")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Liver Cirrhosis of Unknown Etiology and Its Predictors in Eastern Ethiopia
Authors Mekuria AN , Nedi T , Gong YY, Abula T, Engidawork E
Received 30 September 2023
Accepted for publication 18 January 2024
Published 22 January 2024 Volume 2024:17 Pages 225—232
DOI https://doi.org/10.2147/RMHP.S425954
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Haiyan Qu
Abraham Nigussie Mekuria,1 Teshome Nedi,1 Yun Yun Gong,2 Teferra Abula,1 Ephrem Engidawork1
1Department of Pharmacology and Clinical Pharmacy, School of Pharmacy, College of Health Sciences, Addis Ababa University, Addis Ababa, Ethiopia; 2School of Food Science and Nutrition, University of Leeds, Leeds, UK
Correspondence: Ephrem Engidawork; Teferra Abula, Email [email protected]; [email protected]
Background: The global burden of liver cirrhosis is increasing, with 2.1 million incident cases and nearly 1.5 million deaths in 2019. Despite the enormous progress in our understanding of the etiology of liver cirrhosis, significant cases of the disease have been reported in Eastern Ethiopia due to unidentified causes. Hence, this study aimed to identify predictors of liver cirrhosis of unknown etiology in Eastern Ethiopia.
Methods: A score of 7 out of 11 possible points on the ultrasound-based cirrhosis scale was used as a diagnostic criterion to include 127 liver cirrhosis patients. The study participants’ demographic, dietary, lifestyle, and clinical data were gathered using a structured questionnaire and standardized reporting forms. The associations between the outcome (known and unknown etiology) and independent variables were modeled using binary logistic regression analysis.
Results: The etiology of liver cirrhosis was known in only 23% of patients and attributed to hepatitis B virus (21%), hepatitis C virus (0.8%), and alcohol abuse (0.8%). Sorghum consumption as a staple food (adjusted odds ratio (AOR) =3.8; 95% CI: 1.2, 12.5), splenomegaly (AOR = 4.0; 95% CI: 1.1, 14.4), and a family history of liver disease (AOR = 0.24; 95% CI: 0.06, 0.91) were significantly associated with liver cirrhosis of unknown etiology.
Conclusion: Sorghum consumption was found to be the determinant factor of liver cirrhosis of unknown etiology, suggesting it as a possible source of exposure to aflatoxin B1.
Keywords: liver cirrhosis, unknown etiology, sorghum, splenomegaly, family history of liver disease, Ethiopia
Introduction
Liver cirrhosis, known to be a well-established risk factor for hepatocellular carcinoma (HCC), represents a late stage of progressive hepatic fibrosis characterized by distortion of the hepatic architecture and formation of regenerative nodules.1 Globally, the number of incident cases of liver cirrhosis reached 2.1 million and contributed to nearly 1.5 million deaths in 2019.2
Numerous etiological factors, the prevalence of which varies geographically, have been linked to liver cirrhosis.3 Among the major causes, alcoholic liver disease, hepatitis C virus (HCV) infection, and non-alcoholic fatty liver disease are the most common causes in Western and industrialized countries, whereas chronic hepatitis B virus (HBV) infection is the main etiologic factor in Asia and Africa.4,5 In sub-Saharan Africa, 69% of liver cirrhosis cases were attributed to HBV, HCV, and alcohol consumption. However, the etiology was unknown in the remaining percentage of cases.4 Similarly, a systematic review and meta-analysis study revealed that HBV and HCV infections, as well as alcohol consumption, are the three most important causes of liver cirrhosis in Ethiopia. Nevertheless, the cause is yet to be identified in 45% of the cases.6
In Eastern Ethiopia, despite the high burden of liver cirrhosis of unknown etiology, fewer efforts have been made to explore its potential determinants. In this regard, our recent case‒control study found aflatoxin B1 (AFB1) exposure as a potential missing etiologic factor of liver cirrhosis in Eastern Ethiopia, where significant cases of the disease were cryptogenic.7 Thus, it is imperative to explore the potential predictive factors for the unknown etiology of liver cirrhosis to obtain clues for further missing etiologies and for potential sources of exposure to AFB1 and its predictors. Hence, this study aimed to identify the possible sociodemographic, dietary, lifestyle, and clinical factors associated with the unknown etiology of liver cirrhosis in Eastern Ethiopia.
Materials and Methods
Study Setting and Subjects
This is part of a study conducted in a tertiary hospital in Harar, Eastern Ethiopia, to explore risk factors for liver cirrhosis from 1 January 2020 to 31 July 2021.7 In short, the study included 253 controls who had no history of liver disease and 127 verified instances of hepatic cirrhosis. After explaining the study’s objectives to the participants’, written consent was obtained, and a professional interviewer completed a thorough questionnaire for each case and control. Only liver cirrhosis patients (127 cases) were included in this study to identify factors associated with the unknown etiology of liver cirrhosis in Eastern Ethiopia with a high burden of unexplained cases.
Operational Definition
Patients were screened for the presence of the most important etiologies of liver cirrhosis in Ethiopia, namely, HBV, HCV, and alcohol abuse.6 Those patients whose etiologic factor was not related to one of those mentioned etiologies were categorized as “patients with an unknown etiology of liver cirrhosis”, and vice versa.
Statistical Analysis
Percentages were used for categorical variables. Continuous variables were thought to have a nonnormal distribution and were expressed as medians (inter-quartile range (IQR)). To compare the features of patients with known and unknown etiologies of liver cirrhosis, the Mann–Whitney U-test and χ2 or Fisher exact tests were used for continuous variables and categorical variables, respectively. In the univariate analysis, variables with p<0.25 were scrutinized and fitted to multivariable analysis along with biologically relevant variables (age and gender) to identify predictive factors of unknown etiology for liver cirrhosis. Odds ratios (ORs) along with a 95% confidence interval (CI) were calculated to determine the strength of the relationships described above. The level of significance was considered at p<0.05 in the final logistic regression model. Statistical analysis was performed using Statistical Package for Social Sciences (SPSS) version 26.0.
Ethical Considerations
Ethical clearance was obtained from the Institutional Review Board of the College of Health Sciences, Addis Ababa University (Protocol No. 064/19/SOP and Reference No. CHS/RTTD/229/2020) and the National Ethical Review Committee of the Ministry of Science and Higher Education (Reference No. 04/246/680/21). This study was conducted in accordance with the Declaration of Helsinki.
Results
The etiology of liver cirrhosis was determined in 29 (23%) of the 127 patients and attributed to HBV (21%), HCV (0.8%), and alcohol abuse (0.8%).
Sociodemographic, Lifestyle and Dietary Characteristics
As shown in Table 1, 66% of the study participants were males, and the median age was 32 years (IQR: 28–45). Majority of the patients were farmers (82%), from a rural area (84%), with no formal education (80%), and had consumed sorghum (80.3%) as a staple food (Table 1). The proportion of patients with no family history of liver disease and consume staple food was significantly higher (p < 0.05) in unknown etiology than known etiology group (Table 2).
 |
Table 1 Sociodemographic Characteristics of Liver Cirrhosis Patients in Eastern Ethiopia, 2020/21 |
 |
Table 2 Lifestyle, Dietary and Other Characteristics of Liver Cirrhosis Patients in Eastern Ethiopia, 2020/21 |
Clinical and Ultrasound Findings
Almost all (97%) patients presented with abdominal distention, as shown in Table 3. Patients with unknown etiology of liver cirrhosis were more likely to present with splenomegaly than those in whom the etiology was identified. Otherwise, there were no distinguishing clinical features between the two groups. The major findings on liver ultrasound were heterogeneous liver parenchyma (87%), undulant liver surface (66.0%), spleen size index >20cm2 (87%), and ascites (96.0%). There was a significant difference (p<0.05) in terms of spleen size index between the two groups.
 |
Table 3 Clinical and Ultrasound Features of Liver Cirrhosis Patients in Eastern Ethiopia, 2020/21 |
Laboratory Findings
More or less abnormal lab findings were observed in a somewhat higher percentage of patients with known etiology than patients with unknown etiology of liver cirrhosis. However, there were no significant differences in laboratory findings between the two groups (Table 4).
 |
Table 4 Laboratory Findings of Liver Cirrhosis Patients in Eastern Ethiopia, 2020/21 |
Predictors for Unknown Etiology of Liver Cirrhosis
Staple foods, body mass index, family history of liver disease, splenomegaly, age, gender, and abnormal serum levels of albumin and creatinine were entered into the final logistic regression model. Family history of liver disease, consumption of sorghum as a staple food, and splenomegaly were found to be significantly associated with unknown etiology of liver cirrhosis (Table 5). Accordingly, patients with a family history of liver disease had a decreased odds (AOR=0.24; 95% CI: 0.06, 0.91) of developing liver cirrhosis of unknown etiology by 76% compared with those without a family history. Patients who consumed sorghum as a staple food were 3.8 times (AOR=3.8; 95% CI: 1.2, 12.5) more likely to be diagnosed with liver cirrhosis of unknown etiology. Likewise, patients with splenomegaly had 4.0 times (AOR=4.0; 95% CI: 1.1, 14.4) higher odds of having liver cirrhosis of unknown etiology than patients without splenomegaly (Table 5).
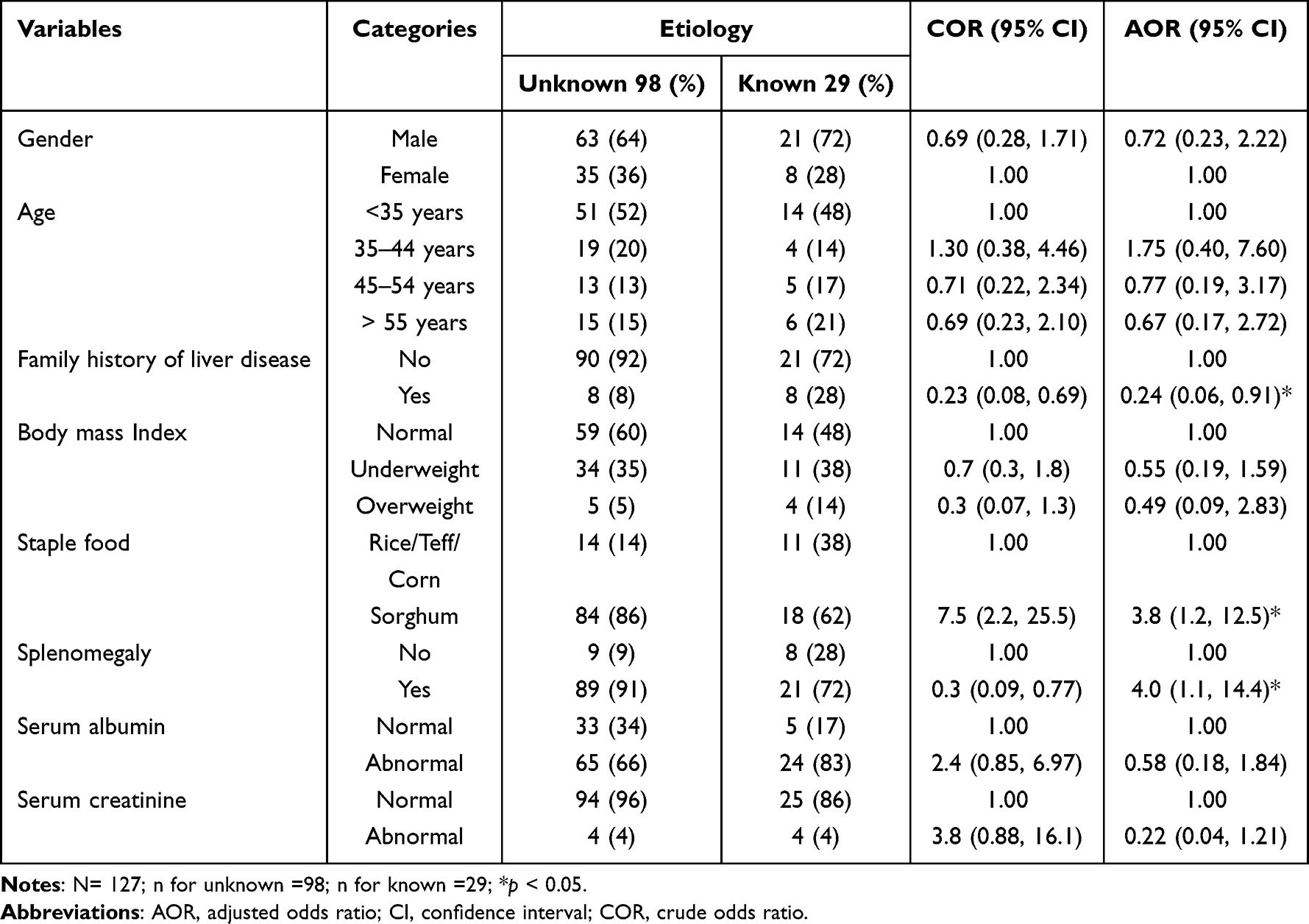 |
Table 5 Predictors of Unknown Etiology of Liver Cirrhosis in Eastern Ethiopia, 2020/21 |
Discussion
Despite the assumed heavy burden of liver cirrhosis of unknown etiology, limited data have been available on its predictors in Eastern Ethiopian populations.8,9 In this study, the magnitude of liver cirrhosis of unknown etiology was 77%, which is higher than that in a previous study performed among chronic liver disease patients in Eastern Ethiopia (55%).8 This discordance might be due to the focus of our study on the major etiologies of liver cirrhosis in Ethiopia and the difference in the prevalence of HBV infection detected in the studies (21% vs 37%). However, the prevalence of HBV infection in our study was similar to that in a study performed at Addis Ababa (20%).10 Thus, further investigation is needed to determine other risk factors that contribute to liver cirrhosis in Eastern Ethiopia.
In the current study, majority of the participants consumed sorghum as a staple food (80%), and a strong and significant association was noticed between the consumption of sorghum and liver cirrhosis of unknown etiology. It is known that sorghum flour alone or mixed with other cereals is used for making Injera, a local circular pancake used for serving a common meal known as “La fiso” in Eastern Ethiopia.11 Meanwhile, majority of the farmers in Eastern Ethiopia store sorghum grain in underground pits. These pits usually elevate grain moisture and storage temperature to levels that favor insect pests and fungi contamination, causing grain spoilage.12
In support of this, several studies performed in the area reported a high level of AFB1 in sorghum grain and sorghum Injera samples,13–17 when compared against the limits set by the East African Community (EAC) (5 µg/kg for AFB1 and 10 µg/kg for total aflatoxins).18 Accordingly, aflatoxin analysis performed on fresh or stored sorghum samples as well as sorghum injera samples collected from this region revealed AFB1 concentrations ranging from 10 to 53.3 μg/kg.15,16
The present study also revealed that patients with splenomegaly were more likely to have an unknown etiology of liver cirrhosis. Although there are no previous observational studies that reported such differences between patients with known and unknown etiology of liver cirrhosis in Ethiopia, splenomegaly has been known to be the most common sign and symptom of liver cirrhosis,19 and based on the present study, the occurrence seemed to be higher in patients with unknown etiology. Splenomegaly is known to be associated with continued exposure to environmental oxidants20–23 and parasitic diseases, including Schistosoma mansoni.24 It is generally accepted that S. mansoni infection alone does not lead to cirrhosis and is known to be characterized by periportal fibrosis associated with portal hypertension in the presence of preserved liver parenchyma and function.25 This, however, was not observed in our patients, ruling out the role of S. mansoni. A previous study performed in the same area reported toxic liver injury in patients with unknown etiology of the disease and found an association with khat consumption, a commonly used psychostimulant in the Horn of Africa, including Ethiopia.8,9 However, in our study, there was no detectable difference between patients with known and unknown etiology in terms of khat chewing habits, casting doubt on the role of khat. On the other hand, a preliminary study performed in Kenya involving school children reported a 43% increase in the prevalence of hepatomegaly or hepatosplenomegaly for each natural-log-unit increase in AFB1-albumin adduct level after adjusting for S. mansoni and Plasmodium infections.20
Patients with a family history of liver disease were less likely to be diagnosed with liver cirrhosis of unknown etiology. According to studies, various established etiologies of liver cirrhosis involve inflammation and oxidative stress as hallmarks of pathogenesis.26,27 In this regard, variations in genes involved in the antioxidant enzymes,28 DNA repair pathway,29 immunologically important signaling pathways, and other players in combating oxidative damage were identified as predisposing factors of the disease.30 Hence, patients with a family history of liver disease would have a lower likelihood of developing cryptogenic hepatic cirrhosis, which is no surprise. To the best of our knowledge, this study is the first to provide an impetus for further investigation and action on the association between dietary staple foods and the risk of cirrhosis of unknown etiology in Ethiopia, where people feed on a diet contaminated with a high burden of AFB1. However, we acknowledge that due to the inherent limitation of the study design, this study cannot establish an association or possible causality between the exposures and outcome.
Conclusions
In this study, majority of the patients with liver cirrhosis had an unknown etiology. Sorghum consumption, splenomegaly, and family history of liver disease were found to be predictors of unexplained cases of the disease. The strong association of sorghum consumption with liver cirrhosis of unknown etiology and the available evidence of its contamination with AFB1 suggest sorghum consumption as a possible source of exposure to AFB1 in Eastern Ethiopia.
Ethics Statement
Ethical clearance was obtained from the Institutional Review Board of the College of Health Sciences, Addis Ababa University (Protocol No. 064/19/SOP and Reference No. CHS/RTTD/229/2020) and the National Ethical Review Committee of the Ministry of Science and Higher Education (Reference No. 04/246/680/21). This study was conducted in accordance with the Declaration of Helsinki.
Author Contributions
All authors made a significant contribution to the work reported whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Zuñiga-Aguilar E, Ramírez-Fernández O. Fibrosis and hepatic regeneration mechanism. Transl Gastroenterol Hepatol. 2022;7:9. doi:10.21037/tgh.2020.02.21
2. Lan Y, Wang H, Weng H, et al. The burden of liver cirrhosis and underlying etiologies: results from the Global Burden of Disease Study 2019. Hepatol Commun. 2023;7(2):e0026–e0026. doi:10.1097/HC9.0000000000000026
3. Wong MCS, Huang J. The growing burden of liver cirrhosis: implications for preventive measures. Hepatol Int. 2018;12(3):201–203. doi:10.1007/s12072-018-9865-y
4. Mokdad AA, Lopez AD, Shahraz S, et al. Liver cirrhosis mortality in 187 countries between 1980 and 2010: a systematic analysis. BMC Med. 2014;12(1):145. doi:10.1186/s12916-014-0145-y
5. Zhai M, Long J, Liu S, et al. The burden of liver cirrhosis and underlying etiologies: results from the global burden of disease study 2017. Aging. 2021;13(1):279–300. doi:10.18632/aging.104127
6. Tesfaye BT, Feyissa TM, Workneh AB, et al. Chronic Liver Disease in Ethiopia with a Particular Focus on the Etiological Spectrums: a Systematic Review and Meta-Analysis of Observational Studies. Can J Gastroenterol Hepatol. 2021;2021:8740157. doi:10.1155/2021/8740157
7. Mekuria A, Xia L, Ahmed TA, et al. Contribution of Aflatoxin B1 Exposure to Liver Cirrhosis in Eastern Ethiopia: a Case-Control Study. Int J Gen Med. 2023;16:3543–3553. doi:10.2147/IJGM.S425992
8. Orlien SMS, Ismael NY, Ahmed TA, et al. Unexplained chronic liver disease in Ethiopia: a cross-sectional study. BMC Gastroenterol. 2018;18(1):27.
9. Orlien SMS, Sandven I, Berhe NB, et al. Khat chewing increases the risk for developing chronic liver disease: a hospital-based case-control study. Hepatol. 2018;68(1):248–257. doi:10.1002/hep.29809
10. Samson E, Bisrat D, Hailu D, et al. Liver Disease: a Retrospective Hospital Based Study in Addis Ababa-Ethiopia. J Spleen Liver Res. 2021;1(4):1–7. doi:10.14302/issn.2578-2371.jslr-21-3912
11. Mekbib F. Folksong based appraisal of bioecocultural heritage of sorghum (Sorghum bicolor (L.) Moench): a new approach in ethnobiology. J Ethnobiol Ethnomed. 2009;5:19. doi:10.1186/1746-4269-5-19
12. Dejene M, Yuen J, Sigvald R. Effects of storage methods, storage time and different agro-ecological zones on chemical components of stored sorghum grain in Hararghe, Ethiopia. J Stored Prod Res. 2006;42(4):445–456. doi:10.1016/j.jspr.2004.07.006
13. Chala A, Taye W, Ayalew A, et al. Multimycotoxin analysis of sorghum (Sorghum bicolor L. Moench) and finger millet (Eleusine coracana L. Garten) from Ethiopia. Food Control. 2014;45:29–35. doi:10.1016/j.foodcont.2014.04.018
14. Taye W, Ayalew A, Chala A, et al. Aflatoxin B(1) and total fumonisin contamination and their producing fungi in fresh and stored sorghum grain in East Hararghe, Ethiopia. Food Addit Contam Part B Surveill. 2016;9(4):237–245. doi:10.1080/19393210.2016.1184190
15. Marie S. Level of Aflatoxin in Sorghum Injera from Eastern Ethiopia. M.Sc. Thesis. Addis Ababa University; 2017.
16. Mamo FT, Abate BA, Tesfaye K, et al. Mycotoxins in Ethiopia: a Review on Prevalence. Economic Health Impacts Toxins. 2020;12(10):65.
17. Mohammed A, Bekeko Z, Yusufe M, et al. Fungal Species and Multi-Mycotoxin Associated with Post-Harvest Sorghum (Sorghum bicolor (L.) Moench) Grain in Eastern Ethiopia. Toxins. 2022;14(7):473. doi:10.3390/toxins14070473
18. Boni S, Beed F, Kimanya M, et al. Aflatoxin contamination in Tanzania: quantifying the problem in maize and groundnuts from rural households. World Mycotoxin J. 2021;14(4):1–12. doi:10.3920/WMJ2020.2646
19. Li L, Duan M, Chen W, et al. The spleen in liver cirrhosis: revisiting an old enemy with novel targets. J Transl Med. 2017;15(1):111. doi:10.1186/s12967-017-1214-8
20. Gong YY, Wilson S, Mwatha JK, et al. Aflatoxin exposure may contribute to chronic hepatomegaly in Kenyan school children. Environ Health Perspect. 2012;120(6):893–896. doi:10.1289/ehp.1104357
21. Makhdoumi P, Hossini H, Ashraf GM, et al. Molecular Mechanism of Aniline Induced Spleen Toxicity and Neuron Toxicity in Experimental Rat Exposure: a Review. Curr Neuropharmacol. 2019;17(3):201–213. doi:10.2174/1570159X16666180803164238
22. Benkerroum N. Chronic and Acute Toxicities of Aflatoxins: mechanisms of Action. Int J Environ Res Public Health. 2020;17(2):423. doi:10.3390/ijerph17020423
23. Sule RO, Condon L, Gomes AV. A Common Feature of Pesticides: oxidative Stress—The Role of Oxidative Stress in Pesticide-Induced Toxicity. Oxid Med Cell Longev. 2022;2022:5563759. doi:10.1155/2022/5563759
24. Cosenza-Contreras M, de Oliveira ECRA, Mattei B, et al. The Schistosomiasis SpleenOME: unveiling the Proteomic Landscape of Splenomegaly Using Label-Free Mass Spectrometry. Front Immunol. 2018;9:3137. doi:10.3389/fimmu.2018.03137
25. Santos JC, Pereira CLD, Domingues ALC, et al. Noninvasive diagnosis of periportal fibrosis in schistosomiasis mansoni: a comprehensive review. World J Hepatol. 2022;14(4):696–707. doi:10.4254/wjh.v14.i4.696
26. Seen S. Chronic liver disease and oxidative stress – a narrative review. Exp Rev Gastroenterol Hepatol. 2021;15(9):1021–1035. doi:10.1080/17474124.2021.1949289
27. Conde de la Rosa L, Goicoechea L, Torres S, et al. Role of Oxidative Stress in Liver Disorders. Livers. 2022;2(4):283–314.
28. Prysyazhnyuk V, Sydorchuk L, Sydorchuk R, et al. Glutathione-S-transferases genes-promising predictors of hepatic dysfunction. World J Hepatol. 2021;13(6):620–633. doi:10.4254/wjh.v13.i6.620
29. Rybicka M, Woziwodzka A, Sznarkowska A, et al. Liver Cirrhosis in Chronic Hepatitis B Patients Is Associated with Genetic Variations in DNA Repair Pathway Genes. Cancers (Basel). 2020;12(11):3295. doi:10.3390/cancers12113295
30. Ashouri S, Khor SS, Hitomi Y, et al. Genome-Wide Association Study for Chronic Hepatitis B Infection in the Thai Population. Front Genet. 2022;13:887121. doi:10.3389/fgene.2022.887121
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.