Back to Journals » Nature and Science of Sleep » Volume 14
Longitudinal Associations Between Sleep Habits, Screen Time and Overweight, Obesity in Preschool Children
Authors Reyna-Vargas ME, Parmar A, Lefebvre DL, Azad MB, Becker AB, Turvey SE, Moraes TJ, Lou W, Subbarao P, Sears MR, Mandhane PJ, Narang I ![]()
Received 2 March 2022
Accepted for publication 13 June 2022
Published 5 July 2022 Volume 2022:14 Pages 1237—1247
DOI https://doi.org/10.2147/NSS.S363211
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Myrtha E Reyna-Vargas,1 Arpita Parmar,2 Diana L Lefebvre,3 Meghan B Azad,4– 6 Allan B Becker,4,5 Stuart E Turvey,7 Theo J Moraes,1 Wendy Lou,8 Padmaja Subbarao,1,8 Malcolm R Sears,3 Piushkumar J Mandhane,9 Indra Narang1,10
1Translational Medicine Program, The Hospital for Sick Children, Toronto, ON, Canada; 2Sculich School of Medicine and Dentistry, Western University, London, ON, Canada; 3Department of Medicine, McMaster University, Hamilton, ON, Canada; 4Department of Pediatrics and Child Health, University of Manitoba, Winnipeg, MB, Canada; 5Developmental Origins of Chronic Diseases in Children Network (DEVOTION), Children’s Hospital, Winnipeg, MB, Canada; 6Department of Food and Human Nutritional Sciences, University of Manitoba, Winnipeg, MB, Canada; 7Department of Pediatrics, BC Children’s Hospital, University of British Columbia, Vancouver, BC, Canada; 8Dalla Lana School of Public Health, University of Toronto, Toronto, ON, Canada; 9Department of Pediatrics, University of Alberta, Edmonton, AB, Canada; 10Faculty of Medicine, University of Toronto, Toronto, ON, Canada
Correspondence: Indra Narang, The Hospital for Sick Children, 555 University Ave-Hill Wing Room #4534, Toronto, ON, M5G 1X8, Canada, Email [email protected]
Introduction: Decreased sleep duration and increased screen time as early as preschool age may contribute to overweight and obesity. The effects of bedtime together with nocturnal sleep duration remain unclear with a paucity of data evaluating these associations longitudinally. We aim to evaluate the independent and joint effects of sleep duration, sleep bedtime, and screen time at 3 years of age on BMI status, particularly overweight and obesity by age 5 years.
Methods: Data from 2185 participants of the CHILD Cohort Study were analyzed longitudinally using generalized estimating equations (GEE). Models included changes in overweight/obesity status from 3 to 5 years of age as outcome, and nocturnal sleep duration, bedtime, and daily screen time at 3 years of age as explanatory variables. The joint effects of nocturnal sleep time and excess screen time, late bedtime on overweight/obesity were subsequently analyzed.
Results: The median nocturnal sleep time at 3 and 5 years of age was 11.0 hours/night [IQR 10.5, 11.5]. A total of 14.5% children went to bed after 9PM at 3 years and 7.2% at 5 years. Median screen time was 1.0 hr/day [IQR 1.0, 2.0] at both ages. Longitudinal analyses showed that sleeping less than 10.5 hours at age 3 years was associated with 46% greater odds of overweight/obesity by age 5 years (OR 1.46, 95% CI 1.07, 2.00). The risk was higher when coupled with late bedtime after 9pm (OR 1.60, 95% CI 1.12, 2.31). Children with both short nocturnal sleep duration and excess screen time (> 1hr/day) had twice the associated risk of overweight/obesity by age 5 years (OR 1.96, 95% CI 1.34, 2.88).
Conclusion: Nocturnal sleep duration and screen time are modifiable risk factors in young children, which may have important implications for obesity prevention as early as infancy.
Keywords: Nocturnal sleep, bedtime, BMI
Introduction
The prevalence of overweight and obesity in preschool children has grown to epidemic proportions in the past two decades, with over 40 million preschool children worldwide either overweight or obese.1 Concurrently, a similar epidemic of chronic sleep deprivation has been reported.2 Although the National Sleep Foundation recommends 10–13 hours of nocturnal sleep for preschool children,3,4 a study of over 5000 North American children observed an average of 9.5hrs of nocturnal sleep between 3 and 5 years of age.5 Moreover, recommendations of other components of sleep such as bedtime remain unclear.
While numerous cross-sectional studies have shown clear associations between shorter sleep duration and increased risk of higher body mass index (BMI),6–12 recent reviews highlight the lack of longitudinal studies with heterogeneous samples that have explored these associations.9,13 Furthermore, there is insufficient evidence on how sleep habits such as bedtime and other modifiable factors such as screen time act together to influence childhood obesity. Increased screen time, for example, has been associated with both obesity7 and decrements in sleep duration.9,12 Of relevance, preschool children in Canada spend an average of 2 hours per day using screen-based entertainment,14 and only 15% meet the current Canadian Sedentary Behaviour Guidelines for the Early Years of less than 1 hour of daily screen time.15
To date, three studies have analyzed the joint effect of bedtime and sleep duration on BMI16–18 with a lack of consistent conclusions across the studies, which may be attributed to modelling limitations as well as inadequate consideration of important confounders such as screen time. Two further studies assessed how sleep duration and screen time affect weight in preschool children using a longitudinal approach.10,11 However, neither of these studies evaluated the effect of a late bedtime, and were limited by restricting screen time to television viewing only.
The aim of this study is to prospectively evaluate the independent and joint effects of sleep duration, sleep bedtime, and screen time at 3 years of age on BMI status, particularly overweight and obesity by age 5 years.
Materials and Methods
This study uses data from the CHILD Cohort Study; a Canadian multidisciplinary, longitudinal, population-based birth cohort study.19 The CHILD Cohort Study recruited 3264 mothers and their infants (born >35 gestational weeks) from four sites across Canada (Vancouver, Edmonton, Manitoba, and Toronto) between 2008 and 2012 and has been previously described in detail.19 This study was approved by the Human Research Ethics Boards at McMaster University and the Universities of Manitoba, Alberta and British Columbia, and the Hospital for Sick Children (Toronto), and informed consent was obtained from a parent or legal guardian. All procedures and data collection were followed according to the Helsinki Declaration of the World Medical Association.
Outcome Variables
The primary outcome of this study was overweight/obesity status at 3 and 5 years of age. Trained research assistants performed weight and height measurements at clinic visits in each center when children were 3 and 5 years old. All children were required to remove shoes and outerwear for weight (Scaletronix scale) and height (standard stadiometer) measurements.
Age and sex adjusted BMI z-scores (BMI-z) were calculated following the World Health Organization (WHO) classification system for children.20 Following WHO growth indicators for children under 5 years of age and those between 5 and 19 years of age, BMI-z were used to classify subjects into normal (≤2 standard deviation [SD] at 3 years, ≤1SD at 5 years) and overweight/obesity (>2SD at 3 years, >1SD at 5 years).21
Exposure Variables
Bedtime, nocturnal sleep duration (NSD), and screen time at 3 and 5 years of age were the main exposure variables in this study. Sleep information was obtained through parent reported questionnaires, where they were asked to write down the child’s usual bedtime, wake time, and usual naptime on weekdays per 24-hour period. Subjects were classified into sleep categories based on tertiles of nocturnal sleep duration to account for the wide distribution of sleep duration data. NSD was categorized into: less than or equal to 10.5 hours, more than 10.5–11.0 hours, and more than 11.0 hours, similar to classifications used in published studies.10,22 Subjects were also classified according to their usual bedtime as early (≤9PM) and late (>9PM) bedtime.18 Total sleep duration (nocturnal sleep duration + naptime) was analyzed as a secondary exposure.
Screen time was reported by parents as the average screen time of all electronic devices (TV/DVDs, computer/tablet, cell phones, video games) in hours per day at age 3 and 5 years. Daily screen time was categorized as excess screen time when total screen time was more than 1hr/day (following guidelines for preschool children).15
Statistical Analysis
Demographic differences between the two visits (3 and 5 years old) were evaluated using paired t-test or paired Wilcoxon rank test on continuous variables, and McNemar’s test on binary variables. Longitudinal associations of bedtime, NSD, and screen time at 3 years of age on overweight/obesity status at 3 and 5 years of age were analyzed in separate models using generalized estimation equations (GEE) with a binomial distribution. Sex was additionally analyzed as a moderator by adding interaction terms to all models. A sensitivity analysis exploring longitudinal associations within 5-year NSD groups was completed (Online Supplement). Cross-sectional analyses at 3 and 5 years were additionally performed (Online Supplement).
To analyze if the associated risk of shorter nocturnal sleep time on overweight/obesity was attenuated by earlier bedtime or shorter screen time, children were grouped into profiles determined a priori, and their association with overweight/obesity was examined in GEE models. Bedtime profiles were classified as: early bedtime + longer NSD (>11hrs), late bedtime + longer NSD (>11hrs), early bedtime + shorter NSD (≤11hrs) and late bedtime + shorter NSD (≤11hrs); while screen time profiles included: screen time >1hr + longer NSD, screen time ≤1hr + longer NSD, screen time >1hr + shorter NSD and screen time ≤1hr + longer NSD. Inclusion of interaction terms was purposefully avoided due to high correlation between main exposure variables.
All analyses were adjusted for variables known to be associated with BMI and sleep in children23,24: sex, birth weight (grams), maternal education level (post-secondary), postnatal maternal BMI, breastfeeding status at 6 months of age, maternal perceived stress score (PSS), daily caloric intake at 5 years of age, and organized physical activity at 5 years of age (≥2hrs/week).25 Breastfeeding status was classified as exclusively breastfed, partial, and not breastfed, and was determined from standardized questionnaires completed by caregivers.26 PSS scores of more than 13 points were classified as high maternal perceived stress.27
Statistical analyses were performed using SAS software (Version 9.4).
Results
A total of 2185 participants with available sleep data at age 3 years and BMI data at age 3 and 5 years were included in this study (eFigure 1). Participants with missing sleep or BMI data excluded from this study (n=882) had no substantial differences in sex, race and maternal BMI compared to those included in analyses, but those excluded had higher maternal perceived stress score, slightly higher BMI-z at 3 years of age, and lower proportion of breastfeeding (eTable 1).
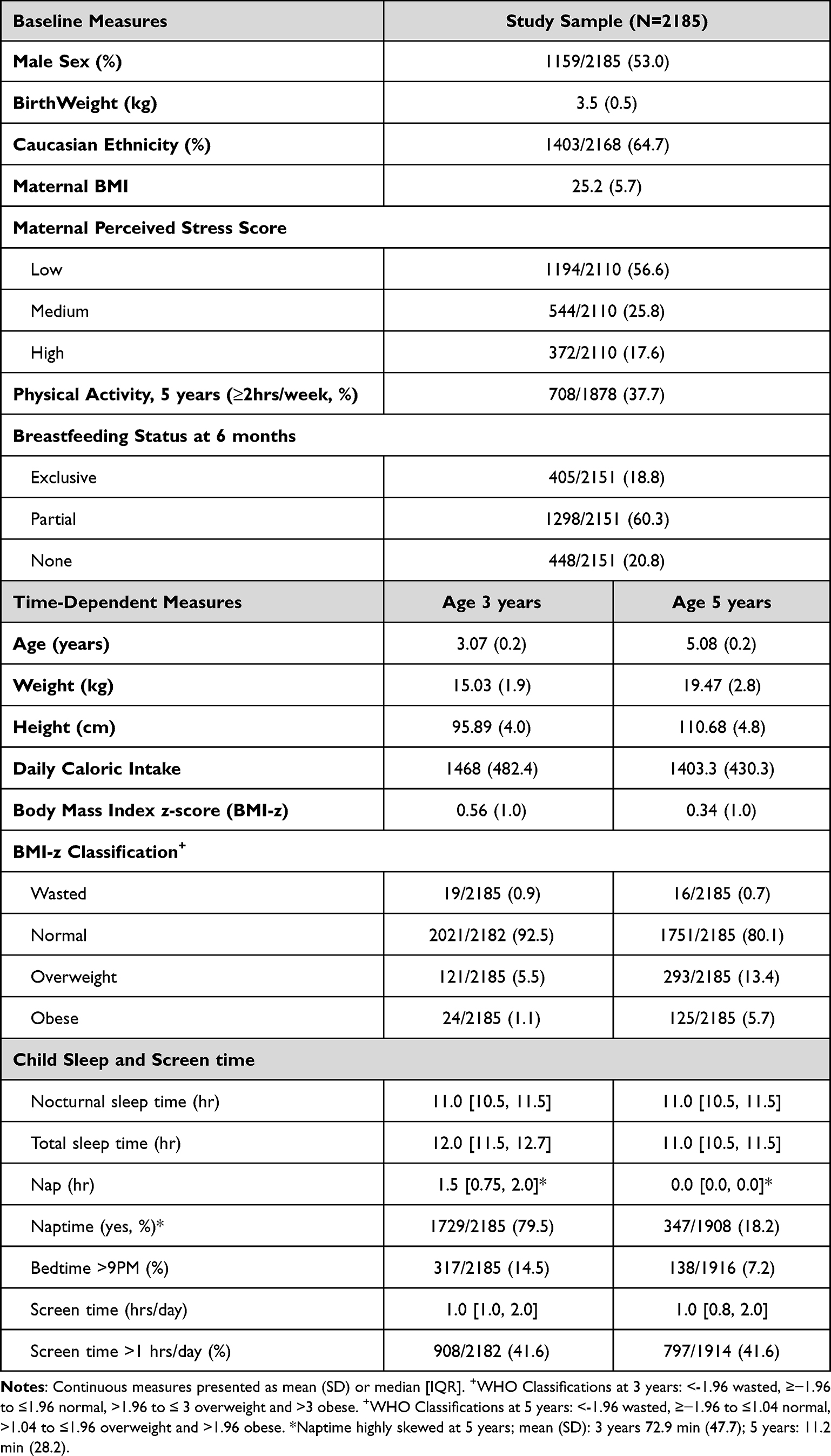 |
Table 1 Population Characteristics at 3 and 5 Years of Age |
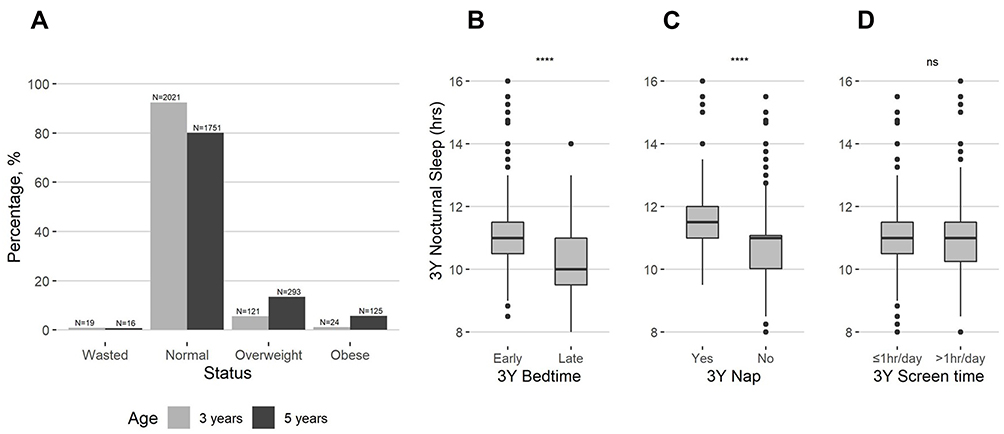 |
Figure 1 (A) Proportion of CHILD Cohort Study participants in waisted, normal weight, overweight and obese BMI-z categories at 3* and 5+ years of age. Nocturnal Sleep Duration at 3 years by (B) Bedtime, (C) Nap status, and (D) Screen time groups at the same age. P-values calculated by Wilcoxon rank-sum test (****p<0.001). *WHO Classifications at 3 years: <-1.96 wasted, ≥−1.96 to ≤1.96 normal, >1.96 to ≤ 3 overweight and >3 obese. +WHO Classifications at 5 years: <-1.96 wasted, ≥−1.96 to ≤1.04 normal, >1.04 to ≤1.96 overweight and >1.96 obese. |
Among 2185 with BMI data at 3 years of age, 5.5% (n=121) were overweight and 1.1% (n=24) were obese; at 5 years of age, proportions of obesity and overweight increased to 13.4% (n=293) and 5.7% (n=125), respectively (Table 1, Figure 1A).
At 3 years of age, the proportion of children in each nocturnal sleep group was fairly balanced; 38.3% (n=833) of children had 10.5 hours of nocturnal sleep or less, 30.1% (n=654) slept between >10.5 and 11.0 hours, and 31.6% (n=687) slept more than 11.0 hours. Children who went to bed before 9PM at age 3 (85.5%, N=1930) had significantly longer nocturnal sleep duration (Figure 1B). Similarly, children who took naps at 3 years also had significantly longer nocturnal sleep compared to children who did not nap during the day (Figure 1C).
Total sleep time decreased significantly with age, from a median of 12hrs [IQR 11.5, 12.7] at 3 years of age to 11hrs [IQR 10.5, 11.5] at 5 years of age (Paired Wilcoxon p<0.001), as naptime decreased and was highly skewed by 5 years, with only 18% of children napping at that age (Table 1). At ages 3 and 5, the same median nocturnal sleep time of 11.0 hours/night [IQR 10.5, 11.5] was observed.
The proportion of children going to bed after 9PM was significantly lower at 5 years (7.2%) compared to 3 years (14.5%) (McNemar p<0.001). Daily screen time remained stable over time, with a median of 1.0hr/day [IQR 1.0, 2.0] at both ages; 41.6% of children at age 3 and 5 years reported more than 1 hour of daily screen time (Table 1). While nocturnal sleep duration did not differ by daily screen time (Figure 1D), the latter was highly correlated with bedtime. Children with bedtime >9PM had a median of 1hr more daily screen time than those going to bed before 9PM (Table 2).
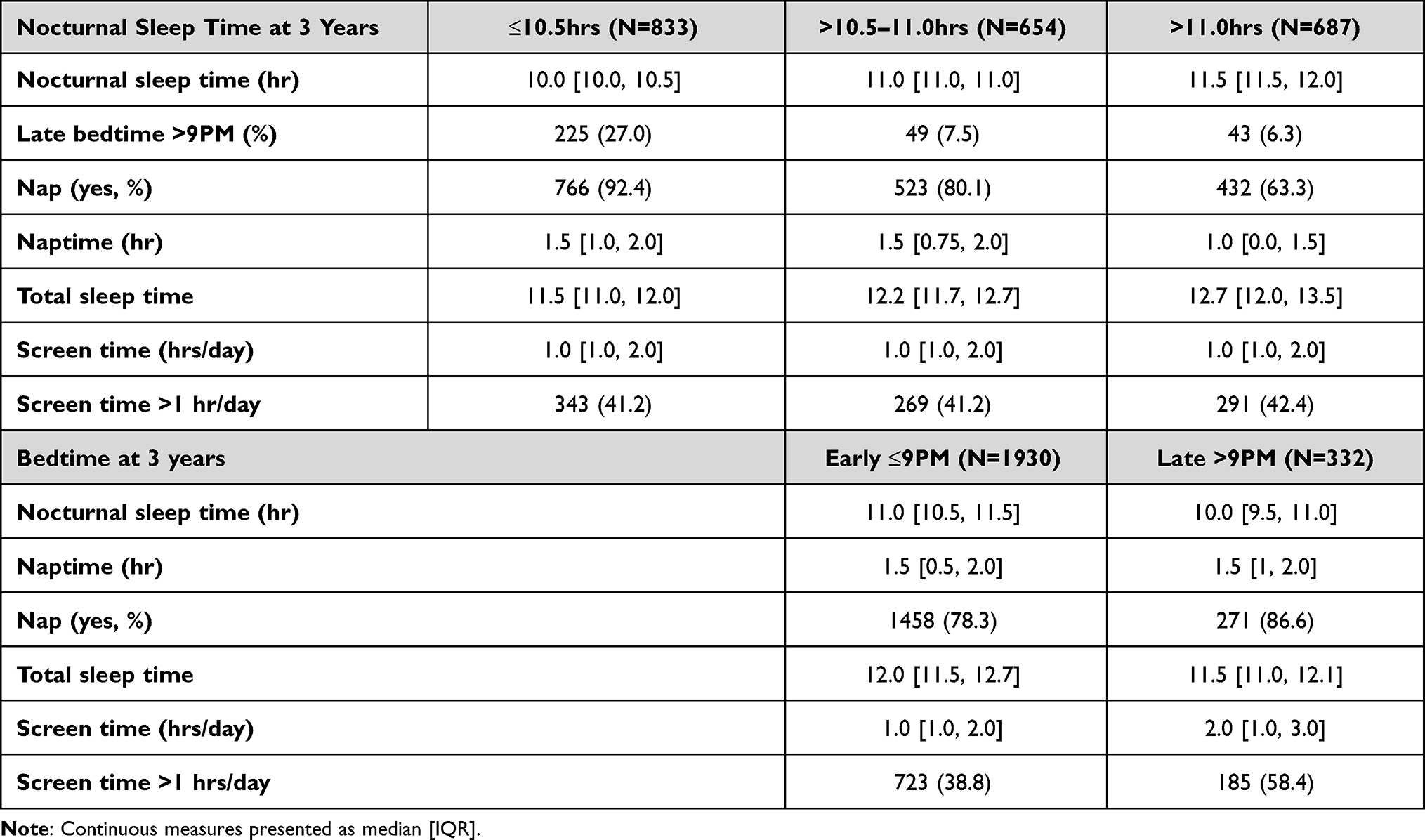 |
Table 2 Median [IQR] Sleep Duration and Sleep Habit Proportions by 3 Years’ Nocturnal Sleep and Bedtime Groups |
Association Between Sleep Habits, Screen Time and Overweight/Obesity
Regression models including only NSD showed a dose response trend between nocturnal sleep duration and risk of overweight/obesity (Figure 2A) after adjustment for covariates (sex, birth weight, breastfeeding status, maternal perceived stress, maternal education, daily caloric intake, physical activity at 5 years, and maternal BMI). Children who slept 10.5 hours or less at 3 years of age had a 46% higher associated risk of being overweight/obese by age 5 years compared to children that slept 11hrs or more (OR 1.46, 95% CI 1.07, 2.00), the risk decreased slightly for children that sleep between 10.5hrs and 11hrs (OR 1.35, 95% CI 0.96, 1.88) (Table 3). Total sleep time (NSD + naptime) of ≤11hrs increased the risk of overweight/obesity by 39% (OR 1.39, 95% CI 1.04,1.86) compared to children with >13hrs of total sleep time.
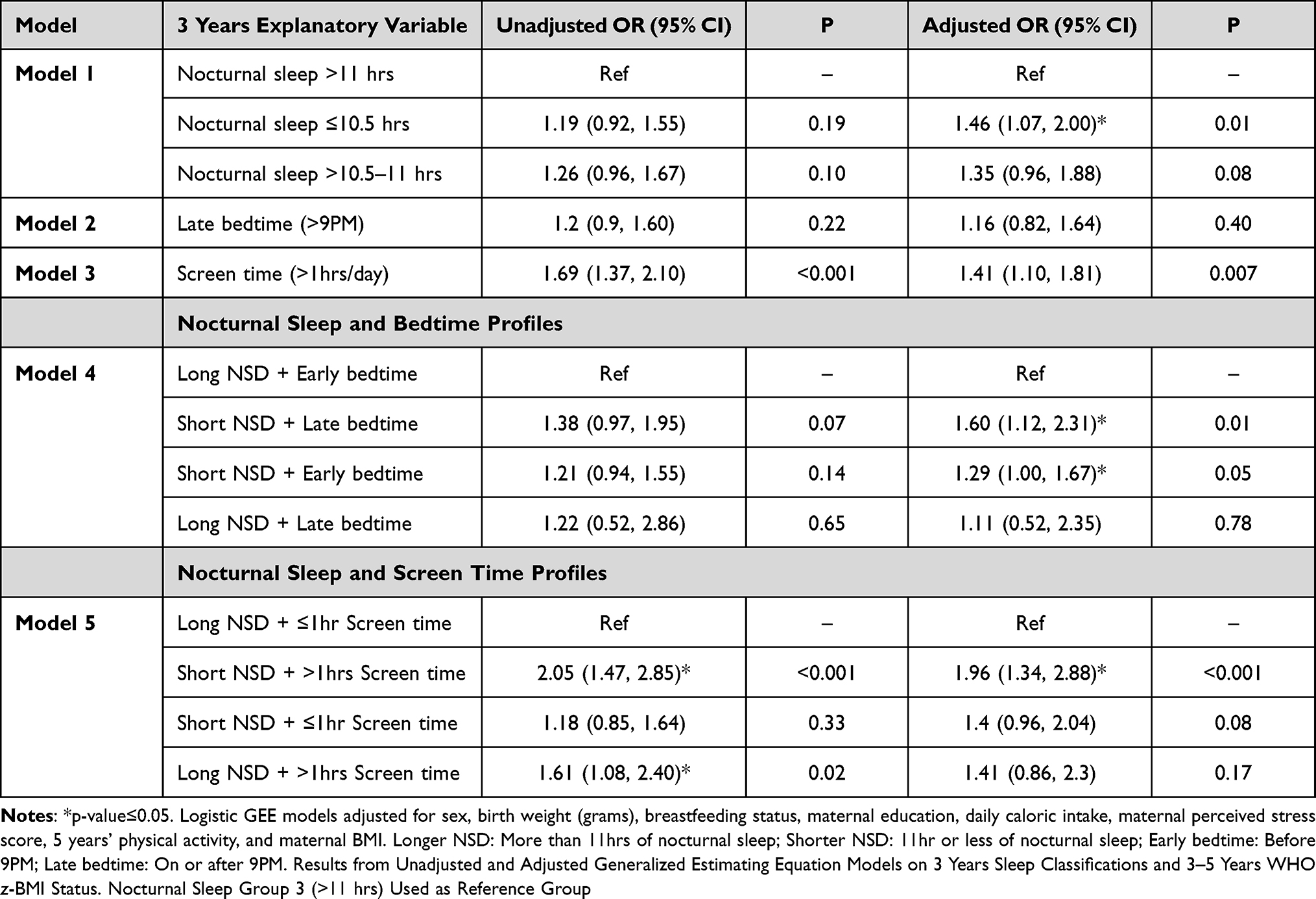 |
Table 3 Sleep Time and BMI Longitudinal Analysis. |
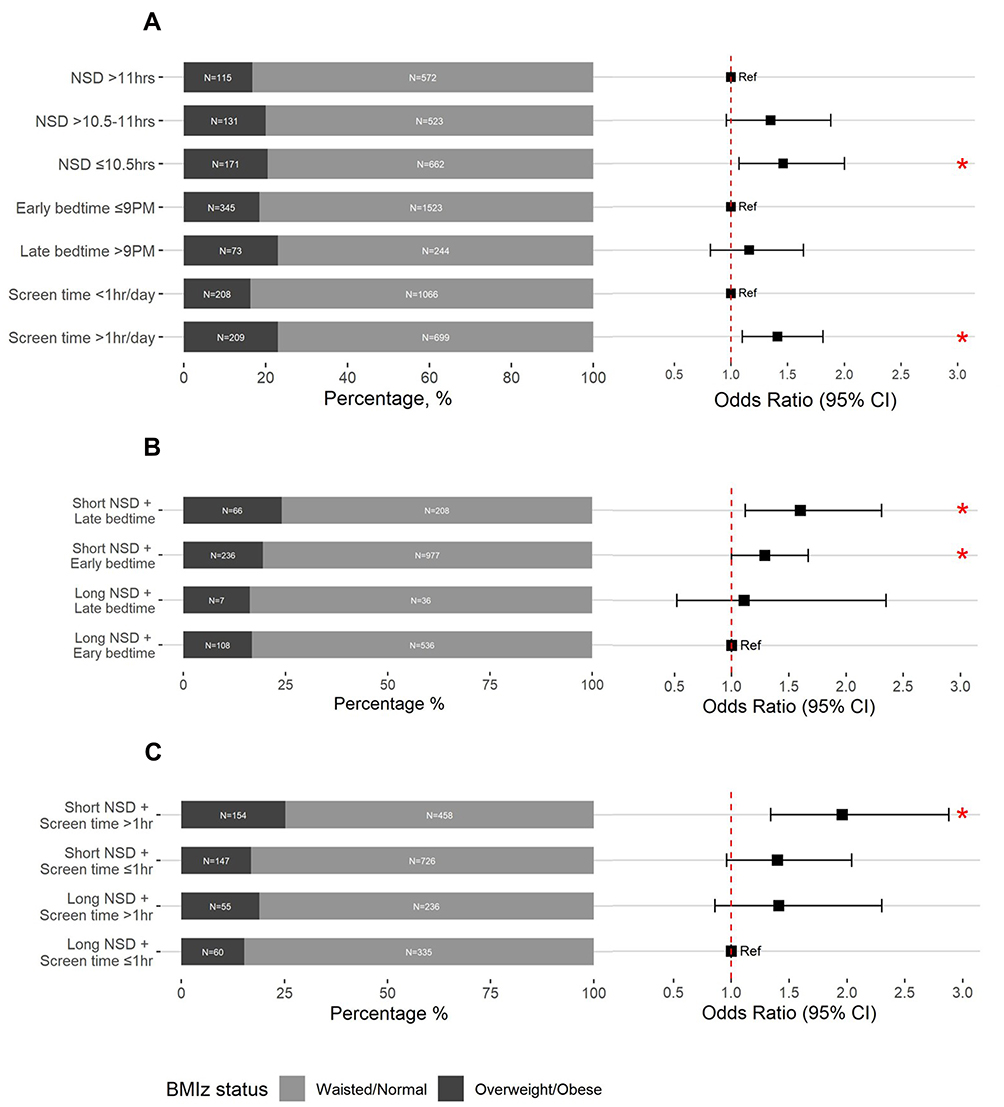 |
Figure 2 (A) Proportions of overweight/obese at 5 years and GEE adjusted odds ratio for nocturnal sleep duration (NSD), bedtime, and screen time groups at 3 years. (B) Proportions of overweight/obese at 5 years and GEE adjusted odds ratio for nocturnal sleep duration (NSD) and bedtime profiles at 3 years. (C) Proportions of overweight/obese at 5 years and GEE adjusted odds ratio for nocturnal sleep duration (NSD) and screen time profiles at 3 years. *P≤0.05. |
Screen time of more than 1hr per day at 3 years was associated with a 41% increased risk of being overweight/obese (OR 1.41, 95% CI 1.10, 1.81) after adjusting for covariates. Late bedtime (>9PM) was not associated with risk of overweight/obesity by 5 years (OR 1.16, 95% CI 0.82, 1.64).
Interaction terms showed that sex acted as an effect modifier of bedtime only (p=0.01). Further stratification by sex showed that bedtime was significantly associated to increased risk of overweight/obesity in girls only (Girls: OR 1.83, 95% CI 1.16, 2.9; Boys: OR 0.75, 95% CI 0.44, 1.27) (eTable 2).
Cross-sectionally, nocturnal sleep time and bedtime were not associated with risk of overweight/obesity at age 3 years (eTable 3). At 5 years, adjusted cross-sectional analysis showed an association of 97% increased risk of obesity/overweight for children sleeping less than 10.5 hours per night (OR 1.97, 95% CI 1.39, 2.78). Later bedtime at age 5 years was not significantly associated with overweight/obesity at the same age. Screen time was associated with overweight/obesity at both 3 and 5 years; however, the association at 5 years became not significant after adjustment for covariates (eTable 3).
Screen Time and Bedtime as Moderators of Nocturnal Sleep
Within the early bedtime group, 16.7% (n=108) and 19.5% (n=236) of children in the long (>11hrs) and short (≤11hrs) NSD groups at 3 years, respectively, were overweight/obese at 5 years (Chi-square p=0.08). Within the late bedtime group, the proportion of overweight/obese in the long NSD group was 16.3% (n=7), compared to 24.1% in the short NSD group (n=66) (Chi-square p=0.30).
Nocturnal sleep time of ≤11hrs (but not >11hrs) was associated with increased overweight/obesity for both early and late bedtime groups (Table 3, Figure 2B). Notably, children with a late bedtime were not associated with increased risk of overweight/obesity, as long as their nocturnal sleep was longer than 11hrs. (OR 1.11, 95% CI 0.52, 2.35).
The proportion of overweight and obese children at 5 years with >1hr daily screen time in infancy was significantly higher in the short NSD group (25.2%, n=154) than the long NSD group (18.9%, n=55) (Chi-square p=0.04). These differences were not significant within the 1≤hr screen time group (Overweight/obese proportions for: Short NSD 16.8%, n=147; Long NSD 15.2%, n=60; Chi-square p=0.35). Accordingly, children that concurrently had >1hr daily screen time and shorter nocturnal sleep (<11hrs) at 3 years had almost twice the associated risk of overweight and obesity (OR 1.96, 95% CI 1.34, 2.88) compared to children with shorter screen time and longer NSD. On the other hand, children that complied with either a moderate screen time, or longer nocturnal sleep did not have increased risk of overweight/obesity (Table 3, Figure 2C).
Discussion
In this longitudinal multicentered study with a diverse population from across Canada, we found a robust longitudinal association between short sleep duration (specifically less than 10.5 hours at night) and increased screen time at 3 years and subsequent overweight and obesity up to 5 years. This study highlights the importance of adequate nocturnal sleep time to reduce the risk of overweight and obesity in preschool children, noting that taking naps during the day may not fulfill the same role of sleep as longer nocturnal sleep duration in this age group. Interestingly, associations between bedtime and risk of overweight/obesity were limited to girls only. Our findings were significant after controlling for important confounding variables including sex, birth weight, breastfeeding, maternal BMI, maternal education, daily caloric intake, organized physical activity, and maternal perceived stress. Findings from cross-sectional analyses at age 5 years were consistent with those obtained following a longitudinal approach.
The exact mechanisms whereby why shorter nocturnal sleep time may contribute to obesity in preschool children have not been fully clarified. Shorter sleep duration may be linked to daytime fatigue resulting in less physical activity and increased sedentary activity which could lead to obesity. Additionally, children with shorter sleep duration and later bedtimes may demonstrate obesogenic eating behaviours such as emotional eating, eating in response to external cues and restrained eating,28 while having more opportunities to eat as they are awake longer.29 In our study, we found that children with late bedtime were not associated to increased risk of overweight/obesity, as long as their sleep was longer than 11 hours. While a late bedtime at 3 years of age has been negatively correlated with nocturnal sleep duration in this and other studies,30 the effects of late bedtime associated with a long sleep duration on sleep quality and circadian rhythm changes are unclear. In one study with children aged 4.5–5 years of age evaluating melatonin secretion (known to regulate circadian rhythm), children with delayed bedtimes had more delayed melatonin onset times,31 whereby delay of melatonin release may influence a delay in the wake up time and sleep quality.32,33
The biological mechanisms underpinning weight gain following chronic sleep deprivation are an area of important research. Shorter sleep duration may be linked to disruption of the circadian rhythm34 as well as hypothalamic mechanisms that regulate body weight and metabolism, including lower leptin and higher ghrelin levels, which can result in greater hunger, appetite and increased preference and intake of high-calorie food.35,36 However, in one fMRI study of young healthy adults, neural changes in the frontal and insular cortex were associated with increased desire for weight-gain promoting high-calorie foods.37 A separate study showed the likelihood of overeating following sleep deprivation was behavioural and not related to hormonal mechanisms.38 Whether these mechanisms hold in younger population is unknown, and data on eating habits or the timing of sugar intake were not available in our population to verify these assumptions.
Findings from our study are consistent with a longitudinal study by Wang et al, in 16,028 preschool children in China, which showed that sleeping <10 hours at 3 years of age was associated with a 48% increase in overweight (OR 1.48, 95% CI 1.26–1.74) and a 77% increase in obesity (OR 1.77, 95% CI 1.30, 2.40) at 5 years of age after adjusting for confounders.23 However, although that study adjusted for multiple confounders, screen time data were not available. This consideration is important because screen time has been reported to be associated with adiposity. In one study, Padmapriya et al reported screen time in 956 preschool children and observed that greater screen time at 2–3 years of age was significantly associated with BMI at 3–5 years of age39 and specifically, every hour of daily screen time (eg, TV, handheld devices) was associated with a BMI increase of 0.12 kg/m2.39 Interestingly, this association was only significant in boys, which contrasts with our study where significance was seen in the entire population.
In contrast to our study, the aforementioned studies did not analyze the modified effect of nocturnal sleep duration on BMI by both late bedtime and longer screen time, but rather examined their effects individually. Here, we observed that both early and late bedtimers with shorter sleep duration were associated to higher risk of overweight and obesity. While early bedtime increased such risk by 29%, having a late bedtime further magnified the associated risk to 60% (compared to children with longer nocturnal sleep and early bedtime). Further research is needed to evaluate whether adverse consequences associated with a late bedtime can be compensated or mitigated for with a long sleep duration.
Similarly, the associated risk of shorter nocturnal sleep duration on overweight and obesity was almost doubled when paired with prolonged screen time (OR 1.96, 95% CI 1.34, 2.88) but was not significant when longer nocturnal sleep was undertaken.
Associations between shorter sleep duration, excessive screen time and increased risk of higher BMI have been found in observational studies8,9,24; however most studies reporting these associations on preschool children are cross-sectional. Only two studies assess how sleep duration and screen time affect weight in preschool children using a longitudinal approach.10,11 The first study of 900 children in the United Kingdom found that nocturnal sleep of <10.5 hours and screen time of >8 hours of television/week at 3 years of age were associated with obesity at 7 years.10 The second study of 1589 preschool children from ‘fragile families’ (unmarried parents and their children) in the United States of America, found that parent-reported shorter sleep duration and watching more than 2 hours of television per day at 3 years of age were associated with obesity at 5 years of age.11 Furthermore, increased television viewing has been found to partially mediate the relationship between short sleep duration and higher BMI in children.40 Interestingly, even though our study showed similar amounts of daily screen time irrespective of nocturnal sleep, only children with >1hr daily screen time in addition to <11hrs of nocturnal sleep had double the associated risk of overweight and obesity, noting that preschool children with prolonged access to electronic devices may limit their risk of overweight and obesity if their nocturnal sleep is greater than 11hrs.
In this study, it was interesting to see that sex acted as an effect modifier only on bedtime, and not nocturnal sleep or screen time. Furthermore, a sensitivity analysis stratified by sex showed that a bedtime after 9PM increased the risk of overweight and obesity by 83% in girls only. It has been suggested that a delayed sleep onset provides more opportunities to be exposed to low nutritional advertisements, which females may be more influenced by, resulting in greater consumption of high calorie foods and higher BMI.41–43 A study by Plancoulaine et al also reported sex-dependent differences among a French cohort of children aged 3 years, where shorter sleep duration was associated with high BMI z-scores and higher screen time among males, and lower intake of healthier foods – independent of BMI – among females.44 Similarly, among children aged 4–17 years, Golshevsky et al found that higher screen time was associated with higher BMI in females, while shorter sleep time was associated with higher BMI in males.45 Bedtime was not evaluated in these previous studies. Overall, the role of sex in sleep habits at preschool age remains unclear46,47 and further research is needed to examine this relationship.
The limitations of this study require consideration. Firstly, sleep duration and habits were assessed subjectively by parent report measures, which may over or underestimate actual sleep times. Nevertheless, many studies have shown high agreement between parental reports and objective sleep measures such as actigraphy duration.48 Secondly, although this study controlled for various confounders, some variables were not taken into account, such as home environment characteristics, parental sleep times, sleeping arrangements including frequency of co-sleeping, dietary intake, which may be associated with sleep habits, screen time and consequently BMI.49,50
Conclusion
This longitudinal study highlights that short nocturnal sleep duration (<11 hours) and excessive screen time (>1 hour daily) are associated with overweight and obesity in preschool children, and that these associations are independent of bedtime. Since sleep habits are modifiable risk factors, further education, awareness, and targeted interventions such as improved sleep hygiene are essential to mitigate the long-term impact of reduced sleep and delayed bedtimes in preschool children.
Abbreviations
NSD, nocturnal sleep duration; BMI, body mass index; WHO, World Health Organization.
Acknowledgment
We thank the CHILD Cohort Study participant families for their dedication and commitment to advancing health research and the whole CHILD Cohort Study team, which includes interviewers, nurses, computer and laboratory technicians, clerical workers, research scientists, volunteers, managers, and receptionists.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work. Piushkumar J Mandhane and Indra Narang are joint co-senior authors.
Funding
This work was supported by AllerGen 12CHILD – Canadian Healthy Infant Longitudinal Development (CHILD) Study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. De OM, Blossner M, Borghi E. Global prevalence and trends of overweight and obesity among preschool children. Am J Clin Nutr. 2010;92:1257–1264. doi:10.3945/ajcn.2010.29786
2. Patel SR, Frank HB. Short sleep duration and weight gain: a systematic review. Obesity. 2008;16(3):643–653. doi:10.1038/oby.2007.118
3. Pacheco D. Children and sleep [internet]. 2020. Available from: https://www.sleepfoundation.org/children-and-sleep.
4. Suni E. How much sleep do we really need?; 2020. Available from: https://www.sleepfoundation.org/articles/how-much-sleep-do-we-really-need.
5. Sadeh A, Mindell JA, Luedtke K, Wiegand B. Sleep and sleep ecology in the first 3 years: a web-based study. J Sleep Res. 2009;18(1):60–73. doi:10.1111/j.1365-2869.2008.00699.x
6. Fang K, Mu M, Liu K, He Y. Screen time and childhood overweight/obesity: a systematic review and meta-analysis. Child Care Health Dev. 2019;45(5):744–753. doi:10.1111/cch.12701
7. Lumeng JC, Rahnama S, Appugliese D, Kaciroti N, Bradley RH. Television exposure and overweight risk in preschoolers. Arch Pediatr Adolesc Med. 2006;160(4):417–422. doi:10.1001/archpedi.160.4.417
8. Carrillo-Larco RM, Bernabé-Ortiz A, Miranda JJ. Short sleep duration and childhood obesity: cross-sectional analysis in Peru and patterns in four developing countries. PLoS One. 2014;9(11):1–9. doi:10.1371/journal.pone.0112433
9. Stiglic N, Viner RM. Effects of screentime on the health and well-being of children and adolescents: a systematic review of reviews. BMJ Open. 2019;9(1):1–15. doi:10.1136/bmjopen-2018-023191
10. Reilly JJ, Armstrong J, Dorosty AR, et al. Early life risk factors for obesity in childhood: cohort study. BMJ. 2005;330:1357. doi:10.1136/bmj.38470.670903.E0
11. Suglia SF, Duarte CS, Chambers EC, Boynton-Jarrett R. Social and behavioral risk factors for obesity in early childhood. J Dev Behav Pediatr. 2013;34(8):549–556. doi:10.1097/DBP.0b013e3182a509c0
12. Mistry KB, Minkovitz CS, Strobino DM, Borzekowski DLG. Children’s television exposure and behavioral and social outcomes at 5.5 years: does timing of exposure matter? Pediatrics. 2007;120(4):762–769. doi:10.1542/peds.2006-3573
13. Li L, Zhang S, Huang Y, Chen K. Sleep duration and obesity in children: a systematic review and meta-analysis of prospective cohort studies. J Paediatr Child Health. 2017;53(4):378–385. doi:10.1111/jpc.13434
14. Is Canada in the running? The 2014 active healthy physical activity for children and youth. [cited 2017 Apr 11]; 2014. Available from: http://dvqdas9jty7g6.cloudfront.net/reportcard2014/AHKC_2014_ReportCard_ENG.pdf.
15. Are Canadian kids too tired to move? The participaction report card on physical activity for children and youth. WellSpring; 2016:1–4. Available from: https://www.participaction.com/en-ca/resources/report-card.
16. Roy M, Haszard JJ, Savage JS, et al. Bedtime, body mass index and obesity risk in preschool‐aged children. Pediatric Obesity; 2020. Available from: https://onlinelibrary.wiley.com/doi/10.1111/ijpo.12650.
17. Scharf RJ, DeBoer MD. Sleep timing and longitudinal weight gain in 4- and 5-year-old children: sleep timing and obesity in preschoolers. Pediatr Obes. 2015;10(2):141–148. doi:10.1111/ijpo.229
18. Miller AL, Kaciroti N, Lebourgeois MK, Chen YP, Sturza J, Lumeng JC. Sleep timing moderates the concurrent sleep duration-body mass index association in low-income preschool-age children. Acad Pediatr. 2014;14(2):207–213. doi:10.1016/j.acap.2013.12.003
19. Subbarao P, Anand SS, Becker AB, et al. The Canadian Healthy Infant Longitudinal Development (CHILD) study: examining developmental origins of allergy and asthma. Thorax. 2015;70(10):998–1000. doi:10.1136/thoraxjnl-2015-207246
20. Onis M D, Onyango AW. WHO child growth standards. Lancet. 2008;371(9608):204. doi:10.1016/S0140-6736(08)60131-2
21. Onis M D, Onyango AW, Borghi E, Siyam A, Siekmann J. Development of a WHO growth reference for school-aged children and adolescents. Bull World Health Organ. 2007;85(9):660–667. doi:10.2471/BLT.07.043497
22. Von Kries R, Toschke AM, Wurmser H, Sauerwald T, Koletzko B. Reduced risk for overweight and obesity in 5- and 6-y-old children by duration of sleep - A cross-sectional study. Int J Obes. 2002;26(5):710–716. doi:10.1038/sj.ijo.0801980
23. Wang F, Liu H, Wan Y, et al. Sleep duration and overweight/obesity in preschool-aged children: a prospective study of up to 48,922 children of the Jiaxing birth cohort. Sleep. 2016;39(11):2013–2019. doi:10.5665/sleep.6234
24. Carter PJ, Taylor BJ, Williams SM, Taylor RW. Longitudinal analysis of sleep in relation to BMI and body fat in children: the FLAME study. BMJ. 2011;342(7809):4–5. doi:10.1136/bmj.d2712
25. Tamana SK, Ezeugwu V, Chikuma J, et al. Screen-time is associated with inattention problems in preschoolers: results from the CHILD birth cohort study. PLoS One. 2019;14(4):1–15. doi:10.1371/journal.pone.0213995
26. Azad MB, Vehling L, Chan D, et al. Infant feeding and weight gain: separating breast milk from breastfeeding and formula from food. Pediatrics. 2018;142(4):4. doi:10.1542/peds.2018-1092
27. Chow A, Dharma C, Chen E, et al. Trajectories of depressive symptoms and perceived stress from pregnancy to the postnatal period among Canadian women: impact of employment and immigration. Am J Public Health. 2019;109(S3):S197–204. doi:10.2105/AJPH.2018.304624
28. Burt J, Dube L, Thibault L, Gruber R. Sleep and eating in childhood: a potential behavioral mechanism underlying the relationship between poor sleep and obesity. Sleep Med. 2014;15(1):71–75. doi:10.1016/j.sleep.2013.07.015
29. Tatone-Tokuda F, Dubois L, Ramsay T, et al. Sex differences in the association between sleep duration, diet and body mass index: a birth cohort study. J Sleep Res. 2012;21(4):448–460. doi:10.1111/j.1365-2869.2011.00989.x
30. Kohyama J, Shiiki T, Ohinata-Sugimoto J, Hasegawa T. Potentially harmful sleep habits of 3-year-old children in Japan. J Dev Behav Pediatr. 2002;23(2):67–70. doi:10.1097/00004703-200204000-00001
31. Akacem LD, Wright KP, LeBourgeois MK. Bedtime and evening light exposure influence circadian timing in preschool-age children: a field study. Neurobiol Sleep Circadian Rhythms. 2016;1(2):27–31. doi:10.1016/j.nbscr.2016.11.002
32. Barion A, Zee PC. A clinical approach to circadian rhythm sleep disorders. Sleep Med. 2007;8(6):566–577. doi:10.1016/j.sleep.2006.11.017
33. Lack L, Wright H. The effect of evening bright light in delaying the Circadian Rhythms and lengthening the sleep of early morning awakening insomniacs. Sleep. 1993;16(5):436–443. doi:10.1093/sleep/16.5.436
34. Kawai M. Disruption of the circadian rhythms and its relationship with pediatric obesity. Pediatrics International; 2022. Available from: https://onlinelibrary.wiley.com/doi/10.1111/ped.14992.
35. Article L, Taheri S. The link between short sleep duration and obesity: we should recommend more sleep to prevent obesity. Arch Dis Child. 2006;91:881–884. doi:10.1136/adc.2005.093013
36. Bell JF, Zimmerman FJ. Shortened nighttime sleep duration in early life and subsequent childhood obesity. Arch Pediatr Adolesc Med. 2021;164(9):840–846.
37. Greer SM, Goldstein AN, Walker MP. The impact of sleep deprivation on food desire in the human brain. Nat Commun. 2013;4(1):2259. doi:10.1038/ncomms3259
38. Rihm JS, Menz MM, Schultz H, et al. Sleep deprivation selectively upregulates an amygdala–hypothalamic circuit involved in food reward. J Neurosci. 2019;39(5):888–899. doi:10.1523/JNEUROSCI.0250-18.2018
39. Padmapriya N, Aris IM, Mya T, et al. Sex-specific longitudinal association of screen viewing time in children at 2–3 years with adiposity at 3–5 years. Int J Obes. 2019;43(7):1334–1343. doi:10.1038/s41366-019-0344-x
40. Magee C, Caputi P, Iverson D. Lack of sleep could increase obesity in children and too much television could be partly to blame. Acta Paediatr Int J Paediatr. 2014;103(1):27–31. doi:10.1111/apa.12447
41. Powell LM, Schermbeck RM, Szczypka G, Chaloupka FJ, Braunschweig CL. Trends in the nutritional content of television food advertisements seen by children in the United States: analyses by age, food categories, and companies. Arch Pediatr Adolesc Med. 2011;165(12):1078–1086. doi:10.1001/archpediatrics.2011.131
42. Fleig D, Randler C. Association between chronotype and diet in adolescents based on food logs. Eat Behav. 2009;10(2):115–118. doi:10.1016/j.eatbeh.2009.03.002
43. Anderson GH, Khodabandeh S, Patel B, Luhovyy BL, Bellissimo N, Mollard RC. Mealtime exposure to food advertisements while watching television increases food intake in overweight and obese girls but has a paradoxical effect in boys. Appl Physiol Nutr Metab. 2014;40(2):162–167. doi:10.1139/apnm-2014-0249
44. Plancoulaine S, Lioret S, Regnault N, et al. Gender-specific factors associated with shorter sleep duration at age 3 years. J Sleep Res. 2015;24(6):610–620. doi:10.1111/jsr.12308
45. Golshevsky DM, Magnussen C, Juonala M, Kao KT, Harcourt BE, Sabin MA. Time spent watching television impacts on body mass index in youth with obesity, but only in those with shortest sleep duration. J Paediatr Child Health. 2020;56(5):721–726. doi:10.1111/jpc.14711
46. Becker SP, Sidol CA, Van Dyk TR, Epstein JN, Beebe DW. Intraindividual variability of sleep/wake patterns in relation to child and adolescent functioning: a systematic review. Sleep Med Rev. 2017;34:94–121. doi:10.1016/j.smrv.2016.07.004
47. McDonald L, Wardle J, Llewellyn CH, van Jaarsveld CHM, Fisher A. Predictors of shorter sleep in early childhood. Sleep Med. 2014;15:536–540. doi:10.1016/j.sleep.2014.01.005
48. Sekine M, Chen X, Hamanishi S, Wang H, Yamagami T, Kagamimori S. The validity of sleeping hours of healthy young children as reported by their parents. J Epidemiol. 2002;12(3):237–242. doi:10.2188/jea.12.237
49. Petit D, Touchette É, Tremblay RE, et al. Associations between sleep duration patterns and overweight/obesity at age 6. Sleep. 2008;31(11):1507–1514. doi:10.1093/sleep/31.11.1507
50. Olafsdottir S, Eiben G, Prell H, et al. Young children’s screen activities, sweet drink consumption and anthropometry: results from a prospective European study. Int J Public Health. 2014;59(1):67–75. doi:10.1007/s00038-013-0473-2
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.