")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Long-Term Effects of Anxiety on the Metabolic Control of Recently Diagnosed Type 2 Diabetes Patients: Results from the CAIPaDi Cohort Study
Authors Rodríguez-Ramírez AM , Alcántara-Garcés MT , Hernández-Jiménez S , García-Ulloa AC , Arcila-Martínez D, Velázquez-Jurado H , Arizmendi-Rodríguez RE
Received 8 October 2022
Accepted for publication 6 January 2023
Published 23 January 2023 Volume 2023:19 Pages 197—207
DOI https://doi.org/10.2147/NDT.S392672
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Video abstract presented by Alejandra Monserrat Rodríguez-Ramírez.
Views: 161
Alejandra Monserrat Rodríguez-Ramírez, María Teresa Alcántara-Garcés, Sergio Hernández-Jiménez, Ana Cristina García-Ulloa, Denise Arcila-Martínez, Héctor Velázquez-Jurado, Rodrigo Eduardo Arizmendi-Rodríguez On behalf of the study group CAIPaDi
Centro de Atención Integral del Paciente con Diabetes (CAIPaDi) Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Mexico City, Mexico
Correspondence: María Teresa Alcántara-Garcés, Centro de Atención Integral del Paciente con Diabetes (CAIPaDi) Instituto Nacional de Ciencias Médicas y Nutrición Salvador Zubirán, Vasco de Quiroga No. 15, Colonia Sección XVI Tlalpan, Mexico City, 14080, Mexico, Tel +1 52 55 54870900 (5045), Email [email protected]
Introduction: Anxiety disorders (AXD) are among the most prevalent mental health conditions in patients with type 2 diabetes (T2D). Previous data have established an association of other psychiatric conditions with poor metabolic control and increased odds of diabetes-related complications. Nonetheless, follow-up information about the effects of AXD on the metabolic control of patients with TD2 is still limited.
Objective: Evaluate the effects of AXD on the metabolic parameters of patients with T2D over 12 months of follow-up in a multidisciplinary comprehensive care model.
Methods: Prospective study of T2D subjects enrolled in a comprehensive care program with follow-up at 3 and 12 months of treatment. Patients were assessed using the Mini-International Neuropsychiatric Interview and the Hospital Anxiety and Depression Scale (HADS). We registered clinical and metabolic characteristics from each visit. Metabolic parameters over time were analyzed with a mixed model of repeated measures using AXD and time as interaction variables.
Results: Our sample included 2703 patients at baseline, and 1161 (43%) subjects continued the follow-up at 12 months. The AXD group had more females, lower age, and fewer years of formal education compared with subjects without AXD at baseline, 3 and 12 months. Patients with AXD also reported higher mean fasting glucose at three months, and higher HbA1c at three and 12 months. Our MMRM for HbA1c reported significant differences over time in subjects with and without AXD. The differences in means between groups increased from 0.17% at three months to 0.31% at 12 months. The variables from the HADS anxiety score, sex, age, years of diagnosis, and insulin treatment were also associated with HbA1c parameters over time.
Conclusion: Patients with AXD had the worst glycemic control at 3 and 12 months of follow-up. HbA1c differences in patients with AXD compared with non-AXD subjects increases over time in association with anxiety symptoms.
Keywords: diabetes care, psychiatric comorbidity, anxiety, glycemic control
Introduction
Type 2 diabetes (T2D) is a worldwide public health problem.1 The International Diabetes Federation estimated that one in every ten adults has T2D (prevalence of 10.5%).2 The global deaths associated with this condition account for 12.2% of the population between 20–79 years.3 Since these patients’ leading causes of death are T2D-related complications, the current focus of treatment is the prevention of those through the enhancement of metabolic control and the management of conditions that may interfere with its achievement.4,5 Psychiatric comorbidities such as anxiety disorders (AXD) are modifiable risk factors related to poor metabolic control,6,7 increased risk of complications,8,9 and mortality in T2D.10 AXD are among the most common mental health affections in these patients, with a prevalence of 19% to 55% depending on the measurement tool.11,12 It has been stated that subjects with this endocrinologic disease have increased odds of presenting AXD compared with controls.13 Different studies have found that anxiety symptoms are as frequent as depression or even more prevalent in T2D.12,14–16 Nonetheless, most of the mental health research in this field has centered on depression, and our knowledge about the AXD effects on metabolic control is still limited.
Previous research on the characteristics of subjects with diabetes and AXD had reported inconsistent results. Some studies showed an association of hyperglycemia with anxiety, whereas others found no connection between those variables. A meta-analysis including patients with type 1 and type 2 diabetes analyzed twelve studies and found no association between anxiety and glycemia in the general data.11 Nonetheless, a sub-analysis of the three studies that used structured diagnostic interviews reported an association of AXD with hyperglycemia (p= 0.003, ES=0.25 [95% CI 0.10 to 0.38]) in the same meta-analysis.11 Other papers identified higher levels of serum high-sensitivity C-protein and a positive association in female sex,17 increased odds of having high blood glucose,16 higher body mass index (BMI), and higher waist circumference18 in T2D subjects with anxiety. It is essential to point out that most of these studies presented a cross-sectional evaluation, which might be an incomplete approach to assessing long-lasting conditions.
Identifying the long-term effects of AXD on the metabolic parameters of subjects with T2D is crucial for the understanding of this comorbidity; and the advance in the development of integrative interventions that improve metabolic control in diabetes care. While anxiety disorders (AXD) are frequent in T2D,12,13 their impact on the metabolic control of recently diagnosed patients is not fully elucidated, and long-term evaluations are needed. In this study, we aim to evaluate the effects of anxiety on the metabolic parameters of recently diagnosed T2D patients over 12 months of follow-up in a multidisciplinary model of comprehensive care.19,20
Materials and Methods
We conducted a prospective study with 12 months of follow-up of patients from a multidisciplinary comprehensive care model, the Center of Comprehensive Care for the Patient with Diabetes (CAIPaDi, an acronym for its name in Spanish).19,20 Three evaluations were made: baseline (enrollment to the center), 3 and 12 months of treatment.
Study Population
Our study included Mexican patients over 18 years old with less than five years of T2D diagnosis, Body Mass Index (BMI) ≤ 45 kg/m2, without disabling complications, non-smokers, or patients with substance use disorder, without a psychotic psychiatric disorder. This study was approved by the Institutional Ethics and Research Committees from the National Institute of Medical Sciences and Nutrition Salvador Zubirán (Ref 1198) and is registered on ClinicalTrials.gov (NCT02836808). We obtained written consent from all subjects who participated in the study, and the research was conducted according to the Declaration of Helsinki standards. All participants were informed about the purpose of the study. Clinical deidentified participant data is available to share throughout the study; email requests must be sent to the corresponding author María Teresa Alcántara-Garcés for consideration. No other documents will be shared.
Procedure
We enrolled patients with type 2 diabetes whose diagnosis was confirmed by blood test according to ADA diagnostic criteria (hemoglobin A1c ≥ 6.5% or fasting plasma glucose ≥ 126mg/dL or random plasma glucose ≥ 200mg/dL).21
Patients were evaluated at each visit by all the interdisciplinary team members as previously described.19,20 An endocrinologist provided all pharmacologic interventions for metabolic control according to the ADA guidelines.22 At baseline, we conducted a psychiatric clinical interview, including the application of the Mini International Neuropsychiatric Interview (M.I.N.I.) and the Hospital Anxiety and Depression Scale (HADS) subscale anxiety. On the first interview, patients diagnosed with psychiatric disorders (including AXD) were offered psychopharmacological treatment.23 Follow-up included a psychiatric evaluation and using HADS to assess symptoms severity at 3 and 12 months. Consultation-liaison psychiatrists provided all psychiatric evaluations and psychopharmacological treatments.
The M.I.N.I. 5.0.0 Spanish version,24,25 is a short diagnostic structured interview to identify 16 psychiatric disorders according to the Diagnostic and Statistical Manual IV-TR edition (DSM-IV-TR) classification; the presence of anxiety disorders, including panic disorder, agoraphobia, social phobia, obsessive-compulsive disorder, post-traumatic stress disorder, and generalized anxiety disorder. The HADS comprises fourteen items and assesses psychologic and somatic symptoms related to anxiety and depression.26 The accuracy and diagnostic usefulness of the Mexican version set a cut-off point for anxiety ≥8 and (α-Cronbach 0.89, Kappa 0.68) set a cut-off point for depression ≥7 (α-Cronbach 0.72, Kappa 0.73).27 Groups were assigned at the first evaluation (baseline) in agreement with the presence or absence of AXD. We registered metabolic parameters, body measurements, and treatments in all visits.
Blood samples were taken during each visit for fasting glucose, creatinine, lipid profile (using colorimetric methods, SYNCHRON CX System), and HbA1c (using HPLC method, Bio-Rad Variant II Turbo HbA1c Kit 2). Body composition was assessed by bioimpedance (body composition analyzer JAWON medical ioi353).
Statistical Analysis
For the statistical analysis, we employed the software STATA 13.0 (StataCorp. 2013. Stata Statistical Software: Release 13. College Station, TX: StataCorp LP). Normal distribution was assessed with the Kolmogorov-Smirnov test. We present our data with means and standard deviation or median with interquartile range according to distribution. Categorical variables are reported in frequency and percentage. A comparative analysis was conducted between groups with and without AXD at each visit (baseline, 3 and 12 months). Continuous variables were compared with Student’s t-test or Mann–Whitney U-test according to the distribution. The comparison between categorical variables was assessed using the χ2 test. We performed an adjusted analysis with linear regressions using sex, age, AXD, and psychopharmacological treatment as independent variables of each metabolic variable that reported significant differences at each time frame.
We constructed a mixed model of repeated measures of the metabolic parameters using AXD and time as interaction variables. HADS anxiety score, age, sex, endocrinologic (class and number of medications), and psychopharmacologic treatment were used as covariates.
Results
Our sample at baseline included 2703 participants, 1508 females, with a mean age of 54.50 ± 10.26 years, 12.77 ± 3.97 years of formal education, and a median of 0 years (1–3) since TD2 diagnosis. At three months of follow-up, 68.4% of subjects remained in the study, and 43% completed one year in the Center. During the study, the proportion of patients with AXD who continued in the program remained stable, as shown in Figure 1. The analysis of the effectiveness of the comprehensive care model, including medications and lifestyle changes, is available for consultation in a previous publication.19,20
 |
Figure 1 Flowchart of patient’s follow-up. Abbreviations: T2D, type 2 diabetes; HbA1c, glycated hemoglobin; AXD, anxiety disorder; Note: *Cause of follow-up losses. |
We performed a comparative analysis on each of the three evaluation moments depicted in Table 1. Three variables presented significant differences in the three-time sets with a similar pattern. The AXD group reported a higher proportion of female subjects, younger age, and fewer years of formal education than those without AXD at baseline, 3, and 12 months. At baseline, patients with AXD had higher total cholesterol, higher HDL-cholesterol, and lower weight than those without AXD. The adjusted analysis by age, sex, and psychopharmacological treatment at baseline reported no association of AXD with total cholesterol (p=0.227), HDL-cholesterol (p=0.125), and weight (p=0.068). In agreement with a psychiatric diagnosis, HADS anxiety scores in the AXD group were higher than in the non-AXD. Antidepressants were prescribed to more than 60% of patients with anxiety disorders at the first visit.
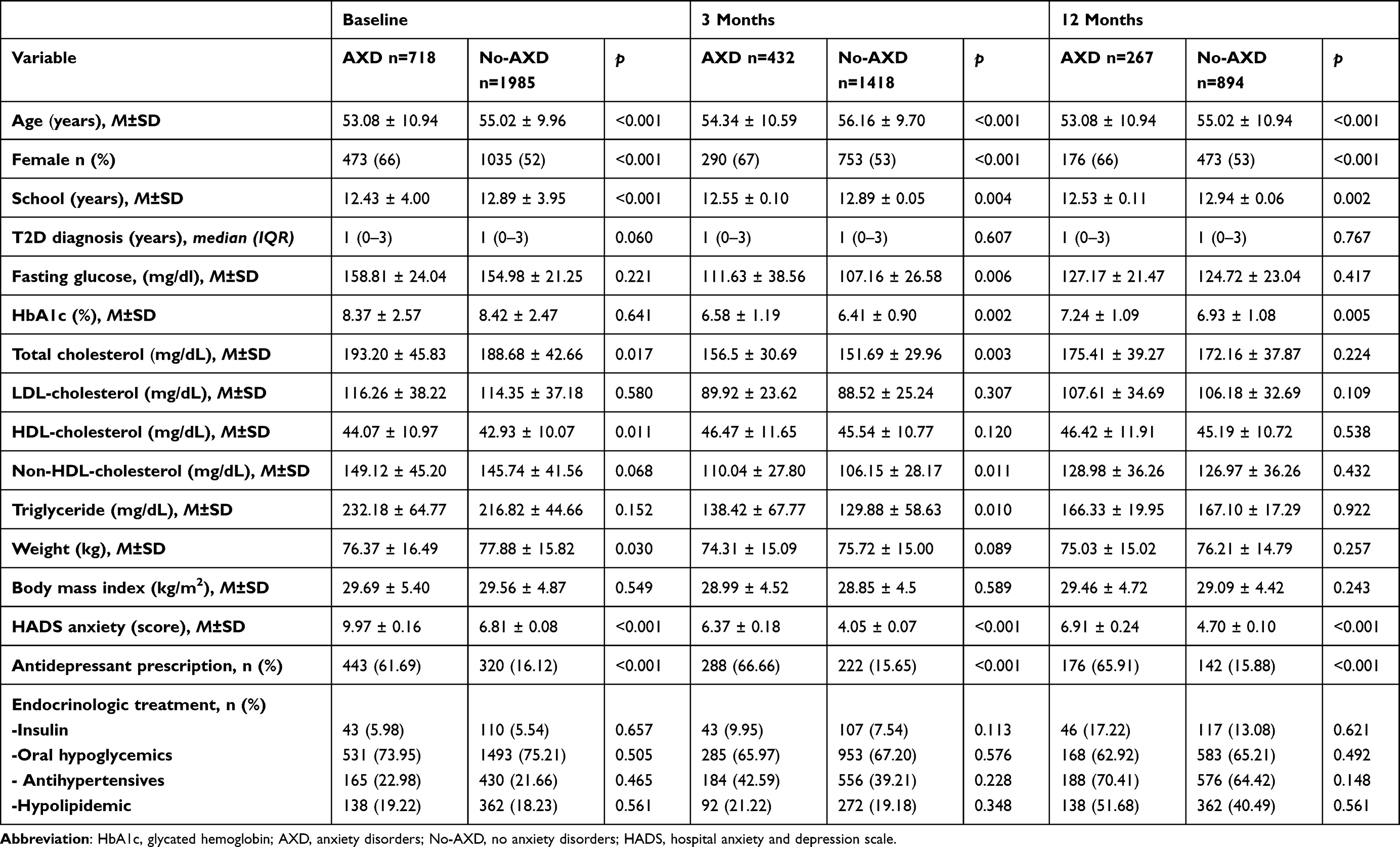 |
Table 1 Comparative Analysis of Clinical and Metabolic Parameters Between AXD and No-AXD Patients at Baseline, 3 and 12 Months |
At three months of follow-up, our group with AXD reported higher fasting glucose, HbA1c, total cholesterol, non-HDL cholesterol, and triglycerides. Over 66% of patients with anxiety disorders had antidepressant treatment. In the adjusted analysis by sex, age, and antidepressants, the association of AXD with fasting glucose (p=0.030) and HbA1c (p=0.017) remained significant. At the same time, the models for total cholesterol (p=0.495), non-HDL cholesterol (p=0.535), and triglycerides (p=0.113) reported no significant association with AXD. Psychopharmacologic treatment was associated with total cholesterol (p=0.012) and non-HDL cholesterol (p=0.014) at three months follow-up.
In the 12-month visit, we identified higher mean HbA1c in the AXD group, which remained significant in the corrected analysis (p=0.019). HADS anxiety scores remained higher in the AXD group at 3 and 12 months of follow-up compared with the non-AXD group. There were no differences in other metabolic parameters and endocrinologic treatments.
We analyzed changes over time in the metabolic parameters of patients with and without AXD through an MMRM using HADS anxiety score, sex, age, years of diagnosis, insulin, antidepressants, hypoglycemic (number and class), hypolipidemic, and antihypertensive treatment as covariates. Our MMRM for HbA1c (p<0.001) reported significant differences over time in subjects with and without AXD (Coef. =−0.19, 95% CI −0.38 to −0.01, p=0.035), as depicted in Figure 2 and Table 2. The differences in means between groups increased from 0.17% at three months to 0.31% at 12 months. The variables HADS anxiety score (Coef. =0.03, 95% CI 0.01 to 0.04, p<0.001), sex (Coef.=−0.26, 95% CI −0.39 to −0.13, p<0.001), age (Coef.=−0.03, 95% CI −0.03 to −0.02, p<0.001), years of diagnosis (Coef.=0.22, 95% CI 0.18 to 0.26, p<0.001), and insulin treatment (Coef.=0.20, 95% CI 0.01 to 0.04, p<0.001), were also associated with HbA1c parameters. Antidepressants (p=0.985), hypoglycemic (p=0.941), hypolipidemic (p=0.297), and antihypertensive (p=0.110) drugs were not associated with HbA1c changes in this model. Time was also associated with HbA1c levels at 3 (Coef. =−1.91, 95% CI −2.03 to −1.80, p<0.001) and 12 months (Coef. =−1.34, 95% CI −1.47 to −1.21, p<0.001). There was also a significative interaction between time and AXD at 3 (Coef. =0.24, 95% CI 0.03 to 0.46, p=0.025) and 12 months (Coef. =0.48, 95% CI 0.22 to 0.74, p<0.001).
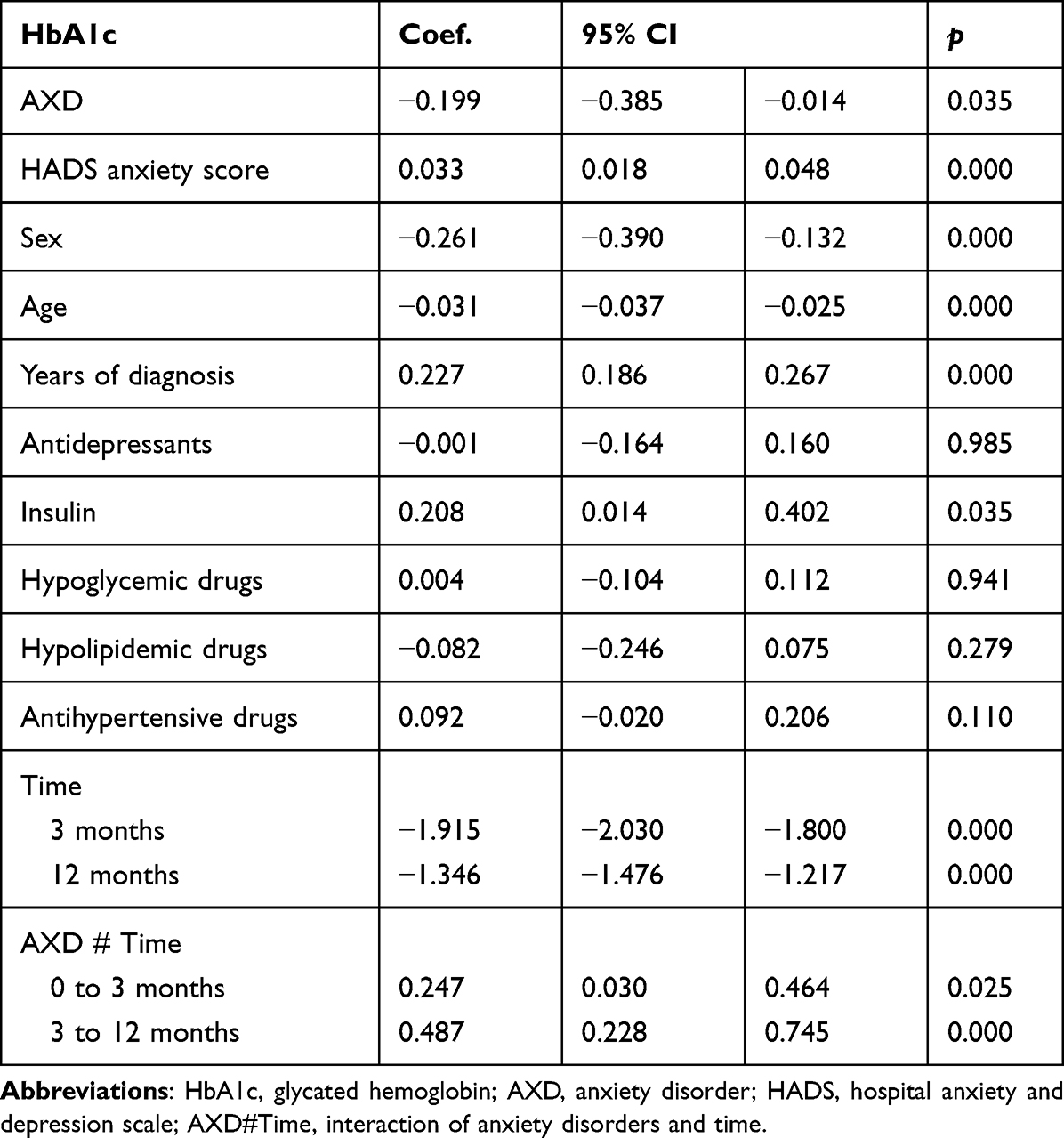 |
Table 2 Results of the Mixed Model of Repeated Measures for HbA1c |
 |
Figure 2 HbA1c levels of patients with and without anxiety disorders through 12 months of follow-up. Abbreviation: HbA1c, glycated hemoglobin. Note: *p<0.05; ***p<0.001. |
The models for fasting glucose (p=0.653), total cholesterol (p=0.354), LDL-cholesterol (p=0.450), HDL-cholesterol (p=0.667), triglycerides (p=0.176), and BMI (p=0.236) reported no association of AXD with the changes in metabolic parameters over time.
Discussion
This longitudinal study analyzed the long-term effects of AXD on the metabolic parameters of patients with less than five years of T2D over 3 and 12 months of follow-up. As the main results, we identified differences in the metabolic profile of patients with AXD compared with no AXD subjects in the three evaluations. We also found an association between HbA1c levels and AXD with a distinctive pattern of changes through time. To the best of our knowledge, this is the first longitudinal analysis to report an association of AXD with HbA1c in T2D Latin-American patients with a recent diagnosis.
Previous studies reported heterogeneous results about the influence of anxiety on metabolic parameters.11 The differences in the measurement tools of anxiety and methodological design might be implicated in the heterogeneity of findings about AXD among T2D patients. For instance, the prevalence of anxiety ranges from 19.7% to 57.9%16,28 using symptom scales, whereas a recent study reported a prevalence of AXD of 21.3% using a psychiatric diagnostic structured interview.29 In our sample, at baseline, 26.5% had some AXD; at three months following, 23.3% had some AXD, and at 12 months following, 23% had some AXD. The high frequency of AXD in this population highlights the clinical relevance of anxiety in diabetes care. The relationship between these conditions had been linked with genetic factors, adverse early environment, and unhealthy lifestyles.30 Also, brain metabolism dysregulation, central insulin signalization, inflammation, and oxidative stress are among the postulated pathways to explain the interrelation between AXD and T2D.31
Three characteristics were constantly associated with AXD during the evaluations of our study: female sex, younger age, and fewer years of formal education. Sex differences in anxiety disorders are well-established, with females being at higher risk than males. Those differences have been linked with genetic factors, brain structure, sex hormones, and their effects on disparities in adiposity and metabolic inflammation, adverse childhood events, stress adaptation, and gender stereotype.32,33 Patients with T2D are not an exception; a Norwegian study reported a higher prevalence of anxiety in female subjects with T2D compared with males.16 Younger age was also associated with AXD in all time frames of our study. A previous publication of our group already reported an association of younger age with psychiatric disorders and worst metabolic parameters in patients with a recent diagnosis of T2D.29 There are different potential explanations for these findings related to our sample. Since our study included patients with less than five years of T2D diagnosis, younger subjects might represent a population with early onset diabetes, which has been associated with an increased risk of complications, higher inflammatory biomarkers, and worse insulin resistance.34,35 Previous studies had associated insulin resistance with alterations in the function of neuronal and glial cells in the central nervous system (CNS), which might explain cognitive and behavioral alterations compatible with AXD.36–40 The third factor constantly associated with AXD was education; we observed lower mean years of formal education in subjects with AXD at baseline, 3, and 12 months. There is extensive evidence about this phenomenon in non-T2D subjects,41 and fewer years of formal education had already been linked with anxiety in T2D patients as a response to stress, coping abilities, indices of adjustment, and personality traits.12,14 Nonetheless, replicating these findings in our study highlights the importance of evaluating anxiety, particularly in patients with any of the three characteristics we previously discussed.
Basal metabolic parameters were not substantially different between groups, our results initially showed higher levels of total cholesterol, non-HDL cholesterol, and HDL cholesterol and lower weight in the AXD group; however, the differences did not remain significant after the adjusted analysis. These basal results can be better explained by age and sex variables, which had been previously reported involved in metabolic parameters among T2D.42
At three months, higher levels of fasting glucose, HbA1c, total cholesterol, non-HDL cholesterol, and triglycerides were reported in the AXD group. However, only two variables remained significant after the adjusted analysis: fasting glucose and HbA1c. Previous cross-sectional studies also reported higher fasting glucose28 and HbA1c11 in T2D patients with anxiety. It is noteworthy that antidepressants were associated with total cholesterol and non-HDL cholesterol at this time, but fasting glucose and HbA1c were not. These findings align with previous research reporting alterations in lipid homeostasis in association with antidepressant use43 and, on the other hand, the extensive evidence of glycemic control improvement after the start of antidepressant therapy.44,45
At 12 months, we found higher levels of HbA1c in AXD patients that remained significant after the adjusted analysis. Similar results were reported in Denmark’s population with TD2 in a study conducted by Kristensen et al (2021), where patients with new TD2 and preexisting anxiety were analyzed and found higher means in HbA1c in the anxiety group compared with individuals without mental disorders in baseline and 12 months of follow-up.46
Nonetheless, the main results of our study are centered on the evolution of HbA1c levels through time. According to our analysis, AXD and non-AXD patients started at similar HbA1c levels. However, over time we found increasing differences in measures between groups to end up with a mean HbA1c 0.31% higher in AXD at 12 months. Our MMRM also reported an association of HADS anxiety score with the increase in HbA1c levels over time, which implies a negative effect of anxiety symptoms severity on the glycemic control of patients. Even when the mean HADS anxiety score of both of our groups is below the threshold of a probable anxiety disorder at 3 and 12 months, which expresses a remission of AXD after treatment, the presence of subsyndromal anxiety symptoms in our sample is evident since HADS anxiety score of AXD patients is higher than the non-AXD group in all the time sets. Hence, residual anxiety symptoms might interfere with glucose control.
Different factors might be implicated in the accumulative increase of glucose levels of patients with AXD. The presence of AXD has been previously related to unhealthy behaviors and diminished self-care that complicate glycemic control;7,47 nonetheless, there are other critical neurobiological aspects to discuss. Glucose homeostasis is a complex and essential function where the central nervous system is highly implicated; one of the main regions invested in this process is the hypothalamus.48 Glucose metabolism and insulin actions are mediated through the hypothalamic activation of several neuroendocrine processes, such as insulin release and the regulation of food intake.49 There is extensive evidence about the involvement of hypothalamic structures in AXD neurobiology.50,51 The hypothalamus plays a crucial role in two main theories about anxiety’s neurophysiological pathways: hypothalamus-pituitary-adrenal (HPA) axis activation and limbic hyperactivation.51 Considering the hypothalamic role in glucose homeostasis, an anxiety-related alteration on the function of this structure might modify glucose metabolism and potentially explain our findings. Also, HPA axis activation in AXD modifies the function of different neurotransmitters and hormones that alter glucose metabolisms such as corticotropin-releasing hormone (CRH), adrenocorticotropic hormone (ACTH), cortisol, glutamate, and g-amino-butyric-acid (GABA).51,52 Hence, AXD-related HPA axis activation might affect glucose control in patients with T2D.
Nonetheless, all of these are hypotheses that the design of our study does not allow us to probe. So far, we can only ascertain an increase over time in the differences in HbA1c in patients with AXD compared with non-AXD subjects independent of psychopharmacological treatment and symptom remission; but closely associated with anxiety subsyndromal symptoms.
We must acknowledge some limitations in our study, such as the loss of patients during follow-up, and the higher proportion of female subjects. Nonetheless, we have some crucial strengths like sample size, detailed follow-up, selection criteria that limited potential confounding factors (smoking), and the use of standardized clinimetric instruments.
Conclusion
This study monitored AXD and non-AXD T2D patients with a recent diagnosis and analyzed the metabolic parameters of the groups through 12 months of follow-up. Our most important findings are the differences in glycemic control between groups with higher measures of HbA1c in AXD patients at 3 and 12 months, and the increase over time in the differences between groups in association with anxiety symptoms severity. In line with our findings, we are compelled to highlight the importance of the detection and close follow-up of AXD patients with T2D, acknowledging the presence of subsyndromal anxiety symptoms as a potential source of glucose metabolism alteration.
Acknowledgments
Study Group CAIPaDi
Michelle Díaz-Pineda, Humberto Del Valle-Ramírez, Arturo Flores García, Fernanda Garnica-Carrillo, Eduardo González-Flores, Mariana Granados-Arcos, Arely Hernández-Jasso, Diana Hernández-Juárez, Héctor Infanzón-Talango, Victoria Landa-Anell, Claudia Lechuga-Fonseca, Marco Antonio Melgarejo-Hernández, Angélica Palacios-Vargas, Liliana Pérez-Peralta, Sofía Ríos-Villavicencio, David Rivera de la Parra, Francis Rojas-Torres, Sandra Sainos-Muñoz, María Luisa Velasco-Pérez, Andrea Villegas-Narvaez, Luz Elena Urbina-Arronte, Verónica Zurita-Cortés, Carlos A. Aguilar-Salinas, Francisco J Gómez-Pérez, David Kershenobich-Stalnikowitz.
Others
Oswaldo Briseño-González, Eder Patiño-Rivera, Victor Trejo-Terreros.
Funding
The CAIPaDi program has received grants from Astra Zeneca, Fundación Conde de Valenciana, Novartis, Consejo Nacional de Ciencia y Tecnología (Proyectos de Desarrollo Científico para Atender Problemas Nacionales 2013 project 214718), Nutrición Médica y Tecnología, NovoNordisk, Boehringer Ingelheim, Dirección General de Calidad y Educación en Salud, Eli Lilly, Merck Serono, MSD, Silanes, Chinoin, and Carlos Slim Health Institute.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Khan MAB, Hashim MJ, King JK, Govender RD, Mustafa H, Kaabi J. Epidemiology of Type 2 diabetes - Global burden of disease and forecasted trends. J Epidemiol Glob Health. 2020;10(1):107–111. doi:10.2991/JEGH.K.191028.001
2. International Diabetes Federation. IDF diabetes atlas; 2021. Available from: www.diabetesatlas.org.
3. Sun H, Saeedi P, Karuranga S, et al. IDF Diabetes Atlas: global, regional and country-level diabetes prevalence estimates for 2021 and projections for 2045. Diabetes Res Clin Pract. 2021;183:109119. doi:10.1016/j.diabres.2021.109119
4. Laiteerapong N, Ham SA, Gao Y, et al. The legacy effect in type 2 diabetes: impactofearlyglycemiccontrol on future complications (the Diabetes & Aging study). Diabetes Care. 2019;42(3):416–426. doi:10.2337/dc17-1144
5. American Diabetes Association. Facilitating behavior change and well-being to improve health outcomes: standards of medical care in diabetes−2021. Diabetes Care. 2021;44:S53–S72. doi:10.2337/dc21-S005
6. Lerman I, Lozano L, Villa AR, et al. Psychosocial factors associated with poor diabetes self-care management in a specialized Center in Mexico City. Biomed Pharmacother. 2004;58(10):566–570. doi:10.1016/j.biopha.2004.09.003
7. Whitworth SR, Bruce DG, Starkstein SE, Davis WA, Davis TME, Bucks RS. Lifetime depression and anxiety increase prevalent psychological symptoms and worsen glycemic control in type 2 diabetes: the Fremantle Diabetes Study Phase II. Diabetes Res Clin Pract. 2016;122:190–197. doi:10.1016/j.diabres.2016.10.023
8. Whitworth SR, Bruce DG, Starkstein SE, et al. Depression symptoms are persistent in Type 2 diabetes: risk factors and outcomes of 5-year depression trajectories using latent class growth analysis. Diabetic Med. 2017;34(8):1108–1115. doi:10.1111/dme.13372
9. Lloyd CE, Nouwen A, Sartorius N, et al. Prevalence and correlates of depressive disorders in people with Type 2 diabetes: results from the International Prevalence and Treatment of Diabetes and Depression (INTERPRET-DD) study, a collaborative study carried out in 14 countries. Diabetic Med. 2018;35(6):760–769. doi:10.1111/DME.13611
10. Naicker K, Johnson JA, Skogen JC, et al. Type 2 diabetes and comorbid symptoms of depression and anxiety: longitudinal associations with mortality risk. Diabetes Care. 2017;40(3):352–358. doi:10.2337/dc16-2018
11. Anderson RJ, Mary Groot B, Grigsby AB, et al. Anxiety and poor glycemic control: a meta-analytic review of the literature. Int J Psychiatry Med. 2002;32(3):235–247. doi:10.2190/KLGD-4H8D-4RYL-TWQ8
12. Grigsby AB, Anderson RJ, Freedland KE, Clouse RE, Lustman PJ. Prevalence of anxiety in adults with diabetes A systematic review. J Psychosom Res. 2002;53:1053–1060. doi:10.1016/S0022-3999(02)00417-8
13. Huang CJ, Chiu HC, Lee MH, Wang SY. Prevalence and incidence of anxiety disorders in diabetic patients: a national population-based cohort study. Gen Hosp Psychiatry. 2011;33(1):8–15. doi:10.1016/j.genhosppsych.2010.10.008
14. Smith KJ, Béland M, Clyde M, et al. Association of diabetes with anxiety: a systematic review and meta-analysis. J Psychosom Res. 2013;74(2):89–99. doi:10.1016/j.jpsychores.2012.11.013
15. Chaturvedi SK, Manche Gowda S, Ahmed HU, et al. More anxious than depressed: prevalence and correlates in a 15-nation study of anxiety disorders in people with type 2 diabetes mellitus. Gen Psychiatr. 2019;32:4. doi:10.1136/gpsych-2019-100076
16. Naicker K, Øverland S, Johnson JA, et al. Symptoms of anxiety and depression in type 2 diabetes: associations with clinical diabetes measures and self-management outcomes in the Norwegian HUNT study. Psychoneuroendocrinology. 2017;84:116–123. doi:10.1016/j.psyneuen.2017.07.002
17. Yang QQ, Shao D, Li J, Yang CL, Fan MH, Cao FL. Positive association between serum levels of high-sensitivity C-reactive protein and depression/anxiety in female, but not male, patients with type 2 diabetes mellitus. Biol Res Nurs. 2020;22(2):178–187. doi:10.1177/1099800419894641
18. Kendzor DE, Chen M, Reininger BM, et al. The association of depression and anxiety with glycemic control among Mexican Americans with diabetes living near the U.S.-Mexico border. BMC Public Health. 2014;14(1). doi:10.1186/1471-2458-14-176
19. Hernandez-Jimenez S, Garcia-Ulloa C, Mehta R, Aguilar-Salinas C, Kershenobich-Stalnikowitz D. Innovative models for the empowerment of patients with type 2 diabetes: the CAIPaDi program. Recent Pat Endocr Metab Immune Drug Discov. 2014;8(3):202–209. doi:10.2174/1872214808999141110155515
20. Hernández-Jiménez S, García-Ulloa AC, Bello-Chavolla OY, Aguilar-Salinas CA, Kershenobich-Stalnikowitz D. Long-term effectiveness of a type 2 diabetes comprehensive care program. The CAIPaDi model. Diabetes Res Clin Pract. 2019;151:128–137. doi:10.1016/j.diabres.2019.04.009
21. Cefalu WT, Berg EG, Saraco M, et al. Classification and diagnosis of diabetes: standards of medical care in diabetes-2021. Diabetes Care. 2021;44:S15–S33. doi:10.2337/dc21-S002
22. American Diabetes Association. Pharmacologic approaches to glycemic treatment: standards of medical care in diabetes—2022. Diabetes Care. 2022;45(Supplement_1):S125–S143. doi:10.2337/dc22-S009
23. Generalised anxiety disorder and panic disorder in adults: management clinical guideline; 2011. Available from: www.nice.org.uk/guidance/cg113.
24. Ferrando L, Bobes J, Gibert J, Soto M, Soto O. MINI entrevista neuropsiquiátrica internacional (MINI International Neuropsychiatric Interview, MINI). Detección Orientación Diagnóstica. 2000;2000:1–25.
25. Lecrubier Y, Sheehan DV, Weiller E, et al. The Mini International Neuropsychiatric Interview (MINI). A short diagnostic structured interview: reliability and validity according to the CIDI. Euro Psychiatry. 1997;12(5):224–231. doi:10.1016/S0924-9338(97)83296-8
26. Zigmond AS, Snaith RP. The Hospital Anxiety and Depression Scale. Acta Psychiatr Scand. 1983;67(6):361–370. doi:10.1111/j.1600-0447.1983.tb09716.x
27. López-Alvarenga JC, Vázquez-Velázquez V, Arcila-Martínez D, et al. Accuracy and diagnostic usefulness of Hospital Anxiety and Depression Scale (HAD) in a sample of Mexican obese subjects; 2002. Available from: www.imbiomed.com.mx.
28. Khuwaja AK, Lalani S, Dhanani R, Azam IS, Rafique G, White F. Anxiety and depression among outpatients with type 2 diabetes: a multi-centre study of prevalence and associated factors. Diabetol Metab Syndr. 2010;2(1):72. doi:10.1186/1758-5996-2-72
29. Alcántara-Garcés MT, Rodríguez-Ramírez AM, García-Ulloa AC, Hernández-Jiménez S. Comorbidity between recent diagnosis of type 2 diabetes and non-psychotic psychiatric disorders: metabolic characteristics and clinical correlates. Neuropsychiatr Dis Treat. 2022;18:1151–1163. doi:10.2147/NDT.S364556
30. Guidi J, Lucente M, Sonino N, Fava GA. Allostatic Load and Its Impact on Health: a Systematic Review. Psychother Psychosom. 2021;90(1):11–27. doi:10.1159/000510696
31. Galicia-Garcia U, Benito-Vicente A, Jebari S, et al. Pathophysiology of type 2 diabetes mellitus. Int J Mol Sci. 2020;21(17):1–34. doi:10.3390/ijms21176275
32. Altemus M, Sarvaiya N, Neill Epperson C. Sex differences in anxiety and depression clinical perspectives. Front Neuroendocrinol. 2014;35(3):320–330. doi:10.1016/j.yfrne.2014.05.004
33. Chang E, Varghese M, Singer K. Gender and sex differences in adipose tissue. Curr Diab Rep. 2018;18(9):69. doi:10.1007/s11892-018-1031-3
34. García-García E, Aguilar-Salinas CA, Tusié-Luna T, Rull-Rodrigo JA. Early-onset type 2 diabetes in Mexico. IMAJ. 2002;4:444–448.
35. Burns N, Finucane FM, Hatunic M, et al. Early-onset type 2 diabetes in obese white subjects is characterised by a marked defect in beta cell insulin secretion, severe insulin resistance and a lack of response to aerobic exercise training. Diabetologia. 2007;50(7):1500–1508. doi:10.1007/s00125-007-0655-7
36. Kleinridders A, Ferris HA, Cai W, Kahn CR. Insulin action in brain regulates systemic metabolism and brain function. Diabetes. 2014;63(7):2232–2243. doi:10.2337/DB14-0568
37. Milstein JL, Ferris HA. The brain as an insulin-sensitive metabolic organ. Mol Metab. 2021;52:101234. doi:10.1016/J.MOLMET.2021.101234
38. Biessels GJ, Reagan LP. Hippocampal insulin resistance and cognitive dysfunction. Nat Rev Neurosci. 2015;16(11):660–671. doi:10.1038/NRN4019
39. Cai W, Xue C, Sakaguchi M, et al. Insulin regulates astrocyte gliotransmission and modulates behavior. J Clin Invest. 2018;128(7):2914–2926. doi:10.1172/JCI99366
40. Martin H, Bullich S, Guiard BP, Fioramonti X. The impact of insulin on the serotonergic system and consequences on diabetes-associated mood disorders. J Neuroendocrinol. 2021;33:4. doi:10.1111/jne.12928
41. Blanco C, Rubio J, Wall M, Wang S, Jiu CJ, Kendler KS. Risk factors for anxiety disorders: common and specific effects in a national sample. Depress Anxiety. 2014;31(9):756–764. doi:10.1002/da.22247
42. de Jong M, Oskam MJ, Sep SJS, et al. Sex differences in cardiometabolic risk factors, pharmacological treatment and risk factor control in type 2 diabetes: findings from the Dutch Diabetes Pearl cohort. BMJ Open Diabetes Res Care. 2020;8:1. doi:10.1136/bmjdrc-2020-001365
43. McIntyre RS, Soczynka JK, Konarski JZ, Kennedy SH. The effect of antidepressants on lipid homeostasis: a cardiac safety concern? Expert Opin Drug Saf. 2006;5(4):523–537. doi:10.1517/14740338.5.4.523
44. Khapre M, Kant R, Sharma D, Sharma A. Antidepressant use and glycemic control in diabetic population: a meta-analysis. Indian J Endocrinol Metab. 2020;24(4):295–300. doi:10.4103/ijem.IJEM_258_20
45. Gagnon J, Lussier MT, MacGibbon B, Daskalopoulou SS, Bartlett G. The impact of antidepressant therapy on glycemic control in Canadian primary care patients with diabetes mellitus. Front Nutr. 2018;5. doi:10.3389/fnut.2018.00047
46. Kristensen FP, Rohde C, Østergaard SD, Thomsen RW. Four-year HbA1c and LDL-cholesterol trajectories among individuals with mental disorders and newly developed type 2 diabetes. Brain Behav. 2021;11:11. doi:10.1002/brb3.2372
47. Galler A, Tittel SR, Baumeister H, et al. Worse glycemic control, higher rates of diabetic ketoacidosis, and more hospitalizations in children, adolescents, and young adults with type 1 diabetes and anxiety disorders. Pediatr Diabetes. 2021;22(3):519–528. doi:10.1111/pedi.13177
48. Fujikawa T. Central regulation of glucose metabolism in an insulin-dependent and -independent manner. J Neuroendocrinol. 2021;33:4. doi:10.1111/jne.12941
49. Kullmann S, Kleinridders A, Small DM, et al. Central nervous pathways of insulin action in the control of metabolism and food intake. Lancet Diabetes Endocrinol. 2020;8:524–534. doi:10.1016/S2213-8587(20)30113-3
50. Xu J, van Dam NT, Feng C, et al. Anxious brain networks: a coordinate-based activation likelihood estimation meta-analysis of resting-state functional connectivity studies in anxiety. Neurosci Biobehav Rev. 2019;96:21–30. doi:10.1016/j.neubiorev.2018.11.005
51. Martin EI, Ressler KJ, Binder E, Nemeroff CB. The neurobiology of anxiety disorders: brain imaging, genetics, and psychoneuroendocrinology. Psychiatr Clin North Am. 2009;32(3):549–575. doi:10.1016/j.psc.2009.05.004
52. Craske MG, Stein MB, Eley TC, et al. Anxiety disorders. Nat Rev Dis Primers. 2017;3. doi:10.1038/nrdp.2017.24
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.