")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
Levels of IL-6 are Associated with Lifetime Attempted Suicide in Alcohol Use Disorder Patients
Authors Bramness JG , Pandey S , Moe JS, Toft H , Lien L, Walby FA , Myhre MØ, Bolstad I
Received 4 April 2023
Accepted for publication 6 September 2023
Published 12 October 2023 Volume 2023:19 Pages 2141—2148
DOI https://doi.org/10.2147/NDT.S413101
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Jørgen G Bramness,1– 3 Susmita Pandey,1 Jenny Skumsnes Moe,1,3 Helge Toft,4 Lars Lien,1,4 Fredrik A Walby,5 Martin Øverlien Myhre,5 Ingeborg Bolstad1,4
1Norwegian National Advisory Unit on Concurrent Substance Abuse and Mental Health Disorders, Innlandet Hospital Trust, Brumunddal, Norway; 2Norwegian Institute of Public Health, Department of Alcohol, Tobacco and Drugs, Oslo, Norway; 3Institute of Clinical Medicine, UiT – The Arctic University of Norway, Tromsø, Norway; 4Faculty of Social and Health Sciences, Inland Norway University of Applied Sciences, Elverum, Norway; 5National Centre for Suicide Research and Prevention, Institute of Clinical Medicine, University of Oslo, Oslo, Norway
Correspondence: Jørgen G Bramness, Norwegian Institute of Public Health, P.O.Box 222, Oslo, 0213, Norway, Email [email protected]
Background: Patients with alcohol use disorder (AUD) have an increased risk of suicide. Neuroimmunological measures, such as cytokines, are shown to deviate in people with attempted suicide. Few studies have investigated this among AUD patients.
Patients and Methods: One-hundred and fourteen patients undergoing residential treatment for AUD were interviewed on lifetime suicide attempts (SA) along with several other background variables and clinical characteristics. Serum blood samples were drawn for analysis of cytokines.
Results: Thirty-one patients (27%) reported at least one SA. These patients had more symptoms of current affective disorders and more severe dependence. In bivariate analysis only IL-6 and IL-10 appeared to be associated with lifetime SA but without reaching statistical significance. In multivariate linear regression, adjusting for sex, nicotine use, somatic illness, and the use of anti-inflammatory drugs, IL-6 was associated to SA (p = 0.033).
Conclusion: The cytokine IL-6 has repeatedly been found to be associated with suicidality. The present study concurs with this role of IL-6 in a naturalistic observational study of AUD patients.
Keywords: alcohol use disorder, suicide attempted, cytokines, interleukins
Introduction
Alcohol use disorder (AUD) is a leading risk factor for suicide,1,2 only surpassed by schizophrenia and major depression (MD).3,4 As many as 30–40% of people with AUD report at least one lifetime suicide attempt (SA),5,6 which is among the strongest predictors of death by suicide.7 Moreover, people who re-attempt suicide are more likely to have AUD,8 and the increased risk of suicide after an SA may last for more than two decades.9 The causes of SA is complex and not fully understood, but neuroimmunological factors have been suggested to play a role in SA.10 Establishing biomarkers for SA in people with AUD could be of clinical relevance both for suicide prevention and for understanding the underlying pathophysiology.
High and prolonged alcohol use is known to activate the immune system and increase inflammatory responses, possibly through increased gut permeability and immune system activation via Toll-like receptors.11–15 Cytokine concentrations are augmented in people with AUDin particular, during drinking and withdrawal.12 This is true for tumour necrosis factor (TNF)-α, interferon (IFN)-γ, interleukin (IL)‐1β, IL‐6, and others.16 IL-1Ra, IL-8, monocyte chemoattractant protein (MCP)-1 and TNF-α seem to be mostly related to acute alcohol intake.12,13 IL-15 and IL-7 show the highest correlation with number of drinks, followed by IL-5, IL-6, IL, 8, IL-10 and TNF-α,12 and cytokines IL-1β and IL-10 show the highest relationship to craving.12 In people with AUD, IL-6, IL-8 and IL-10 have been investigated the most,12 and higher levels of IL-6 in particular have been demonstrated in patients with high alcohol consumption.
There is a close relationship between MD and levels of peripheral circulating cytokines.17 This relationship is probably bidirectional, and most findings are associations rather than causal studies. For instance, a meta-analysis revealed increased levels of cytokines like IL-6, TNF, IL-10, IL-1RA, and soluble TNF receptor in 79 patients with MD compared to healthy control, whereas the level of IFN-γ was reduced.18 MD is a major risk factor for suicide and SA,19,20 and neuroimmunological alterations are also related to suicidal behaviour, with alterations in circulating cytokines having been detected in people with previous SA.21 The most persistent findings are relations between suicidal behaviour and increased levels of IL-1β, IL-6, IL-8, TNF-α, IFN-γ, and others that have been detected at lower levels.12,21–24 The robustness of associations with IL-1β and IL-6 has led IL-1β and IL-6 to be proposed as clinical biomarkers for suicidal behaviour, however with caution against their clinical applicability, due to the practicalities of cytokine analysis and difficulties in establishing the predictive values of IL-6 on the individual level.25
Given the immune activation in both AUD patients and among those with depression and the high co-morbidity between the two, it is of special interest to investigate cytokine levels in AUD patients with or without SA. To date, there is little, if any, such research. In the current study, we aimed to investigate the relationship between the cytokines IFN-γ, IL-1β, IL-6, IL-8, IL-10, and TNF-α and lifetime SA in a sample of people in treatment for AUD.
Materials and Methods
Study Participants
Data were collected in three residential rehabilitation clinics in the Eastern region of Norway from January 2018 to August 2019. The material from a larger study has been described in a previous publication.26 The clinics offer long-term residential treatment stays (>30 days) for people with substance use disorders (SUD), where the majority have a diagnosis of AUD. Admission to the clinics was after detoxification, most patients being abstinent for 2 weeks or more. People were considered for inclusion in the study unless they were in an unsuitable condition to participate in the study, as assessed by the clinical staff, due to severe somatic illness, psychosis, cognitive impairment, or inability to speak a Scandinavian language. Of the 366 patients who were admitted to treatment in the clinics during our inclusion period, 224 (61%) were considered eligible for participation in this study. Only patients who had current AUD as diagnosed according to the International Classification of Diseases 10th Revision (ICD-10) were eligible participants. Of these, 114 (51%) signed informed written consent and were enrolled. At baseline data collection, the patients had been in treatment for a median of 7 days (1st, 3rd quartile: Interquartile range (IQR): 5–12 days) and reported abstinence from alcohol during the last 19 (IQR 12–30) days.
Measures
Baseline data collection consisted of an interview, clinical examination, and administration of psychometric questionnaires. Selected modules of the Mini International Neuropsychiatric Interview (M.I.N.I.) version 6.0 were conducted by trained staff, while all other information, including Beck Depression Inventory version 2 (BDI-II) and Severity of Dependence Scale (SDS), was collected using self-report forms. The interview and self-report forms were administered at the clinics where the participants were treated. For the current study, we included data on sex, age, and the use of nicotine products, including both smoking and smokeless tobacco, the latter being relatively common in Norway.27 Participants’ BMI was calculated by dividing weight in kg (measured on site) by the square of the height in meters (self-report). Participants were asked about any current somatic illness, which was categorized into absent or very mild (given value 0), moderate (given value 1; eg common cold) or severe (given value 2; eg skin infection). Participants were also asked about the use of anti-inflammatory drugs in the past week (including NSAIDs and glucocorticoids) resulting in a binary variable. Both latter measures are detailed in an earlier publication.28
Mental Health Measures
AUD diagnosis was verified utilizing M.I.N.I. Patients were asked if they had ever attempted suicide and their responses could be either yes or no. No formal instrument was used. The level of depressive symptoms was measured using the Beck Depression Inventory 2 (BDI-II).29,30 This self-report questionnaire consists of 21 questions asking the respondents how they have been feeling in the preceding two weeks, with responses given on a 4-point scale. Reponses are added up into a total score ranging from 0 to 63, where a higher score indicates a higher level of depressive symptoms. Other psychiatric comorbidities were examined using the M.I.N.I (current panic disorder and post-traumatic stress disorder (PTSD), coded as yes/no).
AUD-Related Measures
Severity of alcohol dependence was examined using the Severity of Dependence Scale (SDS). The SDS was originally constructed to measure dependency on illicit drugs,31 but has later been shown to be a reliable and valid measure of AUD as well.32 It consists of five items that target subjective aspects of dependence during the preceding year, such as “Did you think your alcohol use was out of control?” and “Did you wish you could stop drinking?”. The response alternatives range from 0) “Never” to 3) “Always” for each question. The responses are summed up into a total score ranging from 0 to 15, where a higher score indicates more severe dependence.
Cytokines Measured
Based on the available literature about inflammatory effects of chronic alcohol use and our sample, the following cytokines were included in the current study: IFN-γ, IL-1β, IL-6, IL-8, IL-10, and TNF-α.
Blood Collection and Serum Preparation
Venous blood samples were collected using 6 mL ethylenediaminetetraacetic acid (EDTA) Vacutainer blood collection tubes. The tubes were then turned upside down 10 times and centrifuged at 1500 g. The plasma was then transferred with a pipette into Eppendorf microtubes and stored for a short time on site at −20°C before storage at −80°C until use.
After thawing 25 μL human plasma was diluted (1:5) and then analyzed. Cytokines were measured on a MESO® QuickPlex SQ 120 Multiplex Imager using the custom U-PLEX Biomarker Group 1 Multiplex assay from MSD, Rockville, Maryland, USA. A 9-plex assay was used returning values (lower limit of detection (LLOD) in parenthesis) on IFN-γ (1.99 pg/mL), IL-1β (0.03 pg/mL), IL-1ra (0.89 pg/mL), IL-6 (0.10 pg/mL), IL-8 (0.07 pg/mL), IL-10 (0.04 pg/mL), IL-17 (0.70 pg/mL), MCP-1 (0.18 pg/mL) and TNF-α (0.23 pg/mL). Analyses were performed at Vitas Analytical Laboratory AS, Oslo, Norway.
Missing Data
For analyses of some variables (age, sex, smoking status, BMI, current somatic illness, current anti-inflammatory medication, lifetime suicide attempt and PTSD), there were no missing data. For some variables, the persons with missing data were excluded. These include nicotine status (missing N = 2), current BDI-II score (missing N = 29), panic disorder lifetime (missing N = 1), SDS (missing N = 27), and data on some immunological measures. For BDI-II, person-mean imputation was done if 17 or more of the 21 questions were answered (final N = 85). Blood samples were missing in 2 cases and were excluded. For data on most cytokines, no values were below LLOD, except for 1 sample for TNF-α and 34 samples for IL-1β that were excluded. Sample size of each variable included in the analysis are presented in Table 1.
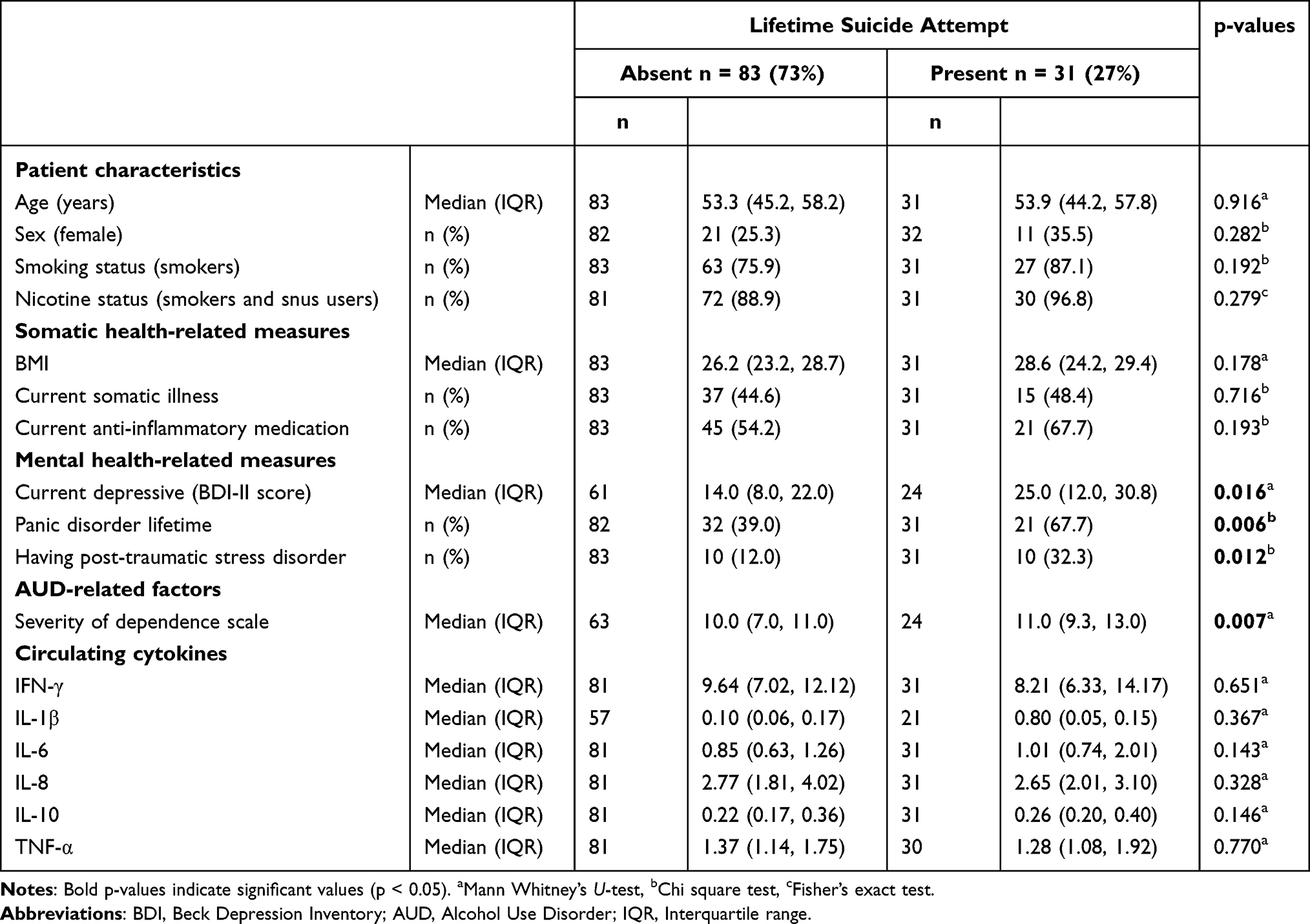 |
Table 1 Difference Between Alcohol Use Disorder Patients with and without Lifetime Suicide Attempts (n = 114) |
Statistical Analyses
Bivariate analyses were used to assess the relationship between AUD patients with and without lifetime suicide attempt. Chi-square tests or Fisher’s exact tests were used to compare categorical variables, while Mann–Whitney U-tests were used to compare continuous variables because the data were non-normally distributed. Cytokines showing the greatest difference between those with or without a lifetime suicide attempt were investigated further (p-values below 0.15 in the Mann–Whitney U-test). Linear regression was used to identify the relationship of these cytokines and the background variables. Logistic regression was used to assess the association between the cytokines of interest and lifetime suicide attempt. These associations were adjusted for background variables identified as relevant in bivariate analysis, but excluding those theoretically too related to the outcome (like anxiety and depression). Exact p-values were given, but p-values below 0.050 were considered significant. SPSS version 23.0 for Windows was used to perform the statistical analyses.
Results
Of the 114 AUD patients, 31 (27%) reported having attempted suicide during their lifetime. Table 1 shows that these patients reported a higher current BDI-II score (p = 0.016), more often reported lifetime panic disorder (p = 0.006), more often reported PTSD (p = 0.012) and had a slightly higher SDS score (p = 0.007). The patients who had attempted suicide did not have a higher score on current somatic illness. For the cytokines, there were no significant differences in circulating levels between the patients who had SA and others, but IL-6 and IL-10 showed the greatest group difference (both p-values <0.150). When dividing the material according to differences in severity of dependence, the difference of IL-6 between those with or without a lifetime suicide attempt was most pronounced among those with the higher dependence (p = 0.022, Supplementary Table S1).
Table 2 shows the bilateral relationships between the background variables that were determined important (based on Table 1 and a theoretical evaluation) and their relationship to IL-6 and IL-10. Levels of IL-6 correlated positively with BMI (p = 0.003) and higher levels of IL-6 were found among those with a current somatic illness (p = 0.004). For the level of IL-10, a similar positive correlation was found with BMI (p = 0.005) and nicotine users (smoking and/or snus) had lower levels of IL-10 (p = 0.001).
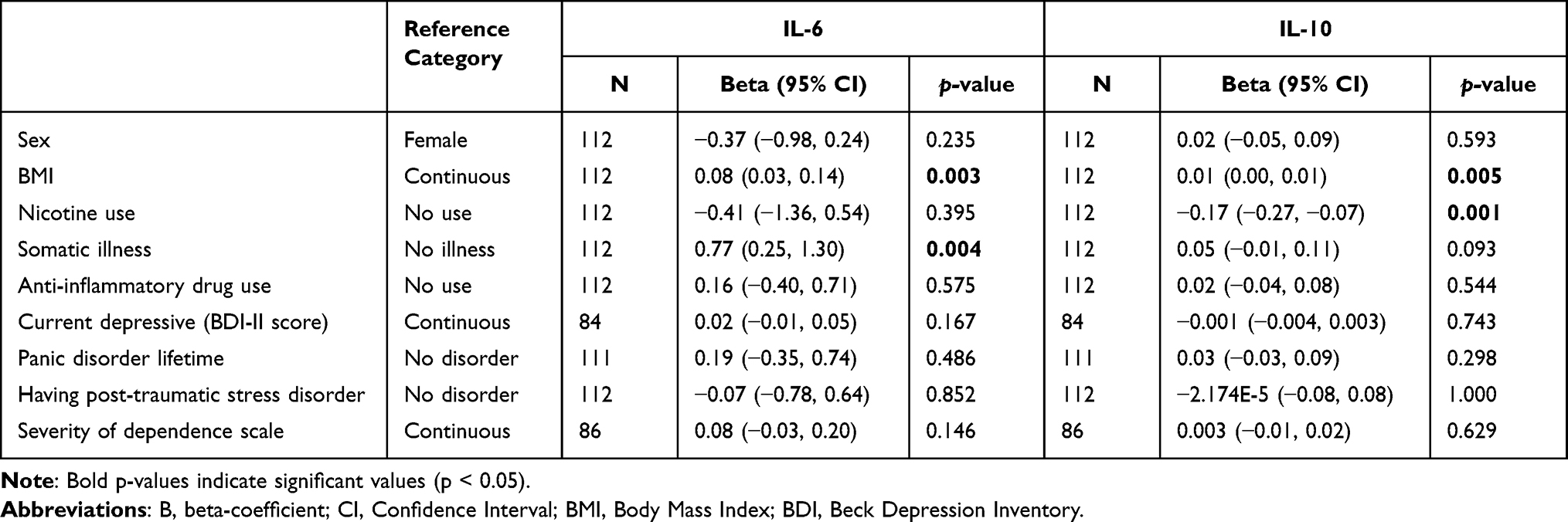 |
Table 2 The Bilateral Relationship Between IL-6 and IL-10 and Different Background Variables That are Related to Suicide Attempts in Patients Treated for AUD. Values are from a Linear Regression and Given as Beta-Value with 95% Confidence Interval (CI). (N = 112) |
Table 3 shows unadjusted and adjusted relationships between reporting a lifetime suicide attempt and the two investigated cytokines. Neither IL-6 nor IL-10 were significantly associated with SA, but after adjusting for the factors determined important from the bivariate analysis IL-6 showed a significant relationship with SA. Adjusting for sex seems to be the most important step, revealing a significant relationship between SA and circulating levels of IL-6, with higher levels of IL-6 in the SA patients. There was a complex relationship between the different co-variates tipping the different regression models in and out of statistical significance, even if they did not change the effect estimate dramatically. Model D, adjusting for sex, nicotine use, somatic illness, and the use of anti-inflammatory drugs showed the greatest difference between patients with and without lifetime SA. None of the models were significant for IL-10, even with the same pattern of adjustments. Supplementary Table S2 shows all the different models.
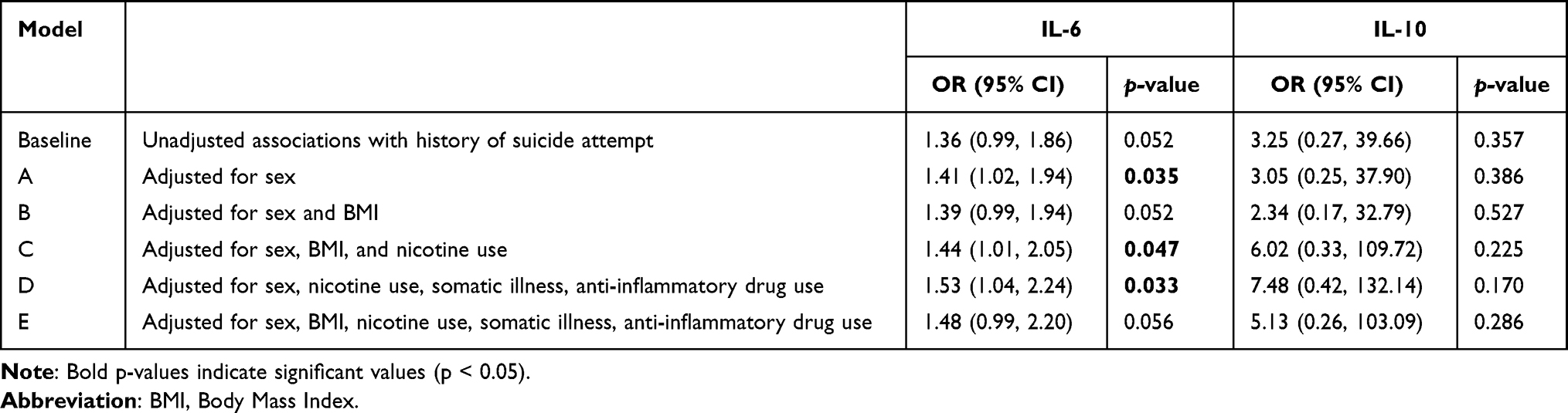 |
Table 3 Logistic Regression Models for Suicide Attempt Among Patients with AUD. Values are from a Linear Regression and Given as Beta-Value with 95% Confidence Interval (CI). (n = 112) |
Discussion
In this study of AUD patients in treatment, we found that cytokine IL-6 was elevated in patients who reported lifetime suicide attempt. This was statistically significant when adjusting for sex, nicotine use, somatic illness, and the use of anti-inflammatory drugs.
IL-6 has been found in many studies to be associated with both MD33 and attempted suicide.34 The close relationship between MD and attempted suicide makes it a challenge to separate the two, but higher IL-6 levels have been measured in the cerebrospinal fluid of patients that have attempted suicide,35 more so in violent,36 and impulsive37 suicide attempts. In blood samples of patients with SA, increased levels of IL-6 have been identified, both compared to patients without SA and to healthy controls,25 making IL-6 levels a well-established marker of suicide behaviour.24 None of these findings, however, can isolate the IL-6 finding to suicidal behaviour, rather than MD. Furthermore, elevated IL-6 is also found among patients with AUD.12 If increased levels of IL-6 are involved in both MD and AUD, it could lead to difficulties in identifying differences in IL-6 levels between non-depressed and depressed AUD patients.38 Indeed, earlier findings by our group indicate that the higher the severity of the AUD, the less difference there is in cytokine levels related to MD.38 Thus, finding a difference in IL-6 levels between people who attempted suicide and others in the present study indicates that IL-6 is a marker of value.
The difference in IL-6 levels was only found to be significant after adjusting for some of the covariates. Sex is known to influence the level of IL-6, as women show higher IL-6 reactivity to an acute mental stressor.39,40 Nicotine use is usually related to elevated levels of IL-6,41 but not in AUD patients. Another study by our group suggests that the increased levels of IL-6 in AUD patients can be downregulated by the use of nicotine products.28 This might explain the negative relationship between IL-6 and nicotine use in the current study. The influence on IL-6 levels of somatic illness and the use of anti-inflammatory drugs is more self-evident, as somatic illness will trigger immune reactions and the indications for anti-inflammatory drugs are such illnesses. We chose not to include depressive score in the current analysis, because of its close relationship to SA, not wanting to “over adjust” in the multivariate analyses.
We found no differences in cytokine levels between the patients who had attempted suicide and the others for the cytokines IFN-γ, IL-1β, IL-8, IL-10 and TNF-α, despite that these have been shown to be related to suicide attempts in several studies,10,12,21,22 however less consistently than for IL-6.42–45 Again, the lack of findings could be partially explained by the general elevation of cytokines in AUD patients, possibly masking factors that would otherwise be visible.38 It could also reflect the high comorbidity suffered by AUD patients in treatment, and further differing effect sizes associated with different cytokines. The unclear shared and unique pathophysiology between AUD, MD and somatic illness will necessarily hamper interpretations of results.
This study was performed in a relatively small group of AUD patients, with some selection. It is, however, difficult to predict the impact of a possible selection bias. The limited sample size may have left the study underpowered to find important differences in the risk factors for suicide attempt and limited the number of variables introduced to the multivariate analysis. We could, eg, have included more measures on alcohol use, but the sample size did not allow for too many variables to be included. Furthermore, the outcome measure “suicide attempt” was measured as a dichotomous self-report variable and did not differentiate between time elapsed since the last attempt, the method (violent or not/impulsive or not), or the number of attempts. Also, being a naturalistic study, which included patients with a variety of characteristics and multi-morbidities, results will need to be confirmed before clear-cut conclusions can be drawn.
The robustness of findings of IL-6 being elevated among people who have attempted suicide has made some authors speculate that it could be a biomarker of suicidality, potentially of clinical use.37 Despite caution being warranted regarding the predictive value on an individual level, the repeated findings of elevated IL-6 levels across many clinical samples of suicide attempters give valuable information on the biological correlates of suicide, which could contribute to understand the pathophysiology. The current cross-sectional study concurs with the findings of IL-6 being associated with suicidal behaviour, with differences being detectable even in a sample of people with AUD, which is found to be associated with IL-6. Despite its limitations, the current study contributes to the validity of IL-6 as a marker of suicidality across different groups of patients.
Ethical Statement
The study was approved by the Norwegian Regional Ethics Committee and in accordance with the Helsinki Declaration (ID no: 21505/2017/1314). Participants were informed of the possibility of talking to staff on site if they had any questions, eg, regarding suicide, or were experiencing anything as troubling.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
The study was partially funded by a research grant from the Norwegian Research Council (reference: 251140) and by internal funding from different institutions. The publication charges for this article have been funded by a grant from the publication fund of UiT The Arctic University of Norway.
Disclosure
None of the authors have any conflicts of interest to report for this work.
References
1. Edwards AC, Ohlsson H, Sundquist J, Sundquist K, Kendler KS. Alcohol use disorder and risk of suicide in a Swedish population-based cohort. Am J Psych. 2020;177(7):627–634. doi:10.1176/appi.ajp.2019.19070673
2. Kõlves K, Draper BM, Snowdon J, De Leo D. Alcohol-use disorders and suicide: results from a psychological autopsy study in Australia. Alcohol. 2017;64:29–35. doi:10.1016/j.alcohol.2017.05.005
3. Ferrari AJ, Norman RE, Freedman G, et al. The burden attributable to mental and substance use disorders as risk factors for suicide: findings from the global burden of disease study 2010. PLoS One. 2014;9(4):e91936. doi:10.1371/journal.pone.0091936
4. Rizk MM, Herzog S, Dugad S, Stanley B. Suicide risk and addiction: the impact of alcohol and opioid use disorders. Curr Addict Rep. 2021;2021:1–14.
5. Wojnar M, Ilgen MA, Czyz E, et al. Impulsive and non-impulsive suicide attempts in patients treated for alcohol dependence. J Affect Disord. 2009;115(1–2):131–139. doi:10.1016/j.jad.2008.09.001
6. Sher L. Risk and protective factors for suicide in patients with alcoholism. TheScientificWorldJOURNAL. 2006;6:1405–1411. doi:10.1100/tsw.2006.254
7. Bostwick JM, Pabbati C, Geske JR, McKean AJ. Suicide attempt as a risk factor for completed suicide: even more lethal than we knew. Am J Psych. 2016;173(11):1094–1100. doi:10.1176/appi.ajp.2016.15070854
8. Parra-Uribe I, Blasco-Fontecilla H, Garcia-Parés G, et al. Risk of re-attempts and suicide death after a suicide attempt: a survival analysis. BMC Psychiat. 2017;17(1):163. doi:10.1186/s12888-017-1317-z
9. Probert-Lindström S, Berge J, Westrin Å, Öjehagen A, Skogman Pavulans K. Long-term risk factors for suicide in suicide attempters examined at a medical emergency in patient unit: results from a 32-year follow-up study. BMJ Open. 2020;10(10):e038794. doi:10.1136/bmjopen-2020-038794
10. Mann JJ, Rizk MM. A Brain-Centric Model of Suicidal Behavior. Am J Psychiatry. 2020;177(10):902–916. doi:10.1176/appi.ajp.2020.20081224
11. Barr T, Helms C, Grant K, Messaoudi I. Opposing effects of alcohol on the immune system. Prog Neuropsychopharmacol Biol Psychiatry. 2016;65:242–251. doi:10.1016/j.pnpbp.2015.09.001
12. Adams C, Conigrave JH, Lewohl J, Haber P, Morley KC. Alcohol use disorder and circulating cytokines: a systematic review and meta-analysis. Brain Behav Immun. 2020;89:501–512. doi:10.1016/j.bbi.2020.08.002
13. Neupane SP, Skulberg A, Skulberg KR, Aass HC, Bramness JG. Cytokine changes following acute ethanol intoxication in healthy men: a crossover study. Mediators Inflamm. 2016;2016:3758590. doi:10.1155/2016/3758590
14. Crews FT, Nixon K. Mechanisms of neurodegeneration and regeneration in alcoholism. Alcoh Alcoh. 2009;44(2):115–127. doi:10.1093/alcalc/agn079
15. Calleja-Conde J, Echeverry-Alzate V, Bühler KM, et al. The immune system through the lens of alcohol intake and gut microbiota. Int J Mol Sci. 2021;22(14):7485. doi:10.3390/ijms22147485
16. Huang W, Zhou H, Hodgkinson C, Montero A, Goldman D, Chang SL. Network meta-analysis on the mechanisms underlying alcohol augmentation of COVID-19 pathologies. Alcohol Clin Exp Res. 2021;45(4):675–688. doi:10.1111/acer.14573
17. Beurel E, Toups M, Nemeroff CB. The bidirectional relationship of depression and inflammation: double trouble. Neuron. 2020;107(2):234–256. doi:10.1016/j.neuron.2020.06.002
18. Köhler CA, Freitas TH, Maes M, et al. Peripheral cytokine and chemokine alterations in depression: a meta-analysis of 82 studies. Acta Psychiatr Scand. 2017;135(5):373–387. doi:10.1111/acps.12698
19. Malone KM, Haas GL, Sweeney JA, Mann JJ. Major depression and the risk of attempted suicide. J Affect Disord. 1995;34(3):173–185. doi:10.1016/0165-0327(95)00015-F
20. Bostwick JM, Pankratz VS. Affective disorders and suicide risk: a reexamination. Am J Psychiatry. 2000;157(12):1925–1932. doi:10.1176/appi.ajp.157.12.1925
21. Neupane SP. Psychoneuroimmunology: the new frontier in suicide research. Brain Behav Immun Health. 2021;17:100344. doi:10.1016/j.bbih.2021.100344
22. Serafini G, Parisi VM, Aguglia A, et al. A specific inflammatory profile underlying suicide risk? Systematic review of the main literature findings. Int J Environ Res Public Health. 2020;17(7):2393. doi:10.3390/ijerph17072393
23. Rengasamy M, Zhong Y, Marsland A, et al. Signaling networks in inflammatory pathways and risk for suicidal behavior. Brain Behav Immun Health. 2020;7. doi:10.1016/j.bbih.2020.100122
24. Ganança L, Oquendo MA, Tyrka AR, Cisneros-Trujillo S, Mann JJ, Sublette ME. The role of cytokines in the pathophysiology of suicidal behavior. Psychoneuroendocrinology. 2016;63:296–310. doi:10.1016/j.psyneuen.2015.10.008
25. Black C, Miller BJ. Meta-analysis of cytokines and chemokines in suicidality: distinguishing suicidal versus nonsuicidal patients. Biol Psychiatry. 2015;78(1):28–37. doi:10.1016/j.biopsych.2014.10.014
26. Bolstad I, Lien L, Bramness JG. ADHD symptoms as risk factor for PTSD in inpatients treated for alcohol use disorder. Psychiatry Res. 2021;300:113904. doi:10.1016/j.psychres.2021.113904
27. Zhou H, Polimanti R, Yang B-Z, et al. Genetic risk variants associated with comorbid alcohol dependence and major depression. JAMA Psychiat. 2017;74(12):1234–1241. doi:10.1001/jamapsychiatry.2017.3275
28. Bolstad I, Lien L, Moe JS, Pandey S, Toft H, Bramness JG. Inflammatory cytokines in alcohol use disorder patients are lower in smokers and users of smokeless tobacco. Alcohol. 2023;47(7):1352–1363. doi:10.1111/acer.15103
29. Beck AT, Ward CH, Mendelson M, Mock J, Erbaugh J. An inventory for measuring depression. Arch Gen Psychiatry. 1961;4:561–571. doi:10.1001/archpsyc.1961.01710120031004
30. McPherson A, Martin CR. A narrative review of the Beck Depression Inventory (BDI) and implications for its use in an alcohol-dependent population. J Psychiatr Ment Health Nurs. 2010;17(1):19–30. doi:10.1111/j.1365-2850.2009.01469.x
31. Gossop M, Best D, Marsden J, Strang J. Test-retest reliability of the Severity of Dependence Scale. Addiction. 1997;92(3):353. doi:10.1111/j.1360-0443.1997.tb03205.x
32. Gossop M, Marsden J, Stewart D. Dual dependence: assessment of dependence upon alcohol and illicit drugs, and the relationship of alcohol dependence among drug misusers to patterns of drinking, illicit drug use and health problems. Addiction. 2002;97(2):169–178. doi:10.1046/j.1360-0443.2002.00028.x
33. Howren MB, Lamkin DM, Suls J. Associations of depression with C-reactive protein, IL-1, and IL-6: a meta-analysis. Psychosom Med. 2009;71(2):171–186. doi:10.1097/PSY.0b013e3181907c1b
34. Fernández-Sevillano J, González-Ortega I, MacDowell K, et al. Inflammation biomarkers in suicide attempts and their relation to abuse, global functioning and cognition. World J Biol Psychiatry. 2021;2021:1–11.
35. Enache D, Pariante CM, Mondelli V. Markers of central inflammation in major depressive disorder: a systematic review and meta-analysis of studies examining cerebrospinal fluid, positron emission tomography and post-mortem brain tissue. Brain Behav Immun. 2019;81:24–40. doi:10.1016/j.bbi.2019.06.015
36. Lindqvist D, Janelidze S, Hagell P, et al. Interleukin-6 is elevated in the cerebrospinal fluid of suicide attempters and related to symptom severity. Biol Psychiatry. 2009;66(3):287–292. doi:10.1016/j.biopsych.2009.01.030
37. Isung J, Aeinehband S, Mobarrez F, et al. High interleukin-6 and impulsivity: determining the role of endophenotypes in attempted suicide. Transl Psychiatry. 2014;4(10):e470. doi:10.1038/tp.2014.113
38. Neupane SP, Lien L, Martinez P, et al. High frequency and intensity of drinking may attenuate increased inflammatory cytokine levels of major depression in alcohol-use disorders. CNS Neurosci Ther. 2014;20(10):898–904. doi:10.1111/cns.12303
39. Edwards KM, Burns VE, Ring C, Carroll D. Sex differences in the interleukin-6 response to acute psychological stress. Biol Psychol. 2006;71(3):236–239. doi:10.1016/j.biopsycho.2005.06.006
40. Endrighi R, Hamer M, Steptoe A. Post-menopausal women exhibit greater interleukin-6 responses to mental stress than older men. Ann Behav Med. 2016;50(4):564–571. doi:10.1007/s12160-016-9783-y
41. Ung TT, Nguyen TT, Lian S, et al. Nicotine stimulates IL-6 expression by activating the AP-1 and STAT-3 pathways in human endothelial EA.hy926 cells. J Cell Biochem. 2019;120(4):5531–5541. doi:10.1002/jcb.27837
42. Huang TL, Lee CT. T-helper 1/T-helper 2 cytokine imbalance and clinical phenotypes of acute-phase major depression. Psychiatry Clin Neurosci. 2007;61(4):415–420. doi:10.1111/j.1440-1819.2007.01686.x
43. Keaton SA, Madaj ZB, Heilman P, et al. An inflammatory profile linked to increased suicide risk. J Affect Disord. 2019;247:57–65. doi:10.1016/j.jad.2018.12.100
44. Wiener CD, Moreira FP, Portela LV, et al. Interleukin-6 and Interleukin-10 in mood disorders: a population-based study. Psychiatry Res. 2019;273:685–689. doi:10.1016/j.psychres.2019.01.100
45. Isung J, Mobarrez F, Nordström P, Asberg M, Jokinen J. Low plasma vascular endothelial growth factor (VEGF) associated with completed suicide. World J Biol Psychiatry. 2012;13(6):468–473. doi:10.3109/15622975.2011.624549
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.