")
Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 16
Liver Fibrosis Scores and Coronary Artery Disease: Novel Findings in Patients with Metabolic Dysfunction-Associated Fatty Liver Disease
Authors Lu C , Chen Y , Zhang Y, Zhao X
Received 15 June 2023
Accepted for publication 21 August 2023
Published 29 August 2023 Volume 2023:16 Pages 2627—2637
DOI https://doi.org/10.2147/DMSO.S426102
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Antonio Brunetti
Chuan Lu,1,* Yan Chen,1,* Yue Zhang,2 Xin Zhao1
1Department of Cardiology, The Second Hospital of Dalian Medical University, Dalian, 116023, People’s Republic of China; 2Department of Gastroenterology, The Second Hospital of Dalian Medical University, Dalian, 116023, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Xin Zhao; Yue Zhang, Tel +86-17709870535 ; +86-17709870662, Email [email protected]; [email protected]
Background: Metabolic dysfunction-associated fatty liver disease (MAFLD) is a recently proposed term as a more appropriate definition for nonalcoholic fatty liver disease (NAFLD). Previous studies have shown an association between liver fibrosis scores and cardiovascular disease (CVD) in patients with NAFLD. In this study, we aimed to investigate the relationship between liver fibrosis scores and coronary artery disease (CAD) severity in patients with MAFLD.
Methods: This study was conducted on 1346 patients with MAFLD at the Second Hospital of Dalian Medical University between January 2018 and December 2021. We calculated the liver fibrosis scores, including the fibrosis 4 (FIB-4) score, nonalcoholic fatty liver disease fibrosis score (NFS), and aspartate aminotransferase-to-platelet ratio index (APRI). We divided the participants into three groups based on the degree of coronary artery stenosis assessed using coronary computed tomography angiography (CCTA): CAD (≥ 50%), non-obstructive (1– 49%), and normal (no stenosis).
Results: An increased FIB-4 score and NFS were significantly associated with CAD severity in patients with MAFLD. The percentage of patients with a high FIB-4 score was higher in the CAD group than in the other two groups (5.80%, 4.31%, and 2.24%, respectively; p< 0.001), as was the percentage of patients with NFS (11.12%, 5.19%, and 0.93%, respectively; p< 0.001). Carotid atherosclerosis, creatinine levels, and CAC scores were significant predictors of CAD. The FIB-4 score and NFS were independently associated with CAD even after adjusting for sex and well-known cardiovascular risk factors. The APRI was not a significant factor for CAD in any model. In the bivariate correlation analysis, the FIB-4 score and NFS were directly correlated with CAC scores.
Conclusion: Non-invasive liver fibrosis scores (FIB-4 and NFS) were significantly associated with the CAD severity and CAC scores in patients with MAFLD. Screening for CAD may be beneficial for subjects with high liver fibrosis risk MAFLD.
Keywords: metabolic dysfunction-associated fatty liver disease, coronary artery disease, liver fibrosis scores, coronary artery calcium scores, nonalcoholic fatty liver disease
Introduction
Fatty liver disease is a prevalent and significant health issue worldwide, and is characterized by the accumulation of excess fat in the liver. It has been recognized as the most rapidly increasing cause of liver-related mortality for several decades and affects nearly a quarter of the adults in the general population.1–3
The definition of nonalcoholic fatty liver disease (NAFLD) has been used for decades, excluding viral hepatitis, autoimmune diseases, and heavy drinking as the underlying cause of the disease. However, this definition does not accurately reflect the contribution of systemic metabolic dysregulation to liver diseases. To address this, an international panel of experts proposed a new definition in early 2020, called metabolic dysfunction-associated fatty liver disease (MAFLD).4 The new definition emphasizes the importance of metabolic abnormalities in the development and progression of the disease. The diagnostic criteria for MAFLD are hepatic steatosis of ≥5%5 and the presence of one of the following three conditions: type 2 diabetes mellitus (T2DM), overweight/obesity by body mass index (BMI) classifications, and metabolic risk abnormalities (Box 1).4
 |
Box 1 Metabolic Risk Abnormalities - 2 Out of 7 |
The new definition is not only a name change but also highlights the association of this common liver disease with metabolic risk and coexisting extrahepatic diseases.6 NAFLD is known to be a significant risk factor for cardiovascular disease (CVD), which is the leading cause of death in patients with NAFLD.7 There are several common risk factors shared by NAFLD and CVD, such as hypertension, T2DM, lipid abnormality, obesity, and smoking. Recently, the American Heart Association has recognized NAFLD as an underappreciated and independent risk factor for CVD.8 However, the relationship between the newly redefined MAFLD and CVD has not been well investigated.
Liver fibrosis is a progressive condition that is associated with both NAFLD and MAFLD. Recent evidence indicates that liver fibrosis severity is related to an increased risk of fatal and non-fatal CVD events.9 Several mechanisms contribute in liver fibrosis to CVD risk, such as hepatic insulin resistance, systemic low-grade inflammation, adhesion molecules, and endothelial dysfunction.10 Although liver biopsy remains the gold standard for diagnosing liver fibrosis, several noninvasive liver fibrosis scores have been developed, such as the fibrosis 4 (FIB-4) score,11 nonalcoholic fatty liver disease fibrosis score (NFS),12 and aspartate aminotransferase to platelet ratio index (APRI),13 which have been used to evaluate the degree of liver fibrosis. Studies have shown that liver fibrosis scores can predict the prognosis of CAD in patients with NAFLD.14–16 We hypothesized that liver fibrosis scores could serve as feasible markers for assessing cardiovascular risk. In this cross-sectional study, we aimed to evaluate the association between liver fibrosis scores (FIB-4, NFS, and APRI) and CAD severity in MAFLD patients.
Methods
Study Population
We conducted a retrospective cross-sectional study of patients hospitalized at the Second Hospital of Dalian Medical University between January 2018 and December 2021. We included patients who met the diagnostic criteria for MAFLD, and assessed their degree of hepatic steatosis using ultrasonography. Among these patients, we included 1568 who underwent a coronary computed tomography angiography (CCTA) scan due to suspicion of CAD or for health checkups. We excluded patients who had pre-existing CAD or other severe diseases, including (1) previous history of CAD, structural heart disease, and heart failure; (2) severe hepatic or renal insufficiency; (3) hematological disease; (4) acute or chronic infectious disease; or (5) insufficient medical records. Finally, we analyzed 1346 participants in this study. All subjects enrolled in the study gave informed consent in writing. Our study complied with the Declaration of Helsinki and was approved by the local ethics committee of the Second Hospital of the Dalian Medical University.
Assessment
Professional clinicians collected clinical data, such as age, sex, hypertension, T2DM, and CAD. Weight and height were measured using a digital scale on the day of admission, and BMI was calculated as weight in kilograms divided by height in meters squared. Blood pressure was measured in the right arm after 20 minutes in the seated position using an electronic sphygmomanometer. Biochemical parameters were measured by automatic biochemical analyzer (Siemens), including complete blood counts, lipid profiles (total cholesterol, triglyceride (TG), high-density lipoprotein cholesterol (HDL-C), and low-density lipoprotein cholesterol (LDL-C)), and aspartate aminotransferase (AST), alanine aminotransferase (ALT), fasting plasma glucose, glycosylated hemoglobin (HbA1c), uric acid (UA), and creatinine levels, were measured after overnight fasting blood tests. The estimated glomerular filtration rate (eGFR) was calculated according to the Modification of Diet in Renal Disease equation. The severity of hepatic steatosis was determined by ultrasonography.
We used the following formula to calculate NAFLD fibrosis scores, including the FIB-4 score, NFS, and APRI:13,17 FIB-4= age (years)×AST (U/L)/platelet count (×109/L)×[square root of ALT(U/L)]; NFS=−1.675+0.037×age(years)+0.094×BMI(kg/m2)+1.13×impaired fasting glucose/diabetes (yes=1, no=0)+0.99×AST/ALT ratio-0.013×platelet(×109/L)-0.66×albumin (g/dL); APRI=[AST(U/L)/upper normal limit of AST(U/L)]/platelet count (× 109/L) × 100.
Definitions
The criterion for MAFLD utilizes the same standard for hepatic steatosis evidence as NAFLD. However, metabolic dysfunction factors must also be considered during the diagnosis. This requires meeting at least one of the following three criteria: T2DM, overweight/obesity by BMI, or two or more metabolic risk abnormalities, as listed in Box 1.4
Abdominal Ultrasonography
Abdominal ultrasonography was performed using LOGIQ 9 (GE Healthcare) scanner equipped with a 2.5–4.0 MHz linear matrix transducer by experienced radiologists at the Second Hospital of Dalian Medical University. They were blinded to the clinical and laboratory data. Hepatic steatosis was diagnosed by the following criteria: (1) parenchymal brightness; (2) liver to kidney contrast; (3) deep beam attenuation; and (4) vessel blurring.
Coronary Computed Tomography Angiography
We performed CCTA using a 256-multislice scanner (Philips Healthcare) in patients hospitalized at the Second Hospital of Dalian Medical University. In addition to evaluating the degree of coronary artery stenosis, we also calculated coronary artery calcium (CAC) scores using the method described by Agatston et al.18 Three experienced physicians with at least five years of experience in cardiac CT read all images.
CAD severity was assessed based on CCTA imaging and CAC scores. CAD was defined as > 50% degree of coronary artery stenosis. Therefore, we divided the participants into three groups based on the degree of coronary artery stenosis: CAD (≥50%), non-obstructive (1–49%), and normal (no stenosis).
Statistical Analysis
We used the Statistical Package for the Social Sciences version 27.0 to perform all statistical analyses. Continuous variables were presented as mean ± standard deviation or median (Q1–Q3 quartiles), while categorical variables were summarized as frequencies and percentages. For normally distributed continuous variables, we compared the groups using a one-way analysis of variance with the Scheffe post-hoc test. For non-normally distributed continuous variables, we compared the groups using the Mann–Whitney U-test. We analyzed categorical variables using the chi-square test. We used Pearson or Spearman correlation analysis to assess the correlation of liver fibrosis scores with clinical parameters.
To evaluate the association between clinical characteristics and CAD, we used multivariate binary logistic regression analysis. We performed univariate and multivariate binary logistic regression analyses to identify the risk factors for CAD. In the multivariate analysis, we included statistically significant factors (p<0.05) and probably associated characteristics based on clinical experience as covariates. In the multivariable regression model, we adjusted the liver fibrosis scores for sex (model 1) and progressively added other statistically significant covariates (model 2 and model 3). Statistical significance was defined as p<0.05.
Results
Baseline Characteristics
Table 1 displays the baseline characteristics of the 1346 participants, with a mean age of 58.4± 11.2 years. Out of the participants, 662 were male (49.2%). Patients with CAD demonstrated significantly higher age, systolic pressure, fasting glucose, glycosylated hemoglobin, creatinine, FIB-4 score, NFS, CAC scores, percentage of T2DM, and carotid atherosclerosis compared to the normal and non-obstructive groups (p<0.05). However, no significant differences were observed in the BMI, diastolic pressure, platelet count, UA, AST, TB, TG, HDL-C, LDL-C, apolipoprotein B (Apo B), and APRI.
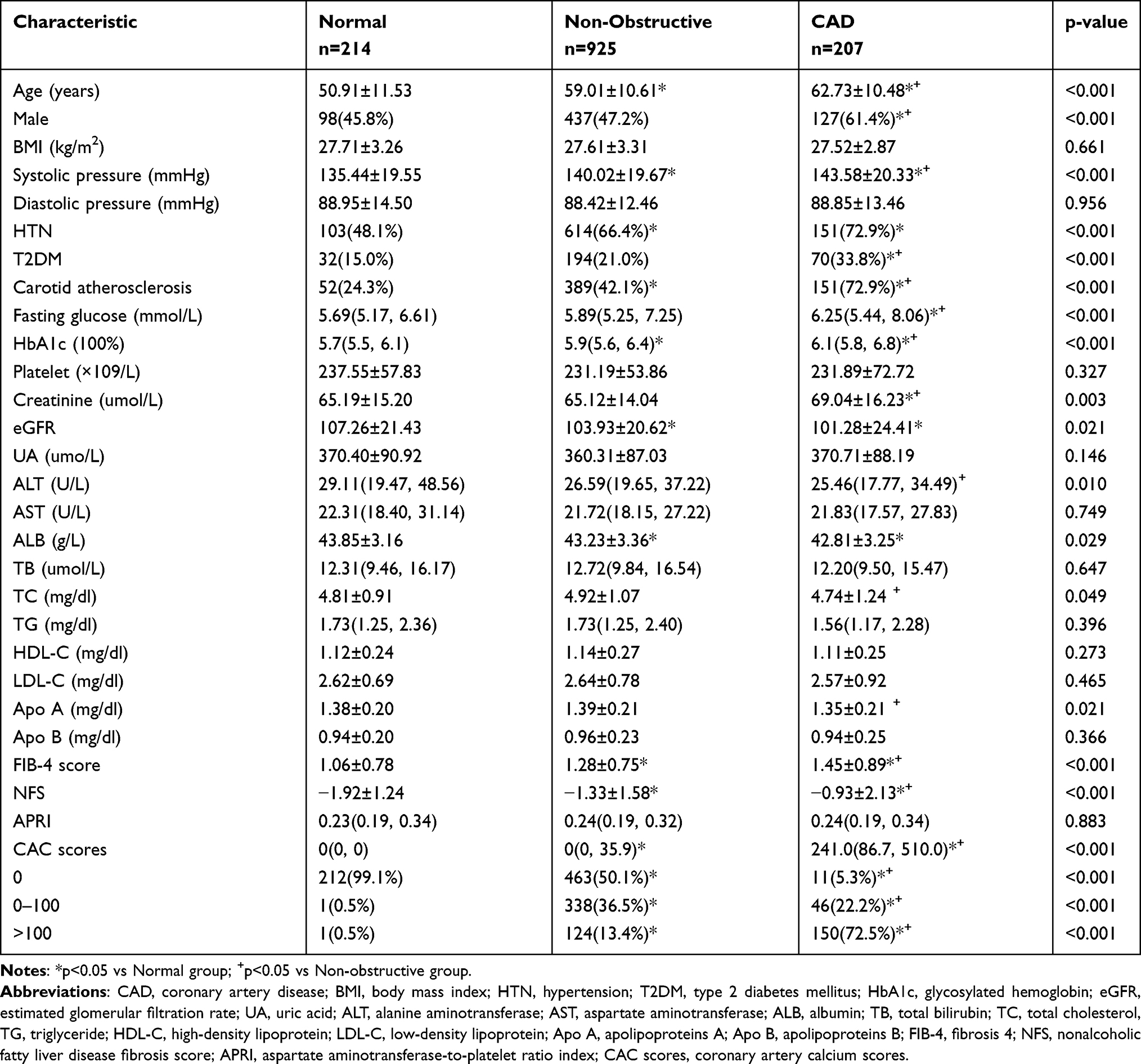 |
Table 1 Baseline Characteristics of the Participants |
Sub-Analysis of Liver Fibrosis Risk and the Presence of CAD in MAFLD Patients
To analyze the correlation between liver fibrosis risk and the presence of CAD, we calculated the FIB-4 score with cut-offs of 1.30 and 2.67 for the low-, intermediate-, and high-risk categories, respectively. Similarly, the cutoff values for NFS were −1.455 and 0.676, respectively. Figures 1 and 2 displays the percentage of liver fibrosis risk divided by the FIB-4 score and NFS in the normal, non-obstructive, and CAD groups. The percentages of high FIB-4 score and NFS were significantly higher in the CAD group than in the other two groups. Statistical differences were observed between the groups, and statistical comparisons were performed using the Chi-square test.
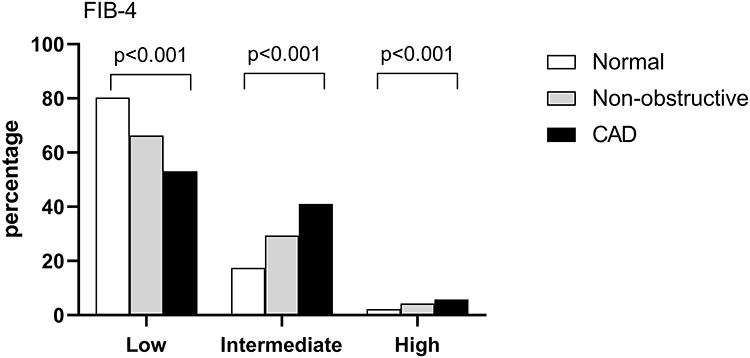 |
Figure 1 The percentage of liver fibrosis risk divided by the FIB-4 score in the normal, non-obstructive, and CAD groups. The percentage of high FIB-4 score were significantly higher in the CAD group than in the other two groups (p<0.01). Abbreviations: FIB-4, fibrosis 4; CAD, coronary artery disease. |
 |
Figure 2 The percentage of liver fibrosis risk divided by the NFS in the normal, non-obstructive, and CAD groups. The percentage of high NFS were significantly higher in the CAD group than in the other two groups (p<0.01). Abbreviations: NFS, nonalcoholic fatty liver disease fibrosis score; CAD, coronary artery disease. |
Factors Associated with CAD in MAFLD Patients
Table 2 summarizes the results of logistic regression analysis studying the association of CAD with clinical parameters. The univariate binary logistic regression analysis identified 14 factors that were significantly associated with CAD. Including these factors, the multivariate binary logistic regression analysis revealed that the presence of carotid atherosclerosis, creatinine, and CAC scores were significant factors for predicting CAD (p<0.001, p=0.010, and p<0.001, respectively) (Table 2).
 |
Table 2 Factors Associated with CAD in Subjects with MAFLD: Logistic Regression |
Associations of Noninvasive Fibrosis Scores with CAD in Subjects with MAFLD
To assess the association between NFS, FIB-4 score, and CAD, a multivariate analysis adjusted for potential confounders was subsequently performed. The FIB-4 score (OR 1.345, 95% CI 1.142–1.583) and NFS (OR 1.191, 95% CI 1.080–1.313) were independently associated with CAD in the base model. In model 1, which was adjusted for sex, the FIB-4 score and NFS were significant predictive factors for CAD. In addition, adjustments for the presence of hypertension, DM, and carotid atherosclerosis, total cholesterol, creatinine, FIB-4 score, and NFS were also significant predictive factors for CAD (model 2 and model 3) (Table 3). Unlike the other two noninvasive fibrosis markers, the APRI was not a significant factor for CAD in each model.
 |
Table 3 Associations of Noninvasive Fibrosis Scores with CAD in Subjects with MAFLD: Logistic Regression |
Correlation of Liver Fibrosis Scores with Clinical Parameters
In bivariate correlation analysis (Pearson or Spearman correlation) performed on the whole population, the FIB-4 score and NFS were inversely correlated with diastolic pressure, TC, TG, LDL-C, and directly correlated with CAC scores (Table 4).
 |
Table 4 Correlation of Liver Fibrosis Scores with Clinical Parameters: Correlation Analysis |
Discussion
The primary finding of our study was a significant positive correlation between FIB-4 score and NFS and CAD severity in patients with MAFLD. Among the MAFLD patients enrolled in this study, those with combined CAD had a significantly higher risk of liver fibrosis, as calculated using the FIB-4 score and NFS. Additionally, we found an association between the FIB-4 score and NFS and several clinical parameters, particularly CAC scores, which are recognized as essential predictors of CAD prognosis. Furthermore, even after adjusting for sex and other metabolic variables, the risk of CAD was independently associated with the FIB-4 score and NFS. Therefore, non-invasive liver fibrosis scores, such as the FIB-4 score and NFS, can be used to assess the risk of CAD in patients with MAFLD.
The relationship between fatty liver disease and cardiovascular disease has attracted considerable attention globally due to the increasing number of patients with fatty liver disease. There is growing evidence that NAFLD is a multi-system disease that increases the risk of early carotid atherosclerosis, cardiovascular disease, chronic kidney disease, and T2DM.7,19,20 Targher et al suggested that NAFLD is strongly associated with early carotid atherosclerosis, independent of classical risk factors such as insulin resistance.21 A retrospective observational study of a nationwide population-based cohort in Sweden conducted by Shang et al found that NAFLD was associated with a higher risk of nonfatal cardiovascular disease, and NAFLD patients had a lower life expectancy than the general population.22 Alon L et al also observed similar results, where the risk of myocardial infarction, ischemic stroke, atrial fibrillation, and heart failure increased in patients with NAFLD.23
Although the underlying mechanism by which fatty liver disease increases the risk of cardiovascular disease remains unclear, several possibilities have been suggested. First, impaired endothelial dysfunction is considered to be the early stage of atherosclerosis,24 and hence is crucial in CVD development. This pathophysiological process is triggered by oxidative stress and chronic inflammation, which play an important role in fatty liver disease progression.25–27 Therefore, endothelial dysfunction is considered a link between fatty liver disease and CVD risk. Second, the liver plays a central role in lipid and glucose metabolisms.28 Fatty liver disease is associated with abnormal lipid metabolism, increased levels of TG and LDL-C, and decreased levels of HDL-C, which have been proven to be risk factors for CVD. Diabetes mellitus and insulin resistance are also recognized as basic components of cardiometabolic diseases. Patients with fatty liver disease had a higher prevalence of diabetes and dyslipidemia, which is consistent with the results of our study. Fatty liver disease may be linked to CVD because they share common metabolic dysfunction.29
Nonalcoholic steatohepatitis (NASH) is a progressive form of NAFLD characterized by liver damage and fibrosis. The incidence of progression of NASH was > 20%.30 Previous studies have shown that NASH and CAD share many pathophysiological mechanisms, including endothelial dysfunction, oxidative stress, lipid metabolism, and chronic inflammation.31 The progression of both liver fibrosis and arteriosclerosis may be induced by these common mechanisms.32 Thus, CAD and liver fatty disease are the clinical consequences of metabolic disorders in different organs. Various biomarkers that assess liver fibrosis are considered useful for predicting the risk of CAD. Although liver biopsy remains the gold standard for assessing the fibrosis stage, non-invasive fibrosis scoring systems, including the FIB-4 score, NFS, and APRI, are widely used for their non-invasiveness.
Non-invasive liver fibrosis scores have also recently been suggested to have a predictive value for adverse outcomes in patients with cardiovascular diseases.33 For example, Liu et al found that high liver fibrosis scores might be useful for predicting adverse prognosis in patients with CAD following percutaneous coronary intervention (PCI).34 In a cohort of 5143 patients with CAD, Jin et al suggested that the FIB-4 score and NFS were significantly related to CAD severity, coronary artery calcium (CAC) scores, and cardiovascular events.14 Chen et al reported similar results; higher liver fibrosis scores were associated with increased risks of all-cause and cardiovascular mortality among patients with CAD. In addition, in other groups, such as T2DM, subclinical atherosclerosis, and NAFLD, non-invasive liver fibrosis scores have also been shown to have predictive and diagnostic values for CAD.35–37 Our study revealed that CAD severity was associated with FIB-4 score and NFS, even after adjusting for sex and relatively well-known cardiovascular risk factors.
Previous cross-sectional studies and meta-analyses have reported that CAC scores reflect CAD severity and are associated with adverse cardiovascular outcomes.38–40 Park et al also reported a significant association between liver fibrosis and coronary artery calcification development.15 Therefore, we conducted further analysis and found that FIB-4 score and NFS were directly correlated with CAC scores, consistent with a previous study.
Notably, previous studies have been conducted in the field of NAFLD. Since the introduction of the term “metabolic dysfunction-associated fatty liver disease”, there have been key areas in which the superiority of MAFLD over traditional NAFLD terminology has been demonstrated.41–43 The application of the new term MAFLD has shown advantages in assessing the risk of liver and extrahepatic mortality, as well as identifying high-risk individuals.44–46 Our study extended these previous observations to a new concept and discovered significant results regarding the predictive value of non-invasive liver fibrosis scores for CAD in patients with MAFLD. Risk screening for this population is necessary, considering the risk of extrahepatic comorbidity in MAFLD. Furthermore, we found that the percentage of patients with CAD in MAFLD was higher, especially those with a high liver fibrosis risk assessed using non-invasive liver fibrosis scores, which is consistent with our study. This novel finding suggests that calculating noninvasive liver fibrosis scores among MAFLD patients is necessary to identify individuals at a high risk of CAD. Although routine screening for CAD in patients with pre-existing MAFLD is not currently recommended, CCTA examination is a good recommendation for patients with a high risk of liver fibrosis, according to our study.
Several potential limitations existed in our present study. First, it was a retrospective cross-sectional study with a relatively small sample size, and the results should not be used to draw causal conclusions. Second, we used ultrasonography and noninvasive liver fibrosis scores to diagnose and stratify the severity of MAFLD instead of liver biopsy, which is regarded as the “gold standard.” Third, a follow-up was not performed in our study. Further long-term follow-up studies are warranted to evaluate CAD progression and cardiovascular events.
Conclusion
In conclusion, our study suggests that noninvasive liver fibrosis scores (FIB-4 score and NFS) are significantly related to the severity of CAD and CAC scores in patients with MAFLD. This noninvasive index may be a useful risk assessment tool for CAD and can be widely used owing to its non-invasiveness and convenience. Therefore, subjects with a high liver fibrosis risk in MAFLD may benefit from screening for coronary artery disease at an early stage.
Abbreviations
ALT, alanine aminotransferase; Apo B, apolipoprotein B; APRI, aminotransferase to platelet ratio index; AST, aspartate aminotransferase; BMI, body mass index; CAC, coronary artery calcium; CAD, coronary artery disease; CCTA, coronary computed tomography angiography; CVD, cardiovascular disease; eGFR, estimated glomerular filtration rate; FIB-4, fibrosis 4; HbA1c, glycosylated hemoglobin; HDL-C, high-density lipoprotein cholesterol; LDL-C, low-density lipoprotein cholesterol; NAFLD, nonalcoholic fatty liver disease; NASH, nonalcoholic steatohepatitis; NFS, nonalcoholic fatty liver disease fibrosis score; MAFLD, metabolic dysfunction-associated fatty liver disease; PCI, percutaneous coronary intervention; T2DM, type 2 diabetes mellitus; TB, total bilirubin; TG, triglyceride; UA, uric acid.
Funding
There is no funding to report.
Disclosure
Chuan Lu and Yan Chen are co-first authors for this study. The authors declare that there are no conflicts of interest in this work.
References
1. Sung KC, Yoo TK, Lee MY, Byrne CD, Zheng MH, Targher G. Comparative associations of nonalcoholic fatty liver disease and metabolic dysfunction-associated fatty liver disease with coronary artery calcification: a cross-sectional and longitudinal cohort study. Arterioscler Thromb Vasc Biol. 2023;43(3):482–491. doi:10.1161/ATVBAHA.122.318661
2. Younossi Z, Anstee QM, Marietti M, et al. Global burden of NAFLD and NASH: trends, predictions, risk factors and prevention. Nat Rev Gastroenterol Hepatol. 2018;15(1):11–20. doi:10.1038/nrgastro.2017.109
3. Chan KE, Koh T, Tang A, et al. Global prevalence and clinical characteristics of metabolic-associated fatty liver disease: a meta-analysis and systematic review of 10 739 607 individuals. J Clin Endocrinol Metab. 2022;107(9):2691–2700. doi:10.1210/clinem/dgac321
4. Eslam M, Newsome PN, Sarin SK, et al. A new definition for metabolic dysfunction-associated fatty liver disease: an international expert consensus statement. J Hepatol. 2020;73(1):202–209. doi:10.1016/j.jhep.2020.03.039
5. Chalasani N, Younossi Z, Lavine JE, et al. The diagnosis and management of nonalcoholic fatty liver disease: practice guidance from the American Association for the Study of Liver Diseases. Hepatology. 2018;67(1):328–357. doi:10.1002/hep.29367
6. Eslam M, Sanyal AJ, George J. MAFLD: a consensus-driven proposed nomenclature for metabolic associated fatty liver disease. Gastroenterology. 2020;158(7):1999–2014.e1. doi:10.1053/j.gastro.2019.11.312
7. Targher G, Byrne CD, Tilg H. NAFLD and increased risk of cardiovascular disease: clinical associations, pathophysiological mechanisms and pharmacological implications. Gut. 2020;69(9):1691–1705. doi:10.1136/gutjnl-2020-320622
8. Duell PB, Welty FK, Miller M, et al. Nonalcoholic fatty liver disease and cardiovascular risk: a Scientific Statement From the American Heart Association. Arterioscler Thromb Vasc Biol. 2022;42(6):e168–e185. doi:10.1161/ATV.0000000000000153
9. Mantovani A, Csermely A, Petracca G, et al. Non-alcoholic fatty liver disease and risk of fatal and non-fatal cardiovascular events: an updated systematic review and meta-analysis. Lancet Gastroenterol Hepatol. 2021;6(11):903–913. doi:10.1016/S2468-1253(21)00308-3
10. Gutiérrez-Cuevas J, Santos A, Armendariz-Borunda J. Pathophysiological molecular mechanisms of obesity: a link between MAFLD and NASH with cardiovascular diseases. Int J Mol Sci. 2021;22(21):11629. doi:10.3390/ijms222111629
11. Angulo P, Hui JM, Marchesini G, et al. The NAFLD fibrosis score: a noninvasive system that identifies liver fibrosis in patients with NAFLD. Hepatology. 2007;45(4):846–854. doi:10.1002/hep.21496
12. Sterling RK, Lissen E, Clumeck N, et al. Development of a simple noninvasive index to predict significant fibrosis in patients with HIV/HCV coinfection. Hepatology. 2006;43(6):1317–1325. doi:10.1002/hep.21178
13. Wai CT, Greenson JK, Fontana RJ, et al. A simple noninvasive index can predict both significant fibrosis and cirrhosis in patients with chronic hepatitis C. Hepatology. 2003;38(2):518–526. doi:10.1053/jhep.2003.50346
14. Jin JL, Zhang HW, Cao YX, et al. Liver fibrosis scores and coronary atherosclerosis: novel findings in patients with stable coronary artery disease. Hepatol Int. 2021;15(2):413–423. doi:10.1007/s12072-021-10167-w
15. Park HE, Kwak MS, Kim D, Kim MK, Cha MJ, Choi SY. Nonalcoholic fatty liver disease is associated with coronary artery calcification development: a longitudinal study. J Clin Endocrinol Metab. 2016;101(8):3134–3143. doi:10.1210/jc.2016-1525
16. Chen Q, Li Q, Li D, et al. Association between liver fibrosis scores and the risk of mortality among patients with coronary artery disease. Atherosclerosis. 2020;299:45–52. doi:10.1016/j.atherosclerosis.2020.03.010
17. Tokushige K, Ikejima K, Ono M, et al. Evidence-based clinical practice guidelines for nonalcoholic fatty liver disease/nonalcoholic steatohepatitis 2020. J Gastroenterol. 2021;56(11):951–963. doi:10.1007/s00535-021-01796-x
18. Agatston AS, Janowitz WR, Hildner FJ, Zusmer NR, Viamonte M
19. Byrne CD, Targher G. NAFLD: a multisystem disease. J Hepatol. 2015;62(1 Suppl):S47–64. doi:10.1016/j.jhep.2014.12.012
20. Bonora E, Targher G. Increased risk of cardiovascular disease and chronic kidney disease in NAFLD. Nat Rev Gastroenterol Hepatol. 2012;9(7):372–381. doi:10.1038/nrgastro.2012.79
21. Targher G, Bertolini L, Padovani R, et al. Relations between carotid artery wall thickness and liver histology in subjects with nonalcoholic fatty liver disease. Diabetes Care. 2006;29(6):1325–1330. doi:10.2337/dc06-0135
22. Shang Y, Nasr P, Widman L, Hagström H. Risk of cardiovascular disease and loss in life expectancy in NAFLD. Hepatology. 2022;76(5):1495–1505. doi:10.1002/hep.32519
23. Alon L, Corica B, Raparelli V, et al. Risk of cardiovascular events in patients with non-alcoholic fatty liver disease: a systematic review and meta-analysis. Eur J Prev Cardiol. 2022;29(6):938–946.
24. Vanhoutte PM. Endothelial dysfunction: the first step toward coronary arteriosclerosis. Circ J. 2009;73(4):595–601. doi:10.1253/circj.CJ-08-1169
25. Federico A, Dallio M, Masarone M, Persico M, Loguercio C. The epidemiology of non-alcoholic fatty liver disease and its connection with cardiovascular disease: role of endothelial dysfunction. Eur Rev Med Pharmacol Sci. 2016;20(22):4731–4741.
26. Francque SM, van der Graaff D, Kwanten WJ. Non-alcoholic fatty liver disease and cardiovascular risk: pathophysiological mechanisms and implications. J Hepatol. 2016;65(2):425–443. doi:10.1016/j.jhep.2016.04.005
27. Targher G, Day CP, Bonora E. Risk of cardiovascular disease in patients with nonalcoholic fatty liver disease. N Engl J Med. 2010;363(14):1341–1350. doi:10.1056/NEJMra0912063
28. Neuschwander-Tetri BA. Hepatic lipotoxicity and the pathogenesis of nonalcoholic steatohepatitis: the central role of nontriglyceride fatty acid metabolites. Hepatology. 2010;52(2):774–788. doi:10.1002/hep.23719
29. Katakami N. Mechanism of development of atherosclerosis and cardiovascular disease in diabetes mellitus. J Atheroscler Thromb. 2018;25(1):27–39. doi:10.5551/jat.RV17014
30. Song DS, Chang UI, Kang SG, Song SW, Yang JM. Noninvasive serum fibrosis markers are associated with coronary artery calcification in patients with nonalcoholic fatty liver disease. Gut Liver. 2019;13(6):658–668. doi:10.5009/gnl18439
31. Ismaiel A, Dumitraşcu DL. Cardiovascular risk in fatty liver disease: the liver-heart axis-literature review. Front Med (Lausanne). 2019;6:202. doi:10.3389/fmed.2019.00202
32. Turan Y. The nonalcoholic fatty liver disease fibrosis score is related to epicardial fat thickness and complexity of coronary artery disease. Angiology. 2020;71(1):77–82. doi:10.1177/0003319719844933
33. Puchner SB, Lu MT, Mayrhofer T, et al. High-risk coronary plaque at coronary CT angiography is associated with nonalcoholic fatty liver disease, independent of coronary plaque and stenosis burden: results from the ROMICAT II trial. Radiology. 2015;274(3):693–701. doi:10.1148/radiol.14140933
34. Liu HH, Cao YX, Jin JL, et al. Liver fibrosis scoring systems as novel tools for predicting cardiovascular outcomes in patients following elective percutaneous coronary intervention. J Am Heart Assoc. 2021;10(3):e018869. doi:10.1161/JAHA.120.018869
35. Wang C, Cai Z, Deng X, et al. Association of hepatic steatosis index and fatty liver index with carotid atherosclerosis in type 2 diabetes. Int J Med Sci. 2021;18(14):3280–3289. doi:10.7150/ijms.62010
36. Mangla N, Ajmera VH, Caussy C, et al. Liver stiffness severity is associated with increased cardiovascular risk in patients with type 2 diabetes. Clin Gastroenterol Hepatol. 2020;18(3):744–746.e1. doi:10.1016/j.cgh.2019.05.003
37. Lee J, Kim HS, Cho YK, et al. Association between noninvasive assessment of liver fibrosis and coronary artery calcification progression in patients with nonalcoholic fatty liver disease. Sci Rep. 2020;10(1):18323. doi:10.1038/s41598-020-75266-4
38. Maeda D, Kanzaki Y, Sakane K, et al. Prognostic value of the liver fibrosis marker fibrosis-5 index in patients with acute heart failure. ESC Heart Fail. 2022;9(2):1380–1387. doi:10.1002/ehf2.13829
39. Kramer CK, Zinman B, Gross JL, et al. Coronary artery calcium score prediction of all cause mortality and cardiovascular events in people with type 2 diabetes: systematic review and meta-analysis. BMJ. 2013;346:f1654. doi:10.1136/bmj.f1654
40. Otton JM, Yu CY, McCrohon J, Sammel N, Feneley M. Accuracy and clinical outcomes of computed tomography coronary angiography in the presence of a high coronary calcium score. Heart Lung Circ. 2013;22(12):980–986. doi:10.1016/j.hlc.2013.05.647
41. Gofton C, Upendran Y, Zheng MH, George J. MAFLD: how is it different from NAFLD. Clin Mol Hepatol. 2023;29(Suppl):S17–S31. doi:10.3350/cmh.2022.0367
42. Chun HS, Lee M, Lee JS, et al. Metabolic dysfunction associated fatty liver disease identifies subjects with cardiovascular risk better than non-alcoholic fatty liver disease. Liver Int. 2023;43(3):608–625. doi:10.1111/liv.15508
43. Kim H, Lee CJ, Ahn SH, et al. MAFLD predicts the risk of cardiovascular disease better than NAFLD in asymptomatic subjects with health check-ups. Dig Dis Sci. 2022;67(10):4919–4928. doi:10.1007/s10620-022-07508-6
44. Liu HH, Cao YX, Jin JL, et al. Metabolic-associated fatty liver disease and major adverse cardiac events in patients with chronic coronary syndrome: a matched case-control study. Hepatol Int. 2021;15(6):1337–1346. doi:10.1007/s12072-021-10252-0
45. Lee H, Lim TS, Kim SU, Kim HC. Long-term cardiovascular outcomes differ across metabolic dysfunction-associated fatty liver disease subtypes among middle-aged population. Hepatol Int. 2022;16(6):1308–1317. doi:10.1007/s12072-022-10407-7
46. Chen X, Chen Z, Jiang L, Huang J, Zhu Y, Lin S. MAFLD is associated with increased all-cause mortality in low cardiovascular-risk individuals but not in intermediate to high-risk individuals. Nutr Metab Cardiovasc Dis. 2023;33(2):376–384. doi:10.1016/j.numecd.2022.11.007
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.