")
Back to Journals » Risk Management and Healthcare Policy » Volume 17
Level of Knowledge on Sexual and Reproductive Health Rights Among the Teenage Mothers and Their Parents in Rwanda: A Comparative Cross-Sectional Study
Authors Lutasingwa D, Favina A , Ochora M , Rukanikigitero JMV, Gutabarwa LT , Kagaba A, Kaggwa MM
Received 26 August 2023
Accepted for publication 11 January 2024
Published 16 January 2024 Volume 2024:17 Pages 159—169
DOI https://doi.org/10.2147/RMHP.S437217
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Haiyan Qu
Dan Lutasingwa,1 Alain Favina,2 Moses Ochora,3 Jean Marie Vianney Rukanikigitero,1 Louange Twahirwa Gutabarwa,1 Aflodis Kagaba,1 Mark Mohan Kaggwa4,5
1Department of Research, Health Development Initiative, Kicukiro District, Kigali City, Rwanda; 2Department of Psychiatry, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 3Department of Pediatric, Faculty of Medicine, Mbarara University of Science and Technology, Mbarara, Uganda; 4Department of Psychiatry and Behavioural Neurosciences, McMaster University, Hamilton, ON, Canada; 5Forensic Psychiatry Program, St. Joseph Healthcare, Hamilton, ON, Canada
Correspondence: Dan Lutasingwa, Email [email protected]
Background: Parents are the primary caregivers and influential figures in adolescents’ lives. They play a crucial role in shaping their children’s attitudes, beliefs, and behaviors regarding sexual reproductive health. A vast difference in knowledge between adolescents and their parents indicates failure in knowledge translation and is associated with sexual and reproductive consequences, such as teenage pregnancies.
Methods: In this cross-sectional study between December 2020 and December 2021, 834 teenage mothers and their parents/guardians (n = 861) were enrolled from all five provinces of Rwanda. Knowledge of sexual reproductive health (SRH) rights was assessed, and the differences between the understanding of parents and their children were analyzed using Chi-square tests.
Results: There were statistically significant differences for all the assessed aspects of SRH knowledge rights between parents and their teenagers (ie, on the age of consent, safe abortion, right to education for teenage mothers, understanding of financial responsibilities, and perceptions of legal consequences).
Conclusion: There is a significant knowledge difference between the two generations regarding their understanding of SRH rights. It is recommended that future programming should devise innovative ways that bring together parents and their children to discuss sexual reproductive health rights, which will result in empowered children and teenagers in Rwanda. Also, awareness programs are needed to improve the knowledge gaps regarding SRH in the public by policymakers, NGOs, and educators.
Keywords: teenage pregnancies, parents, Rwanda, sexual reproductive health, knowledge, adolescent mothers
Introduction
Adolescence is a phase between childhood and adulthood characterized by rapid physical, cognitive, and psychosocial growth.1 This growth is influenced by constant structured and unstructured learning, even in the realm of sexual and reproductive health and rights. The consequence of poor knowledge sets a precedent for poor health outcomes, like acquiring HIV, unplanned pregnancies, and many others, which have a downward bearing on the general quality of life of an individual.2 The government of Rwanda has made significant strides in promoting sexual and reproductive health (SRH) and rights, like implementing the Rwanda Family Planning/Adolescent Sexual Reproductive Health Strategic Plan and National Family Planning Costed Implementation Plan, which emphasize comprehensive sexuality education and accessible SRH services.3 Despite these implementations, various challenges have persisted, such as uninformed advice from family members and the unpopularity of female condoms, among others.4 These numerous persistent challenges hinder policy translation into practice. One of the bottlenecks is the intergenerational knowledge transfer.5,6 Parents are the primary caregivers and influential figures in adolescents’ lives. They play a crucial role in shaping their children’s attitudes, beliefs, and behaviors regarding SRH.7,8 However, research indicates that parents often are ill-equipped to address SRH topics with their teenage children due to cultural norms, discomfort, lack of knowledge, or misconceptions surrounding SRHR.6,9,10 These create a knowledge gap between parents and their children since children are left to explore SRH with minimum parental guidance.9,10
Despite previous studies reporting the discrepancy in the intergenerational knowledge about SRHR, this has not yet been explored in Rwanda, where mothers are considered the epitome of knowledge. Therefore, this cross-sectional study compares the knowledge levels, attitudes, and beliefs regarding SRHR in Rwanda. The findings of this study are expected to inform the development of evidence-based interventions and programs that can enhance SRHR knowledge, communication, and decision-making within families.
Methods
Study Design and Setting
A cross-sectional study based on convenience sampling approach was conducted between December 2020 and December 2021 in the five provinces of Rwanda, among 25 study sites. A sample size of 834 teenage mothers was included in the study, representing an average of 22 teenagers per district. At least one of the parents/guardians was also included, totaling 861. Six rural study sites in Southern Rwanda (ie, Huye, Nyamagabe, Kamonyi, Muhanga, Ruhango, and Nyanza); Six rural Study sites in Eastern Rwanda (ie, Gatsibo, Kayonza, Kirehe, Ngoma, Nyagatare, and Rwamagana); six study sites in Western Rwanda (ie, Karongi, Nyamasheke, Ngorero, Nyabihu, Rubaru, and Rutsiro); four rural study sites in Northern Rwanda (ie, Gakenke, Burera, Musanze, and Rulindo); and three urban study sites in Kigali City (ie, Gasabo, Nyarugenge, and Kicukiro). Health Development Initiative (HDI) – Rwanda recruited participants by contacting district hospitals and contacting the target populations (parents and teenagers). Those contacted were encouraged to reach out to others who met the same inclusion criteria. The study was disrupted by the Covid-19 pandemic in Rwanda, with related control measures, including movement, meeting restrictions, and lockdowns.
Inclusion and Exclusion Criteria
People identified as teen mothers who had given birth to a child at or before 19 years within the past two years were included. The teen mothers were then requested to bring along their parents. We excluded Teen mothers who did not consent to participate in the study and those with speech or auditory disabilities since most were not trained in sign language.
Study Variables and Data Collection
HDI Rwanda managed the data collection process. A pre-designed questionnaire was administered to teenage mothers by four trained research assistants. Different study variables were collected, including:
Sociodemographic Characteristics
All the sociodemographic characteristics were collected as categorical variables except for age that was continuous. Based on this self-reporting questionnaire, the following sociodemographic variables were collected:
For teenage mothers, age, medical insurance (ie, presence vs absence), the profession of the progenitor (ie, unemployed, employed, or student), rank number among other siblings (ie, first, second, third, fourth, fifth, sixth, or seventh and above position), level of education (ie, none, primary, secondary, or tertiary), age at the first pregnancy, whether the pregnancy was planned (ie, yes vs no), number of pregnancies, approximate age of the father, the identity of the father of the child (ie, church member, stranger, friend, coworker, family member, neighbor, local leader, or boss at work) and family allow the teenage to stay home (ie, yes vs no).
For the parents, the following sociodemographic characteristics were collected age, sex (male vs female), marital status, place of residence, employment status, relationship with parent, how many daughters were pregnant in the same household, and the level of education.
Note: Based on the educational system in Rwanda, the level of education was classified in four levels: (i) none (no formal education), (ii) primary (first six years of education), (iii) secondary (subsequent six years of education), and (iv) tertiary (university training or vocational trainings).
Knowledge Regarding Sexual and Reproductive Health Rights
Knowledge of sexual reproductive health rights assessment was generated following provisions in the constitution as revised in 2015, Law N° 68/2018 of 30/08/2018 Determining Offences, and Penalties in General,11 Ministerial order n°002/moh/2019 of 08/04/2019 determining conditions to be satisfied for a medical doctor to perform an abortion,12 Law No. 59/2008 of 2008 on Prevention and Punishment of Gender-Based Violence13 and Law N°71/2018 of 31/08/2018 relating to the Protection of the Child were assessed.14 Two scenarios with sets of statements were formulated. They were meant to be answered by both teenagers and parents by responding yes/no, then comparing the answers to see if there was a difference in how they understood the laws. The statements in the first scenario examining child rights were as follows; It is legal for a man who is 20 years old to have sex with a 15-year-old girl. If it is legal for a girl under 18 who has been defiled to access safe abortion, a teenage mother must register her child, and an adolescent mother is not allowed to return to school after her child is born. Scenario 2 compared teenagers’ and parents’ knowledge of the law regarding an adult man impregnating an underage teenager. The scenario sheds light on the understanding of repercussions and responsibilities in such situations, and it opens meaningful discussions about legal and moral obligations; the statements were as follows: this man should give money to the teenage mother to help her raise the child, this man should help to increase the child, this man should go to jail, this man should not be held responsible for the pregnancy.
Ethical Considerations
The research team sought ethical approval from the Rwanda National Ethics Committee, under reference No947/RNEC/2020, on November 19, 2020. Informed consent or assent from all the participants or their legal guardians in case of participants below age 16 and/or were illiterate.
Statistical Analysis
The data was exported into STATA-16 for formal analysis. Descriptive statistics were presented using frequencies and proportions for categorical variables and mean and standard deviation for continuous variables. The knowledge for SRH between teenage mothers and their parents was compared based on chi-square and Student’s t-test. All statistics were calculated at a 95% level of confidence and 5% statistical error.
Results
Sociodemographic Characteristics of Teenage Mothers
The average age of teenagers that participated in the study was 18.93 years, the majority (83.33%) were from rural settings, and many 463 (55.2%) had at least attended primary school. Among them, 594 were employed (71.22%), while most 780 (93.53%) had given birth only once. The average age at first pregnancy was 16.85 years (Table 1).
 |
Table 1 Sociodemographic Characteristics of Teenage Mothers |
Sociodemographic Characteristics of Teenage Mother’s Parents
The average age of parents participating was 46.74±9.61 years and were predominantly female 738 (85.71%). The married were 515 (59.81%), and 79.91% were from rural settings. Most parents had attained primary level of education 437 (50.75%), and 645 (74.91%) were farmers. In total 741 (86.06%) reported that only one of their daughters had gotten pregnant as a teenager (Table 2).
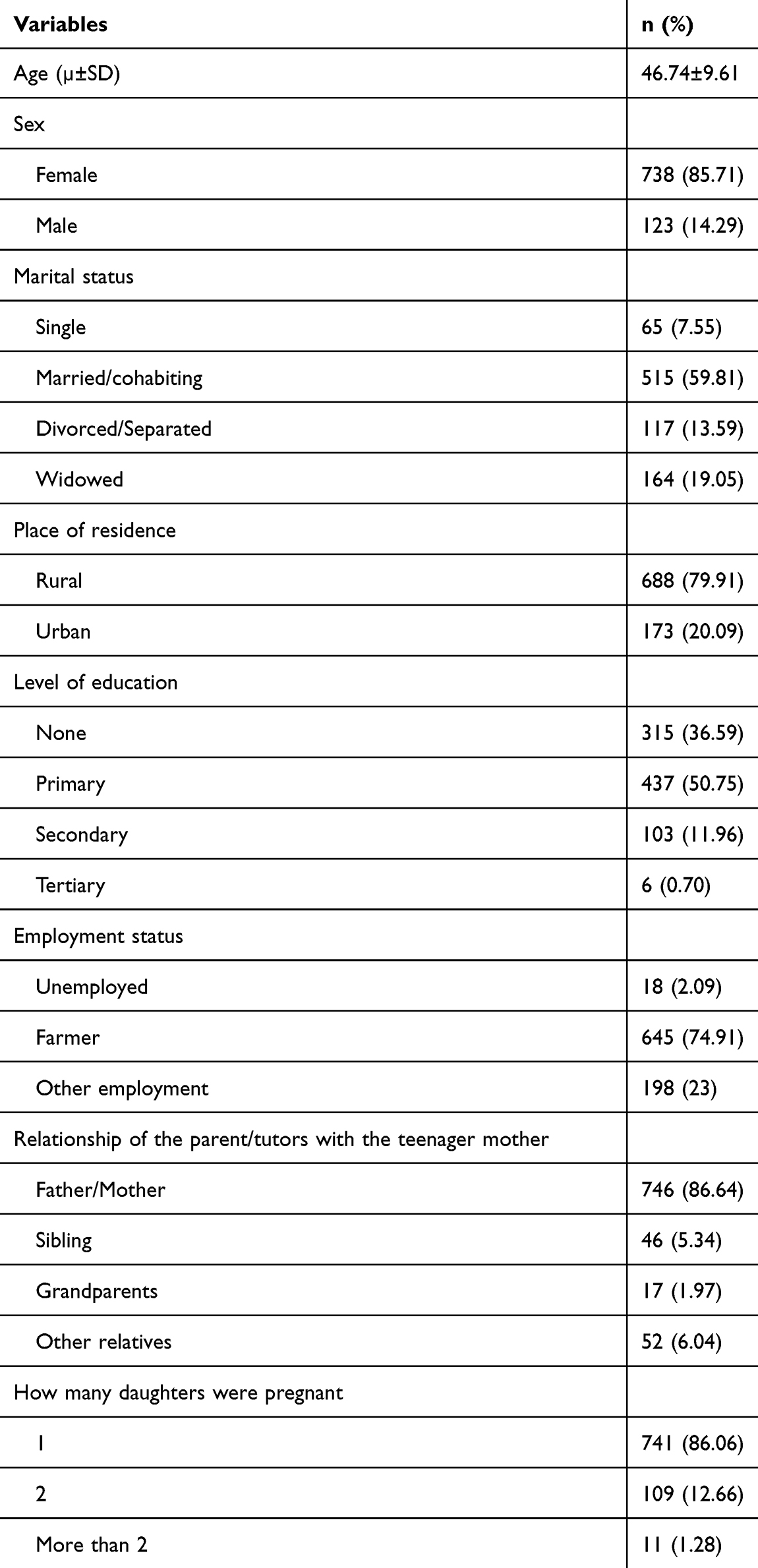 |
Table 2 Demographic Factors for Parents |
Knowledge About Sexual and Reproductive Health
There were significant differences between the knowledge of parents and their teenage daughters in all aspects assessed in the current study (Table 3).
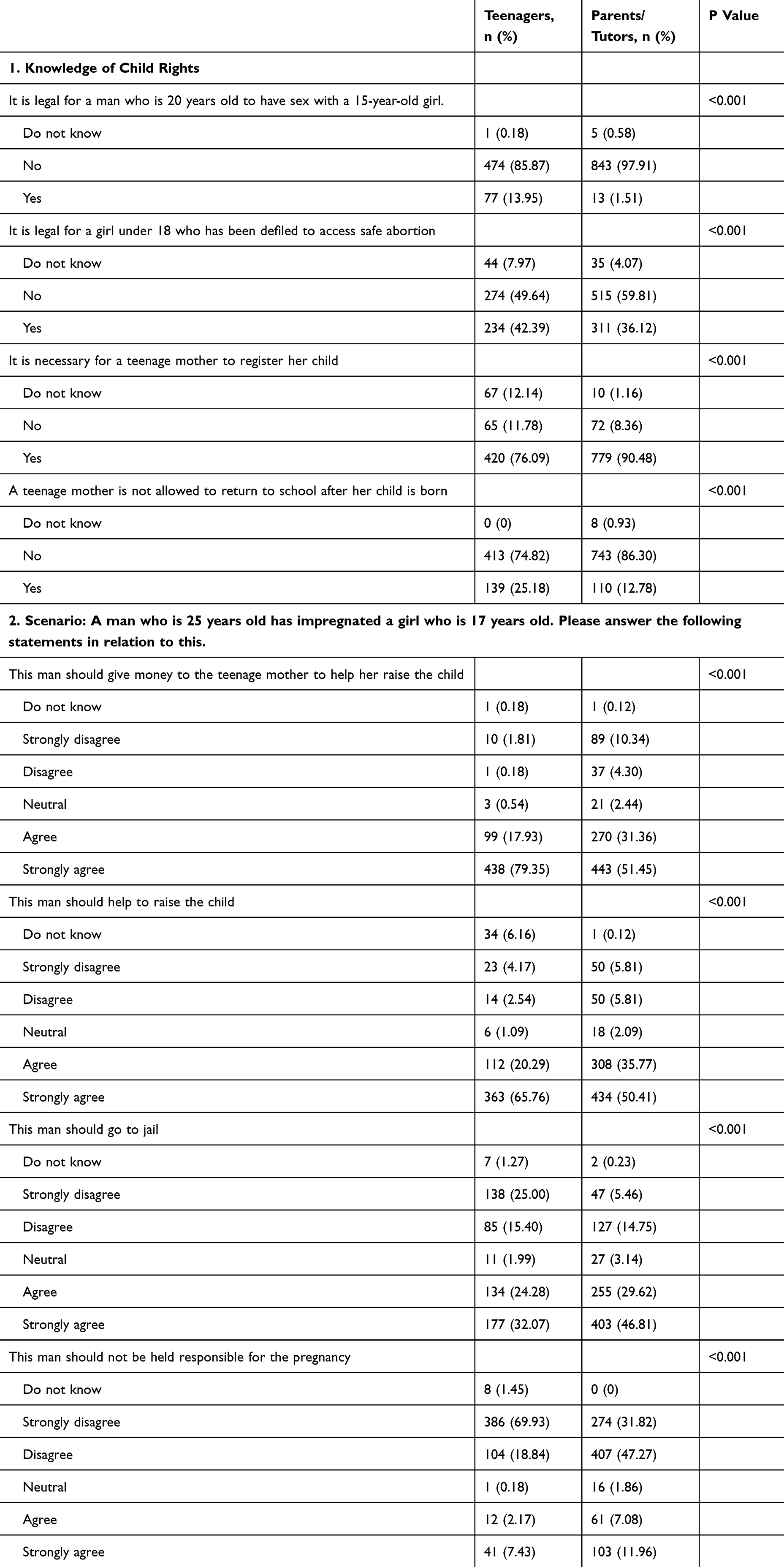 |
Table 3 Comparison of the Knowledge of Child Rights and Different Scenarios Between Teenage Mothers and Parents |
Comparing knowledge of child rights law of Rwanda between teenagers and parents/guardians by asking different scenarios revealed that when both were asked whether it was legal for a man who is 20 years old to have sex with a 15-year-old girl, more (13.95%) teenagers affirmed. In contrast, only 1.51% of the parents had the same view. When asked whether access to safe abortion for a teenager who had been defiled was legal, fewer teenage mothers compared to their parents responded that it was illegal (49.64% vs 59.81%). Furthermore, when participants were asked about the right to education after a teenage mother gives birth, more teenage mothers thought it was not allowed compared to their parents (25.18% vs 12.78%).
Scenario 2 compares knowledge of the law regarding an adult man siring a child with a minor, explicitly examining understanding of repercussions and responsibilities. The responses were as follows. When asked if the man should give money to the teenager to help raise the child, only 1.81% of teenage mothers strongly disagreed, compared to 10.34% of parents. When asked whether the man should help raise the child, over half of the parents and their daughters agreed, but more teenage mothers agreed to this than their parents (65.76% vs 50.41%). The responses regarding jail for the man mentioned above also differed in the two groups. Approximately 25% of teenagers strongly disagreed that the man should not go to jail compared with 5.46% of parents.
Discussion
This study used everyday scenarios to compare knowledge about SRH between teenage mothers and their parents. There exists a knowledge difference between parents and their daughters regarding SRH. This finding was in accordance with other previous studies conducted to evaluate the knowledge about SRH among parents and adolescents. A study conducted in Nepal in 2023 revealed that only one-third of parents had the correct knowledge about SRH15 and according to a study conducted in 2020 in eight sites across sub-Saharan Africa by Finlay et al, many adolescents lacked knowledge about SHR except for the knowledge related to HIV.16
The knowledge difference indicates that parents, guardians, and children are not discussing SRH. This difference may be attributed to parents being uncomfortable or not discussing SRH with their children, a common problem in many developing countries.6,9,10 A study in Nigeria showed that only 12.3% of parents discuss SRH matters with their adolescent girls,17 while another done in Ethiopia revealed that 14.7% of the discussion was with mothers and 3.9% with fathers.18 These low numbers seem to be more prevalent in less developed nations, yet they are the ones that grapple more with teenage pregnancies.19,20 A study done in the US showed that 70.6% of parents discuss SRH issues with their children, implying a high knowledge gap would be inexistent in such countries.21 The other aspect may be due to cultural differences, with most SRH issues, left to aunties and relatives other than the parents in most parts of Africa.22
Age of Consent Scenario
Compared to their parents, more teenage mothers believed it was legal for a 20-year-old man to have sex with a 15-year-old girl. This finding proves again the discrepancy in different laws in relation to the age for sexual consent. The majority of countries in Latin America have established the minimum age for sexual consent between 14 and 16 years, while many countries in Africa, including Rwanda, consider 18 years old the minimum age for sexual consent.23,24 This suggests a notable gap in understanding the age of consent laws between teenagers and parents/guardians. Addressing this difference in knowledge is crucial, as it has significant implications for protecting minors from exploitation and abuse. A recent systematic review by Kandi et al25 found that parents were the primary information source for teenagers. It went ahead to mention that education to children, on average, led to 77.43% more awareness and resulted in protection against sexual abuse and rape. However, this knowledge discrepancy may also be due to a lack of education from schools and other government programs concerning the legal age for sexual activities between citizens. Awareness campaigns are still needed to improve the public perception and knowledge about the age of consenting sex so that children and adolescents can be protected better.
Safe Abortion Scenario
Regarding access to safe abortion for a teenager who had been defiled, over half of both parents and their daughters thought it was illegal. Still, more parents, compared to teenage mothers, had this ideology. This shows that both groups have misconceptions about the legal status of safe abortion in cases of sexual violence. This may be attributed to the recent change in the law concerning medically assisted abortion for this group of victims in Rwanda.26 It is essential to provide accurate information to teenagers and parents about the legal rights and options available to young victims of sexual abuse. This role must be promoted by all the various stakeholders (NGOs, Ministry of Health, health workers, and educators) to ensure the public receives accurate knowledge. The lack of this knowledge is not isolated to Rwanda alone; a study in Nepal also found that knowledge among teenagers was, in some instances, as low as 21%.27 Also a review about abortion in Africa by Atuhaire et al28 underlines the importance of more awareness of safe abortion laws to curb increasing cases of unsafe abortion.
Right to Education for Teenage Mothers
When asked about the right to education after a teenage mother gives birth, fewer parents, compared to their daughters, thought it was not allowed. This finding highlights the need to address the perception that adolescent mothers may not have the right to education. Ensuring that all teenage mothers have access to education is vital for their empowerment and the well-being of their children.29,30 These results indicate the importance of comprehensive and accurate teaching about child rights and legal protections for teenagers and parents/guardians. With more teenage mothers believing that they are not allowed to get back to school may lead to low motivation to study following pregnancy, leading to internalized stigma. Such attitudes may significantly affect the academic performance of those who may be forced back to school. Like in South Africa,31 public awareness campaigns and educational programs should be designed and implemented to bridge the knowledge gap and dispel misconceptions about child rights law in Rwanda. Programs to assist teenage mothers’ mental well-being when they return to school should also be implemented to ensure smooth progress and reintegration in school. In addition, further research is warranted to explore the factors influencing knowledge disparities and identify effective strategies to improve understanding and compliance with child rights laws in Rwanda.
Understanding of Financial Responsibilities
Varying perceptives were reported, but both parents and their daughters, with more teenage mothers believing the man should support them during the pregnancy, and few parents agreed. Comparable results were obtained in a research involving pregnant teenagers who reported that father’s capacity to support the baby financially was important.32 The difference between teenage mothers and parents suggests that there might be varying perspectives on adolescent mothers’ financial obligations and burdens towards their children and may require additional support from the man. In a study conducted in South Africa by Nkani et al,33 about the ethnography of teenager’s mothers, they reported that teenager’s mothers are in need of financial support but also emotional support from the man who impregnated their daughters. Teenagers mothers are the one facing most of the challenges and consequences which may put them in position of financial need.34 It is essential to explore the reasons behind these differences and consider factors such as cultural norms, legal awareness, and social perceptions of financial support in such cases using qualitative methodology in future studies.
Involvement in Child Rearing
Teenagers strongly supported the man’s involvement in child rearing, yet their parents were not as affirmative. This also could be explained by parents of teenagers not trusting the fathers of their young babies, and studies have shown that these fathers are usually young with financial constraints and low educational background.35 Every stakeholder in such a situation should be well versed in the significance of active parental involvement for the well-being of the child as stated in the meta analysis about fathers’ absence and child well-being.36
Perceptions of Legal Consequences
The responses regarding potential jail time for the man were also divergent between the two groups. One in four teenagers strongly disagreed compared to one in 20 parents. This discrepancy indicates varying levels of understanding about the legal repercussions for siring a child with a minor. The finding may be due to the strength of the relationship and the romantic bond between the man and the teenager, which could impact the teenage mother’s perception of the need for the man to face legal consequences. In addition, some of the laws regarding punishment for men regarding offences against teenagers, such as Gender-Based Violence, have recently been amended, ie, 2019, and this might be more recent for people to be well aware of the consequences, and some may confuse the punishments.13 The discussion can delve into the importance of awareness of child protection laws and the need to prevent exploitative relationships.
Implication of Study Findings
The results above highlight the need to explore potential strategies for disseminating accurate information, such as school-based programs, community workshops, media campaigns, and free hotline services open 24 hours (like at HDI) to provide accurate information. Policies and interventions should be developed to promote child rights and protection. These should include community-based interventions to improve precise knowledge and awareness of child rights laws among teenagers and their parents.
Strengths and Limitation
This study covers most parts of the country through the various study sites in all districts of Rwanda. Thus, producing more generalizable findings to the country. In addition, the sample size was large to make adequate statistical power to assess for statistical differences between the two study groups. However, this study had some limitations that should be considered when interpreting the findings: The tools used were designed by the research team based on the current laws and no adequate psychometric analysis was considered to ensure the validity of the various assessed properties of SRH.11,13 Having a pregnancy as a teenager in the context of Rwanda is a sensitive issue, and desirable answers could have been provided. Thus, introducing bias to the findings. Also, recall bias could have been introduced since this cross-sectional survey’s assessed experience could have changed over time. Lastly, since the sampling method changed from purposive to convenience because of the pandemic, selection bias could have been introduced that limits the generalizability of the study findings.
Conclusion
A significant knowledge gap exists between parents and their children in Rwanda concerning sexual reproductive health rights. This implies that many families need to discuss these issues. It is recommended that future programming should devise innovative ways that bring together parents and their children to discuss sexual reproductive health, which will result in empowered children and teenagers in Rwanda. Also, awareness programs are needed to improve the knowledge gaps regarding SRH in the public by policymakers, NGOs, and educators.
Data Sharing Statement
The data is owned by HDI – Rwanda. Requests for data utilization should be sent to Aflodis Kagaba at [email protected].
Ethical Approval
The research team sought ethical approval from the Rwanda National Ethics Committee, under reference No947/RNEC/2020, on November 19, 2020. All participants provided informed written consent before enrollment in the study in accordance with the declaration of Helsinki. Approval from authors’ affiliated institutions was not required.
Acknowledgment
We are grateful to all study participants for their time. We all appreciate the efforts of staff from HDI.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Data collection was funded by resources from the Lucille and David Packard Foundation.
Disclosure
We have no conflict of interest.
References
1. WHO. Adolescent health. 2022; Available from: https://www.who.int/health-topics/adolescent-health#tab=tab_1.
2. Fantaye AW, Buh AW, Idriss-Wheeler D, et al. Effective educational interventions for promoting sexual and reproductive health and rights for school-age children in low-and middle-income countries: a systematic review protocol. Syst Rev. 2020;9(1):1–8. doi:10.1186/s13643-020-01464-w
3. Cressey SGupta R, Li M, et al. Adolescent Pregnancy and Sexual Reproductive Health and Rights in Rwanda. Policy Brief. London: Gender and Adolescence: Global Evidence; 2020.
4. Ndayishimiye P, Uwase R, Kubwimana I, et al. Availability, accessibility, and quality of adolescent Sexual and Reproductive Health (SRH) services in urban health facilities of Rwanda: a survey among social and healthcare providers. BMC Health Serv Res. 2020;20(1):1–11. doi:10.1186/s12913-020-05556-0
5. Silva M, Kassegne S, Nagbe RHet al. Determining the most significant changes on intergenerational communication and young people’s family planning and reproductive health outcomes: qualitative evaluation of the merci mon héros media campaign in niger and côte d’Ivoire. 2022.
6. Nilsson B, Edin K, Kinsman J, et al. Obstacles to intergenerational communication in caregivers’ narratives regarding young people’s sexual and reproductive health and lifestyle in rural South Africa. BMC Public Health. 2020;20(1):1–11. doi:10.1186/s12889-020-08780-9
7. Wamoyi J, Wight D, Remes P. The structural influence of family and parenting on young people’s sexual and reproductive health in rural northern Tanzania. Cult Health Sex. 2015;17(6):718–732. doi:10.1080/13691058.2014.992044
8. Maina BW, Ushie BA, Kabiru CW. Parent-child sexual and reproductive health communication among very young adolescents in korogocho informal settlement in Nairobi. Kenya Reprod Health. 2020;17(1):1–14.
9. Mataraarachchi D, Buddhika Mahesh PK, Pathirana TEA, et al. Mother’s perceptions and concerns over sharing sexual and reproductive health information with their adolescent daughters-A qualitative study among mothers of adolescent girls aged 14–19 years in the developing world, Sri Lanka. BMC Women’s Health. 2023;23(1):223. doi:10.1186/s12905-023-02369-1
10. Nurachmah E, Yona S, Ismail R, et al. Adolescent–parent communication about sexual and reproductive health among junior high school students in five areas with the highest prevalence of HIV in Indonesia: a qualitative study. Enfermería clínica. 2019;29:194–198. doi:10.1016/j.enfcli.2019.04.053
11. Office, P.M.s. Law n° 68/2018 of 30/08/2018 determining offences and penalties in general. 2018; Available from: https://rwandalii.africanlii.org/sites/default/files/gazette/OG%2Bno%2BSpecial%2Bof%2B27-09-2018.pdf.
12. Office, P.M.s. Ministerial order n°002/moh/2019 of 08/04/2019 determining conditions to be satisfied for a medical doctor to perform an abortion. 2019; Available from: file:///C:/Users/hp/Downloads/Ministerial_order_Abortion_conditions-2-12.pdf.
13. Office, P.M.s. Law No. 59/2008 of 2008 on Prevention and Punishment of Gender-Based Violence. 2008; Available from: https://www.refworld.org/docid/4a3f88812.html.
14. Office, P.M.s. N°71/2018 of 31/08/2018 Law relating to the protection of the child. 2018; Available from: https://www.migeprof.gov.rw/index.php?eID=dumpFile&t=f&f=13285&token=8af0700a140c59647a4ce75d41ff882b528f81f0.
15. Singh DR, Shrestha S, Karki K, et al. Parental knowledge and communication with their adolescent on sexual and reproductive health issues in Nepal. PLoS One. 2023;18(7):e0289116. doi:10.1371/journal.pone.0289116
16. Finlay JE, Assefa N, Mwanyika‐Sando M, et al. Sexual and reproductive health knowledge among adolescents in eight sites across sub‐Saharan Africa. Trop Med Int Health. 2020;25(1):44–53. doi:10.1111/tmi.13332
17. Malango NT, Hegena TY, Assefa NA. Parent–adolescent discussion on sexual and reproductive health issues and its associated factors among parents in Sawla town, Gofa zone. Ethiopia Reprod Health. 2022;19(1):108. doi:10.1186/s12978-022-01414-w
18. Abebe N, Mullu G. Assessment of parent adolescent communication on sexual and reproductive health issues and associated factors in alamata high school, northern Ethiopia. Int J Sci. 2013;7(1):83–92.
19. Cartes RM, Araya EG. Teenage pregnancy. J Pediatr Adolesc Gynecol. 2012;22:302–331.
20. Kirchengast S, Teenage pregnancies: a worldwide social and medical problem. An analysis of contemporary social welfare issues; 2016. 13.
21. Robin L, Dittus P, Whitaker D, et al. Behavioral interventions to reduce incidence of HIV, STD, and pregnancy among adolescents: a decade in review. J Adolesc Health. 2004;34(1):3–26. doi:10.1016/S1054-139X(03)00244-1
22. Kaggwa MM, Chaimowitz GA, Olagunju AT. Labia minora elongation: a neglected form of genital mutilation with mental and sexual health concerns. eClinicalMedicine. 2023;58:1
23. UNICEF. Legal minimum ages and the realization of adolescents’ rights; 2015; Available from: https://www.unicef.org/lac/sites/unicef.org.lac/files/2018-07/2._DIG._min_age_of_sexual_consent_PDF_BAJA_0.pdf#:~:text=Across%20the%20region%2C%20the%20overwhelming%20majority%20of%20countries,on%20the%20basis%20of%20gender%20and%20sexual%20orientation.
24. AgeofConsent. Legal Ages of Consent By Country. 2023; Available from: https://www.ageofconsent.net/world.
25. Kandi ZRK, Ebadi Fard Azar F, Khalajabadi Farahani F, et al. Significance of knowledge in children on self-protection of sexual abuse: a systematic review. Iran J Public Health. 2022;51(8):1755. doi:10.18502/ijph.v51i8.10257
26. Påfs J, Rulisa S, Klingberg-Allvin M, et al. Implementing the liberalized abortion law in Kigali, Rwanda: ambiguities of rights and responsibilities among health care providers. Midwifery. 2020;80:102568. doi:10.1016/j.midw.2019.102568
27. Adhikari R. Knowledge on legislation of abortion and experience of abortion among female youth in Nepal: a cross sectional study. Reprod health. 2016;13(1):1–9. doi:10.1186/s12978-016-0166-4
28. Atuhaire S. Abortion among adolescents in Africa: a review of practices, consequences, and control strategies. Int J Health Plann Manag. 2019;34(4):e1378–e1386. doi:10.1002/hpm.2842
29. Nkani N, Bhana D. Sexual and reproductive well-being of teenage mothers in a South African township school. S Afr J Educ. 2016;36(2):1–10. doi:10.15700/saje.v36n2a1181
30. Mezmur H, Assefa N, Alemayehu T. Teenage pregnancy and its associated factors in eastern Ethiopia: a community-based study. Int J Women’s Health. 2021;Volume 13:267–278. doi:10.2147/IJWH.S287715
31. Salam RA, Faqqah A, Sajjad N, et al. Improving adolescent sexual and reproductive health: a systematic review of potential interventions. J Adolesc Health. 2016;59(4):S11–S28. doi:10.1016/j.jadohealth.2016.05.022
32. Whitehead E. Exploring relationships in teenage pregnancy. Int J Nurs Pract. 2008;14(4):292–295. doi:10.1111/j.1440-172X.2008.00695.x
33. Nkani FN, An ethnographic study of teenage pregnancy: femininities and motherhood among pregnant teenagers and teenage mothers at school in Inanda. 2012.
34. Anayochukwu GI. Teenage pregnancy and its consequences: evidence from a south-eastern rural community of Nigeria. Int J Humanit Soc Sci. 2022;2(3):245–267. doi:10.35912/jshe.v2i3.977
35. Bunting L, McAuley C. Research review: teenage pregnancy and parenthood: the role of fathers. Child Fam Soc Work. 2004;9(3):295–303.
36. Adamsons K, Johnson SK. An updated and expanded meta-analysis of nonresident fathering and child well-being. J Family Psychol. 2013;27(4):589. doi:10.1037/a0033786
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.