Back to Journals » Clinical Ophthalmology » Volume 19
Long-Term in vivo Positional Stability of a Suprachoroidal Telemetric Intraocular Pressure Sensor Implant
Authors Englisch CN ![]() , Wakili P, Trouvain AM, Van Drunen WJ
, Wakili P, Trouvain AM, Van Drunen WJ ![]() , Dick HB
, Dick HB ![]() , Mansouri K, Hoffmann EM, Mackert MJ
, Mansouri K, Hoffmann EM, Mackert MJ ![]() , Langenbucher A, Boden KT
, Langenbucher A, Boden KT ![]() , Szurman P
, Szurman P
Received 22 July 2025
Accepted for publication 24 September 2025
Published 20 December 2025 Volume 2025:19 Pages 4737—4745
DOI https://doi.org/10.2147/OPTH.S555570
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Colya N Englisch,1,2 Philip Wakili,1 André M Trouvain,1 Wouter J Van Drunen,3 H Burkhard Dick,4 Kaweh Mansouri,5,6 Esther M Hoffmann,7 Marc J Mackert,8 Achim Langenbucher,2 Karl T Boden,1,9 Peter Szurman1,9
1Eye Clinic Sulzbach, Knappschaft Hospitals Saar, Sulzbach/Saar, 66280, Germany; 2Department of Experimental Ophthalmology, Saarland University, Homburg/Saar, 66421, Germany; 3Implandata Ophthalmic Products GmbH, Hannover, 30159, Germany; 4Knappschaftskrankenhaus Eye Clinic, University Hospital of the Ruhr University Bochum, Bochum, Germany; 5Swiss Visio Glaucoma Research Centre, Montchoisi Clinic, Lausanne, Switzerland; 6Department of Ophthalmology, University of Colorado, Denver, CO, USA; 7Department of Ophthalmology, University Medical Centre of the Johannes Gutenberg University Mainz, Mainz, Germany; 8Department of Ophthalmology, LMU University Hospital, LMU Munich, Munich, Germany; 9Klaus Heimann Eye Research Institute (KHERI), Sulzbach/Saar, 66280, Germany
Correspondence: Colya N Englisch, Eye Clinic Sulzbach, Knappschaft Hospitals Saar, An der Klinik 10, Sulzbach/Saar, 66280, Germany, Email [email protected] André M Trouvain, Eye Clinic Sulzbach, Knappschaft Hospitals Saar, An der Klinik 10, Sulzbach/Saar, 66280, Germany, Email [email protected]
Background: The aim of this study was to evaluate the long-term in vivo positional stability of a novel suprachoroidal telemetric intraocular pressure (IOP) sensor implant.
Methods: In this prospective, open-label, multicenter interventional study, 24 patients undergoing nonpenetrating glaucoma surgery with simultaneous implantation of the suprachoroidal EyeMate-SC IOP sensor were considered (Implandata Ophthalmic Products GmbH, Hannover, Germany). Overall, 11 patients were excluded owing to incomplete data. Of the remaining patients, 11 were diagnosed with primary open-angle glaucoma, 1 with pseudoexfoliative glaucoma, and 1 with uveitic glaucoma. The sensor position was measured intraoperatively via surgical video analysis and postoperatively via swept-source anterior segment optical coherence tomography (Anterion, Heidelberg Engineering GmbH, Heidelberg, Germany) with reference to the anatomical limbus. Postoperative assessments were conducted at 10, 30, 90, 180, 270, 360, 540, 720, 900, and 1080 days.
Results: Unilateral implantation was successful in all 24 cases. No dislocations occurred. In one patient, partial suprachoroidal positioning was observed intraoperatively, with subsequent autonomous repositioning into full suprachoroidal placement within weeks. Excluding this case, the absolute implant position was 1.6 ± 0.8 mm at day 0, 1.7 ± 1.0 mm at day 360, 1.9 ± 1.8 mm at day 720, and 2.1 ± 0.9 mm at day 1080. Notably, the relationship between ΔIOP (Goldmann applanation tonometry – EyeMate-SC reading) and absolute implant position remained nonsignificant, regardless of whether the patient with the initially incomplete implantation was included (r = − 0.08, 95% CI: − 0.32 to 0.38) or excluded (r = − 0.11, 95% CI: − 0.37 to 0.36).
Conclusion: This study indicates high long-term in vivo positional stability of the EyeMate-SC IOP sensor. The observed variations were within measurement uncertainty. This supports the sensor’s potential for safe and continuous IOP monitoring in glaucoma care.
Keywords: glaucoma, intraocular pressure, telemetric monitoring, telemedicine, suprachoroidal sensor, positional stability
Introduction
Glaucoma is a progressive optic neuropathy that remains a leading cause of irreversible blindness worldwide, despite considerable research efforts.1 Lowering the intraocular pressure (IOP) is known to slow glaucoma progression.2,3 However, achieving favourable treatment outcomes with ocular hypotensive medications or glaucoma surgery depends on adequate IOP monitoring.4 Goldmann applanation tonometry (GAT) is the current gold standard for IOP measurement, but its intermittency often fails to capture IOP fluctuations.5–7
Continuous IOP monitoring using innovative approaches could overcome the limitations of infrequent measurements, enabling better detection of IOP fluctuations and improving the reliability of IOP assessment.5,6,8,9 Telemetric intraocular sensor devices have emerged as valuable tools for continuous IOP monitoring. We recently introduced the EyeMate-SC, a novel miniaturized IOP sensor designed for suprachoroidal implantation during nonpenetrating glaucoma surgery (NPGS), in a prospective, open-label, multicenter interventional trial.10–12 This implant enables on-demand IOP monitoring via an external wireless handheld reader (i.e., mesograph). The safety and measurement accuracy of the EyeMate-SC have been validated in reference to GAT,10–12 and its suprachoroidal placement has been shown not to impact long-term postoperative astigmatism.13
During implantation, an ophthalmic viscosurgical device (OVD) is used to expand the suprachoroidal cavity for implant insertion while protecting the surrounding tissues. After the OVD is resorbed, the sensor remains positioned between the choroid and sclera, with its convex side aligned with the concave scleral surface to ensure optimal pressure sensitivity. Importantly, the implant is not firmly anchored or sutured in place. Instead, it is stabilized by the surrounding choroidal tissue, which molds itself around the implant’s perimeter. Even slight device migration could result in complications such as vascular injury. A shift toward the macula would be particularly disastrous, posing a serious threat to vision. Therefore, this study aimed to evaluate the long-term in vivo positional stability of the EyeMate-SC IOP sensor.
Methods
Design
This study included data from the one-year prospective, open-label, single arm, multicenter interventional ARGOS-SC01 trial and the corresponding two-year follow-up ARGOS-SC01_FU trial.10–12 The study was conducted at Eye Clinic Sulzbach, the Eye Clinic at the University Hospital of the Ruhr University Bochum, the Swiss Visio Glaucoma Research Centre at Montchoisi Clinic in Lausanne, the Department of Ophthalmology in the University Medical Centre at Johannes Gutenberg University Mainz, and the Department of Ophthalmology at Ludwig-Maximilian University Hospital. The study adhered to the tenets of the Declaration of Helsinki, and each patient provided written informed consent. Ethics approval was obtained from the Institutional Review Board in charge (Ethikkommission bei der Ärztekammer des Saarlandes, ID: CIV-18-07-025065; Approval Number: 141/18; Date: 2018.10.30).
Patients
All patients were issued from the ARGOS-SC01 trial,10,11 had received an indication for NPGS (irrespective of trial enrollment), and were strictly eligible for unilateral sensor implantation. All female participants were required to present a negative pregnancy test within 24 h before surgery. Exclusion criteria included neovascular and angle-closure glaucoma, axial myopia exceeding –6 diopters (D), hyperopia greater than +4 D, axial length outside the range of 22–26 mm, other known ocular pathologies, previous glaucoma surgery, non-glaucoma ocular surgery within 6 months and cataract surgery within 3 months prior to EyeMate-SC implantation. Patients with active electronic medical implants in the head or neck region or with severe systemic disease were also excluded.
Device
The EyeMate-SC is a microelectromechanical IOP sensor device designed for implantation in the suprachoroidal space [Figure 1A; 7.5 × 3.5 mm (length × width) with a thickness gradually tapering from 1.3 mm in the middle to 0.9 mm in the periphery; Implandata Ophthalmic Products GmbH, Hannover, Germany]. The lenticular outer surface smoothly adapts to the curved shape of the inner sclera (Figure 1B). Its application-specific integrated circuit (ASIC) incorporates pressure and temperature sensors, identification and analog-to-digital encoders, and a telemetry unit. The ASIC is connected to a wire-wound gold microcoil and is embedded within a soft medical-grade silicone material with a well-established biocompatibility profile. Importantly, the device, strictly containing non-magnetic metals (aluminum and gold), is magnetic resonance (MR) conditional and thus allows for MR imaging scans.
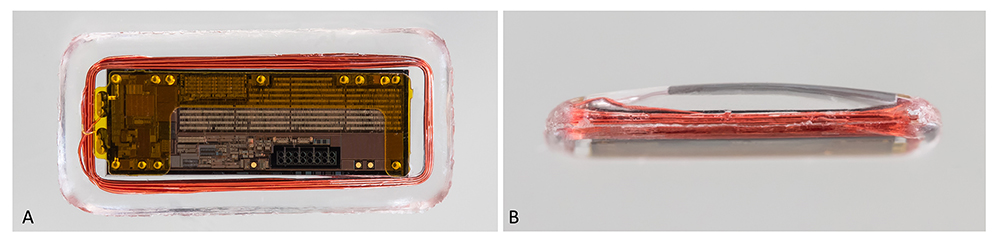 |
Figure 1 EyeMate-SC sensor device (A) 7.5 × 3.5 mm (length × width) with a centrifugal decreasing thickness from 1.3 mm in the middle to 0.9 mm in the periphery with a lenticular-shaped outer surface (B). |
The sensor is calibrated prior to sterilization, and test IOP measurements are performed to check for plausibility before implantation. Measurement data can be retrieved either wired or wirelessly from a separate handheld reader device (i.e., mesograph), which can store up to 3000 readings. For high precision, each read builds the average of 10 consecutive measurements within 1 s. The battery-free sensor harvests energy via electromagnetic coupling from the reader device that in turn acts as a power source.
Surgery
The device was implanted either during nonpenetrating deep sclerectomy or canaloplasty. After conjunctival opening at 12 o’clock, a 5 × 5 mm superficial scleral flap was created. Depending on the surgeon’s preference, a deeper scleral flap (4 × 4 mm) was prepared, leaving a basal thin scleral flap of 10–50 µm (90% thickness technique) or until complete choroid exposure (100% thickness technique). Afterwards, the deep scleral flap was augmented beyond the scleral spur to incise the Schlemm canal and create a trabecular Descemet window. Then, the deep scleral flap was excised and the juxtacanalicular trabecular meshwork peeled. For canaloplasty, the Schlemm canal was probed using a microcatheter and tightened with a 10–0 Prolene suture. The scleral window was enlarged using OVD to enable smooth EyeMate-SC sensor device insertion between the choroid and sclera, just behind the ciliary body, at a right angle to the limbus, limbus parallel, or at an angle of 45° towards the limbus. Padded forceps were used to protect the sensor’s sensitive composites. No artificial fixation of the sensor, such as suturing, was performed. Finally, the superficial scleral flap and conjunctiva were sutured watertight.
Measurements
Device position measurements were scheduled on the day of implantation (D0), after 10 days (D10), 30 days (D30), 90 days (D90), 180 days (D180), 270 days (D270), 360 days (D360), 540 days (D540), 720 days (D720), 900 days (D900), and 1080 days (D1080).
Before closing the superficial scleral flap (D0), the position of the implant between the anatomical limbus and the eye equator was assessed based on available surgery video recordings and analyzed on a frame-to-frame basis. The implant position was defined as the distance between the EyeMate-SC sensor’s most centrally placed edge and the anatomical limbus. At a 45° orientation toward the limbus, the distance was measured from the implant’s corner, whereas for a parallel orientation, it was measured from the closest point of the implant’s long side to the anatomical limbus. The sensor device’s width of 3.5 mm served as the scaling reference (Figure 2A–C).
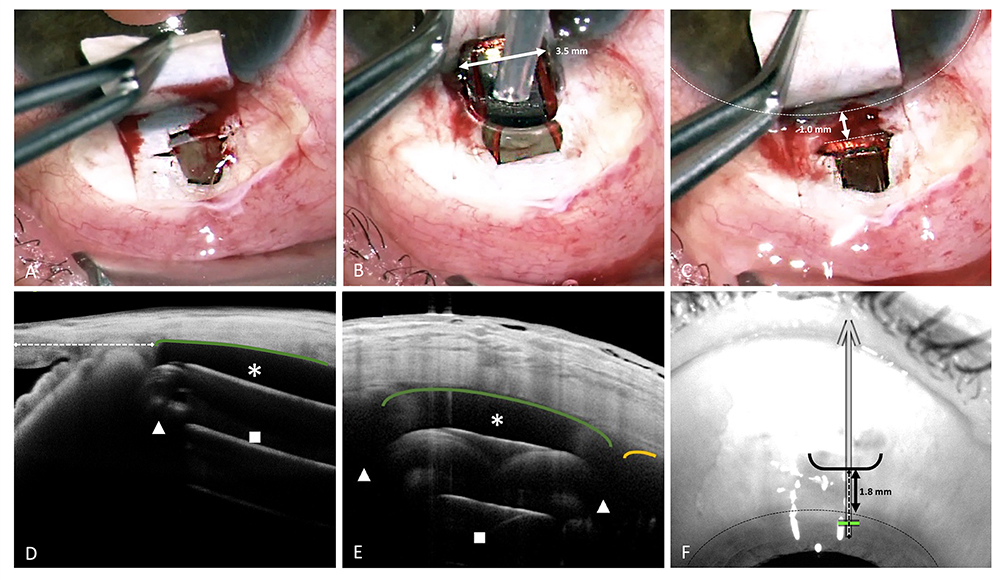 |
Figure 2 Determination of the EyeMate-SC sensors’ position intraoperatively (A–C) and postoperatively (D–F). Suprachoroidal implantation of the EyeMate-SC sensor device: Preparation with 100% thickness technique: the deep flap is prepared until the choroid is completely exposed (A). At the end of nonpenetrating glaucoma surgery, viscoelastics are injected into the suprachoroidal space, and the EyeMate-SC sensor is carefully inserted using padded implantation forceps (B). Before closing the superficial scleral flap (C), the EyeMate-SC sensor’s position relative to the anatomical limbus was determined using the EyeMate-SC sensor’s dimensions as a reference (B). Imaging 6 months after suprachoroidal implantation of the EyeMate-SC sensor using anterior segment optical coherence tomography (AS-OCT) with meridional [(D) longitudinal sensor cut] and limbus-parallel [(E) transversal sensor cut] scans and the corresponding overview image (F). The sensor remained stable between the choroid (orange line) and sclera at the site of implantation. The AS-OCT image horizontal width (D) corresponds to the scan length (here B-scan length of 12.00 mm). The scan’s orientation and direction is depicted as a superimposed arrow with corresponding length on the overview image (F). AS-OCT visualizes the microelectronics carrier substrate (■) and gold coil (▲), but not the silicone encapsulation (* and green line adjacent to sclera). |
For longitudinal postoperative assessment (D10, 30, 90, 180, 270, 360, 540, 720, 900, and 1080), the implant position was determined using, whenever available, swept-source anterior segment optical coherence tomography (AS-OCT; Anterion, Heidelberg Engineering GmbH, Heidelberg, Germany) and the Heidelberg Eye Explorer image-management platform (HEYEX, Heidelberg Engineering GmbH, Heidelberg, Germany). Figure 2D–F shows how the position of the EyeMate-SC sensor was determined in the corresponding AS-OCT’s overview image [Figure 2F: 1.8 mm from the anatomical limbus, obtained by correlation of the AS-OCT scan (Figure 2D) to the AS-OCT’s overview image (Figure 2F)].
Starting at D10, IOP was measured using both the EyeMate-SC sensor and GAT, as previously described.10–12
Analysis
Statistical analysis was performed using GraphPad Prism software (Version 10.3.0). Absolute and relative implant position data (i.e., referring to the intraoperative baseline position, D0) are represented as mean ± standard deviation. To investigate the implant’s positional measurement accuracy over time, the 95% confidence interval (CI) was determined. The relationship between absolute implant position and ΔIOP (GAT − EyeMate-SC reading) was assessed using Spearman correlation analysis.
Results
A total of 24 patients were subjected to NPGS with simultaneous implantation of the suprachoroidal telemetric EyeMate-SC IOP sensor. A total of 11 patients were excluded from further analysis owing to lack of data: in 9 patients, postoperative AS-OCT measurements were unavailable, and in another 2 patients, measurements were insufficient for time-course analysis. This is because a number of study centers either did not install or did not have available the optional swept-source AS-OCT device for imaging the anterior segment at one or more visits.
Of the remaining 13 patients (6 male and 7 female) that were eligible for analysis, 11 had been diagnosed with primary open-angle glaucoma, 1 with pseudoexfoliative glaucoma, and 1 with uveitic glaucoma. The mean age at surgery was 66.6 ± 9.0 years. Among the eyes, 8 were right and 5 left. A total of 7 eyes were phakic, 4 were pseudophakic, and 2 additional phakic eyes were subjected to simultaneous phacoemulsification and NPGS. Altogether, 10 eyes underwent canaloplasty, and 3 eyes received deep sclerectomy. The mean number of topical antiglaucomatous medications was 2.1 ± 1.2 (range: 0–4).
Implantation was successful in all cases. In one case, implant insertion in the suprachoroidal space was incomplete, with one-sixth of the implant resting on the thin scleral lamella resulting from the 90% preparation technique. However, this proved to be a temporary situation: by day 90, the implant had completely flipped back into the suprachoroidal space (Figure 3A–C). No implant dislocations, trauma signs, or biocompatibility issues were noted.
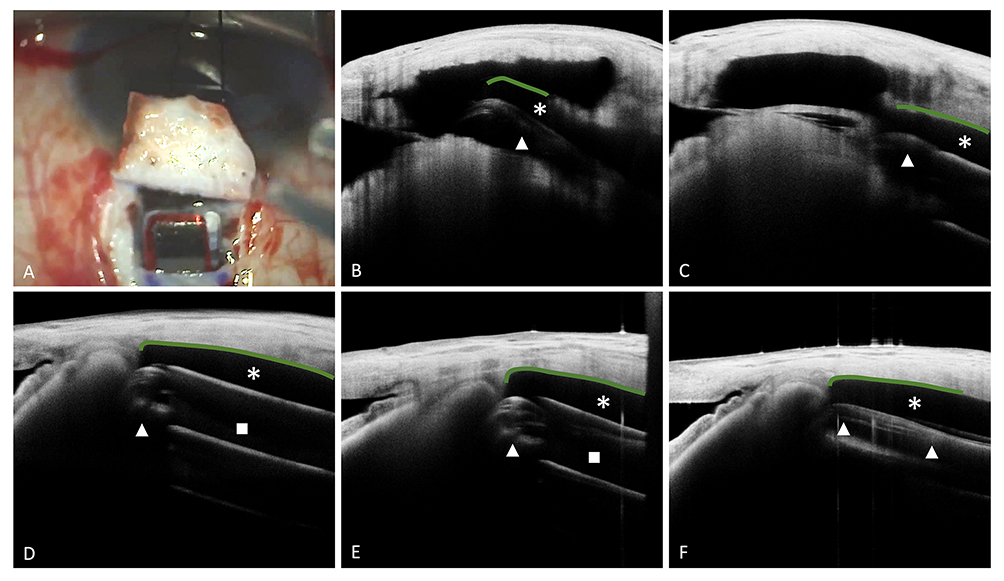 |
Figure 3 EyeMate-SC sensor’s position over time for the case of incomplete suprachoroidal placement (A–C) and in a normal case (D–F). Intraoperative photography of the former case, in which the EyeMate-SC sensor was incompletely placed in the suprachoroidal space initially, with one-sixth of the implant resting on the thin scleral lamella. The green line demarcates silicone encapsulation of the sensor (A). Corresponding anterior segment optical coherence tomography (AS-OCT) image at 10 days postoperatively (B), after which the position of the EyeMate-SC sensor changed minimally, stabilizing the implant in the suprachoroidal space [(C) AS-OCT image at 3 months]. Example of a normal course at midterm [(D) 12 months], mid to long term [(E) 24 months], and long term [(F) 30 months]. The EyeMate-SC sensor lies in the suprachoroidal space, as intended, and fits with the concave inner scleral surface. Its position is stable, with no evidence of migration or dislocation. AS-OCT visualizes the microelectronics carrier substrate (■) and gold coil (▲), but not the silicone encapsulation (* and green line adjacent to sclera). |
Measurement data from video recordings on D0 were available for 8 of the 13 patients. In any case, postoperative AS-OCT imaging was used for follow-up positional analysis of the EyeMate-SC sensor. In all but three cases, the EyeMate-SC sensor’s orientation was meridional, that is, at a right angle to the anatomical limbus and towards the equator of the eye, as shown in Figure 2 (0°, i.e., short side of the implant oriented towards the limbus). At the surgeon’s discretion and in line with the manufacturers’ instructions for use, the devices were placed limbus parallel (90°, i.e., long side of the implant oriented towards the limbus) in two cases, and at an angle of 45° towards the limbus and oriented towards the lateral side of the eye in one case.
Of the 130 possible AS-OCT measurements (13 patients × 10 postoperative visits), 53 were used in total. An additional 32 AS-OCT images were available but unprocessable for this analysis owing to missing reference points such as AS-OCT overlays and the inability to determine the closest distance between the implant and anatomical limbus. This limitation arose from issues related to limbus-parallel AS-OCT imaging of the implant or meridional AS-OCT imaging at an angle to the implant. “No participation” or “voluntary withdrawal” were recorded in four cases, leading to a loss of 12 data points. In 33 cases, AS-OCT measurements were not performed as part of the visit-related examinations for unspecified reasons.
Figure 3D–F illustrates a typical course with a stable implant. Figure 4A displays the individual courses of the absolute implant position throughout the observation period. Excluding the patient of initial partial suprachoroidal positioning, implant position relative to the anatomical limbus was 1.6 ± 0.8 at D0, 1.7 ± 1.0 at D360, 1.9 ± 1.8 at D720, and 2.1 ± 0.9 mm at D1080.
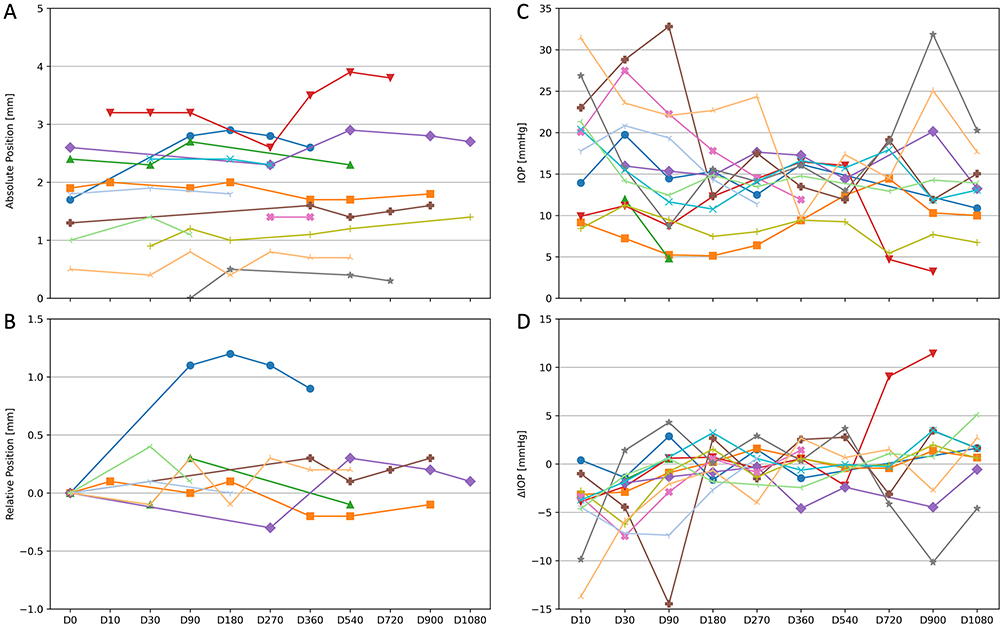 |
Figure 4 Absolute implant position throughout the observation period (mm). A total of 8, 2, 7, 8, 7, 6, 7, 8, 3, 3, and 2 measurements were available for D0, 10, 30, 90, 180, 270, 360, 540, 720, 900, and 1080, respectively (A). Relative implant position for the patients for whom initial video recording–based implant-to-limbus distance determination was possible. Data are presented as differences between values from follow-up time points and baseline (mm). A total of 8, 1, 4, 5, 4, 3, 4, 5, 1, 3, and 1 measurements were available for D0, 10, 30, 90, 180, 270, 360, 540, 720, 900, and 1080, respectively (B). EyeMate-SC IOP (C) and ΔIOP (Goldmann applanation tonometry – EyeMate-SC reading) (D) data recorded for each patient and starting at D10. Each symbol represents one patient’s data. |
Figure 4B displays the individual courses of the relative implant position (i.e., for the patients whose initial video recording–based absolute implant positions could be determined). A change of ~1 mm in the relative implant position was observed only in the case in which the implant was initially not fully inserted into the suprachoroidal space but shifted spontaneously into the correct position, where, notably, it remained stable.
As the uncertainty in implant-to-limbus distances is high, the obtained absolute implant positions are estimated to be accurate to ± 0.5 mm (i.e., 95% CI). Of note, the initial video recording–based measurements and the earliest postoperative OCT were highly correlated (r = 0.99, P < 0.01, Spearman; excluding the case of initial partial suprachoroidal positioning).
Figure 4C shows the IOP data from the EyeMate-SC, and Figure 4D displays the ΔIOP (GAT – EyeMate-SC reading) for each patient and visit. As shown in Figure 5, the relationship between ΔIOP and absolute implant position remained nonsignificant, regardless of whether the patient with incomplete initial implantation was included (r = −0.08, 95% CI: −0.32 to 0.38) or excluded (r = −0.11, 95% CI: −0.37 to 0.36).
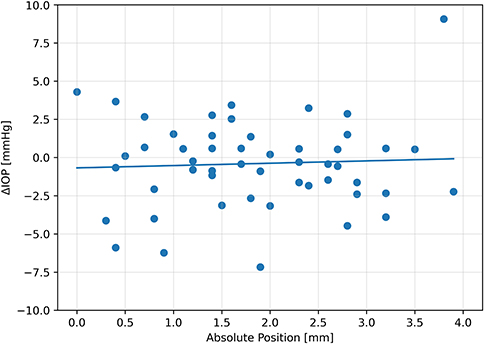 |
Figure 5 Relationship between ΔIOP (Goldmann applanation tonometry – EyeMate-SC reading) and absolute implant position in the 13-patient collective (i.e., including the patient with incomplete initial implantation). |
Discussion
This study’s main objective was to investigate the long-term in vivo positional stability of the EyeMate-SC sensor. This assessment is based on original implantation video recording analysis and longitudinal AS-OCT data on the implant’s intraocular position over a three-year period.
Overall, the AS-OCT imaging analysis confirms dihedral angle matching between the implant’s convex scleral side and the sclera’s concave inner surface, as indicated by the long-term in vivo positional stability of the implant in the suprachoroidal space. Of note, the implant is not firmly anchored or sutured in place. Instead, it is stabilized by the surrounding choroidal tissue, which molds itself around the implant’s perimeter, leaving room for migration.
Adverse effects such as implant dislocation, trauma signs, migration, or potential biocompatibility issues were not observed. Even in the patient whose implant was only partially inserted into the suprachoroidal space initially, the implant remained stable throughout the follow-up period, after spontaneously slipping into the correct position within several weeks. This minimal shift in implant position supports the anatomical compatibility between implant and eye.
Overall, long-term variations in IOP sensor limbal distance measurements relative to the initial intraoperative position were minimal, deemed negligible, and not attributable to actual position changes. Thus, the suprachoroidal position at 12 o’clock, just behind the ciliary body, appears to be a good location for sensor placement. This assessment is also based on the fact that no unintended effects or adverse events were reported during the ARGOS-SC01/FU trials.10–12 Adverse effects arising directly from positional implant instability could potentially include impaired retinal function, optical image distortion, perforation of the residual Descemet’s membrane, or IOP measurement capacity deterioration. In addition, the dataset shows no evidence that ΔIOP, as an indicator of telemetric accuracy relative to GAT, depends on sensor position within the observed range.
While implant position within the suprachoroidal space and surrounding tissue layers can be assessed using AS-OCT imaging, the in-depth information of the eye globe obtained using AS-OCT does not reflect the real layer thickness within the eye, as for this, knowledge of the respective refractive index is required. Nevertheless, the horizontal scan length corresponds to the actual scan length and thus allows for accurate estimates.
The accuracy of the obtained absolute implant position (i.e., implant-to-limbus distance) may be affected by several factors and is therefore difficult to quantify. On the one hand, the implant position is determined by analysing implantation video recordings initially while analysing AS-OCT images for follow-up. Secondly, although the resolution of the AS-OCT images is good, it is still limited. No minimum-quality threshold was defined as long as mandatory reference points (i.e., AS-OCT overlays, anatomical limbus, and the implant’s most central edge) were visible. Implant position was analyzed using HEYEX reports, with AS-OCT scan length chosen at the examiner’s discretion. Furthermore, the anatomical limbus position was estimated, directly affecting the measured shortest implant-to-limbus distance. As a result, the implant-to-limbus distance measurements are estimates of the absolute values, even though repeated implant-to-limbus distance measurements indicate an accuracy of ± 0.5 mm. Finally, our study is limited by its small sample size, highlighting the need for future research on larger cohorts to draw definitive conclusions regarding the positional stability of the EyeMate-SC device. Notably, the major reason that nearly half (i.e., 11 of 24) of the participants were not included in the analysis was the lack of available OCT data. Not all examination sites had the swept-source AS-OCT device available or installed. The availability of this AS-OCT device was not a prerequisite of the clinical ARGOS-SC01 and ARGOS-SC01_FU trials.10–12 In 33 cases, AS-OCT measurements were not performed for unspecified reasons; however, this was unrelated to the implant, as all other visit-related examinations were completed uneventfully.10–12
Taken together, the EyeMate-SC IOP sensor itself is atraumatic, and long-term evaluation displays no signs of device migration or dislocation. These findings indicate that this novel suprachoroidal device has high in vivo positional stability, ultimately reinforcing its tremendous potential clinical benefits in the context of IOP monitoring, and even more broadly, of glaucoma treatment.
Data Sharing Statement
Data can be obtained from the corresponding author (CNE) upon reasonable request.
Ethics Statement and Consent for Publication
The study was approved by the local Institutional Review Board (Ethikkommission bei der Ärztekammer des Saarlandes, ID: CIV-18-07-025065; Approval Number: 141/18; Date: 2018.10.30) and adhered to the tenets of the Declaration of Helsinki. Written informed consent was obtained from each patient after explanation of the nature and possible consequences of the study.
Acknowledgments
We thank Stefan Meyer for great statistical and visualization support.
Author Contributions
Research design: C.N.E. and P.S.; Data acquisition: C.N.E., W.J.V.D., K.M., H.B.D., E.M.H., M.J.M., and P.S.; Data analysis: C.N.E. and W.J.V.D.; Interpretation: C.N.E., P.W., A.T., W.J.V.D., K.M., H.B.D., E.M.H., M.J.M., A.L., K.T.B. and P.S.; Writing – original draft: C.N.E.; Writing – review and editing: C.N.E., P.W., A.T., W.J.V.D., K.M., H.B.D., E.M.H., M.J.M., A.L., K.T.B. and P.S.; All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study received support from Implandata Ophthalmic Products GmbH (Hannover, Germany), which produced and provided the medical devices under investigation.
Disclosure
P.S. has a pending international patent for the EyeMate-SC system (PCT/EP2015/062976). E.M.H. reports grants from Allergan, Novartis, Heidelberg Engineering, Santen, and Thea which are unrelated to the submitted work. K.M. reports grants from Implandata and unrelated financial disclosures from Santen, Abbvie, New World Medical, and iStar Medical. M.M. reports grants from Implandata and unrelated financial disclosures from Abbvie, Acufocus, Alcon, Allergan, Bausch and Lomb, Bayer, DORC, Heidelberg Engineering, iStar, Iridex, SightSciences, Novartis, Oculus, Optos, Roche, Santen, Topcon, and Zeiss. W.J.V.D. is an employee at Implandata Ophthalmic Products GmbH. The authors report no other conflicts of interest in this work.
References
1. Vision Loss Expert Group of the Global Burden of Disease S, Blindness GBD, Vision Impairment C. Global estimates on the number of people blind or visually impaired by glaucoma: a meta-analysis from 2000 to 2020. Eye. 2024;38(11):2036–2046. doi:10.1038/s41433-024-02995-5
2. Weinreb RN, Leung CK, Crowston JG, et al. Primary open-angle glaucoma. Nat Rev Dis Primers. 2016;2:16067. doi:10.1038/nrdp.2016.67
3. Huang AS, Minasyan L, Weinreb RN. Glaucoma-intraocular pressure reduction. Handb Exp Pharmacol. 2017;242:181–207. doi:10.1007/164_2016_24
4. Konstas AG, Kahook MY, Araie M, et al. Diurnal and 24-h intraocular pressures in glaucoma: monitoring strategies and impact on prognosis and treatment. Adv Ther. 2018;35(11):1775–1804. doi:10.1007/s12325-018-0812-z
5. Aptel F, Weinreb RN, Chiquet C, Mansouri K. 24-h monitoring devices and nyctohemeral rhythms of intraocular pressure. Prog Retin Eye Res. 2016;55:108–148. doi:10.1016/j.preteyeres.2016.07.002
6. Gazzard G, Jayaram H, Roldan AM, Friedman DS. When gold standards change: time to move on from Goldmann tonometry? Br J Ophthalmol. 2021;105(1):1–2. doi:10.1136/bjophthalmol-2020-317112
7. Brusini P, Salvetat ML, Zeppieri M. How to measure intraocular pressure: an updated review of various tonometers. J Clin Med. 2021;10(17):3860. doi:10.3390/jcm10173860
8. Wu KY, Mina M, Carbonneau M, Marchand M, Tran SD. Advancements in wearable and implantable intraocular pressure biosensors for ophthalmology: a comprehensive review. Micromachines. 2023;14(10):1915. doi:10.3390/mi14101915
9. Englisch CN, Trouvain A, Wakili P, et al. Intraocular pressure fluctuations recorded by a telemetric sensor after nonpenetrating glaucoma surgery in primary open-angle glaucoma. Ophthalmol Glaucoma. 2025. doi:10.1016/j.ogla.2025.07.007
10. Szurman P, Gillmann K, Seuthe AM, et al. EYEMATE-SC trial: twelve-month safety, performance, and accuracy of a suprachoroidal sensor for telemetric measurement of intraocular pressure. Ophthalmology. 2023;130(3):304–312. doi:10.1016/j.ophtha.2022.09.021
11. Szurman P, Mansouri K, Dick HB, et al. Safety and performance of a suprachoroidal sensor for telemetric measurement of intraocular pressure in the EYEMATE-SC trial. Br J Ophthalmol. 2023;107(4):518–524. doi:10.1136/bjophthalmol-2021-320023
12. Micheletti E, Mansouri K, Dick HB, et al. Long-term safety and performance of a suprachoroidal pressure sensor system: results of the EYEMATE-SC trial follow-up study. Ophthalmology. 2025;132:775–784. doi:10.1016/j.ophtha.2025.01.021
13. Englisch CN, Boden KT, Szurman P, et al. Long-term astigmatism after intraocular pressure sensor implantation and nonpenetrating glaucoma surgery: EYEMATE-SC trial. J Cataract Refract Surg. 2024;50(9):899–905. doi:10.1097/j.jcrs.0000000000001470
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Efficacy and Patient Tolerability of Omidenepag Isopropyl in the Treatment of Glaucoma and Ocular Hypertension
Matsuo M, Matsuoka Y, Tanito M
Clinical Ophthalmology 2022, 16:1261-1279
Published Date: 26 April 2022
Retrospective Analysis of Switching Bimatoprost 0.01% to Bimatoprost 0.03% in Patients with Various Types of Glaucoma and Ocular Hypertension
Xu KM, Cho R, Chan TYB
Clinical Ophthalmology 2022, 16:2385-2390
Published Date: 29 July 2022
Multicenter Effectiveness and Disease Stability Through 3 Years After iStentTrabecular Micro-Bypass with Phacoemulsification in Glaucoma and Ocular Hypertension
Clement C, Howes F, Ioannidis A, Shiu M, Manning D, Lusthaus JA, Skalicky SE, Goodwin TW
Clinical Ophthalmology 2022, 16:2955-2968
Published Date: 1 September 2022
Triple Fixed-Combination Bimatoprost/Brimonidine/Timolol in Glaucoma and Ocular Hypertension in India: A Multicenter, Open-Label, Phase 3 Study
Menon MG, Goodkin ML
Clinical Ophthalmology 2022, 16:3559-3569
Published Date: 20 October 2022
Trabeculectomy Vs Non‐penetrating Deep Sclerectomy for the Surgical Treatment of Open-Angle Glaucoma: A Long-Term Report of 201 Eyes
Correia Barbosa R, Gonçalves R, Bastos R, Alves Pereira S, Basto R, Viana AR, Tenedório P
Clinical Ophthalmology 2023, 17:1619-1627
Published Date: 6 June 2023