Back to Journals » Journal of Pain Research » Volume 15
Long-Term Exposure to Morphine Induces Cross-Tolerance to Acute Antinociceptive Effect of Remifentanil on Somatic and Visceral Stimuli in Rats
Authors Mori H, Hashimoto T, Nikai T, Furuya M, Hattori M, Katsube Y, Saito Y ![]()
Received 14 September 2022
Accepted for publication 15 November 2022
Published 22 December 2022 Volume 2022:15 Pages 4047—4054
DOI https://doi.org/10.2147/JPR.S389929
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor E Alfonso Romero-Sandoval
Hideaki Mori,1 Tatsuya Hashimoto,1 Tetsuro Nikai,1 Motohide Furuya,2 Mai Hattori,1 Yukiko Katsube,1 Yoji Saito1
1Department of Anesthesiology, Shimane University Faculty of Medicine, Izumo, Shimane, Japan; 2Department of Psychiatry, Shimane University Faculty of Medicine, Izumo, Shimane, Japan
Correspondence: Tatsuya Hashimoto, Department of Anesthesiology, Shimane University Faculty of Medicine, 89-1 Enya-Cho, Izumo, Shimane, 693-8501, Japan, Tel +81-853-20-2295, Fax +81-853-20-2292, Email [email protected]
Purpose: Remifentanil is one of the most commonly used opioids intraoperatively. Previous reports indicate that long-term use of opioids may lead to cross-tolerance to remifentanil, which poses a challenge in the control of acute pain intraoperatively. However, there is limited information regarding cross-tolerance to remifentanil, especially in visceral pain. Therefore, this study aimed to examine cross-tolerance to remifentanil in somatic and visceral tolerance using morphine-tolerant rats.
Methods: Six male Sprague-Dawley rats were allocated to the morphine and saline groups each. Tolerance to the antinociceptive effect of morphine was induced in rats in the morphine group. Remifentanil was continuously infused intravenously at 10 mcg/kg/min for 120 min to assess cross-tolerance from morphine to remifentanil. The antinociceptive effects on somatic and visceral nociceptive stimuli were measured using the tail-flick (TF) and colorectal distension (CD) tests, respectively. The antinociceptive efficacy was evaluated by converting the response threshold to the percentage maximal possible effect (%MPE).
Results: Remifentanil increased the %MPE in the morphine and saline groups in both the tests; however, the increase in %MPE was attenuated significantly in the morphine group compared with that in the saline group at 60, 90, and 120 min (all P < 0.01) in the TF test and at 90 and 120 min in the CD test (all P < 0.05).
Conclusion: Our results indicate that morphine-tolerant rats exhibit cross-tolerance to remifentanil’s acute antinociceptive effects on somatic and visceral stimuli. Cross-tolerance to remifentanil should be considered in the perioperative management of patients using morphine.
Keywords: remifentanil, morphine, cross-tolerance, somatic, visceral
Introduction
Opioids are the most common and widely used drugs in the treatment of acute, chronic, and cancer pain.1 However, long-term use of opioids may lead to analgesic tolerance and cross-tolerance to other opioids, which can cause an apparent decrease in analgesic efficacy and a simultaneous severe deterioration in the quality of life of patients.2 Therefore, the emergence of opioid tolerance and cross-tolerance is a serious medical problem among patients with long-term opioid use.
Opioid tolerance has been extensively studied, and many studies have elucidated the characteristics of opioid tolerance, including its onset, time course, and magnitude.3 However, studies about cross-tolerance on analgesic effects between opioids used intraoperatively are limited. Some clinical reports have indicated that the long-term use of opioids before surgery increases the dosage of opioids used intraoperatively.4,5 In the perioperative setting, opioid cross-tolerance may diminish analgesic effectiveness during surgery in patients with long-term opioid use; therefore, acute pain management for these patients has been a clinical challenge.6 Remifentanil is ultra-short-acting and good at regulation, enabling hemodynamic stability and rapid recovery with minimal side effects,7 which leads to its frequent use intraoperatively. Several studies have demonstrated that remifentanil is also associated with acute analgesic tolerance,8,9 and a few clinical studies have suggested that preoperative long-term opioid usage causes cross-tolerance to remifentanil antinociceptive effects.10
Nociceptive pain can be classified into somatic and visceral types. Recently, it was reported that visceral and somatic pain differ in many neurobiological mechanisms that mediate sensation.11 A key point of anesthesia management is to consider the pain pathway arising from somatic or visceral. However, previous studies on opioid tolerance mainly focused on somatic pain. Only a few studies have examined the development of opioid tolerance to visceral antinociception caused by long-term opioid use;12 therefore, further research is warranted.
Information on cross-tolerance from opioids used preoperatively to remifentanil administered intraoperatively is vital for analgesic management in the perioperative period. However, there is limited information about cross-tolerance to remifentanil, especially in visceral pain. Morphine is a commonly used opioid preoperatively. Therefore, this study aimed to examine cross-tolerance from morphine to remifentanil antinociceptive effects, especially the difference between somatic and visceral tolerance, using morphine-tolerant rats.
Materials and Methods
Animals
All experiments were approved by the Animal Care and Use Committee of Shimane University (approval no. IZ27-128) and complied with the Guide for the Care and Use of Laboratory Animals of Japan.
Male Sprague-Dawley rats weighing 200–250 g (CLEA Japan, Tokyo, Japan) were used in this study. They were housed in individual cages and maintained on a 12-h light and 12-h dark cycle at 24 ± 1°C and provided free access to food and water. The rats were acclimatized to the cage and experimental environment for 4 days before the experiments. We randomly assigned 12 rats to the morphine and saline groups (n = 6 per group). Figure 1 illustrates the experimental schedule. The exclusion criterion was only weight loss. If the rats lost more than 20% of their body weight due to eating or drinking disorders compared with that at the beginning of the experiment, they were excluded and euthanized.
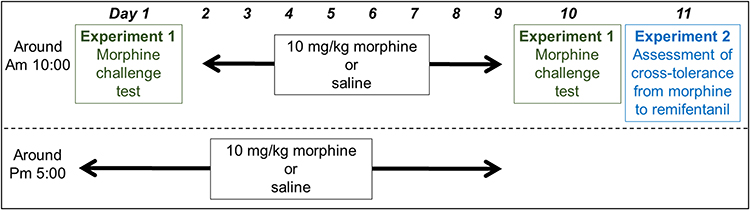 |
Figure 1 Timeline of the experimental schedule. |
Inducing Morphine Tolerance
After the challenge test on day 1, at approximately 5:00 pm, 10 mg/kg morphine (Takeda Pharmaceutical, Tokyo, Japan) dissolved in physiological saline was injected subcutaneously in the morphine group or saline in the saline group. Thereafter, from day 2 to day 9, 10 mg/kg morphine or saline was injected subcutaneously twice a day (around 10:00 am and 5:00 pm) in the morphine and saline groups, respectively, to induce tolerance to the antinociceptive effect of morphine. The morphine doses were determined by referring to a previous study that reported injecting 10 mg/kg morphine subcutaneously twice a day for 8 days.13
Morphine Challenge Test (Experiment 1)
For the challenge test on days 1 and 10, the rats in the morphine group were administered 5 mg/kg morphine subcutaneously to examine the development of morphine tolerance, whereas those in the saline group were administered equal amounts of saline.
Assessment of Cross-Tolerance from Morphine to Remifentanil (Experiment 2)
On day 11, a continuous intravenous infusion of 10 mcg/kg/min of remifentanil was administered to assess cross-tolerance from morphine to remifentanil. Referring to our unique animal study in which remifentanil was administered continuously and intravenously to rats;14 the dose of remifentanil was set at 10 mcg/kg/min to ensure that the cutoff value was achieved in the control group. The tail vein at the tail root of each rat was flushed with heparinized saline after inserting a 24-gauge catheter (Jelco Clear, Smiths Medical Japan, Tokyo, Japan). Remifentanil (Ultiva, Janssen Pharmaceuticals, Tokyo, Japan) was dissolved in physiological saline and administered systemically using an infusion syringe pump (KD Scientific, Holliston, MA, USA). The behavioral tests described below were performed to assess cross-tolerance to remifentanil in morphine-tolerant rats.
Behavioral Testing
Responses to nociceptive somatic and visceral stimuli were measured using the tail-flick (TF) and colorectal distension (CD) tests, respectively. All 12 rats were used for both behavioral tests. Both behavioral tests were performed before subcutaneous injection and 30, 60, and 90 min after subcutaneous injection for the morphine challenge test on days 1 and 10 (Experiment 1). On day 11 (Experiment 2), both behavioral tests were performed every 30 min for 120 min during remifentanil infusion and 30 min after infusion termination. Both tests were performed in a blinded manner. Figure 2 illustrates the time course of the experimental procedures.
 |
Figure 2 Timeline of the experimental procedures for Experiments 1 (A) and 2 (B). |
Tail-Flick Test
The TF test was used to measure the responses to nociceptive somatic stimuli, as described previously.15 Heat from a source (a 24 V and 100 W projector lamp) was applied to an area approximately 5 cm from the tip of the tail. TF latency was defined as the behavior of shaking off the tail as an escape behavior from heat. The TF unit (Ugo Basile, Comerio, Italy) was calibrated such that its reference value was approximately 4 s. A cutoff time of 10s was used to avoid tail damage. Three responses were averaged for each time point per rat. To analyze the antinociceptive effect, TF latency was converted to the percentage maximal possible effect (%MPE = [postdrug value − baseline value] / [cutoff value – baseline value] × 100) at each time point per rat.
Colorectal Distension Test
The CD test was used to measure the responses to a visceral nociceptive stimulus, as described previously.15 The CD test used an approximately 8 cm long in-house system comprising a stimulating balloon that dilates the intestinal tract and a sensing balloon that senses escape behavior. The internal pressure of both balloons was measured using in-line pressure transducers. This in-house system was inserted transanally under isoflurane anesthesia. The CD test was performed 20 min after awakening from isoflurane anesthesia. The pressure of the stimulating balloon dilating the intestine was increased from 0 mmHg/s to 2.5 mmHg/s in increments. The internal pressure of the stimulating balloon was measured as the response threshold to the visceral nociceptive stimulus when the internal pressure of the sensing balloon increased rapidly. A cutoff distension pressure of 60 mmHg was used to avoid colon damage. Three responses were averaged for each time point per rat, and the CD threshold was converted to %MPE.
Statistical Analysis
All data are presented as mean ± standard error of the mean. Two-way repeated measures analysis of variance was conducted to analyze the differences between days 1 and 10 for the time point and day comparisons in Experiment 1, and between groups for time point and group comparisons in Experiment 2. Non-sphericity was compensated by the Greenhouse–Geisser correction. Two-sided Dunnett’s post hoc test was used to compare the variables at each time point. All statistical analyses were performed using IBM SPSS statistics 27 (IBM Corp. Armonk, NY, USA), and the differences were considered statistically significant at P < 0.05.
Results
A total of 12 rats were used in Experiments 1 and 2. No rats were excluded from either experiment.
Morphine Challenge Test (Experiment 1)
Figure 3 illustrates the time course of somatic and visceral antinociception induced by morphine challenge tests on days 1 and 10.
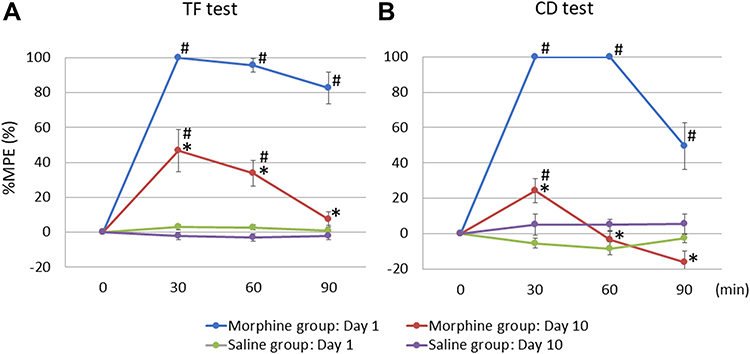 |
Figure 3 Results of the morphine challenge tests on days 1 and 10 (Experiment 1) in the tail-flick test (A) and colorectal distension test (B). Time course effects on percentage maximal possible effect (%MPE) after 5 mg/kg morphine or saline subcutaneous injection on days 1 and 10 are presented. The %MPE was significantly lower on day 10 than that on day 1 in both the tests in the morphine group, whereas the saline subcutaneous injection did not change in either test. Abbreviations: %MPE, percentage maximal possible effect; TF, tail-flick; CD, colorectal distension. Notes: Values are presented as the mean ± standard error of the mean (SEM) for the six rats in each group. The mean and SEM of the %MPE were examined for up to 90 min. Time 0 corresponds to immediately before the subcutaneous injection. *P < 0.05 compared with day 1, #P < 0.05 compared with baseline. |
Significant differences were found between days 1 and 10, and between time points [Fday (1, 5) = 141.053, P < 0.001, η2p = 0.966; Ftime (3, 15) = 70.481, P < 0.001, η2p = 0.934; Finteraction (3, 15) = 12.491, P < 0.001, η2p = 0.714 in the TF test (Figure 3A), and Fday (1, 5) = 607.815, P < 0.001, η2p = 0.992; Ftime (1.382, 6.911) = 50.913, P < 0.001, η2p = 0.911; Finteraction (3, 15) = 26.792, P < 0.001, η2p = 0.843 in the CD test (Figure 3B)] in the morphine group. Subcutaneous injection of morphine significantly increased %MPE compared with baseline at all time points in the TF and CD tests on day 1 (all P < 0.001). On day 10, morphine significantly increased %MPE at 30 and 60 min (P = 0.001 and 0.013) but not at 90 min (P = 0.816) in the TF test and at only 30 min (P = 0.007) but not at 60 and 90 min (P = 0.915 and 0.075) in the CD test compared with that at baseline. Compared with day 1, the %MPE on day 10 was significantly attenuated at every time point in both tests [F30 min (1, 5) = 19.350, P = 0.007, η2p = 0.795; F60 min (1, 5) = 50.671, P = 0.001, η2p = 0.910; F90 min (1, 5) = 54.521, P = 0.001, η2p = 0.916 in the TF test, and F30 min (1, 5) = 122.638, P < 0.001, η2p = 0.961; F60 min (1, 5) = 435.670, P < 0.001, η2p = 0.989; F90 min (1, 5) = 25.627, P = 0.004, η2p = 0.837 in the CD test].
No differences were found between days 1 and 10, or between time points [Fday (1, 5) = 2.876, P = 0.151, η2p = 0.365; Ftime (3, 15) = 0.137, P = 0.936, η2p = 0.027; Finteraction (3, 15) = 1.379, P = 0.287, η2p = 0.216 in the TF test, and Fday (1, 5) = 4.923, P = 0.077, η2p = 0.496; Ftime (3, 15) = 0.279, P = 0.840, η2p = 0.053; Finteraction (3, 15) = 2.075, P = 0.147, η2p = 0.293 in the CD test] in the saline group.
Cross-Tolerance from Morphine to Remifentanil (Experiment 2)
Figure 4 illustrates the time course of %MPE during remifentanil infusion.
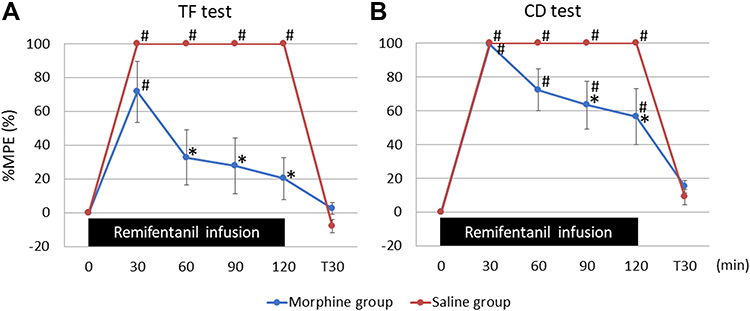 |
Figure 4 Results of the assessment for cross-tolerance from morphine to remifentanil on day 12 (Experiment 2) in the tail-flick test (A) and colorectal distension test (B). The %MPE was lower in the morphine group than that in the saline group in both tests. Abbreviations: %MPE, percentage maximal possible effect; TF, tail-flick; CD, colorectal distension. Notes: Values are presented as the mean ± standard error of the mean (SEM) for the six rats in each group. The mean and SEM of the %MPE were examined during a 10-mcg/kg/min remifentanil infusion and after a 30-min remifentanil infusion. Time 0 corresponds to immediately before remifentanil infusion. Time T30 corresponds to after a 30-min remifentanil infusion. *P < 0.05 compared with the saline group, #P < 0.05 compared with the baseline. |
In the TF test (Figure 4A), statistical differences were found both between the groups and between the time points [Fgroup (1, 10) = 15.564, P = 0.003, η2p = 0.609; Ftime (2.135, 21.354) = 63.351, P < 0.001, η2p = 0.864; Finteraction (5, 50) = 17.244, P < 0.001, η2p = 0.633]. In the morphine group, remifentanil significantly increased %MPE in the first 30 min (P < 0.001) compared with that at baseline but not at 60, 90, 120, and T30 min (P = 0.075, 0.158, 0.41, and 1, respectively), and the increase in %MPE was significantly attenuated compared with that in the saline group at 60, 90, and 120 min (P = 0.002, 0.001 and P < 0.001) but not at 30 and T30 min (P = 0.148 and 0.073).
In the CD test (Figure 4B), statistical differences were found between the groups and between the time points [Fgroup (1, 10) = 6.280, P = 0.031, η2p = 0.386; Ftime (1.964, 19.637) = 93.752, P < 0.001, η2p = 0.904; Finteraction (5, 50) = 5.937, P < 0.001, η2p = 0.373]. In the morphine group, remifentanil significantly increased %MPE throughout the duration of remifentanil infusion compared with that at baseline (all P < 0.001); %MPE returned to the baseline values at T30 min (P = 0.606).
The increase in %MPE was significantly attenuated in the morphine group compared with that in the saline group at 90 and 120 min (P = 0.026 and 0.025) but not at 30, 60, and T30 min (P = 0.341, 0.054, and 0.316).
In contrast, in the saline group, remifentanil significantly increased %MPE to the cutoff values throughout remifentanil infusion in both tests (all values were 100 ± 0%), and those were significantly increased compared with that at baseline (all P < 0.001). %MPE returned to the baseline values after 30 min from the termination of remifentanil in both tests (TF test: −8.1 ± 3.9%, P = 0.056; CD test: 9.0 ± 4.5%, P = 0.051).
Discussion
This study investigated the development of cross-tolerance to the antinociceptive effect of remifentanil in morphine-tolerant rats on somatic and visceral nociceptive stimulation and demonstrated two important phenomena. Morphine-tolerant rats exhibit cross-tolerance to acute antinociceptive effects of remifentanil on somatic and visceral stimuli. Cross-tolerance to the antinociceptive effect of remifentanil can be higher and faster on somatic stimulus than that on visceral stimulus.
Long-term opioid use, such as morphine, induces tolerance to their antinociceptive effects.16 Some clinical reports have indicated a cross-tolerance from morphine to remifentanil. The use of sustained-release morphine for 1 month induced cross-tolerance to remifentanil in a clinical setting.10 In experimental animal studies, intraperitoneal injection of remifentanil induced cross-tolerance to morphine in normal mice.17 However, to the best of our knowledge, no basic animal research has demonstrated that chronic administration of morphine induces cross-tolerance to remifentanil, especially with continuous intravenous remifentanil infusion. Furthermore, our results demonstrated that morphine-tolerant rats were also tolerant to the acute antinociceptive effects of remifentanil on somatic and visceral stimuli. Similar to a clinical study,9 which showed that the analgesic effect was reduced by continuous administration of remifentanil, the antinociceptive effect reduction by continuous remifentanil administration was accelerated in the morphine-tolerant rats in our study, suggesting that the antinociceptive effect of remifentanil intraoperatively would be mitigated in patients with long-term use of opioids for cancer pain or those suffering from opioid addiction. Multiple mechanisms have been reported for the development of tolerance to opioid analgesics that are complexly regulated and interact with each other.18 Opioid cross-tolerance is even more complex and remains poorly understood. Chronic administration of morphine desensitizes the μ-opioid receptor, as reported previously.3 Although our study did not examine the mechanism of cross-tolerance, our results suggest that chronic administration of morphine caused desensitization of the μ-opioid receptor, and in this state, the antinociceptive effect of remifentanil seemed to be attenuated. Elucidation of the neurobiological or neurophysiological mechanisms should be the next subject of research.
Further, cross-tolerance to the somatic stimulus can be higher and faster than that to the visceral stimulus. According to our morphine challenge test on day 10, both the TF and CD tests showed that the antinociceptive effect of morphine decreased significantly compared with that on day 1 by 30 min after subcutaneous injection. During the continuous infusion of remifentanil, %MPE in the TF test reduced the antinociceptive effect faster than that in the CD test. In addition, the CD test showed a significant antinociceptive effect until the end of remifentanil administration; however, the antinociceptive effect in the TF test waned after 90 min. These results suggest that morphine-tolerant rats had higher and faster cross-tolerance to remifentanil antinociceptive effects on somatic nociceptive stimulation than that on visceral stimulation. It was difficult to directly compare the results of two tests with different stimuli such as the TF and CD tests. Thus, we converted the measured values to %MPE so that relative comparisons could be made. Since %MPE varies depending on cutoff values, we set the cutoff value to a frequently used value. Our results are consistent with those of a clinical study reporting that morphine-treated patients developed tolerance to the antinociceptive effects of remifentanil using experimental somatic nociceptive stimuli.10 This study confirmed cross-tolerance to antinociceptive effect for somatic pain; however, it did not examine the cross-tolerance to antinociceptive effect for visceral pain. Although the mechanism is unclear, the fundamental differences in the peripheral mechanisms between visceral and somatic pain, including the density of afferent innervation, quantitative differences in the afferent nerve counts, size distribution of fibers present, and difference in afferent fiber projects,19 may contribute to the difference between the results of the TF and CD tests. A few reports have studied the difference between the somatic and visceral antinociceptive effects and tolerance to opioids.20 However, remifentanil has not been studied for its antinociceptive effect on visceral stimuli; therefore, the mechanism underlying the difference between somatic and visceral tolerances remains unclear.
Laparoscopic surgery has become increasingly popular recently. Laparoscopic surgeries cause fewer scars on the body surface but offer visceral stimuli, such as the extension of the peritoneum by pneumoperitoneum, as much as conventional open abdominal surgeries. Few clinical studies have examined opioid cross-tolerance to antinociceptive effect for visceral pain. Our results suggest that cross-tolerance from morphine to remifentanil occurs for somatic as well as visceral antinociceptive effects in patients taking morphine for a long time and that cross-tolerance to somatic antinociceptive effects can be more attenuated than to visceral antinociceptive effect. Anesthesiologists must consider the development of cross-tolerance to remifentanil antinociceptive effect, even during laparoscopic procedures for patients under long-term opioid therapy. Notably, when the somatic antinociceptive effect of remifentanil was reduced by cross-tolerance that occurs faster than that of visceral antinociceptive effect, anesthesiologists could cover somatic analgesia with nerve blocks or local anesthetic filtration.
We used an experimental method that is as similar to clinical practice as possible. For example, we used the CD test to assess visceral nociception and continuous intravenous remifentanil administration as performed in clinical practice. Although there are different methods for measuring the visceral antinociceptive effects, we used the CD test as visceral nociception during surgery, originating mainly from distension or dilation of the peritoneal and intestinal tracts.
Nevertheless, our study had some limitations. First, we used normal rats rather than pain model rats in this study. Painful inflammation accompanied by glial cell activation reportedly attenuated the development of opioid tolerance.21 Fewer stimuli are usually required to induce visceral pain sensations in pathological conditions.22 It would have been better to perform these experiments using a rat model of cancer pain and incisional pain since the results may have been different if these model rats were used in this study. Second, female rats were excluded from this study because of sexual cycle. However, it has been reported that the mean of some measurements may differ significantly between male and female rats depending on the test.23 In particular, animal studies with rodents have reported that opioid analgesia is more potent in males than in females.24 Nevertheless, the lack of female rats is a limitation of the present study; therefore, our results are only valid for male rats.
Conclusion
We indicated for the first time that morphine-tolerant rats have cross-tolerance to acute antinociceptive effects of remifentanil on somatic and visceral stimuli. Therefore, cross-tolerance to the antinociceptive effects of remifentanil for somatic and visceral pain should be considered in the perioperative management of patients using morphine preoperatively.
Abbreviations
%MPE, percentage maximal possible effect; TF, Tail-flick; CD, Colorectal distension; SEM, Standard error of the mean.
Acknowledgments
The authors wish to extend their gratitude to the staff of the animal facilities, Faculty of Medicine, Shimane University, for technical help and animal care.
Funding
This work was supported by Japan Society for the Promotion of Science KAKENHI Grant Number 16K10937.
Disclosure
Dr Hideaki Mori reports grants from Japan Society for the Promotion of Science, during the conduct of the study; personal fees from Nihon Kohden, outside the submitted work. Dr Tatsuya Hashimoto reports personal fees from Shionogi, Daiichi Sankyo, and Hisamitsu, outside the submitted work. Dr Yoji Saito reports lecture fees from Daiichi Sankyo, Shionogi, Phizer, Nipponzoki, Kyowa Kirin, Terumo, Mundipharma, and Nihon Kohden, outside the submitted work. The authors report no other conflicts of interest in this work.
References
1. Al-Hasani R, Bruchas MR. Molecular mechanisms of opioid receptor-dependent signaling and behavior. Anesthesiology. 2011;115(6):1363–1381. doi:10.1097/ALN.0b013e318238bba6
2. Nersesyan H, Slavin KV. Current approach to cancer pain management: availability and implications of different treatment options. Ther Clin Risk Manag. 2007;3(3):381–400.
3. Williams JT, Ingram SL, Henderson G, et al. Regulation of μ-opioid receptors: desensitization, phosphorylation, internalization, and tolerance. Pharmacol Rev. 2013;65(1):223–254. doi:10.1124/pr.112.005942
4. Davis JJ, Johnson KB, Egan TD, Vezina DP, Snell TE, Swenson JD. Preoperative fentanyl infusion with pharmacokinetic simulation for anesthetic and perioperative management of an opioid-tolerant patient. Anesth Analg. 2003;97(6):1661–1662. doi:10.1213/01.ANE.0000090151.13573.42
5. Athanasos P, Smith CS, White JM, Somogyi AA, Bochner F, Ling W. Methadone maintenance patients are cross-tolerant to the antinociceptive effects of very high plasma morphine concentrations. Pain. 2006;120(3):267–275. doi:10.1016/j.pain.2005.11.005
6. de Aquino JP, Parida S, Avila-Quintero VJ, et al. Opioid-induced analgesia among persons with opioid use disorder receiving methadone or buprenorphine: a systematic review of experimental pain studies. Drug Alcohol Depend. 2021;228:109097. doi:10.1016/j.drugalcdep.2021.109097
7. Gemma M, Tommasino C, Cozzi S, et al. Remifentanil provides hemodynamic stability and faster awakening time in transsphenoidal surgery. Anesth Analg. 2002;94(1):163–168. doi:10.1213/00000539-200201000-00031
8. Kim SH, Stoicea N, Soghomonyan S, Bergese SD. Remifentanil-acute opioid tolerance and opioid-induced hyperalgesia: a systematic review. Am J Ther. 2015;22(3):e62–e74. doi:10.1097/MJT.0000000000000019
9. Vinik HR, Kissin I. Rapid development of tolerance to analgesia during remifentanil infusion in humans. Anesth Analg. 1998;86(6):1307–1311. doi:10.1213/00000539-199806000-00033
10. Chu LF, D’Arcy N, Brady C, et al. Analgesic tolerance without demonstrable opioid-induced hyperalgesia: a double-blinded, randomized, placebo-controlled trial of sustained-release morphine for treatment of chronic nonradicular low-back pain. Pain. 2012;153(8):1583–1592. doi:10.1016/j.pain.2012.02.028
11. Cervero F. Visceral versus somatic pain: similarities and differences. Dig Dis. 2009;27(suppl 1):3–10. doi:10.1159/000268115
12. Ness TJ, Follett KA. The development of tolerance to intrathecal morphine in rat models of visceral and cutaneous pain. Neurosci Lett. 1998;248(1):33–36. doi:10.1016/S0304-3940(98)00327-9
13. Parkitna JR, Obara I, Wawrzczak-Bargiela A, Makuch W, Przewlocka B, Przewlocki R. Effects of glycogen synthase kinase 3beta and cyclin-dependent kinase 5 inhibitors on morphine-induced analgesia and tolerance in rats. J Pharmacol Exp Ther. 2006;319(2):832–839. doi:10.1124/jpet.106.107581
14. Ishida R, Nikai T, Hashimoto T, Tsumori T, Saito Y. Intravenous infusion of remifentanil induces transient withdrawal hyperalgesia depending on administration duration in rats. Anesth Analg. 2012;114(1):224–229. doi:10.1213/ANE.0b013e318237f678
15. Miyamoto H, Saito Y, Kirihara Y, Hara K, Sakura S, Kosaka Y. Spinal coadministration of ketamine reduces the development of tolerance to visceral as well as somatic antinociception during spinal morphine infusion. Anesth Analg. 2000;90(1):136–141. doi:10.1097/00000539-200001000-00030
16. Kissin I, Brown PT, Robinson CA, Bradley EL. Acute tolerance in morphine analgesia: continuous infusion and single injection in rats. Anesthesiology. 1991;74(1):166–171. doi:10.1097/00000542-199101000-00025
17. Nowoczyn M, Marie N, Coulbault L, et al. Remifentanil produces cross-desensitization and tolerance with morphine on the mu-opioid receptor. Neuropharmacology. 2013;73:368–379. doi:10.1016/j.neuropharm.2013.06.010
18. Mercadante S, Arcuri E, Santoni A. Opioid-induced tolerance and hyperalgesia. CNS Drugs. 2019;33(10):943–955. doi:10.1007/s40263-019-00660-0
19. McMahon SB. Are there fundamental differences in the peripheral mechanisms of visceral and somatic pain? Behav Brain Sci. 1997;20(3):381–391. doi:10.1017/S0140525X97231481
20. Saito Y, Kaneko M, Kirihara Y, Sakura S, Kosaka Y. Interaction of intrathecally infused morphine and lidocaine in rats (part II): effects on the development of tolerance to morphine. Anesthesiology. 1998;89(6):1464–1470. doi:10.1097/00000542-199812000-00024
21. Eidson LN, Murphy AZ. Persistent peripheral inflammation attenuates morphine-induced periaqueductal gray glial cell activation and analgesic tolerance in the male rat. J Pain. 2013;14(4):393–404. doi:10.1016/j.jpain.2012.12.010
22. Coutinho SV, Meller ST, Gebhart GF. Intracolonic zymosan produces visceral hyperalgesia in the rat that is mediated by spinal NMDA and non-NMDA receptors. Brain Res. 1996;736(1–2):7–15. doi:10.1016/0006-8993(96)00661-0
23. Becker JB, Prendergast BJ, Liang JW. Female rats are not more variable than male rats: a meta-analysis of neuroscience studies. Biol Sex Differ. 2016;7:34. doi:10.1186/s13293-016-0087-5
24. Romanescu M, Buda V, Lombrea A, et al. Sex-related differences in pharmacological response to CNS drugs: a narrative review. J Pers Med. 2022;12(6):907. doi:10.3390/jpm12060907
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.