")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 16
Listening to Caregivers: Narratives of Health Seeking for Children Under Five with Pneumonia and Diarrhea: Insights from the NIGRAAN Trial in Pakistan
Authors Huda M , Rabbani F, Shipton L, Aftab W, Khan KS, Marini MG
Received 13 April 2023
Accepted for publication 13 October 2023
Published 24 November 2023 Volume 2023:16 Pages 3629—3640
DOI https://doi.org/10.2147/JMDH.S417102
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Maryam Huda,1 Fauziah Rabbani,1,2 Leah Shipton,1,3 Wafa Aftab,1 Kausar S Khan,1 Maria Giulia Marini4
1Department of Community Health Sciences, Aga Khan University, Karachi, Pakistan; 2Brain & Mind Institute, Aga Khan University, Karachi, Pakistan; 3Dalla Lana School of Public Health, University of Toronto, Toronto, Canada; 4Research and Health Care Director, Fondazione ISTUD per la Cultura d’Impresa e di Gestione, Milan, Italy
Correspondence: Fauziah Rabbani, Email [email protected]
Background: Understanding health-seeking behaviors of caregivers is important to reduce child mortality. Several factors influence decision-making related to childhood illnesses.
Objective: The objective of this study was to gather caretaker narratives to develop a comprehensive understanding of the context and process of caregiving at household level during all stages of an episode of diarrhea and pneumonia in children < 5.
Methods: Using a narrative interview approach, stories from caregivers of children < 5 were collected from a rural district in Sindh Pakistan. Eleven households with children < 5 were randomly selected and purposive sampling was done to interview 20 caregivers. All data collection was conducted privately in participants’ homes and informed consent taken. Manual content analysis was carried out by three independent researchers and emerging themes drawn.
Results: The role of joint family system is integral in making decisions and the child’s paternal grandmother, is an important and trusted source of information regarding child sickness in the household. They often promote home remedies with considerable authority prior to formal consultation with the health care system. Caregivers were generally dissatisfied with doctors in the public sector who were perceived to be providing free consultation with a poor quality of care and long waiting time as compared to private doctors. Financial considerations and child support were favorably addressed in households with a joint family system.
Conclusion: The joint family system provides a strong support system, but also tends to reduce parental autonomy in decision-making and delay first contact with formal health providers. Prevalent home remedies, and authority of elders in the family influence management practices. Interventions for reducing improving child mortality should be cognizant of the context of decision-making and social influences at the household level.
Keywords: narrative interviews, health-seeking behavior, joint family system, pneumonia, diarrhea, children < 5, caregivers
Background
The devastating impact of pneumonia and diarrhea on child mortality in low and middle-income countries (LMICs) is well documented1,2. Worldwide, 15% and 9% of deaths are attributable to pneumonia and diarrhea, respectively, with 74% of the global burden skewed to 15 LMICs in sub-Saharan Africa and South Asia.1,3,4 Social determinants such as poverty, inaccessible health services, and poor water quality and sanitation infrastructure create conditions for malnutrition, unhygienic practices and indoor air pollution that are direct risk factors for pneumonia and diarrhea.1,5,6 Pakistan is the third country carrying the greatest burden of child mortality with approximately 90,398 deaths from pneumonia and diarrhea in 2020.7
Access to health services is an important aspect of reducing child mortality and is influenced by health-seeking behaviors of caregivers.5,8,9 Yet the 2017–2018 Demographic Health Survey in Pakistan found that on average 84% and 71% of caregivers seek treatment from health facilities for pneumonia and diarrhea, respectively, with wide variation among the provinces.10 In studies in LMIC settings, distance to health services, transportation, treatment cost, caregiver access to household finances, perceived quality of available health providers, availability and comprehension of health information, social and religious norms (including gender-based mobility), and perceived severity of illness are factors that affect health-seeking behavior.9,11,12 However, the determinants of health-seeking and decision-making for under five children with pneumonia and diarrhea in Pakistan are scarcely researched.13
A review of general health-seeking behavior in Pakistan (63% population resides in rural areas) found that generally mothers opt for home remedies when they first identify that their child is sick with pneumonia or diarrhea, and if symptoms persist, they visit a private practitioner, and as a last resort, a hospital.14,15 The studies also found that mothers prefer private practitioners to government facilities and consult multiple family members before seeking treatment for their child. The studies also reported some difficulty among mothers in identifying the symptoms and causes of pneumonia.14–16
The narrative medicine approach is used in patient–practitioner relationships and in research to explore how people view an illness in the context of their lives.17 This study aimed to develop in-depth and comprehensive understanding of the social context and process of care giving for childhood pneumonia and diarrhea in order to highlight the complexities and dynamics of health seeking in rural Sindh, Pakistan. It is an ethnographic approach illustrating caregiver stories of the context in which childcare decisions are made at household level throughout an illness episode. The literature on health seeking behavior for childcare generally rests on the perspectives of mothers13,16. Our study is unique as it intentionally sought perspectives (in the form of narrative stories) from additional caregivers, such as grandmothers/fathers and sister-in-laws, in order to broaden understanding of the family care giving process at the household level.
Methods
Study Setting
This study was conducted in district Badin in southern Pakistan as part of the “Nigraan trial” on community case management of childhood diarrhea and pneumonia.18 The latter trial had children <5 registered for regular surveillance and hence provided a reasonable sampling frame to choose households with children <5 years. Badin has a population of about 1.35 million, of which 84% is rural. Badin’s economy is mainly dependent on agriculture and fishing. The literacy rate of the district is approximately 25%. Male literacy is three times higher than female literacy19. This is a poor rural district with an average monthly household income of less than 50 US $. 62% of the population in Pakistan resides in rural areas as compared to 38% living in urban areas. Urban and rural areas differ depending on population density, services, resources, trade and land, with better opportunities in urban versus rural Pakistan.
Data Collection Tool
In-depth interviews were conducted to gather stories of care giving for children <5 with pneumonia and diarrhea. The interview tool was developed by co-author Maria Giulia Marini (MGM), a narrative medicine expert20. The questions and probes provided by MGM in English were translated to Sindhi. The probes encouraged participants to share stories and experiences of care giving for children <5 with pneumonia and diarrhea. The probes for the narrative stories focused on family, home, and community dynamics, daily routine of participants, perception about healthy and sick child, knowledge about diarrhea and pneumonia in general, decision-making, and health-seeking processes before, during and after an episode of childhood diarrhea and pneumonia and health providers consulted (Refer to Figure 1: Key probes used in Narrative interviews). The tool was pilot tested before the interviews.
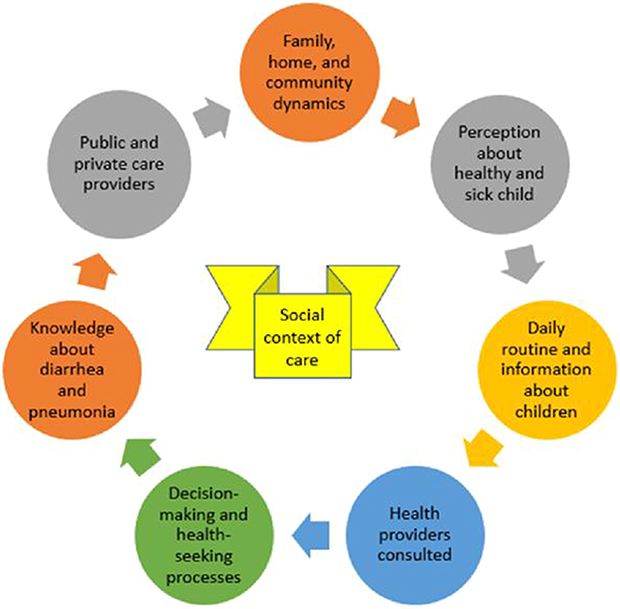 |
Figure 1 Key probes used in narrative interviews. |
Participant Selection
Twenty caregivers from 11 households participated in in-depth interviews. The households were randomly drawn from the sampling frame of Nigraan trial selecting households with children <5. Those households which did not have children <5 years were excluded. Purposive sampling was employed to identify a range of participants from the same households (eg, father, mother, and grandparents, etc.) who were involved in childcare and consented to participate in the study and describe the process of care giving during an illness episode. Thus, multiple caregivers from the same household could be selected for face-to-face narrative interviewing to understand the household dynamics of decision-making during a usual episode of childhood diarrhea or pneumonia irrespective of when the last illness episode had occurred.
Data Collection
All interviews were conducted privately in participants’ homes over a two-week period. The first nine interviews were conducted by three interviewers together, and after discussion, two interviewers were deemed appropriate for the remaining eleven interviews. One interviewer was an intern with a bachelor’s degree and the other two were medical doctors with added qualification of master’s in public health. The latter had prior experience of working in rural settings and conducting narrative interviews. Interviews were conducted in English, Urdu, and Sindhi. To gain the trust of participants, the interviews started with an informal introduction and explanation of study objectives. Participants were informed that the research aimed to better understand caregiver decision-making processes for children <5 years who get sick with diarrhea and pneumonia. The interviews were between 45 and 105 minutes in length and were audiotaped. Field notes were made during the interviews regarding the setting, gestures, and expressions of the participants and how the whole process of interview proceeded.
Data Analysis
A transcriptionist fluent in English, Urdu, and Sindhi was separately hired for transcribing the interviews. Manual content analysis was carried out. During analysis, researchers remained open to exploring the experiences prioritized and told by participants. The first stage of analyzing the interviews with community caregivers involved three researchers independently reading each interview transcript twice to familiarize themselves with the participants’ narratives.
Prior to reading each transcript, researchers reviewed the notes taken during and after the interview by the interview team. After being acquainted with the transcripts, all three researchers met to discuss and compare notes regarding the tone and emerging themes of each interview. The interviews were conducted till the point of saturation. The interviews of participants from the same household were first discussed separately, and then compared among the researchers to identify differences and similarities in the tone, stories told, and emerging themes. The data were read and reread and then broken down into component parts that are codes. Free codes were formulated. These codes were then merged into main themes. The transcripts were not returned to participants, nor their feedback sought; however, a dissemination seminar was held at project conclusion and findings were shared with various stakeholders including community representatives.
Two overarching themes and multiple sub-themes were developed and presented to the larger research team, and through peer debriefing the sub-themes were reshaped and refined (Refer to Figure 2). The two overarching themes reflected the experience of caregiving for children <5 as told by participants: 1 – the context of caregiving, which explores how socioeconomic status, family and household structure, and perceived severity of pneumonia and diarrhea influences health seeking for children <5, and 2 – the process of caregiving, describes how caregivers prevent and identify pneumonia and diarrhea, manage the illnesses at home, make decisions about health seeking, and fulfill the treatment plan for their under five children.
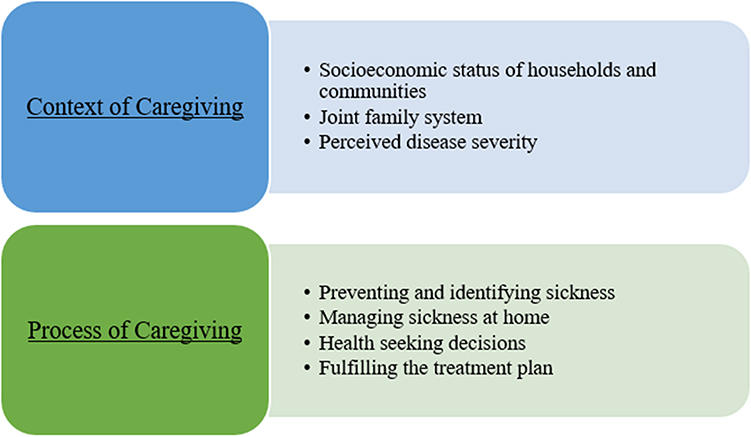 |
Figure 2 Themes and subthemes to reflect the experience of caregiving for under five children. |
Trustworthiness of study findings (credibility, transferability, dependability, and conformability) was attained by researchers having expert knowledge regarding the narrative approach, the use of appropriate methodology in qualitative inquiry, pilot testing data collection tool devised by the narrative medicine expert on the research team and using content analysis to get an insight into the stories of care giving. Moreover, a comprehensive description of the research methodology is a testament to the rigor of the study.
Ethics
This study was part of the NIGRAAN trial which had approval from the Aga Khan University’s Ethics Review Committee. All participants gave written or if illiterate, thumb printed, informed consent after thorough explanation of the study objectives. The participants’ informed consent included publication of anonymized responses. Confidentiality and privacy of the participants was maintained by keeping their identity undisclosed. All verbatim quotes in text are completely anonymized. A very small amount of stipend was given to the participants as compensation for their time off from work.
Results
Table 1 displays the characteristics of the 20 community caregivers that participated in this study. Nobody refused to participate and there was no drop out. Caregivers were primarily (n = 13, 65%) mothers or fathers of children <5, had various levels of education, and diverse occupations. In one of the households, there was a couple with a child under 5 and also had a grandchild <5. Hence, the participants had multiple roles; grandfather/father and grandmother/mother at the same time. The latter thus described their caregiving experience as parents/grandparents for their own child and their grandchild. The children < years residing in households with a joint family system were therefore provided care by multiple caregivers with each caregiver bringing in their unique perspective to childcare.
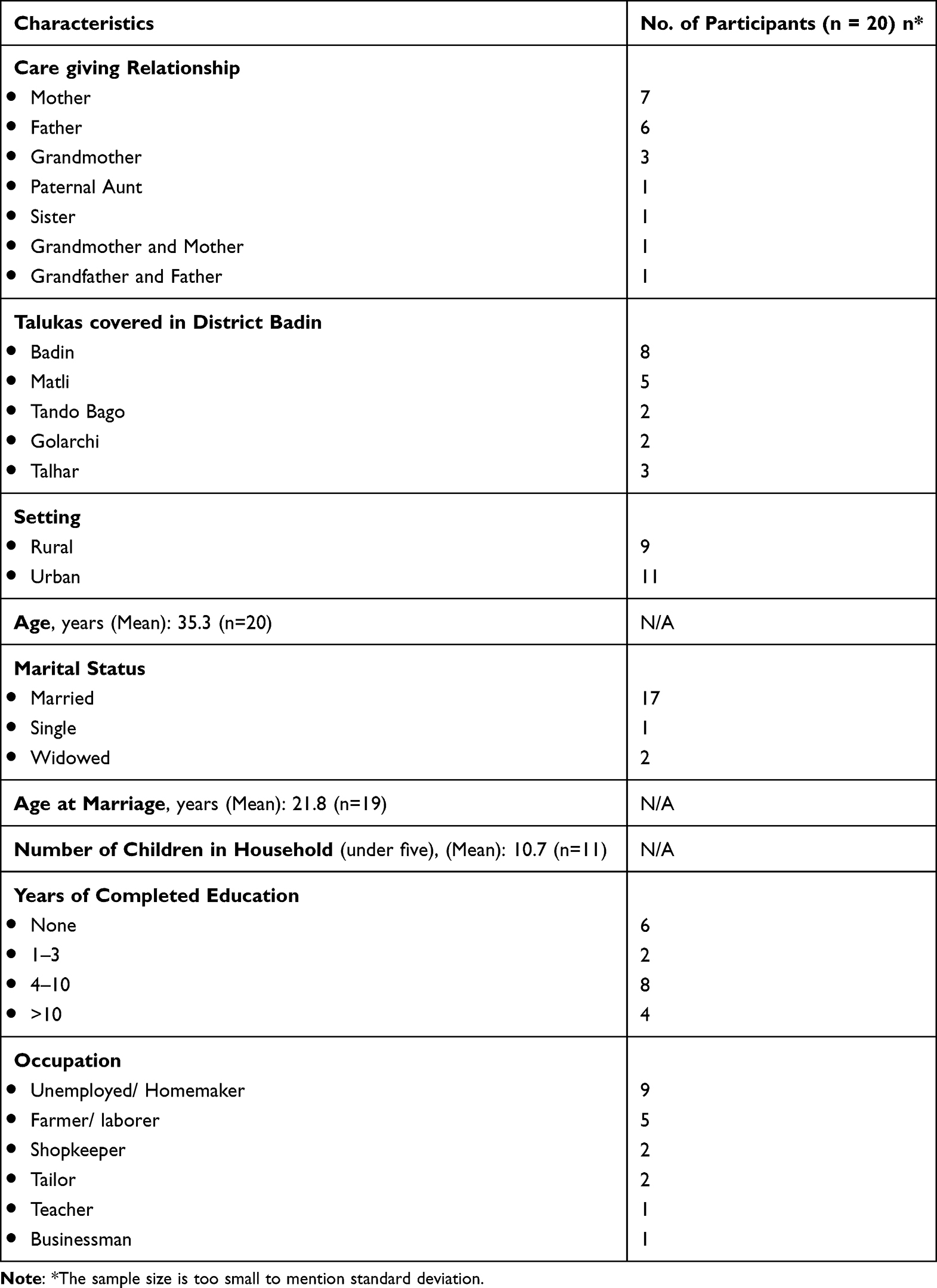 |
Table 1 Sociodemographic Characteristics of Participants |
Context and Process of Caregiving
Context of Caregiving
Socioeconomic Status of Households and Communities
The caregivers interviewed generally were of poor socioeconomic status. Participant narratives illustrated that caregiver education/literacy and financial stability influenced their ability to identify symptoms of pneumonia and diarrhea and their decision to seek care. In two poor rural households, participants shared that gender norms in their community prevent girls from receiving education which contributes to a lack of awareness about signs and symptoms of childhood illnesses. Mrs. S, a mother of two children <5 shares that:
In cities people are literate so they know how to take care of the child. However, in the rural communities the females are illiterate, and they are unaware of how to prevent sickness in their children.
Mrs. N, a mother, on the other hand, affirms why the cycle of poverty impedes appropriate health seeking:
We work [the] whole day but we only get 150 rupees in our hand. See we are two earning members and 8–10 people who are eating, and we also have to feed our cow. When they get sick, first we see whether we have money or not. If we have then we take them for treatment otherwise we have to either wait or we borrow from some neighbors or the community members.
Joint Family System
Nuclear family system is a family unit consisting of parents and their dependent children21 A joint family system is two or more nuclear families that form a corporate economic unit. Most caregivers lived in such a system, meaning in the latter, often the families of a set of brothers, lived in the same compound. In such households shared decision-making occurs with a lot of respect for the elders Mrs. F, grandmother to three children <5, narrates:
I decide or my sons decide because they are the fathers. I also decide because I am the head of the family … and the elder one in the family … whatever I say has to happen.
As grandmothers had authority in the household, their daughters-in-law could be limited in their ability to make decisions for their child’s health. Although Mrs. M, a mother to four children <5 feels limited in her decision-making influence, she also explains how the joint family system can be beneficial:
[It is difficult to seek care without permission] because we have joint family s system. If [children’s] grandmother is at home, then she takes care of them. We live in a combined family so if my child is sick then my sister-in-law will help me in my work. Thanks God, I have support.
Overall, the joint family system provides a strong support system, while also having the potential to reduce the autonomy of parents in decision-making.
Perceived Disease Severity
Caregivers perceived diarrhea to be more common than pneumonia in their communities, and as Mr. J, father to one child under five, explains, they worry that their children will die from the illness:
Diarrhea is most common here. [A] couple of children have lost their lives. We really feel bad about it, that our child could be also one of them.
Other caregivers were overwhelmed and exhausted with the severity and frequency of illness that their children experience.
My children are never healthy they are always sick. They are fine for one month, [but then] and again they become sick. There is sanitation problem you must have seen that; we go complain in the town, but they don’t come. – Mr. I (Urban poor father of two children <5)
I don’t know why [she gets sick]. The doctor says that diarrhea occurs because of poor hygiene, but I always take care of her hygiene [and] her diet, and despite that she gets sick. I am confused and sometimes I get irritated because she gets sick repeatedly. – Mrs. H (Urban mother of two children <5)
Caregivers live in areas without adequate infrastructure and resources to protect their children from pneumonia and diarrhea. The constant threat of children falling ill is an emotional and financial burden to households.
Process of Caregiving
Preventing and Identifying Sickness
Caregivers are more confident in their knowledge of causes, signs, and symptoms of diarrhea than they are for pneumonia. The source of this knowledge is primarily from their own experience, guidance from elders or female relatives living in their household, doctors, and NGOs. For example, Mrs. S who is a young mother of two children under five, shares how her sister-in-law taught her to identify and manage symptoms of pneumonia and diarrhea:
Initially I was unaware [of symptoms], but then my sisters-in-law informed me about these things. After marriage I came to know.
Mrs. S also reflects on how she learned to identify and prevent pneumonia and diarrhea in her children:
My elders told me, but I have learned by my experiences because I am a mother now.
Managing Sickness at Home
All caregivers used home remedies and over-the-counter medicines as a first step in treating their children’s mild sickness affordably and conveniently at home. Caregiver education, finances, and age influence the type of home remedies used. Mr. N, a poor urban father of two children under five opts for home treatment first to save money:
Initially we go for cheap treatment. We go to the medical store, and they give me medicine for fever or syrup for cough. We give that medicine to the child first then take them to the doctor.
Mrs. K describes the home remedies she recommends to her daughters-in-law when their children under five are sick, often these remedies cause more harm than relief and result in delay in seeking formal health care:
We give mixture of egg yolk and some honey. Then we dip the cotton in the egg yolk and tie on the chest of the child and that is how they get relief … We always try these remedies. If the child is not getting better, then we take the child to the doctor.
Often mothers will use home remedies under the recommendation of their mother-in-law and sisters-in-law:
[Doctors] are not in the favor of these home remedies and they don’t encourage us to use them… [I continue using them] because my mother in law and sister- in-law tell me, maybe my child will get some benefit – Mrs. U (Urban poor, mother of two children under five)
Based on these narratives, managing children’s sickness at home seems to be influenced by availability of money for treatment, education and perception of home remedies, household dynamic and elder authority, and frequency of sickness.
Health Seeking Decisions
Numerous family members are involved in deciding when and from whom the child will receive additional care. For example, although Mrs. S prefers taking her child to a doctor when the sickness persists, she abides by mother-in-law’s preference for traditional healers:
Both me and my husband decide. We always prefer doctors but my mother-in- law prefers traditional healers first. She is elderly in our house so I can’t say anything to her directly. We let her try whatever she wants to do. Family values are very important to us.
Below is a narrative reflecting the views of four grandmothers interviewed about their role in decision-making:
I decide because I am the elder one in the family… they ask me, and I take the final decision … I suggest taking the child to the doctor.
This practical social support, most often provided by family members in joint households, is imperative to seeking care for sick children and also assuring financial provision to bear the cost of treatment. For caregivers who do not have or are denied strong family support, friends or bosses are the only other option, as is Mr. N’s situation:
For money I just contact my friends. [I don’t go to my brothers] because I know their situation, and if they have money, they will not give it to me. I know that that’s why I don’t ask from them.
Practical support from household is very important, especially when mothers need to be accompanied to the doctor with a male relative. Mr. A, father to three children under five, shares his brother’s supportive role:
If I am not present in the home and [my wife] needs to visit the doctor then my elder brother accompanies her. This is the benefit of living together. When I am not at home, my elder brother is here and when he is not at home, I am responsible for all work.
Caregivers also receive support from their sisters-in-law or other children. For example, Mrs. R shared that her sister-in-law “takes care of my [household] work when child is sick”. Mrs. N, who must work as a laborer during the day, has to leave her children under five with their elder siblings for childcare:
[Elder children] care for sick child, but sometimes they go to play. Child cries [and] cries, and a time comes when they stop crying because they don’t have anyone to take care of them.
Physically accessing healthcare is very difficult for many caregivers, especially those who do not own any form of transportation. Mr. J, father to one child under five, and who lives in a poor rural household, explains how they reach a doctor when their child is sick:
Here in village, we face transportation problem, if we get the vehicle then we reach early otherwise we go by walk.
Mrs. Z, a mother and grandmother to children <5 living in a rural poor household, describes her frustration with a doctor’s comments regarding the time taken to reach the hospital:
One doctor scolded me once that why I use home remedies. He said, ‘you should come to the hospital. I said, it was midnight [and] we don‘t have any vehicle, how should I take the child to the doctor?
When the caregivers do decide to take their sick child to a doctor, they tend to prefer private doctors rather than government doctors. Although government doctors and medicines are free, so many caregivers do resort to their care, they still associate private doctors with better care because they have shorter wait times and doctors give them more attention. Mr. I shares his frustration with government doctors:
Government doctors don’t even listen to us. They are just eating food all the time, and despite that they are getting salaries. Why do they come to the hospital?
However, other caregivers perceive private doctors less favorably:
Private doctors are greedy that’s why they give proper attention because we give them money. – Mr. J (Poor rural father of one child under five)
Overall, caregivers expect higher standards of care from private doctors because they are paying for their services. But because many caregivers are financially insecure, they bring their children to government doctors first, and if they do not cure their child, they move on to private doctors.
Fulfilling the Treatment Plan
After visiting the doctor, mothers are expected to implement the treatment plan. However, the treatment plan may not be fulfilled if the mother does not properly comprehend and adhere to the instructions, and if they cannot afford medicines. Mrs. A and Mrs. U explain their difficulties managing the treatment plan:
If the doctor says give medicines for 10 days and child gets better in few days then we stop giving medicines. – Mrs. A (Sister of two children <5 living in urban middle-class household)
When [the] doctor gives a lot of medicines then sometimes I get confused about timings when medicine should be given. – Mrs. U (Urban poor mother of two children <5)
Mrs. H and Mr. N describe how their financial situation prevents them from providing their children the treatment plan:
If we cannot afford those expensive medicines then we keep that prescription aside. If we can afford, then we buy. – Mrs. H (Middle class urban mother of two children <5)
If we don’t have that much money then we take half the medicines. If we have less money, I buy medicine for 1 day. – Mr. N (Poor urban father of two children <5)
Discussion
It is ironic that the pattern of decision-making for child healthcare has remained unchanged in Pakistan over the past three decades. The uniqueness of this study is the exploration of care seeking at household level comprehensively taking into account all actors and power dynamics within the household and not just the perception of mothers. Managing children’s sickness at home seems to be influenced by availability of money for treatment, use of home remedies, household dynamics, and elder authority. Moreover, the caregivers expect higher standards of care from private doctors as compared to the public health care system.
The results from the in-depth narrative interviews indicated that the joint family system provides a strong support system, while also having the potential to reduce the autonomy of parents in decision-making. Joint family households increase the support available to address the financial and practical considerations of health seeking and implementing treatment plans for pneumonia and diarrhea. Unlike nuclear households, caregivers of children <5 in joint family households have numerous family members to rely on for support. A study from India revealed how joint families can be a source of economic help and social support in times of trouble.22 Evidence from Kenya shows how households with three generations help share various duties including childrearing and household chores.23
However, in households where family relationships are not positive, caregivers have to seek financial support from their friends or employers. Furthermore, these caregivers have less practical support from family members, so if their children are sick, fathers have to take time off from work to accompany them to the hospital. Nevertheless, joint family system also decreases parental autonomy in seeking childcare services. A study from Abbottabad shows that daughters-in-law have limited say and less involvement in decision-making in joint family systems.24
Elders and female relatives, especially the child’s paternal grandmother, are an important and trusted source of knowledge regarding child sickness in the household. Inexperienced mothers rely on elders and female relative’s knowledge to learn the signs and symptoms of pneumonia and diarrhea. Overall, paternal grandmothers hold the most influential voice in the household in deciding when and from whom to seek treatment for a sick child. Mothers and fathers are the second line of decision-making in such cases. This includes decisions about whether to seek care from government or private doctors. Study from rural Ghana has shown that grandmothers serve as gatekeepers for health-seeking behavior, especially with regard to their daughters and daughters-in-law.25 Our findings on decision-making also align with a review of general health seeking behavior (not specific to child illness) in Pakistan and a qualitative study that interviewed mothers on health seeking for children <5 in rural Rajasthan, India.26,27 Both studies found that the authority of fathers or male relatives, mother-in-law/grandmothers, and other elders in the household prolonged the decision-making process and reduced the mother’s autonomy in accessing care for her child. In the Pakistan study, however, a greater variety of public and private sector outlets was shown to be available in urban areas, thus expanding the choices of seeking healthcare when compared to rural settings. Another study from India also mentioned that those women who lived with mothers-in-law had less decision-making power28. In addition to these findings, our interviews illustrate that mother’s decision-making authority for her child’s illness is limited and yielded to her husband, male relatives, or elders. The study in Pakistan recommends that policy makers must understand health behaviors and health care use at the district level. However, there is not enough evidence to highlight that action plans incorporate enhancing maternal autonomy in healthcare decision-making.
Furthermore, the practice of home remedies is inherited from their mother-in-law and older sisters-in-law in the household. Home remedies can be useful for affordably treating mild symptoms of pneumonia and diarrhea, but the household hierarchy can be problematic if home remedies are harmful. A study from Nepal mentions that healthcare is sought only after the home remedies fail.29
In our study, caregivers were generally dissatisfied with all doctors, but associated private doctors with higher quality care because they paid for their services and had shorter wait times. A study from rural Pakistani community uncovered that seventy-five percent caregivers sought care from private providers for diarrhea and pneumonia13,16. However, in practice, caregivers tended to take their children to government doctors, and to private doctors only when their child’s illness worsened. This process of pursuing less expensive treatment and services first (ie, home remedies, self-prescribed medicines, and government doctors) before opting for expensive private doctors and medicines is a practice described in other studies of health seeking in LMICs like sub-Saharan Africa and Bangladesh, etc.30–32 Another evidence from South Africa also shows use of traditional medicines for treatment of diarrhea in children33.
Our findings compare with those of a systematic review of health seeking for child illnesses in sub-Saharan Africa, which found household perceptions of illness prevention and treatment to have important influence on the decision-making process.30
Limitations
The most important limitation to consider in this study was the influence of interviewers on the participants’ answers. The interview team consisted of one of two Pakistani doctors (one man, one woman) and a white Canadian woman researcher. The interview team also represented a highly reputable university in Pakistan. The presence of these interviewers likely influenced the answers and experiences that participants felt comfortable or wanted to share, potentially depending on their socioeconomic status and gender. Moreover, there could be a reporting bias present where participants were interviewed together especially in the presence of mothers-in-law. However, as per guidance by MGM, the researchers approached each household and interviewed each participant in a way that minimized discomfort and misunderstandings. Our team spoke at length with household members to clarify the purpose and use of our research, took time to answer specific participant questions, paused the interviews when requested, and respected cultural norms and attire.
Overall, the narrative inquiry served to be a useful tool to illicit caregivers’ contextual experiences of health seeking for managing children with diarrhea and pneumonia.
Conclusions
It is ironic that the pattern of decision-making for child healthcare has remained unchanged in Badin district, southern Pakistan over the past three decades. Elderly females play a major role in the type of health care to be provided to the child. Illiteracy and finance are the major players in health-sick behavior. A joint family has an important role in resource-limited settings. The determinants of childcare still include lack of maternal autonomy, overuse of home remedies and preference for care seeking in the private sector. All of these factors contribute to the stagnant rate of under 5 mortalities attributable to diarrhea and pneumonia.
The usual pattern of childcare emerging at the household level includes initial identification and interpretation of illness by all the actors in the joint family system, and overemphasis on use of home remedies prior to seeking care in the formal healthcare sector.
Broader health promotion programs should therefore address the significant others (elders, mothers-in-law and fathers) in their policies.
Data Sharing Statement
Data and materials are in the custody of the University and could be made available on request, keeping the individual identity of the participants confidential.
Ethics Approval and Consent to Participate
Ethical approval was sought from the Ethical Review Committee of the Aga Khan University and informed consent was taken from the participants before the interviews.
Acknowledgments
The authors would like to extend their special gratitude to Dr. Sajid Bashir Soofi, Department of Pediatrics & Child Health, Associate Director, Center of Excellence in Women & Child Health, Aga Khan University for supporting the NIGRAAN trial.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was funded by the Alliance for Health Policy and Systems Research, WHO, Geneva with support from the Norwegian Government Agency for Development Cooperation (NORAD), the Swedish International Development Cooperation Agency (SIDA) and the UK Department for International Development (DFID). The technical coordination and support were provided by the Department of Maternal Newborn Child and Adolescent Health, WHO Geneva.
Disclosure
The authors report no competing interests in this work.
References
1. Walker CLF, Rudan I, Liu L, et al. Global burden of childhood pneumonia and diarrhoea. Lancet. 2013;381(9875):1405–1416. doi:10.1016/S0140-6736(13)60222-6
2. Bhutta ZA, Das JK. Global burden of childhood diarrhea and pneumonia: what can and should be done? Pediatrics. 2013;131(4):634–636. doi:10.1542/peds.2012-3737
3. Leung DT, Chisti MJ, Pavia AT. Prevention and control of childhood pneumonia and diarrhea. Pediatric Clin. 2016;63(1):67–79. doi:10.1016/j.pcl.2015.08.003
4. Gill CJ, Young M, Schroder K, et al. Bottlenecks, barriers, and solutions: results from multicountry consultations focused on reduction of childhood pneumonia and diarrhoea deaths. Lancet. 2013;381(9876):1487–1498. doi:10.1016/S0140-6736(13)60314-1
5. Ghimire M, Bhattacharya S, Narain J. Pneumonia in South-East Asia region: public health perspective. Indian J Med Res. 2012;135(4):459.
6. Chang AY, Riumallo-Herl C, Salomon JA, Resch SC, Brenzel L, Verguet S. Estimating the distribution of morbidity and mortality of childhood diarrhea, measles, and pneumonia by wealth group in low-and middle-income countries. BMC Med. 2018;16:1–13. doi:10.1186/s12916-018-1074-y
7. Sudrajat T, Hakim W, Rahman T, Shah R. ‘STOP Pneumonia’–a successful advocacy campaign for preventing and protecting Indonesia’s children from pneumonia. Public Health Indon. 2021;7(1):1–4. doi:10.36685/phi.v7i1.400
8. World Health Organization. Ending Preventable Child Deaths from Pneumonia and Diarrhoea by 2025: The Integrated Global Action Plan for Pneumonia and Diarrhoea (GAPPD). World Health Organization; 2013.
9. World Health Organization. World Health Statistics 2016 [OP]: Monitoring Health for the Sustainable Development Goals (Sdgs). World Health Organization; 2016.
10. National Institute of Population Studies (NIPS) [Pakistan] and ICF. Islamabad. Pakistan Demographic and Health Survey 2017–18. Pakistan, and Rockville, Maryland, USA: NIPS and ICF; 2019. Available from: https://www.nips.org.pk/study_list.php.
11. Wardlaw T, You D, Hug L, Amouzou A, Newby H. UNICEF Report: enormous progress in child survival but greater focus on newborns urgently needed. Reprod Health. 2014;11(1):1–4. doi:10.1186/1742-4755-11-82
12. Pillai RK, Williams SV, Glick HA, Polsky D, Berlin JA, Lowe RA. Factors affecting decisions to seek treatment for sick children in Kerala, India. Soc Sci Med. 2003;57(5):783–790. doi:10.1016/S0277-9536(02)00448-3
13. Aftab W, Shipton L, Rabbani F, et al. Exploring health care seeking knowledge, perceptions and practices for childhood diarrhea and pneumonia and their context in a rural Pakistani community. BMC Health Serv Res. 2018;18(1):1–10. doi:10.1186/s12913-018-2845-z
14. Kundi MM, Anjum M, Mull DS, Mull JD. Maternal perceptions of pneumonia and pneumonia signs in Pakistani children. Soc Sci Med. 1993;37(5):649–660. doi:10.1016/0277-9536(93)90104-C
15. Mull DS, Mull JD. Insights from community‐based research on child pneumonia in Pakistan. Med Anthropol. 1993;15(4):335–352. doi:10.1080/01459740.1994.9966098
16. D’souza RM. Role of health-seeking behaviour in child mortality in the slums of Karachi, Pakistan. J Biosoc Sci. 2003;35(1):131–144. doi:10.1017/S0021932003001317
17. Kalitzkus V, Matthiessen PF. Narrative-based medicine: potential, pitfalls, and practice. Perm J. 2009;13(1):80. doi:10.7812/TPP/09.996
18. Rabbani F, Mukhi AAA, Perveen S, et al. Improving community case management of diarrhoea and pneumonia in district Badin, Pakistan through a cluster randomised study—the NIGRAAN trial protocol. Implem Sci. 2014;9(1):1–10. doi:10.1186/s13012-014-0186-9
19. Rabbani F, Shipton L, Aftab W, Sangrasi K, Perveen S, Zahidie A. Inspiring health worker motivation with supportive supervision: a survey of lady health supervisor motivating factors in rural Pakistan. BMC Health Serv Res. 2016;16:1–8. doi:10.1186/s12913-016-1641-x
20. Marini MG. Narrative Medicine: Bridging the Gap Between Evidence-Based Care and Medical Humanities. Springer; 2015.
21. Itrat A, Taqui AM, Qazi F, Qidwai W. Family systems: perceptions of elderly patients and their attendents presenting at a university hospital in Karachi, Pakistan. J Pakist Med Assoc. 2007;57(2):106.
22. Chadda RK, Deb KS. Indian family systems, collectivistic society and psychotherapy. Indian J Psychiatry. 2013;55(Suppl 2):299. doi:10.4103/0019-5545.105555
23. Abubakar A, Van Baar A, Fischer R, Bomu G, Gona JK, Newton CR. Socio-cultural determinants of health-seeking behaviour on the Kenyan coast: a qualitative study. PLoS One. 2013;8(11):e71998. doi:10.1371/journal.pone.0071998
24. Lodhi FS, Khan AA, Raza O, Zaman TU, Farooq U, Holakouie-Naieni K. Level of satisfaction and its predictors among joint and nuclear family systems in District Abbottabad, Pakistan. Med J Islam Repub Iran. 2019;33:59. doi:10.34171/mjiri.33.59
25. Gupta ML, Aborigo RA, Adongo PB, et al. Grandmothers as gatekeepers? The role of grandmothers in influencing health-seeking for mothers and newborns in rural northern Ghana. Glob Public Health. 2015;10(9):1078–1091. doi:10.1080/17441692.2014.1002413
26. Shaikh BT, Hatcher J. Health seeking behaviour and health service utilization in Pakistan: challenging the policy makers. J Public Health. 2005;27(1):49–54. doi:10.1093/pubmed/fdh207
27. Mohan P, Iyengar S, Agarwal K, Martines J, Sen K. Care-seeking practices in rural Rajasthan: barriers and facilitating factors. J Perinatol. 2008;28(2):S31–S37. doi:10.1038/jp.2008.167
28. Singh-Manoux A, Clarke P, Marmot M. Multiple measures of socio-economic position and psychosocial health: proximal and distal measures. Int J Epidemiol. 2002;31(6):1192–1199. doi:10.1093/ije/31.6.1192
29. Pokhrel S, Sauerborn R. Household decision-making on child health care in developing countries: the case of Nepal. Health Policy Plan. 2004;19(4):218–233. doi:10.1093/heapol/czh027
30. Colvin CJ, Smith HJ, Swartz A, et al. Understanding careseeking for child illness in sub-Saharan Africa: a systematic review and conceptual framework based on qualitative research of household recognition and response to child diarrhoea, pneumonia and malaria. Soc Sci Med. 2013;86:66–78. doi:10.1016/j.socscimed.2013.02.031
31. Geldsetzer P, Williams TC, Kirolos A, et al. The recognition of and care seeking behaviour for childhood illness in developing countries: a systematic review. PLoS One. 2014;9(4). doi:10.1371/journal.pone.0093427
32. Najnin N, Bennett CM, Luby SP. Inequalities in care-seeking for febrile illness of under-five children in urban Dhaka, Bangladesh. J Health Popul Nutr. 2011;29(5):523. doi:10.3329/jhpn.v29i5.8907
33. Cunnama L, Honda A. A mother’s choice: a qualitative study of mothers’ health seeking behaviour for their children with acute diarrhoea. BMC Health Serv Res. 2016;16(1):1–11. doi:10.1186/s12913-016-1911-7
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.