")
Back to Journals » Clinical Epidemiology » Volume 14
Lifestyle in Pregnancy and Hypospadias in Sons: A Study of 85,923 Mother-Son Pairs from Two Danish Pregnancy Cohorts
Authors Kjersgaard CL , Arendt LH, Ernst A, Lindhard MS, Olsen J, Henriksen TB , Strandberg-Larsen K , Ramlau-Hansen CH
Received 20 September 2021
Accepted for publication 16 December 2021
Published 9 February 2022 Volume 2022:14 Pages 149—157
DOI https://doi.org/10.2147/CLEP.S335877
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Lars Pedersen
Camilla Lomholt Kjersgaard,1 Linn Håkonsen Arendt,1,2 Andreas Ernst,1,3 Morten Søndergaard Lindhard,4,5 Jørn Olsen,1,6 Tine Brink Henriksen,5 Katrine Strandberg-Larsen,7 Cecilia Høst Ramlau-Hansen1
1Department of Public Health, Research Unit for Epidemiology, Aarhus University, Aarhus, Denmark; 2Department of Obstetrics and Gynecology, Horsens Regional Hospital, Horsens, Denmark; 3Department of Urology, Aarhus University Hospital, Aarhus, Denmark; 4Department of Pediatrics, Randers Regional Hospital, Randers, Denmark; 5Perinatal Epidemiology Research Unit, Department of Pediatrics, Aarhus University Hospital, Aarhus, Denmark; 6Department of Clinical Epidemiology, Aarhus University Hospital, Aarhus, Denmark; 7Department of Public Health, Section of Epidemiology, Copenhagen University, Copenhagen, Denmark
Correspondence: Camilla Lomholt Kjersgaard
Department of Public Health, Research Unit for Epidemiology, Aarhus University, Bartholins Allé 2, Aarhus, 8000, Denmark
Tel +45 40 19 44 38
Email [email protected]
Purpose: Hypospadias is one of the most frequent male congenital malformations. It remains controversial whether maternal lifestyle during pregnancy may affects the risk of having a son with hypospadias, especially for smoking with many suggesting lower risk. We assessed the individual and joint associations between maternal cigarette smoking, pre-pregnancy body mass index (BMI), alcohol consumption, binge drinking, and caffeine consumption and occurrence of hypospadias in sons.
Patients and Methods: This cohort study utilized the Danish National Birth Cohort and the Aarhus Birth Cohort, holding detailed information on lifestyle factors in early pregnancy between 1989 and 2012. The Danish health registers were used to identify boys with hypospadias, according to International Classification of Diseases. Potential confounders and covariates were identified by literature search and use of directed acyclic graphs. Missing data were handled by multiple imputation and Cox proportional hazards models were applied to analyse data.
Results: In total, 85,923 live-born singleton boys were included in the study of whom 502 (0.6%) were diagnosed with hypospadias. Maternal smoking in early pregnancy was associated with lower occurrence of hypospadias. An increase of one cigarette smoked per day was associated with lower risk of having a son with hypospadias (adjusted hazard ratio (HR) 0.97 (95% confidence interval (CI) 0.94, 1.00)). However, sub-analyses suggested that the results may be prone to unadjusted confounding. We found no association between pre-pregnancy BMI, alcohol consumption, binge drinking, or caffeine consumption and hypospadias.
Conclusion: Maternal smoking during pregnancy was associated with lower occurrence of hypospadias but we cannot exclude uncontrolled confounding. The other investigated maternal lifestyle factors were not associated with hypospadias in sons.
Keywords: smoking, prenatal exposures, alcohol, caffeine, BMI, birth defects
Introduction
Hypospadias is a male congenital malformation, characterized by an abnormal urethral fusion during gestational weeks 8–14, locating the urethral meatus on the ventral side of the penis, scrotum or perineum.1 Hypospadias require early surgical repair and affected boys may suffer from complications due to surgery, cosmetic unsatisfying results or post-repair physiological problems like voiding dysfunction.2
The estimated prevalence is 0.5%.3 Being born preterm or small for gestational age have consistently been associated with hypospadias,4 and researchers have questioned whether lifestyle and environmental factors might also be part of the etiology.3 In particular, findings from studies on maternal smoking have puzzled researchers and raised queries since some studies have found that maternal smoking is associated with lower risk of hypospadias.5,6
This study aimed to investigate whether maternal cigarette smoking, pre-pregnancy body mass index (BMI), maternal average alcohol consumption, binge drinking, and caffeine consumption, were associated with hypospadias, using two large birth cohorts with detailed information on maternal lifestyle collected early in pregnancy and thereby facilitating adjustment for important confounders. In addition, we also investigated the potential combined effect of the different lifestyle factors in two different sub-analyses.
Materials and Methods
This study uses data from two large Danish birth cohorts; The Danish National Birth Cohort (DNBC)7 and the Aarhus Birth Cohort (ABC).8 The DNBC (1996–2002) is nationwide and includes approximately 92,000 pregnant women and their 96,000 children. The women participated in computer-assisted telephone interviews scheduled around gestational weeks 12 and 30, providing detailed information on health and lifestyle factors (participation rate 60%).7 The ABC was established in 1989, and is still ongoing, currently with approximately 100,000 pregnant women enrolled (participation rate: 80%).8 Around gestational week 12, the women completed a self-administered questionnaire concerning health and lifestyle factors. From 1989 to 1999, the ABC also included a second questionnaire filled out in early third trimester. The questions used to collect information on lifestyle factors in the two cohorts were almost identical, and when not, the least detailed information was used enabling us to combine data and compare results between cohorts.
We included women, who gave birth to a live-born singleton son from 1989 to 2012, who had completed the first interview (DNBC) or the first questionnaire (ABC).
Exposure
The telephone interviews and questionnaires provided early pregnancy information on lifestyle. For women participating in both the DNBC and the ABC (n= 3479), the DNBC served as the main source of information. We primarily used information from the first interview/questionnaire; if some information was missing, we added information from the second interview or questionnaire. Finally, the Danish Medical Birth Register (DMBR) supplemented data on maternal cigarette smoking (n=230), height (n=106) and weight (n=58), when cohort data remained missing.
Cigarette smoking during pregnancy was categorized as: non-smoking (reference), stopped smoking, 1–9 and ≥10 cigarettes/day. We also included a continuous smoking variable since all women who reported smoking in pregnancy, also reported the specific number of cigarettes smoked per day: “Each increase in number of cigarettes smoked per day.” Women who reported to have stopped smoking at the time of the first interview or questionnaire scheduled around gestational week 12, were excluded from the analysis since we do not know, whether they smoked during gestational week 8–14 which is considered the critical period for the development of hypospadias.9 However, in a sub-analysis, we included the “stopped smokers” in the continuous variable according to the number of cigarettes, they reported to have smoked before quitting.
Weekly alcohol intake during pregnancy was the combined average weekly intake of alcoholic beverages. One alcoholic drink was defined as one bottle of beer (0.33 L), one glass of wine, or one glass of liqueur (12.5 g alcohol per unit). The total weekly intake was categorized into 0-<1 (reference), 1–2, and ≥3 drinks/week.
Binge drinking was defined as the number of times drinking ≥5 units of alcohol at one occasion during pregnancy, categorized as 0 (reference) and ≥1 time.10 In ABC, this information was only available from 1998 onwards.
Maternal pre-pregnancy BMI (kg/m2) was calculated from the self-reported height and weight. Biologically implausible values (height <100 cm) were recoded to missing and imputed as described below. We categorized the women according to WHO definition11 as: underweight: <18.5 kg/m2, normal weight: 18.5–24.9 kg/m2 (reference), overweight: 25.0–29.9 kg/m2 and obese: ≥30.0 kg/m2.
Caffeine intake during pregnancy included caffeine from coffee, tea and cola and was categorized into 0, 1–300 (reference), and >300 mg caffeine per day. One cup of coffee was estimated to include 100 mg of caffeine, one cup of tea as 50 mg and ½ L of cola as 50 mg.12,13
Outcome
The unique civil registration number14 allowed unambiguous linkage to the Danish health registries. The Danish National Patient Register (DNPR),15 provided information on outcome with data on all hospital visits, including discharge diagnoses- and surgical codes. All degrees of hypospadias were included and were defined using International Classification of Diseases (ICD)-8 (1977–1993): 75220, 75221, 75222, 75228, 75229, ICD-10 (1994–2012): DQ54 and Nordic classification of surgical procedures codes: KKGH60.
Covariates
We had information on covariates from the two cohorts, and the DMBR provided information on factors related to pregnancy and birth.16 The Danish Integrated Database for Labour Market Research with information on educational level.17 Covariates were identified a priori from the existing literature and by use of directed acyclic graphs (DAGs) (Supplementary Material 1). All models were adjusted for birth cohort, maternal age at delivery, years of education and parity. All five exposures were mutually adjusted. To account for difference in follow-up time, the change in prevalence of diagnosed genital anomalies over time, as well as the change from ICD-8 to ICD-10, we adjusted for calendar year at birth. The analyses of cigarette smoking, weekly alcohol intake, binge drinking episodes and caffeine intake were further adjusted for self-reported time to pregnancy.
Missing Information
Missing values ranged from 0% for maternal age, calendar year of birth and birth cohort to 11.6% for maternal binge drinking. When missing information on maternal binge drinking was ignored, 84% of the study population had complete information on all variables included in the statistical analysis (Table 1).
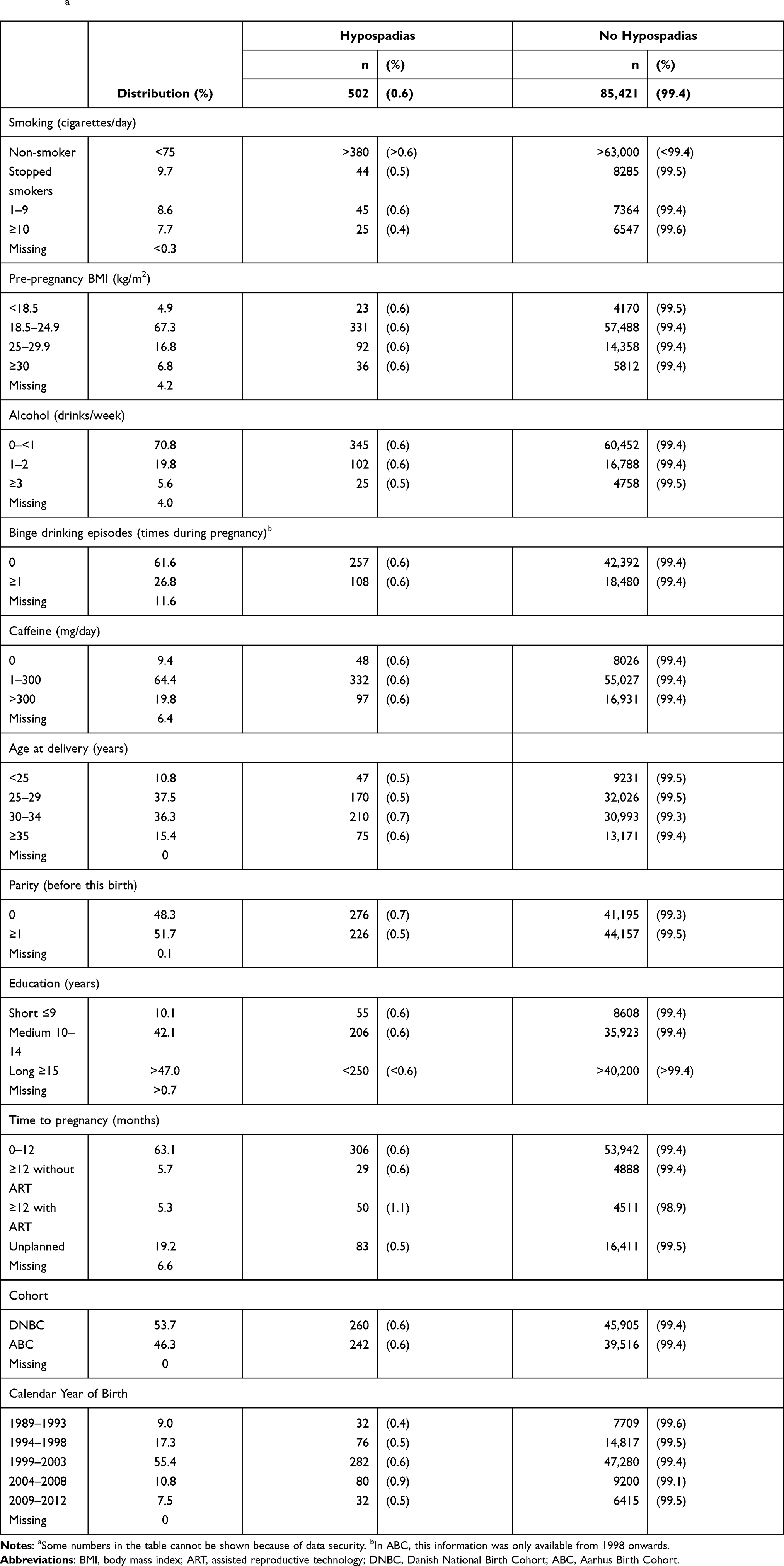 |
Table 1 Distribution of Maternal Characteristics According to Hypospadias Among 85,923 Singleton Live-Born Boys, Denmark, 1989–2012a |
As results from complete-cases analysis may be prone to bias, we handled missing data using multiple imputation,18 under the assumption that data were missing at random (Supplementary Material 2 for detailed description of the multiple imputation).
Statistical Analyses
Follow-up of the children started at birth and ended at time of diagnosis, emigration, death or December 31st 2012, whichever came first. Not all boys had the same age at the time of diagnosis, and some may not have reached the age where the majority of hypospadias were diagnosed. We accounted for this by using a Cox proportional hazards model, with the boys’ age as the underlying time axis. Crude and adjusted hazard ratios (HRs) with 95% confidence intervals (CIs) for hypospadias according to maternal lifestyle factors were estimated, using robust standard errors to account for clustering of siblings (n=19,634). The assumption of proportional hazards was visually evaluated with log-minus-log plots. A test for trend was conducted treating the categorized exposure variables as continuous variables.
In sensitivity analyses, the main results were compared with complete case analyses, and with the results from the two cohorts separately. We further explored the combined effect of up to three maternal lifestyle factors, and subsequently this was analysed in more detail with different combinations. Data were analysed in STATA version 11.2 at Statistics Denmark.
Ethics Approval and Informed Consent
The Declaration of Helsinki were followed, and the Danish Data Protection Agency approved the study (No.2013-41-1964). The DNBC is further approved by the Danish Data Protection Agency (No. 2008-54-0431 and No. 2012-41-0379) and the Committee for Health Research Ethics Approval (VEK) in Denmark (KF 01-471/94). Statens Serum Institut (SSI) has approved the data handling in the DNBC (No. 18/04608) and it is covered by the SSI’s general approval. When enrolled in the DNBC and the ABC, all the mothers provided a written informed consent including both the mother’s and the son’s participation. According to Danish legislation, Institutional Review Board approval is not required for register-based research.
Results
Of the 85,923 live-born singleton boys included, 502 (0.6%) were diagnosed with hypospadias (mean follow-up time (range): 12 (0–25) years and mean time to diagnosis: 1.9 (95% CI 1.7–2.1) years). The distribution of maternal lifestyle factors and baseline characteristics are shown in Table 1.
The hazard for hypospadias in sons of mothers smoking ≥10 cigarettes/day (highest exposure group) was 0.66 (95% CI 0.43, 1.02) times that of sons of non-smoking mothers. Each increase in number of cigarettes smoked per day was associated with lower risk of hypospadias (HR 0.97 (95% CI 0.94, 1.00)). The results were essentially the same (0.98 (95% CI 0.96, 1.01)) when including the women, who reported to have stopped smoking in early pregnancy in the sub-analysis.
We found no association between BMI, weekly alcohol consumption, binge drinking, or caffeine consumption and hypospadias (Table 2). The complete case analysis (Supplementary Table 1) and the analyses of the two cohorts separately showed results quite similar to those obtained in the main analysis (data not shown). Still, the association between smoking ≥10 cigarettes/day and hypospadias were more pronounced in the main analysis (0.66 (95% CI 0.43, 1.02)) compared to the results from the complete case analysis (0.80 (95% CI 0.51, 1.26)). We observed no association between hypospadias and the combined hazardous lifestyle factors (Supplementary Table 2a, 2b, 3a and 3b). When evaluating combined parental smoking, we found associations in similar direction as for maternal smoking, but the point-estimate remained strongest for maternal cigarette smoking alone (HR 0.63 (95% CI 0.39, 1.02) (Table 3)).
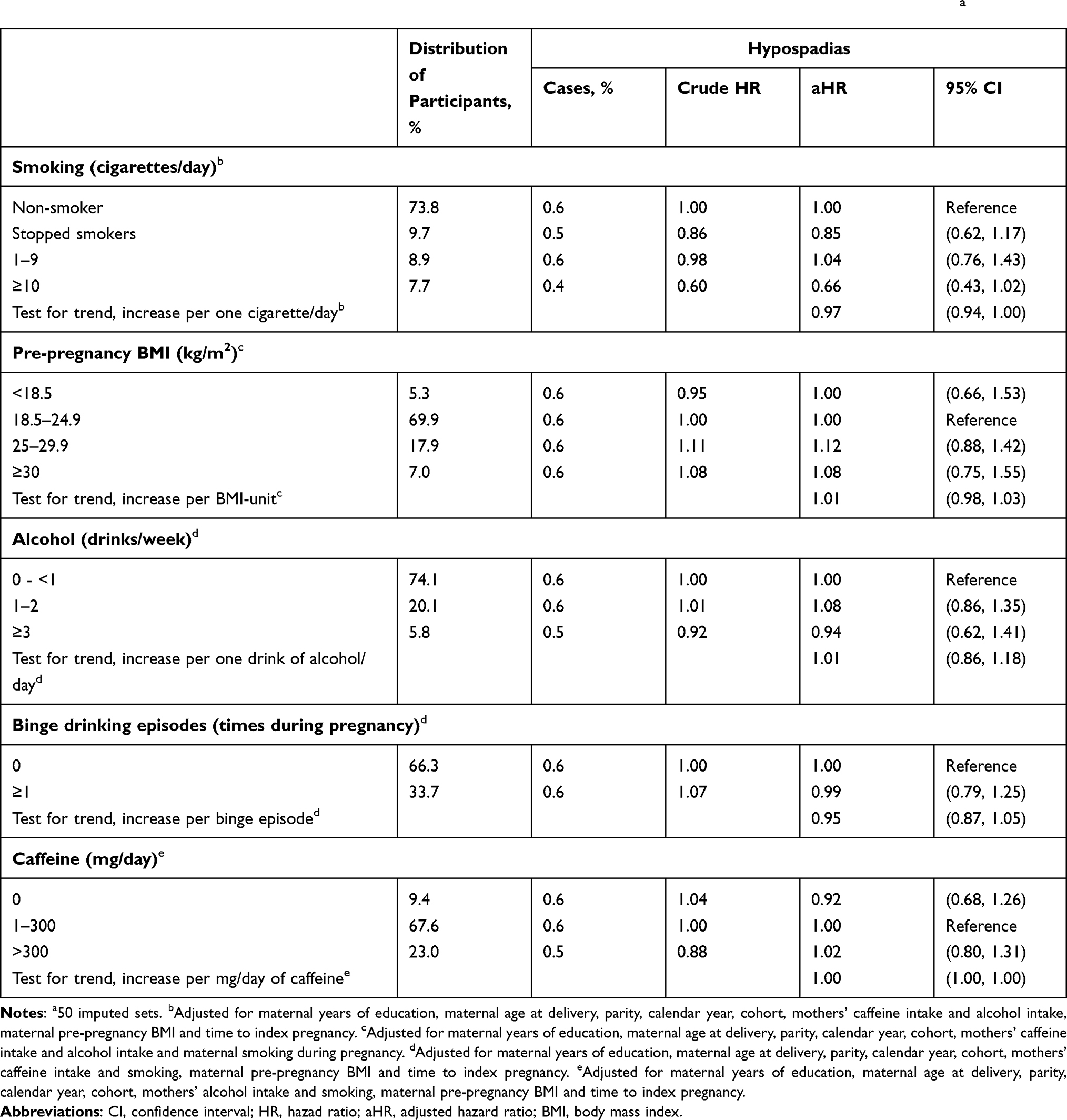 |
Table 2 Hazard Ratios (HR) for Hypospadias According to Maternal Smoking, Weekly Alcohol Intake, Binge Drinking, Pre-Pregnancy Body Mass Index and Caffeine Intake During Pregnancy Among 85,923 Singleton Live-Born Boys, Denmark 1989–2012a |
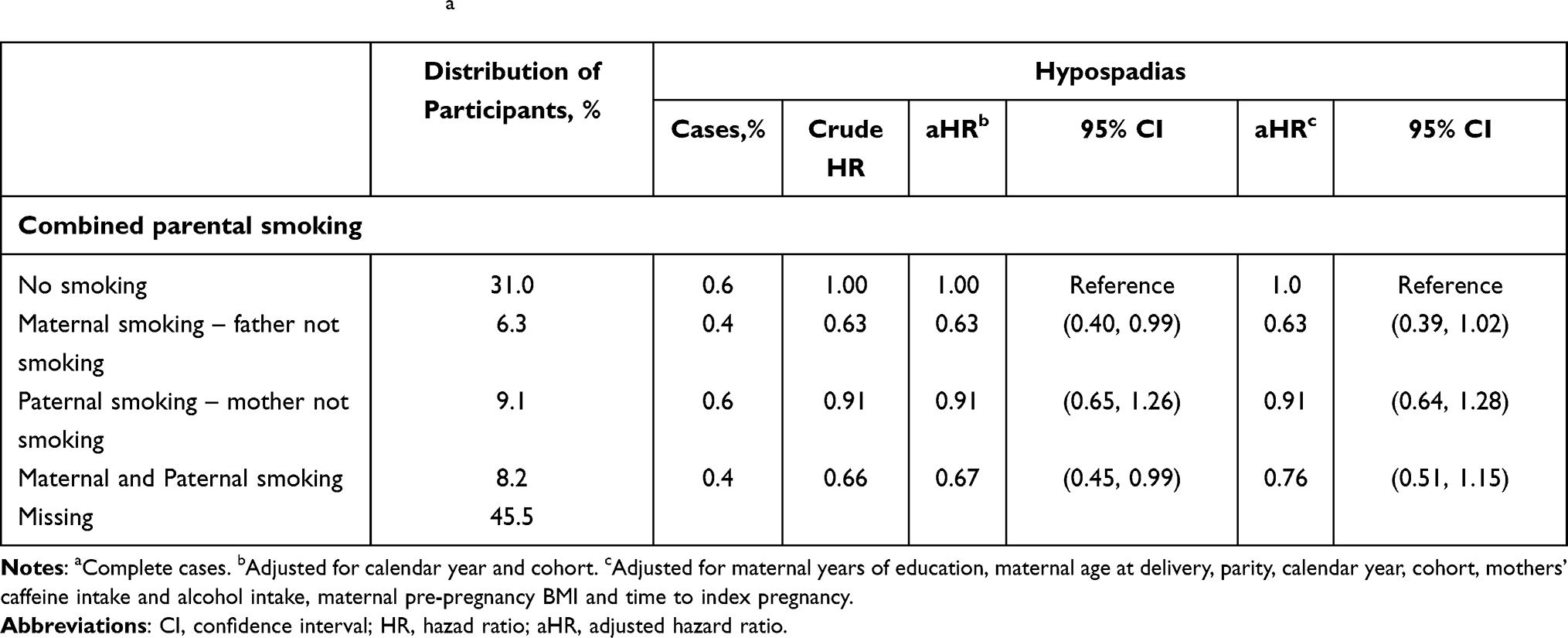 |
Table 3 Hazard Ratios (HR) for Hypospadias According to Paternal and Parental Smoking During Pregnancy Among 85,923 Singleton Live-Born Boys, Denmark 1989–2012a |
Discussion
Maternal cigarette smoking during pregnancy was associated with lower occurrence of hypospadias in this large population-based cohort study including 85,923 mother–son pairs. Neither alcohol intake, caffeine intake nor BMI were strongly associated with hypospadias.
Previous studies have also linked maternal cigarette smoking to lower risk of hypospadias.5,6 A meta-analysis from 2011 including 15 studies, found an overall lower risk for hypospadias (OR 0.90 (95% CI 0.85; 0.95)).5 Two of the original studies, Källen et al19 and Rodrigues-Pinilla et al20 observed a statistically significantly lower risk, whereas the other studies included did not. Following the meta-analysis, a few studies have been conducted,21–24 and in 2017 Carmichael et al reported that boys born to mothers with several hazardous lifestyle factors during pregnancy had lower risk of hypospadias.6 We also explored the combined impact of maternal lifestyle factors (Supplementary Table 3a), but did not corroborate their results. A causal association between smoking and hypospadias is supported by the doses-response analyses as well as the analysis of combined parental smoking. If causal, it could possibly be explained by the antiestrogenic effect of smoking during pregnancy.25 However, the finding may be due to familial and genetic confounding. We therefore conducted a sensitivity analysis with the E-value26 to examine the level of uncontrolled confounding that would be needed to explain away the estimate observed for maternal smoking during pregnancy (0.66, 95% CI 0.43, 1.02). We found an E = 2.4 for the estimate and E = 1 for the upper confidence interval. According to VanderWeele and Ding,26 the E-value concludes that by a risk ratio of 2.4-fold each, above and beyond our measured confounders, unmeasured confounding associated with both smoking and hypospadias could explain away the entire association observed, but weaker confounding could not. We already adjusted for several important confounders, so a very strong additional confounder would be needed to explain away the entire observed association. On the other hand, the E-value for the confidence interval was 1, indicating that the estimate may be prone to unmeasured confounding (see calculation in Supplementary Material 3).26,27
Previous studies have found a dose-response association between maternal BMI and hypospadias.28 We found no association between maternal BMI and hypospadias in the present study but since obese women were few (6.8%), we had low exposure contrast. Moreover, body weight may be underreported and misclassification cannot be rejected.29 Our results for alcohol, binge drinking and caffeine were similar to the majority of previous studies6,24,30–33 but it cannot be rejected that higher exposure levels, not highly present in our data, could be associated with hypospadias.
Selection bias cannot be excluded even though we utilized two large Danish birth cohorts with high participation rates34 in combination with the unique and comprehensive registration in the Danish health registers. We do know that the mothers, who participated in the two cohorts had higher socioeconomic status and were slightly healthier than non-participants,35 but this has been suggested not to introduce selection bias when examined for some well-known associations in the DNBC, but rather affect the generalizability.34 More importantly, we have almost complete follow-up, since the outcome information were registrations in the DNPR and thereby available for essentially all subjects. Further, we do not consider live-birth bias a major issue in our study because hypospadias is considered a mild congenital malformation in non-syndrome cases, and syndromic cases of hypospadias were excluded from our study population. We used detailed information on potential confounding factors, but unknown or residual confounding may still exist. We did not adjust for maternal country of birth since the majority of participants in the two cohorts were Caucasians. Information on hypospadias was only obtained from the DNPR diagnoses, which has been shown to be accurate with a high positive predictive value, but the validity of the diagnose subtype codes were not good enough to distinguish our results for type/degree of hypospadias.36 It is possible that some mild forms of hypospadias are never recognized by doctors or parents and therefore never diagnosed. A study from 2005 by Boisen et al, found the prevalence in Denmark to be 4.64% when following Danish boys from birth to 3 years of age.37 The much larger number of hypospadias diagnoses in the study was due to milder cases of hypospadias, but in our study, we do not expect this to differ by maternal lifestyle. We expect some degree of misclassification on self-reported maternal lifestyle factors, however, most likely non-differential, as data were collected in early pregnancy. The data confirmed the well-known association between maternal cigarette smoking and lower birthweight,38 which strengthens the validity of the information (data not shown).
Despite the large number of participants, we did not have sufficient power to perform a sibling analysis which provide better confounder control.39 Such design could potentially provide additional future insights as to whether environmental, social and genetic factors shared between siblings may explain the findings in our study.
Conclusion
In conclusion, maternal smoking during pregnancy was associated with lower occurrence of hypospadias. Whether the association is causal or spurious or due to bias remains unknown.
Acknowledgments
The establishment of DNBC was possible with a significant grant from the Danish National Research Foundation. Further support was given from the Danish Regional Committees; the Pharmacy Foundation; the Egmont Foundation, the March of Dimes Birth Defects Foundation; the Health Foundation and other minor grants. Additionally, supported by the Danish Medical Research Council [grant numbers SSVF 0646, 271-08-0839/06-066023, O602-01042B, 0602-02738B]; The Innovation Fund Denmark [grant number 0603-00294B 09-067124]; the Lundbeck Foundation [grant number 195/04, R100-A9193]; the Nordea Foundation [grant number 02-2013-2014]; Aarhus Ideas [grant number AU R9-A959-13-S804]; University of Copenhagen Strategic Grant [grant number IFSV 2012], and the Danish Council for Independent Research [grant numbers DFF – 4183-00594, DFF - 4183-00152]. The Danish Research Council; the Danish Agency for Science; Technology and Innovation; Aase and Einar Danielsen’s Fond, and Tryg-Fonden supported the ABC.
Disclosure
This work was supported by The Danish Council for Independent Research by providing a scholarship [grant number DFF – 6110-00360] to Camilla Lomholt Kjersgaard. The authors reports no other conflicts of interest in this work.
References
1. Carmichael SL, Shaw GM, Laurent C, Lammer EJ, Olney RS; National Birth Defects Prevention Study. Hypospadias and maternal exposures to cigarette smoke. Paediatr Perinat Epidemiol. 2005;19(6):406–412. doi:10.1111/j.1365-3016.2005.00680.x
2. Mieusset R, Soulie M. Hypospadias: psychosocial, sexual, and reproductive consequences in adult life. J Androl. 2005;26(2):163–168. doi:10.1002/j.1939-4640.2005.tb01078.x
3. Lund L, Engebjerg MC, Pedersen L, Ehrenstein V, Norgaard M, Sorensen HT. Prevalence of hypospadias in Danish boys: a longitudinal study, 1977–2005. Eur Urol. 2009;55(5):1022–1026. doi:10.1016/j.eururo.2009.01.005
4. Jensen MS, Wilcox AJ, Olsen J, et al. Cryptorchidism and hypospadias in a cohort of 934,538 Danish boys: the role of birth weight, gestational age, body dimensions, and fetal growth. Am J Epidemiol. 2012;175(9):917–925. doi:10.1093/aje/kwr421
5. Hackshaw A, Rodeck C, Boniface S. Maternal smoking in pregnancy and birth defects: a systematic review based on 173 687 malformed cases and 11.7 million controls. Hum Reprod Update. 2011;17(5):589–604. doi:10.1093/humupd/dmr022
6. Carmichael SL, Ma C, Shaw GM; National Birth Defects Prevention Study. Maternal smoking, alcohol, and caffeine exposures and risk of hypospadias. Birth Defects Res. 2017;109(14):1127–1133. doi:10.1002/bdr2.1044
7. Olsen J, Melbye M, Olsen SF, et al. The Danish National Birth Cohort–its background, structure and aim. Scand J Public Health. 2001;29(4):300–307. doi:10.1177/14034948010290040201
8. Henriksen TB, Baird DD, Olsen J, Hedegaard M, Secher NJ, Wilcox AJ. Time to pregnancy and preterm delivery. Obstet Gynecol. 1997;89(4):594–599. doi:10.1016/S0029-7844(97)00045-8
9. Welsh M, Saunders PT, Fisken M, et al. Identification in rats of a programming window for reproductive tract masculinization, disruption of which leads to hypospadias and cryptorchidism. J Clin Invest. 2008;118(4):1479–1490. doi:10.1172/JCI34241
10. Gladstone J, Nulman I, Koren G. Reproductive risks of binge drinking during pregnancy. Reprod Toxicol. 1996;10(1):3–13. doi:10.1016/0890-6238(95)02024-1
11. World Health Organization. Body mass index – BMI; 2020. Available from: http://www.euro.who.int/en/health-topics/disease-prevention/nutrition/a-healthy-lifestyle/body-mass-index-bmi.
12. Bunker ML, McWilliams M. Caffeine content of common beverages. J Am Diet Assoc. 1979;74(1):28–32. doi:10.1016/S0002-8223(21)39775-9
13. Bracken MB, Triche E, Grosso L, Hellenbrand K, Belanger K, Leaderer BP. Heterogeneity in assessing self-reports of caffeine exposure: implications for studies of health effects. Epidemiology. 2002;13(2):165–171. doi:10.1097/00001648-200203000-00011
14. Pedersen CB. The Danish civil registration system. Scand J Public Health. 2011;39(7 Suppl):22–25. doi:10.1177/1403494810387965
15. Lynge E, Sandegaard JL, Rebolj M. The Danish national patient register. Scand J Public Health. 2011;39(7 Suppl):30–33. doi:10.1177/1403494811401482
16. Knudsen LB, Olsen J. The Danish medical birth registry. Dan Med Bull. 1998;45(3):320–323.
17. Petersson F, Baadsgaard M, Thygesen LC. Danish registers on personal labour market affiliation. Scand J Public Health. 2011;39(7 Suppl):95–98. doi:10.1177/1403494811408483
18. Sterne JA, White IR, Carlin JB, et al. Multiple imputation for missing data in epidemiological and clinical research: potential and pitfalls. BMJ. 2009;338:b2393. doi:10.1136/bmj.b2393
19. Kallen K. Role of maternal smoking and maternal reproductive history in the etiology of hypospadias in the offspring. Teratology. 2002;66(4):185–191. doi:10.1002/tera.10092
20. Rodriguez-Pinilla E, Mejias C, Prieto-Merino D, Fernandez P, Martinez-Frias ML, Group EW. Risk of hypospadias in newborn infants exposed to valproic acid during the first trimester of pregnancy: a case-control study in Spain. Drug Safe. 2008;31(6):537–543. doi:10.2165/00002018-200831060-00008
21. Huang Y, Wang HY, Li PQ, Xing P. [Risk factors for different types of hypospadias]. Zhonghua Nan Ke Xue. 2017;23(5):441–447. Chinese.
22. Winston JJ, Meyer RE, Emch ME. Geographic analysis of individual and environmental risk factors for hypospadias births. Birth Defects Res a Clin Mol Teratol. 2014;100(11):887–894. doi:10.1002/bdra.23306
23. Kovalenko AA, Brenn T, Odland JO, Nieboer E, Krettek A, Anda EE. Risk factors for hypospadias in Northwest Russia: a Murmansk County birth registry study. PLoS One. 2019;14(4):e0214213. doi:10.1371/journal.pone.0214213
24. Xu LF, Liang CZ, Lipianskaya J, et al. Risk factors for hypospadias in China. Asian J Androl. 2014;16(5):778–781. doi:10.4103/1008-682X.131704
25. Michnovicz JJ, Naganuma H, Hershcopf RJ, Bradlow HL, Fishman J. Increased urinary catechol estrogen excretion in female smokers. Steroids. 1988;52(1–2):69–83. doi:10.1016/0039-128X(88)90218-8
26. VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value. Ann Intern Med. 2017;167(4):268–274. doi:10.7326/M16-2607
27. Mathur MB, Ding P, Riddell CA, VanderWeele TJ. Website and R package for computing E-values. Epidemiology (Cambridge, Mass.). 2018;29(5):e45–e47. doi:10.1097/EDE.0000000000000864
28. Arendt LH, Ramlau-Hansen CH, Lindhard MS, et al. Maternal overweight and obesity and genital anomalies in male offspring: a population-based Swedish cohort study. Paediatr Perinat Epidemiol. 2017;31:317–327. doi:10.1111/ppe.12373
29. Fattah C, Farah N, O’Toole F, Barry S, Stuart B, Turner MJ. Body Mass Index (BMI) in women booking for antenatal care: comparison between selfreported and digital measurements. Eur J Obstet Gynecol Reprod Biol. 2009;144(1):32–34. doi:10.1016/j.ejogrb.2009.01.015
30. Giordano F, Carbone P, Nori F, Mantovani A, Taruscio D, Figà‐Talamanca I. Maternal diet and the risk of hypospadias and cryptorchidism in the offspring. Paediatr Perinat Epidemiol. 2008;22(3):249–260. doi:10.1111/j.1365-3016.2007.00918.x
31. Carbone P, Giordano F, Nori F, et al. The possible role of endocrine disrupting chemicals in the aetiology of cryptorchidism and hypospadias: a population-based case-control study in rural Sicily. Int J Androl. 2007;30(1):3–13. doi:10.1111/j.1365-2605.2006.00703.x
32. Gaspari L, Paris F, Jandel C, et al. Prenatal environmental risk factors for genital malformations in a population of 1442 French male newborns: a nested case-control study. Human Reprod. 2011;26(11):3155–3162. doi:10.1093/humrep/der283
33. Hussain N, Chaghtai A, Herndon CD, Herson VC, Rosenkrantz TS, McKenna PH. Hypospadias and early gestation growth restriction in infants. Pediatrics. 2002;109(3):473–478. doi:10.1542/peds.109.3.473
34. Nohr EA, Frydenberg M, Henriksen TB, Olsen J. Does low participation in cohort studies induce bias? Epidemiology. 2006;17(4):413–418. doi:10.1097/01.ede.0000220549.14177.60
35. Jacobsen TN, Nohr EA, Frydenberg M. Selection by socioeconomic factors into the Danish National Birth Cohort. Eur J Epidemiol. 2010;25(5):349–355. doi:10.1007/s10654-010-9448-2
36. Arendt LH, Ernst A, Lindhard MS, et al. Accuracy of the hypospadias diagnoses and surgical treatment registrations in the Danish National Patient Register. Clin Epidemiol. 2017;9:483–489. doi:10.2147/CLEP.S143118
37. Boisen KA, Chellakooty M, Schmidt IM, et al. Hypospadias in a cohort of 1072 Danish newborn boys: prevalence and relationship to placental weight, anthropometrical measurements at birth, and reproductive hormone levels at three months of age. J Clin Endocrinol Metab. 2005;90(7):4041–4046. doi:10.1210/jc.2005-0302
38. England LJ, Kendrick JS, Gargiullo PM, Zahniser SC, Hannon WH. Measures of maternal tobacco exposure and infant birth weight at term. Am J Epidemiol. 2001;153(10):954–960. doi:10.1093/aje/153.10.954
39. Sjölander A, Frisell T, Öberg S. Causal interpretation of between-within models for twin research. Epidemiol Method. 2012;1:217–237. doi:10.1515/2161-962X.1015
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.