Back to Journals » International Journal of General Medicine » Volume 16
Lived Experience and Perceptions of Adolescents on Prevention, Causes and Consequences of Double Burden of Malnutrition in Debre Berhan City, Ethiopia: A Qualitative Study
Authors Getacher L ![]() , Wondafrash Ademe B
, Wondafrash Ademe B ![]() , Belachew T
, Belachew T
Received 23 November 2022
Accepted for publication 20 January 2023
Published 26 January 2023 Volume 2023:16 Pages 337—356
DOI https://doi.org/10.2147/IJGM.S398330
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Mihajlo Jakovljevic
Lemma Getacher,1,2 Beyene Wondafrash Ademe,2 Tefera Belachew2
1School of Public Health, Asrat Woldeyes Health Science Campus, Debre Berhan University, Debre Berhan, Ethiopia; 2Department of Nutrition and Dietetics, Faculty of Public Health, Institute of Health, Jimma University, Jimma, Ethiopia
Correspondence: Lemma Getacher, Debre Berhan University, P.O. Box: 445, Debre Berhan, Ethiopia, Email [email protected]
Background: The coexistence of undernutrition, overweight, and obesity within the same households and populations is recognized as the Double Burden of Malnutrition (DBM). A paradigm shift thinking is needed to mitigate its impact. School adolescents are the most vulnerable groups to DBM. However, lived experiences and perceptions on prevention, causes, and consequences of DBM were not well studied. Therefore, this study aims to explore the lived experiences and perceptions of adolescents about the prevention, causes, and consequences of DBM in Ethiopia.
Methods: A qualitative research method using phenomenology design was conducted among 20 purposively selected participants from private and government schools from June 3 to July 10, 2022. The further sampling process was guided by a saturation of ideas. In-depth and key informant interviews were conducted to collect the data. The most recent version of Open code 4.03 was utilized to generate meaningful codes, subthemes, and themes. The results were displayed using thematic analysis and respondents’ well-spoken verbatims.
Results: The study explored the perceptions of adolescents on the causes, prevention, and consequences of DBM. The main causes of DBM identified were poor dietary and drinking habits, poor knowledge and attitude about nutrition, low financial income, unemployment, food insecurity, poor feeding culture, physical inactivity, poor food management, educational and school-related issues, national-related issues, frequent use of ultra-processed foods, and frequent out of home eating. The majority of students were not aware of how DBM will affect their health and academic performance over the long run.
Conclusion: The findings showed that despite school adolescents’ variations in knowledge, lived experience, attitude, and perceptions, most of them have a poor understanding of the causes, consequences, and prevention mechanisms of the double burden of malnutrition. The results suggest the need for instituting double-duty interventions that have a double impact on the prevention of DBM.
Keywords: lived experiences, awareness, perception, school adolescents, double burden of malnutrition, Ethiopia
Introduction
The coexistence of undernutrition, overweight, and obesity among the same individuals, households, and populations at the national and international levels is referred to as the Double Burden of Malnutrition (DBM). It is the leading cause of morbidity and mortality worldwide, particularly in low- and middle-income countries.1,2 Globally, it is estimated that 820 million are hungry, whereas one-third of the world’s population people are overweight or obese.3 As growing segments of adolescents are not spared from DBM, there has been a paradigm shift in thinking about the DBM to mitigate its impact on the health of adolescents.4–6
Adolescence is defined as the age range of 10 to 19 years, which is a developmental stage that begins with puberty and lasts until early adulthood. Adolescence is a time of tremendous growth, but it is also a time of significant risk, which is frequently overlooked in the childhood-adulthood care continuum. On the other hand, adolescent growth is the second fastest, next to the first 1000 days of life, implying that this age group requires direct nutrition intervention.4,7,8
The global nutrition transition situations which manifested as changes in dietary patterns and physical activity have been shown to occur more quickly in some low-income countries than in high-income countries. Economic status improvements, mass media, and urbanization have all been identified as driving forces behind these rapid changes in dietary behavior.9–12 The host (people), the environment (the set of external factors to which people are exposed), and the vector (food and drink) all of these factors influence energy balance (the balance between low and high intake).13
The Ethiopian government prioritizes adolescent nutrition for a variety of reasons. To begin, this group accounts for a sizable portion of the population (33.8%). Second, as this generation enters the labor force, the health foundations established will have far-reaching social, political, and economic consequences. Third, healthy adolescents are a valuable asset and resource, capable of making significant contributions to their families, communities, and the nation as agents of social change rather than simply recipients of social programs now and in the future. Increased interest in adolescent and youth health is also due to a better global understanding of the developmental process during adolescence, which guides the design and delivery of tailored interventions for specific subgroups.14
There is a growing interest in the health of adolescents, and a focus on their nutrition is even more recently because they are future parents15 and one of the most nutritionally vulnerable periods of life due to increased pubertal development, linear growth, and neurodevelopmental issues.4–6
According to the pooled analysis study conducted in Bangladesh utilizing four consecutive DHS, underweight prevalence increased from 10.5% in 2004 to 24.2% in 2014, while overweight and obesity prevalence increased from 32.2% in 2004 to 18.3% in 2014.16 In the same area, a research in Palestine that included 1484 school children aged 5 to 16 found that stunting was 7% common, underweight was 3%, and that 12% of pupils were overweight and 6% were obese.17
The results of the combined Demographic and Health Surveys (DHS) of West and Central African countries from 1998 to 2017 indicated that the prevalence of teenage anemia and undernutrition in the region remained high during the past 20 years at 45% and 19%, respectively.18 The prevalence of general undernutrition, stunting, and thinness was found to be 35.1%, 29.4%, and 11.2%, respectively, in Burkina Faso.19
According to a research conducted in Addis Ababa, stunting (low height for age), underweight (low body mass index for age), and overweight/obesity (high body mass index for age) were all prevalent among school-aged adolescents, with prevalence rates of 7.2%, 6.2%, and 8.5%, respectively.20 Adolescent DBM prevalence was found in a community-based cross-sectional study conducted in the Babile district. Accordingly, 4.8% were overweight (+ 1 SD and + 2 SD), 6.6% were very thin (- 3 SD), 15.0% were thin (- 3 SD and −2 SD), 72.6% had normal range (>-2 SD and less than +SD), and 2 (1.1%) of them were obese (> + 2 SD).21
However, the lived experience, awareness, and perceptions of Ethiopian school adolescents regarding the prevention of the double burden of malnutrition are not well studied in Ethiopia. In addition to school adolescents, teachers and parents of students will be participated to increase the diversity of ideas and data. This qualitative research will answer the following questions using a phenomenology design. 1) What are the lived experiences, challenges, and perceptions of secondary school adolescents on the prevention of DBM? 2) How do secondary school adolescents understand the DBM in their local area? 3) What are the factors that affect the lived experience and perceptions of secondary school adolescents on the prevention of DBM? Furthermore, the purpose of this study is to explore the health, sociodemographic, economic, political, and education-related factors that may affect the lived experience, challenges, and perceptions of secondary school adolescents on the prevention, causes, and consequences of DBM.
Methods and Materials
Study Setting, Period, and Design
The study was conducted in Debre Berhan Regiopolitan city (DRBC), North Shoa zone, Central Ethiopia. The city is located 130 kilometers from Ethiopia’s capital, Addis Ababa, and 690 kilometers from Bahir Dar, the capital of the Amhara Region. The elevation of the city is 2840 meters above sea level. The study employed a phenomenology research design to explore the lived experiences of the study participants. The study period was from June 3 to July 10, 2022.
Population
During the study period, the source population consisted of all secondary school adolescents in Debre Berhan City (DBC). The study participants were chosen from the community’s selected schools based on their presence in the study areas.
Sample Size and Sampling Technique
Even though there is no predetermined and completely agreed method of calculating sample size for qualitative studies,22–28 the sampling and data collection process were guided by the point of saturation of ideas. This study enlisted the participation of twenty people, including nine students and eleven key informants (six teachers and five parents). Purposive sampling was used to collect data, which took into account the knowledge, perception, and understanding of secondary school adolescents and key informants. A rich source of information was used to collect data on respondents’ lived experiences, awareness, and perceptions. Respondents were purposefully identified for interviews who were considered relevant to the study due to their experience with the study’s topic.
Data Collection Methods
An unstructured interview guide was used to explore each participant’s lived experience and perceptions of nutrition, dietary practice, malnutrition, DBM causes, consequences, and prevention mechanisms. The guides were back-translated into Amharic by an independent translator and pretested to check their appropriateness to the local context. In-depth interviews (IDIs) with study participants and key informant interviews (KIIs) with teachers and parents were conducted to obtain sufficient information about their awareness and perception of the double burden of malnutrition.
Since this is the era of the COVID-19 pandemic, appropriate safety, and precautionary measures were maintained during data collection through a face-to-face interview, such that the interviewer and interviewee wore a face mask, maintained appropriate physical distance, and avoided direct sneezing toward another person. In addition to face-to-face interviews with participants, telephone and technology-assisted interviews were considered based on participants’ interests and accessibility, as well as other contextual factors. The research team conducted the interview, and all interviews were voice recorded in addition to taking notes.
Tools and Interview Guides
The study’s tools and interview guides were designed to address participants’ awareness, understanding, and perception of the DBM, as well as their lived experience with the prevention mechanism of DBM. The guide covered a wide range of DBM-related topics, including effect of taking proper nutrition, causes, consequences, and prevention methods of the DBM. Each of these major themes was accompanied by several possible probes and follow-up questions to gain a thorough understanding of secondary school adolescents’ awareness and perceptions of DBM. Interview guides were written in English first and then translated into the local language (Amharic) for clarity.
Ensuring Trustworthiness
The study’s credibility was ensured throughout the research process by using appropriate quality measurements. Quality assurance entails keeping and controlling the entire research process to ensure its quality and trustworthiness. This study considered various quality assurance issues in exploring the awareness and perceptions of secondary school adolescents in DBC using a phenomenology study design was used.23
The principal investigator and the research team supervised and gathered data, respectively. The audio-recorded interviews were transcribed verbatim immediately after the interview on the same day concurrently. The verbatim transcription was translated into English for analysis. The translated data were read line by line repeatedly to understand the context, and meanings, and to increase immersion into the data. To determine the true value of the data, multiple coders participated in the coding, categorization, analysis, and interpretations. A members check was conducted with selected interviews regarding the researcher’s interpretations of the realities and meanings.
Data Analysis Process
Data were exported to the latest version of Open Code version 4.03 software for further analysis and generation of meaningful codes. For data analysis, deeper immersion, chucking, clustering (thematization), and coding were used. As new codes emerged from the text, the initial codes were discussed and refined throughout the data coding period. Multiple coders contributed to the coding and categorization of the codes. These codes were combined into larger themes, which were then divided into sub-themes. Sub-themes were examined further to develop overarching themes. The data were then summarized and reported, along with some key direct quotes to illustrate the findings.
Results
Background Characteristics of Respondents
Twenty people took part in this exploratory qualitative study. Of the total respondents, 45% were students, of them 25% were grade ten students, 40% were degree teachers, and 70% were male respondents (Table 1).
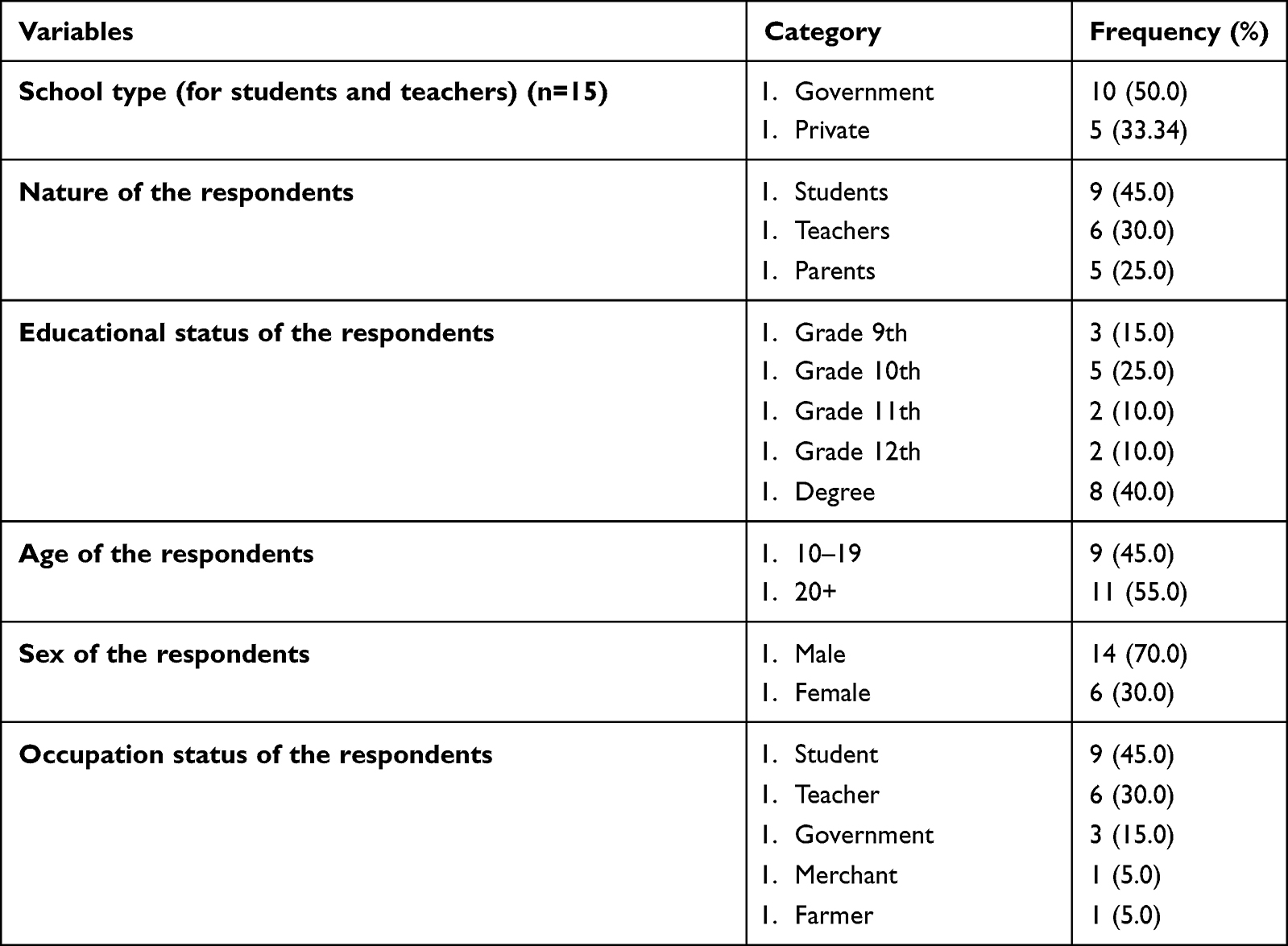 |
Table 1 The Background Characteristics of Respondents (n=20) in Debre Berhan City, Ethiopia, 2022 |
Number of Themes and Sub-Themes Identified
Overall, four main themes and twenty-five sub-themes with more than one hundred twenty-five (125) super (parent) codes and four hundred twelve (412) child codes were identified. The main findings of the study revolve around one central theme: Despite disparities in their knowledge, experience, attitude, and perceptions, most school adolescents have a poor understanding of the causes, consequences, and prevention mechanisms of the double burden of malnutrition. One of the respondents stated the following perspective,
… as an adolescent student, I would be pleased if I could understand the importance of good nutrition and practice all of the prevention mechanisms of the double burden of malnutrition to be protected from all forms of malnutrition and to have good dietary practice and nutritional status. However, the environment around me is not assisting me in doing so as I expected or perceived. (Student, 17 years old grade 11th respondent)
The themes and subthemes identified in this finding are summarized in Figure 1.
 |
Figure 1 The summary of main theme, themes, and subthemes identified in the thematic analysis of the study among adolescents in Debre Berhan City, Ethiopia, 2022. |
Theme I: Perception on the Literacy, Importance, and Effect of Good Nutrition
Perception on the Literacy of Good Nutrition
Most of the students have a poor understanding of the meaning, essentials, and effects of good nutrition. Regarding the understanding of students about the definitions of nutrition, some students can understand nutrition as it is a science that studies food, eating a balanced diet, eating nutritious food, and eating food rich in carbohydrates, protein, and vitamins. The literacy of nutrition among the study participants in the study area is relatively poor. For example, one participant said,
… I think we students have no good understanding of a healthy diet for us. I also do not know which food is very important enough for my health and education (Student, grade 12th and 19 years old).
Another respondent added… I don’t think that all of the food taken by the students contains all nutrients and food groups. I will never imagine that they have a complete diet. Because to say a diet is balanced, it has to contain all parts of the food and should be full of nutrients. I think, there is no complete dish (complete food table). (Key informant, 35 years teacher and male respondent)
Even though most of the study participants have a poor understanding of nutrition, some study participants were able to explain nutrition as eating nutritious food and taking a balanced diet to maintain health. They understand that food is a basic need that contains many ingredients which are very essential for humans. They also understand that, as it is known, man cannot live without food and water. It is the most important determinant factor to maintain good health. One of the participants stated the following to corroborate this,
… some school adolescents can take vegetables and fruits among the different types of food they take. I take grains, injera, bread, animal products, etc. I think these foods can provide carbohydrates, proteins, vitamins, and water. (Student, male and 19 years school adolescent)
Perception of Students About Foodstuffs They Take
Some students are taking foodstuffs such as grains, pasta, vegetables, energy-providing foods, and restorative foods from the normal food system. Some students believe that taking lentils, potatoes, vegetables, fruits, grains, and “Shiro wet” is very important because it provides carbohydrates, protein, fats, water, minerals, and vitamins. One of the students explains the following on this issue
… the different foodstuffs that I take for my diet are vegetables, fruits, and grains. These types of foods help me to get carbohydrates, proteins, fats, vitamins, and minerals. (a female, 16 years grade 10th student)
Another female, 14 years, and a grade 10th student said
… as young people, I think we should eat foods that give us energy. It is especially important to eat nutritious and restorative foods, and we usually get these foods from protein and carbohydrates rich foods.
However, the foodstuffs are dependent on the lifestyle of the student’s family. Because family food is one of the most determinant issues. One of the respondents said
… I eat my diet according to my family’s standard. But all food categories are not covered in the family (Student, male and 18 years school adolescent).
Perception of Students on the Importance of Good Nutrition
Better nutrition is very important for all of us, but it is especially important for secondary school adolescents, particularly adolescent girls, because they are the foundation of future generations. One of the key informants stated the following to reflect how adolescent nutrition is for the future of society,
… I believe that the issue of nutrition and malnutrition is being widely discussed in our country. Because our diet reflects society. The society must have a better diet to produce a generation of competent, efficient, and active workers capable of building the country (a male, 58 years degree teacher).
Better nutrition is also important for disease prevention. Foods such as salt-free, sugar-free, and low-saturated food products should be used to protect against disease. Some students may consume leftover food in the hotel, even if it is of poor quality. One of the students uttered the following the relevance of good nutrition to health.
… there are various types of foods. For example, in the current trend known as big illness protection, they use a type of food. At every age, individuals with disease consume sugar-free and salt-free foods. (a male, 17 years old, 11th-grade student)
Another student believes that
diabetes mellitus patients should not consume high sugar, hypertensive patients should not consume high salt, and patients with a gastric problem should not consume all foods as they want, therefore, they have to follow their doctor’s medical advice and recommendation. (Student, male and 17 years school adolescent)
Perception on the Effect of Good Nutrition on the Educational Status of Students
Students have the perception that good nutrition is central to well-being and better education.
For instance, one student said
… because I eat fruits, grains, vegetables, animal products, and bread that contain different food groups, different food types, and different foodstuffs, I believe that I will have good nutritional and educational status. Injera, “Shiro wet”, meat and meat products, milk and milk products will also provide me carbohydrates, proteins, vitamins, and minerals, allowing me to be more effective in learning and studying (17 years old grade 10 student).
Perception on Determinants of the Choice of Good Nutrition
One of the most important issues in school adolescent nutrition is the practice of making appropriate and healthy food choices. School-aged adolescents must choose a healthy diet to maintain a healthy nutritional status. However, a variety of factors influence and determine food selection practices among school-aged adolescents. Some of the most common determinant factors identified by research participants are poor knowledge of nutrition, poor attitude towards nutrition, economical problem, feeding culture, unemployment, and inadequate food supply. One of the key informants stated the following to explain this state of affairs,
… It depends on our capacity, our family’s capacity, purchasing power, economic capacity, income status, and so on. As a result, it is generally dependent on the student’s family’s capacity. On the other hand, it may stem from ignorance, a lack of knowledge, poor practice, and a negative attitude (Key informant, a degree teacher, and 58-years old respondent).
Theme II: Perception on Literacy, Causes, and Consequences of DBM
Most of the study participants did not understand well the meaning, type, level of occurrence, causes, and consequences of the double burden of malnutrition.
Perception on Literacy of Double Burden of Malnutrition
According to some student’s points of view, the presence of a double burden of malnutrition can be defined as the presence of both undernutrition and overnutrition, the presence of both overeating and undereating, a problem with the amount of food and the quality of food, eating too little or eating too much, and a lack of food or food abundance. Despite the study participants’ poor understanding of the types of malnutrition, DBM can be broadly classified as undernutrition or overnutrition. The majority of study participants have little understanding of the phenomenon. The respondents stated the following showing their level of understanding,
… I have heard, but I do not know much about DBM. I believe that man must make his diet as healthy as possible. (a 33-year-old male teacher).
Another respondent said,
… I have no specific information about it (DBM) (a male key informant and 30 years old).
A 35-year-old male key informant and teacher also described
…I do not have a lot of information. I think it appears that both under-eating and overeating are present in our nations
One of the students’ problems is a lack of knowledge and literacy about malnutrition. Some students understand malnutrition as food that does not contain enough nutrients, eating too little/too much, not properly understanding the benefits and harms of diet, food shortage, lack of food, food that does not contain the minimum dietary preference, incompleteness of various essential nutrients such as food that does not contain protein, vitamins, food that does not meet nutritional requirements, and poor food groups such as bread, cereals, fruits, injera, and vegetables. Students may experience a lack of attention to education, reading, study, and work as a result of mental health problems and economic problems. Malnutrition is a significant community and widespread problem in our country. One of the key informants stated the following issue,
… when we say malnutrition, even though I am not a biology teacher, it is a scarcity of food that cannot meet an individual’s minimum dietary preference, most commonly, food groups that contain essential nutrients such as cereals, Injera, bread, and vegetables. So, malnutrition occurs when there is a lack of cereals, Injera, bread, and vegetables, all of which contain important nutrients such as carbohydrates, protein, vitamins, minerals, and essential fatty acids. (Key informant, 54 years old male and teacher)
Perception of Undernutrition
Few students have a perception of undernutrition as it is only eating too little. Furthermore, they could clearly understand the causes, consequences, and effects of malnutrition on their educational status and future health. For instance, one of the key informants said the following,
… undernutrition is defined as a low consumption of food parts that lack vitamins, carbohydrates, and proteins and thus do not meet our nutritional requirements. (Key informant, 35-year-old male teacher)
Perception of Overnutrition
Few students comprehend the status of overnutrition as avoiding excessive eating, reducing added sugar, butter, fatty foods, high-fat foods, and salt. However, because most students are following a poor feeding style, they did not understand it well. Furthermore, they are not oblivious to the causes, consequences, and effects of overnutrition on their future health and educational status.
I don’t believe I’m overweight. I don’t think weight gain will catch up with me. Because it is commonly held that a thin person does not gain weight (Student, 17-year-old male school adolescent respondent).
Perception on Double Burden of Malnutrition
The prevalence of DBM can be found at the individual, population, national, and international levels. Thinness, stunting, and overnutrition in school adolescents can result in a double burden of malnutrition in our country. However, almost all study participants did not comprehend this level of occurrence well. For instance, one of the students stated,
… I believe that the double burden of malnutrition cannot affect all populations equally and may not occur at all population levels. I believe it primarily affects children under the age of five and mothers. (Key informant, a 58-year-old male respondent).
Perception on Causes of DBM
According to the different perspectives of the participants, the cause of DBM had variant circumstances. The causes that are identified in this study from the different respondents are listed as follows.
Poor Dietary and Drinking Habits
Study participants stated that poor feeding habits, not consuming nutritious food and adequate nutrients, drinking too much alcohol, drinking too much sugary and soft drinks, lack of experience in food preparation, focusing solely on sweet foods, low or high frequency of meals, eating a large number of foods (overeating), foods cheap in cost but not important, eating too much and getting less exercise, consuming fast foods, packed foods, street foods, fried foods, a lack of exercise, consuming fast foods, packed foods, street foods, and fried foods were the causes of DBM.
Presences of Diseases
According to the respondents, the presence of diseases and/or pain, whether they have acute or chronic nature, had a significant impact on the nutritional status of school adolescents. From the common disease and/or illnesses, diarrhea, malabsorption, loss of appetite, nutrient change for immune response, and urinary nitrogen loss all contribute to nutrient losses and further damage to defense mechanisms in a sick person. As a result, dietary intake is reduced. Due to these illnesses, adolescents will have low consumption of fruits, vegetables, whole grains, and low-fat dairy foods.
Poor Knowledge of Nutrition
The most common determinants of DBM in students were a lack of good nutrition knowledge, a lack of knowledge to build enough capacity to have good nutrition, a lack of nutrition literacy in the community, and a family with a good income but poor nutrition knowledge. One of the key informants stated,
… those with a good income have a problem with attitude, understanding, and a lack of educational focus on nutrition. I don’t think students and other communities understand the food they eat and its health benefits very well right now. Most people only consider the filling of their stomachs, not the health benefits. (35-year-old male key informant)
Poor Attitude About Nutrition
Giving higher value to only one food, such as meat, following an ignorant feeding habit despite having a good economic capacity, becoming an ignorant family to properly manage children’s diet, problems related to their attitude, poor attitude despite having a good income, and always using Injera even in the presence of other foods. Purchasing one kilo of meat costs more than 500 Ethiopian Birr (the current cost of one-kilo meat during data collection time). One of the study participants stated the following to explain this,
… another issue is that assigning a higher value to only one type of food (mostly meat) is a problem related to our attitude. One kilo of meat will cost more than 500 birrs. However, this birr could be used to purchase foods other than meat that are high in nutrients. So, we do not have enough understanding (a male respondent, 35 years teacher).
Financial Problems
Economic power has a significant impact on food preferences. Food selection is influenced by economic capacity, family income status, inflation, purchasing power, lack of assets for living, low standard of living, and the cost of living. Poor income management, on the other hand, has a significant impact on food choices. In our system, the majority of people are impoverished. Because of their limited financial resources, they are unable to feed their children from various food groups and have no opportunity to do so. Some people, however, are wealthy. They eat a lot because they have enough money to do so. Richman is prone to chronic diseases like DM, hypertension, overnutrition, and dominantly eating meat products. One of the key informants said,
… food selection is determined by a family’s economic capacity, purchasing power, and income status, among other factors. As a result, it is generally dependent on the student’s family’s capacity. (a male, 58 years old degree teacher)
Unemployment of the Family/Students
One of the most important determinants of food choice for student parents is unemployment or a lack of adequate working conditions. One of the key informants thought,
… the first and most important factor is income to practice good food selection. The presence of unemployment will cause us to make poor food choices. The second problem is a complete lack of adequate working conditions. (a male degree teacher, 54 years old)
Food Insecurity or Low Food Supply
Most school adolescents did not achieve their preferences due to a lack of adequate food supply in the market. Due to the lack of adequate food supply in the surrounding environment, most students, particularly those from rural areas, are exposed to malnutrition. In the presence of an adequate food supply, another issue that influences student food selection is food preparation. One of the participants supposed,
… there is no completely affordable food for everyone at all times. As a result, preventing food shortages should be a government strategy, program, and policy. It is difficult to obtain nutritious food for everyone in our family as a complete diet. It is difficult to say what is nutritious food for students because their living conditions determine what they eat. It could be due to a lack of food supply. If they have a food supply, their food choices may be satisfying (a male, 30 years old respondent).
Family and Student-Related Problems
Most families of students cannot feed their children well, have food problems, do not help their children with good feeding, do not understand the benefits of nutrition, use only one type of crop produced in the area, and lack of adequate product in families. There are also absences of family support, low family educational status, and poor knowledge of nutrition. According to students, the family’s capacity considers only filling their stomachs and there is a lack of understanding of food and nutrition and feeding traditions. For example, one of the students stated the following,
… some of the barriers that prevent students from consuming nutritious foods include lack of money to buy food, low standard of living, lack of assets for living, inflation, lack of knowledge, attitude, and experience about food and nutrition, as well as a failure to properly understand the benefits and harms of food, among other things (14-year-old 9th-grade student).
Feeding Tradition/Cultures
Even though traditional or cultural foods are recommended to students, families, and the community, they are ignored and not regarded as food by students, families, and the community. Culturally acceptable foods assist students in becoming physically fit and strong. The current generation does not use or consume culturally accepted foods such as porridge, “Kita”, and “Kollo.” One of the schoolteachers thought
… there are two things/factors that influence students’ food selection habits. One is poor feeding culture and the other is economic status. Our food culture should come from a variety of food groups. For instance, “kinche”, “Kita”, “Kollo”, and other cultural foods. (a 33-year-old male schoolteacher).
Expansion of Cities
Another point of view expressed by respondents in this study on the determinants of food choice is an expansion of the city. Farmers have lost their cultivable land as a result of the city’s expansion. In this case, the student’s family is unable to grow vegetables and grains and obtain adequate food groups. This is a typical problem for rural farmers living around the city, according to the study respondents. One of the key informants stated the following m trying to explain this,
… especially for students who come from the surrounding rural areas, getting special food is not pretty possible. When they go with their families, this is not always well balanced. They come from the countryside and do not get that when they go to the city. This is also difficult because their families live on the city’s outskirts, some kilometers away. Their family had lost their land due to the city’s expansion. Their family would not grow various vegetables, cereals, and so on. As a result, they are unable to feed their children from their land and the students are unable to consume sufficient food. (Key informant, a 54-year-old male schoolteacher)
Food Management Problems
Poor food safety practices, poor food management during production, transportation, storage, preparation, and consumption, and system management problems are all the causes of DBM. One of the key informants stated,
… there is an issue with an understanding of food preparation, food safety, food management, and food production (Key informant, male teacher, 54 years old).
Social Relationship Problems
The students stated that failure to fall in love with a peer, hearing about love from other students, peer pressure, not receiving help from others, no proper imitation from others, and frustration that prevents them from eating or led them to eat more can leads them to develop a double burden of malnutrition. One of the students stated,
… you will not eat if you have failed in love with a peer, even if I am not facing it, I am aware of it through the people around me and my friends. I hear them when they say, even I can’t eat well. On the other hand, some of them eat more due to over-happiness. (A male student in the eleventh grade)
Stress
According to the student’s understanding, DBM can be caused by stress. Some students recognize that anxiety, frustration, general stress, stress due to national issues, stress about getting food, stressful conditions, and barriers to eating and taking adequate food will prevent them from eating and taking adequate food. However, most students only had a hazy understanding of such a scenario.
… It can also be stressful conditions. Stress can also influence them not to take nutritious food due to national issues, educational issues, etc (Male, grade 9th student, 19 years old).
Physical Inactivity
Not getting enough physical exercise, not participating in cultural playing and activities, not playing football, not walking on foot, sitting too much, frequent use of public transportation, and not doing simple tasks are the most common causes of malnutrition.
… not doing moderate-intensity physical exercise, especially in the morning, continuous use of public transportation, sitting too much, and physical inactivity are the causes of DBM. (17 years old, grade 10th student)
Educational and School-Related Causes
The majority of respondents believed that poor nutritional status would lead to poor academic performance, a lack of attention to education, reading, study, and work, more time spent on reading without comprehension, all time spent on education but no consideration, and an inability to learn by self-sufficiency. One of the key informants thought,
… I think poor nutritional status would be a cause for poor academic performance, low attention to education, students not spending their time reading properly, and did not understand education is worth (Key informant, 19 years old student).
Furthermore, they believed that a lack of school feeding contributed to students’ lack of academic focus and achievement. A key informant explained,
… In our school, there is no school feeding. If our school has school feeding, but it does not, students who faint while teaching or learning in class will be fed. (key informant, 49 years old respondent)
National-Related Issues
Some of the respondents reported that national issues, our country’s current situation, unresolved national issues, and peace and security issues affected their nutritional status directly or indirectly. One of the students perceived,
… peace and security national issues, current situations in our country, and unresolved national issues caused students to be stressed and not eat nutritious food, resulting in a decrease in their educational performance. (IDI, 17 years old and female student)
Frequent Use of Ultra-Processed and Market Foods
Rare students understand that purchasing packed foods from the market, avoiding frequent consumption of packed foods, and controlling the expiration date of packed foods, fast foods, and fried foods from the customer side are all important. A female student stated,
… Don’t eat foods with a lot of oil in them, don’t eat too much-fried food, and don’t eat too many potato chips, which lead to obesity.” Purchasing fruits, pulses, and vegetables at a lower cost than meat and eating clean food (A female student of 16 years old).
Frequent Out-of-Home Eating
Rare students understand that out-of-home eating, not making our food at home, and using foreign-style foods too much, which are promoted in media are the causes of DBM. A male key informant detailed,
… I think frequent use of out-of-home eating can be a cause of malnutrition. Because we don’t know the type of food we eat in the restaurant, sometimes there is food adulteration, mixing of food with other materials, sweets, food contamination, and food poisoning. (Key informant, 40 years old male respondent)
Perception on Consequences of DBM
Few school-aged adolescents believed that the double burden of malnutrition harmed their health and educational status. In terms of their perception of the health consequences of DBM, they believe that the presence of DBM exposed them to acute diseases, non-communicable chronic diseases, weight gain, and weight gain-related diseases. On the other hand, some students believed that DBM had an impact on their academic performance and achievement. However, the majority of students were unaware of the long-term effects of DBM on their health and educational status.
… I believe that malnutrition has an effect on our health, educational achievement, educational performance, and grade result (Students, a female, and 14 years old respondent).
Theme III: The Lived Experience of Students on Dietary Practice and the Prevention of DBM
Lived Experience of Adolescent Students on Their Dietary Practice
In terms of their lived experience with adequate and appropriate adolescent nutrition, almost all students have a negative experience with their dietary practices. The most common student experiences are not able to avoid eating too little or too much, being unable to distinguish the benefits and harms of food well, eating only one food, sometimes eating too much fat and fatty foods, not taking different types of food, not having an appropriate feeding style, and not increasing intake of fruits and vegetables. One of the parents of the students thought,
… really, most students have no experience on how to choose a balanced diet, how to distinguish the benefits and harms of food, how to take different types of food, have no appropriate feeding style, and not taking of fruits and vegetables as it is expected. (Parent, 58 years old male respondent)
Lived Experience of Adolescent Students on Prevention of DBM
Limited students combined with their families have a lived experience with dietary interventions to reduce the prevalence of the double burden of malnutrition. The most important dietary interventions practiced by the respondents are planting fruits and vegetables in the garden, eating as nutritious food as possible, having an adequate diet, and taking more fruits, grains, and vegetables. One student experience poor nutritional status and visits a health facility suspecting malnutrition.
… I was worried about malnutrition and going to the health facility. But now health professionals are consulting me and telling me the problem and I am fine now. After I get a piece of medical advice, now I am fine and I share this knowledge with my family. To reduce undernutrition, using vegetables because they are relatively cheap compared to others, protects them from malnutrition (19 years old, grade 12th male student).
Students stated that we must take care of ourselves, we have not just said we are not hungry and protect ourselves from malnutrition by eating adequate foods. One of the respondents stated,
… I always keep my meal time, eat nutritious food for myself, eat on time, eat food that prevents undernutrition, keep meal time, eat by time, and do sports for good health. We always keep meal times and eat on time, sometimes I spend six hours thinking about eating at eight when I may not be hungry. (17-years-old government school student in 11th grade)
Reducing ultra-processed foods and packed foods is one of the methods to overcome DBM because they are low or high in energy. Some street foods are not safe for us to eat. For example, “sambusa” can cause weight gain and biscuits can cause stomach aches due to oil they may not be healthy because packed biscuits are oxidized with sugar. Reducing street foods like “sambusa” and biscuits can reduce DBM. Therefore, the recommended things are eating less packed market foods, avoiding eating too many sweet things, and not using a lot of salt. One of the school adolescents understood,
… on the street, biscuits and “sambusa” are sold alongside each other. Biscuits can cause stomach aches because they contain oil, which is not good for us. “Sambusa” has the potential to cause weight gain. Foods sold in a store (shop), on the other hand, come from a factory and are oxidized with sugar, which means that sugar pressure has no effect. Controlling these market foods, eating less, and eating less frequently, for example, not eating packaged foods, fast foods, or avoiding purchasing food sold on the street, such as fried foods will thus reduce the double burden of malnutrition (Grade 11th government school student, 17 years old).
Theme IV: Expected Responsibility from All Responsible Stakeholders to Prevent DBM
The study participants suggested that every part of society, especially the city administration and the school administration, has the responsibility to overcome the nutritional problems in school adolescents. Some of the expected responsibilities reported by the respondents are explained as follows.
Expected Responsibility from Students Themselves
To achieve good grades in school and increase school performance and solve a problem concerning the literacy of nutrition, students should understand food preparation, food safety, food management, food storage, and food consumption. Adolescent students have the responsibility to care about their nutrition status and dietary practice. They should have to create a conducive environment with their parents, teachers, school administration, and other responsible stakeholders to increase their awareness of better nutrition and the prevention of malnutrition. In most schools, students have no good communication with teachers and other school communities. To bring a change, create good communication, and increase awareness of students about student nutrition, there must be coordination, cooperation, and smooth communication. One of the parents of the students suggested,
… adolescent students have a great expected responsibility to care about their total health, especially their nutrition status and dietary practice, to be effective in their education and achieve a good grade result at the end of the day in coordination with their parents and teachers (Parent, 57 years old male respondent).
Expected Responsibility from School Administration
To increase the understanding of healthy diet by the students, school administrators should initiate school feeding programs, and invite health care workers for nutrition education and nutrition behavior change communication. To do this, strong school management and administration are needed. A fifty-four-age key informant said,
… while others are also needed, a good school administration and management are very important and vital (Key informant, 54 years old male respondent).
Expected Responsibility from Teachers
A strong teacher is needed to apply effective teaching practices on nutrition and the health of school adolescents. School teachers should establish different school clubs related to nutrition, and include nutrition in the curriculum, and sports teachers have to educate about moderate physical exercises. All professionals of the school must educate students, especially biology teachers have a higher responsibility to educate the student about good feeding practices and nutrition behavior change education. One of the key informants suggested,
… All of the school teachers, especially biology subject teachers, have a higher responsibility to educate their students through different school clubs about the nutrition of their students. However, they are not ready to do this. The biggest thing is that students and teachers are not united and have no good communication. (Key informant, 54 years old male respondent)
Expected Responsibility from Healthcare Workers and Health Sector
Healthcare workers should give nutrition education on food-based approaches, nutrition counseling, and nutrition behavior change communication at a programmed education at least every two months as most of the respondents reported. The health bureau has the responsibility to give health and nutrition-related training to students, teachers, and other school communities. A male key informant said,
… health care providers and health bureau must provide such an important and behavior change education, especially nutrition behavior change communication (Key informant, 58 years old male respondent).
Expected Responsibility from Family About Their Child’s Feeding Experience
It is the responsibility of the family to monitor their student’s diet and suggest healthy eating habits. Furthermore, they are responsible for monitoring their child’s educational performance and achievement, nutritional status, attainment of minimum dietary diversity, the effect of feeding habits on health, and the consequences of feeding on nutritional status.
… we students require our parents to monitor our educational and nutritional status. Due to poor nutritional status and follow-up, we will not be able to achieve good grades in our education unless our family has followed us frequently and effectively. (10th-grade student who is 15 years old)
As a parent, I did not monitor my children’s nutritional status for better education. I’ve learned from this because I have to monitor my child’s nutritional status and educational achievement. (Parent, respondent of 42 years old)
Expected Responsibility from the Local and National Government and NGO
The government’s role in preventing the country’s double burden of malnutrition is critical. It should allocate sufficient nutrition experts, create a strong food system, plan a nutrition program, and develop a nutrition strategy, and policy to curb DBM. The government is also responsible for increasing food production, working hard to improve diet and food supply, avoiding inappropriate property distribution, controlling the market regarding the sale of expired date foods, and monitoring the country’s economic, political, and social systems related to nutrition. Most of the time, there is no appropriate message, administration, or follow-up. It has also solved the national problem of peace security to increase the country’s food production stability.
… when viewed broadly, this is directly related to the country’s political, social, and economic system. There will be a strong food system if there is a strong government and a strong legal system. This is what we faced in this country because the community is now the largest case of a nutritional issue due to poor government follow-up. One of the most common issues is the improper distribution of property throughout the country (Key informant, 54 years old male respondent).
Moreover, Non-Governmental Organizations (NGOs) working in national and local settings had a significant expected responsibility to prevent school-age malnutrition. They have specifically supported school feeding for students. A male key informant stated the following,
… I believe that non-governmental organizations should assist the local government in improving the nutritional status of school adolescents, particularly through the implementation of school feeding in all of the city’s schools. (Key informant, 58 years old male respondent)
Expected Responsibility from Media
It is the responsibility of the national and local media to promote appropriate food and feeding styles for students. Furthermore, providing nutrition education for students, families, communities, and all through media such as radio and television are a mandatory duty from all respected media. A grade twelve student stated the following,
… the media bears a significant responsibility in promoting a healthy diet for all populations in the country, particularly for school-aged children with a great focus. Because school adolescents are exposed to poor feeding habits at this time (Student, grade 12th and 19 years old respondent).
Expected Responsibility from Merchant and Stockers
According to the majority of respondents, there is no right and actual merchant. Respondents believe that most merchants intentionally or unintentionally sell expired food, and we do not know how long the packed food is kept in stock. As a result, it is expected that merchants will avoid selling expired date food intentionally or unintentionally. One of the key informants explained,
… there is no such thing as a good merchant or a good shopkeeper. This is because the property will only be in the hands of a few people, who will sell it as they see fit. On the other hand, some merchants feel compelled to emulate Richman by defrauding the community. As a result, in addition to food, this effect affects many other systems. [Key informant, 36 years old respondent]
Expected Responsibility from Farmers and the Agriculture Sector
Respondents suggested that farmers use better farming techniques to increase output. Because agriculture is the main backbone of food production, it should provide all necessary materials such as soil fertilizer and better seeds.
… farmers must have good farm products to effectively feed their children and other community members. They should practice better farming techniques. … If farmers grow effectively if they have access to soil fertilizer and appropriate seed, they will produce a high-quality product, and students and the surrounding consumer community will benefit. The surrounding society will receive a high-quality product for consumption. [Key informant, 45 years old male respondent]
Discussion
The results of this exploratory qualitative study examined the lived experience and perspectives of school adolescents on the prevention, causes, and consequences of a double burden of malnutrition in Debre Berhan City, Ethiopia. The participants gave detailed accounts of their personal experiences and opinions regarding the prevention, causes, and effects of the double burden of malnutrition. Beyond that, they emphasized the expected accountability of all accountable parties to address the dual burden of malnutrition in the study area.
According to this study, the majority of school-aged teenagers have a limited understanding of the effects, and preventative measures of the double burden of malnutrition despite their disparity in knowledge, attitude, experience, and perspectives. This finding is similar to the reports of other studies on the risk and challenges of health behavior. 23,24
When we discuss the perception of students on their understanding of good nutrition, most students have little understanding of the meaning, significance, and benefits of healthy eating. According to studies, some children can understand nutrition as a science that examines food, having a balanced diet, eating healthy food, and eating food rich in carbohydrates, protein, and vitamins. The level of dietary literacy among the study participants is comparatively low. This result is consistent with the qualitative study done on feeding practices, knowledge, and attitudes on child nutrition framework.31
Related to the perception of students about foodstuffs they take, some students are taking food from the standard food system, including grains, pasta, vegetables, meals that give them energy, and foods that heal them. Because they contain carbohydrates, protein, lipids, water, minerals, and vitamins, some students feel that consuming lentils, potatoes, vegetables, fruits, cereals, and “Shiro wet” is crucial. A similar perception was reported in the previous study.32
Regarding the perception of respondents on the importance of good nutrition, it is crucial for secondary school students, especially adolescent females, to require it because they are the future of society. An improved diet is good to have active and more productive workers, a better society, healthy physical development, and the advancement of the nation. It can also produce a better, more competent, and more efficient generation. In general, the diet of schoolchildren reflects the future makeup of society. And a healthier diet is crucial for disease prevention. To ward off illness, people should consume foods that are low in saturated fat, salt, and sugar. Consistent findings were reported from the previous studies.26,27,31
Concerning the perception of the effect of good nutrition on the educational status of students, participants stated that students should eat well and have a healthy diet to learn effectively, acquire higher grades, be talented in class, attend class regularly, have good reading habits, and have better study habits. Related to the perception of determinants of the choice of good nutrition, making proper and nutritious food choices is one of the most crucial aspects of school-age nutrition. Adolescents in school must choose a nutritious diet to keep their nutritional status in check. However, several variables affect and determine how school teenagers choose their food. Poor nutrition knowledge, a negative attitude towards nutrition, economic problems, food insecurity, poor minimum dietary diversity practice, feeding customs, unemployment, and insufficient food supplies are some of the most prevalent determinant factors mentioned by research participants. The determinants of the choice of good nutrition for adolescents were similar to other studies.26,28,30,32–34
According to the perception of students about the literacy of the double burden of malnutrition, the majority of students struggled to grasp the definition, nature, frequency, causes, and effects of the double burden of malnutrition. Some students believe that the existence of both undernutrition and overnutrition, overeating and undereating, a problem with the quantity and quality of food, eating too little or eating too much, and a lack of food or an abundance of food constitute the presence of a double burden of malnutrition. Most study participants were vaguely familiar with the phenomenon. This is insight found to be consistent with other findings24,35.
Concerning their perception of overnutrition, few students are aware that preventing excessive eating, and cutting back on added sugar, butter, fatty foods, high-fat foods, and salt all contribute to overnutrition. However, most of them do not understand it well because of their bad food habits. They are also aware of the origins, effects, and repercussions of overnutrition on their long-term health and educational standing. A similar observation was reported from the previous studies.
Regarding the causes of the double burden of malnutrition, poor dietary and drinking habits, diseases, poor nutrition knowledge, poor nutrition attitude, financial problems, family unemployment, food insecurity, poor feeding culture, physical inactivity, city expansion, poor food management, peer pressure, stress, educational and school-related issues, national-related issues, frequent use of energy-dense and market foods, and frequent use of out-of-home eating were the main causes of DBM identified in this study. The identified causes were in line with the already existing body of knowledge.24,29,35–39
Concerning the lived experience of adolescent students on their dietary practice, almost all students have a negative experience with their dietary practices in terms of adequate and appropriate adolescent nutrition. Not being able to avoid eating too little or too much, being unable to distinguish the benefits and harms of food well, eating only one food, sometimes eating too much fat and fatty foods, not taking different types of food, and not having an appropriate feeding style, and not increasing intake of fruits and vegetables are among the most common student experiences. The perceived dietary experience of respondents is consistent with other findings.40–42
Related to the lived experience of adolescent students on the prevention of DBM, few students, in collaboration with their families have firsthand knowledge of dietary interventions to reduce the prevalence of the double burden of malnutrition. Planting fruits and vegetables in the garden, eating as much nutritious food as possible, having an adequate diet, and eating more fruits, grains, and vegetables are the most important dietary interventions practiced by respondents. Similarly, other DBM prevention mechanisms include adjusting daily meal frequency, the experience of eating original food rather than ultra-processed foods because they are low or high in energy, avoiding sleep immediately after a meal, taking disease-fighting foods for thin students, taking fat in moderation, especially for those who are overweight, and eating nutritious food such as proteins, vegetables, vitamins, and water. The lived experience of respondents is in line with the previous research findings.26,34,43–51
Reducing high energy-dense and packed foods due to their low or high energy content. Some street foods are unsafe for us to consume. Sambusa, for example, can cause weight gain, and biscuits can cause stomach aches due to oil, and it may not be healthy because packed biscuits oxidize with sugar. Reduced consumption of street foods such as sambusa and biscuits can help to lower DBM. As a result, eating less packaged market foods, avoiding excessive sweets, and limiting salt consumption are all recommended. This paper is in line with other studies done on energy-dense and packed foods.52–57
Regarding the expected responsibility from all responsible stakeholders to prevent DBM, participants in the study suggested that every aspect of society, particularly the city administration and school administration, bears higher responsibility for addressing nutritional issues in school adolescents. Students, families, teachers, school administration, local and national government, NGO, education bureau, health bureau, health care workers, media, merchants, and stockers are among the other responsible bodies to reduce DBM reported by respondents. This idea is similar to the other South African findings done on the management of school nutrition programs to improve environmental justice in schools.58
Regarding the strength of the study, all of the interviews were conducted in the participant’s native language. The interviewers’ nearly identical cultural and linguistic backgrounds aided the flow of the interviews and made participants feel more at ease sharing their experiences openly. The richness of our description of the study’s findings based on participant experiences should allow readers to assess the transferability of findings to other studies on similar topics, and the research team was able to reach a consensus on each theme and subtheme. Perhaps verbatim quotations will help readers consider whether they agree with some of our study’s participants. Whereas, the study has a limitation in that no generalizations to larger populations can be made.
Conclusion
According to this study, despite their disparities in knowledge, attitude, experience, and perspectives, the majority of school-aged teenagers, teachers, and parents have a limited understanding of the origins, effects, and preventative measures of the DBM. The main causes of the double burden of malnutrition were poor dietary and drinking habits, diseases, poor nutrition knowledge, poor nutrition attitude, financial problems, family unemployment, food insecurity, poor feeding culture, physical inactivity, city expansion, poor food management, peer pressure, stress, educational and school-related issues, national-related issues, frequent use of energy-dense and market foods, and frequent out-of-home eating.
The findings imply that all segments of society, particularly city administration and school administration, should take a greater role in addressing nutritional issues in school adolescents. Moreover, other sectors are responsible for addressing nutritional issues, but the health, education, agriculture, and finance sectors bear the greatest burden.
Among the expected responsibilities reported by respondents for reducing the double burden of malnutrition are students, families, teachers, school administration, local and national government, non-governmental organizations (NGOs), health care workers, media, merchants, and stockers. Finally, it is recommended that double-duty interventions that have a double impact on DBM prevention be used.
Data Sharing Statement
The data used to support the findings of this study are available from the corresponding author upon reasonable request.
Ethical Considerations
The study was conducted following the criteria of the Helsinki Declaration.59 The study proposal was ethically approved by Jimma University, Institute of Health, Institutional Review Boards (IRB) with reference number JUIH/IRB/104/22 before the start of data collection. Furthermore, permission to collect data was first obtained from the Debre Berhan city and Zonal education bureau. Before obtaining informed consent, each study participant was given a detailed explanation of the study’s title, purpose, procedure, and duration, as well as the potential risks and benefits. Before any interview or measurement, each secondary school adolescent was provided verbal, written, and signed informed consent. The participants were informed about publication of anonymized responses. The data were kept confidential by not including any personally identifiable information on the questionnaires and asking them in a secure free room. Personal identifiers and other data elements were separated. Their rights were protected during the interview. For those under the age of eighteen years, both assent from the students and consent from their parents were obtained. Finally, any ethical issues that arose during this study were resolved through continuous discussion between the researcher and JU’s IRB.
Acknowledgments
Our special thanks and sincere appreciation go to the Debre Berhan University and Jimma University for fund support. We also thank Jimma University for the approval of the ethical clearance. I would also like to acknowledge study participants, supervisors, data collectors, and data clerks for their tremendous role throughout the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Debre Berhan University and Jimma University in collaboration support this study.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shimpton R, Rokx C. The Double Burden of Malnutrition: A Review of Global Evidence. Health, Nutrition and Population (HNP) Discussion Paper. World Bank; 2012.
2. Kulkarni B. Addressing the double burden of malnutrition in developing countries: need for strategies to improve the lean body mass. Food Nutr Bull. 2018;39:S69–76. doi:10.1177/0379572118768572
3. Development Initiatives. Global Nutrition Report 2020: Action on Equity to End Malnutrition. Bristol, UK: Development Initiatives; 2020.
4. Das JK, Salam RA, Thornburg KL, et al. Nutrition in adolescents: physiology, metabolism, and nutritional needs. Ann N Y Acad Sci. 2017;1393(1):21–33. doi:10.1111/nyas.13330
5. Hofman K, Erzse A, Kruger P, Abdool Karim S, May J. Double burden and double duty: government action required to improve child nutrition. South Afr Child Gauge. 2020;2020:135–151.
6. Society T. Addressing Nutritional Disorders in Adolescents. J Adolesc Heal. 2018;63(1):120–123.
7. Nicholson A, Fawzi W, Canavan C, Keshavjee S. Advancing global nutrition for adolescent and family health: innovations in research and training. proceedings of the Harvard Medical School Center for Global Health Delivery–Dubai. Dubai, United Arab Emirates; 2018.
8. Sethi V, Lahiri A, Bhanot A, et al. Adolescents, diets and nutrition: growing well in a Changing world. CNNS. 2019;2019(1):1–4.
9. Popkin BM, Adair LS, Ng SW. Global nutrition transition and the pandemic of obesity in developing countries. Nutr Rev. 2012;70(1):3–21.
10. Popkin BM, Corvalan C, Grummer-Strawn LM. Dynamics of the double burden of malnutrition and the changing nutrition reality. Lancet. 2020;395:65–74. doi:10.1016/S0140-6736(19)32497-3
11. Vaezghasemi M. Nutrition transition and the double burden of malnutrition in Indonesia A mixed method approach exploring social and contextual determinants of malnutrition. Umeå, Sweden; 2017. Available from: http://umu.diva-portal.org/.
12. Mbogori T, Kimmel K, Zhang M, Kandiah J, Wang Y. Nutrition transition and double burden of malnutrition in Africa: a case study of four selected countries with different social economic development. AIMS Public Heal. 2020;7(3):425–439. doi:10.3934/publichealth.2020035
13. Romieu I, Dossus L, Barquera S, et al. Energy balance and obesity: what are the main drivers? Cancer Causes Control. 2017;28(3):247–258. doi:10.1007/s10552-017-0869-z
14. Ministry of Health of Ethiopia. National adolescent and youth Health strategy (2016–2020); 2017. Available from: http://www.ncpd.go.ke/wp-content/uploads/2016/11/2015-National-Adolescents-and-Youth-Survey-Preliminary-Report.pdf.
15. Jones N, Baird S, Presler-Marshall E, et al. Adolescent well-being in Ethioipia: exploring gendered capabilities, contexts and change strategies. A synthesis report on GAGE Ethiopia baseline findings. An Exec Summ. 2019;2019:104.
16. Tanwi TS, Chakrabarty S, Hasanuzzaman S. Double burden of malnutrition among ever-married women in Bangladesh: a pooled analysis. BMC Womens Health. 2019;19(1):2–9. doi:10.1186/s12905-019-0725-2
17. Massad S, Deckelbaum RJ, Gebre-Medhin M, et al. Double burden of undernutrition and obesity in Palestinian schoolchildren. Food Nutr Bull. 2016;37(2):144–152. doi:10.1177/0379572116637720
18. Le DAS, Sagalova V, Sodjinou R, et al. Levels and trends of adolescent girl’s undernutrition and anemia in West and Central Africa from 1998 to 2017. J Glob Health. 2021;11:1–6.
19. Erismann S, Knoblauch AM, Diagbouga S, et al. Prevalence and risk factors of undernutrition among schoolchildren in the Plateau Central and Centre-Ouest regions of Burkina Faso. Infect Dis Poverty. 2017;6(1):1–14. doi:10.1186/s40249-016-0230-x
20. Gebreyohannes Y, Shiferaw S, Demtsu B, Bugssa G. Nutritional status of adolescents in selected government and private secondary schools of Addis Ababa, Ethiopia. Int J Nutr Food Sci. 2014;3(6):504. doi:10.11648/j.ijnfs.20140306.13
21. Gultie T. Nutritional status and associated factors among orphan children below the age of five years in Gondar City, Ethiopia. J Food Nutr Sci. 2014;2(4):179.
22. Wertz FJ, Giorgi A. The descriptive phenomenological method in psychology: a modified Husserlian approach. J Phenomenol Psychol. 2011;41(2):269–276. doi:10.1163/156916210X526079
23. Braun V, Clarke V. Using thematic analysis in psychology; in qualitative research in psychology. Uwe Bristol. 2006;3(2):77–101.
24. Bevan MT. A method of phenomenological interviewing. Qual Health Res. 2014;24(1):136–144. doi:10.1177/1049732313519710
25. Cleary M, Hayter M, Horsfall J. Data collection and sampling in qualitative research: does size matter? J Adv Nurs. 2012;2012:473–475.
26. Cypress B. Qualitative research methods: a phenomenological focus. Dimens Crit Care Nurs. 2018;37(6):302–309. doi:10.1097/DCC.0000000000000322
27. Friedman DR. Building blocks for diet-related food security analysis. Int Diet Data Expans Proj. 2021;2021:8–10.
28. Sandelowski M. Sample size in qualitative research. Res Nurs Health. 1995;18(2):179–183. doi:10.1002/nur.4770180211
29. Rodham K, Brewer H, Mistral W, Stallard P. Adolescents’ perception of risk and challenge: a qualitative study. J Adolesc. 2006;29(2):261–272. doi:10.1016/j.adolescence.2005.05.012
30. Nelson MC, Kocos R, Lytle LA, Perry CL. Understanding the perceived determinants of weight-related behaviors in late adolescence: a qualitative analysis among college youth. J Nutr Educ Behav. 2009;41(4):287–292. doi:10.1016/j.jneb.2008.05.005
31. Kruger R, Gericke G. A qualitative approach for exploration of feeding practices, knowledge, and attitudes on child nutrition framework. J Fam Ecol Consum Sci. 2010;32(1):36–45.
32. Rakhshanderou S, Ramezankhani A, Mehrabi Y, Ghaffari M. Determinants of fruit and vegetable consumption among Tehranian adolescents: a qualitative research. J Res Med Sci. 2014;19(6):482–489.
33. Martins J, Marques A, Sarmento H, Carreiro Da Costa F. Adolescents’ perspectives on the barriers and facilitators of physical activity: a systematic review of qualitative studies. Health Educ Res. 2014;30(5):742–755. doi:10.1093/her/cyv042
34. Krolner R, Rasmussen M, Brug J, Klepp K-I, Wind M, Due P. Determinants of fruit and vegetable consumption among children and adolescents: a review of the literature. Part II: qualitative studies. Int J Behav Nutr Phys Act. 2011;6(4):1–38.
35. Gonçalves H, González DA, Araújo CP, et al. Adolescents’ perception of causes of obesity: unhealthy lifestyles or heritage? J Adolesc Heal. 2012;51(SUPPL.6):S46–52. doi:10.1016/j.jadohealth.2012.08.015
36. Klein JD, Wilson KM, Sesselberg TS, Gray NJ, Yussman S, West J. Adolescents’ knowledge of and beliefs about herbs and dietary supplements: a qualitative study. J Adolesc Heal. 2005;37(5):409.e1–409.e7. doi:10.1016/j.jadohealth.2005.02.003
37. Kahsay A, Gebregziabher H, Hadush Z, Yemane D, Hailemariam A, Mulugeta A. Exploration of barriers to the uptake of nutritional services among adolescent girls from the rural communities of Tigray Region, Northern Ethiopia: a qualitative study. Adolesc Health Med Ther. 2020;11:157–171. doi:10.2147/AHMT.S276459
38. Getacher L, Egata G, Alemayehu T, Bante A, Molla A. Minimum dietary diversity and associated factors among lactating mothers in ataye district, North Shoa zone, central Ethiopia: a community-based cross-sectional study. J Nutr Metab. 2020;2020:5. doi:10.1155/2020/1823697
39. Getacher L, Egata G, Aynalem YA, et al. Food insecurity and its predictors among lactating mothers in North Shoa Zone, Central Ethiopia: a community based cross-sectional study. BMJ Open. 2020;10(11):1–9. doi:10.1136/bmjopen-2020-040627
40. Sondari M, Brouwer I, Februhartanty J. Eating behaviour of adolescent schoolgirls in Malang, East Java: a qualitative study. Malays J Nutr. 2019;25(23):S87–96.
41. Gavaravarapu SM, Rao KM, Nagalla B, Avula L. Assessing differences in risk perceptions about obesity among “normal-weight” and “overweight” adolescents—a qualitative study. J Nutr Educ Behav. 2015;47(6):488–497.e1. doi:10.1016/j.jneb.2015.07.001
42. Dapi LN, Omoloko C, Janlert U, Dahlgren L, Håglin L. “I eat to be happy, to be strong, and to live.” perceptions of rural and urban adolescents in Cameroon, Africa. J Nutr Educ Behav. 2007;39(6):320–326.
43. Ortega FB, Ruiz JR, Sjostrom M. Understanding environmental influences on nutrition and physical activity behaviors: where should we look and what should we count? Int J Behav Nutr Phys Act. 2007;4:61–71.
44. Dagnaw E. Determinants of overnutrition among secondary and preparatory school adolescents in Debre Berhan Town, North Shewa Zone, Amhara Region, Ethiopia, 2020 / 21 (unmatched case control study). Dsp Inst Inst Rep. 2021;21:1.
45. Caetano MC, Ortiz TT, Terreri MTSLR, et al. Inadequate dietary intake of children and adolescents with juvenile idiopathic arthritis and systemic lupus erythematosus. J Pediatr. 2009;85(6):509–515.
46. Stephens LD, McNaughton SA, Crawford D, Ball K. Nutrition promotion approaches preferred by Australian adolescents attending schools in disadvantaged neighbourhoods: a qualitative study. BMC Pediatr. 2015;15(1):1–12.
47. Fitzgerald A, Heary C, Nixon E, Kelly C. Factors influencing the food choices of Irish children and adolescents: a qualitative investigation. Health Promot Int. 2010;25(3):289–298.
48. Do Amaral E, Melo GR, Silva PO, et al. Family meal frequency and its association with food consumption and nutritional status in adolescents: a systematic review. PLoS One. 2020;15:1–29.
49. Mukanu MM, Thow AM, Delobelle P, McHiza ZJR. School food environment in Urban Zambia: a qualitative analysis of drivers of adolescent food choices and their policy implications. Int J Environ Res Public Health. 2022;19(12):1.
50. Kubberød E, Ueland Ø, Tronstad Å, Risvik E. Attitudes towards meat and meat-eating among adolescents in Norway: a qualitative study. Appetite. 2002;38(1):53–62.
51. Naughton P, McCarthy M, McCarthy S. Acting to self-regulate unhealthy eating habits. An investigation into the effects of habit, hedonic hunger and self-regulation on sugar consumption from confectionery foods. Food Qual Prefer. 2015;46:173–183.
52. Boyland EJ, Harris JL. Regulation of food marketing to children: are statutory or industry self-governed systems effective? Public Health Nutr. 2017;20(5):761–764.
53. Vandevijvere S, Soupen A, Swinburn B. Unhealthy food advertising directed to children on New Zealand television: extent, nature, impact and policy implications. Public Health Nutr. 2017;20(17):3029–3040.
54. Fisher L, Dahal M, Hawkes S, Puri M, Buse K. Barriers and opportunities to restricting marketing of unhealthy foods and beverages to children in Nepal: a policy analysis. BMC Public Health. 2021;21(1):1–13.
55. Taillie LS, Bercholz M, Popkin B, Reyes M, Colchero MA, Corvalán C. Changes in food purchases after the Chilean policies on food labelling, marketing, and sales in schools: a before and after study. Lancet Planet Heal. 2021;5(8):e526–33.
56. Zamora-Corrales I, Jensen ML, Vandevijvere S, Ramírez-Zea M, Kroker-Lobos MF. Television food and beverage marketing to children in Costa Rica: current state and policy implications. Public Health Nutr. 2019;22(13):2509–2520.
57. León-Flández K, Royo-Bordonada MÁ, Moya-Geromini MÁ, Bosqued-Estefanía MJ, López-Jurado L, Damián J. Marketing techniques in television advertisements of food and drinks directed at children in Spain, 2012. Int J Public Health. 2018;63(6):733–742.
58. Mawela A, van den Berg G. Management of school nutrition programmes to improve environmental justice in schools: a South African case study. South Afr J Clin Nutr. 2018;33(2):30–35.
59. World Health Organization, World Medical Association Declaration of Helsinki. Ethical principles for medical research involving human subjects. World Health Organization. 2001;79:373–374.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.