 IUI is mainly used in male patients with mild asthenospermia, female patients with cervical infertility, and patients with psychological factors leading to sexual dysfunction and unexplained infertility.10,11 IUI has the characteristics of simple, non-invasive, low cost, and closer to natural conception, but its clinical pregnancy rate is low (8% to 25%).12 The high rate of pregnancy failure after IUI increases the psychological pressure of infertility patients, so it is very important to actively explore the influencing factors of pregnancy failure after IUI. Studies have shown that female age and smoking influence pregnancy rates in IUI, while there was no significant correlation between ovarian stimulation regimens, endometrium and pregnancy rate.13,14 Study has shown that different follicle-stimulating hormone (FSH) influence reproductive outcomes of intrauterine insemination cycles.15 Other studies have shown that IUI pregnancy rates are associated with male age and ovarian stimulation regimens.16 The pregnancy rate after assisted reproduction is related to the immunophenotype of endometrial transformation.17,18 In addition, study has suggested that the pregnancy rate of IUI is not related to the above factors.19
To sum up, the success rate of IUI is affected by many factors, and there is no uniform conclusion on the influence of each factor on the pregnancy rate, and there are some different reports in different studies. Therefore, it is of great significance to explore the influencing factors of IUI to guide patients with infertility to develop personalized treatment plan and improve the success rate of pregnancy assistance. Therefore, the purpose of this study was to analyze the related influencing factors of pregnancy failure after IUI. In this study, infertility patients who received IUI in our hospital from March 2014 to June 2023 were selected as subjects.
Materials and Methods
As of June 2023, there were 1464 cycles with assisted reproductive outcomes among the IUI cycles carried out by the Reproductive Medicine Center of Meizhou People’s Hospital. In this study, we analyzed the relationship between some factors and outcomes of these cycles during assisted reproduction. This study is guided by the Declaration of Helsinki and approved by the Ethics Committee of Meizhou People’s Hospital.
Detailed information on parental characteristics and IUI procedures was collected from the electronic medical records of Reproductive Medicine Centers. Pregnancy outcomes were obtained from the follow-up database. The risk factors of pregnancy failure investigated in this study were maternal age, paternal age, cycle type (natural cycle or ovulation induction cycle), hormone level on the day of endometrial transformation (estradiol (E2), luteinizing hormone (LH), and progesterone (P)), endometrial thickness on the day of endometrial transformation, and forward motile sperm concentration after treatment.
Maternal age and paternal age was divided into 2 subgroups (≤35 years, and >35 years), respectively. According to the pregnancy outcomes, they were divided into clinical pregnancy and pregnancy failure. Clinical pregnancy refers to positive blood human chorionic gonadotropin (hCG) on the 14th day after IUI, a vaginal ultrasound examination at the 4th week after IUI indicates that there is a pregnancy sac in the uterine cavity. Patients were treated in a natural cycle in case of regular cycles. Ovarian stimulation with clomiphene citrate (CC) or human menopausal gonadotrophin (HMG)/FSH protocols was used in cases of oligo ovulation or anovulation. With the CC protocol, a single dose of clomiphene citrate (50 mg or 100 mg) was administered on days 3, 4, 5, 6 and 7 of the cycle. HMG and/or FSH were administered in a minimal dose step-up regimen, starting off with 50 IU or 75 IU on day 3 of the cycle. The partner’s semen sample was first collected and analyzed 30 minutes later, and being prepared using density gradients. The concentration and motility of all samples were checked. The soft catheter (Ellios®) was used for all IUI.
Demographics and clinical characteristics of pregnancies conceived through IUI were calculated by χ2 test. The distributions of continuous variables were evaluated by Student’s t-test or the Mann–Whitney U-test. Logistic regression analysis was applied to assess the associations between the risk factors and pregnancy failure. Data analysis was performed using SPSS 21.0 (IBM Inc., USA). P<0.05 was considered to represent statistical significance.
Results
Demographics and Clinical Characteristics of Infertility Patients Performed with IUI
In this study, there were 1296 (88.5%) cycles with the maternal age ≤ 35 years old, and 168 (11.5%) cycles with the maternal age > 35 years old. There were 1113 (76.0%) cycles with the paternal age ≤ 35 years old, and 351 (24.0%) cycles with the paternal age > 35 years old. The IUI cycles included 184 (12.6%) natural cycles and 1280 (87.4%) ovulation induction cycles. On the day of endometrial transformation, the average E2 level was 581.15±577.33pg/mL, the average LH level was 20.10±17.66mIU/mL, and the average P level was 0.79±0.82ng/mL. On the day of endometrial transformation, there were 298 (20.4%), 1121 (76.6%) and 45 (3.1%) cycles with endometrial thickness less than 8mm, 8–13mm and greater than 13mm, respectively. There were 772 (52.7%) and 692 (47.3%) cycles with forward motile sperm concentration after treatment less than 30 ×106/mL and not lower than 30 ×106/mL, respectively. In the outcome of assisted reproduction, there were 268 (18.3%) cycles with clinical pregnancy, 26 (1.8%) cycles with biochemical pregnancy, and 1170 (79.9%) cycles with pregnancy failure. During the cycles with clinical pregnancy, there were 25 (12.9%) preterm births and 169 (87.1%) full-term births (Table 1).
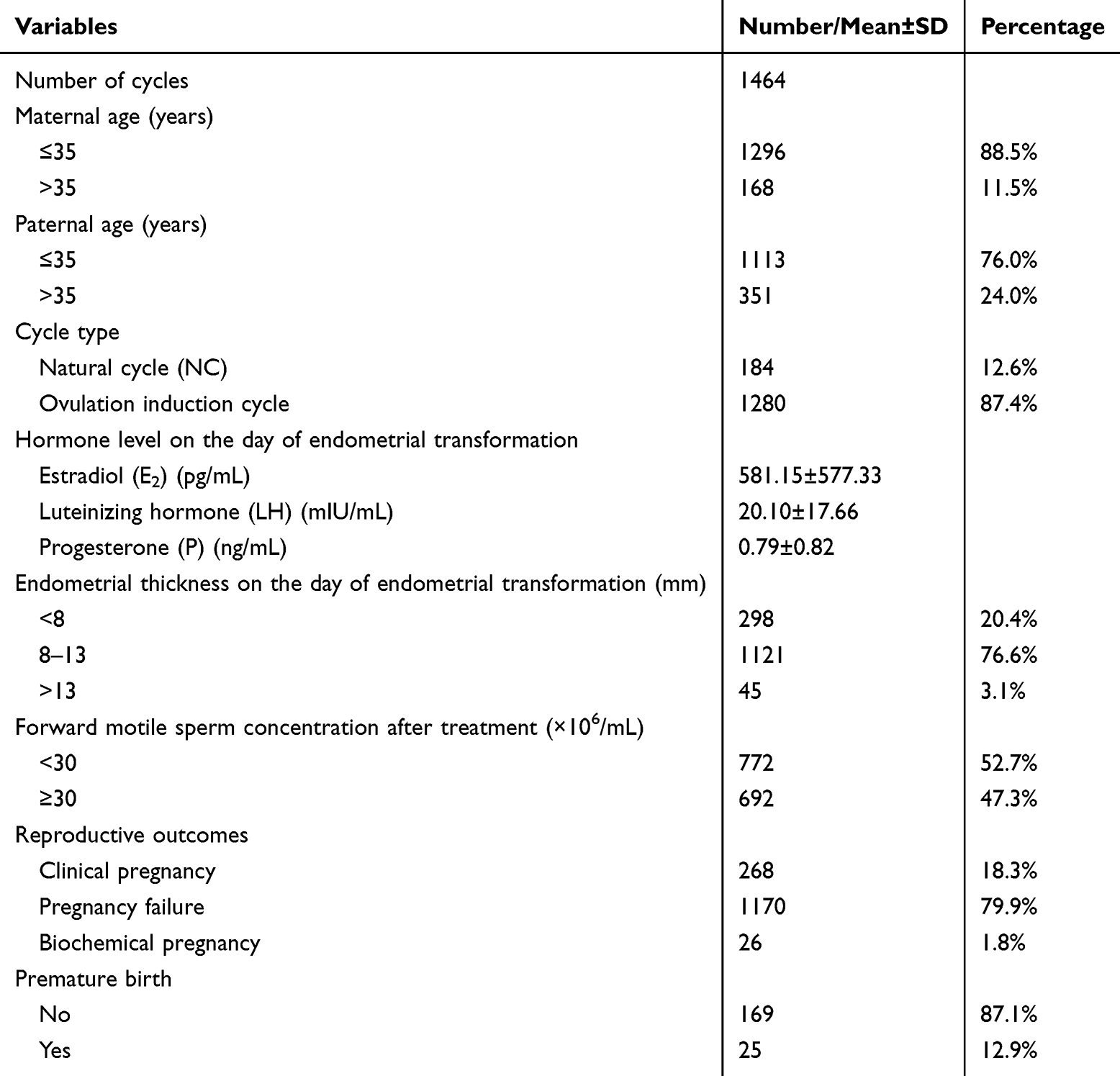 |
Table 1 Demographics and Clinical Characteristics of Infertility Patients in This Study |
Comparison of characteristics between clinical pregnancy and pregnancy failure groups among infertility patients performed IUI
The demographic and clinical characteristics of infertility patients who experienced clinical pregnancy and pregnancy failure after IUI treatment were compared. Among the cycles with clinical pregnancy, there were 246 (91.8%) cycles with the maternal age ≤ 35 years old and 22 (8.2%) cycles with the maternal age > 35 years old; there were 215 (80.2%) cycles with the paternal age ≤ 35 years old and 53 (19.8%) cycles with the paternal age > 35 years old. In the cycles with pregnancy failure, there were 1029 (87.9%) cycles with the maternal age ≤ 35 years old and 141 (12.1%) cycles with the maternal age > 35 years old; there were 882 (75.4%) cycles with the paternal age ≤ 35 years old and 288 (24.6%) cycles with the paternal age > 35 years old. There was no relationship between the age of couples with infertility and the difference in IUI outcomes (P>0.05). Clinical pregnancy rate was higher in ovulation induction cycles (240/1257, 19.1%) than in natural cycles (28/181, 15.5%), but the difference was not statistically significant (P=0.263). The E2 level on the day of endometrial transformation in clinical pregnancy group was higher than that in the pregnancy failure group (658.79±656.02 vs 561.21±558.83 pg/mL) (P=0.025). The clinical pregnancy group had a higher percentage of endometrial thickness between 8 and 13mm on the day of endometrial transformation than the pregnancy failure group (83.2% vs 75.0%)(P=0.002). And there was no difference found in LH and P levels on the day of endometrial transformation, and forward motile sperm concentration after treatment between the two groups (all P>0.05) (Table 2).
 |
Table 2 Comparison of Characteristics Between Clinical Pregnancy and Pregnancy Failure Groups Among Infertility Patients Performed IUI |
Comparison of Demographic and Clinical Characteristics of Full-Term Birth Group and Premature Birth Group
There was no difference found in maternal age, paternal age, cycle type, hormone level on the day of endometrial transformation, and endometrial thickness on the day of endometrial transformation between full-term birth group and premature birth group (all P>0.05). The proportion of forward motile sperm concentration after treatment not lower than 30 ×106/mL was higher in full-term birth group than that in premature birth group (47.9% vs 36.0%), but the difference was not statistically significant (P=0.290) (Table 3).
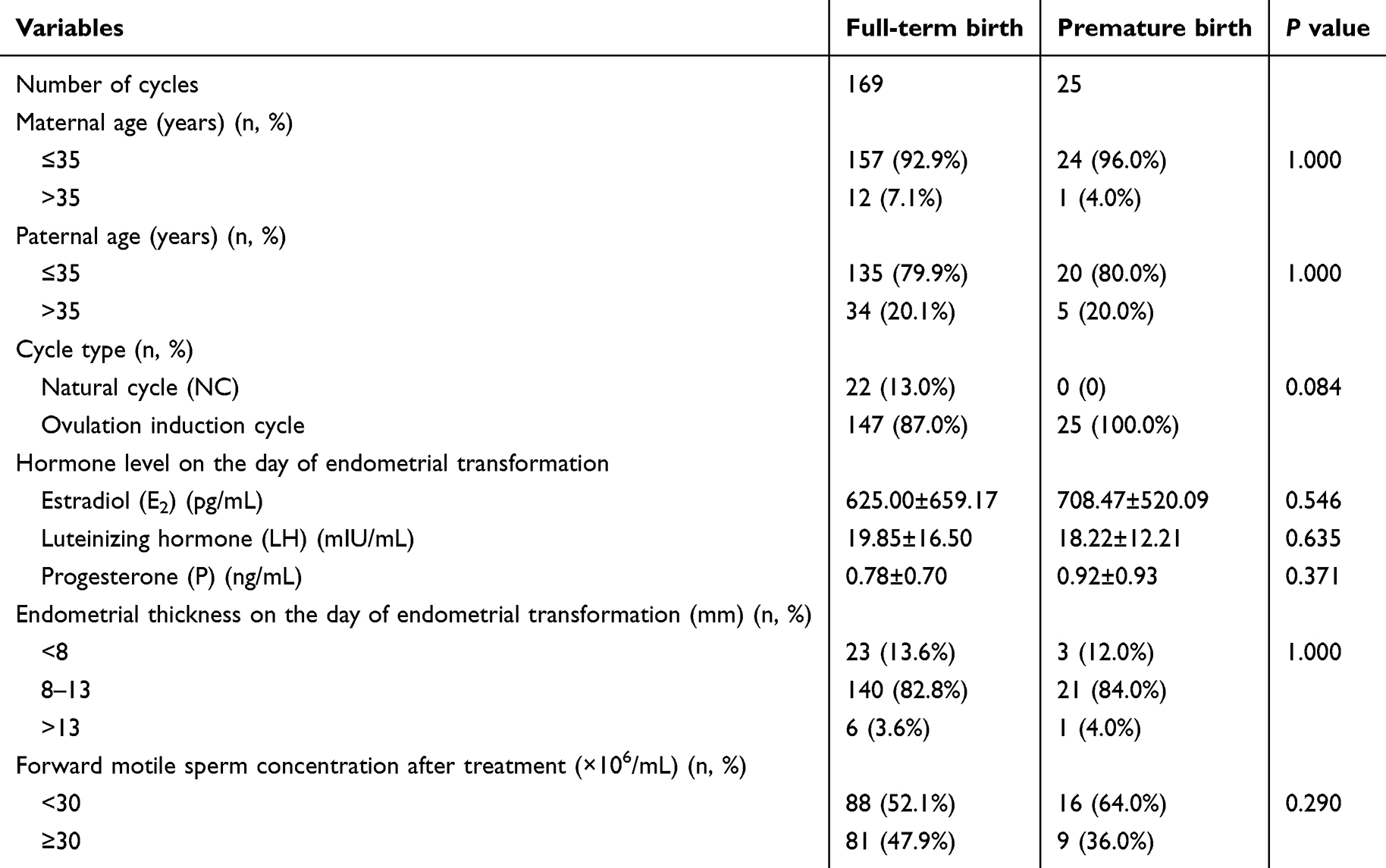 |
Table 3 Comparison of Demographic and Clinical Characteristics of Full-Term Birth Group and Premature Birth Group |
Logistic Regression Analysis of Risk Factors for Pregnancy Failure and Premature Birth
Receiver operating characteristic (ROC) curve analysis was used to determine the optimal cut-off value of E2 level. When clinical pregnancy was taken as the end point of E2 level, the cut-off value of E2 was 238.3 pg/mL. To gain insight into the independent influence of clinical characteristics on pregnancy failure, logistic regression analysis was performed. The results of univariate logistic analysis indicated that low E2 level on the day of endometrial transformation and endometrial thickness <8mm on the day of endometrial transformation may have some effect on pregnancy failure after performed IUI. The results of multiple logistic regression analysis showed that low E2 level on the day of endometrial transformation (<238.3 pg/mL vs ≥238.3 pg/mL: OR 1.493, 95% CI: 1.086–2.052, P=0.014), and endometrial thickness <8mm on the day of endometrial transformation (<8mm vs 8–13mm: OR 1.886, 95% CI: 1.284–2.771, P=0.001) may increase risk of pregnancy failure performed IUI. In addition, the results of logistic regression analysis showed no association between the clinical characteristics and the risk of preterm birth (Table 4).
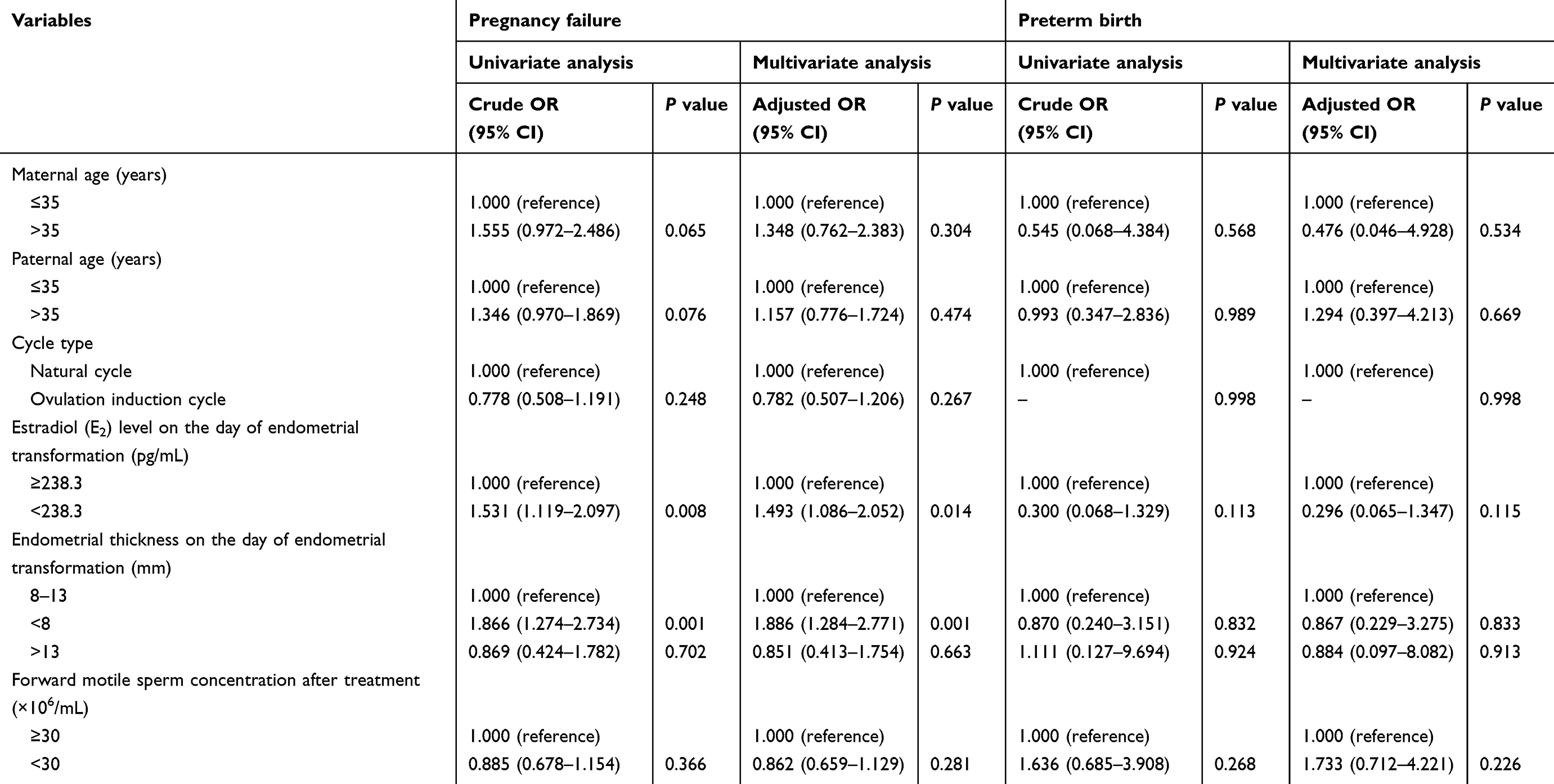 |
Table 4 Logistic Regression Analysis of Risk of Pregnancy Failure and Preterm Birth After IUI |
Discussion
Compared with in vitro fertilization/intracytoplasmic sperm injection embryo transfer (IVF/ICSI-ET), IUI has the advantages of simple, safe, and non-invasive,20,21 and is still the first line of infertility couples to assist pregnancy.22 There are many factors affecting the pregnancy outcome of IUI.13,16 We mainly analyzed the influencing factors of pregnancy after IUI, including the maternal age, paternal age, cycle type, hormone level on the day of endometrial transformation, endometrial thickness on the day of endometrial transformation, and forward motile sperm concentration after treatment in this study. The research results showed that low E2 level on the day of endometrial transformation <238.3 pg/mL, and endometrial thickness <8mm on the day of endometrial transformation may increase risk of pregnancy failure performed IUI.
Estradiol is an estrogen substance that can maintain endocrine balance, promote female follicle and genital development, and can be used to evaluate ovarian function. It would be suggested that the individuals with low E2 level may have premature menopause, premature ovarian failure, follicle development and other conditions that affect pregnancy.23 Arzu Yavuz et al showed that lower level of E2 significantly influenced the clinical pregnancy rate after IUI.24 Dickey RP et al found that E2 is associated with birth rate after IUI.25 In addition, study has found that an increase in E2 concentration on day 3 of the natural menstrual cycle is associated with clinical pregnancy rates during IUI treatment.26 Wolff EF et al showed that the pregnancy rate after IUI was significantly increased with the increasing serum E2 level.27 However, another study has found that the clinical pregnancy rate of IUI was not affected by serum E2 level.28
Endometrial thickness in the 10.5–13.9 mm range was associated with higher conception rates and clinical pregnancy rates.29 Studies have shown that endometrial thickness was positively correlated with pregnancy rate after IUI.16,30–32 Li et al found that the increase of endometrial thickness can significantly improve the clinical pregnancy rate after IUI.33 In addition, study has shown that endometrial thickness has no predictive value for IUI outcomes.34 Wolff EF et al showed that the pregnancy rate after IUI was significantly increased with the increasing endometrial thickness.27 Maher MA et al found that endometrial thickness had an effect on the outcome, as the likelihood of pregnancy increased with the increasing endometrial thickness.35 In a retrospective study from China, endometrial thickness <7mm or >14mm is associated with a lower pregnancy rate.36 In addition, there are some studies that show no relationship between endometrial thickness and pregnancy after IUI.37,38 In addition, Amerigo Vitagliano et al found that endometrial scratch injury was associated with a higher clinical pregnancy rate of IUI cycles.39 Therefore, it is necessary to consider “endometrial factor” in the process of IUI.40
There are some studies have shown that the total motile sperm was positively correlated with pregnancy outcome after IUI.30,41–43 Huniadi et al found that sperm concentration and motility are important factors in determining IUI outcome.32 Most studies agree that high sperm motility is the key to pregnancy after IUI, but different studies have shown different thresholds for total motile sperm count. Most data agree that IUI is appropriate for men with a total motile sperm count of more than 5 million and a post-wash sperm count of more than 1 million.9 Muthigi A et al found that IUI pregnancy is the best with total motile sperm not lower than 9 million, below this level, the pregnancy rate gradually decreased.44 Muthigi A et al suggested that IUI applies to couples when the total sperm count more than 5 million.45 In addition, there are some studies show no relationship between total motile sperm and pregnancy after IUI.38,46–49 In this study, there was no statistically significant difference of pregnancy rate between forward motile sperm concentration not lower than 30 million per milliliter group and forward motile sperm concentration lower than 30 million per milliliter group.
Through a cohort with a certain number of cycles and corresponding cycle characteristics data, the study results obtained some factors that may affect pregnancy after IUI. This study has several shortcomings. First of all, this is a retrospective study, not a randomized controlled study. Secondly, anti-mullerian hormone and ovulation related hormones are important indicators to evaluate ovarian reserve function, and relevant data were lacking in this study. In addition, due to the numerous factors affecting pregnancy, the influence of known or unknown confounding factors cannot be excluded, and the study results may still be biased.
Conclusions
In summary, the factors associated with pregnancy failure after intrauterine insemination were identified through a cohort study, the results showed that low estradiol level, and endometrial thickness on the day of endometrial transformation may increase risk of pregnancy failure performed intrauterine insemination. This study provides reference data for predicting pregnancy rate after intrauterine insemination by evaluating estradiol level and endometrial thickness.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was approved by the Ethics Committee of Medicine, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences. All participants signed informed consent in accordance with the Declaration of Helsinki.
Acknowledgments
The author would like to thank other colleagues whom were not listed in the authorship of Reproductive Medicine Center, Meizhou People’s Hospital, Meizhou Academy of Medical Sciences for their helpful comments on the manuscript.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was supported by the Science and Technology Program of Meizhou (Grant No.: 2019B0202001), and the Scientific Research Cultivation Project of Meizhou People’s Hospital (Grant No.: PY-C2021030).
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Szamatowicz M, Szamatowicz J. Proven and unproven methods for diagnosis and treatment of infertility. Adv Med Sci. 2020;65(1):93–96. doi:10.1016/j.advms.2019.12.008
2. Vander Borght M, Wyns C. Fertility and infertility: definition and epidemiology. Clin Biochem. 2018;62:2–10. doi:10.1016/j.clinbiochem.2018.03.012
3. Shah PK, Gher JM. Human rights approaches to reducing infertility. Int J Gynaecol Obstet. 2023;162(1):368–374. doi:10.1002/ijgo.14878
4. Sun H, Gong TT, Jiang YT, Zhang S, Zhao YH, Wu QJ. Global, regional, and national prevalence and disability-adjusted life-years for infertility in 195 countries and territories, 1990-2017: results from a global burden of disease study, 2017. Aging. 2019;11(23):10952–10991. doi:10.18632/aging.102497
5. Zhou Z, Zheng D, Wu H, et al. Epidemiology of infertility in China: a population-based study. BJOG. 2018;125(4):432–441. doi:10.1111/1471-0528.14966
6. Sharma A, Shrivastava D. Psychological problems related to infertility. Cureus. 2022;14(10):e30320. doi:10.7759/cureus.30320
7. Swift A, Reis P, Swanson M. Infertility-related stress and quality of life in women experiencing concurrent reproductive trauma. J Psychosom Obstet Gynaecol. 2022;43(2):171–176. doi:10.1080/0167482X.2021.2008901
8. Hilbert SM, Gunderson S. Complications of assisted reproductive technology. Emerg Med Clin North Am. 2019;37(2):239–249. doi:10.1016/j.emc.2019.01.005
9. Starosta A, Gordon CE, Hornstein MD. Predictive factors for intrauterine insemination outcomes: a review. Fertil Res Pract. 2020;6(1):23. doi:10.1186/s40738-020-00092-1
10. Kandavel V, Cheong Y. Does intra-uterine insemination have a place in modern ART practice? Best Pract Res Clin Obstet Gynaecol. 2018;53:3–10. doi:10.1016/j.bpobgyn.2018.08.003
11. Osmanlıoğlu Ş, Şükür YE, Tokgöz VY. Intrauterine insemination with ovarian stimulation is a successful step prior to assisted reproductive technology for couples with unexplained infertility. J Obstet Gynaecol. 2022;42(3):472–477. doi:10.1080/01443615.2021.1916805
12. Cabry-Goubet R, Scheffler F, Belhadri-Mansouri N, et al. Effect of gonadotropin types and indications on homologous intrauterine insemination success: A study from 1251 cycles and a review of the literature. Biomed Res Int. 2017;2017:3512784. doi:10.1155/2017/3512784
13. Guan H, Tang H, Pan L, Song H, Tang L. Pregnancy predictors in unexplained infertility after intrauterine insemination. J Gynecol Obstet Hum Reprod. 2021;50(8):102071. doi:10.1016/j.jogoh.2021.102071
14. Osaikhuwuomwan J, Osemwenkha A, Iribhogbe O, Aziken M, Orhue A. The effect of female age on the outcome of intrauterine insemination treatment in a public hospital-assisted reproduction technology unit. Niger J Clin Pract. 2018;21(8):988–992. doi:10.4103/njcp.njcp_248_16
15. Di Paola R, Garzon S, Giuliani S. Are we choosing the correct FSH starting dose during controlled ovarian stimulation for intrauterine insemination cycles? Potential application of a nomogram based on woman’s age and markers of ovarian reserve. Arch Gynecol Obstet. 2018;298(5):1029–1035. doi:10.1007/s00404-018-4906-2
16. Wang X, Zhang Y, Sun HL, et al. Factors affecting artificial insemination pregnancy outcome. Int J Gen Med. 2021;14:3961–3969. doi:10.2147/IJGM.S312766
17. Alfer J, Popovici RM, Fattahi A, et al. Endometrial delay is found to be part of a normal individual dynamic transformation process. Arch Gynecol Obstet. 2021;304(6):1599–1609. doi:10.1007/s00404-021-06086-8
18. Sudoma I, Goncharova Y, Dons’koy B, Mykytenko D. Immune phenotype of the endometrium in patients with recurrent implantation failures after the transfer of genetically tested embryos in assisted reproductive technology programs. J Reprod Immunol. 2023;157:103943. doi:10.1016/j.jri.2023.103943
19. Vichinsartvichai P, Siriphadung S, Traipak K, Promrungrueng P, Manolertthewan C, Ratchanon S. The influence of women age and successfulness of intrauterine insemination (IUI) cycles. J Med Assoc Thai. 2015;98(9):833–838. PMID: 26591391.
20. Bahadur G, Homburg R. Growing body of evidence supports intrauterine insemination as first line treatment and rejects unfounded concerns about its efficacy, risks and cost effectiveness. JBRA Assist Reprod. 2019;23(1):62–67. doi:10.5935/1518-0557.20180073
21. Leusder M, van Elten HJ, Ahaus K, Hilders CGJM, van Santbrink EJP. Protocol for improving the costs and outcomes of assistive reproductive technology fertility care pathways: a study using cost measurement and process mining. BMJ Open. 2023;13(6):e067792. doi:10.1136/bmjopen-2022-067792
22. Man JK, Parker AE, Broughton S, Ikhlaq H, Das M. Should IUI replace IVF as first-line treatment for unexplained infertility? A literature review. BMC Women's Health. 2023;23(1):557. doi:10.1186/s12905-023-02717-1
23. Parisi F, Fenizia C. The pathophysiological role of estrogens in the initial stages of pregnancy: molecular mechanisms and clinical implications for pregnancy outcome from the periconceptional period to end of the first trimester. Hum Reprod Update. 2023;29(6):699–720. doi:10.1093/humupd/dmad016
24. Yavuz A, Demirci O, Sözen H, Uludoğan M. Predictive factors influencing pregnancy rates after intrauterine insemination. Iran J Reprod Med. 2013;11(3):227–234. PMID: 24639750.
25. Dickey RP, Olar TT, Taylor SN, Curole DN, Rye PH, Matulich EM. Relationship of follicle number, serum estradiol, and other factors to birth rate and multiparity in human menopausal gonadotropin-induced intrauterine insemination cycles. Fertil Steril. 1991;56(1):89–92. doi:10.1016/s0015-0282(16)54423-9
26. Fukuda M, Fukuda K, Yding Andersen C, Byskov AG. Do basal oestradiol and oestradiol:androgens and oestradiol:FSH ratios reflect pregnancy potential of women receiving intrauterine insemination during natural cycles? Reprod Biomed Online. 2003;6(4):452–455. doi:10.1016/s1472-6483(10)62167-0
27. Wolff EF, Vahidi N, Alford C, Richter K, Widra E. Influences on endometrial development during intrauterine insemination: clinical experience of 2929 patients with unexplained infertility. Fertil Steril. 2013;100(1):194–199.e191. doi:10.1016/j.fertnstert.2013.03.023
28. Ozçakir HT, Göker EN, Terek MC, et al. Relationship of follicle number, serum estradiol level, and other factors to clinical pregnancy rate in gonadotropin-induced intrauterine insemination cycles. Arch Gynecol Obstet. 2002;266(1):18–20. doi:10.1007/pl00007493
29. Liu Y, Ye XY, Chan C. The association between endometrial thickness and pregnancy outcome in gonadotropin-stimulated intrauterine insemination cycles. Reprod Biol Endocrinol. 2019;17(1):14. doi:10.1186/s12958-019-0455-1
30. Esmailzadeh S, Faramarzi M. Endometrial thickness and pregnancy outcome after intrauterine insemination. Fertil Steril. 2007;88(2):432–437. doi:10.1016/j.fertnstert.2006.12.010
31. Huang X, Sun Q, Tang X, et al. Factors influencing the pregnancy outcome of intrauterine insemination and follow-up treatment. J Hum Reprod Sci. 2023;16(1):42–49. doi:10.4103/jhrs.jhrs_130_22
32. Huniadi A, Bimbo-Szuhai E, Botea M. Fertility predictors in intrauterine insemination (IUI). J Pers Med. 2023;13(3):395. doi:10.3390/jpm13030395
33. Li Q, Zhu M, Deng Z, et al. Effect of gonadotropins and endometrial thickness on pregnancy outcome in patients with unexplained infertility or polycystic ovarian syndrome undergoing intrauterine insemination. J Int Med Res. 2020;48(10):300060520966538. doi:10.1177/0300060520966538
34. Masrour MJ, Yoonesi L, Aerabsheibani H. The effect of endometrial thickness and endometrial blood flow on pregnancy outcome in intrauterine insemination cycles. J Family Med Prim Care. 2019;8(9):2845–2849. doi:10.4103/jfmpc.jfmpc_212_19
35. Maher MA, Abdelaziz A, Shehata YA. Effect of follicular diameter at the time of ovulation triggering on pregnancy outcomes during intrauterine insemination. Int J Gynaecol Obstet. 2017;139(2):174–179. doi:10.1002/ijgo.12291
36. Chen XJ, Wu LP, Lan HL, Zhang L, Zhu YM. Clinical variables affecting the pregnancy rate of intracervical insemination using cryopreserved donor spermatozoa: a retrospective study in China. Int J Fertil Steril. 2012;6(3):179–184. PMID: 24520436.
37. Zheng J, Cai J, Liu L, Guo Y, Sun J, Ren J. Low BMI is associated with poor IUI outcomes: a retrospective study in 13,745 cycles. J Assist Reprod Genet. 2022;39(12):2819–2825. doi:10.1007/s10815-022-02658-y
38. Do Amaral VF, Ferriani RA, Dos Reis RM, De Sala MM, De Moura MD. Effect of inseminated volume on intrauterine insemination. J Assist Reprod Genet. 2001;18(8):413–416. doi:10.1023/a:1016678519490
39. Vitagliano A, Noventa M, Saccone G, et al. Endometrial scratch injury before intrauterine insemination: is it time to re-evaluate its value? Evidence from a systematic review and meta-analysis of randomized controlled trials. Fertil Steril. 2018;109(1):84–96.e84. doi:10.1016/j.fertnstert.2017.09.021
40. Vitagliano A, Saccardi C, Noventa M, Di Spiezio Sardo A, Laganà AS, Litta PS. Does endometrial scratching really improve intrauterine insemination outcome? Injury timing can make a huge difference. J Gynecol Obstet Hum Reprod. 2018;47(1):33–34. doi:10.1016/j.jogoh.2017.11.001
41. Yousefi B, Azargon A. Predictive factors of intrauterine insemination success of women with infertility over 10 years. J Pak Med Assoc. 2011;61(2):165–168. PMID: 21375168.
42. Miller DC, Hollenbeck BK, Smith GD, et al. Processed total motile sperm count correlates with pregnancy outcome after intrauterine insemination. Urology. 2002;60(3):497–501. doi:10.1016/s0090-4295(02)01773-9
43. Mathes M, Kastrick E, Sayles H, Gustin S. How low is too low? Postwash total motile sperm count effect on pregnancy outcomes in intrauterine insemination. Hum Fertil. 2022;25:1–6. doi:10.1080/14647273.2022.2036492
44. Muthigi A, Jahandideh S, Bishop LA, et al. Clarifying the relationship between total motile sperm counts and intrauterine insemination pregnancy rates. Fertil Steril. 2021;115(6):1454–1460. doi:10.1016/j.fertnstert.2021.01.014
45. Hajder M, Hajder E, Husic A. The Effects of total motile sperm count on spontaneous pregnancy rate and pregnancy after IUI treatment in couples with male factor and unexplained infertility. Med Arch. 2016;70(1):39–43. doi:10.5455/medarh.2016.70.39-43
46. Gordon CE, Hammer KC, James K. Optimizing pregnancy outcomes in intrauterine insemination cycles by stratifying pre-wash total motile count and patient-specific factors: a patient counseling tool. J Assist Reprod Genet. 2022;39(12):2811–2818. doi:10.1007/s10815-022-02636-4
47. Kleppe M, van Hooff MH, Rhemrev JP. Effect of total motile sperm count in intra-uterine insemination on ongoing pregnancy rate. Andrologia. 2014;46(10):1183–1188. doi:10.1111/and.12212
48. Hassan N, Agbo C, Dahan MH. Pregnancy rates unaffected by sperm count in intrauterine insemination: a retrospective cohort study. Minerva Ginecol. 2017;69(1):6–12. doi:10.23736/S0026-4784.16.03892-2
49. Lin H, Li Y, Ou S, et al. The relationship of total progressive motile sperm count with the outcome of IUI? An analysis of 5171 cycles. Gynecol Endocrinol. 2022;38(11):954–959. doi:10.1080/09513590.2022.2126453
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.