")
Back to Journals » Clinical Epidemiology » Volume 14
Life-Course Trajectories of Physical Activity and Melanoma Risk in a Large Cohort of Norwegian Women
Authors Perrier F , Ghiasvand R , Lergenmuller S, Robsahm TE , Green AC , Borch KB , Sandanger TM, Weiderpass E, Rueegg CS, Veierød MB
Received 16 July 2022
Accepted for publication 29 November 2022
Published 22 December 2022 Volume 2022:14 Pages 1571—1584
DOI https://doi.org/10.2147/CLEP.S382454
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Henrik Sørensen
Flavie Perrier,1 Reza Ghiasvand,2,3 Simon Lergenmuller,1 Trude E Robsahm,3 Adele C Green,4,5 Kristin B Borch,6 Torkjel M Sandanger,6 Elisabete Weiderpass,7 Corina S Rueegg,2 Marit B Veierød1
1Oslo Centre for Biostatistics and Epidemiology, Department of Biostatistics, Institute of Basic Medical Sciences, University of Oslo, Oslo, Norway; 2Oslo Centre for Biostatistics and Epidemiology, Oslo University Hospital, Oslo, Norway; 3Cancer Registry of Norway, Institute of Population-Based Cancer Research, Oslo, Norway; 4QIMR Berghofer Medical Research Institute, Brisbane, QLD, Australia; 5Cancer Research UK Manchester and Faculty of Biology, Medicine and Health, University of Manchester, Manchester, UK; 6Department of Community Medicine, Faculty of Health Sciences, UiT The Arctic University of Norway, Tromsø, Norway; 7International Agency for Research on Cancer, Lyon, France
Correspondence: Flavie Perrier, Oslo Centre for Biostatistics and Epidemiology, Department of Biostatistics, Institute of Basic Medical Sciences, University of Oslo, PO Box 1122, Blindern, Oslo, N-0317, Norway, Email [email protected]
Purpose: Physical activity (PA) is a cornerstone in disease prevention and varies throughout life. A pooled analysis of cohort studies and a meta-analysis of cohort studies found positive associations between PA and melanoma risk. However, previous studies focused on PA at specific ages and often lacked information on ultraviolet radiation (UVR) exposure. Using the population-based Norwegian Women and Cancer (NOWAC) cohort, including information on PA and UVR exposure, we estimated life-course PA trajectories from adolescence to adulthood and their associations with melanoma.
Methods: Total PA across different domains (recreation, occupation, transport, household) was reported for ages 14 and 30 years, and when responding to the questionnaire (31– 76 years) using a 10-point scale, validated to rank PA levels in Norwegian females. We estimated life-course PA trajectories using a latent class mixed model in 152,248 women divided into three subcohorts depending on age at questionnaire completion: 31– 39 (n = 27,098), 40– 49 (n = 52,515) and ≥ 50 years (n = 72,635). The unique 11-digit identity number of Norwegian citizens was used to link NOWAC to the Cancer Registry of Norway for information on cancer diagnoses, emigration and death. Associations between PA trajectories and melanoma risk were estimated in each subcohort using multivariable Cox regression.
Results: Five classes of individual life-course PA trajectories were identified in subcohort 31– 39 years (low, moderate, high, decreasing, increasing PA) and four in subcohorts 40– 49 and ≥ 50 years (low, moderate, high, decreasing PA). No significant association was found between life-course PA trajectories and melanoma risk in any subcohort. Hazard ratios (95% confidence intervals) for the high versus moderate trajectory were 0.92 (0.66– 1.29), 1.15 (0.97– 1.37) and 0.90 (0.78– 1.05) for subcohorts 31– 39, 40– 49 and ≥ 50 years, respectively.
Conclusion: Our results do not support a positive association between PA and melanoma risk found in previous studies, which is important for public health guidelines promoting regular PA.
Keywords: physical activity, cutaneous melanoma, trajectory, cohort, women, Norway
Introduction
Physical activity (PA) varies during life in terms of frequency, duration and intensity. Thus, identifying life-course trajectories of PA is important to assess differences in PA behaviors and to understand the long-term effects of PA on health and disease risk. In recent years, several studies have estimated PA trajectories in specific age periods and associations with sociodemographic characteristics, health behaviors and outcomes such as chronic disease risk and mortality.1–8 To our knowledge, no study to date has examined life-course trajectories of PA and cutaneous melanoma occurrence. With 325,000 new cases and 57,000 deaths estimated globally in 2020, melanoma remains an important public health concern.9
PA is assumed to prevent cancer development by enhancing immune function, increasing DNA repair capacity, reducing oxidative stress, decreasing chronic inflammation and controlling weight.10–13 The studies of PA and melanoma risk have reported mixed results, including positive,14–17 inverse associations18 and no association.19–22 In particular, a pooled analysis of prospective cohort studies found a positive association between recreational PA and melanoma risk,15 and a meta-analysis of cohort studies found a positive association between cardiorespiratory fitness and melanoma risk.17 However, very few studies had information on ultraviolet radiation (UVR) exposure14,20,22 and pigmentary characteristics,14,18,20,22 the major melanoma risk factors, and none of the studies included in the pooled and meta-analysis adjusted for UVR.
Differences in the assessment of PA and geographical location may have also contributed to the mixed results. Apart from two studies that used occupational history to assess PA,14,21 most studies assessed PA (recreational, occupational or combination of the two) at a specific time in adulthood. The large population-based Norwegian Women and Cancer (NOWAC) cohort includes information on PA, UVR exposure and pigmentary characteristics and is linked to the Cancer Registry of Norway (CRN). We aimed to i) estimate life-course trajectories of PA from age 14 through adulthood and ii) investigate the association between these trajectories and subsequent development of melanoma taking UVR exposure into account.
Materials and Methods
NOWAC Cohort
Between 1991 and 2007, questionnaires were sent to over 320,000 women aged 31–76 years, randomly drawn from the Norwegian National Population Register.23 More than 172,000 participants answered (response 54%). A first and a second follow-up questionnaire was sent after five to seven years (response >79%). All women in NOWAC provided informed consent, and data were handled in accordance with the relevant ethical guidelines and regulations. The study has been approved by the Regional Committees for Medical Health Research Ethics of North Norway (2021/252094/REK Nord) and the Norwegian Centre for Research Data (2021/147992).
Physical Activity (PA)
Participants reported their current level of PA at recruitment, first or second follow-up along with their past level of PA at ages 14 and 30, using a validated 10-point scale.24 The scale was accompanied by the following explanation: “By physical activity we mean activity both at work and outside work, at home, as well as training/exercise and other physical activity, such as walking, etc. Please mark the number that best describes your level of physical activity; 1 being very low and 10 being very high”.25 Based on this question, PA refers to total amount of PA across different domains (recreation, occupation, transport, and household) at ages 14 and 30, and age at PA questionnaire completion, either at recruitment or follow-up questionnaire. The scale has been validated to rank PA levels in the Norwegian female population, but not to quantify the “dose” of PA (intensity, duration, frequency).24 The PA scale was compared with aerobic fitness (intra-class correlation coefficient 0.62), and PA energy expenditure acceleration and hours/day of moderate-to-vigorous intensity PA obtained from a heart rate and movement sensor (correlation coefficients 0.36–0.46). PA at questionnaire completion has previously been positively associated with sunbathing vacations and indoor tanning and inversely associated with sunburns.22
Other Exposures
Questions about pigmentation characteristics and UVR exposure in NOWAC have been described in detail,26–28 and reproducibility was good (kappa/intraclass correlation coefficients 0.49–0.77) and independent of age, education and skin color.27 Hair color (black/dark brown, brown, blond/yellow, or red) and untanned skin color (using a color scale graded from 1 (very fair) to 10 (very dark)) were reported. Ambient UVR of residence was categorized based on mean ambient UVR hours of the region of residence (latitudes, 70°–58°N), as low (northern Norway), medium-low (central Norway), medium (southwestern Norway) and highest (southeastern Norway).28,29 Annual number of severe sunburns, annual number of weeks spent on sunbathing vacations in countries of low (typically southern European countries) and high latitudes (within Norway/northern countries) and frequency of indoor tanning during various periods of adulthood were recorded at baseline and updated during follow-up.28 For the most recent age period (5–10 years prior to the questionnaire), we categorized annual number of sunburns as never, 1, and ≥2, annual number of weeks of sunbathing vacations as never, 1, 2–3 and ≥4, and frequency of indoor tanning use as never, rarely and ≥1 time/month.
Participants also reported years of education (categorized as ≤10, 11–13 and ≥14 years) and smoking status (never, former, current). Body mass index (BMI, kg/m2) was calculated from self-reported height and weight (categorized as normal weight <25.0, overweight 25.0–29.9 and obese ≥30.0)30 at baseline and updated during follow-up.
Follow-Up and Endpoints
Using the unique 11-digit identity number of Norwegian citizens, the NOWAC cohort was linked to the CRN for information on cancer incidence, emigration and death. Melanoma cases were defined as first incident invasive melanoma.
Study Samples
Baseline was defined as the first returned questionnaire (recruitment, first or second follow-up) with information on current PA. Among 172,472 participants who answered the recruitment questionnaire, we excluded 7836 women with missing information on PA in all questionnaires (Figure 1), ie, who never received PA questions (n = 298) or who never reported PA at ages 14 and 30, recruitment, 1st and 2nd follow-up (n = 7538). Baseline was set at recruitment for participants who did not report current PA in any of the questionnaires (neither recruitment nor follow-up questionnaires) but who reported past PA at age 14 and/or 30. We further excluded women with melanoma or other cancers diagnosed prior to baseline (n = 12,120), women who died or emigrated before returning the baseline questionnaire (n = 21) and women who reported very dark skin color (grades 9–10, n = 247).31 In total, 152,248 participants were included in this study, aged 31–76 years, and had the opportunity to retrospectively report PA at ages 14, 30 and at baseline. Because of the wide age range at baseline, participants were analyzed in three subcohorts based on age when reporting PA at baseline: 31–39 years (n = 27,098), 40–49 years (n = 52,515) and ≥50 years (n = 72,635).
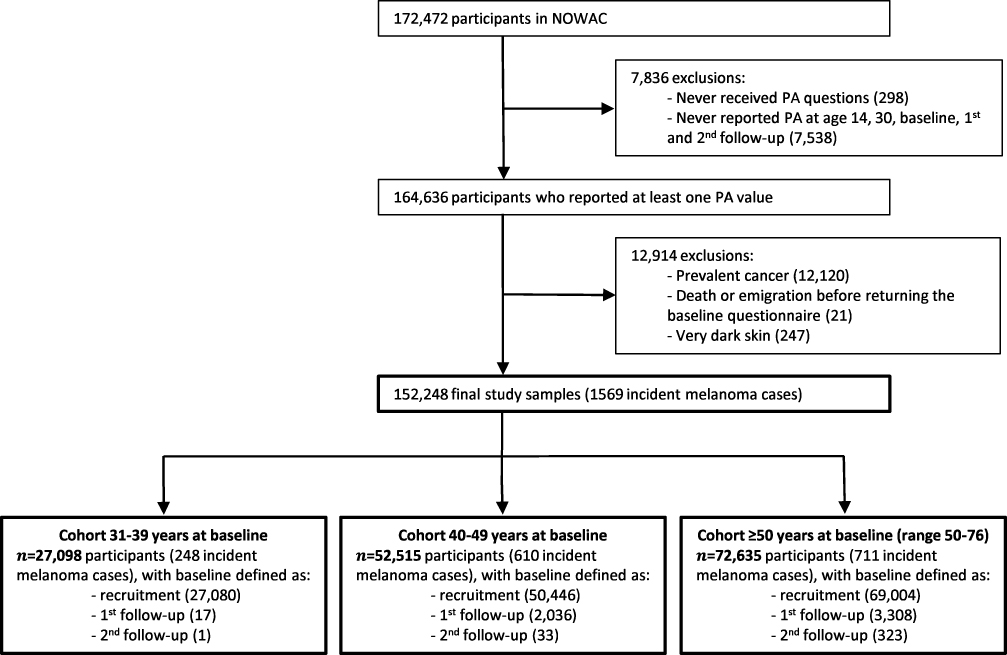 |
Figure 1 Flowchart of the subcohorts from the Norwegian Women and Cancer (NOWAC) study for the analysis of life-course trajectories of physical activity (PA) and risk of melanoma, 1991–2018. |
Statistical Analyses
Trajectories
LCMM (also known as growth mixture modeling) was used to estimate life-course PA trajectories, ie, classes (groups) of participants following a similar PA pattern over time,32 separately in each subcohort (31–39 years, 40–49 years and ≥50 years at baseline). Age (14, 30 and age at baseline) was set as time indicator and included as fixed terms (linear and quadratic) and class-specific terms (linear and quadratic). For each subcohort, trajectory models including 2, 3, 4 and 5 classes were evaluated. We chose the number of classes (k) that best fit with our data based on Akaike Information Criterion (AIC), Bayesian Information Criterion (BIC), entropy, classes’ distribution and posterior probability. A grid of 100 initial values was used to prevent any convergence toward a local maximum. Participants who reported PA at least once were included (LCMM takes into account incomplete exposure).
Three-Step Approach
To assess the association between PA trajectories and melanoma risk, we used a three-step approach33,34 combined with Cox proportional hazards regression. The trajectory analysis, described above, is the first step. The second step consists in assigning class membership to each participant. Posterior probabilities of belonging to each of the k classes were computed for each participant. We then used the proportional assignment method,34,35 ie, each participant was replicated k times in the dataset and assigned to each of the k classes together with its related posterior probabilities. In the third step, we investigated the association between class membership of PA trajectories from step 2 and melanoma risk in a Cox proportional hazard model estimating hazard ratios (HRs) and 95% confidence intervals (CIs). To take the uncertainty of classification into account, the posterior probabilities from step 2 were used as weights. We used age as time-scale, calculating person-years from baseline to date of diagnosis of first melanoma or any other primary cancer, emigration, death or end of follow-up (31st December 2018) whichever occurred first. A directed acyclic graph (DAG) was used to model the relationship between PA trajectories and melanoma risk, based on current knowledge on melanoma risk factors (Figure S1). Based on this DAG, we used three adjustment sets of covariates. Model 0 is the age-adjusted model. In model 1, we additionally adjusted for education and smoking corresponding to the minimal set of covariates necessary to control for confounding when estimating the total effect of PA on melanoma risk based on the DAG. In model 2, we further adjusted for hair color as a proxy of sensitivity to UVR exposure,26 residential ambient UVR exposure and height, corresponding to the maximal set of covariates based on the DAG. Sunbathing vacations, sunburn, indoor tanning and obesity were not included in the maximal set of covariates identified by the DAG as they are mediators on the path from PA trajectories to melanoma. Only participants with complete information for all adjustment covariates were included in step 3.
Additional adjustment for sunbathing vacations, sunburn, indoor tanning and BMI (as a proxy of obesity) was also carried out. We also conducted sensitivity analysis based on an alternative DAG in which the arrow between PA trajectories and obesity was reversed (Figure S2). Based on this alternative DAG, we further adjusted for BMI in model 1 and for BMI and indoor tanning in model 2.
Naïve Approach
In addition to the 3-step approach, we also implemented a naïve approach. For this approach, PA at ages 14, 30 and baseline were regrouped into three categories: low (1–4), moderate (5–6) and high (7–10).36 Thus, there were 27 possible naïve trajectories combining the three categories of PA at the three time points. We regrouped the 27 possible naïve trajectories into five groups: low, moderate, high, decreasing and increasing (Table S1). The association between the naïve trajectories and melanoma risk was then investigated using Cox proportional hazard models with the same adjustment sets as in the three-step approach in each subcohort. Only participants with complete information for PA at ages 14, 30 and baseline were included in the naïve trajectories.
For graphical representations of predicted life-course trajectories and Sankey diagrams of PA trajectory classes obtained with latent class mixed model (LCMM) and naïve life-course trajectory analysis, participants needed to belong to a unique trajectory class. Thus, the modal assignment method was used (ie, each participant was assigned to the class with the highest posterior probability computed in step 2 above).
Statistical analyses were carried out using the R software (https://www.r-project.org/), including lcmm package for the LCMM trajectory’s analysis.37 We used two-sided tests and a 5% statistical significance level. The Strengthening the Reporting of Observational studies in Epidemiology (STROBE) reporting guidelines were used (Supplementary Materials).
Results
Characteristics of Study Participants
Women in the youngest subcohort (31–39 years at baseline) were recruited earlier, followed for a longer period and were younger at end of follow-up and at diagnosis compared to the other subcohorts (40–49 years and ≥50 years at baseline, Table 1). Participants from the youngest subcohort were also more likely to be in the highest category of education, currently smoking, have a lower BMI, report fewer sunburns and sunbathing vacations, and use indoor tanning devices more often (Table 1). PA at age 14 and baseline were similar in the three subcohorts (mean PA at age 14: 6.5, 6.5 and 6.8, for subcohorts 31–39, 40–49 and >50 years at baseline, respectively, and mean PA at baseline: 5.7 for all the subcohorts), while PA at age 30 was highest in the oldest subcohort (mean PA: 5.8, 6.2 and 6.7, for subcohorts 31–39, 40–49 and >50 years, respectively) (Table 1 and Figure S3). A total of 248, 610 and 711 women were diagnosed with primary incident melanoma in subcohorts 31–39, 40–49 and ≥50 years, respectively.
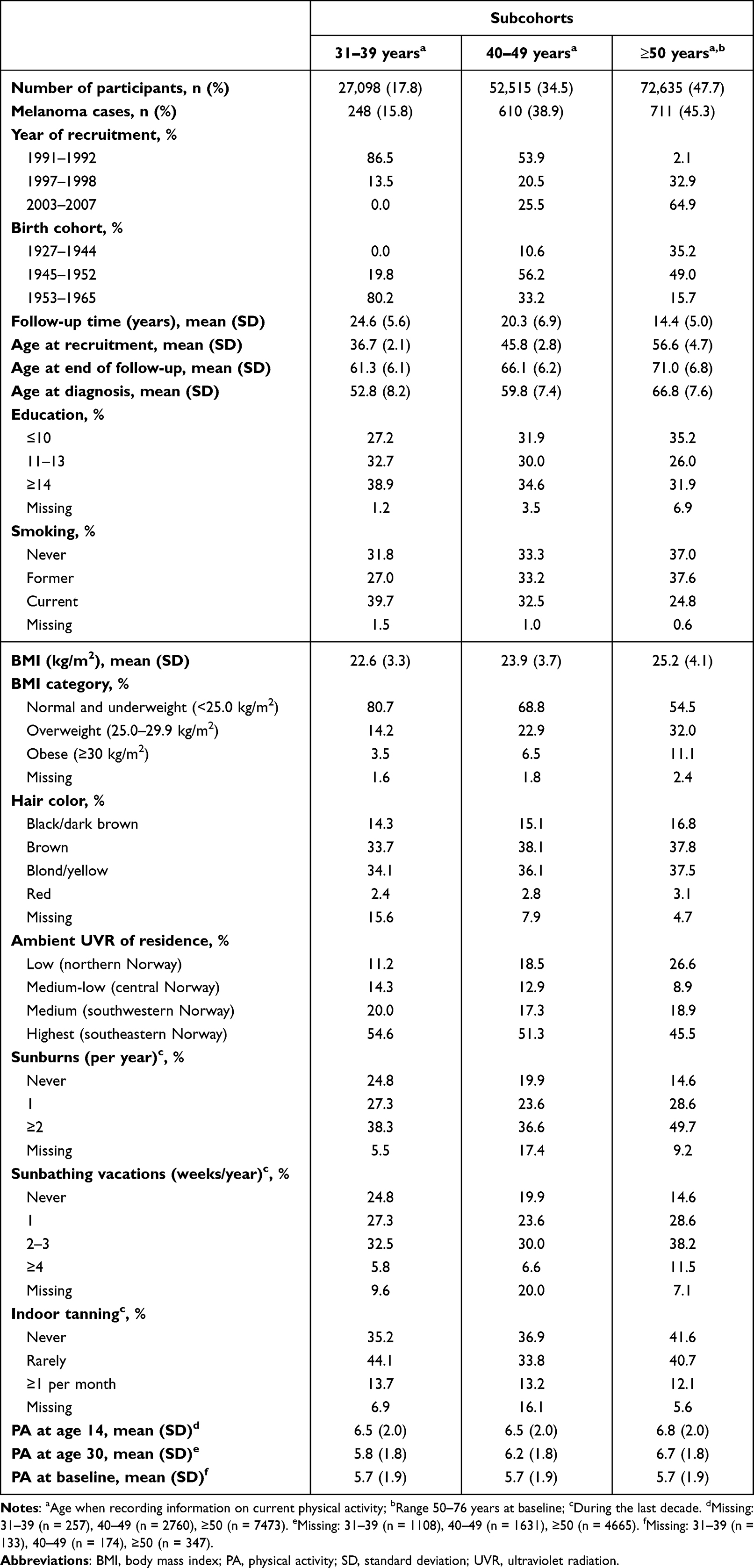 |
Table 1 Baseline Characteristics of the Study Sample from the Norwegian Women and Cancer Study (1991–2018, n = 152,248), Stratified by Subcohorts Labelled According to Age at Baseline |
Trajectory Analysis
Based on the best compromise between discrimination capacity (high entropy), model quality (low AIC and BIC), classes’ distribution and posterior probabilities (Tables S2 and S3), LCMM identified five life-course PA trajectory classes (low, moderate, high, decreasing and increasing) for subcohort 31–39 years (Figure 2A) and four (low, moderate, high and decreasing) for subcohorts 40–49 and ≥50 years (Figure 2B and C). Most participants in the youngest subcohort were in the moderate (34%) or decreasing (33%) classes. An increasing life-course trajectory class (10%) was only identified in the youngest subcohort. Trajectory patterns and participants’ distribution in the four classes were similar up to age 50 in the two oldest subcohorts (Figure 2), except for a steeper decrease by increasing age in the decreasing class in the 40–49 subcohort. In the ≥50 years subcohort, PA decreased in all the classes after age 50. Almost half of the participants in the older cohorts were allocated to the moderate class (46% for 40–49 years and 50% for ≥50 years). In all three subcohorts, participants in the high PA class were more likely to have a lower BMI, less sunburns, use indoor tanning more often and spend more time on sunbathing vacations (Tables S4–S6).
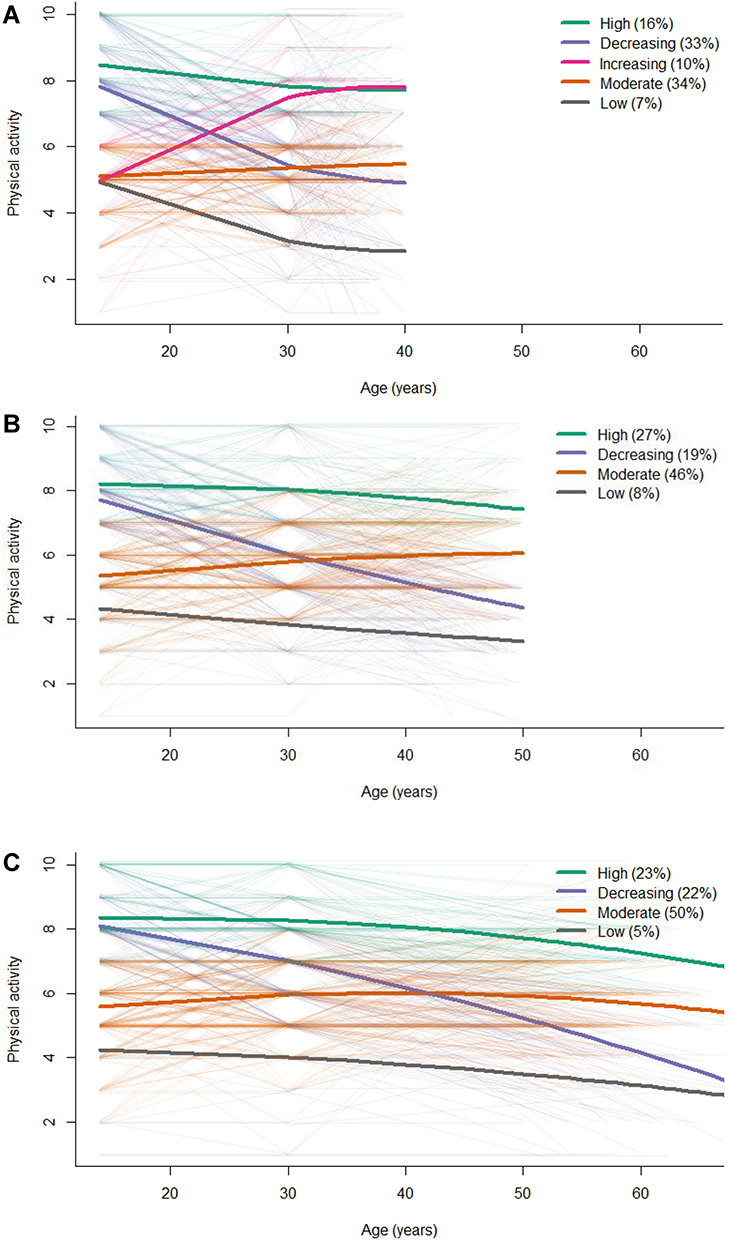 |
Figure 2 Class-specific average predicted life-course trajectories (bold lines) of physical activity for each subcohort: 31–39 years (A), 40–49 years (B) and ≥50 years (C) at baseline, the Norwegian Women and Cancer study, 1991–2018, n = 152,248. Note: The thinner lines in the background represent observed individual trajectories of 500 participants randomly selected in each subcohort. |
With the naïve approach, most participants were assigned to the moderate or high PA life-course trajectory classes for all subcohorts, and there was major overlap between the LCMM and naïve classes (Figure 3 and Figure S4). For subcohorts 40–49 and ≥50 years, the main difference between the two approaches was that the naïve-increasing class was part of the LCMM-moderate class.
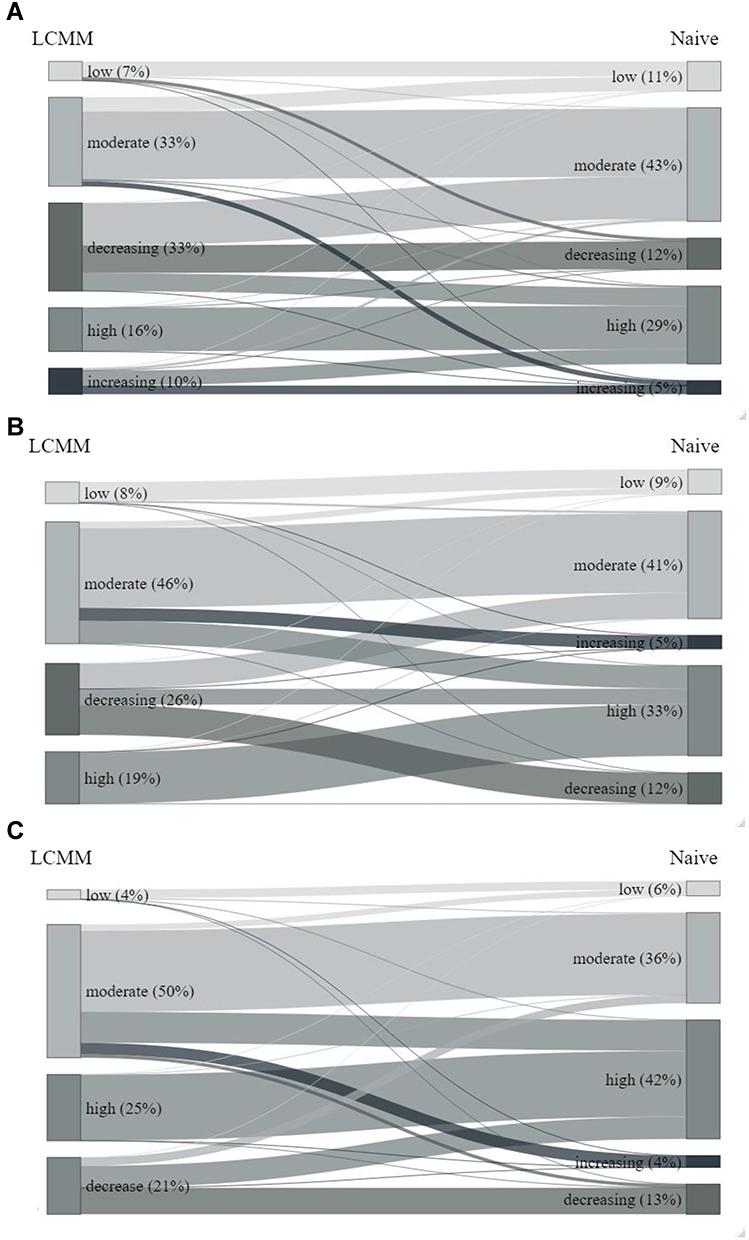 |
Figure 3 Sankey diagrams of physical activity trajectory classes obtained with latent class mixed model (LCMM) and naïve life-course trajectory analysis, for each subcohort: 31–39 years (A), 40–49 years (B) and ≥50 years (C) at baseline, in the Norwegian Women and Cancer study, 1991–2018, n = 137,800. |
PA Trajectories and Melanoma Risk
Using the moderate trajectory as reference, LCMM life-course PA trajectories were not significantly associated with melanoma in any subcohorts with models 0, 1 and 2 (Table 2; HR (95% CI) for high versus moderate with model 2 were 0.92 (0.66–1.29), 1.15 (0.97–1.37) and 0.90 (0.78–1.05) for subcohorts 31–39, 40–49 and ≥50 years at baseline, respectively). In the youngest subcohort, women who increased their level of PA from adolescence to adulthood had a non-significant lower risk of melanoma compared to moderately active women (HR = 0.77, 95% CI = 0.54–1.08, model 2). Further adjustment for sunbathing vacations, sunburns, indoor tanning and BMI did not change the results (Table S7). Sensitivity analysis using an alternative DAG where the arrow between PA and obesity was reversed also gave similar results (Table S8).
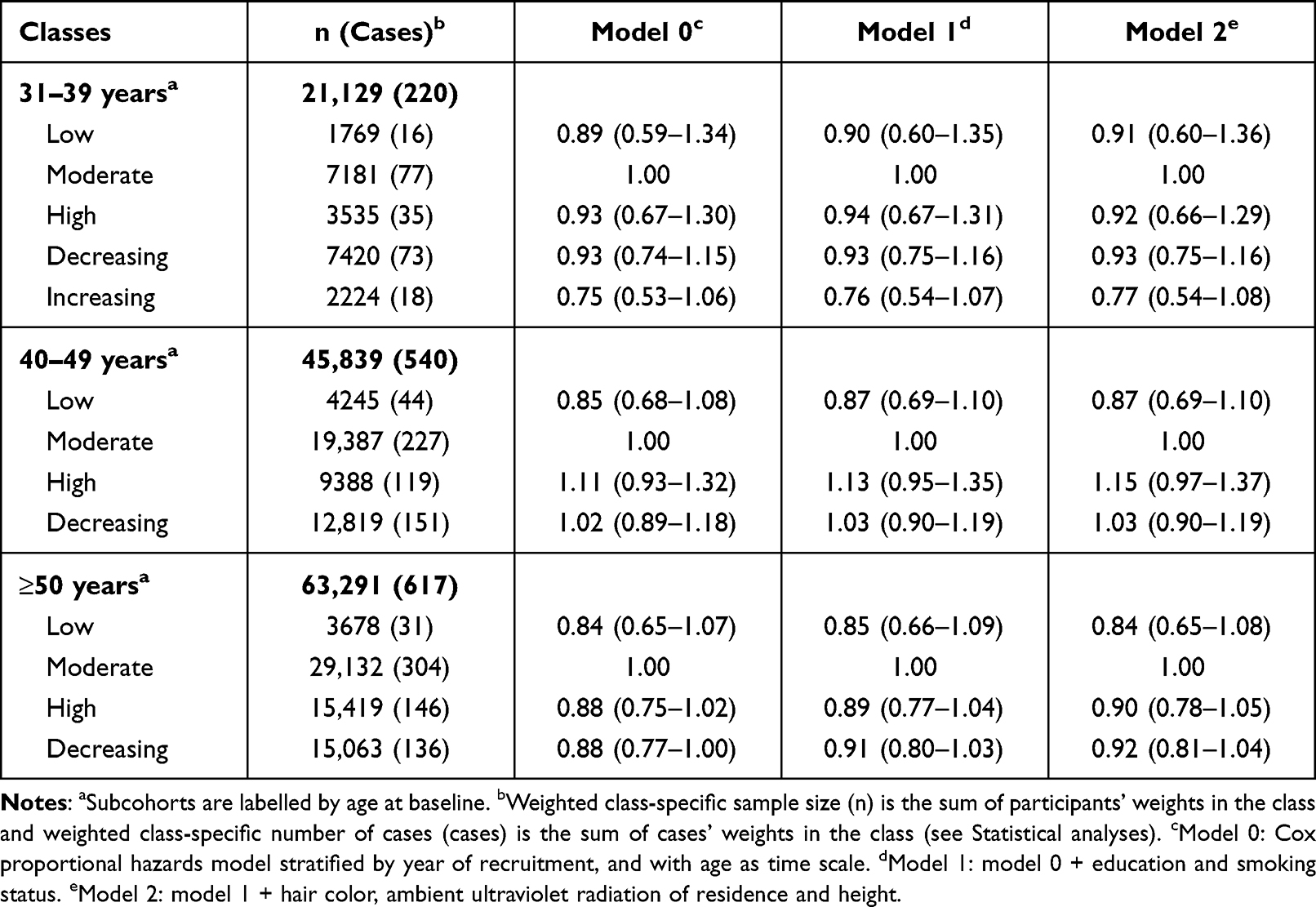 |
Table 2 Hazard Ratios (HRs) and 95% Confidence Intervals (CIs) for Melanoma Risk in Life-Course Physical Activity Trajectories (Latent Class Mixed Model) Using the Moderate Trajectory Class as Reference in Each Subcohort of the Norwegian Women and Cancer Study, 1991–2018, n = 130,259 |
As for LCMM trajectories, the naïve PA trajectories were not associated with melanoma risk in any subcohort, regardless of adjustment for UVR exposure (Table 3). In the oldest subcohort, a non-significantly reduced risk of melanoma was found for women in the low compared to the moderate trajectory (HR = 0.69, 95% CI = 0.46–1.04, model 2). The 40–49 years subcohort was the only subcohort with positive (though non-significant) associations.
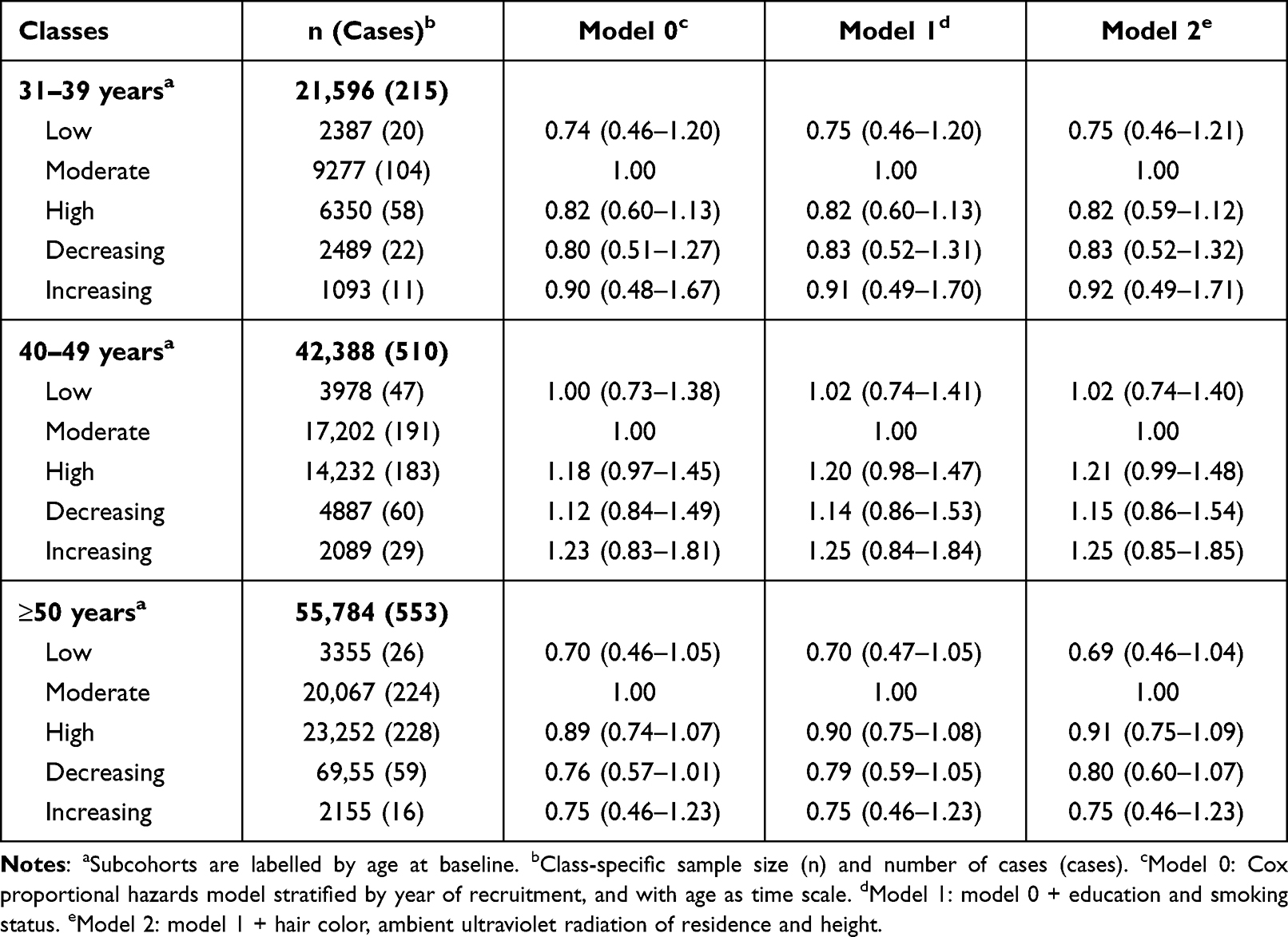 |
Table 3 Hazard Ratios (HRs) and 95% Confidence Intervals (CIs) for Melanoma Risk in Life-Course Naïve Trajectories of Physical Activity Using the Moderate Trajectory Class as Reference for Each Subcohort in the Norwegian Women and Cancer Study, 1991–2018, n = 119,768 |
Discussion
Using three measures of PA from adolescence through adulthood, the LCMM approach identified five life-course trajectory classes for the subcohort aged 31–39 years at baseline (low, moderate, high, decreasing and increasing) and four for the subcohorts 40–49 and ≥50 years at baseline (low, moderate, high and decreasing). These trajectory classes overlapped largely in all subcohorts with the five naïve classes (low, moderate, high, decreasing and increasing). We did not find any significant associations between the LCMM or naïve life-course PA trajectory classes and melanoma risk.
PA trajectories have been studied during different periods in life, including childhood/adolescence6 and different periods of adulthood (early, mid and old).3–5,36,38,39 A recent systematic review found that three to five PA trajectory classes were reported by most studies.1 However, a maximum of 10 classes has also been reported.8 Differences between studies in number of trajectories might be explained by differences in age periods, length of trajectory period, number of PA measures used, PA type, sex, sample size and method used to estimate the trajectories.
Since age when assessing current PA at baseline ranges over several age decades in women participating in the NOWAC study, we divided the cohort into three subcohorts and investigated PA trajectories in each subcohort separately. Different patterns of PA trajectories were obtained in the subcohorts. In particular, no increasing PA class was found for the two oldest subcohorts. Participants in the increasing PA class in the youngest subcohort might decrease their level of PA later in life and thereby move to the moderate PA class when reaching the age of the oldest subcohort. Indeed, in subcohorts 40–49 and ≥50 years at baseline, participants assigned to the increasing PA class using the naïve method were assigned to the moderate PA class by LCMM. The absence of increasing class was also reported by a systematic review of PA trajectories, for the studies including the oldest participants.1
To our knowledge, this is the first study investigating the association between trajectories of life-course PA and melanoma. Our result of no association between PA trajectories and incident invasive melanoma is in agreement with some previous studies that used measures of PA at one specific time,16,19–21 and with our previous study in NOWAC investigating PA at recruitment and updated during follow-up.22 However, some studies found a positive association between PA and melanoma risk.14,15,17 Regular physical activity is recommended by public health authorities,40 thus our finding of no association of increased PA over lifetime with melanoma is reassuring.
Most studies examining the association between trajectory classes and an outcome used modal assignment (assignment of the class with the highest posterior probability) without including posterior probabilities as weights in the analysis of the association between trajectory classes and an outcome.2,4,6,8,41 We used proportional assignment for PA trajectory classes to take the classification uncertainty into account in the Cox regression.
Our study included population-based data from a large prospective cohort and a combination of occupational and recreational PA, reported at baseline for up to three different time points (ages 14, 30 and study baseline) for more than 150,000 Norwegian women. The linkage to the CRN is also an important strength. Reporting of incident cancers to the CRN is compulsory in Norway, and 99.9% of the melanomas are morphologically verified.42,43 However, some misclassification of PA may exist. Questionnaires were used to record PA by a 10-point scale validated to rank current PA levels in the Norwegian female population,24 thus considered a suitable measure to differentiate PA in our study. However, no validation study has been conducted for the retrospective assessment of PA at ages 14 and 30. PA included any type of PA (occupational, recreational, commuting, home duties, etc.) and has been used to investigate PA and risk of other cancer sites.36,44–46 Depending on the subcohort, PA trajectories were estimated based on up to three PA measures over an average period of 13 to 33 years. A strength of the LCMM method applied in the current study is that it includes participants with incomplete data (ie, who did not report PA for all time points).37 As PA might change from age 30 to age at baseline, more PA measures would have improved the estimation of PA trajectories. Moreover, there may be more misclassification of PA at ages 14 and 30 years in the oldest subcohort, since the time period from age 30 to baseline was much longer (20–46 years) than for the youngest subcohort (1–9 years). Importantly, misclassification is likely non-differential since this is a cohort study with exposure recorded prior to cancer diagnosis. In addition, the PA assessment lacks information of whether PA was practiced indoor or outdoor, and the intensity, frequency and duration of PA. Studies with cardiorespiratory fitness measures would be needed to validate our findings.
The NOWAC women live in a high-latitude country. In a previous study from this cohort, we found positive associations between PA and sunbathing vacations and indoor tanning, and an inverse association between PA and sunburns.22 The latter is in contrast to studies from other climates where a positive association has been found between PA and sunburns.47–50 Our analysis was based on DAGs, taking UVR sensitivity and UVR exposure into account. Adjusting for UVR sensitivity (model 2) and UVR exposure (sensitivity analysis) did not change the results. An explanation might be that PA included both indoor and outdoor activities and UVR exposure referred to general UVR habits and did not include UVR exposure while practicing PA. Thus, our findings might not be generalizable to populations in more sunny climates where the association between PA and sun exposure is more important.50
Conclusion
In this prospective cohort study of Norwegian women aged 31–76 years at inclusion, we investigated PA trajectories over the life course with retrospective assessments of PA in adolescence and early adulthood. We identified five classes of life-course PA trajectories in the youngest subcohort and four trajectory classes in the oldest subcohorts. We did not find any associations between PA trajectories and melanoma risk. Our result does not support a positive association between PA and cutaneous melanoma risk found in previous studies, which is important for public health guidelines promoting regular PA.
Abbreviation
AIC, Akaike information criterion; BIC, Bayesian information criterion; CI, Confidence interval; CRN, Cancer Registry of Norway; DAG, Directed acyclic graph; BMI, Body mass index; HR, Hazard ratio; LCMM, Latent class mixed model; NOWAC, Norwegian Woman and Cancer; PA, Physical activity; UVR, Ultraviolet radiation.
Data Sharing Statement
The data generated and/or analysed in the current study can be accessed upon reasonable request to the originating cohort ([email protected]). Access will be conditional to adherence to local ethical and security policy. The R code used to conduct specific analyses will be shared on reasonable request (of the specific code) to the corresponding author.
Ethics Approval and Consent to Participate
All women provided informed consent, and data were handled in accordance with the relevant ethical regulations. The study has been approved by the Regional Committees for Medical and Health Research Ethics of North Norway (2021/252094/REK Nord) and the Norwegian Centre for Research Data (2021/147992) and complies with the Declaration of Helsinki.
Disclaimer
Where authors are identified as personnel of the International Agency for Research on Cancer/World Health Organization, the authors alone are responsible for the views expressed in this article and they do not necessarily represent the decisions, policy or views of the International Agency for Research on Cancer/World Health Organization.
Acknowledgments
The authors are grateful to all the women who participated in the NOWAC cohort and without whom this work would not have been possible.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the Norwegian Cancer Society (project 197975, F.P.); and the Institute of Basic Medical Sciences, University of Oslo (S.L.). The funding source had no role in the design and conduct of the study; collection, management, analysis, and interpretation of the data; preparation, review, or approval of the manuscript; and decision to submit the manuscript for publication.
Disclosure
The authors declare that they have no conflicts of interest in this work.
References
1. Lounassalo I, Salin K, Kankaanpää A, et al. Distinct trajectories of physical activity and related factors during the life course in the general population: a systematic review. BMC Public Health. 2019;19(1):271. doi:10.1186/s12889-019-6513-y
2. Coughlan D, Saint-Maurice PF, Carlson SA, Fulton J, Matthews CE. Leisure time physical activity throughout adulthood is associated with lower medicare costs: evidence from the linked NIH-AARP diet and health study cohort. BMJ Open Sport Exer Med. 2021;7(1):e001038. doi:10.1136/bmjsem-2021-001038
3. Gomes GAO, Brown WJ, Codogno JS, Mielke GI. Twelve year trajectories of physical activity and health costs in mid-age Australian women. Int J Behav Nutr Phys Activity. 2020;17(1):101. doi:10.1186/s12966-020-01006-6
4. Pettee Gabriel K, Griswold ME, Wang W, et al. Physical activity trajectories and subsequent fall risk: ARIC Study. Prev Med. 2019;121:40–46. doi:10.1016/j.ypmed.2019.02.007
5. Mok A, Khaw KT, Luben R, Wareham N, Brage S. Physical activity trajectories and mortality: population based cohort study. BMJ. 2019;365:l2323. doi:10.1136/bmj.l2323
6. Roda C, Mahmoud O, Peralta GP, et al. Physical-activity trajectories during childhood and lung function at 15 years: findings from the ALSPAC cohort. Int J Epidemiol. 2020;49(1):131–141. doi:10.1093/ije/dyz128
7. Salin K, Kankaanpaa A, Hirvensalo M, et al. Smoking and physical activity trajectories from childhood to midlife. Int J Environ Res Public Health. 2019;16(6). doi:10.3390/ijerph16060974
8. Saint-Maurice PF, Coughlan D, Kelly SP, et al. Association of leisure-time physical activity across the adult life course with all-cause and cause-specific mortality. JAMA Netw Open. 2019;2(3):e190355–e190355. doi:10.1001/jamanetworkopen.2019.0355
9. Arnold M, Singh D, Laversanne M, et al. Global burden of cutaneous melanoma in 2020 and projections to 2040. JAMA Dermatol. 2022;158(5):495–503. doi:10.1001/jamadermatol.2022.0160
10. Cash SW, Beresford SAA, Vaughan TL, et al. Recent physical activity in relation to DNA damage and repair using the comet assay. J Phys Act Health. 2014;11(4):770–776. doi:10.1123/jpah.2012-0278
11. de Sousa CV, Sales MM, Rosa TS, Lewis JE, de Andrade RV, Simões HG. The antioxidant effect of exercise: a systematic review and meta-analysis. Sports Med. 2017;47(2):277–293. doi:10.1007/s40279-016-0566-1
12. Cao Dinh H, Beyer I, Mets T, et al. Effects of physical exercise on markers of cellular immunosenescence: a systematic review. Calcif Tissue Int. 2017;100(2):193–215. doi:10.1007/s00223-016-0212-9
13. Fedewa MV, Hathaway ED, Ward-Ritacco CL. Effect of exercise training on C reactive protein: a systematic review and meta-analysis of randomised and non-randomised controlled trials. Br J Sports Med. 2017;51(8):670. doi:10.1136/bjsports-2016-095999
14. Lee TK, MacArthur AC, Gallagher RP, Elwood MJ. Occupational physical activity and risk of malignant melanoma: the Western Canada Melanoma Study. Melanoma Res. 2009;19(4):260–266. doi:10.1097/CMR.0b013e32832e0bae
15. Moore SC, Lee IM, Weiderpass E, et al. Association of leisure-time physical activity with risk of 26 types of cancer in 1.44 million adults. JAMA Intern Med. 2016;176(6):816–825. doi:10.1001/jamainternmed.2016.1548
16. Robsahm TE, Falk RS, Heir T, et al. Cardiorespiratory fitness and risk of site-specific cancers: a long-term prospective cohort study. Cancer Med. 2017;6(4):865–873. doi:10.1002/cam4.1043
17. Behrens G, Niedermaier T, Berneburg M, Schmid D, Leitzmann MF. Physical activity, cardiorespiratory fitness and risk of cutaneous malignant melanoma: systematic review and meta-analysis. PLoS One. 2018;13(10):e0206087. doi:10.1371/journal.pone.0206087
18. Gogas H, Trakatelli M, Dessypris N, et al. Melanoma risk in association with serum leptin levels and lifestyle parameters: a case-control study. Ann Oncol. 2008;19(2):384–389. doi:10.1093/annonc/mdm464
19. Veierod MB, Thelle DS, Laake P. Diet and risk of cutaneous malignant melanoma: a prospective study of 50,757 Norwegian men and women. Int J Cancer. 1997;71(4):600–604. doi:10.1002/(sici)1097-0215(19970516)71:4<600::aid-ijc15>3.0.co;2-f
20. Shors AR, Solomon C, McTiernan A, White E. Melanoma risk in relation to height, weight, and exercise (United States). Cancer Causes Control. 2001;12(7):599–606. doi:10.1023/A:1011211615524
21. Parent ME, Rousseau MC, El-Zein M, Latreille B, Desy M, Siemiatycki J. Occupational and recreational physical activity during adult life and the risk of cancer among men. Cancer Epidemiol. 2011;35(2):151–159. doi:10.1016/j.canep.2010.09.004
22. Perrier F, Ghiasvand R, Lergenmuller S, et al. Physical activity and cutaneous melanoma risk: a Norwegian population-based cohort study. Prev Med. 2021;106556. doi:10.1016/j.ypmed.2021.106556
23. Lund E, Dumeaux V, Braaten T, et al. Cohort profile: the Norwegian women and cancer study--NOWAC--Kvinner og kreft. Int J Epidemiol. 2008;37(1):36–41. doi:10.1093/ije/dym137
24. Borch KB, Ekelund U, Brage S, Lund E. Criterion validity of a 10-category scale for ranking physical activity in Norwegian women. Int J Behav Nutr Phys Act. 2012;9:2. doi:10.1186/1479-5868-9-2
25. Lund E, Kumle M, Braaten T, et al. External validity in a population-based national prospective study--the Norwegian Women and Cancer Study (NOWAC). Cancer Causes Control. 2003;14(10):1001–1008. doi:10.1023/b:caco.0000007982.18311.2e
26. Veierod MB, Weiderpass E, Thorn M, et al. A prospective study of pigmentation, sun exposure, and risk of cutaneous malignant melanoma in women. J Natl Cancer Inst. 2003;95(20):1530–1538. doi:10.1093/jnci/djg075
27. Veierod MB, Parr CL, Lund E, Hjartaker A. Reproducibility of self-reported melanoma risk factors in a large cohort study of Norwegian women. Melanoma Res. 2008;18(1):1–9. doi:10.1097/CMR.0b013e3282f120d2
28. Ghiasvand R, Rueegg CS, Weiderpass E, Green AC, Lund E, Veierod MB. Indoor tanning and melanoma risk: long-term evidence from a prospective population-based cohort study. Am J Epidemiol. 2017;185(3):147–156. doi:10.1093/aje/kww148
29. Edvardsen K, Veierød MB, Brustad M, Braaten T, Engelsen O, Lund E. Vitamin D-effective solar UV radiation, dietary vitamin D and breast cancer risk. Int J Cancer. 2011;128(6):1425–1433. doi:10.1002/ijc.25463
30. World Health Organization. Obesity: preventing and managing the global epidemic. Report of a WHO consultation. World Health Organ Tech Rep Ser. 2000;894:i–xii, 1–253.
31. Lergenmuller S, Ghiasvand R, Robsahm TE, et al. Association of lifetime indoor tanning and subsequent risk of cutaneous squamous cell carcinoma. JAMA Dermatol. 2019;1–9. doi:10.1001/jamadermatol.2019.2681
32. Proust-Lima C, Amieva H, Jacqmin-Gadda H. Analysis of multivariate mixed longitudinal data: a flexible latent process approach. Br J Math Stat Psychol. 2013;66(3):470–487. doi:10.1111/bmsp.12000
33. Asparouhov T, Muthén B. Auxiliary variables in mixture modeling: three-step approaches using mplus. Struct Equation Model. 2014;21(3):329–341. doi:10.1080/10705511.2014.915181
34. Bakk Z, Vermunt JK. Robustness of stepwise latent class modeling with continuous distal outcomes. Struct Equation Model. 2016;23(1):20–31. doi:10.1080/10705511.2014.955104
35. Vermunt JK. Latent class modeling with covariates: two improved three-step approaches. Political Analysis. 2010;18(4):450–469. doi:10.1093/pan/mpq025
36. Oyeyemi SO, Braaten T, Licaj I, Lund E, Benjaminsen Borch K. Physical activity patterns and the risk of colorectal cancer in the Norwegian Women and Cancer study: a population-based prospective study. BMC Cancer. 2018;18(1):1216. doi:10.1186/s12885-018-5092-0
37. Proust-Lima C, Philipps V, Liquet B. Estimation of extended mixed models using latent classes and latent processes: the R package lcmm. ArXiv. 2017;78(2):56. doi:10.18637/jss.v078.i02
38. Badon SE, Gabriel KP, Karvonen-Gutierrez C, et al. Dual trajectories of physical activity and blood lipids in midlife women: the Study of Women’s Health Across the Nation. Maturitas. 2021;146:49–56. doi:10.1016/j.maturitas.2021.02.002
39. Aggio D, Papachristou E, Papacosta O, et al. Association between 20-year trajectories of nonoccupational physical activity from midlife to old age and biomarkers of cardiovascular disease: a 20-year longitudinal study of British men. Am J Epidemiol. 2018;187(11):2315–2323. doi:10.1093/aje/kwy157
40. World Health Organization. WHO Guidelines on Physical Activity and Sedentary Behaviour. World Health Organization; 2020.
41. Arem H, Loftfield E, Saint-Maurice PF, Freedman ND, Matthews CE. Physical activity across the lifespan and liver cancer incidence in the NIH-AARP diet and health study cohort. Cancer Med. 2018;7(4):1450–1457. doi:10.1002/cam4.1343
42. Larsen IK, Småstuen M, Johannesen TB, et al. Data quality at the Cancer Registry of Norway: an overview of comparability, completeness, validity and timeliness. Eur J Cancer. 2009;45(7):1218–1231. doi:10.1016/j.ejca.2008.10.037
43. Cancer Registry of Norway. Cancer in Norway 2020 - Cancer Incidence, Mortality, Survival and Prevalence in Norway. Cancer Registry of Norway; 2021.
44. Borch KB, Weiderpass E, Braaten T, Jareid M, Gavrilyuk OA, Licaj I. Physical activity and risk of endometrial cancer in the Norwegian Women and Cancer (NOWAC) study. Int J Cancer. 2017;140(8):1809–1818. doi:10.1002/ijc.30610
45. Borch KB, Weiderpass E, Braaten T, Hansen MS, Licaj I. Risk of lung cancer and physical activity by smoking status and body mass index, the Norwegian Women and Cancer Study. Eur J Epidemiol. 2019;34(5):489–498. doi:10.1093/aje/kww148
46. Borch KB, Lund E, Braaten T, Weiderpass E. Physical activity and the risk of postmenopausal breast cancer - the Norwegian women and cancer study. J Negat Results Biomed. 2014;13:3. doi:10.1186/1477-5751-13-3
47. Jardine A, Bright M, Knight L, Perina H, Vardon P, Harper C. Does physical activity increase the risk of unsafe sun exposure? Health Promot J Austr. 2012;23(1):52–57. doi:10.1071/he12052
48. Gilchrist JD, Morris KL, Dwyer LA, Conroy DE. Patterns of sun safety behaviors in parents: associations with physical activity, sedentary behavior, and access to neighborhood physical activity resources. Prev Med. 2020;132:105976. doi:10.1016/j.ypmed.2019.105976
49. Holman DM, Ding H, Guy GP, Watson M, Hartman AM, Perna FM. Prevalence of sun protection use and sunburn and association of demographic and behaviorial characteristics with sunburn among US adults. JAMA Dermatol. 2018;154(5):561–568. doi:10.1001/jamadermatol.2018.0028
50. Green AC, Marquart L, Clemens SL, Harper CM, O’Rourke PK. Frequency of sunburn in Queensland adults: still a burning issue. Med J Aust. 2013;198(8):431–434. doi:10.5694/mja12.11499
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms.php
and incorporate the Creative Commons Attribution
- Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.