Back to Journals » Neuropsychiatric Disease and Treatment » Volume 13
Long-acting formulations delivering aripiprazole: beyond single-value characterizations of steady-state pharmacokinetics
Authors McConnell SA, Desai DN, Faldu SP, Hard ML, Wehr AY, Weiden PJ ![]() , von Moltke L
, von Moltke L
Received 6 June 2017
Accepted for publication 7 June 2017
Published 12 July 2017 Volume 2017:13 Pages 1815—1816
DOI https://doi.org/10.2147/NDT.S143337
Checked for plagiarism Yes
Editor who approved publication: Dr Roger Pinder
Scott A McConnell,1 Dharmik N Desai,1 Sejal P Faldu,1 Marjie L Hard,2 Angela Y Wehr,3 Peter J Weiden,1 Lisa von Moltke3
1Medical Affairs, Alkermes, Inc., Waltham, MA, 2Nuventra Pharma Sciences, Durham, NC, 3Clinical Research, Alkermes, Inc., Waltham, MA, USA
The recent publication by Salzman et al1 compared pharmacokinetic (PK) data from population PK (popPK) models for two long-acting antipsychotic formulations: aripiprazole once-monthly 400 mg (AOM 400) and aripiprazole lauroxil (AL). We would like to address a few major concerns. The AL popPK model has been well described in a peer-reviewed publication.2 However, Salzman et al omitted publishing information regarding the development and validation of the AOM popPK model, including any critical discussion of the covariates, other key characteristics, assumptions and limitations of the AOM model. Thus, a reader cannot objectively assess the simulated values for AOM reported in the publication.
View the original paper by Salzman and colleagues.
Dear editor
The recent publication by Salzman et al1 compared pharmacokinetic (PK) data from population PK (popPK) models for two long-acting antipsychotic formulations: aripiprazole once-monthly 400 mg (AOM 400) and aripiprazole lauroxil (AL). We would like to address a few major concerns. The AL popPK model has been well described in a peer-reviewed publication.2 However, Salzman et al omitted publishing information regarding the development and validation of the AOM popPK model, including any critical discussion of the covariates, other key characteristics, assumptions and limitations of the AOM model. Thus, a reader cannot objectively assess the simulated values for AOM reported in the publication.
In addition, the authors compared simulations from these two popPK models and focused only on selected PK parameters: the steady-state exposures (Cavg,ss and Cmin,ss). With the statement, “At least half of the observed aripiprazole Cmin,ss for AL 441 mg were below the median Cmin,ss for oral aripiprazole 10 mg daily,” the authors seem to imply that the median minimum plasma concentration of 94 ng/mL, which results from the lowest effective dose of oral aripiprazole (10 mg daily), is a necessary threshold for efficacy, rather than a summary PK value. By definition of the term “median”, half of the minimum plasma concentration values for the 10 mg oral aripiprazole dose would also fall below 94 ng/mL. More importantly, the efficacy of AL 441 mg every 4 weeks, with its associated PK profile, was established in a Phase III study.3 Focusing on a single median steady-state exposure value ignores the intricacies of the entire PK profile and does not contribute to an understanding of overall clinical effectiveness.
The entire aripiprazole concentration–time curve following the administration of AL provides a complete and more meaningful view of the AL PK profile. The prodrug formulation of AL enables sustained release of aripiprazole with consistent drug levels maintained over the dosing interval.2 The PK profile of AOM 400 mg, however, is different, with peak–trough fluctuations as shown in Figure 1.4 The half-life of AL doses ranges from 53.9 days to 57.2 days, while the half-life of AOM 400 is 46.5 days.5,6 Thus, the PK profiles of 882 mg every 4 weeks and AOM 400 mg are not equivalent. These contrasting PK profiles have clinical implications including different dosing intervals and missed dose recommendations for AOM and AL.5,6
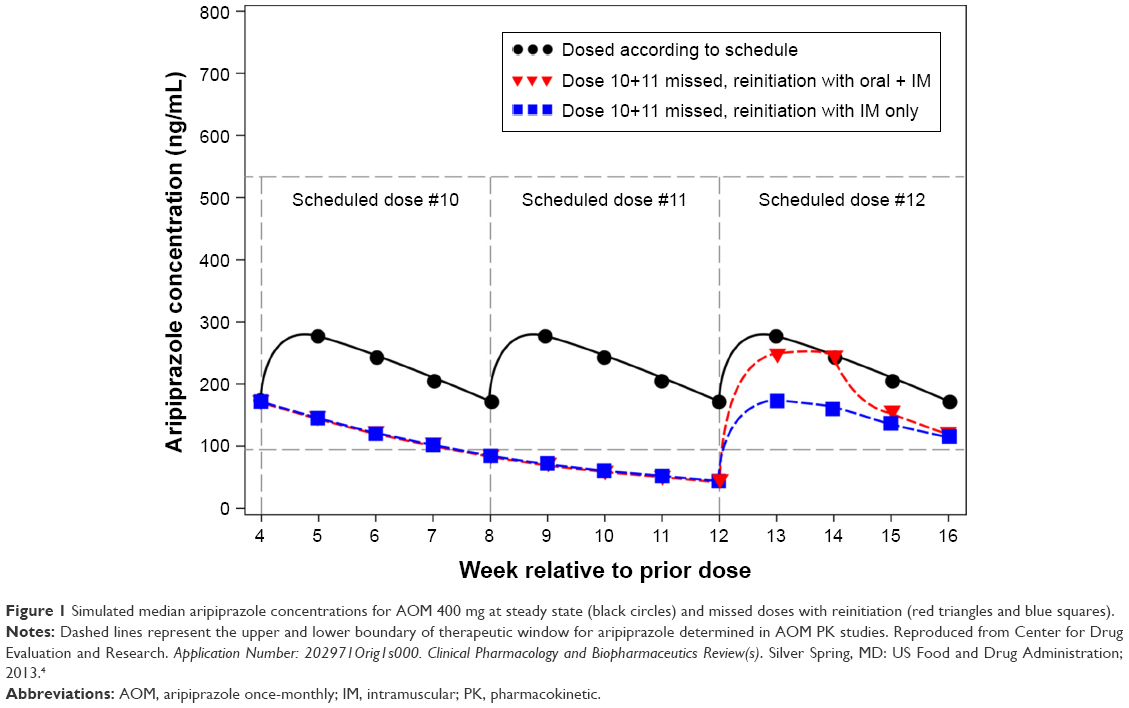 | Figure 1 Simulated median aripiprazole concentrations for AOM 400 mg at steady state (black circles) and missed doses with reinitiation (red triangles and blue squares). |
In summary, the efficacy of AL 441 mg and 882 mg dosed every 4 weeks has been demonstrated, with the 882 mg dose offering higher exposures than 441 mg. All AL doses exhibit stable exposures over the 4–6-week dosing intervals and offer clinicians multiple exposure options to match patients’ individual treatment needs.
Disclosure
All of the authors are current or former employees of Alkermes, Inc. and MLH is an employee of Nuventra Pharma Sciences. The authors report no other conflicts of interest in this communication.
References
Salzman PM, Raoufinia A, Legacy S, Such P, Eramo A. Plasma concentrations and dosing of 2 long-acting injectable formulations of aripiprazole. Neuropsychiatr Dis Treat. 2017;13:1125–1129. | ||
Hard ML, Mills RJ, Sadler BM, Turncliff RZ, Citrome L. Aripiprazole lauroxil: pharmacokinetic profile of this long-acting injectable antipsychotic in persons with schizophrenia. J Clin Psychopharmacol. 2017;37(3):289–295. | ||
Meltzer HY, Risinger R, Nasrallah HA, et al. A randomized, double-blind, placebo-controlled trial of aripiprazole lauroxil in acute exacerbation of schizophrenia. J Clin Psychiatry. 2015;76(8):1085–1090. | ||
Center for Drug Evaluation and Research. Application Number: 202971Orig1s000. Clinical Pharmacology and Biopharmaceutics Review(s). Silver Spring, MD: US Food and Drug Administration; 2013. | ||
ABILIFY MAINTENA® [prescribing information]. Tokyo, Japan: Otsuka Pharmaceutical Co., Ltd.; 2017. | ||
ARISTADA® [prescribing information]. Waltham, MA: Alkermes, Inc.; 2017. | ||
Dove Medical Press encourages responsible, free and frank academic debate. The content of the Neuropsychiatric Disease and Treatment ‘letters to the editor’ section does not necessarily represent the views of Dove Medical Press, its officers, agents, employees, related entities or the Neuropsychiatric Disease and Treatment editors. While all reasonable steps have been taken to confirm the content of each letter, Dove Medical Press accepts no liability in respect of the content of any letter, nor is it responsible for the content and accuracy of any letter to the editor. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.