Back to Journals » International Journal of Women's Health » Volume 18
Local Triamcinolone Injection versus Anti-Tuberculosis Triple Therapy for Non-Puerperal Mastitis: A Comparative Study
Authors Yang L, Wang H, Ma L, Gao D, Qu R
Received 1 April 2026
Accepted for publication 28 June 2026
Published 13 July 2026 Volume 2026:18 613713
DOI https://doi.org/10.2147/IJWH.S613713
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Matteo Frigerio
Video abstract of “Triamcinolone vs Anti-Tuberculosis Triple Therapy in Mastitis” [613713].
Views: 4
Li Yang, Huijing Wang, Lixia Ma, Dan Gao, Rui Qu
Department of Breast and Thyroid Surgery, The Third Affiliated Hospital of Zunyi Medical University (Zunyi First People’s Hospital), Zunyi, 563000, People’s Republic of China
Correspondence: Rui Qu, Email [email protected]
Introduction: This study aims to compare the performance of local triamcinolone injection and anti-tuberculosis triple therapy in treating patients with non-puerperal mastitis (NPM).
Methods: This retrospective cohort study included patients diagnosed with NPM at the Breast Surgery Department of the First People’s Hospital of Zunyi City between October 2021 and December 2024. Patients were categorized into the triamcinolone group and the anti-tuberculosis group based on the treatment administered. The remission rates, treatment duration, and drug-related adverse reactions were compared between the two groups.
Results: A total of 92 cases were included for final analysis, with 44 in the triamcinolone group and 48 in the anti-tuberculosis treatment group. The median treatment duration (41.50 (30.00– 60.50) days vs 120.00 (90.00– 187.50) days, P < 0.001), and complication rate (13.6% vs 66.7%, P < 0.001) were significantly lower in patients of the triamcinolone group, while the remission rate (91.95 (81.62– 100.00)% vs 82.35 (54.55– 100.00)%, P = 0.029) and partial remission rate (97.7% vs 68.8%, P < 0.001) were significantly higher. The multivariate logistic regression analysis showed that pathological type (OR = 0.296, 95% CI: 0.091– 0.963, P = 0.040) and first affected area (OR = 1.099, 95% CI: 1.025– 1.178, P = 0.008) were independent influencing factors of remission rate.
Conclusion: Intralesional triamcinolone injection appears to be associated with shorter treatment duration, higher short-term remission rates, and fewer complications compared with antituberculosis triple therapy in patients with NPM. Given the retrospective design, these findings should be validated in prospective randomized studies.
Keywords: non-puerperal mastitis, treatment remission rate, triamcinolone, anti-tuberculosis triple therapy, pathological subtype
Introduction
Non-puerperal mastitis (NPM) is a benign condition characterized by chronic inflammation of the breast. Its main pathological types include plasma cell mastitis (PDM) and granulomatous lobular mastitis (GLM). Both conditions have similar clinical manifestations, including breast lumps, nipple discharge, skin redness and swelling, and sinus tract formation. The disease course generally lasts 9 to 12 months and is prone to recurrence, severely affecting the patient’s quality of life.1 During the acute phase (disease course ≤ 3 months), breast tissue often exhibits rapidly progressing inflammatory infiltration and abscess formation. The recurrence rate after surgical resection alone can reach up to 50%, and some patients may experience recurrence even after undergoing multiple surgeries.2,3 Studies have shown that the onset of NPM may be related to various factors, including changes in hormone levels, abnormalities in the immune system, and microbial infections.4–6 Due to the low detection rate of bacterial culture,7 treatment strategy for NPM has long relied on empirical approaches, lacking targeted drug selection.
Currently, the treatment methods for NPM mainly include broad-spectrum antibiotics, corticosteroids, anti-tuberculosis drugs, surgical excision, and observational therapy.8 Surgery is considered a radical approach and suitable for NPM patients with severe symptoms.9 Meanwhile, due to poor cosmetic outcomes, delayed wound healing, and high recurrence rates,2,3 reducing the extent of inflammation before surgery becomes crucial to balancing efficacy and appearance preservation. Therefore, empirical antibiotic treatments (such as levofloxacin and azithromycin) have been widely used before surgery, but some studies reported limited efficacy and easily induce resistance due to the lack of etiological guidance.10 Oral glucocorticoids (such as prednisone) can alleviate symptoms in the short term, but long-term use over several months carries risks such as Cushing’s syndrome and osteoporosis,11,12 however, the study performed by Mizrakli et al reported that appropriate corticosteroid treatment could help avoid unnecessary surgery in patients with mastitis.13
In recent years, local injection of triamcinolone has gained attention because its efficacy is comparable while significantly reducing systemic complications.14,15 The rifampicin-based triple therapy also shows considerable efficacy in treating NPM, but the 6–8 month medication regimen may lead to liver and kidney function impairment.16
Although there were many treatment options, but current treatment methods vary considerably across institutions and geographic regions, and no universally accepted first-line therapy has been established.17 And the aim of this study is to compare the treatment outcomes between local triamcinolone injection and anti-tuberculosis treatment in patients with NPM.
Materials and Methods
Study Design and Patients
This retrospective study included patients diagnosed with NPM at the First People’s Hospital of Zunyi City between October 2021 and December 2024. The inclusion criteria were as follows: (1) Age ≥ 18 years; (2) Clinical manifestations, physical examination, and ultrasound findings suggestive of inflammatory breast lesions; (3) Pathologically confirmed NPM; (4) Patients who had no prior treatment with triamcinolone or anti-tuberculosis therapy. Patients with incomplete clinical data were excluded from the study. This study was approved by the Ethics Committee of the First People’s Hospital of Zunyi City (Approval ID: # (2024)-1-217), and the requirement for written informed consent was waived due to the retrospective nature of the study. As patient consent to review medical records was not required by the Ethics Committee, all patient data were anonymized and handled confidentially throughout the study.
Treatment
All included patients were divided into the triamcinolone group and the anti-tuberculosis group according to the patients’ treatment. Patients in both groups first received empirical treatment with broad-spectrum antibiotics (levofloxacin and cefuroxime) for 1–2 weeks to control the acute inflammatory response.
For patients without abscess or sinus tract formation in the triamcinolone group, triamcinolone acetonide was injected directly. For patients with abscesses or sinus tract formation, pus was aspirated under ultrasound guidance, and the abscess cavity was rinsed with 0.9% sodium chloride solution until clear. Then, a triamcinolone suspension (30–40 mg per session) was injected along the deep edge of the inflammation, followed by compression bandaging, once a week. At weeks 1–2, the single dose of triamcinolone acetonide was 30–40 mg, while at weeks 3–4, the single dose of triamcinolone acetonide decreased to 20–30 mg. If the remission rate remained > 60% after 4 weeks, the patient could receive a single dose of triamcinolone acetonide ≤20 mg at week 5–6 based on their preference (Figure S1A).
For patients without abscess or sinus tract formation in the anti-tuberculosis group, oral anti-tuberculosis triple drugs were given directly. For patients with abscesses or sinus tract formation, abscesses were managed with ultrasound-guided aspiration drainage or incision drainage. Rifampicin (450 mg/d), isoniazid (300 mg/d), and ethambutol (15 mg/kg/d) were administered orally. Treatment continued until 1 month after ultrasound confirmation of resolution of inflammation, with a minimum duration of 4 weeks. If disease progression or serious adverse events (SAEs) occur during treatment, the treatment is terminated, and the protocol is adjusted.
Patients in both groups reached the predetermined reduction area, and based on the patient’s preference, an expanded excision of the lesion was performed (with the margin at least 5 mm from the ultrasound-visible inflammation boundary), with intraoperative rapid pathology confirming negative margins. Clinical and ultrasound assessments will be conducted monthly after treatment, with re-examinations every 3 months following recovery. Specifically, the ultrasound assessments were performed by two experienced breast radiologists with ≥5 years of experience in breast imaging. To minimize inter-observer variability, all measurements were obtained using a standardized protocol (maximum cross-sectional area on each orthogonal plane, recorded at fixed timepoints: baseline, 1, 3, and 6 months).
Data Collection and Outcome Measurement
Demographic data and clinical characteristics were extracted from patient medical records. Clinical manifestations combined with ultrasound images are used for ultrasonic classification, which includes abscess type, mass type, and refractory type (sinus tract formation).18 According to the time of onset, they can be divided into acute phase (≤3 months), subacute phase (3~6 months), and chronic phase (>6 months).2
The primary outcome indicators are the remission rate of inflammation and the treatment duration. Secondary endpoints include complications, recurrence, response rate of pathological subtypes, and adverse events. High-frequency ultrasound was performed using GE LOGIQ E9 (USA) and Mindray Resona (China, R9) equipped with a 10–14 MHz probe to dynamically monitor changes in the lesion area, and the images were independently reviewed by two experienced breast ultrasonographers who were blinded to the treatment group whenever feasible. The largest cross-sectional inflammatory area was measured using the same predefined protocol, in cases of multiple masses, the areas are summed in an overlapping manner. And the final measurement was determined by consensus or by consultation with a senior reviewer in cases of disagreement. After that, the efficacy evaluation was assessed using the remission rate, which was calculated according to the following formula:

With the complete remission (CR) and partial remission (PR) defined as remission rates ≥ 90 and ≥ 60%, respectively.16 No response (NR) was defined as failure to achieve PR or the development of new ulcers or sinus tracts. Recurrence was defined as the appearance of new nodules or sinus tracts, worsening of symptoms, or an increase in lesion area by ≥ 20%.
Adverse events were monitored using identical laboratory and clinical protocols in both groups, minimizing the likelihood of differential ascertainment bias according to the Common Terminology Criteria for Adverse Events (CTCAE) version 4.0. To ensure comparable ascertainment of adverse events across groups, all patients underwent standardized follow-up assessments once per month. Laboratory monitoring (complete blood count, liver function tests, renal function tests) was performed at each monthly visit in both groups, irrespective of symptoms, to minimize differential detection bias.
Statistical Analysis
Data analysis was conducted using R software (version 4.1.1). Continuous variables were assessed for normality using the Shapiro–Wilk test and summarized as mean ± standard deviation or median (interquartile range) and compared using the independent samples T-test or the Wilcoxon rank-sum test, accordingly. Categorical variables were expressed as n (%) and compared using the chi-square test or Fisher’s exact test. Multivariate logistic regression was employed to assess the independent influence of factors on remission rate. A two-tailed P-value < 0.05 was considered statistically significant in this study.
Results
Characteristics of the Study Population
In this study, 162 patients with pathologically confirmed NPM were screened, after exclusion of 43 patients who chose alternative treatment options and 27 lost follow-up, a total of 92 patients were included for final analysis. Among the 92 patients, 44 were in the triamcinolone group, and 48 were in the anti-tuberculosis group. In the triamcinolone group, 8 cases underwent surgical excision after achieving a reduced size, and 2 cases underwent surgery due to recurrence. In the anti-tuberculosis group, 10 cases chose surgical excision after reduction, and 6 cases underwent surgery due to recurrence. The remaining patients opted for conservative follow-up treatment. Ultrasound classification showed there was no significant difference between the two groups (P=0.108). The distribution of pathological types was consistent between the two groups (75.0% PDM vs 70.8% PDM, P=0.83). There were no statistical differences between the groups in other baseline characteristics such as age, initial area, pathological type, obesity, smoking history, and breastfeeding history (all P > 0.05) (Table 1).
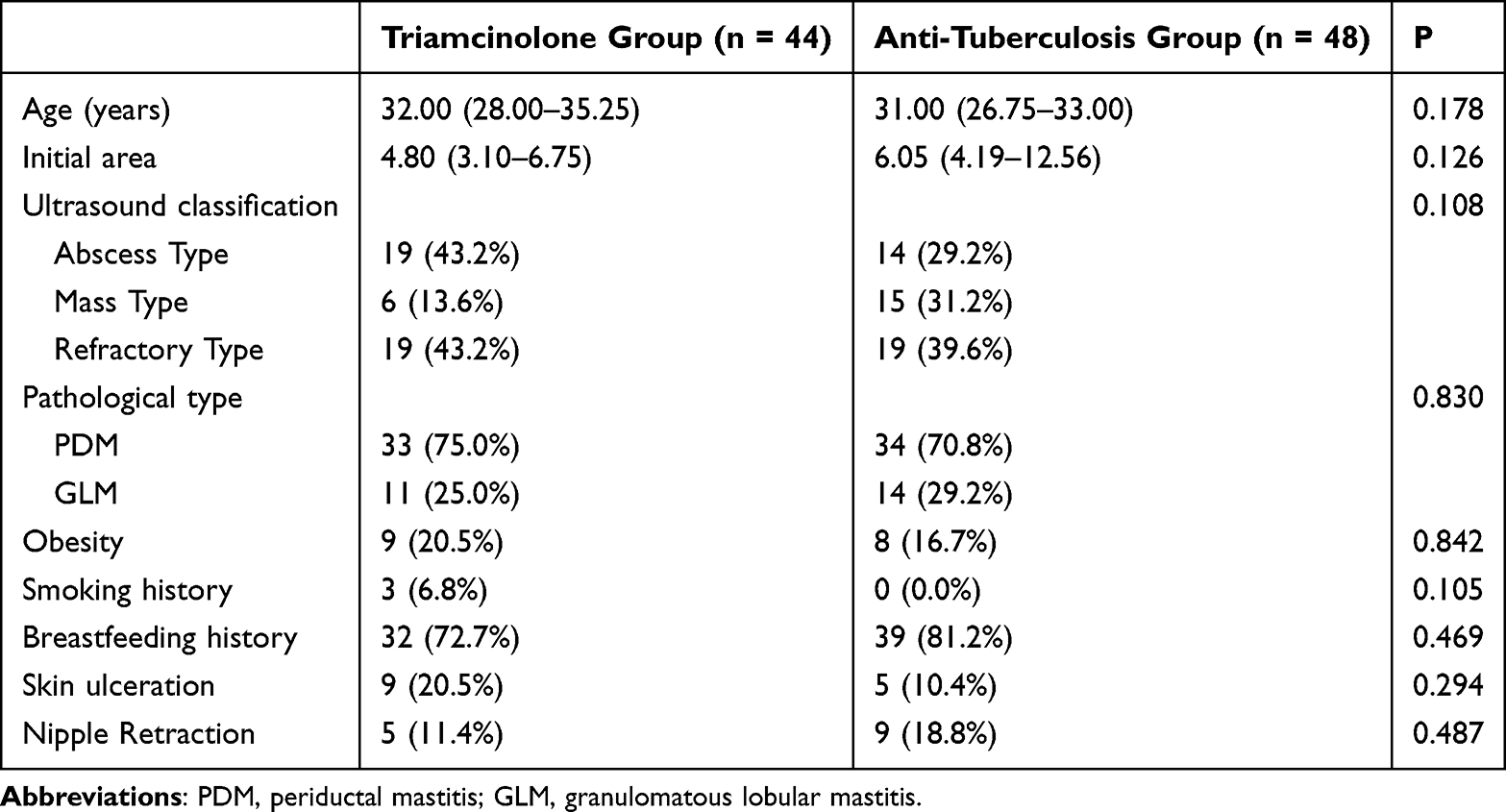 |
Table 1 Demographic and Clinical Characteristics of Participants |
Comparison of Treatment Performance Between the Two Groups
Compared with the anti-tuberculosis group, patients in the triamcinolone group had significantly shorter treatment duration (41.50 (30.00–60.50) vs 120.00 (90.00–187.50) days, P < 0.001), shorter follow-up time (90.50 (57.50–145.50) vs 150.00 (90.00–277.50) days, P < 0.001), and a lower complication rate (13.6% vs 66.7%, P < 0.001). The triamcinolone group also showed significantly higher overall remission rate (91.95 (81.62–100.00%) vs 82.35 (54.55–100.00%), P = 0.029) and partial remission rate (97.7% vs 68.8%, P < 0.001). However, regarding cure rate, there was no statistical significance (52.3% vs 39.6%, P = 0.312) (Table 2).
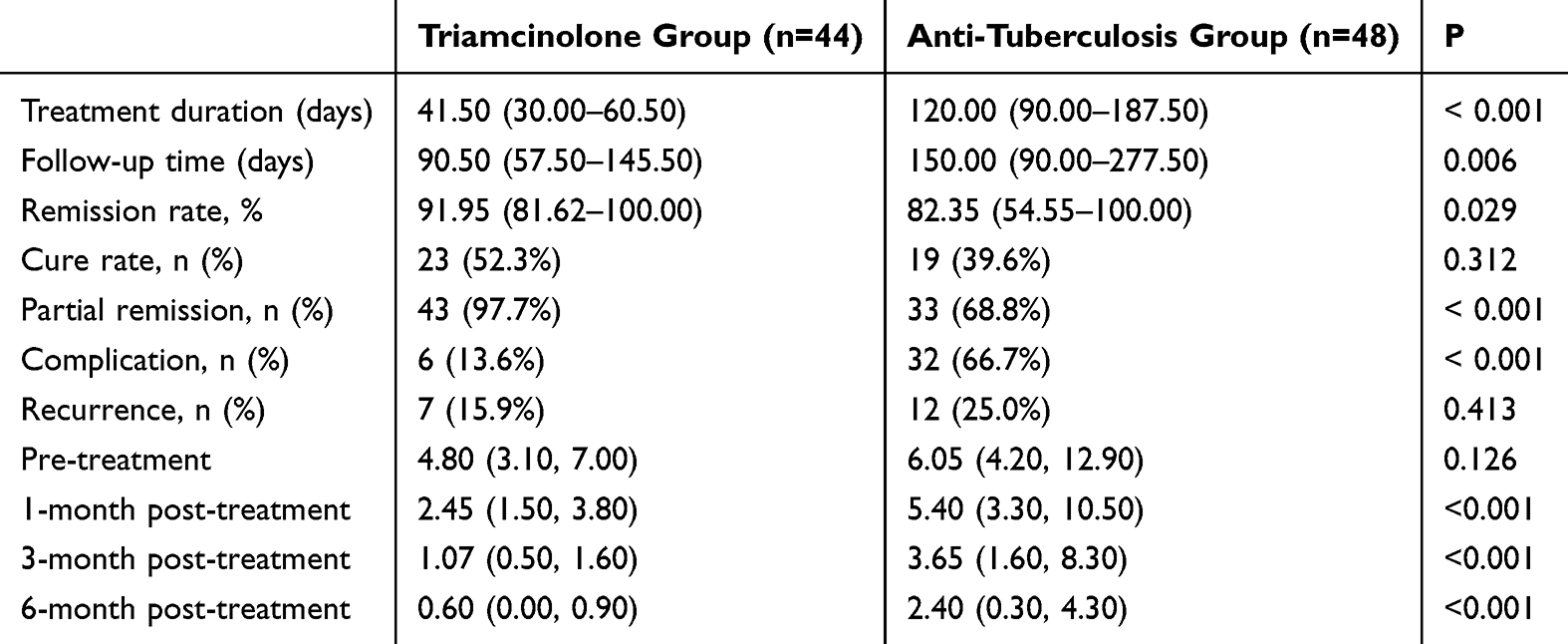 |
Table 2 Treatment Performance and Lesion Areas Between Two Groups |
There was no significant difference in lesion areas between the two groups at pre-treatment (4.800 (3.1, 7.0) vs 6.050 (4.2, 12.9), P = 0.126). However, after 1-month, 3-month, and 6-month of treatment, the lesion areas were significantly lower in patients of Triamcinolone group (2.45 (1.50, 3.80) vs 5.40 (3.30, 10.50), P < 0.001), (1.07 (0.50, 1.60) vs 3.65 (1.60, 8.30), P < 0.001), and (0.60 (0.00, 0.90) vs 2.40 (0.30, 4.30), P < 0.001) (Table 2). After three months of treatment, the inflammatory area in the Triamcinolone group was reduced by 77.7% compared to the baseline, which was significantly greater than the 39.7% reduction observed in the Anti-tuberculosis group (P < 0.001). In a typical case of a 36-year-old female patient with granulomatous mastitis receiving local intralesional injection therapy, imaging follow-up showed a progressive reduction in lesion size from 3.97 cm2 to 0.18 cm2, indicating effective resolution of the inflammatory lesion (Figure S1B–E). Among the pathological subtypes, the efficacy of GLM and PDM in the triamcinolone group was significantly different (GLM 93.1% vs PDM 91.1%, P < 0.001), while in the Anti-tuberculosis group, the remission rate of GLM was higher than that of PDM (GLM 86.5% vs PDM 74.9%, P < 0.001).
Regarding complications, most patients experienced two or more adverse events during treatment. In the triamcinolone group, the main complications were menstrual disorders (11.3%) and weight gain (11.3%). In contrast, liver and kidney function abnormalities were the predominant complications in the anti-tuberculosis group (54.1% and 18.7%) (Table 3).
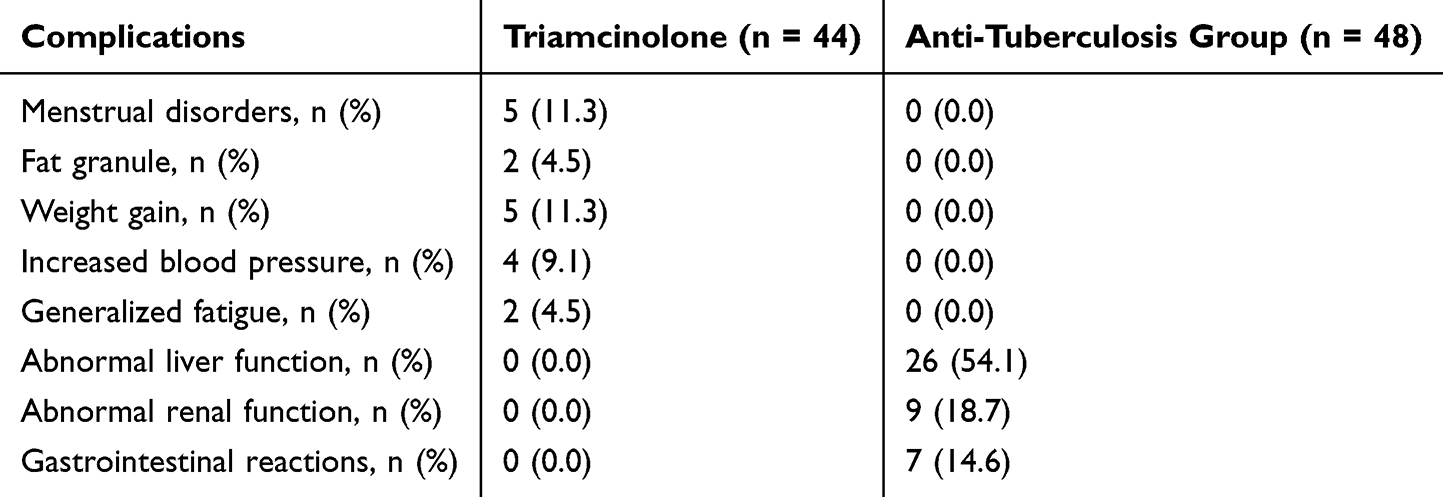 |
Table 3 Complications in the Two Groups |
Multivariate Logistic Regression Analysis
The results of multivariate logistic regression analysis showed that pathological type (OR = 0.296, 95% CI: 0.091–0.963, P = 0.040) and first affected area (OR = 1.099, 95% CI: 1.025–1.178, P = 0.008) were independently associated with remission rate. Clinically, this suggests that patients with certain pathological types of PDM may have a lower likelihood of remission, while a larger initial lesion area may be associated with better treatment response (Table 4).
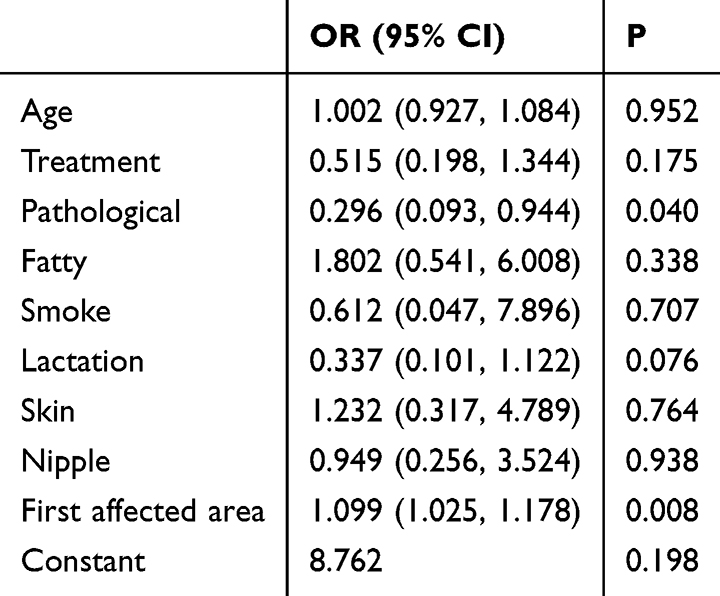 |
Table 4 Multivariate Logistics Analysis of Remission Rate |
Recurrence Rate
The comparison the recurrence rate between the two group showed that in recurrence patients of the triamcinolone group, both the follow-up time (62.00 (54.50–66.50) vs 32.00 (30.00–60.00), P = 0.035) and complication rate (42.9% vs 8.1%, P = 0.042) were significantly higher, but the difference in the number of injections was not statistically significant (P = 0.093) (Table 5).
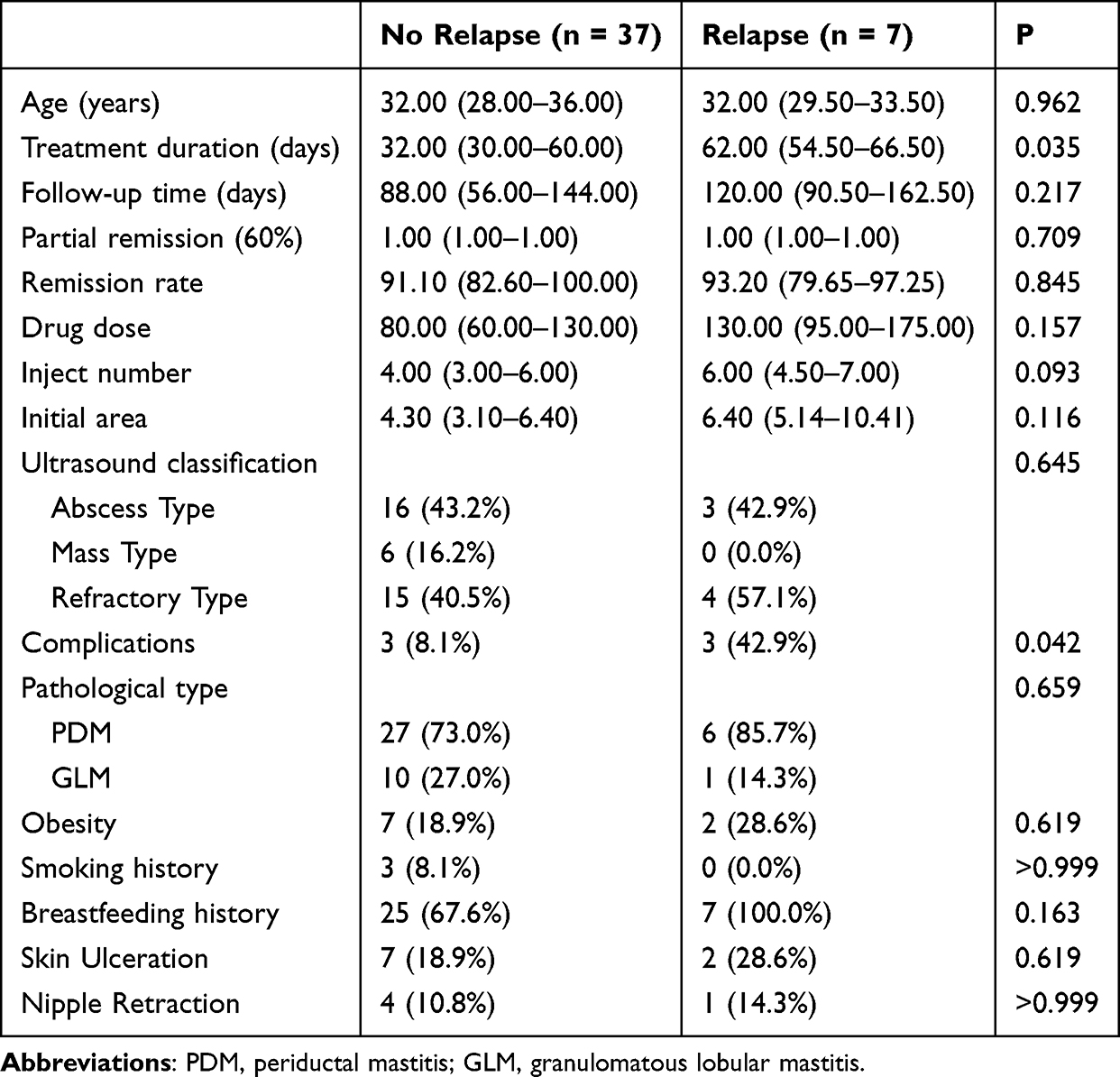 |
Table 5 Comparison of Characteristics Among Patients of Relapse Group and Non-Relapse Group |
Discussion
The results of this study showed that triamcinolone exhibited shorter treatment duration, higher remission rates, and fewer complications. Lesion areas reduced significantly faster in patients of the triamcinolone group, moreover, anti-tuberculosis therapy had higher liver/kidney toxicity. Multivariate analysis revealed that pathological type and first affected area were independent influencing factors of remission rate. This study exhibited that triamcinolone has better performance than anti-tuberculosis drugs for NPM patients, though longer follow-up is still needed.
We found that the long-term efficacy results of the two groups were similar. Compared to the anti-tuberculosis triple therapy, the treatment cycle of the Triamcinolone group was shortened by 2.8 times, the acute phase remission rate increased by 38.1%, and the risk of complications was significantly reduced. This result may be attributed to the dual mechanism of action of glucocorticoids: on one hand, they rapidly inhibit the expression of pro-inflammatory factors such as IL-6 and TNF-α, blocking the differentiation of B cells into plasma cells,19 and directly suppresses the local inflammation cascade reaction. On the other hand, it can maintain the stability of the lesion microenvironment, thereby creating better conditions for subsequent surgery. Therefore, ultrasound-guided local injection of triamcinolone for treating NPM has a significant advantage in rapidly reducing lesion size in the short term, facilitating a transition to surgery. However, in the present study, only 8 cases decided to receive surgery after triamcinolone treatment.
In the treatment of periductal mastitis (PDM), previous studies have often recommended surgery combined with antibiotic therapy, empirically choosing options such as clindamycin, levofloxacin, or azithromycin.20 In adherence to the principle that appropriate treatment of the cause of infection must be carried out before the use of steroids.21 The study performed a 1-week course of broad-spectrum antibiotics before triamcinolone or anti-tuberculosis treatment, and both methods showed a great mean remission rate of > 80%, in patients who received local triamcinolone, the median remission rate even reached 92%, which also supports the finding by Zhou’s team that NPM is typically caused by a local immune inflammatory response in the breast.6 In addition, this study found that patients with PDM had a lower lesion remission rate compared to those with GLM (OR = 0.296, 95% CI: 0.093–0.944, P = 0.040), which may be related to the higher propensity of sinus tract formation in PDM. However, to date, no study has specifically compared the prognostic outcomes between GLM and PDM.
For the treatment of GLM, local steroid injection therapy was chosen to reduce systemic complications.22 Studies have shown that triamcinolone local injection combined with surgery for GLM demonstrates advantages such as rapid onset, high efficacy, and fewer adverse reactions compared to oral glucocorticoids.23 In the study performed by Tang et al, they also revealed that Intralesional steroid injection is an effective treatment; they showed that intralesional steroid injection could achieve resolution with an average of 2 months,24 while in the present study, the median treatment duration was even lower (41.5 days). Although triamcinolone showed great performance, the adverse reactions, such as reversible menstrual disorders, increased blood pressure, and weight gain, were also observed, especially for the menstrual disorders; the incidence reached 11.3%, which was slightly higher than a previous study, where 8 out of 95 females experienced menstrual disorders.25
Regarding adverse events and effect size, the complication rate was substantially lower in the triamcinolone group. This large between-group difference primarily reflects the high incidence of hepatic toxicity and renal toxicity observed in the anti-tuberculosis group, which aligns well with previous literature.26,27 In contrast, the triamcinolone group exhibited predominantly mild and reversible systemic effects mainly caused by corticosteroid, including menstrual irregularity, weight gain, and elevated blood pressure. The magnitude of this safety advantage is both clinically meaningful and pharmacologically plausible, given the distinct mechanisms and systemic exposure profiles of the two therapeutic approaches. More importantly, adverse events were ascertained using identical clinical and laboratory monitoring protocols across both groups: all patients underwent standardized monthly follow-up visits, and routine laboratory assessments.28 The recurrence rate was 15.9% in the triamcinolone group, which was higher than the recurrence rate of 8–11% for most combinations of single-drug hormones with antibiotics and hormones.29,30 All these results indicated that the optimal dosage of triamcinolone should be further explored in the large-scale study with dosage gradients.
The anti-tuberculosis performance on the GLM group is comparable to that of PDM, suggesting that the mechanism of GLM may be related to bacterial factors. Liu Tiangang’s team found that the detection rate of Corynebacterium kroppenstedtii in GLM lesions was 72.4%, and rifampicin had a strong inhibitory effect on this bacterium,23 which explains the 74.9% remission rate of GLM in the anti-tuberculosis group in this study. In our study, the partial remission rate of the anti-tuberculosis group in NPM was 68.8%, which is lower than a previous study reported by Yu et al, who showed that all patients were cured after anti-mycobacterial drug treatment plus surgery, while 16 out of 27 (59.3%) were cured with drug treatment alone.31 The difference is due to the different remission rate criteria, with their study using 30% while ours used 60%. The performance was also affected by the ultrasonographic classification; a higher incidence of sinus tract cases was observed in their study compared to ours. Even though the overall remission rate in our anti-tuberculosis group was 82.35%, the risk of complications from tuberculosis treatment limited its wider application.
Although our findings support the short-term superiority of intralesional triamcinolone in managing NPM, their generalizability must be interpreted with caution, considering ongoing debates regarding disease etiology. Our study did not assess microbial burden, immune profiling, or host–pathogen interactions within lesions.32 Consequently, it remains unclear whether treatment response is modified by underlying etiological subtypes. Future high-quality studies should integrate clinical phenotyping with molecular diagnostics to identify predictive biomarkers that could guide personalized therapy.33,34 Patients with confirmed bacterial involvement might benefit from a combined or sequential approach, using local steroids for rapid inflammation control followed by targeted antimicrobials to address residual infection. Such a precision medicine framework would represent a significant step toward evidence-based, individualized management of NPM.
This study still had several limitations, firstly, the small sample size and retrospective nature limit the generalizability of the results, classification based on patient preference rather than random assignment may introduce selection bias, the ultrasound examinations were performed by experienced radiologists therefore no inter-observer reliability test was performed, also, complete blinding of ultrasound assessors to treatment allocation was not feasible, which may introduce potential measurement bias in lesion area assessment; secondly, the follow-up period was relatively short (with a median of 90.5 days in the triamcinolone group), which could hinder the comprehensive assessment of long-term efficacy, such as cure rate and recurrence risk, future study should focus more on the long-term prognosis; thirdly, the inclusion of both PDM and GLM within a single cohort, while justified by their shared clinical management pathway, introduces pathological heterogeneity that may dilute treatment effect estimates, and more in-depth stratified research is needed for validation; fourthly, all patients received 1–2 weeks of empirical broad-spectrum antibiotic therapy to control acute superinfection prior to definitive treatment allocation, although the pre-treatment may introduce a potential confounding effect for the final outcome, it also helps standardize baseline inflammatory status. Additionally, combining imaging or biomarker dynamic monitoring of lesion changes may provide more precise evidence for efficacy evaluation. The combined sequential strategy (triamcinolone injection during the acute phase followed by anti-tuberculosis consolidation during the stable phase) is worth exploring in the future.
Conclusion
Both triamcinolone and anti-tuberculosis therapies demonstrate efficacy in the management of NPM. However, intralesional triamcinolone injection appears to be associated with shorter treatment duration, higher short-term remission rates, and fewer complications. Given the retrospective design and limited follow-up of this study, these findings should be interpreted with caution. Further prospective, randomized studies are warranted to confirm long-term efficacy and optimize patient selection.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
This study was approved by the Ethics Committee of the First People’s Hospital of Zunyi City (Approval ID: # (2024)-1-217), I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments, and the requirement for individual written informed consent was waived by the Ethics Committee of the First People’s Hospital of Zunyi City owing to the retrospective design of the study. As patient consent to review medical records was not required by the Ethics Committee, all patient data were anonymized and handled confidentially throughout the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was carried out with support from the Zunyi Science and Technology Plan Project Science and Technology Cooperation, under grant number HZ (2025)34.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Feng J, Gao Q, Qu W, et al. Clinical characteristics of non-puerperal mastitis: a retrospective analysis of 724 patients. Int J Womens Health. 2024;16:2113–9. doi:10.2147/IJWH.S485461
2. Wilson JP, Massoll N, Marshall J, Foss RM, Copeland EM, Grobmyer SR. Idiopathic granulomatous mastitis: in search of a therapeutic paradigm. Am Surg. 2007;73(8):798–802. doi:10.1177/000313480707300813
3. Hur SM, Cho DH, Lee SK, et al. Experience of treatment of patients with granulomatous lobular mastitis. J Korean Surg Soc. 2013;85(1):1–6. doi:10.4174/jkss.2013.85.1.1
4. Sripathi S, Ayachit A, Bala A, Kadavigere R, Kumar S. Idiopathic granulomatous mastitis: a diagnostic dilemma for the breast radiologist. Insights Imag. 2016;7(4):523–529. doi:10.1007/s13244-016-0497-2
5. Shi L, Wu J, Hu Y, et al. Biomedical indicators of patients with non-puerperal mastitis: a retrospective study. Nutrients. 2022;14(22):4816. doi:10.3390/nu14224816
6. Zhou Y, Gong J, Deng X, Shen L, Liu L. Novel insights: crosstalk with non-puerperal mastitis and immunity. Front Immunol. 2024;15:1431681. doi:10.3389/fimmu.2024.1431681
7. Kıvılcım T, Altıntoprak F, Memiş B, et al. Role of bacteriological agents in idiopathic granulomatous mastitis: real or not? Eur J Breast Health. 2019;15(1):32–36. doi:10.5152/ejbh.2018.4249
8. Jiao Y, Chang K, Jiang Y, Zhang J. Identification of periductal mastitis and granulomatous lobular mastitis: a literature review. Ann Transl Med. 2023;11(3):158. doi:10.21037/atm-22-6473
9. Xu H, Liu R, Lv Y, et al. Treatments for periductal mastitis: systematic review and meta-analysis. Breast Care. 2022;17(1):55–62. doi:10.1159/000514419
10. Salmanov AG, Savchenko SE, Chaika K, et al. Postpartum mastitis in the breastfeeding women and antimicrobial resistance of responsible pathogens in Ukraine: results a multicenter study. Wiad Lek. 2020;73(5):895–903. doi:10.36740/WLek202005111
11. Zhao ZM, Ding JM, Li Y, Wang DC, Kuang MJ. Human umbilical cord mesenchymal stem cell-derived exosomes promote osteogenesis in glucocorticoid-induced osteoporosis through PI3K/AKT signaling pathway-mediated ferroptosis inhibition. Stem Cells Transl Med. 2025;14(3). doi:10.1093/stcltm/szae096
12. Nachawi N, Li D, Lansang MC. Glucocorticoid-induced adrenal insufficiency and glucocorticoid withdrawal syndrome: two sides of the same coin. Cleve Clin J Med. 2024;91(4):245–255. doi:10.3949/ccjm.91a.23039
13. Mizrakli T, Velidedeoglu M, Yemisen M, et al. Corticosteroid treatment in the management of idiopathic granulomatous mastitis to avoid unnecessary surgery. Surg Today. 2015;45(4):457–465. doi:10.1007/s00595-014-0966-5
14. Chen X, Huang H, Huang H, et al. Ductal lavage followed by observation versus oral corticosteroids in idiopathic granulomatous mastitis: a randomized trial. Nat Commun. 2024;15(1):9144. doi:10.1038/s41467-024-53143-2
15. Cabioglu N, Uras C, Mutlu H, et al. Local steroid injection in severe idiopathic granulomatous mastitis as a new first-line treatment modality with promising therapeutic efficacy. Front Med Lausanne. 2023;10:1251851. doi:10.3389/fmed.2023.1251851
16. Zhou F, Li H, Wang F, et al. Efficacy and safety of rifampicin-based triple therapy for non-puerperal mastitis: a single-arm, open-label, prospective clinical trial. Int J Infect Dis. 2024;140:25–30. doi:10.1016/j.ijid.2023.12.008
17. Zhou F, Shang XC, Tian XS, Yu ZG. Clinical practice guidelines for diagnosis and treatment of patients with non-puerperal mastitis: chinese society of breast surgery (CSBrS) practice guideline 2021. Chin Med J. 2021;134(15):1765–1767. doi:10.1097/CM9.0000000000001532
18. Tan H, Li R, Peng W, Liu H, Gu Y, Shen X. Radiological and clinical features of adult non-puerperal mastitis. Br J Radiol. 2013;86(1024):20120657. doi:10.1259/bjr.20120657
19. Strehl C, Ehlers L, Gaber T, Buttgereit F. Glucocorticoids-all-rounders tackling the versatile players of the immune system. Front Immunol. 2019;10:1744. doi:10.3389/fimmu.2019.01744
20. Yuan QQ, Xiao SY, Farouk O, et al. Management of granulomatous lobular mastitis: an international multidisciplinary consensus (2021 edition). Mil Med Res. 2022;9(1):20. doi:10.1186/s40779-022-00380-5
21. Dilaveri C, Degnim A, Lee C, DeSimone D, Moldoveanu D, Ghosh K. Idiopathic granulomatous mastitis. Breast J. 2024;2024:6693720. doi:10.1155/2024/6693720
22. Vercoe J, Sedaghat N, Brennan ME. Intralesional steroid injections for management of granulomatous mastitis: a systematic review of treatment protocols and clinical outcomes. Breast J. 2025;2025(1):2592366. doi:10.1155/tbj/2592366
23. Zhou Y, Xu L. Clinical efficacy of different methods for treatment of granulomatous lobular mastitis: a systematic review and network meta-analysis. PLoS One. 2025;20(2):e0318236. doi:10.1371/journal.pone.0318236
24. Tang A, Dominguez DA, Edquilang JK, Green AJ, Khoury AL, Godfrey RS. Granulomatous mastitis: comparison of novel treatment of steroid injection and current management. J Surg Res. 2020;254:300–305. doi:10.1016/j.jss.2020.04.018
25. Kozaki A, Inoue R, Yaji N, Nishiyama K, Inoue T. Subcutaneous injections of triamcinolone acetonide for upper eyelid retraction and swelling associated with thyroid eye disease: a retrospective case series study. Clin Ophthalmol. 2024;18:2147–2154. doi:10.2147/OPTH.S456543
26. Wang D, Wang S, Jin Z, et al. Tet2 protects against isoniazid-induced hepatotoxicity via regulating autophagy. FASEB j. 2025;39(23):e71300. doi:10.1096/fj.202500245R
27. Saito N, Yoshii Y, Kaneko Y, et al. Impact of renal function-based anti-tuberculosis drug dosage adjustment on efficacy and safety outcomes in pulmonary tuberculosis complicated with chronic kidney disease. BMC Infect Dis. 2019;19(1):374. doi:10.1186/s12879-019-4010-7
28. Chih LH, On AWF, Huang YS. Correlation of antituberculosis drug-related liver injury and liver function monitoring: a 12-year experience of the Taiwan drug relief foundation. J Food Drug Anal. 2014;22(3):356–362. doi:10.1016/j.jfda.2013.10.001
29. Burcu B, Çetinoğlu I, Hacim NA, et al. Comparing the efficacy of intralesional injection versus systemic steroids in treating idiopathic granulomatous mastitis: insights from a single-center experience. Breast Care. 2024;19(6):307–315. doi:10.1159/000541707
30. Sarmadian R, Safi F, Sarmadian H, Shokrpour M, Almasi-Hashiani A. Treatment modalities for granulomatous mastitis, seeking the most appropriate treatment with the least recurrence rate: a systematic review and meta-analysis. Eur J Med Res. 2024;29(1):164. doi:10.1186/s40001-024-01761-3
31. Yu HJ, Wang Q, Yang JM, et al. Anti-mycobacteria drugs therapy for periductal mastitis with fistula. Zhonghua Wai Ke Za Zhi. 2012;50(11):971–974.
32. Qu W, Sun J, Shao S, et al. Associations of obesity-related mammary intraductal secretions with inflammatory severity, immune dysregulation, and adverse prognosis in non-puerperal mastitis: a retrospective cohort study. Lipids Health Dis. 2025;24(1):329. doi:10.1186/s12944-025-02725-0
33. Dai Q, Zhou Y, Wu J, Liao M. Characteristics of metabolites analysis for patients with granulomatous lobular mastitis. Front Cell Infect Microbiol. 2025;15:1514315. doi:10.3389/fcimb.2025.1514315
34. Tu S, Yin Y, Ma L, Chen H, Ye M. Diagnosis of non-puerperal mastitis based on “whole tongue” features: non-invasive biomarker mining and diagnostic model construction. Front Cell Infect Microbiol. 2025;15:1602883. doi:10.3389/fcimb.2025.1602883
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.