Back to Journals » Diabetes, Metabolic Syndrome and Obesity » Volume 15
Life-Course Influence of Adolescent Behaviour Problems on Type 2 Diabetes in Midlife: Results from 1958 British Birth Cohort Study
Authors Saad SM, Iwundu C, Ibrahim MS ![]() , Randhawa G, Pang D
, Randhawa G, Pang D
Received 15 October 2021
Accepted for publication 26 December 2021
Published 29 March 2022 Volume 2022:15 Pages 963—972
DOI https://doi.org/10.2147/DMSO.S308620
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Ming-Hui Zou
Sadiq M Saad, Chukwuma Iwundu, Musa S Ibrahim, Gurch Randhawa, Dong Pang
Institute for Health Research, University of Bedfordshire, Luton, Bedfordshire, LU2 8LE, England
Correspondence: Musa S Ibrahim, Institute for Health Research, University of Bedfordshire, Putteridge Bury, Luton, Bedfordshire, LU2 8LE, England, Tel +447918698231, Email [email protected]
Purpose: To assess whether there is a long-term relationship between childhood behaviour problems and type 2 diabetes in midlife. The study will also investigate whether any of such relationship is independent of other factors which may be associated with type 2 diabetes.
Design: Cohort study.
Participants: A total of 9377 members of the 1958 British birth cohort participated in the biomedical survey at age 45 years. The cohort has been followed up at regular intervals in childhood (age 7, 11 and 16 years) and adulthood (23, 33, 42 and 45 years).
Predictor Variables: Information regarding childhood behaviour collected during follow-ups at ages 7, 11 and 16 years.
Main Outcome Variables: Type 2 diabetes assessed using HbA1c at age 45 years.
Results: Unadjusted estimates show that teachers reported adolescent behaviour problems at age of 16 are associated with increased risk of type 2 diabetes in midlife. After adjustment for potential confounders and mediators in childhood and adulthood, a relationship was observed between the severity of adolescent behaviour problems and type 2 diabetes risk in midlife (mild behaviour problems: OR 2.17, 95% CI 1.11– 4.23; severe behaviour problems: OR 4.40, 95% CI 1.14– 16.99). However, no such relationship was observed between behaviour problems at 7 and 11 years and type 2 diabetes in midlife.
Conclusion: There is an association between adolescent behaviour problems and an increased risk of type 2 diabetes in midlife. Further molecular/genetic studies are required to understand the biological basis for this observed association.
Keywords: type 2 diabetes, adolescent behaviour problems, 1958 British birth cohort, National Child Development Study, HbA1c
Introduction
The prevalence of childhood behaviour problems is about 6–11%.1 Childhood behaviour problems are associated with a range of medical conditions, such as chronic widespread pain,2 mental Health problems (depression and anxiety),3,4 adult health behaviours (cigarette smoking, alcohol abuse, substance misuse),4 injury and mortality in adult life.5,6 A previous study from Scotland showed that childhood emotional problems were associated with increased odds of self-reported type 2 diabetes in midlife.7 The study assessed childhood behaviour problems among 6- to 12-year olds, and type 2 diabetes was self-reported by participants during a general health survey at 46–51 years. In this study, childhood behaviour was assessed at a single time point in childhood, and diagnosis of type 2 diabetes was based on self-report only. Furthermore, previous studies suggested associations between depression in adulthood and type 2 diabetes, with increased risks of type 2 diabetes by 25% to 60% among individuals with depression.8,9 The aim of this study is to assess whether there is a long-term relationship between childhood behaviour problems and type 2 diabetes in midlife using British birth cohort data. The study will also investigate whether any of such relationship is independent of other factors that may be associated with type 2 diabetes, birth weight, gestational age, childhood cognitive ability, family history, smoking, BMI, physical activity and social class.
Subjects and Methods
Participants
The 1958 British birth cohort, also known as the National Child Development Study (NCDS), consists of over 17,000 people born within the first week of March 1958 in Britain. The cohort has been followed up at regular intervals in childhood (age 7, 11 and 16 years) and adulthood (23, 33, 42 and 45 years). During the first 3 follow-ups in childhood, information was obtained from parents, local authority and class teachers. At age 45 years, 9377 members participated in a biomedical survey, accounting for 72.1% of the 13,009 available individuals. Despite attrition due to 45 years of follow-up, the participating sample at 45 years has been shown to be a representative of the surviving cohort.10 Access to anonymised data from the surveys of the 1958 British birth cohort was granted by the United Kingdom Data Service at the Economic and Social Research Council, University of Essex, UK. Ethical approval for the present study was obtained from the University of Bedfordshire Institute for Health Research Ethics Committee. The data used in the present study can be accessed by researchers through the UK Data Service at the University of Essex.
Childhood Behaviour Problems
Measures of childhood behaviour problems were used as explanatory variables in this study. These measures were obtained during childhood at ages 7, 11 and 16 years from parents and class teachers. Reports from both parents and class teachers rating of the child’s behaviour were independently carried out at different age intervals by using different measurement scales. The measurements were mainly focused on behavioural maladjustments, hostility patterns, personality and locus of control. The two scales of child behaviour measurement used were the Bristol Social Adjustment Guide (BSAG) and the Rutter Child Behaviour Questionnaire. The Rutter Child Behaviour Questionnaire was shown to be a valid and reliable tool for assessing behaviour problems in childhood.11 In the present study, teacher-reported childhood behaviour was used because in situations that involve different formal tasks and social demands, teachers are in a better position to assess each child and make comparison with the child’s peers. Teachers rated childhood behaviour problems at school using the Rutter behaviour scale B at 16 years12 (see Appendix 1). The Bristol Social Adjustment Guide (BSAG) was used by teachers to rate childhood behaviour problems at 7 and 11 years.13 In the Rutter behaviour scale B, there were 26 items at 16 years (0–52 scale). Items on this scale were coded as 0 = does not apply/never, 1 = applies somewhat/sometimes or 2 certainly applies/frequently. The score of individual item on the scale was added for each follow-up age to obtain a total behaviour score.2 A total of 150 descriptions of behaviour or attitude at school which applies to the child is identified by the BSAG completed by teachers. These were then grouped into core syndromes as follows: unforthcomingness, withdrawal, depression, anxiety for acceptance by adults, hostility towards adults, writing off of adults and adult standards, anxiety for acceptance by children, restlessness, inconsequential behaviour, miscellaneous symptoms and miscellaneous nervous symptoms.14 To obtain a measure of childhood behaviour for this research, individual scores of each behaviour instrument were added to get a total behaviour score at different childhood ages: Rutter behaviour scale A at 7 and 11 years, 14 items (0–28 scale), and 18 items at age 16 (0–36 scale). Rutter behaviour scale B has 26 items at 16 years (0–52 scale). Each item on both scales (A and B) was recorded to have a uniform coding protocol, 0 = does not apply/never, 1 = applies somewhat/sometimes, or 2 = certainly applies/frequently. The score of the individual items on each scale were added for different follow-up age to obtain a total behaviour score for that age.2 A total behaviour score of all items on the BSAG (0–99) was obtained, with a high score indicating social maladjustment. Furthermore, to investigate whether individuals with scores suggesting behaviour problems have higher tendency of having type 2 diabetes, children (at age 7, 11 and 16 years) were grouped into 3 behaviour groups: those with normal behaviour (having a score below the 80th percentile) mild-moderate behaviour problems (having a score between 80th and 95th percentile) and severe behaviour problems (having a score above 95th percentile). This classification of children behaviour was necessary because the original behaviour scores were not comparable across the 3 age points due to different rating scales.
Type 2 Diabetes
At age 45 years, blood samples were collected in a biomedical follow-up survey, blood glucose was measured as glycosylated haemoglobin (HbA1c). HbA1c was assessed by the use of ion-exchange high performance liquid chromatography HLC-723GHbA1c 2.2; Tosoh Corp, Tokyo Japan.15,16 The presence of diabetes was determined by the measurement of glycosylated haemoglobin. Participants were classified as having type 2 diabetes if HbA1c was 6.5% (48 mmol/mol) or above;16–18
Covariates
A range of potential confounders/mediators, such as childhood cognitive ability, social class (at birth and at age 42 years), family history of diabetes, gestational age, birth weight and adult health behaviours (smoking, alcohol consumption and physical activity) were taken into account in the analysis. As a measure of childhood cognition, the Childhood General Ability test19 was utilised. The test, which had verbal (range = 0–40) and non-verbal (range = 0–40) components was administered to participants (aged 11 years) at school. Social class was classified as professional, managerial/technical, skilled non-manual, skilled manual, semi-skilled and unskilled,20 according to the Registrar General’s classification of father’s occupation in 1958. Social class at age 42 was based on the most recent occupation at age 42 years or at age 33 years, whichever is available.
Gestational age was calculated as number of weeks from the mothers’ last menstrual period to delivery. Birth weight, originally recorded in pounds and ounces,21 was converted to kilograms. Family history of diabetes was obtained from parents of study participants. Participant’s height was measured using a stadiometer. We computed body mass index (BMI) as weight in kilograms divided by height in meters squared.22 Data on smoking habit were obtained at 42 years, and participants were categorised as current smoker (if smokes 1 or more cigarette per day), former smoker or never smoker. Participant’s exercise was obtained at age 42 and was categorised as <2–3 times per month, once a week, 2–3 times per week, or 4–7 times per week. Alcohol consumption was categorised as 0, 1–2, 3–4, 5–6 or >7 units per day.
Analysis
We assessed the association between childhood behaviour problems and type 2 diabetes in adulthood using logistic regression. Odds ratio and 95% confidence interval were used to measure the association. Type 2 diabetes was treated as a binary dependent variable in the regression analysis. Analyses were carried out for teachers’ reporting of childhood behaviour problems at age 7, 11 and 16 years. Odds ratios were estimated after adjustment for childhood confounders, such as childhood cognitive ability, social class at birth, birth weight, gestational age and adulthood confounders, such as family history of diabetes, social class at 42 years, alcohol consumed at 42 years, exercise at 42 years and smoking habit. We carried out analyses for individuals with complete data on the variables examined. All analyses were carried out using Stata 13.23
Results
Table 1 shows the characteristics of study subjects in the cohort. Of the 9408 study subjects, there are 201 individuals with type 2 diabetes. The prevalence of type 2 diabetes was higher in males than females (2.8% vs 1.5%).
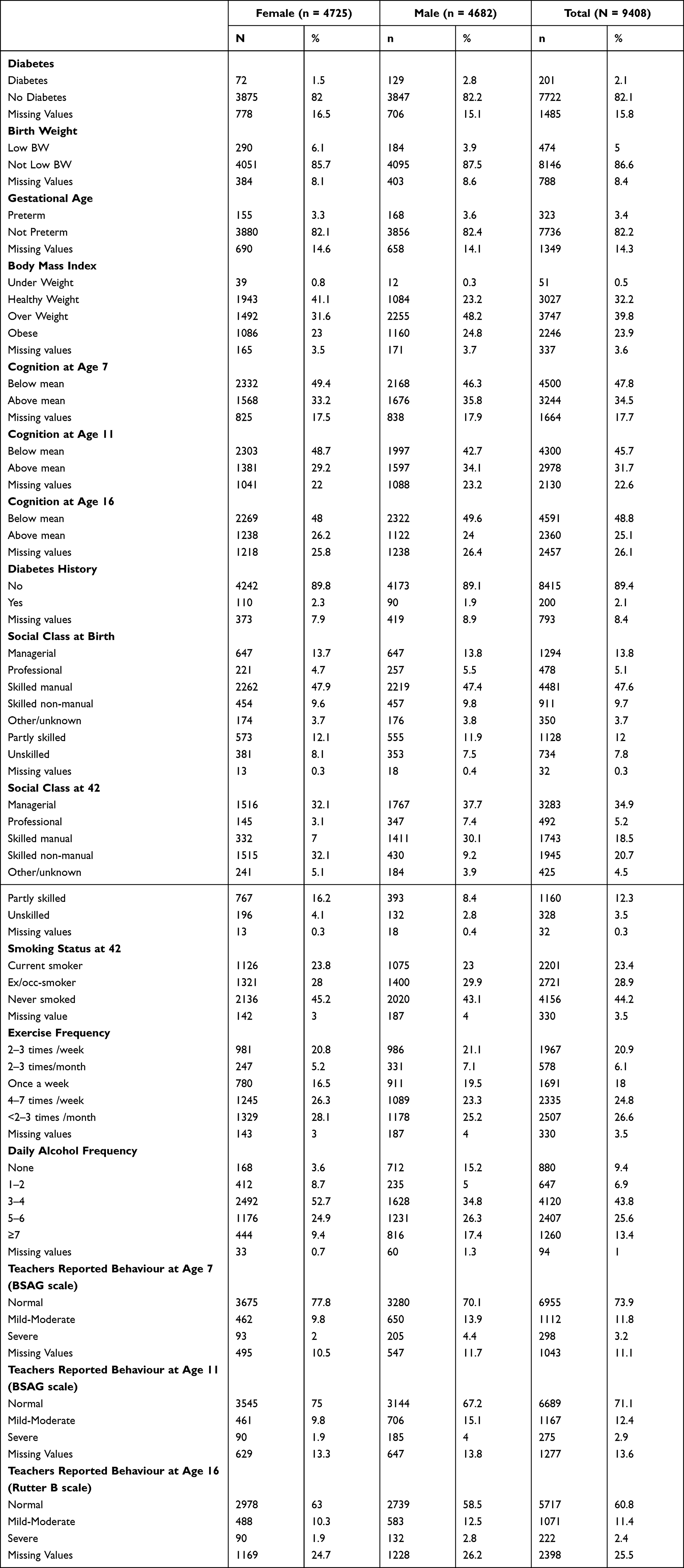 |
Table 1 Characteristics of Study Subjects |
Table 2 shows the relationship between childhood behaviour problems and type 2 diabetes at 45. There are increased odds of type 2 diabetes at 45 among individuals with mild behaviour problems at 16 (OR 1.69, 95% CI 1.14–2.51) and among those with severe problems at 16 (OR 2.29, 95% CI 1.14–4.60). These associations become stronger after adjustment for potential childhood and adulthood confounders. Compared to individuals with normal behaviour, those with mild behaviour problems at 16 have more than 2-fold increased odds of type 2 diabetes at 45 (OR 2.17, 95% CI 1.11–4.23) and those with severe behaviour problems have more than 4-fold increased odds of type 2 diabetes (OR 4.40, 95% CI 1.14–16.99), after adjustment for birthweight, gestational age, cognition, diabetes history, smoking status at 42, social class at birth, social class at 42, exercise frequency and daily alcohol consumption. In particular, males with mild-moderate behaviour problems have more than 3-fold increased odds of diabetes compared to those with normal behaviour (OR 3.38, 95% CI 1.33–8.60). Similarly, females with severe behaviour problems have more than 9-fold increased odds of diabetes compared to those with normal behaviour (OR 9.09, 95% CI 1.20–68.96). However, no such relationship was observed between behaviour problems at 7 and 11 years and type 2 diabetes at 45.
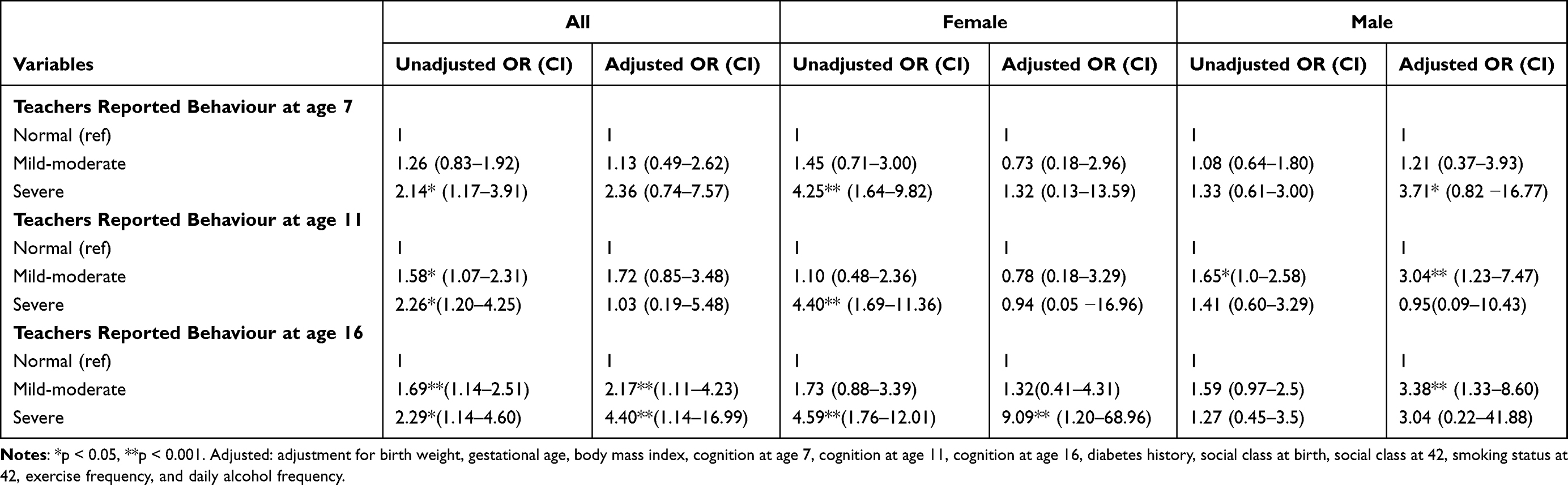 |
Table 2 Risk of Type 2 Diabetes in Midlife (Odds Ratio) According to Teachers’ Reporting of Childhood Behaviour |
Furthermore, we carried out an analysis of parental reporting of childhood behaviour problems. There are no significant findings for childhood behaviour problems at ages 7, 11 or 16 (results not shown).
Discussion
In this study, we have shown that childhood behaviour problems at 16 assessed by teachers are associated with an increased risk of type 2 diabetes in midlife. These associations were not explained away by potential childhood and adulthood confounding factors.
However, we should be cautious to draw a causal association. If consistent with other previously published studies of its kind, the observed association could be suggestive of a true causal association. However, to the best of our knowledge, this is the first study to report epidemiological evidence of the effect of childhood behaviour on type 2 diabetes in midlife. So at the time of the writing, it is difficult to know whether this result can be repeated in other populations or in different settings. However, this is possible because associations between early life environments and health outcomes in later life have already been reported. For example, studies have demonstrated links between childhood socioeconomic position and adult chronic diseases such as cardiovascular disease24 and type 2 diabetes.25,26 Also, exposure to emotional stress during childhood has been found to be associated with the risk of obesity and type 2 diabetes in midlife.27,28 It has also been suggested that exposure to psychological stress in childhood may increase the risk of adverse health behaviours like smoking29–31 and alcohol abuse.32,33 Our finding is consistent with a previous study by Thomas et al which examined the effect of childhood adversities on obesity and glucose control in the 1958 British birth cohort. Their finding suggests that stressful emotional childhood experiences increase the risk of obesity, thereby increasing the risk of type 2 diabetes.27 Similarly, a regional study by von Stumm et al has shown an association between childhood emotional problems among 6–12-year olds and self-reported type 2 diabetes in midlife among women in a Scottish birth cohort.7
In this study, the odds of having type 2 diabetes increased with increasing severity of childhood behaviour problems at 16 years. In particular, the pattern was more striking among women. In addition, the observed association with childhood behaviour was not specific to type 2 diabetes in adulthood. Childhood behaviour problems have been found to be associated with other chronic conditions such as chronic widespread pain2 and long-term mental health problems in adulthood.3,4,34
The exact mechanism underlying the observed association remains unknown; however, there are possible explanations. It is likely to be a behavioural cause of both childhood behavioural problems and type 2 diabetes. Previous evidence suggests a link between type 2 diabetes on the one hand, and obesity resulting from excess intake of calories and limited physical activity on the other, with potential interplay with other psychosocial factors.35–42 In the same vein, behaviour around food intake and activity has been implicated as a cause of the excess type 2 diabetes cases observed among individuals with mental illness and depression.43,44 Alternatively, there could be a neuroendocrine or molecular genetic defect underlying this relationship. Childhood behavioural problems could affect the developing brain, especially during the sensitive period. This is supported by genetic studies, both in animals45,46 and humans.47 Similarly, the role of long-term neuroendocrine dysregulation (hypothalamic–pituitary–adrenal axis (HPA), sympathetic nervous system (SNS) and the sympathoadrenal medullary system (SAMS))48–51 are being explored by researchers. Noteworthy, most of the evidence so far is derived from research conducted on rats. Studies have shown that the brain releases counter-regulatory hormones as a response to psychological stress, which counteracts the effect of insulin, hence raising blood glucose level.52,53 Furthermore, specific genes and receptors are implicated both in animal and human studies.54–58 Childhood behaviour problems may affect the brain via raised levels of glucocorticoids and neuroendocrine dysregulation to confer the risk of obesity, which in turn leads to subsequent type 2 diabetes. A similar suggestion was made for children with emotional disturbances.59 Other possible mechanism could be that exposure to psychological stress in early life may lead to alteration in the expression of hypothalamic feeding neuropeptide which may lead to partial increase in food intake and adiposity in adult life, Or remotely, through the mediating effect of 11β-hydroxysteroid dehydrogenase type I (11β-HSD1) in metabolic functions.60 Further genetic or molecular studies are required.
A major limitation of this study is attrition bias. Attrition bias is possible due to such a long follow-up. Of the 18,558 participants, 9377 individuals participated in the survey at 45 years. However, a recent study showed that the surviving cohort was broadly similar to the original birth population in terms of gender and social class at birth.61 Another limitation of the study is the use of only the father’s occupation to decide social class at birth. A better approach would be to include the mother’s occupation, compare the two and then select the one which is higher. The NCDS data lack detailed information about the mother’s occupation in 1958. However, father’s occupation has been used successfully in the past to denote childhood socioeconomic position in previous studies that used the NCDS data.62
Our study has a number of strengths. First, the study is based on a large population-based data, which is representative of the British population who were born in 1958. Second, an objective measure of type 2 diabetes (glycated haemoglobin, ie HbA1c) was used. Third, data on childhood behaviour problems were collected prospectively at three childhood ages 7, 11, and 16 years, free of recall bias, which is often encountered in a case-control study. Fourth, child’s behaviour was rated by both parents and class teachers. In situations that involve different formal tasks and social demands, teachers are in a better position to assess each child and make comparison with the child’s peers.2
Conclusion
In conclusion, for the first time, we demonstrated that there is an association between childhood behaviour problems and an increased risk of type 2 diabetes in midlife.
Highlights
- This study demonstrated that childhood behaviour problems are associated with an increased risk of type 2 diabetes in midlife.
- Further molecular/genetic studies are required to understand the biological basis for this observed association.
Acknowledgments
No funding received. The abstract of this paper was presented at the ‘27th European Diabetes Congress, June 20-21, 2018 Rome, Italy’ as a poster presentation with interim findings. The poster’s abstract was published in “Poster Abstracts” in J Diabetes Metabolism: https://eur03.safelinks.protection.outlook.com/?url=https%3A%2F%2Fwww.omicsonline.org%2Fconference-proceedings%2Feuro-diabetes-2018-posters-accepted-abstracts.digital%2Findex.html%2310&data=04%7C01%7CMusa.Ibrahim%40study.beds.ac.uk%7C8d433b63c20146857a2908d8e0d9301c%7C3133dbdc3c644bdaa66a751445a19275%7C1%7C0%7C637506570702041461%7CUnknown%7CTWFpbGZsb3d8eyJWIjoiMC4wLjAwMDAiLCJQIjoiV2luMzIiLCJBTiI6Ik1haWwiLCJXVCI6Mn0%3D%7C1000&sdata=9WbpH3GT0Vsbi06XQqTfL%2FFfJAmSIHWkX%2Be597hFAWQ%3D&reserved=0
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests.
References
1. Bowen E, Heron J, Steer C, El Komy M. Anti-Social and Other Problem Behaviours Among Young Children: Findings from the Avon Longitudinal Study of Parents and Children. London: Home Office Online Report; 2008.
2. Pang D, Jones GT, Power C, Macfarlane GJ. Influence of childhood behaviour on the reporting of chronic widespread pain in adulthood: results from the 1958 British birth cohort study. Rheumatology. 2010;49(10):1882–1888.
3. Colman I, Murray J, Abbott RA, et al. Outcomes of conduct problems in adolescence: 40 year follow-up of national cohort. BMJ. 2009;338:a2981.
4. Robins LN. Deviant Children Grown Up, a Sociological and Psychiatric Study of Sociopathic Personality. ERIC; 1966.
5. Jokela M, Power C, Kivimäki M. Childhood problem behaviors and injury risk over the life course. J Child Psychol Psychiatry. 2009;50(12):1541–1549.
6. Jokela M, Ferrie J, Kivimäki M. Childhood problem behaviors and death by midlife: the British National Child Development Study. J Am Acad Child Adolesc Psychiatry. 2009;48(1):19–24.
7. Von Stumm S, Deary IJ, Kivimäki M, Jokela M, Clark H, Batty GD. Childhood behavior problems and health at midlife: 35‐year follow‐up of a Scottish birth cohort. J Child Psychol Psychiatry. 2011;52(9):992–1001.
8. Knol MJ, Twisk JW, Beekman AT, Heine RJ, Snoek FJ, Pouwer F. Depression as a risk factor for the onset of type 2 diabetes mellitus. A meta-analysis. Diabetologia. 2006;49(5):837.
9. Cosgrove MP, Sargeant LA, Griffin SJ. Does depression increase the risk of developing type 2 diabetes? Occup Med (Chic Ill). 2007;58(1):7–14.
10. Power C, Elliott J. Cohort profile: 1958 British birth cohort (national child development study). Int J Epidemiol. 2005;35(1):34–41.
11. Klein JM, Gonçalves A, Silva CF. The Rutter children behaviour questionnaire for teachers: from psychometrics to norms, estimating caseness. Psico-USF. 2009;14(2):157–165.
12. Rutter M. A children’s behaviour questionnaire for completion by teachers: preliminary findings. J Child Psychol Psychiatry. 1967;8(1):1–11.
13. Stott DH, Sykes EG. Bristol Social-Adjustment Guides. University of London Press; 1963.
14. Stott DH, Sykes EG, Marston N. The Social Adjustment of Children: Manual of the British Social-Adjustment Guides. Hodder & Stoughton; 1974.
15. Chapelle J, Teixeira J, Maisin D, et al. Multicentre evaluation of the Tosoh HbA1c G8 analyser. Clin Chem Lab Med. 2010;48(3):365–371.
16. Gibb I, Parnham A, Fonfrede M, Lecock F. Multicenter evaluation of Tosoh glycohemoglobin analyzer. Clin Chem. 1999;45(10):1833–1841.
17. Ellison TL, Elliott R, Moyes SA. HbA1c screening for undiagnosed diabetes in New Zealand. Diabetes Metab Res. 2005;21(1):65–70.
18. Barr RG, Nathan DM, Meigs JB, Singer DE. Tests of glycemia for the diagnosis of type 2 diabetes mellitus. Ann Intern Med. 2002;137(4):263–272.
19. Pigeon DA. Details of the fifteen years tests. In: Douglas JWB, Ross JM, Simpson HR, editors. All Our Future. London: Davies; 1968.
20. OPCS. Social Class and Social Mobility. London: Office of Population Censuses and Surveys (OPCS); 1987.
21. Blencowe H, Cousens S, Oestergaard MZ, et al. National, regional, and worldwide estimates of preterm birth rates in the year 2010 with time trends since 1990 for selected countries: a systematic analysis and implications. The Lancet. 2012;379(9832):2162–2172.
22. World Health Organization. Obesity: Preventing and Managing the Global Epidemic. 2000:894
23. Stata C. Stata Release 13 Data Analysis and Statistical Software. College Station, Tex: StataCorp LP; 2013.
24. Galobardes B, Lynch JW, Davey Smith G. Childhood socioeconomic circumstances and cause-specific mortality in adulthood: systematic review and interpretation. Epidemiol Rev. 2004;26(1):7–21.
25. Kumari M, Head J, Marmot M. Prospective study of social and other risk factors for incidence of type 2 diabetes in the Whitehall II study. Arch Intern Med. 2004;164(17):1873–1880.
26. Lidfeldt J, Li TY, Hu FB, Manson JE, Kawachi I. A prospective study of childhood and adult socioeconomic status and incidence of type 2 diabetes in women. Am J Epidemiol. 2007;165(8):882–889.
27. Thomas C, Hypponen E, Power C. Obesity and type 2 diabetes risk in midadult life: the role of childhood adversity. Pediatrics. 2008;121(5):e1240–9.
28. Williamson DF, Thompson TJ, Anda RF, Dietz WH, Felitti V. Body weight and obesity in adults and self-reported abuse in childhood. Int J Obes. 2002;26(8):1075.
29. Anda RF, Croft JB, Felitti VJ, et al. Adverse childhood experiences and smoking during adolescence and adulthood. JAMA. 1999;282(17):1652–1658.
30. Rodgers CS, Lang AJ, Laffaye C, Satz LE, Dresselhaus TR, Stein MB. The impact of individual forms of childhood maltreatment on health behavior. Child Abuse Negl. 2004;28(5):575–586.
31. Kestilä L, Koskinen S, Martelin T, et al. Influence of parental education, childhood adversities, and current living conditions on daily smoking in early adulthood. Eur J Public Health. 2006;16(6):617–626.
32. Hope S, Power C, Rodgers B. The relationship between parental separation in childhood and problem drinking in adulthood. Addiction. 1998;93(4):505–514.
33. Anda RF, Whitfield CL, Felitti VJ, et al. Adverse childhood experiences, alcoholic parents, and later risk of alcoholism and depression. Psychiatric Serv. 2002;53(8):1001–1009.
34. Fergusson DM, John Horwood L, Ridder EM. Show me the child at seven: the consequences of conduct problems in childhood for psychosocial functioning in adulthood. J Child Psychol Psychiatry. 2005;46(8):837–849.
35. Menke A, Rust KF, Fradkin J, Cheng YJ, Cowie CC. Associations between trends in race/ethnicity, aging, and body mass index with diabetes prevalence in the United States: a series of cross-sectional studies. Ann Intern Med. 2014;161(5):328–335.
36. Reis JP, Loria CM, Sorlie PD, Park Y, Hollenbeck A, Schatzkin A. Lifestyle factors and risk for new-onset diabetes: a population-based cohort study. Ann Intern Med. 2011;155(5):292–299.
37. Lao XQ, Deng HB, Liu X, et al. Increased leisure-time physical activity associated with lower onset of diabetes in 44 828 adults with impaired fasting glucose: a population-based prospective cohort study. Br J Sports Med. 2019;53(14):895–900.
38. Grøntved A, Hu FB. Television viewing and risk of type 2 diabetes, cardiovascular disease, and all-cause mortality: a meta-analysis. JAMA. 2011;305(23):2448–2455.
39. Rimm EB, Chan J, Stampfer MJ, Colditz GA, Willett WC. Prospective study of cigarette smoking, alcohol use, and the risk of diabetes in men. BMJ. 1995;310(6979):555–559.
40. Willi C, Bodenmann P, Ghali WA, Faris PD, Cornuz J. Active smoking and the risk of type 2 diabetes: a systematic review and meta-analysis. JAMA. 2007;298(22):2654–2664.
41. Cappuccio FP, D’Elia L, Strazzullo P, Miller MA. Quantity and quality of sleep and incidence of type 2 diabetes: a systematic review and meta-analysis. Diabetes Care. 2010;33(2):414–420.
42. Crump C, Sundquist J, Winkleby MA, Sieh W, Sundquist K. Physical fitness among Swedish military conscripts and long-term risk for type 2 diabetes mellitus: a cohort study. Ann Intern Med. 2016;164(9):577–584.
43. McMartin SE, Jacka FN, Colman I. The association between fruit and vegetable consumption and mental health disorders: evidence from five waves of a national survey of Canadians. Prev Med. 2013;56(3–4):225–230.
44. Weyerer S. Physical inactivity and depression in the community. Int J Sports Med. 1992;13(06):492–496.
45. Do KQ, Cuenod M, Hensch TK. Targeting oxidative stress and aberrant critical period plasticity in the developmental trajectory to schizophrenia. Schizophr Bull. 2015;41(4):835–846.
46. Sarro EC, Sullivan RM, Barr G. Unpredictable neonatal stress enhances adult anxiety and alters amygdala gene expression related to serotonin and GABA. Neuroscience. 2014;258:147–161.
47. Essex MJ, Thomas Boyce W, Hertzman C, et al. Epigenetic vestiges of early developmental adversity: childhood stress exposure and DNA methylation in adolescence. Child Dev. 2013;84(1):58–75.
48. Lehmann J, Feldon J. Long-term biobehavioral effects of maternal separation in the rat: consistent or confusing? Rev Neurosci. 2000;11:383–408.
49. Lippmann M, Bress A, Nemeroff CB, Plotsky PM, Monteggia LM. Long‐term behavioural and molecular alterations associated with maternal separation in rats. Eur J Neurosci. 2007;25(10):3091–3098.
50. Macrì S, Chiarotti F, Würbel H. Maternal separation and maternal care act independently on the development of HPA responses in male rats. Behav Brain Res. 2008;191(2):227–234.
51. Maniam J, Morris MJ. Long-term postpartum anxiety and depression-like behavior in mother rats subjected to maternal separation are ameliorated by palatable high fat diet. Behav Brain Res. 2010;208(1):72–79.
52. Sapolsky RM, Romero LM, Munck AU. How do glucocorticoids influence stress responses? Integrating permissive, suppressive, stimulatory, and preparative actions. Endocr Rev. 2000;21(1):55–89.
53. Musselman DL, Betan E, Larsen H, Phillips LS. Relationship of depression to diabetes types 1 and 2: epidemiology, biology, and treatment. Biol Psychiatry. 2003;54(3):317–329.
54. McEwen BS. Brain on stress: how the social environment gets under the skin. Proc Natl Acad Sci. 2012;109(Supplement 2):17180–17185.
55. Meaney MJ, Szyf M. Maternal care as a model for experience-dependent chromatin plasticity? Trends Neurosci. 2005;28(9):456–463.
56. McGowan PO, Szyf M. The epigenetics of social adversity in early life: implications for mental health outcomes. Neurobiol Dis. 2010;39(1):66–72.
57. Perroud N, Paoloni-Giacobino A, Prada P, et al. Increased methylation of glucocorticoid receptor gene (NR3C1) in adults with a history of childhood maltreatment: a link with the severity and type of trauma. Transl Psychiatry. 2011;1(12):e59.
58. McGowan PO, Roth TL. Epigenetic pathways through which experiences become linked with biology. Dev Psychopathol. 2015;27(2):637–648.
59. Anda RF, Felitti VJ, Bremner JD, et al. The enduring effects of abuse and related adverse experiences in childhood. Eur Arch Psychiatry Clin Neurosci. 2006;256(3):174–186.
60. Maniam J, Antoniadis C, Morris MJ. Early-life stress, HPA axis adaptation, and mechanisms contributing to later health outcomes. Front Endocrinol (Lausanne). 2014;5:73.
61. Atherton K, Fuller E, Shepherd P, Strachan DP, Power C. Loss and representativeness in a biomedical survey at age 45 years: 1958 British birth cohort. J Epidemiol Community Health. 2008;62:216–223.
62. Delpierre C, Fantin R, Barboza-Solis C, Lepage B, Darnaudéry M, Kelly-Irving M. The early life nutritional environment and early life stress as potential pathways towards the metabolic syndrome in mid-life? A lifecourse analysis using the 1958 British Birth cohort. BMC Public Health. 2016;16(1):1–9.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.