")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 13
Lithium in late-life mania: a systematic review
Authors De Fazio P, Gaetano R, Caroleo M, Pavia M , De Sarro G, Fagiolini A , Segura-Garcia C
Received 4 November 2016
Accepted for publication 2 December 2016
Published 9 March 2017 Volume 2017:13 Pages 755—766
DOI https://doi.org/10.2147/NDT.S126708
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Roger Pinder
Pasquale De Fazio, 1 Raffaele Gaetano, 1 Mariarita Caroleo, 1 Maria Pavia, 2 Giovanbattista De Sarro, 3 Andrea Fagiolini, 4 Cristina Segura-Garcia 1
1Department of Health Sciences, Psychiatric Unit, University Magna Græcia of Catanzaro, 2Department of Health Science, University Magna Græcia, 3Department of Health Sciences, Institute of Pharmacology, University Magna Græcia, Catanzaro, 4Department of Molecular Medicine, Division of Psychiatry, University of Siena, Siena, Italy
Abstract: The prevalence of mania among > 65-year-olds ranges from 0.1% to 0.4% and its treatment is a particular challenge for clinicians. Although lithium is the treatment of choice for bipolar disorder (BD), its use in elderly population was recently questioned. This study provides a comprehensive review of literature on the efficacy and tolerability of lithium as a pharmacologic treatment for mania in elderly BD patients. We conducted a systematic review, based on PRISMA guidelines, of articles published between 1970 and August 2016 and indexed in the following databases: EMBASE, MEDLINE, Cochrane Library Databases and PsycINFO. The key words “age”, “late-life”, “geriatric”, “elderly”, and “older” were combined with words indicating pharmacologic treatments, such as lithium and other mood stabilizers and with the diagnostic terms “bipolar disorder” and “mania”. Fifteen out of 196 retrieved studies met our inclusion criteria. Seven studies evaluated both the efficacy and tolerability of lithium treatment in elderly BD patients; a further three evaluated only the efficacy and five assessed tolerability. Only limited data on the treatment of elderly BD patients are available, but evidence suggests that lithium is effective and tolerated in this subgroup of patients and thus should remain a first-line drug. It seems to be more effective at lower doses and close monitoring of plasma concentrations is necessary.
Keywords: bipolar disorder, lithium, elderly, late-life mania, efficacy, tolerability
A Letter to the Editor has been published for this article.
Introduction
Bipolar disorder (BD) is a severe mood disorder characterized by recurrent mania or hypomania and depressive episodes, as defined in Diagnostic and Statistic Manual of Mental Disorders (DSM), 5th edition;1 it is frequently associated with functional and cognitive impairment2 and lower quality of life.3
The lifetime prevalence in community samples is ~2.8%.4,5 A recent meta-analysis of epidemiologic studies noted that the reported prevalence of BD ranged from 0.1% to 7.4%.6 BD is associated with a high risk of suicide.7
BD has a greater impact and higher mortality rate in elderly patients than in younger patients.8,9 Elderly individuals with BD constitute 5%–19% of patients presenting for acute treatment at geriatric psychiatry services10 and represent a particular challenge for clinicians. The reported prevalence of mania among >65-year olds ranges from 0.1% to 0.4%.11,12 Although the psychopathologic manifestations of mania are similar in the elderly and in younger bipolar patients, both the etiology and the response to treatment are extremely variable. Recent data support the hypothesis that in older patients the onset of BD may be related to neurologic or vascular diseases.13 Many neuroimaging studies have shown brain atrophy and cerebrovascular lesions in patients with BD.14
Frequently, mania in the elderly is due to medication or other medical conditions.15 Decisions about the pharmacologic treatment of elderly BD patients must consider safety and tolerability as much as effectiveness.
Elderly people are a heterogeneous group of patients who tend to have comorbidities and poor outcomes. After recognition of BD and careful diagnostic assessment, pharmacotherapy represents the cornerstone of their management. Lithium remains the treatment of choice for bipolar mania in elderly patients.16 Although lithium has greater proven efficacy than other mood stabilizers with respect to treating and preventing manic episodes and reducing suicidal behavior17 there is a dearth of good studies of its use in the elderly population. Its use in this group is based mainly on pharmacokinetic studies and clinical experience18,19 rather than on methodologically rigorous trials. Preliminary data suggest that lithium may have neuroprotective properties and reduce the risk of developing dementia.20
The physiologic changes and the comorbid physical and psychiatric illnesses associated with age can increase vulnerability to side-effects and limit the dosage and, hence, benefits of drug therapies.21 Furthermore, there has been very little epidemiologic research into treatment of late-life mania.15 Given the high risk of lithium overdose close monitoring of plasma levels of the drug is necessary. The variable pharmacodynamics, comorbidities and frequent polypharmacy in the geriatric population mean that it is highly susceptible to life-threatening changes in plasma levels of lithium. Many drugs used in the elderly can increase plasma levels of lithium.22
Lithium and antipsychotics are the agents of choice for treating a manic episode occurring as part of BD and for treating secondary mania.23 Lithium is the oldest mood stabilizer and still one of the most frequently prescribed for the treatment of BD, but it is often replaced by newer mood-stabilizing agents, such as valproic acid, despite the lack of evidence to support such a change in prescription pattern.24 Although expert reviews and guidelines continue to recommend the use of lithium, clinicians’ drug prescription patterns in older adults are changing. The decrease in lithium prescriptions appears to be due to safety concerns.25
This research sought to systematically review evidence from the last 15 years on the use of lithium as an acute and maintenance treatment for BD in elderly patients. Few blind, randomized, placebo-controlled trials of mood stabilizers have been conducted in the older bipolar population.24
Age-specific information on risks and benefits consists, with few exceptions, of case reports and case series based on retrospective data. There is thus a clear lack of evidence to assist clinicians in planning treatment based on an individualized assessment of risks and benefits. Treatment recommendations and guidelines for older adults are based on extrapolation from mixed-age populations or small samples of elderly patients. The limited availability of information on which to base clinical management is striking; guidelines for pharmacotherapy of younger BD patients cannot be directly extrapolated to the care of elderly populations.26
Earlier studies suggested that older people with manic BD show a reduced response to anti-manic and mood stabilizing agents.27 The lack of placebo-controlled trials means that there is continuing uncertainty about the efficacy of mood stabilizers in treating geriatric BD. This systematic review analyses the available data on the efficacy and tolerability of lithium as a treatment for mania in late-life BD patients. According to epidemiologic data, the clinical features and other age-related factors could influence treatment with lithium and its pharmacokinetic and pharmacodynamic properties. The following discussion aimed to propose lithium as a useful tool in clinical practice.
Methodology
Data sources
Articles on the pharmacologic treatment of BD in the elderly published between 1970 and August 2016 in all languages were identified by searching MEDLINE, EMBASE, PsychINFO and Cochrane Library. The following MESH search string was used: Bipolar Disorder OR Mania AND Lithium AND geriatric OR elderly OR aged OR late-life AND efficacy AND tolerability OR safety. The search strategy is shown in Figure 1.
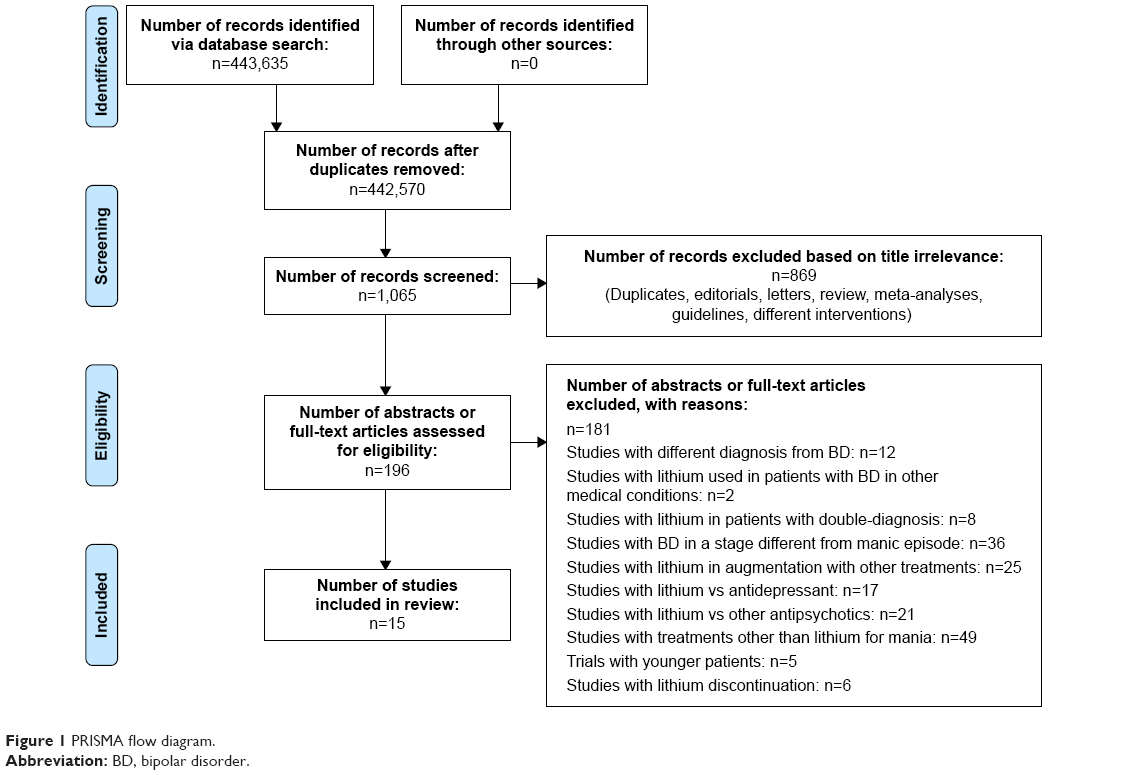 | Figure 1 PRISMA flow diagram. |
Two of the authors independently reviewed all the retrieved studies. Additional data sources included the reference lists of retrieved articles. To improve the clarity and transparency of the review process, we followed the criteria and the key recommendations of the PRISMA statement;28 where full-text articles were not available directly from the online databases or at the university, the authors were contacted to obtain a copy.
Assessment of study quality
This systematic review employed the Jadad29 rating system to check the methodologic quality of studies. Jadad’s procedure enables qualification of a study according to the clearness in describing the randomization, the double blind procedure and the report of withdrawals and dropouts. The score can range between 0 and 5. For this systematic review the inclusion criteria was a Jadad score >3.
Selection criteria
“Elderly” was defined as ≥65 years, as in most of the studies we examined. Nevertheless, we extended our research to patients from the age of 50 until old–old patients (ie, >85 years old people). Seminal articles on lithium therapy for BD in mixed-age samples were included because of their evaluation of age effects. All relevant original articles were reviewed and reported. Conclusion regarding therapy were based primarily on studies with >10 patients. Relevant publications were identified, and the full text of these articles were retrieved and reviewed. Useful publications identified from the reference lists of retrieved articles were also included in this review.
The inclusion criteria were as follows: 1) patients (of either sex) were aged ≥50 years and affected with BD, and the study evaluated the efficacy and safety of lithium in the treatment and prevention of the manic episode; 2) mixed-age samples; 3) sample size of at least ten patients; 4) studies comparing lithium monotherapy with other mood stabilizers or placebo using the main BD psychopathology scales to evaluate outcomes; and 5) evaluations of the tolerability of lithium measured as frequency of discontinuation of lithium.
Studies were excluded if: 1) lithium was prescribed for psychiatric disorders other than BD; 2) lithium was prescribed for patients with BD secondary to general medical condition (GMC); 3) treatment with lithium for other psychiatric diseases; 4) lithium was used to treat other episodes in addition to mania; 5) lithium was used to augment other treatments; and 6) lithium was compared with other classes of drug (antidepressants, typical and atypical antipsychotics).
Results
The combined search string retrieved 443,635 papers (Figure 1) of which only 1,065 were considered sufficiently relevant to warrant review of the abstract. Eight hundred sixty-nine were excluded because they were editorials, letters to editors, reviews, meta-analyses or case reports. One hundred eighty-one out of 196 papers were excluded because they did not fulfill the criteria for inclusion. Only two out of the 15 included studies were randomized clinical trials. Seven studies evaluated both the efficacy and tolerability of lithium in elderly BD patients, a further eight evaluated either efficacy (n=3) or tolerability (n=5). Relevant references in these publications were also identified and reviewed. The eligible publications have been included and cited in this review. Included studies are described in Tables 1 and 2.
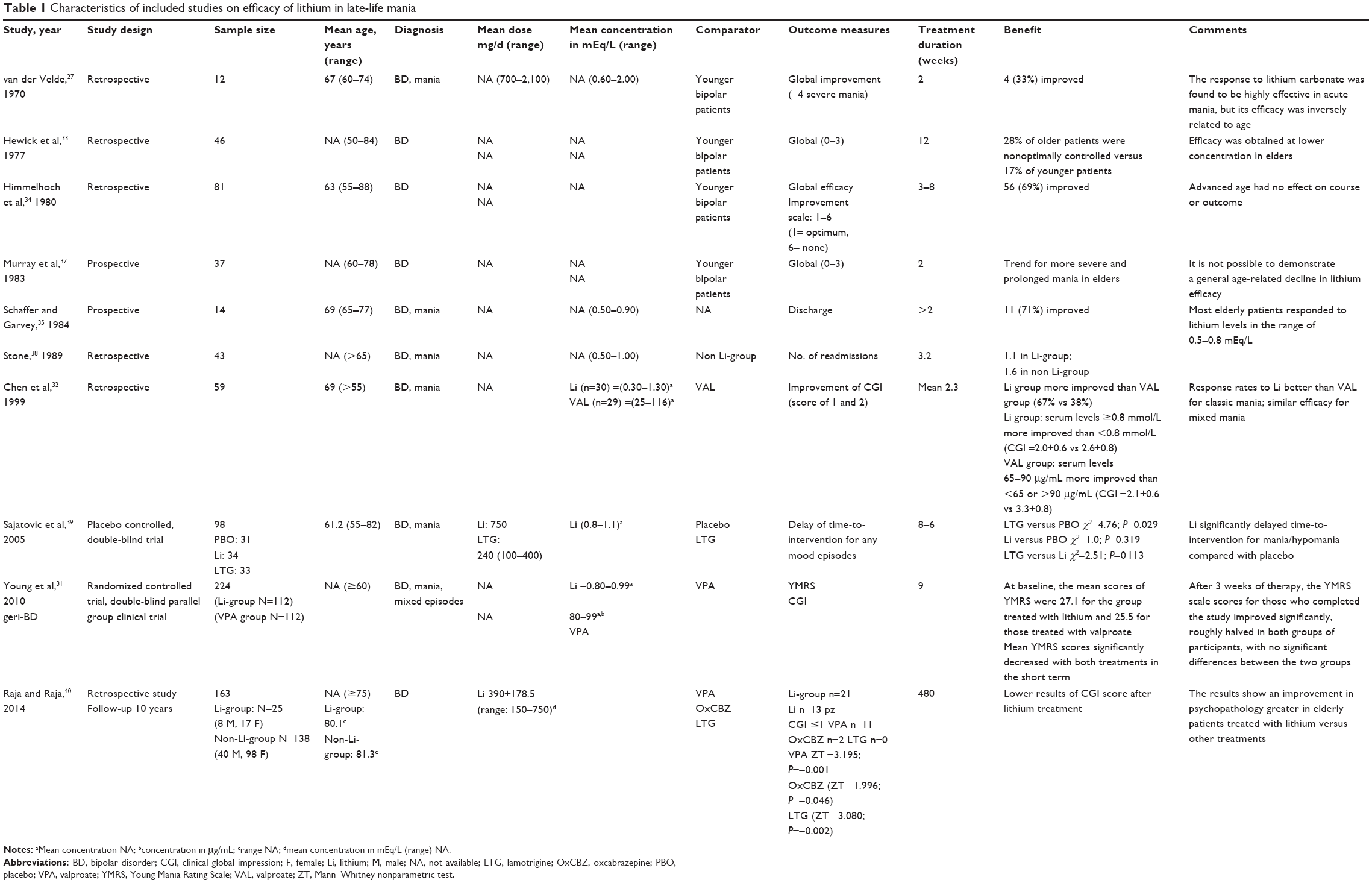 | Table 1 Characteristics of included studies on efficacy of lithium in late-life mania |
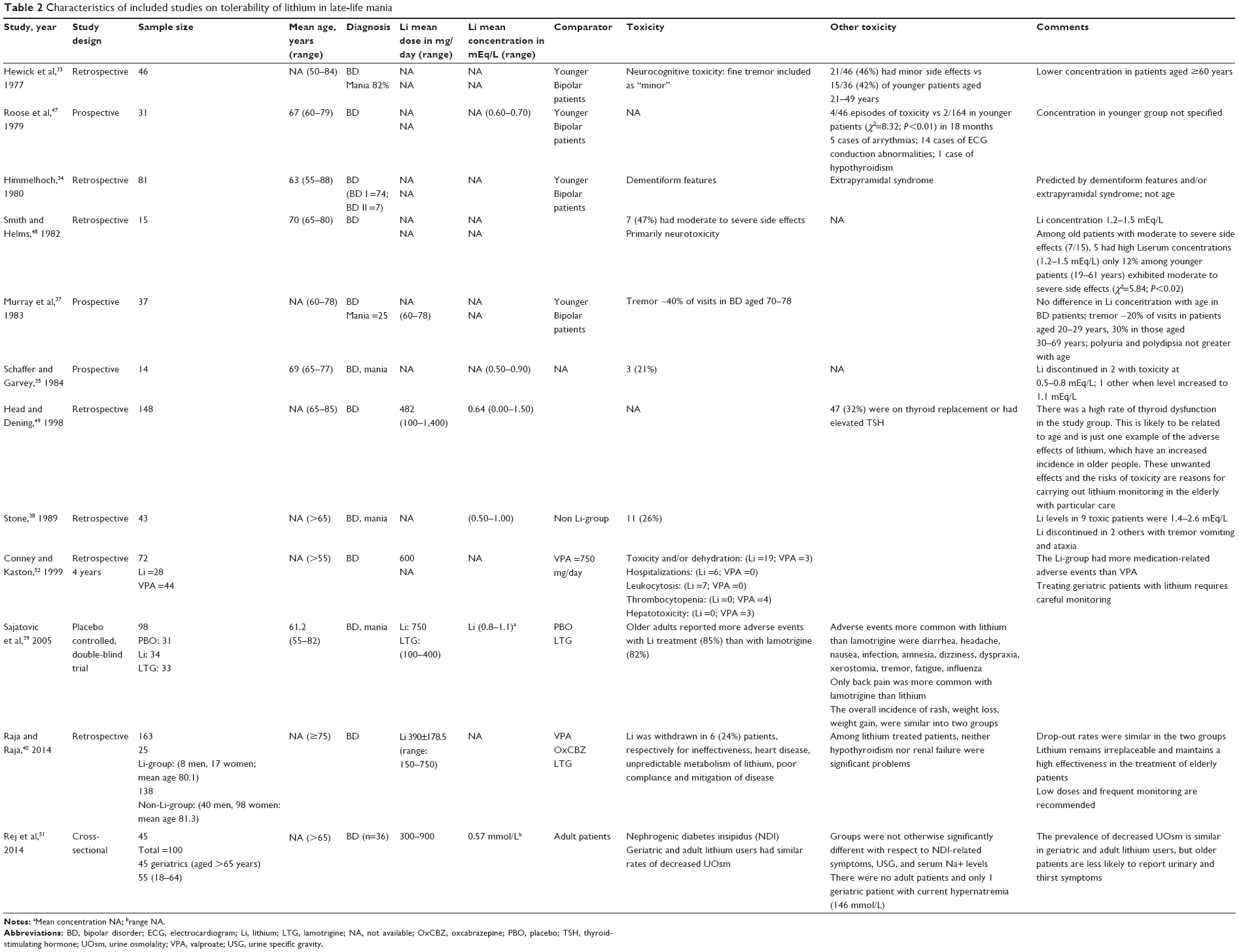 | Table 2 Characteristics of included studies on tolerability of lithium in late-life mania |
Discussion
Efficacy of lithium in late-life bipolar mania
Lithium as a treatment for psychiatric disorders has been studied for >50 years. Over the past four decades multiple studies have validated lithium as the gold standard treatment for BD.25 However, there are few placebo-controlled, double-blind, clinical trials in elderly patients on which to base an assessment of its efficacy and tolerability in this population. Most studies have used naturalistic or retrospective designs. Our literature search identified only two randomized trials of the effectiveness of lithium in late-life mania,30,31 although there were more observational and retrospective studies.27–32
Early studies of the effectiveness of lithium in the elderly used younger bipolar patients as a comparison group and were methodologically very flawed. van der Velde27 showed that lithium was less therapeutically effective in patients >60 years old than in a comparison group of younger patients aged <60 years. These authors were the first to report on responses to lithium carbonate in manic-depressive patients. Lithium carbonate was found to be highly effective as a treatment for acute manic episodes, but its efficacy was inversely related to age. Only three out of the 12 elderly patients responded to treatment with lithium, compared with 51 out of 63 young patients. During the 3 years of follow-up only 8% of elderly patients treated with lithium became clinically stable, compared with 58% of the younger group. Younger patients clearly had superior responses to the drug both during acute episodes of illness and when used as a maintenance treatment. The findings of van der Velde were partially replicated by Hewick et al33 in a retrospective study of 46 BD patients treated with lithium for 12 weeks: treatment with lithium was less effective in the elderly subgroup than in the younger subgroup (28% and 17% of nonresponse, respectively). The mean daily dose of lithium required to reach adequate plasma levels was significantly lower in patients >50 years old. Subsequent studies have, however, reported that lithium is effective for the treatment of acute mania in elderly BD inpatients32,34,35 with an average positive response of 72%, which is comparable to the 78% achieved in younger patients.
In a sample of 30 inpatients aged ≥55 years, Chen et al32 found that lithium was more effective (Clinical Global Impression [CGI] score classed as “improved” or “much improved”) for those with typical manic symptoms than for those with mixed features. Himmelhoch et al34 examined the effectiveness of lithium in 81 patients >55 years undergoing a manic episode and found that 56% of them responded well to lithium. They concluded that although advanced age had no effect on the course or outcome of a manic episode, the response rate for treatment with lithium was lower in patients with comorbid neurologic and/or substance abuse. Many authors have corroborated their main finding, showing that age of onset of BD did not seem to influence the effectiveness of lithium.36
Subsequent studies have clarified the relationship between age and lithium efficacy based on evaluations of patients hospitalized during the manic phase of BD. A prospective study of patients on long-term lithium treatment37 found a higher incidence and severity of manic attacks related to age in a subgroup of elderly patients; however, this was not associated with an increase in the frequency of hospitalization or an age-related decline in lithium efficacy. A retrospective study of 92 patients aged >65 years old who were hospitalized during acute manic episodes, of whom 43 were treated with lithium found that lithium therapy produced little benefit in terms of readmissions. The main limitation of this study was the method of randomization.38
Modern studies have compared lithium with other treatments for mania and demonstrated that lithium has superior or similar efficacy to other mood stabilizers. Our literature search identified only two randomized trials of the effectiveness of lithium in late-life mania.31,39 These trials used rating scales to quantify the severity of manic symptoms.
Sajatovic et al39 evaluated the efficacy of lithium and lamotrigine versus placebo in a subgroup of 34 elderly patients. They found that lithium reduced manic symptoms (as assessed by CGI) and was more effective in reducing subsequent incidence of manic, hypomanic and mixed episodes than placebo or lamotrigine. Lamotrigine was, however, better than lithium at preventing recurrence of depressive episodes. Lithium and valproate were found to be similarly effective in treating mania in elderly patients with BD in a prospective randomized trial, geriatric bipolar disorder (GERI-BD). The study enrolled 224 elderly BD patients in six North American sites with mania or hypomania (Young Mania Rating Scale [YMRS] score ≥18) at the time of the first observation; patients with rapid cycling or dementia were excluded. Half the sample (n=112; mean [M] age 67.6 years; 50% men) received lithium (0.80–0.99 mEq/L) and the other half (n=112, M age =67.6 years old, 53% men) were treated with 80–99 μg/mL of valproate with the possibility of augmentation with risperidone and lorazepam after 3 weeks of treatment if there was no improvement. The efficacy of both therapies was evaluated using the YMRS and CGI-bipolar (BP) at days 4, 9, 15, 21 and then weekly. The mean YMRS scores at baseline were 27.1 and 25.5 for the lithium and valproate groups, respectively. After 3 weeks of therapy the YMRS scores for those who completed the study had roughly halved in both groups and there was no significant difference in efficacy between lithium and valproate.31
The most recent study included in this review confirmed this result. A recent retrospective, naturalistic study of patients aged ≥75 years provided clear and comprehensive evidence for the efficacy and safety of lithium and answered many of the outstanding questions from previous studies. A group of 25 patients treated with lithium was compared with patients who received other therapies. The lithium group showed a bigger improvement in CGI score.40 Although it is difficult to compare the effectiveness of lithium across a very heterogeneous sample of studies, the most recent research provides some accurate information about the efficacy of lithium in the elderly.
Tolerability of lithium in late-life bipolar mania
This review considered the tolerability of lithium in terms of both side-effects and treatment discontinuation. Very few trials have evaluated lithium tolerability in the elderly although most of those that report on its efficacy in this population also report tolerability. This review included both retrospective and prospective studies extrapolated from a population with mixed age. The search only identified one randomized-controlled trial that evaluated the tolerability of lithium as a treatment for manic episodes in the elderly.39 Age-related changes in the pharmacokinetics and pharmacodynamics of lithium make it less safe to use in older adults with BD.41 Renal function decreases with age, so there is an increased risk of toxicity in older patients.41–43
The reduction in renal function can be exacerbated by the toxic effects of lithium. A cross-sectional study compared a group of 61 patients treated with lithium for 16 years with a group of 53 patients receiving electroconvulsive treatment (ECT). Just over one-third (34.4%) of patients treated with lithium developed chronic renal failure compared with 15.1% of the ECT group.44 A recent study of the treatment of adult BD that compared patients aged >60 years with patients aged 20–59 years demonstrated that in elderly patients lithium was prescribed less frequently (29.5% vs 37.8%, P=0.02) and at lower doses (689 vs 1,006 mg/dL; P<0.0001); nevertheless the rate of recovery was twice as high among elderly patients (42.1% vs 21.3%). The authors hypothesized that the greater effectiveness of lithium could be related to the better tolerability of lithium monotherapy.45
A dated retrospective study of 82 psychiatric outpatients aged 21–84 years on therapy with lithium, of whom 37 were in the manic phase, reported that ~46% developed minor side-effects (polyuria, polydipsia, weight gain and edema) but there was no difference between patients under and over 50 years of age. Clinicians reduced the daily weight-related dose of lithium by 50% in older patients to allow lithium excretion and to reduce side-effects to a level comparable to that in younger patients.33
The adverse effects of treatment with lithium may involve various organs and systems: central nervous system, gastrointestinal system, cardiovascular system, endocrine system and kidneys. The elderly may be more susceptible to cognitive impairment and delirium34–37 and there is evidence that neurotoxicity may continue for weeks after discontinuation of treatment, even when serum levels are under range or undetectable.46 A prospective study of 31 patients aged between 60 and 79 years who were treated with lithium found that they were more likely to suffer toxic effects (58% showed electrocardiogram [ECG] changes related to treatment) and had lower serum concentrations of the drug than a younger comparison group.47 Other studies have corroborated these findings, reporting higher rates of adverse reactions and toxicity in elderly patients treated with lithium, who have serum levels considered normal for the adult population.37,38,48 A retrospective evaluation of 92 patients >65 years hospitalized for a manic episode assessed the efficacy and tolerability of lithium therapy in 43 patients. Twenty-six percent of patients treated with lithium showed evidence of toxicity; their plasma concentration of lithium ranged from 1.4 to 2.6 mEq/L. Two patients dropped out because of tremor, vomiting and ataxia. Head and Dening49 retrospectively evaluated lithium treatment in a sample of 148 elderly patients (65–85 years). Similar to others50 their most salient finding was that 32% of patients showed either elevated thyroid-stimulating hormone levels or required levothyroxine replacement therapy, suggesting that hypothyroidism is quite frequent in elderly patients receiving lithium.
Diabetes insipidus, defined as urinary volume ≥3 L/24 h or urine osmolality (UOsm) ≤300 mOsm/kg, is a problematic endocrine side-effect of lithium therapy. It is frequently found in adult patients who take lithium for >5 years, and it is even more frequent in the elderly. Polyuria, polydipsia and hypernatremia are all symptoms suggestive of diabetes insipidus. This clinical picture, in addition to being a severe GMC, requires discontinuation of treatment, leading to a higher rate of relapse. A very recent cross-sectional study of 100 BD patients receiving lithium (45 patients aged >65 years; 55 patients aged 18–64 years) compared the prevalence of diabetes insipidus and low UOsm (<300 mOsm/kg) in the two groups. Although both groups showed similar rates of low UOsm, the older group reported fewer symptoms. Because age, duration of lithium therapy and serum lithium level were all independently associated with UOsm despite the relative lack of subjective symptoms, the authors recommended close monitoring of serum lithium levels and routine screening for decreased UOsm in elderly patients.51
Raja and Raja40 assessed both the efficacy and tolerability of lithium in elderly patients. They found that dropout rates for lithium therapy were comparable to those for other drugs. Hypothyroidism and renal failure were significant problems in patients receiving lithium. Lithium therapy was discontinued in six patients (24%) owing to ineffectiveness (n=1), heart disease not related to lithium treatment (n=1), abnormal metabolism of lithium (n=1), poor adherence to therapy (n=2) and poor clinical improvement (n=1). The authors concluded that treatment with lithium was highly effective in elderly patients and recommended a low dose regime with frequent monitoring of plasma levels.
Another retrospective study of 72 BD patients aged over 55 years estimated the frequency and costs of adverse events associated with lithium or valproate therapy over a 4-year period. The lithium group reported more medication-related adverse events and more severe side-effects than the valproate group. It appears, therefore, that patients being treated with lithium need to be monitored more carefully than those treated with other drugs, because of the increased risk of side-effects; this means that lithium treatment is more expensive than treatment with valproate.52 Sajatovic et al39 evaluated the efficacy and tolerability of mood stabilizers in a double-blind trial involving 588 elderly patients with BD. Patients received lamotrigine (100–400 mg/day), lithium (0.8–1.1 mEq/L) or placebo. The lithium group (n=98) and lamotrigine group had similar rates of side-effects (85% vs 82%, respectively); the adverse events most frequently (>10% of patients) associated with lithium treatment were dyspraxia, tremor, xerostomia, headache, infection, amnesia, dizziness, diarrhea, nausea and fatigue.
Strengths and limitations of the study
To the best of our knowledge, this is the first review to compare the most recent data with the oldest evaluations of lithium efficacy in old patients with bipolar mania. We have also examined the factors affecting lithium tolerability in late life. The possible limitations of this review include the heterogeneity of the included studies, such as the main clinical features of patients, the mean dosage and the blood concentration of lithium. However, the inclusion criteria were designed to select patients for lithium treatment as accurately as possible.
Conclusion
Lithium remains one of the drugs of choice for the treatment of mania in elderly patients with BD. Despite the very strong evidence for its effectiveness there are significant concerns about the tolerability of lithium in the older population. There have been very few controlled studies of the efficacy and safety of lithium among the elderly and use of the drug is probably decreasing because of the risks of interactions with other drugs and its toxicity.
Assessing response to treatment in elderly BD patients is complicated by comorbid medical conditions and drug interactions; nevertheless, we conclude that lithium should still be considered the first choice agent for treatment of mania in BD. Very little evidence supports the use of alternative drugs, such as other mood-stabilizing agents or atypical antipsychotics, in older adults. The currently available data suggest that other drugs, such as valproate, may be as therapeutically effective and better tolerated but at present there is not enough evidence to recommend switching to another mood stabilizer. Lithium, therefore, remains the first-choice drug for treatment of BD in the geriatric population. Lower plasma concentrations of lithium than those usually considered effective in adults, appear to be useful and well-tolerated among older patients. Moreover, it has been reported that BD patients have a higher risk of cognitive impairment and dementia than the general population and recent preclinical and clinical studies suggest that lithium has potential neuroprotective functions.53
Our systematic review of recent evidence underlines the need for close monitoring of plasma concentrations of lithium in the elderly. It also suggests that in the elderly lithium is as effective and better tolerated at lower doses.
Disclosure
The authors report no conflicts of interest in this work.
References
American Psychiatric Association. DSM-V Diagnostic and Statistic Manual of Mental Disorders. Milano: Masson, 2013. | ||
Jansen K, Magalhães PV, Tavares Pinheiro R, Kapczinski F, Silva RA. Early functional impairment in bipolar youth: a nested population-based case-control study. J Affect Disord. 2012;142(1–3):208–212. | ||
Gutierrez-Rojas L, Gurpegui M, Ayuso-Mateos JL, Gutierrez-Ariza JA, Ruiz-Veguilla M, Jurado D. Quality of life in bipolar disorder patients: a comparison with a general population sample. Bipolar Disord. 2008;10(5):625–634. | ||
Merikangas KR, Akiskal HS, Angst J, et al. Lifetime and 12-month prevalence of bipolar spectrum disorder in the National Comorbidity Survey replication. Arch Gen Psychiatry. 2007;64(5):543–552. | ||
Kessler RC, Ormel J, Petukhova M, et al. Development of lifetime comorbidity in the World Health Organization world mental health surveys. Arch Gen Psychiatry. 2011;68(1):90–100. | ||
Montes JM, Alegria A, Garcia-Lopez A, et al. Understanding bipolar disorder in late life: clinical and treatment correlates of a sample of elderly outpatients. J Nerv Ment Dis. 2013;201(8):674–679. | ||
Lala SV, Sajatovic M. Medical and psychiatric comorbidities among elderly individuals with bipolar disorder: a literature review. J Geriatr Psychiatry Neurol. 2012;25(1):20–25. | ||
Shulman KI, Tohen M, Satlin A, Mallya G, Kalunian D. Mania compared with unipolar depression in old age. Am J Psychiatr. 1992;149(3):341–345. | ||
Bartels SJ, Forester B, Miles KM, Joyce T. Mental health service use by elderly patients with bipolar disorder and unipolar major depression. Am J Geriatr Psychiatry. 2000;8(2):160–166. | ||
Yassa R, Nair V, Nastase C, Camille Y, Belzile L. Prevalence of bipolar disorder in a psychogeriatric population. J Affect Disord. 1988;14(3):197–201. | ||
Dols A, Kupka RW, Van Lammeren A, Beekman AT, Sajatovic M, Stek ML. The prevalence of late-life mania: a review. Bipolar Disord. 2014;16(2):113–118. | ||
Brieger P, Hensel J, Marneros A. Bipolar affective and schizoaffective disorders of older age – classification, symptoms and course. Neurol Psychiatr. 2005;73(6):343–351. | ||
Sami M, Khan H, Nilforooshan R. Late onset mania as an organic syndrome: a review of case reports in the literature. J Affect Disord. 2015;188:226–231. | ||
de Melo RC, Lopes R, Alves JC. Bipolar disorder after stroke in an elderly patient. Case Rep Psychiatry. 2014;2014:741934. | ||
van Lammeren A, Dols A, van Gerven H, Kupka RW, Stek ML. Manie op latere leeftijd bipolaire stoornis als diagnose per exclusionem. Mania in late life: bipolar disorder as diagnosis by exclusion. Tijdschr Psychiatr. 2011;53(11):813–823. | ||
Young RC. Evidence-based pharmacological treatment of geriatric bipolar disorder. Psychiatr Clin North Am. 2005;28:837–869. | ||
Baldessarini RJ, Tondo L, Davis P, Pompili M, Goodwin FK, Hennen J. Decreased risk of suicides and attempts during long-term lithium treatment: a meta-analytic review. Bipolar Disord. 2006;8(5):625–639. | ||
Sproule BA, Hardy BG, Shulman KI. Differential pharmacokinetics of lithium in elderly patients. Drugs Aging. 2000;16(3):165. | ||
Tueth MJ, Murphy TK, Evans DL. Special considerations: use of lithium in children, adolescents, and elderly populations. J Clin Psychiatry. 1998;59(Suppl 6):66–73. | ||
Kessing LV, Forman JL, Andersen PK. Does lithium protect against dementia? Bipolar Disord. 2010;12(1):87–94. | ||
Schatzberg AF, Liptzin B, Satlin A, Cole JO. Diagnosis of affective disorders in the elderly. Psychosomatics. 1984;25(2):126–128. | ||
Dunner DL. Optimizing lithium treatment. J Clin Psychiatry. 1997;58(7):76–81. | ||
Aziz R, Lorberg B, Tampi RR. Treatments for late-life bipolar disorder. Am J Geriatr Pharmacother. 2006;4(4):347–364. | ||
Young RC, Gyulai L, Mulsant BH, et al. Pharmacotherapy of bipolar disorder in old age: review and recommendations. Am J Geriatr Psychiatry. 2004;12(4):342–357. | ||
Shulman KI. Lithium for older adults with bipolar disorder: should it still be considered a first-line agent? Drugs Aging. 2010;27(8):607–615. | ||
Nivoli AMA, Murru A, Goikolea JM, et al. New treatment guidelines for acute bipolar mania: a critical review. J Affect Disord. 2012;140(2):125–141. | ||
van der Velde CD. Effectiveness of lithium carbonate in the treatment of manic-depressive illness. Am J Psychiatry. 1970;127(3):345–351. | ||
Welch V, Petticrew M, Petkovic J, et al. Extending the PRISMA statement to equity-focused systematic reviews (PRISMA-E 2012): explanation and elaboration. J Clin Epidemiol. 2016;70:68–89. | ||
Jadad AR, Moore RA, Carroll D, et al. Assessing the quality of reports of randomized clinical trials: is blinding necessary? Control Clin Trials. 1996;17(1):1–12. | ||
Sajatovic M, Madhusoodanan S, Coconcea N. Managing bipolar disorder in the elderly. Drugs Aging. 2005;22(1):39–54. | ||
Young RC, Schulberg HC, Gildengers AG, et al. Conceptual and methodological issues in designing a randomized, controlled treatment trial for geriatric bipolar disorder: GERI-BD. Bipolar Disord. 2010;12(1):56–67. | ||
Chen ST, Altshuler LL, Melnyk KA, Erhart SM, Mille E, Mintz J. Efficacy of lithium vs valproate in the treatment of mania in the elderly: a retrospective study. J Clin Psychiatry. 1999;60(3):181–186. | ||
Hewick DS, Newbury P, Hopwood S, Naylor G, Moody J. Age as a factor affecting lithium therapy. Br J Clin Pharmacol. 1977;4(2):201–205. | ||
Himmelhoch JM, Neil JF, May SJ, Fuchs CZ, Licata SM. Age, dementia, dyskinesias, and lithium response. Am J Psychiatry. 1980;137(8):941–945. | ||
Schaffer CB, Garvey MJ. Use of lithium in acutely manic elderly patients. Clin Gerontol. 1984;3:58–60. | ||
Wylie ME, Mulsant BH, Pollock BG, et al. Age at onset in geriatric bipolar disorder. Effects on clinical presentation and treatment outcomes in an inpatient sample. Am J Geriatr Psychiatry. 1999;7(1):77–83. | ||
Murray N, Hopwood S, Balfour DJ, Ogston S, Hewick DS. The influence of age on lithium efficacy and side-effects in out-patients. Psychol Med. 1983;13(1):53–60. | ||
Stone K. Mania in the elderly. Br J Psychiatry. 1989;155:220–224. | ||
Sajatovic M, Gyulai L, Calabrese JR, et al. Maintenance treatment outcomes in older patients with bipolar I disorder. Am J Geriatr Psychiatry. 2005;13(4):305–311. | ||
Raja M, Raja S. Lithium treatment in elderly patients affected by mood disorders. Riv Psichiatr. 2014;49(4):180–182. | ||
Gyulai L, Young RC. New research perspectives in the treatment of bipolar disorder in older adults. Bipolar Disord. 2008;10(6):659–661. | ||
Hardy BG, Shulman KI, Mackenzie SE, et al. Pharmacokinetics of lithium therapy. J Clin Psychopharmacol. 1987;4:201–205. | ||
Fenn HH, Bauer MS, Altshuler L, et al. Medical comorbidity and health-related quality of life in bipolar disorder across the adult age span. J Affect Disord. 2005;86(1):47–60. | ||
Tredget J, Kirov A, Kirov G. Effects of chronic lithium treatment on renal function. J Affect Disord. 2010;126(3):436–440. | ||
Al Jurdi RK, Marangell LB, Petersen NJ, Martinez M, Gyulai L, Sajatovic M. Prescription patterns of psychotropic medications in elderly compared with younger participants who achieved a “recovered” status in the systematic treatment enhancement program for bipolar disorder. Am J Geriatr Psychiatry. 2008;16(11):922–933. | ||
Nambudiri DE, Meyers BS, Young RC. Delayed recovery from lithium neurotoxicity. J Geriatr Psychiatry Neurol. 1991;4(1):40–43. | ||
Roose SP, Nurnberger JI, Dunner DL, Blood DK, Fieve RR. Cardiac sinus node dysfunction during lithium treatment. Am J Psychiatry. 1979;136(6):804–806. | ||
Smith RE, Helms PM. Adverse effects of lithium therapy in the acutely ill elderly patient. J Clin Psychiatry. 1982;43(3):94–99. | ||
Head L, Dening T. Lithium in the over-65s: who is taking it and who is monitoring it? A survey of older adults on lithium in the Cambridge mental health services catchment area. Int J Geriatr Psychiatry. 1998;13(3):164–171. | ||
Grandjean EM, Aubry J-M. Lithium: updated human knowledge using an evidence-based approach: part III: clinical safety. CNS Drugs. 2009;23(5):397–418. | ||
Rej S, Beaulieu S, Segal M, et al. Lithium dosing and serum concentrations across the age spectrum: from early adulthood to the tenth decade of life. Drugs Aging. 2014;31(12):911–916. | ||
Conney J, Kaston B. Pharmacoeconomic and health outcome comparison of lithium and divalproex in a VA geriatric nursing home population: influence of drug-related morbidity on total cost of treatment. Am J Manag Care. 1999;5(2):197–204. | ||
Diniz BS, Machado-Vieira R, Forlenza OV. Lithium and neuroprotection: translational evidence and implications for the treatment of neuropsychiatric disorders. Neuropsychiatr Dis Treat. 2013;9:493–500. |
 © 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2017 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.