Back to Journals » Journal of Pain Research » Volume 16
Long-Term Radiographic and Clinical Outcomes in Patients Undergoing Transforaminal Endoscopic Lumbar Discectomy: A Propensity Score Matching Study
Received 26 January 2023
Accepted for publication 4 July 2023
Published 1 September 2023 Volume 2023:16 Pages 3019—3027
DOI https://doi.org/10.2147/JPR.S406071
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Krishnan Chakravarthy
Guanzhang Mu,* Lei Yue,* Haolin Sun
Orthopaedic Department, Peking University First Hospital, Beijing, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Haolin Sun, Orthopedic Department, Peking University First Hospital, 8th Xishiku Ave, Beijing, 100034, People’s Republic of China, Tel +86-1083572655, Email [email protected]
Background: Our study aims to investigate the long-term clinical and radiographic effects of transforaminal endoscopic lumbar discectomy (TELD) on lumbar disc herniation.
Patients and Methods: Radiographic and clinical data of patients undergoing TELD in our institution from January 2015 to January 2019 were retrospectively collected. LDH outpatients who had not received surgical treatment during the same period were 1:1 matched by propensity score matching as the conservative group. The radiographic parameters of the two groups at baseline and at the last follow-up (≥ 24 months) were analyzed.
Results: The study included 47 patients in the TELD group, matched with 47 patients in the conservative group. The disc height of the TELD group at the last follow-up was lower than that at the baseline (P < 0.001), and lower than that of the conservative group at the last follow-up (P < 0.05). The disc degeneration grade of the TELD group at the last follow-up was greater than that at the baseline, and greater than that of the conservative group at the last follow-up. There was no significant difference in the facet joint degeneration in the TELD group between the baseline and the last follow-up, and between the TELD group and the conservative group at the last follow-up (P > 0.05). The pain intensity and disability score in the TELD group at 3-month follow-up and at the last follow-up were significantly lower than those at the baseline (P < 0.001). Six patients in the TELD group required additional surgery during the follow-up period.
Conclusion: Our long-term follow-up data shows that the disc height of the operated level was significantly reduced and the disc degeneration was significantly aggravated in TELD-treated patients; in contrast, the facet joint degeneration did not show significant aggravation.
Keywords: endoscopic discectomy, spinal surgery, minimally invasive, lumbar disc herniation
Introduction
Over the past several decades, full-endoscopic discectomy (FED) has undergone significant technological maturity, and its indications have expanded from lumbar disc herniation (LDH) to thoracic and cervical disc herniation.1,2 Compared with open spine surgery, FED has the advantages of less invasiveness, less trauma, faster recovery, and less impact on adjacent intervertebral discs.3,4 However, the widespread use of FED is associated with certain complications, and previous studies have shown that FED procedure per se could result in biomechanical deterioration.5–7 The long-term follow-up for FED is anticipated to examine clinical efficacy, explore postoperative morphological changes, and timely detect complications. Currently, most of the long-term FED follow-up results are limited to patient-reported clinical outcomes, while few studies have investigated the long-term postoperative radiographic changes. Therefore, a long-term follow-up involving both radiographic and clinical analysis is needed to better understand its cost-effectiveness.
The basic unit of lumbar spine movement includes two adjacent vertebral bodies and the connecting structure between them. The connecting structure refers to the three-joint complex (TJC), composed of the intervertebral disc and the facet joints on both sides.8 Transforaminal endoscopic lumbar discectomy (TELD)—a common full-endoscopic lumbar discectomy technique, which is characterized by partial removal of the intervertebral disc and preservation of the facet joint—may be optimal for observing postoperative morphological changes in the TJC. The purpose of this study was to investigate the postoperative radiographic changes in the TJC and the clinical outcomes after at least 2-year follow-up after TELD.
Materials and Methods
This retrospective study was approved by the Ethics Committee of Peking University First Hospital (2021-473), and the subjects in this study were exempted from informed consent, as the study involves no more than minimal risk, or identifiable private information for them. The identifying information of subjects was anonymized to ensure patient data confidentiality. This study was conducted and reported in accordance with the Declaration of Helsinki the STROBE statement.9
Patients
We included patients with a single-level LDH, who had been treated at our institution from January 2015 to January 2019, with a minimum of 2-year follow-up. The patients were divided into two groups based on whether they received TELD (the TELD group) or conservative treatment (the conservative group). Patients with spinal stenosis, spondylolisthesis, spine trauma, ankylosing spondylitis, spinal infection, spinal tumor, or history of a previous spine surgery were excluded. The diagnosis of LDH was consistently made by the same group of surgeons based on clinical manifestations, physical examination, and magnetic resonance imaging (MRI) findings.
Radiographic Parameters
Radiographic parameters were evaluated on MRI (3T GE Discovery MR750, Waukesha, WI, USA), and all of the images were acquired in a supine position in CTL-spine coil, field of view (FOV) of 310 mm, and 16-sagittal slices with 3 mm thickness. The radiographic parameters included disc height,10 disc protrusion size, disc protrusion location,11 disc degeneration grade,12 and facet joint degeneration grade.13 The measurement methods are shown in Figure 1.
 |
Figure 1 Schematic diagram of the imaging classification methods. (A) Disc degeneration grades 1, 2, 3, 4, and 5; (B) disc protrusion locations a, b, and c, and white dashed lines represents midline, 50% of the distance between midline and intra-facet line, and intra-facet line; (C) disc protrusion sizes 1, 2, and 3, and white dashed lines represents posterior edge of disc, 50% of the distance between posterior edge of disc and intra-facet line, and intra-facet line; (D) facet joint degeneration grades 0, 1, 2, and 3. |
Clinical Outcomes
Clinical outcomes were collected and analyzed only for the patients in the TELD group, considering that the conservative group was not clinically comparable because it included asymptomatic patients. Clinical outcomes were Oswestry Disability Index (ODI) and visual analogue scale (VAS) before surgery, 3 months after surgery, and at the last follow-up
The TELD Procedure
The TELD procedure was performed under spinal anesthesia with 6 mL of hypobaric ropivacaine (0.125%). Then, with patients in a prone position, surgical draping was performed on a routine basis. A puncture needle was introduced from the entry point, 8–13 cm from the midline, and placed into the disc space through Kambin’s triangle. Then, a guide wire was inserted through the puncture needle under fluoroscopic guidance, and an 8-mm incision was made at the entry site. A cannulated obturator was inserted along the guide wire; after touching the ventral edge of the superior articular process, a working cannula was inserted along the obturator and the position of the cannula was ascertained by fluoroscopy. Next, endoscope equipment (TESSYS system; Joimax, Germany) was inserted through the cannula. The herniated disc and fibrotic scar tissues were removed using an endoscopic forceps and ablation device (Trigger-Flex, Elliquence, USA). Annulus modulation was performed after the herniated fragment was completely removed, and then the endoscope was removed and a sterile dressing was applied with a single stitch suture.
Postoperative Rehabilitation
The postoperative rehabilitation program for patients undergoing TELD consists of three aspects. First, patients were instructed to wear a lumbar brace when sitting, standing and walking in the first month after surgery. Second, patients were taught to perform isometric quadriceps strength training by a therapist prior to discharge, and were advised to practice isometric quadriceps strength training for six months after surgery. Third, bending was forbidden for patients who underwent TELD, and using a picker was encouraged.
Statistical Analysis
All of the data were anonymized and entered into an Excel spreadsheet (Microsoft, Redmond, WA). Continuous variables were described as the mean and standard deviations (SDs) if normally distributed, or median and interquartile range if not normally distributed. For continuous variables with a normal distribution, independent-sample t-test was used for intergroup comparisons, while paired-sample t-test was used for intragroup comparison. For continuous variables not complying with a normal distribution, the Mann–Whitney U-test was used for intergroup comparisons, and Wilcoxon test was used for intragroup comparison. Categorical variables were described as frequencies and percentages and were analyzed with Fisher’s exact test or the chi-square test. All of the statistical analyses were done using SPSS 27.0 (IBM, Armonk, NY). P < 0.05 was considered to be statistically significant.
The propensity score was determined by multivariate logistic regression, and the finally included variables were age, gender, herniation level, facet joint degeneration grade, and disc degeneration grade. After calculating the propensity score of each subject, the conservative group was matched in a 1:1 ratio to the TELD group using nearest neighbor matching with a 0.12 caliper width. Weighted Kappa analysis was used to determine the interobserver agreement on radiographic measurements. The Kappa coefficient was interpreted as almost perfect (0.81–1.00), substantial (0.61–0.80), moderate (0.41–0.60), fair (0.21–0.4), and none to slight (0.00–0.20).14
Results
Baseline Demographic Characteristics and Radiographic Parameters
From January 2015 to January 2019, 256 patients who had received single-level TELD surgery were screened, and 47 eligible patients were finally enrolled. A total of 47 eligible outpatients who had not received surgery were matched as the conservative group (Figure 2). Demographic characteristics and radiographic parameters were similar in the two groups at baseline, except for the distribution of disc protrusion size (P = 0.001) (Table 1).
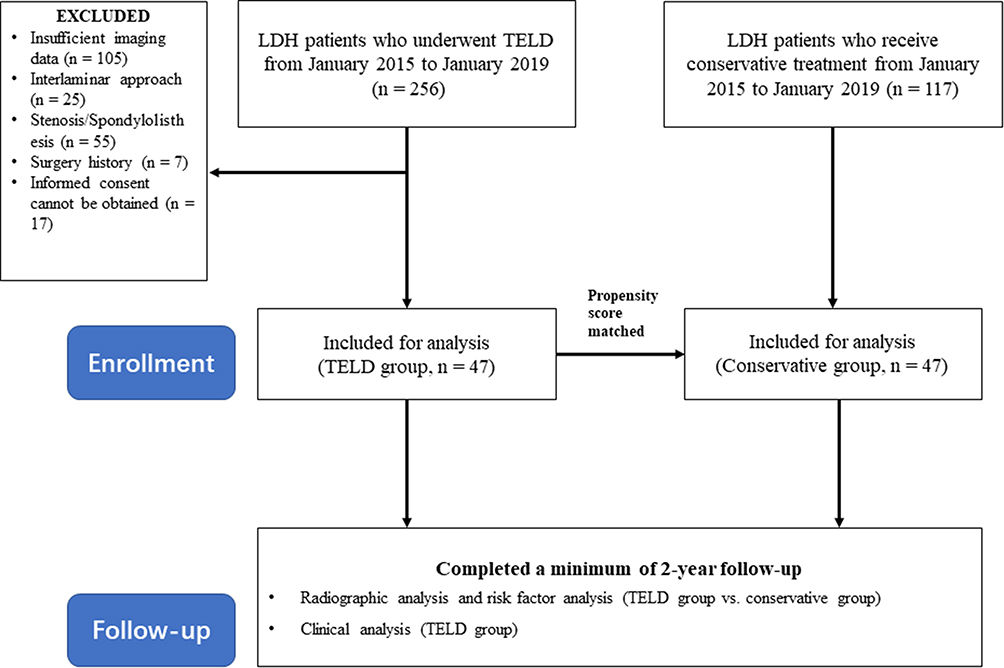 |
Figure 2 The STROBE flowchart of the current study. Abbreviations: LDH, lumbar disc herniation; TELD, transforaminal endoscopic lumbar discectomy. Notes: von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296. Creative Commons.9 |
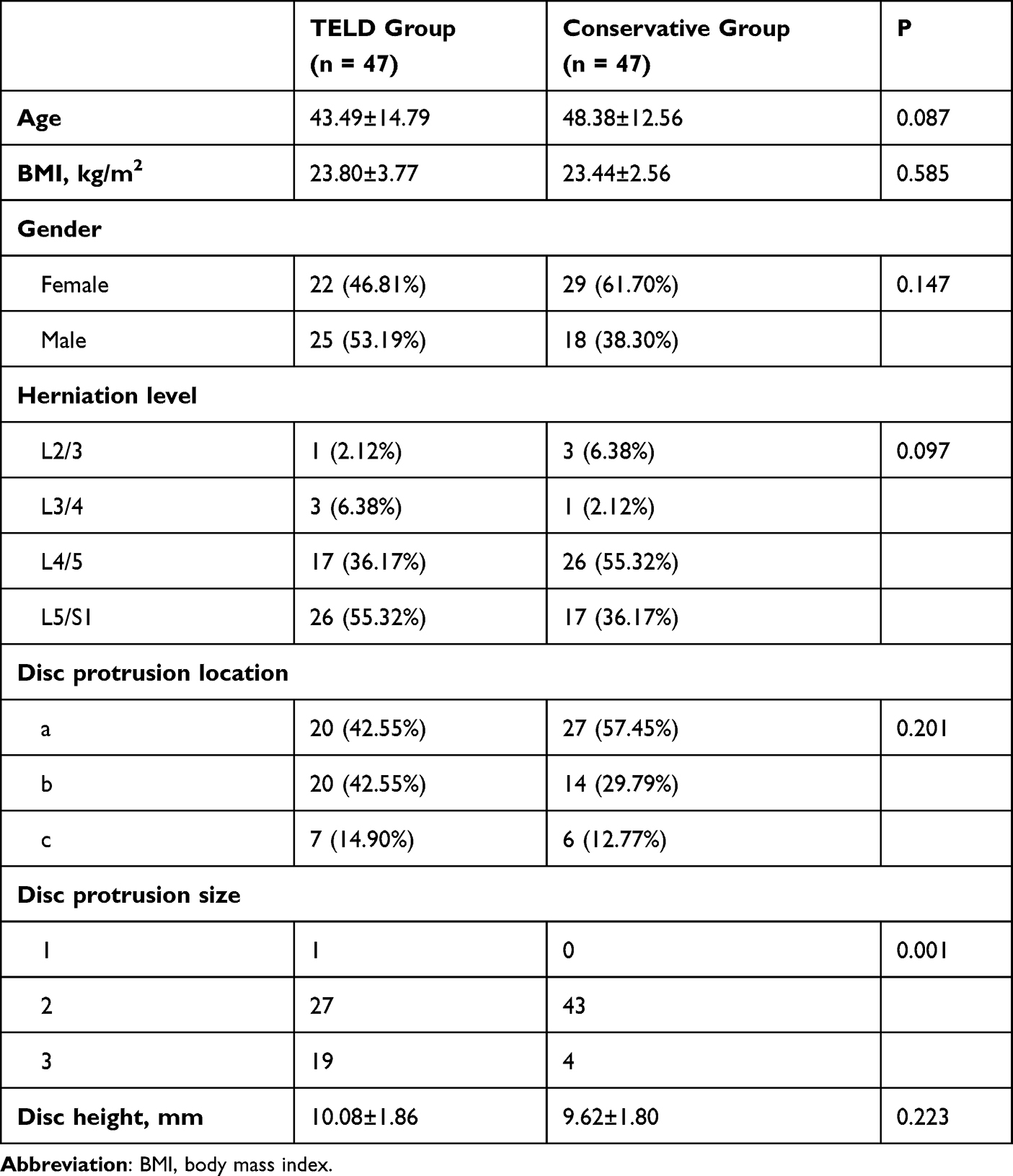 |
Table 1 Baseline Demographic Characteristics and Radiographic Parameters |
Radiographic Outcomes
Intragroup comparisons showed that the disc height in the TELD group at the last follow-up was significantly lower than that at the baseline (8.64±1.88 vs 10.08±1.86, P = 0.000), while the disc height in the conservative group was similar between the baseline and the last follow-up (9.49±1.87 vs 9.62±1.80, P=0.164). Intergroup comparison showed that the disc height at the last follow-up was smaller in the TELD group than in the conservative group (8.64±1.88 vs 9.49±1.87, P = 0.031). Intragroup comparison showed that disc protrusion size in the TELD group at the last follow-up was significantly smaller than that at the baseline (P = 0.000), while disc protrusion size in the conservative group was similar between the baseline and the last follow-up (P = 0.655).
The disc degeneration grade at the last follow-up was greater than that at the baseline in the TELD group (P = 0.000), while disc degeneration grade in the conservative group was similar between the baseline and the last follow-up (P = 0.713). Intergroup comparison at the last follow-up showed that the disc degeneration grade in the TELD group was larger than that in the conservative group (P = 0.033). As for facet joint degeneration grade in both groups, no differences were observed between the last follow-up and the baseline, and the facet joint degeneration grade was similar in both groups at the last follow-up (Table 2).
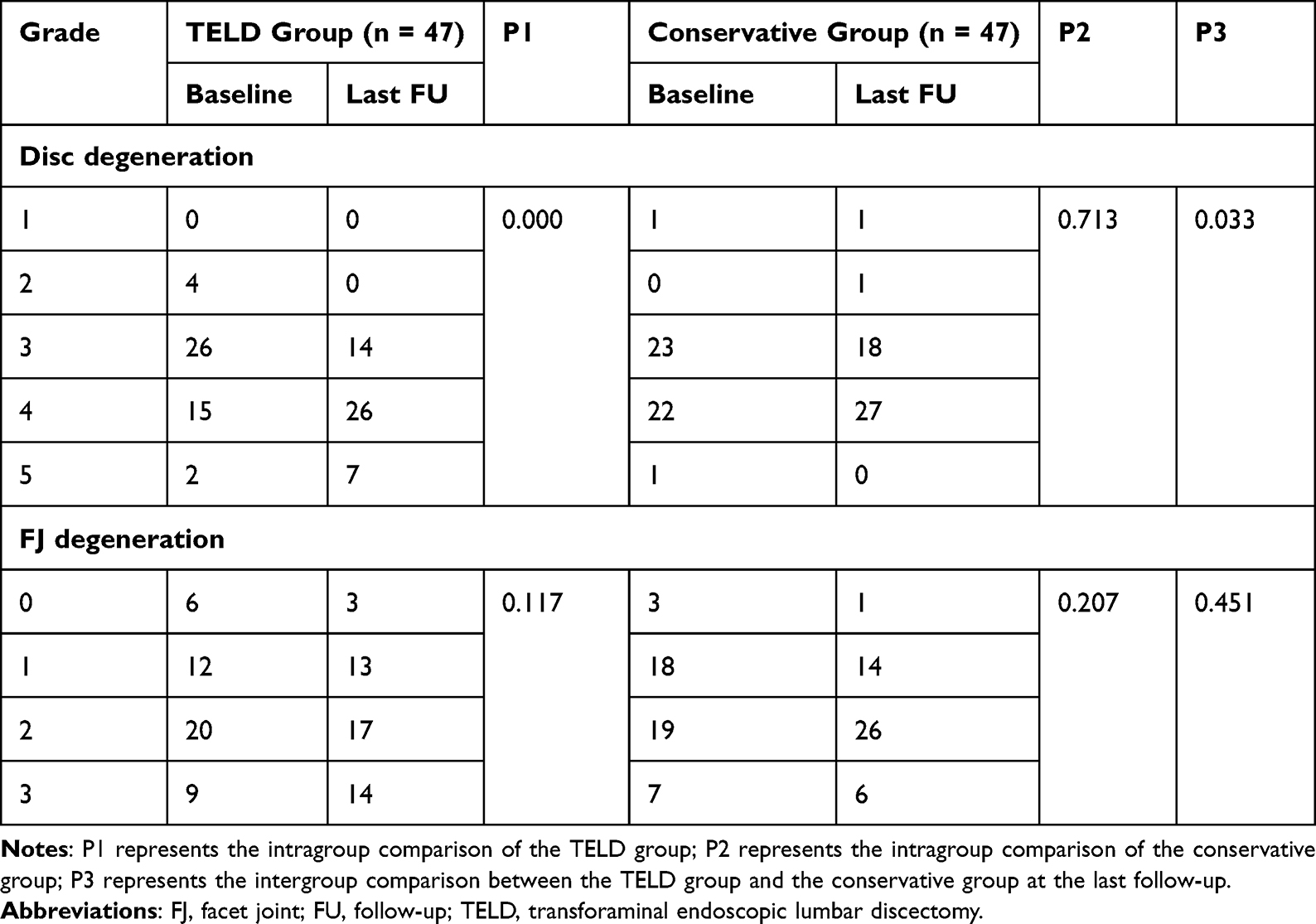 |
Table 2 Degeneration Grade of Disc and Facet Joint in the Two Groups |
Clinical Outcomes
In the TELD group, the VAS score and ODI score at 3 months after surgery and at the last follow-up significantly decreased compared with the baseline (P < 0.001) (Figure 3). In addition, four patients in the TELD group underwent additional surgery for re-herniation at the operated level, and two patients underwent additional surgery for adjacent segment disease (ASD) during the follow-up period.
 |
Figure 3 The follow-up results of clinical outcomes in the TELD group: (A) VAS score of pain decreased significantly at 3 months after surgery and at the last follow-up, compared with the baseline; (B) ODI score at 3 months after surgery and at the last follow-up also significantly decreased compared with the baseline; ****P < 0.001. Abbreviations: FU, follow-up; TELD, transforaminal endoscopic lumbar discectomy. |
Interobserver Agreement Assessment
The interobserver agreement on radiographic measurements was “almost perfect” for disc protrusion size, and “substantial” for disc degeneration, facet joint degeneration, and disc protrusion location (Table 3).
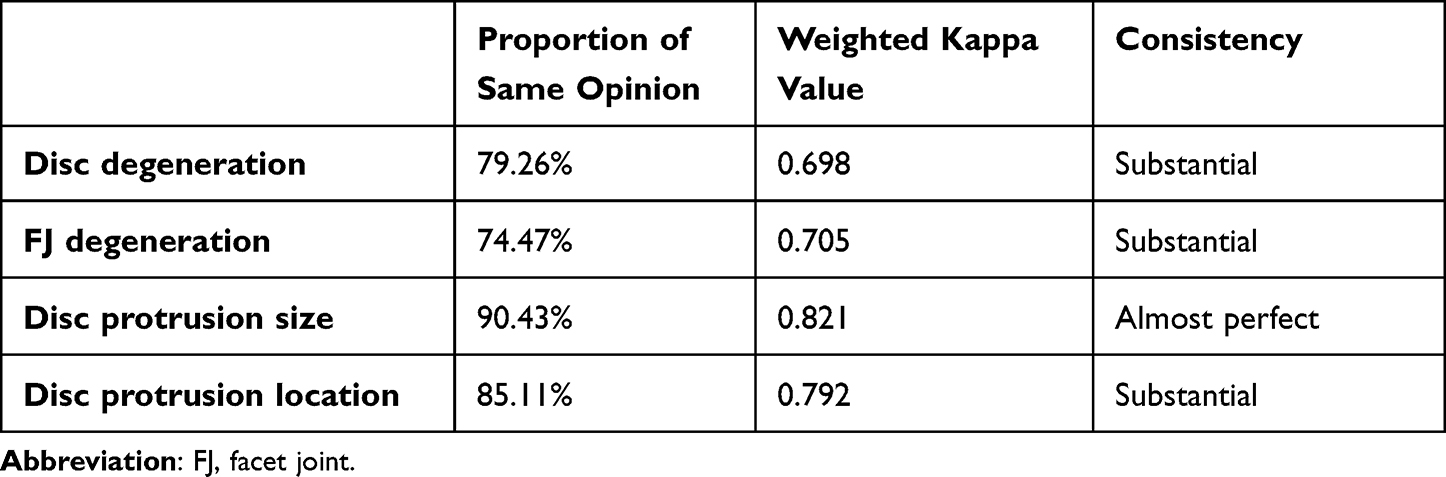 |
Table 3 Interobserver Agreement of Radiographic Parameters |
Discussion
The current study investigated the long-term impact of TELD on patients with LDH, in terms of both radiographic and clinical outcomes. Our results showed that after at least 2 years of follow-up, patients undergoing TELD achieved satisfying clinical outcomes; however, they experienced significant loss of disc height and aggravation of disc degeneration at the operated disc level. Our results also showed that the TELD procedure did not cause aggravation of facet joint degeneration at the long-term follow-up. Moreover, 12.77% of TELD-treated patients required additional surgery during the follow-up period.
Only a few case series have reported long-term follow-up radiographic outcomes after FED, and the disc height change was the most studied parameter. The studies by Lin et al and Sharma et al unanimously found that the disc height remained unchanged at 1-year follow-up compared with baseline.15,16 However, the results from studies with a larger sample size and longer follow-up showed different findings: Mahatthanatrakul et al reported a 67.7% reduction in disc size and 8.4% reduction in disc height at 12 months after TELD (31 patients);17 the 11.22-year follow-up results by Eun et al (38 patients) suggested that the disc height ratio was 81.54% of the original disc height;18 and the seven-year follow-up outcomes by Li et al (42 patients) showed that the postoperative disc height was 84.52%±5.66% of the preoperative disc height.19 However, these results are still not convincing due to the lack of a nonoperated comparator. We designed the control group by propensity score matching LDH outpatients, and further ascertained the disc height loss effect of FED. However, though the disc height was reduced after FED, the reduction was still not as great as that of traditional surgery at long-term follow-up.20,21
Our results also suggested that the disc protrusion size was reduced after FED, which was the basis of the therapeutic efficacy; however, such anticipated efficacy came at a cost of disc degeneration and risk of re-herniation. Similarly, Lin et al showed significant disc degeneration at 1-year follow-up after FED. The results from percutaneous endoscopic cervical discectomy also showed progression of degeneration at the corresponding level at long-term follow-up.22 A major limitation of previous results of degeneration grading is that it was based on subjective grading methods. To solve this problem, we used Pfirrmann grading for evaluation of disc degeneration and Weishaupt grading for evaluation of facet joint degeneration according to suggestions from Kettler et al,23 and we applied interobserver agreement to increase the reliability of the results. We showed that disc size grade was significantly reduced compared with the baseline in 70.21% of TELD-treated patients, which is in line with previous studies.15,22 Moreover, re-herniation of the index level occurred in 8.51% of TELD-treated patients, which is similar to the results of a previous meta-analysis (7.92%).24
TELD often requires foraminal reamer or drill to remove a part of superior articular process (SAP) to enlarge the foramen.25 Therefore, the procedure poses damage to the intervertebral disc and the SAP, which may cause mechanical deterioration of the spine. This is because both discectomy and foraminotomy cause the spinal instability, and the degree of such an effect is related to the amount of the removed disc.6,26,27 Moreover, previous studies have shown that disc removal may also affect the stability of the TJC of the adjacent levels.28 However, the studies on the effect of discectomy on spinal biomechanics are mostly finite element analyses. In contrast, our study investigated the long-term morphological changes in the TJC, and the results indicated aggravated disc degeneration, reduced disc height, and preserved the facet joints. Additionally, although spine fusion has been recognized as a risk factor for ASD,29 our results showed that ASD occurred in two patients treated without fusion, which from the clinical angle verified the impact of discectomy on the adjacent levels. This reminds of clinicians to be aware of ASD even after non-instrumented endoscopic discectomy, especially for patients with high risk factors (smoking, age, disc degeneration at adjacent segments, etc.).30–32
The advantages of this study are as follows: the propensity score method was used to match patients who did not undergo surgery as a control group to increase the reliability of radiographic results, and we adopted interobserver agreement to increase the internal consistency of imaging measurements. However, several limitations in our study should be noted. First, the retrospective nature and the small sample size compromised the reliability of the results. Then, the clinical outcomes of the conservative group were not collected or analyzed due to a considerable proportion of asymptomatic patients in the conservative group, which may have affected the credibility of clinical outcomes. Finally, the amount of disc removal is another factor affecting the radiographic changes after FED, but this information was not available in the current study.33
Conclusion
The long-term follow-up results showed that TELD was associated with the disc height loss, disc degeneration aggravation, and facet joint integrity. In addition, although patients after TELD can achieve good long-term clinical symptom relief, clinicians should be alert to re-herniation at the operated level and adjacent segment disease caused by changes in the local biomechanical environment. Our results may provide a certain reference value for future clinical practice and research.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. YL concepted and designed the study; MGZ collected the data and performed the analysis; YL and MGZ took part in manuscript drafting; SHL revised or critically reviewed the article; all authors have read and approved the final version of the manuscript, and agreed on the submission. All authors agreed to take responsibility and be accountable for the contents of the article.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Mayer HM, Brock M. Percutaneous endoscopic lumbar discectomy (PELD). Neurosurg Rev. 1993;16(2):115–120. doi:10.1007/BF00258242
2. Ahn Y. A historical review of endoscopic spinal discectomy. World Neurosurg. 2021;145:591–596. doi:10.1016/j.wneu.2020.08.008
3. Ruetten S, Komp M, Merk H, Godolias G. Full-endoscopic interlaminar and transforaminal lumbar discectomy versus conventional microsurgical technique: a prospective, randomized, controlled study. Spine. 2008;33(9):931–939. doi:10.1097/BRS.0b013e31816c8af7
4. Chen C, Yuchi CX, Gao Z, et al. Comparative analysis of the biomechanics of the adjacent segments after minimally invasive cervical surgeries versus anterior cervical discectomy and fusion: a finite element study. J Orthop Translat. 2020;23:107–112. doi:10.1016/j.jot.2020.03.006
5. Pan M, Li Q, Li S, et al. Percutaneous endoscopic lumbar discectomy: indications and complications. Pain Physician. 2020;23(1):49–56.
6. Li J, Xu C, Zhang X, et al. TELD with limited foraminoplasty has potential biomechanical advantages over TELD with large annuloplasty: an in-silico study. BMC Musculoskelet Disord. 2021;22(1):616. doi:10.1186/s12891-021-04504-1
7. Qian J, Yu SS, Liu JJ, Chen L, Jing JH. 全脊柱内镜下椎间孔成型对腰椎生物力学的影响 [Biomechanics changes of lumbar spine caused by foraminotomy via percutaneous transforaminal endoscopic lumbar discectomy]. Zhonghua Yi Xue Za Zhi. 2018;98(13):1013–1018. Chinese. doi:10.3760/cma.j.issn.0376-2491.2018.13.012
8. Kong MH, Hymanson HJ, Song KY, et al. Kinetic magnetic resonance imaging analysis of abnormal segmental motion of the functional spine unit. J Neurosurg Spine. 2009;10(4):357–365. doi:10.3171/2008.12.SPINE08321
9. von Elm E, Altman DG, Egger M, Pocock SJ, Gøtzsche PC, Vandenbroucke JP. The Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement: guidelines for reporting observational studies. PLoS Med. 2007;4(10):e296. doi:10.1371/journal.pmed.0040296
10. Jarman JP, Arpinar VE, Baruah D, Klein AP, Maiman DJ, Muftuler LT. Intervertebral disc height loss demonstrates the threshold of major pathological changes during degeneration. Eur Spine J. 2015;24(9):1944–1950. doi:10.1007/s00586-014-3564-8
11. Mysliwiec LW, Cholewicki J, Winkelpleck MD, Eis GP. MSU classification for herniated lumbar discs on MRI: toward developing objective criteria for surgical selection. Eur Spine J. 2010;19(7):1087–1093. doi:10.1007/s00586-009-1274-4
12. Pfirrmann CW, Metzdorf A, Zanetti M, Hodler J, Boos N. Magnetic resonance classification of lumbar intervertebral disc degeneration. Spine. 2001;26(17):1873–1878. doi:10.1097/00007632-200109010-00011
13. Weishaupt D, Zanetti M, Boos N, Hodler J. MR imaging and CT in osteoarthritis of the lumbar facet joints. Skeletal Radiol. 1999;28(4):215–219. doi:10.1007/s002560050503
14. McHugh ML. Interrater reliability: the kappa statistic. Biochem Med (Zagreb). 2012;22(3):276–282. doi:10.11613/BM.2012.031
15. Lin RH, Chen HC, Pan HC, et al. Efficacy of percutaneous endoscopic lumbar discectomy for pediatric lumbar disc herniation and degeneration on magnetic resonance imaging: case series and literature review. J Int Med Res. 2021;49(1):300060520986685. doi:10.1177/0300060520986685
16. Sharma SB, Lin G-X, Jabri H, et al. Radiographic and clinical outcomes of huge lumbar disc herniations treated by transforaminal endoscopic discectomy. Clin Neurol Neurosurg. 2019;185:105485. doi:10.1016/j.clineuro.2019.105485
17. Mahatthanatrakul A, Kotheeranurak V, Lin GX, Hur JW, Chung HJ, Kim JS. Comparative analysis of the intervertebral disc signal and annulus changes between immediate and 1-year postoperative MRI after transforaminal endoscopic lumbar discectomy and annuloplasty. Neuroradiology. 2019;61(4):411–419. doi:10.1007/s00234-019-02174-4
18. Eun SS, Lee SH, Sabal LA. Long-term follow-up results of percutaneous endoscopic lumbar discectomy. Pain Physician. 2016;19(8):E1161–e6.
19. Li X, Bai J, Hong Y, et al. Minimum seven-year follow-up outcomes of percutaneous endoscopic lumbar discectomy for lumbar degenerative disease. Int J Gen Med. 2021;14:779–785. doi:10.2147/IJGM.S293400
20. Lee SH, Chung SE, Ahn Y, Kim TH, Park JY, Shin SW. Comparative radiologic evaluation of percutaneous endoscopic lumbar discectomy and open microdiscectomy: a matched cohort analysis. Mt Sinai J Med. 2006;73(5):795–801.
21. Ren C, Qin R, Li Y, Wang P. Microendoscopic discectomy combined with annular suture versus percutaneous transforaminal endoscopic discectomy for lumbar disc herniation: a prospective observational study. Pain Physician. 2020;23(6):E713–E21.
22. Lee JH, Lee SH. Clinical and radiographic changes after percutaneous endoscopic cervical discectomy: a long-term follow-up. Photomed Laser Surg. 2014;32(12):663–668. doi:10.1089/pho.2014.3806
23. Kettler A, Wilke HJ. Review of existing grading systems for cervical or lumbar disc and facet joint degeneration. Eur Spine J. 2006;15(6):705–718. doi:10.1007/s00586-005-0954-y
24. Ruan W, Feng F, Liu Z, Xie J, Cai L, Ping A. Comparison of percutaneous endoscopic lumbar discectomy versus open lumbar microdiscectomy for lumbar disc herniation: a meta-analysis. Int J Surg. 2016;31:86–92. doi:10.1016/j.ijsu.2016.05.061
25. Pan Z, Ha Y, Yi S, Cao K. Efficacy of Transforaminal Endoscopic Spine System (TESSYS) technique in treating lumbar disc herniation. Med Sci Monit. 2016;22:530–539. doi:10.12659/MSM.894870
26. Zöllner J, Rosendahl T, Herbsthofer B, Humke T, Eysel P. Der Einfluß verschiedener Nucleotomietechniken auf die biomechanischen Eigenschaften der Bandscheibe [The effect of various nucleotomy techniques on biomechanical properties of the intervertebral disk]. Z Orthop Ihre Grenzgeb. 1999;137(3):206–210. German. . doi:10.1055/s-2008-1037394
27. Prado M, Mascoli C, Giambini H. Discectomy decreases facet joint distance and increases the instability of the spine: a finite element study. Comput Biol Med. 2022;143:105278. doi:10.1016/j.compbiomed.2022.105278
28. Cao R, He Y, Qian C, et al. Negative biomechanical effects of large grade nuclectomy in the transforaminal endoscopic discectomy increased the risk of adjacent segment diseases: a finite element study. J Clin Neurosci. 2021;93:141–146. doi:10.1016/j.jocn.2021.09.014
29. Radcliff KE, Kepler CK, Jakoi A, et al. Adjacent segment disease in the lumbar spine following different treatment interventions. Spine J. 2013;13(10):1339–1349. doi:10.1016/j.spinee.2013.03.020
30. Yamashita K, Ohzono K, Hiroshima K. Five-year outcomes of surgical treatment for degenerative lumbar spinal stenosis: a prospective observational study of symptom severity at standard intervals after surgery. Spine. 2006;31(13):1484–1490. doi:10.1097/01.brs.0000219940.26390.26
31. Mok JM, Cloyd JM, Bradford DS, et al. Reoperation after primary fusion for adult spinal deformity: rate, reason, and timing. Spine. 2009;34(8):832–839. doi:10.1097/BRS.0b013e31819f2080
32. Okuda S, Iwasaki M, Miyauchi A, Aono H, Morita M, Yamamoto T. Risk factors for adjacent segment degeneration after PLIF. Spine. 2004;29(14):1535–1540. doi:10.1097/01.BRS.0000131417.93637.9D
33. Heo JH, Kim CH, Chung CK, et al. Quantity of disc removal and radiological outcomes of percutaneous endoscopic lumbar discectomy. Pain Physician. 2017;20(5):E737–e46.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.