Back to Journals » Clinical Ophthalmology » Volume 19
Longitudinal Choriocapillaris and Retinal Vascular Flow Changes on OCTA with Progression to Advanced AMD
Authors Johari Moghadam MM ![]() , Montazeri F, Feldman S, Lee SC, Yiu G, Moshiri A, Emami-Naeini P, Moussa K, Park SS
, Montazeri F, Feldman S, Lee SC, Yiu G, Moshiri A, Emami-Naeini P, Moussa K, Park SS ![]()
Received 12 September 2025
Accepted for publication 28 October 2025
Published 13 December 2025 Volume 2025:19 Pages 4651—4662
DOI https://doi.org/10.2147/OPTH.S562717
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Yousef Fouad
Mohammad Mehdi Johari Moghadam, Fateme Montazeri, Samuel Feldman, Sophie C Lee, Glenn Yiu, Ala Moshiri, Parisa Emami-Naeini, Kareem Moussa, Susanna S Park
Department of Ophthalmology & Vision Science, University of California Davis Eye Center, Sacramento, CA, USA
Correspondence: Susanna S Park, Department of Ophthalmology & Vision Science, University of California Davis Eye Center, Ernest E. Tschannen Eye Institute, 4860 Y Street, Sacramento, CA, 95817, USA, Tel +1 916 734 6080, Fax +1 916 703 5076, Email [email protected]
Purpose: To evaluate retinal and choriocapillaris (CC) vascular flow changes on optical coherence tomography angiography (OCTA) associated with progression of intermediate age-related macular degeneration (iAMD) to geographic atrophy (GA) or neovascular AMD (nAMD).
Patients and Methods: This retrospective, longitudinal cohort study included 68 eyes from 50 patients with iAMD at baseline who underwent OCTA and clinical examination at baseline and at 24 months. Quantitative analysis of CC flow deficits (FDs) and superficial capillary plexus vessel density (VD) was performed at baseline and after 24 months by comparing eyes that progressed to GA or nAMD to eyes that remained stable.
Results: Over 24 months, 7 eyes (10.3%) developed GA and 9 eyes (13.2%) developed nAMD, including 2 that progressed to both. Eyes that developed GA had significantly greater CC FD total area at baseline when compared with stable iAMD eyes (p=0.013) and developed significant decrease in parafoveal VD (p=0.026) and full macular VD (p=0.019) after GA onset. In contrast, eyes that developed nAMD showed no significant OCTA differences at baseline when compared to stable iAMD eyes but developed a new significant increase in CC FD total area (p=0.044) and FAZ perimeter (p=0.036) after nAMD onset (p=0.044).
Conclusion: In iAMD eyes progressing to GA, CC ischemia was detectable before GA onset, with subsequent retinal VD loss after GA development. In iAMD eyes progressing to nAMD, CC ischemia developed concurrent with neovascularization. OCTA-derived CC and retinal flow metrics may serve as non-invasive biomarkers to stratify iAMD eyes at risk for progression.
Keywords: choriocapillaris, geographic atrophy, neovascular AMD, OCT, OCTA
Introduction
Age-related macular degeneration (AMD) is a leading cause of irreversible vision loss, with a rising trend estimated to reach 288 million by 2040.1 While early stages of AMD often present with minimal visual symptoms, advanced forms, such as geographic atrophy (GA) and neovascular AMD (nAMD), can lead to significant visual impairment and reduced quality of life.2,3 For nAMD, long-term intravitreal administration of anti-angiogenic agents remains the preferred treatment.4 For GA, two recently approved therapies, pegcetacoplan and avacincaptad pegol, have been shown to slow GA lesion growth rate and may be particularly valuable for cases where the fovea is still spared.5 All these treatments require early administration to maximize the visual benefit. Thus, identifying eyes that are most likely to progress to advanced AMD would be important, such that appropriate treatment can be administered in a timely manner.6
Optical coherence tomography (OCT) and OCT angiography (OCTA) are non-invasive imaging modalities used to assess structural and vascular flow changes in the retina and choroid.7 Several OCT-based morphologic biomarkers, such as increased central drusen volume, intraretinal hyperreflective foci, and subretinal drusenoid deposits, have been identified to be associated with increased risk of AMD progression.8–10 More recently, OCTA studies have added valuable insights, revealing that choriocapillaris (CC) flow deficits (FDs) are associated with progression to GA and nAMD.11–13 Notably, CC FDs may precede the onset of retinal pigment epithelium (RPE) atrophy with more diffuse CC FD resulting in GA.12,13 Retinal vascular changes on OCTA were studied in eyes with GA and nAMD and retinal vascular alterations, such as enlargement of the foveal avascular zone (FAZ) and decreased macular retinal vascular flow density (VD), have been observed which appear to increase with longer follow-up, especially in GA eyes.14,15 These study findings highlight the possible role of CC and retinal vascular dysfunction in AMD progression.
In this study, we utilize OCTA to investigate both changes in CC and retinal vascular flow in eyes with intermediate AMD (iAMD) at baseline and after 24 months follow-up. Unlike previous longitudinal studies that evaluated either CC FD or retinal VD,13,15 our longitudinal study evaluates both the flow changes in CC and retina concurrently to provide a more comprehensive analysis of flow changes associated with AMD progression.
Materials and Methods
This study was approved by the University of California, Davis Institutional Review Board (IRB#992141). The approved protocol was titled “Clinical and Imaging Outcomes of Retinal Disease and Therapeutic Treatment”. Initial approval was granted on December 6, 2016, with multiple minor modifications, and the most recent approval was on February 15, 2024 (not requiring annual renewal). The study was conducted as a single-site, retrospective chart review. Thus, informed consent and HIPAA authorization were not applicable.
Patient Population
Our study population is a subset of the study population previously included in a published study on retinal VD in AMD patients.14,15 All patients with a diagnosis of AMD in the electronic health record based on International Classification of Diseases (ICD) 9-CM 362.5 or ICD-10-CM H35.3x and seen between January 2017 and July 2021 at the University of California Davis Eye Center were identified. Our study included all patients aged 55 and older with a diagnosis of iAMD at baseline, according to the Beckman classification criteria,16 and with a comprehensive eye exam, macular spectral-domain OCT (SD-OCT) and OCTA imaging at baseline and 24 months later. Patients who had media opacity, concurrent optic neuropathy, or retinopathy other than AMD at baseline and during study follow-up were excluded. Demographic and clinical data, including age, sex, eye laterality, best corrected visual acuity (BCVA, LogMAR), lens status, intraocular pressure (IOP), and AMD severity, were collected at baseline and 24 months follow-up upon review of the electronic health record and OCT/OCTA images (Figure 1).
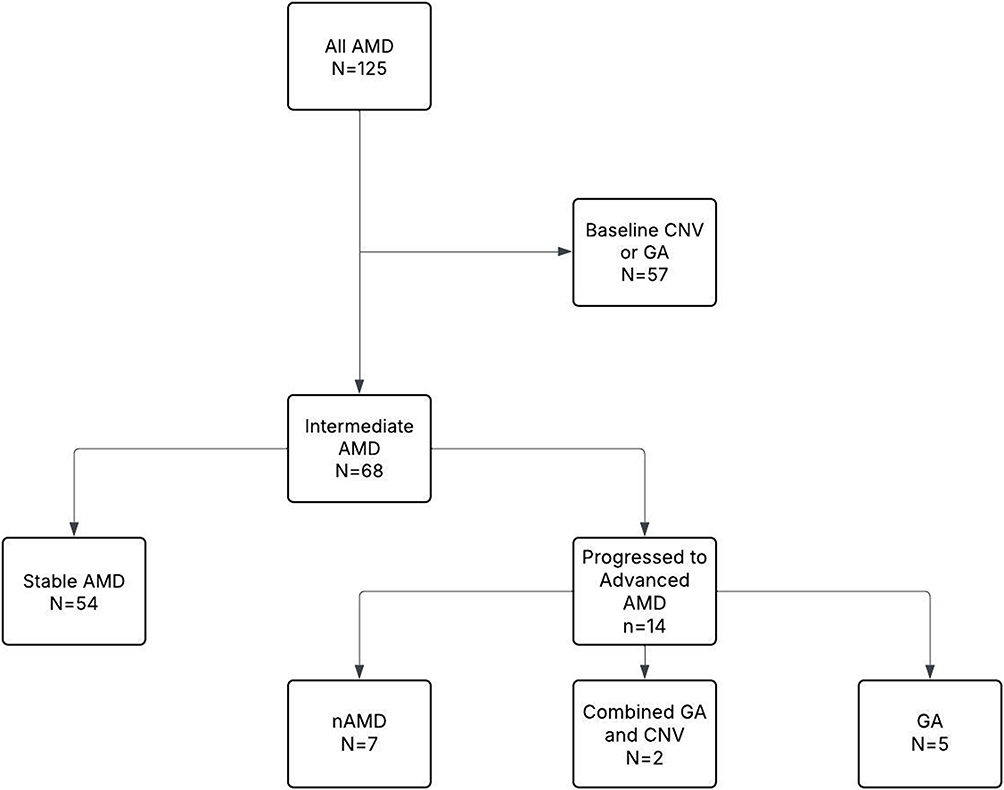 |
Figure 1 Study Flowchart. The original cohort of 125 eyes with age-related macular degeneration (AMD) and OCTA included 57 eyes with advanced AMD at baseline. The remaining 68 eyes with intermediate AMD were followed longitudinally for 24 months and classified into 3 study groups based on AMD stage at follow-up: stable intermediate AMD (54 eyes); progressed to advanced AMD (14 eyes including 5 eyes that progressed to geographic atrophy (GA), 7 eyes that progressed to neovascular AMD (nAMD) and 2 eyes that progressed to both GA and nAMD. |
Imaging Acquisition
Macular OCT and OCTA imaging were performed using the Zeiss Cirrus HD-OCT 5000 with Angioplex software (Carl Zeiss Meditec, v11.0). A 3×3 mm scan, composed of 245×245 A-scans, centered on the fovea, was used. All OCTA scans were reviewed by a trained image grader (MJ) to ensure data quality and consistency. Manual corrections were performed for any misalignment in foveal centration, segmentation errors in the superficial capillary plexus (SCP), or inaccurate delineation of FAZ. Eyes imaged only with 6×6 mm OCTA scans were excluded from analysis due to the lower image resolution expected with larger OCTA scan, which can reduce the accuracy of quantitative measurements such as retinal VD and FAZ metrics.17,18 Retinal VD in the SCP was quantified within three regions defined by the Early Treatment Diabetic Retinopathy Study (ETDRS) grid: the central 1-mm foveal zone, the 3-mm parafoveal ring, and the entire 3-mm circular macular area (full VD). Macular SD-OCT images were reviewed to obtain central subfield thickness (CST) and to evaluate for the presence of complete RPE and outer retinal atrophy (cRORA), incomplete RORA (iRORA), intraretinal fluid (IRF), and subretinal fluid (SRF). The CST was automatically measured using the OCT software and the ETDRS macular thickness map, while line scan OCT images were analyzed to assess GA. GA was defined as cRORA based on the Classification of Atrophy Meetings (CAM) group criteria for OCT assessment.19
Quantification of Choriocapillaris Flow Deficit on OCTA
En-face OCTA scan of the CC layer was extracted using structural and flow images from the OCTA device, with manual segmentation to define the CC slab in all eyes with nAMD and GA to ensure correct and consistent segmentation; a maximum projection was utilized on the segmented volume to produce the en face angiograms. ImageJ Fiji software (National Institutes of Health, Bethesda, MD, USA) was used to analyze CC FDs quantitatively. After segmenting the CC slab in the structural OCT images and locating the corresponding CC flow slab in the OCTA scan, signal compensation was used to correct for CC flow attenuation caused by structural changes in the RPE/Bruch’s membrane complex--, signal attenuation followed by inverse intensity transform enhances the en face structural image.12,20 The processed images were then Gaussian-blurred, multiplied by the CC flow image using the image calculator function, and binarized using the Phansalkar threshold (with a radius of 15 pixels). All CC flow parameters were calculated with and without above correction and four CC metrics were measured using the “Analyze Particles” function in ImageJ: (1) FD count, representing the total number of distinct CC FDs; (2) average FD size, defined as the mean area of individual CC FDs (in mm2); (3) total FD area, calculated as the sum of all individual CC FD areas to reflect the overall extent of CC nonperfusion (in mm2); and (4) FD percentage (FD%), determined by dividing the total FD area by the total image area and multiplying by 100, providing a normalized measure of nonperfusion. (Figure 2).
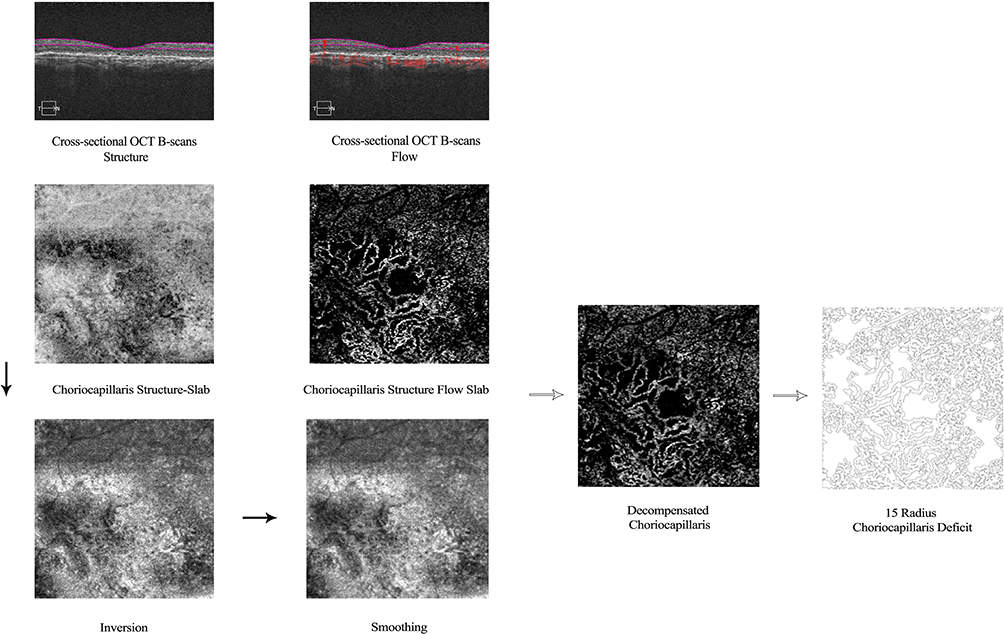 |
Figure 2 Measurement of Choriocapillaris Flow Deficits Using Image J; This figure illustrates the image processing pipeline for quantifying choriocapillaris (CC) flow deficits (FDs) using optical coherence tomography angiography (OCTA). On the left, structural OCT cross-sections and en face images of the CC are preprocessed through inversion and blurring to enhance vessel contrast. On the right, flow-based OCT cross-sections and corresponding en face images of the CC are generated. The two processed images are multiplied to create a decompensated CC map, highlighting FDs. The resulting map is then analyzed to calculate 15-radius CC loss deficits. |
Statistical Analysis
Descriptive statistics were used to characterize the study population, with continuous variables expressed as means and standard deviations (SD), and categorical variables reported as percentages. Appropriate statistical tests, including the Student’s t-test for continuous variables and the Pearson chi-square test for categorical variables, were applied. All statistical analyses were two-sided, with a p-value of less than 0.05 being considered statistically significant. Given the exploratory nature of this study, formal correction for multiple comparisons was not applied. Data analysis was performed using IBM SPSS Statistics for Windows, Version 29.
Results
A total of 68 eyes from 50 patients with iAMD at baseline were analyzed. The study included 54 stable iAMD eyes, 7 eyes that progressed to GA, and 9 eyes that progressed to nAMD (with combined cases represented in both advanced subgroups). The majority of eyes were from White patients (74.1% in stable group, 42.9% in GA group, and 44.4% in nAMD group), followed by much smaller proportions of Hispanic, Asian, and African American individuals. Patient demographics and ocular characteristics are summarized in Table 1. At baseline, the average age of patients was 76.2 ±8 years; the majority was female (35 patients, 70%). All eyes included in the study had iAMD at baseline. After 24 months of follow-up, 14 eyes (20.6%) progressed to advanced AMD: 7 eyes (10.3%) progressed to GA and 9 eyes (13.2%) progressed to nAMD, including 2 eyes that progressed to both GA and nAMD. None of the study eyes were pachychoroid. Patients with eyes that advanced to GA or nAMD were significantly older than patients with AMD eyes that remained stable (p= 0.043). Visual acuity tended to be worse in eyes that progressed to GA or nAMD compared to stable eyes (p= 0.010).
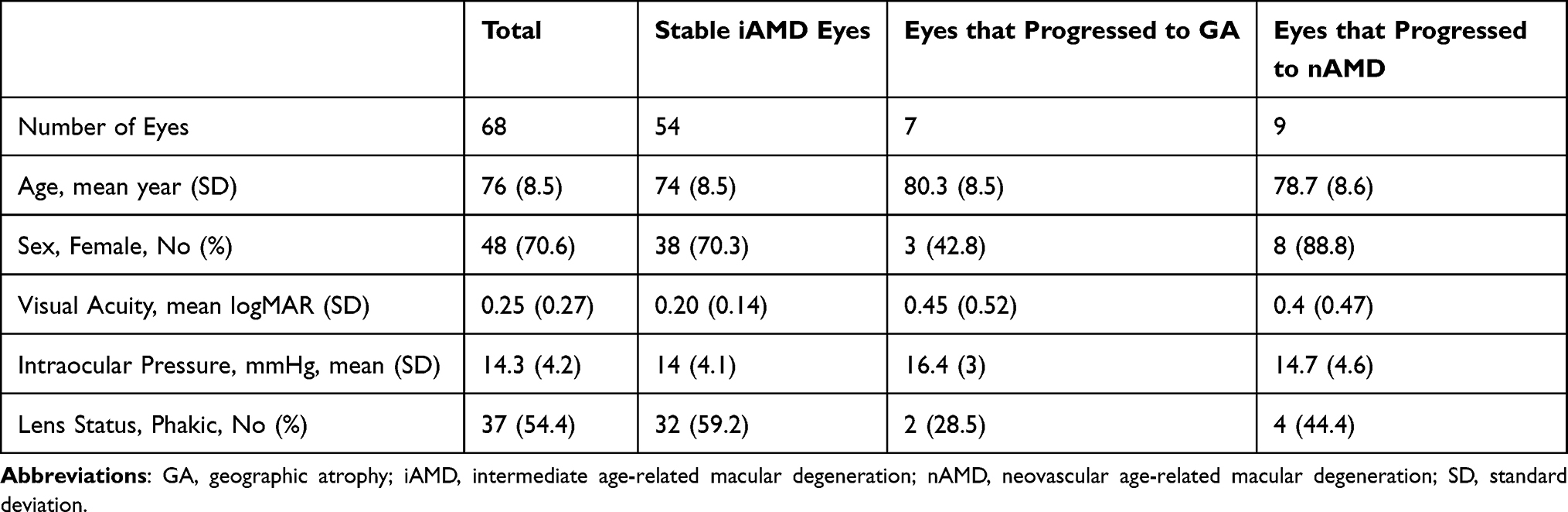 |
Table 1 Baseline Demographics and Clinical Characteristics of Study Eyes and Patients |
Eyes That Progressed to GA
At baseline, eyes that progressed to GA after 24 months follow-up had no significant difference in FAZ parameters and retinal VD when compared to stable iAMD eyes (Table 2; p > 0.05). After 24 months, the retinal VD for the full macular area imaged and parafoveal VD were significantly lower in eyes that developed GA when compared to stable eyes (full VD: p= 0.019; parafoveal VD: p= 0.026) (Table 3).
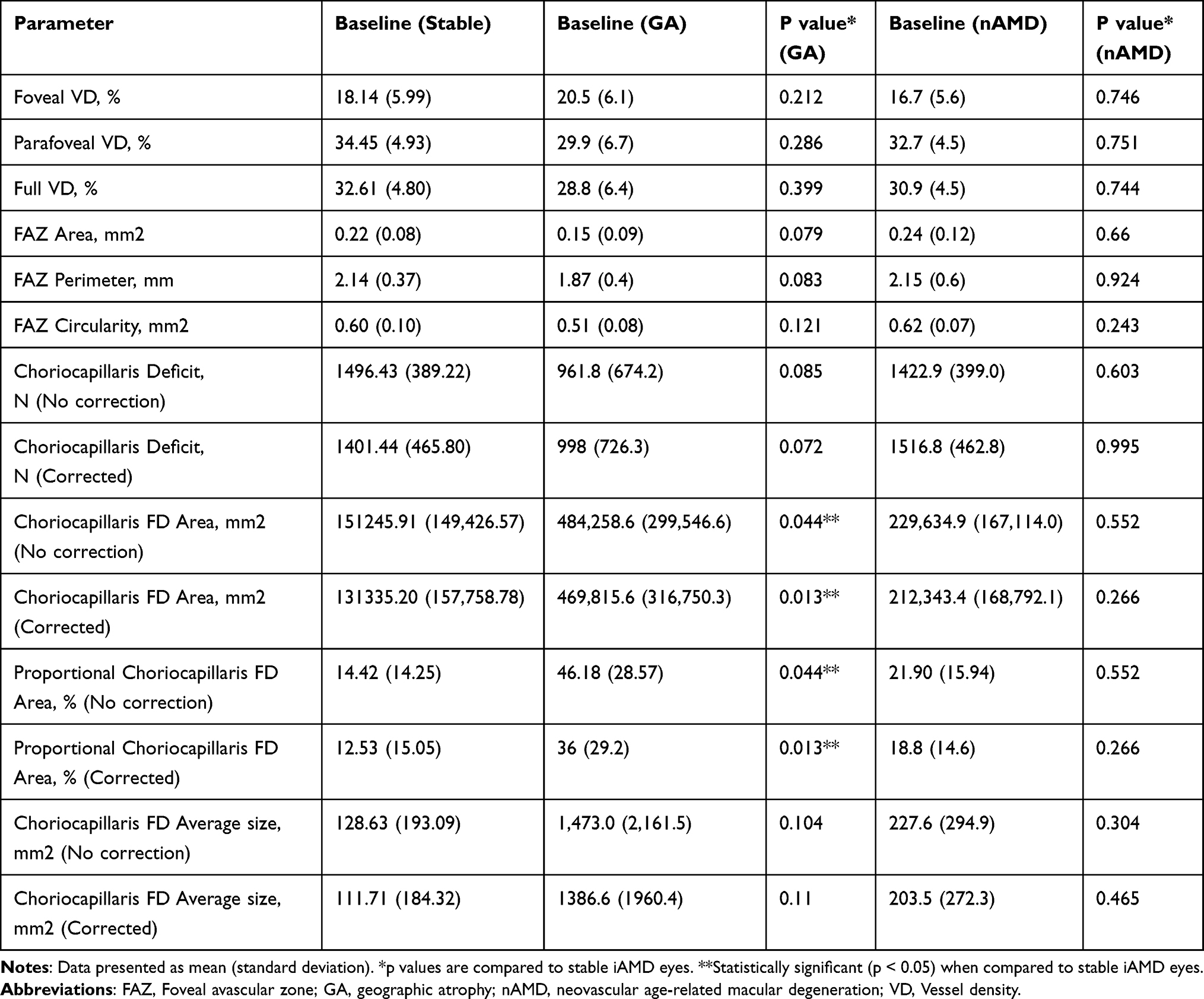 |
Table 2 Retinal and Choroidal Vascular Flow Parameters at Baseline in Intermediate AMD Eyes That Remained Stable or Progressed to GA or nAMD During Follow-Up |
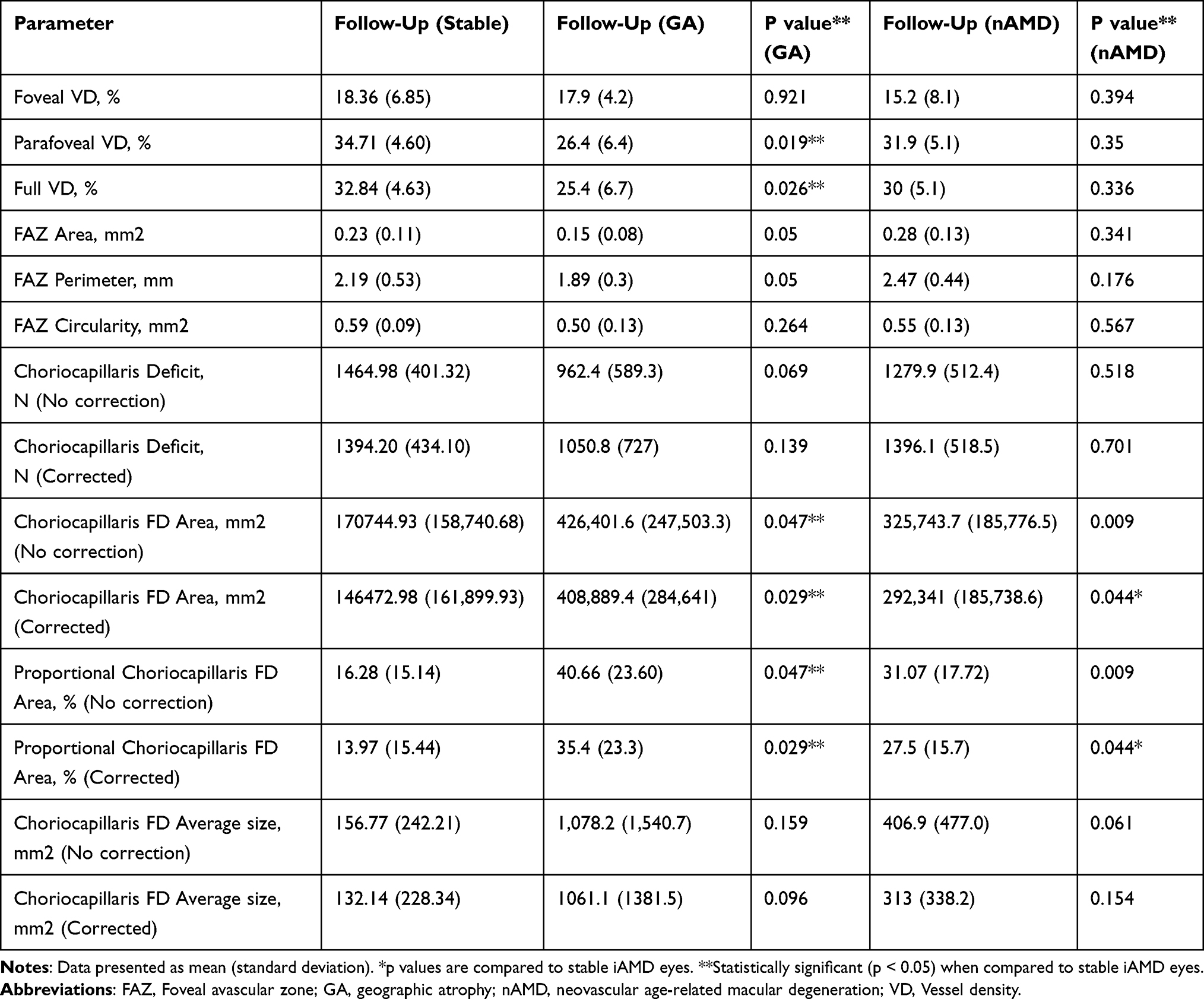 |
Table 3 Retinal and Choroidal Vascular Flow Parameters at 24-Month Follow-Up in Intermediate AMD Eyes That Remained Stable or Progressed to GA or nAMD |
For quantifying CC FD, image J analysis was used, either uncorrected or after correcting to minimize artifacts from overlying structural changes (see Methods). At baseline, the CC FD total area was significantly larger in iAMD eyes that developed GA when compared to stable iAMD eyes, regardless of whether shadowing artifacts correction was incorporated or not (corrected: p = 0.013; uncorrected: p = 0.044; Table 2). After 24-months follow-up, CC FD total area remained larger in eyes that developed GA when compared to stable iAMD eyes (corrected: p = 0.029; uncorrected: p = 0.047; Table 3; Figures 3 and 4).
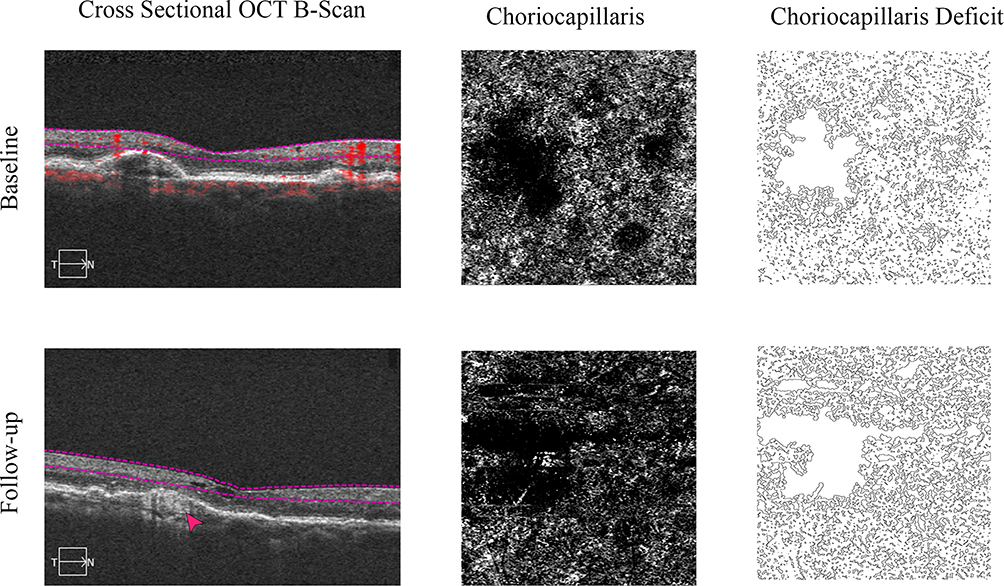 |
Figure 3 Longitudinal follow-up of OCT and OCTA images of a study eye that developed geographic atrophy (GA) and choroidal neovascularization (CNV) over two years follow-up. The top row represents baseline imaging, while the bottom row shows follow-up after two years in the same eye. (First column) B-Scan Structural OCT image, highlighting retinal layers changes. Choriocapillaris OCTA images illustrate vascular perfusion, with darker areas indicating reduced flow. Choriocapillaris flow deficit maps show regions of vascular loss, with white areas marking perfusion deficits. Over time, the OCT images reveal GA progression (Red arrow) and CNV development. Choriocapillaris flow deficit is extensive at baseline with some further increase during 2 years follow-up. |
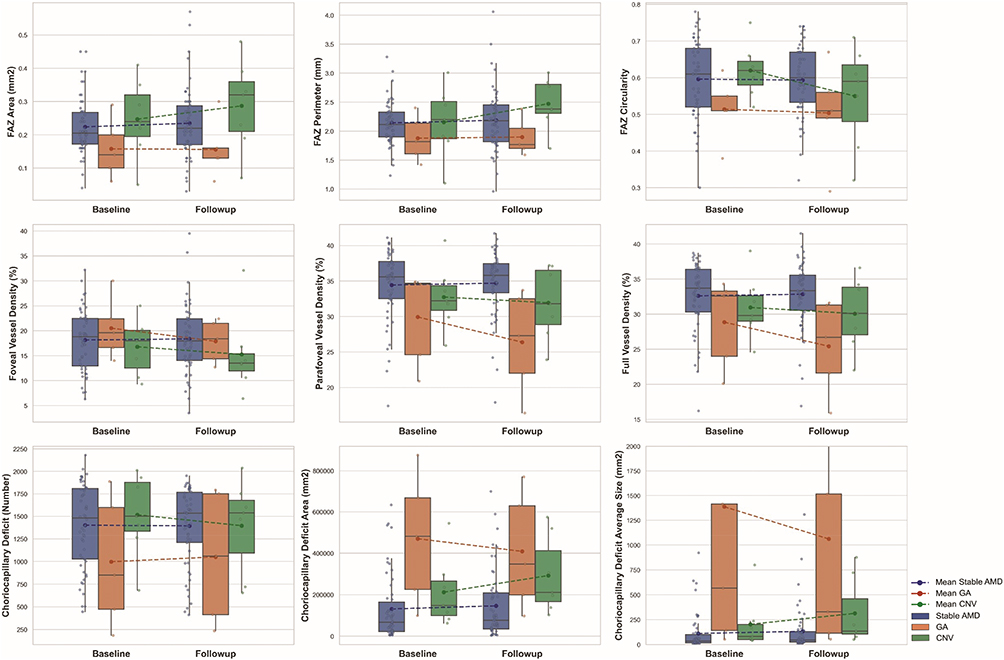 |
Figure 4 Box plots comparing OCTA parameters (foveal avascular zone (FAZ) parameters, retinal vessel density (VD), and choriocapillaris flow deficits) at baseline and after 24 months in eyes with age-related macular degeneration (AMD). The first row depicts FAZ metrics, including FAZ area, FAZ perimeter, and FAZ circularity, which showed no significant differences between stable intermediate AMD eyes (blue box) and eyes that progressed to geographic atrophy (GA; tan box) or neovascular AMD (nAMD; green box). The second row illustrates retinal vascular density (VD) changes, showing a significant reduction in parafoveal and full macular VD after 24 months in eyes that progressed to GA when compared to stable intermediate AMD eyes. The third row demonstrates choriocapillaris flow deficit parameters, revealing significantly larger total flow deficit area at baseline in eyes that later progressed to GA (tan box), and progressive increase in choriocapillaris flow deficit area and deficit size after 24 months follow-up in eyes that progressed to nAMD (green box). |
Eyes That Progressed to nAMD
Among iAMD eyes that progressed to nAMD after 24 months, baseline FAZ parameter, retinal VD and CC FD total area were not significantly different from iAMD eyes that remained stable after 24 months (Table 2; p > 0.05 for all OCTA parameters), However, after 24 months, there was a progressive increase in CC FD total area in eyes that developed nAMD, such that the CC FD total area became significantly higher in eyes that developed nAMD when compared to stable iAMD eyes (corrected: p = 0.044; uncorrected: p = 0.009) (Table 3, Figures 3 and 4).
Longitudinal Changes in Retinal and Choriocapillaris Vascular Parameters in Eyes Progressing to GA or nAMD
Table 4 and Figure 4 summarize the longitudinal changes in retinal and CC OCTA parameters in eyes that progress to GA or nAMD after 24 months when compared to stable iAMD eyes. In eyes that progressed to GA, there was a significant reduction in parafoveal (p = 0.038) and full macular VD (p = 0.042) over 24 months when compared to baseline. FAZ area, perimeter, and circularity remained stable over time in the GA group (all p > 0.05). Choriocapillaris flow deficit (CC FD) parameters, including number of deficits (corrected and uncorrected), total area, proportional area, and average size, showed no statistically significant change from baseline at 24 months follow-up among iAMD eyes that progressed to GA (all p > 0.05).
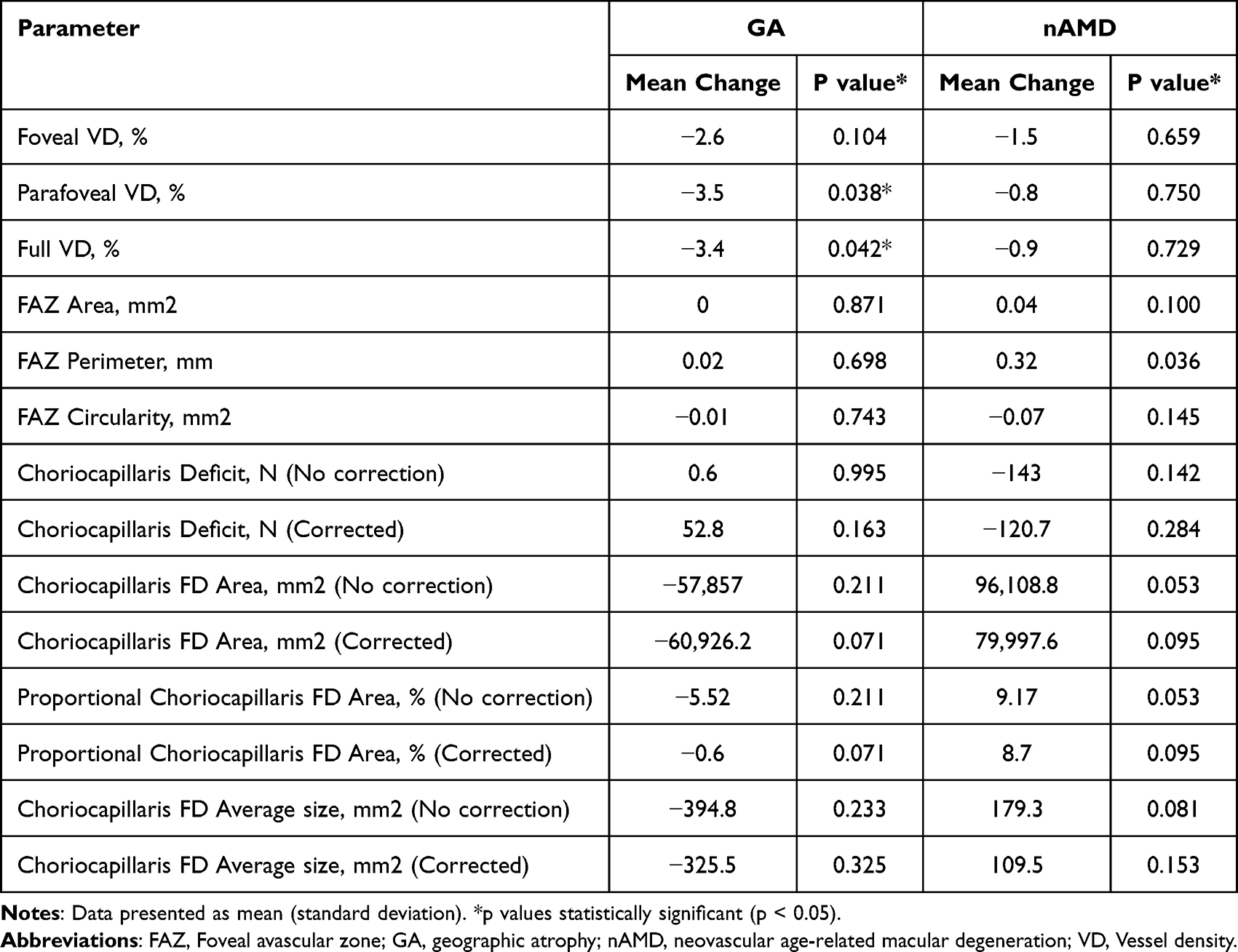 |
Table 4 Longitudinal Changes in Retinal and Choriocapillaris OCTA Parameters Over 24 Months in Intermediate AMD Eyes Progressing to GA or nAMD |
In iAMD eyes that progressed to nAMD, no significant changes were observed over 24 months in retinal VD in the fovea, parafovea, or full macula regions (all p > 0.05). FAZ perimeter increased significantly from baseline in these eyes as they developed nAMD (p = 0.036), but FAZ area and circularity did not change significantly. Among CC FD metrics, both uncorrected CC FD total area and proportional area showed a trend toward increase during 24 months follow-up with nAMD development (p = 0.053 and p = 0.053, respectively; Table 4 and Figure 4).
Discussion
This study used OCTA to quantitate the macular CC and retinal flow in eyes with iAMD at baseline and at 24 months follow-up to determine vascular flow changes that may be associated with progression of iAMD eyes to GA or nAMD. We performed both cross-sectional and longitudinal analysis by comparing OCTA parameters in the subgroup of eyes that progressed to GA or nAMD during the 24-month study to iAMD eyes that remained stable during the same follow-up period. This study provides the most comprehensive and longest longitudinal OCTA analysis of eyes with iAMD associated with AMD progression. Our results show that an increase in CC FD and a decrease in retinal VD can be observed in iAMD eyes that progress to advanced AMD, However, the time course of these changes on OCTA appears to differ in eyes that develop GA when compared to eyes that develop nAMD during 24 months follow-up. As such, the study findings provide some invaluable insight into retinal and choroidal vascular changes associated with the pathogenesis of GA versus nAMD.
In eyes that developed GA over 24 months follow-up, we observed a greater CC FD total area at baseline when compared to iAMD eyes that remained stable during follow-up. The baseline CC FD did not significantly increase further during the 24 months study follow-up as GA developed. In contrast, retinal VD and FAZ parameters at baseline were not significantly different in the eyes that developed GA when compared to stable iAMD eyes. After 24 months follow-up, the retinal VD showed a significant decrease at 24 months follow-up and after development of GA when compared to stable iAMD eyes. These findings suggest that CC ischemia likely precedes the development of GA. The relative retinal ischemia in the macula noted at 24 months follow-up appears to occur later and may be concurrent or secondary to GA development. This theory is supported by a prior OCTA report showing progressive decrease in retinal VD in GA eyes during a 2-year follow-up after development of GA.15
Our study findings also are consistent with prior histologic and OCTA reports also supporting the role of choroidal ischemia in GA development. The CC layer is essential for delivering oxygen and nutrients to the RPE layer and maintaining photoreceptor homeostasis.21 As such, CC flow impairment has been associated with vision loss from various retinal disorders, including AMD.22–25 Ramrattan et al found that CC vascular density decreases with age in normal postmortem eyes, a finding further supported by OCTA studies.26–28 Yet, it remains controversial whether CC degeneration is a primary cause of AMD progression or secondary to RPE and photoreceptor degeneration. Seddon et al examined donor eyes using UEA lectin staining and found a marked CC loss in eyes with GA, especially beneath the area of RPE atrophy.29 Surviving CC vessels showed reduced diameter, suggesting morphological and functional impairment. Bhutto et al, on the other hand, proposed that RPE damage occurs first in AMD, with CC degenerating as a secondary event.30
Our study findings suggest that CC degeneration and ischemia precede the development of GA. Intermediate AMD eyes that progressed to GA had significantly larger total area of CC FD at baseline when compared to stable iAMD eyes. This CC FD total area remained relatively stable at 24 months follow-up after GA developed clinically. Similar observations have been made in prior OCTA studies that examined CC FDs in iAMD eyes progressing to GA.12,13 Concurrent with development of GA at 24 months follow-up, our study also found a significant decrease in retinal VD in the macula in eyes with GA when compared to stable iAMD eyes. Based on our study data, we propose that CC damage leads to RPE and outer retina atrophy, which in turn would lowers metabolic demand of the overlying retina and trigger retinal vasoconstriction and reduced VD in the macula.
In contrast, iAMD eyes that progressed to nAMD had OCTA parameters that were not significantly different at baseline from stable iAMD eyes. However, at 24 months follow-up, these eyes that developed nAMD had a significant increase in CC FD when compared to stable iAMD eyes. Our findings suggest that the development of nAMD is concurrent with a progressive increase in CC ischemia. This is consistent with the mechanism proposed by Bhutto et al for nAMD development.30 Increasing RPE ischemia from CC loss will result in secretion of angiogenic factors, such as vascular endothelial growth factor (VEGF), that stimulate the development of choroidal neovascular membrane. Our findings differ from a small prior OCTA study showing no significant CC FD between nAMD and normal eyes.31 Interestingly, in our study, eyes that developed nAMD did not have significant difference in retinal VD or FAZ parameters when compared to stable iAMD eyes at baseline and after development of nAMD at 24 months. This latter finding differs somewhat from our previous larger cross-sectional study showing decreased retinal VD on OCTA in eyes with nAMD when compared eyes without nAMD.14 This difference may be due to the relatively smaller sample size and limited duration of nAMD of eyes in our current study. Longer duration of nAMD was associated with progressive changes in retinal VD in a longitudinal study.15
GA and nAMD are two subtypes of advanced AMD that share certain clinical features but exhibit distinct patterns of vascular pathology and choroidal involvement.30,31 The balance between residual vascular capacity, molecular signaling (eg VEGF), and genetic predisposition may ultimately determine whether CC ischemia in AMD eyes results in progression to neovascularization or atrophic degeneration. In contrast to the widespread choroidal thinning typically seen in GA, the choroid in nAMD eyes tend to show localized vascular remodeling and dilation in Haller’s and Sattler’s layers.31 This is likely due to the higher metabolic demands resulting from the neovascular complex and disruption of the neighboring CC. In line with this proposed model are recent findings that development of nAMD may slow down enlargement of GA by improving perfusion of the RPE and outer retina.32–37 In contrast, extensive CC loss would favor GA development.
Our study has several limitations. First, this was a retrospective study with a relatively small sample size, which may limit the statistical power and generalizability of our findings. Therefore, the results should be considered as exploratory and hypothesis-generating. Our study may not be powered to detect more subtle differences in OCTA parameters among study groups. Given the small sample size, formal correction for multiple comparisons was not performed. Nonetheless, we observed significant changes in CC FD and retinal VD among our study groups that correlate with the progression of AMD. Second, our study was limited to eyes that had 3×3 mm OCTA images. We used 3×3 OCTA images since smaller scans potentially can produce higher resolution OCTA images with more reliable quantitative OCTA parameters.17,18 In addition, prior studies in AMD eyes have shown most of the changes in CC occur in the central 3mm of the macula.27 As a result, our study limited our analysis to the central 3mm zone of the macula. The potential effect of perfusion changes in the peripheral macula on AMD progression was not evaluated. A prior report found that CC FD in central 3mm of macula was more likely to progress to nAMD while a more diffuse CC FD was more likely to progress to nAMD.13 The reported findings differ from our study where CC FD in the central 3mm at baseline was significantly increased in iAMD eyes that progressed to GA while no significant change in baseline CC FD was observed in eyes that eventually progressed to nAMD. Next, the OCTA software used in our study calculated only the retinal VD of SCP. Vascular flow density of the deep capillary plexus was not evaluated since unavailable. Finally, our study was limited to OCTA analysis at baseline and at 24 months follow-up. As a result, when OCTA changes are observed at 24 months follow-up, we cannot access whether the OCTA changes occurred before, concurrent or after progression to advanced AMD. Additionally, our cohort was composed mostly of self-identified white patients, reflecting the demographics of the patients seen at the study center. The study does not include AMD eyes with pachychoroid features. Thus, the study findings may not be applicable to other races where other phenotypes, such as polypoidal choroidal vasculopathy, are more prevalent. Inclusion of a more diverse populations in future studies would improve generalizability.
Our study strengths include the longitudinal design with two-year follow-up OCTA and clinical data and concurrent analysis of CC and retinal flow changes. This study design provides a more dynamic and complete assessment of CC and retinal vascular flow changes associated with AMD progression. As a result, we were able to observe a difference in the time course of development of CC and retinal ischemia in eyes that developed GA when compared to nAMD eyes. Based on our study findings, we may be able to identify intermediate AMD eyes at risk for progression to GA or nAMD based on the magnitude and time course of onset of choriocapillaris ischemia.
In our study, CC FD was calculated with and without artifact correction. The artifact correction may enhance measurement accuracy, but our study found that the uncorrected metrics still captured early CC ischemic changes valuable for AMD risk stratification.
Conclusion
In conclusion, this study demonstrates that increases in CC FDs and decreases in retinal VD on OCTA are associated with progression of iAMD eyes to advanced AMD. Eyes that developed GA had increased CC FD before GA development and new decreases in retinal VD after GA development when compared to stable iAMD eyes. In contrast, eyes that developed nAMD had no significant difference in OCTA parameters at baseline when compared to stable iAMD eyes but developed new progressive increase in CC FD during the 24 months follow-up with development of nAMD. Whether these OCTA biomarkers of AMD progression are stronger predictors of AMD progression than known morphologic OCT biomarkers are unknown at this time. Nonetheless, our findings highlight the critical role of microvascular dysfunction in the retina and CC in AMD progression, reinforcing the value of OCTA as a non-invasive tool for stratifying risk of progression of AMD eyes. Future larger studies with a more diverse AMD population would be needed to validate our study observations and determine the generalizability of the findings.
Acknowledgments
We thank the patients who participated in this study and the staff at the UC Davis Eye Center for their assistance with data collection and imaging procedures.
Funding
This work was supported in part by the Barbara A. & Alan M. Roth, MD Endowed Chair of Discovery, Education & Patient Care in Visual Science from the University of California Davis (SSP).
Disclosure
The authors report no conflicts of interest in this work. Susanna S. Park has/had contracted clinical research via her employer (University of California, Davis) from Roche/Novartis, Ophtea, and EyePoint; these projects have no overlap with the research summarized in this paper. The abstract of this paper was presented at the Association for Research in Vision and Ophthalmology (ARVO) Annual Meeting as a poster presentation on May 7, 2025, Salt Lake City, UT. The poster’s abstract was published in Invest. Ophthalmol. Vis. Sci. 2025; 66(8):4139. See https://iovs.arvojournals.org/article.aspx?articleid=2807324.
References
1. Bressler NM, Munoz B, Solomon SD, et al. Potential public health impact of age-related eye disease study results: AREDS report no. 11. Arch Ophthalmol. 2003;121(11):1621–1624. doi:10.1001/archopht.121.11.1621
2. Vu TA, Nguyen TT, Pham MT, et al. Vision-related quality of life impact of age-related macular degeneration in older adults aged 60-100 years: a cross-sectional study. Br J Ophthalmol. 2025;109(7):822–828. doi:10.1136/bjo-2024-325713
3. Sunness JS. The natural history of geographic atrophy, the advanced atrophic form of age-related macular degeneration. Mol Vis. 1999;5:25.
4. Bressler NM. Antiangiogenic approaches to age-related macular degeneration today. Ophthalmology. 2009;116(10 suppl):S15–S23. doi:10.1016/j.ophtha.2009.06.037
5. Shughoury A, Sevgi DD, Ciulla TA. The complement system: a novel therapeutic target for age-related macular degeneration. Expert Opin Pharmacother. 2023;24(17):1887–1899. doi:10.1080/14656566.2023.2257604
6. Bressler NM. Early detection and treatment of neovascular age-related macular degeneration. J Am Board Fam Pract. 2002;15(2):142–152. doi:10.3122/15572625-15-2-142
7. Langlo C, Amin A, Park SS. Optical coherence tomography retinal imaging: technological advancements and clinical applications. Ann Transl Med. 2025;13(17):e12345. doi:10.21037/atm-24-211
8. Abdelfattah NS, Zhang H, Boyer DS, et al. Drusen volume as a predictor of disease progression in patients with late age-related macular degeneration in the fellow eye. Invest Ophthalmol Vis Sci. 2016;57(4):1839–1846. doi:10.1167/iovs.15-18687
9. Lei J, Balasubramanian S, Abdelfattah NS, Nittala MG, Sadda SR. Proposal of a simple OCT-based scoring system for progression of age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2017;255(8):1551–1558. doi:10.1007/s00417-017-3671-y
10. Manafi N, Pakravan P, Golestaneh N, et al. Topographic analysis of local OCT biomarkers which predict progression to atrophy in age-related macular degeneration. Graefes Arch Clin Exp Ophthalmol. 2024;262(9):2083–2091. doi:10.1007/s00417-024-06656-0
11. Nassisi M, Tepelus T, Nittala MG, Sadda SR. Choriocapillaris flow impairment predicts the development and enlargement of drusen. Graefes Arch Clin Exp Ophthalmol. 2019;257(10):2079–2085. doi:10.1007/s00417-019-04391-1
12. Corvi F, Pellegrini M, Erba S, Cozzi M, Staurenghi G, Giani A. Choriocapillaris flow deficits as a risk factor for progression of age-related macular degeneration. Retina. 2021;41(4):686–693. doi:10.1097/IAE.0000000000002893
13. Romano F, Toto L, Di Antonio L, et al. Progressive choriocapillaris changes on OCT angiography correlate with stage progression in AMD. Invest Ophthalmol Vis Sci. 2024;65(6):21. doi:10.1167/iovs.65.6.21
14. Lee SC, Lee MW, Oh CM, et al. Retinal vessel density in exudative and nonexudative AMD using OCT angiography. Am J Ophthalmol. 2020;212:7–16. doi:10.1016/j.ajo.2019.12.014
15. Lee SC, Lee MW, Oh CM, et al. Long-term retinal vascular changes in AMD measured using OCT angiography. Ophthalmic Surg Lasers Imaging Retina. 2022;53(9):529–536. doi:10.3928/23258160-20220829-04
16. Ferris FL, Wilkinson CP, Bird A, et al. Clinical classification of age-related macular degeneration. Ophthalmology. 2013;120(4):844–851. doi:10.1016/j.ophtha.2012.10.036
17. Mukkamala L, Nguyen M, Chang M, Park SS. Repeatability of macular vascular density measurements of the three retinal layers using OCT angiography: effect of retinal vasculopathy and macular edema. Clin Ophthalmol. 2021;15:93–103. doi:10.2147/OPTH.S284021
18. Ho J, Dans K, You Q, Nudleman ED, Freeman WR. Comparison of 3×3 vs 6×6-mm OCT angiography scan sizes in evaluation of non-proliferative diabetic retinopathy. Retina. 2019;39(2):259–264. doi:10.1097/IAE.0000000000001984
19. Sadda SR, Guymer R, Holz FG, et al. Consensus definition for atrophy associated with AMD on OCT: classification of atrophy report 3. Ophthalmology. 2018;125(4):537–548. doi:10.1016/j.ophtha.2017.09.028
20. Zhang Q, Zheng F, Motulsky EH, et al. A novel strategy for quantifying choriocapillaris flow voids using swept-source OCT angiography. Invest Ophthalmol Vis Sci. 2018;59(1):203–211. doi:10.1167/iovs.17-22712
21. Strauss O. The retinal pigment epithelium in visual function. Physiol Rev. 2005;85(3):845–881. doi:10.1152/physrev.00021.2004
22. Nagai N, Mushiga Y, Ozawa Y. Diabetic choriocapillaris flow deficits affect the outer retina and correlate with HbA1c and systolic blood pressure. Sci Rep. 2023;13(1):22570. doi:10.1038/s41598-023-49242-2
23. Chu Z, Weinstein JE, Wang RK, Pepple KL. Quantitative analysis of the choriocapillaris in uveitis using en face swept-source OCT angiography. Am J Ophthalmol. 2020;218:17–27. doi:10.1016/j.ajo.2020.05.004
24. Baek J, Kook L, Lee WK. Choriocapillaris flow impairments associated with pachyvessel in early pachychoroid. Sci Rep. 2019;9(1):5565. doi:10.1038/s41598-019-42105-0
25. Nassisi M, Baghdasaryan E, Borrelli E, Ip M, Sadda SR. Choriocapillaris flow impairment surrounding GA correlates with disease progression. PLoS One. 2019;14(2):e0212563. doi:10.1371/journal.pone.0212563
26. Ramrattan RS, van der Schaft TL, Mooy CM, de Bruijn WC, Mulder PG, de Jong PT. Morphometric analysis of Bruch’s membrane, the choriocapillaris, and the choroid in aging. Invest Ophthalmol Vis Sci. 1994;35(6):2857–2864.
27. Kar D, Muller MS, Snyder-Valier B, et al. Choriocapillaris impairment, visual function, and distance to fovea in aging and age-related macular degeneration: ALSTAR2 baseline. Invest Ophthalmol Vis Sci. 2024;64(6):40. doi:10.1167/iovs.64.6.40
28. Tiosano L, Corradetti G, Sadda SR. Progression of choriocapillaris flow deficits in clinically stable intermediate AMD. Eye. 2021;35(12):2991–2998. doi:10.1038/s41433-020-01259-x
29. Seddon JM, McLeod DS, Bhutto IA, et al. Histopathological insights into choroidal vascular loss in clinically documented AMD. JAMA Ophthalmol. 2016;134(11):1272–1280. doi:10.1001/jamaophthalmol.2016.3357
30. Bhutto I, Lutty G. Understanding AMD: relationships between photoreceptor/RPE/Bruch’s membrane/choriocapillaris complex. Mol Aspects Med. 2012;33(4):295–317. doi:10.1016/j.mam.2012.04.005
31. Alagorie AR, Verma A, Nassisi M, Sadda SR. Quantitative assessment of choriocapillaris flow deficits in advanced AMD versus healthy eyes. Am J Ophthalmol. 2019;205:132–139. doi:10.1016/j.ajo.2019.04.005
32. Kaszubski P, Ben Ami T, Saade C, Smith RT. Geographic atrophy and choroidal neovascularization in the same eye: a review. Ophthalmic Res. 2016;55(4):185–193. doi:10.1159/000443210
33. McLeod DS, Grebe R, Bhutto I, Merges C, Baba T, Lutty GA. Relationship between RPE and choriocapillaris in age-related macular degeneration. Invest Ophthalmol Vis Sci. 2009;50(10):4982–4991. doi:10.1167/iovs.09-3639
34. Laiginhas R, Yang J, Rosenfeld PJ, Falcão M. Nonexudative macular neovascularization: a systematic review of prevalence, natural history, and recent insights from OCT angiography. Ophthalmol Retina. 2020;4(7):651–661. doi:10.1016/j.oret.2020.03.005
35. Yu E, Xu W, Zhu S, et al. Targeting the VEGFR2 signaling pathway for angiogenesis and fibrosis regulation in neovascular AMD. Sci Rep. 2024;14(1):25682. doi:10.1038/s41598-024-76258-4
36. Song D, Liu P, Shang K, Ma Y. Application and mechanism of anti-VEGF drugs in age-related macular degeneration. Front Bioeng Biotechnol. 2022;10:943915. doi:10.3389/fbioe.2022.943915
37. DeAngelis MM, Silveira AC, Carr EA, Kim IK. Genetics of age-related macular degeneration (AMD). Hum Mol Genet. 2017;26(R1):R45–R50. doi:10.1093/hmg/ddx228
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Vision-Related Quality of Life and Association Between Retinal Parameters in Patients with Non-Arteritic Anterior Ischemic Optic Neuropathy
Su Y, Bai G, Tian H, Zhang S, Liu Y, Zhang G, Liu L, Chen K
International Journal of General Medicine 2022, 15:5173-5179
Published Date: 24 May 2022
Changes in Ocular Biomarkers from Normal Cognitive Aging to Alzheimer’s Disease: A Pilot Study
Chaitanuwong P, Jariyakosol S, Apinyawasisuk S, Hirunwiwatkul P, Lawanlattanagul H, Hemrungrojn S, Chongpison Y
Eye and Brain 2023, 15:15-23
Published Date: 1 March 2023
Structural-Functional Correlation in Non-Arteritic Acute Ischemic Optic Neuropathy
Wei J, Zhang L, Wang H, Wang Q, Jia W, Wang R, Wang R, Cui Z
Eye and Brain 2025, 17:13-25
Published Date: 3 May 2025