")
Back to Journals » International Journal of General Medicine » Volume 14
Length of Stay and Short-Term Outcomes in Patients with ST-Segment Elevation Myocardial Infarction After Primary Percutaneous Coronary Intervention: Insights from the China Acute Myocardial Infarction Registry
Authors Lv J, Zhao Q, Yang J, Gao X, Zhang X, Ye Y, Dong Q, Fu R, Sun H, Yan X, Li W, Yang Y, Xu H
Received 20 July 2021
Accepted for publication 14 September 2021
Published 22 September 2021 Volume 2021:14 Pages 5981—5991
DOI https://doi.org/10.2147/IJGM.S330379
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Junxing Lv,1 Qinghao Zhao,1 Jingang Yang,1 Xiaojin Gao,1 Xuan Zhang,1 Yunqing Ye,1 Qiuting Dong,1 Rui Fu,1 Hui Sun,1 Xinxin Yan,1 Wei Li,2 Yuejin Yang,1 Haiyan Xu1 On behalf of the China Acute Myocardial Infarction Registry Study Group
1Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100037, People’s Republic of China; 2Medical Research & Biometrics Center, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100037, People’s Republic of China
Correspondence: Haiyan Xu; Yuejin Yang
Department of Cardiology, Fuwai Hospital, National Center for Cardiovascular Diseases, Chinese Academy of Medical Sciences and Peking Union Medical College, Beijing, 100037, People’s Republic of China
Tel +8610-88396082
Email [email protected]; [email protected]
Background: Length of stay (LOS) in patients with ST-segment elevation myocardial infarction (STEMI) is directly associated with financial pressure and medical efficiency. This study aimed to determine impact of LOS on short-term outcomes and associated factors of LOS in patients with ST-segment elevation myocardial infarction (STEMI) after primary percutaneous coronary intervention (PPCI).
Methods: A total of 3615 patients with STEMI after PPCI in the China Acute Myocardial Infarction registry were included in the analysis. Predictors of prolonged LOS were analyzed by multivariate logistic regression model with generalized estimating equation. The impact of LOS on 30-day clinical outcomes was assessed.
Results: The median LOS was 9 (7, 12) days. Patients with a longer LOS (> 7 days) were older, more often in lower-level hospitals, had more periprocedural complications and hospitalization expense. Fourteen variables, such as weekend admission and lower-level hospitals, were identified as independent associated factors of prolonged LOS. There were no significant difference in 30-day major adverse cardiac and cerebrovascular events (MACCE), readmission, and functional status between patients with LOS≤ 7d and LOS> 7d after multivariate adjustment and propensity score matching. However, patients who discharged over one week had better medication adherence (adjusted odds ratio: 0.817, 95% confidence interval: 0.687– 0.971, P=0.022). Significant interaction was observed in medication use between gender and LOS (Pinteraction=0.038).
Conclusion: Patients with STEMI undergoing PPCI experienced a relatively long LOS in China, which resulted in more medical expenses but no improvement on 30-day MACCE, readmission, and functional recovery. Poor 30-day medication adherence with short LOS reflects unsatisfying transition of management from hospital to community. More efforts are needed to reduce LOS safely and improve the efficiency of medical care.
Keywords: length of stay, ST-segment elevation myocardial infarction, primary percutaneous coronary intervention, prognosis
Introduction
Length of stay (LOS) is an important criterion to evaluate medical efficiency.1,2 In some countries, LOS in patients with ST-segment elevation myocardial infarction (STEMI) undergoing primary percutaneous coronary intervention (PPCI) has decreased significantly in several decades.3–5 China faces rising number of patients with STEMI,6 and extremely large medical expenses.7,8 It is of great importance to take more attention to LOS, as its critical role in saving hospital expenses and improving overall medical efficiency.
Reducing LOS was considered to be safe in studies from developed countries.2,9–13 A series of risk assessment tools, such as the second Primary Angioplasty in Myocardial Infarction (PAMI-II) criteria and the Controlled Abciximab and Device Investigation to Lower Late Angioplasty Complications (CADILLAC) risk score, were established and recommended to screen low-risk patients for early discharge.10,14,15 However, few “real-world” studies focused on the impact of LOS on clinical outcomes comprehensively, especially for recovery of social function and medication adherence, which are also important for clinicians to make decisions.16 Additionally, in developing countries with unbalanced medical resources and disparate medical insurance, patient characteristics and predictors of prolonged LOS may be totally different from those in developed countries. It is important to ascertain the impact of LOS on clinical outcomes in developing countries. Therefore, this study aimed to analyze impact of LOS on short-term outcomes and associated factors of LOS in STEMI patients after PPCI in China.
Methods
Study Population
The China Acute Myocardial Infarction registry is a prospective, nationwide, multicenter observational study.17 Briefly, 108 hospitals that cover 27 provinces and 4 municipalities were included throughout Mainland China except Hong Kong and Macau. In China, hospital classification was based on Chinese vertical administrative model (province, prefecture, county, township, and village). One of the largest hospitals (province-level hospital), 1 to 3 prefecture-level hospitals, and 1 to 4 county-level hospitals in every province or municipality were included in the registry.17 Participating hospitals were required to enroll AMI patients consecutively and the final inclusion criteria must meet third Universal Definition for Myocardial Infarction.18 Types 4a and type 5 AMIs were not eligible for this registry. Patient demographics, clinical presentation, medical history, risk factors, laboratory results, medications, LOS, hospital expenses, hospital features, and clinical outcomes were collected by trained clinical cardiologist or cardiovascular fellows. Definitions of elements were based on the ACC/AHA Task Force on clinical data standards and NCDR-ACTION-GWTG element dictionary.
Patients with STEMI undergoing PPCI from January 2013 to September 2014 in China Acute Myocardial Infarction registry were included in this study. Following patients were excluded: patients with in-hospital death; patients who were transferred in from other hospitals; patients who were discharged for further medications; patients who received any repeated revascularization during hospitalization; and patients with no follow-up data or invalid LOS.
Clinical Outcomes
The primary endpoint was 30-day major adverse cardiac and cerebrovascular events (MACCE), including cardiac death, recurrent myocardial infarction, stroke, and cardiovascular readmission. The second endpoints included all-cause readmission, functional status, and medication use within 30 days after discharge. Readmission was counted as a cardiovascular readmission unless a clear non-cardiac cause was documented. Poor functional recovery was defined as keeping resting at home after discharge. Poor medication adherence was defined as stopping at least one drug which were used at discharge.
Statistical Analysis
Patients were divided into 2 groups based on the first quartile of LOS. Continuous variables in normal distribution were presented as mean ± standard deviation and compared by Student t-test. Mann–Whitney U-test was used to compare continuous variables in non-normal distribution, which were presented as medians (quartiles), and examine differences in distribution of LOS stratified by hospital level and location. Categorical variables were described using frequencies (percents) and compared by Chi-square test.
Binary logistic regression model was used to analyze the independent associated factors of LOS and clustering among hospitals was adjusted by general estimating equation method. To avoid omitting factors, variables including patient demographics, medical history, presenting characteristics, procedural and angiographic characteristics, and hospital features were used to fit the model. We further performed multivariate logistic regression models to evaluate association between LOS and clinical outcomes. Propensity score matching based on 1:1 nearest-neighbor matching was also used to compare outcomes between patients discharged in short and long LOS. This logistic regression-based propensity score model was adjusted for age, gender, hospital level, weekend admission, creatinine, left ventricular ejection fraction (LVEF), new-onset heart failure, recurrent myocardial infarction, stroke, intra-aortic balloon pump insertion, symptom onset to admission time, cardiac arrest at admission, Killip class, three-vessel or left main disease, left main or left anterior descending related infarction, stent type, glycoprotein (GP) IIb/IIIa inhibitor, postprocedural Thrombolysis In Myocardial Infarction (TIMI) flow grade, periprocedural complications, previous myocardial infarction, previous heart failure, previous stroke, and previous renal dysfunction. With a caliper of 0.02, 1038 patients with LOS≤7d (87.0%) were matched successfully. The covariate balance was tested by standardized mean difference plot with a threshold of 0.1 (Supplementary Figure 1). Because the standard mean difference of stent type exceeded 10%, it was further adjusted by logistic regression model in the propensity-matched cohort as an additional analysis. Subgroup analyses were carried out based on hospital level, age, gender, PAMI-II criteria, and CADILLAC risk score. Results were expressed using odds ratios (OR) with 95% confidence intervals (CI). Statistical analysis was performed using R software (version 4.0.2, R Foundation for Statistical Computing, Vienna, Austria) and SPSS for Windows (version 23.0, IBM, New York, USA). Two-tailed P<0.05 was considered statistically significant. More details of the statistical analysis were shown in Supplementary Method.
Results
Baseline Characteristics
A total of 3615 patients with STEMI undergoing PPCI who survived at discharge were included in the analysis (Supplementary Figure 2). Distribution of LOS is shown in Supplementary Figure 3. The median LOS was 9 (7, 12) days. Of all patients, 1193 (33.0%) discharged within 7 days and 2422 (67.0%) over one week.
As presented in Table 1, patients with LOS>7d were more often older, non-smokers, and more commonly to pay with health insurance compared with patients with shorter LOS. Systolic blood pressure, hemoglobin, and LVEF were higher in patients discharged earlier compared with those in longer LOS group. Higher Killip class and prevalence of cardiac arrest at admission were mainly seen in patients with longer LOS. Besides, patients were more likely to have an intra-aortic balloon pump, three-vessel or left main disease, periprocedural complications, and in-hospital adverse events in longer LOS group.
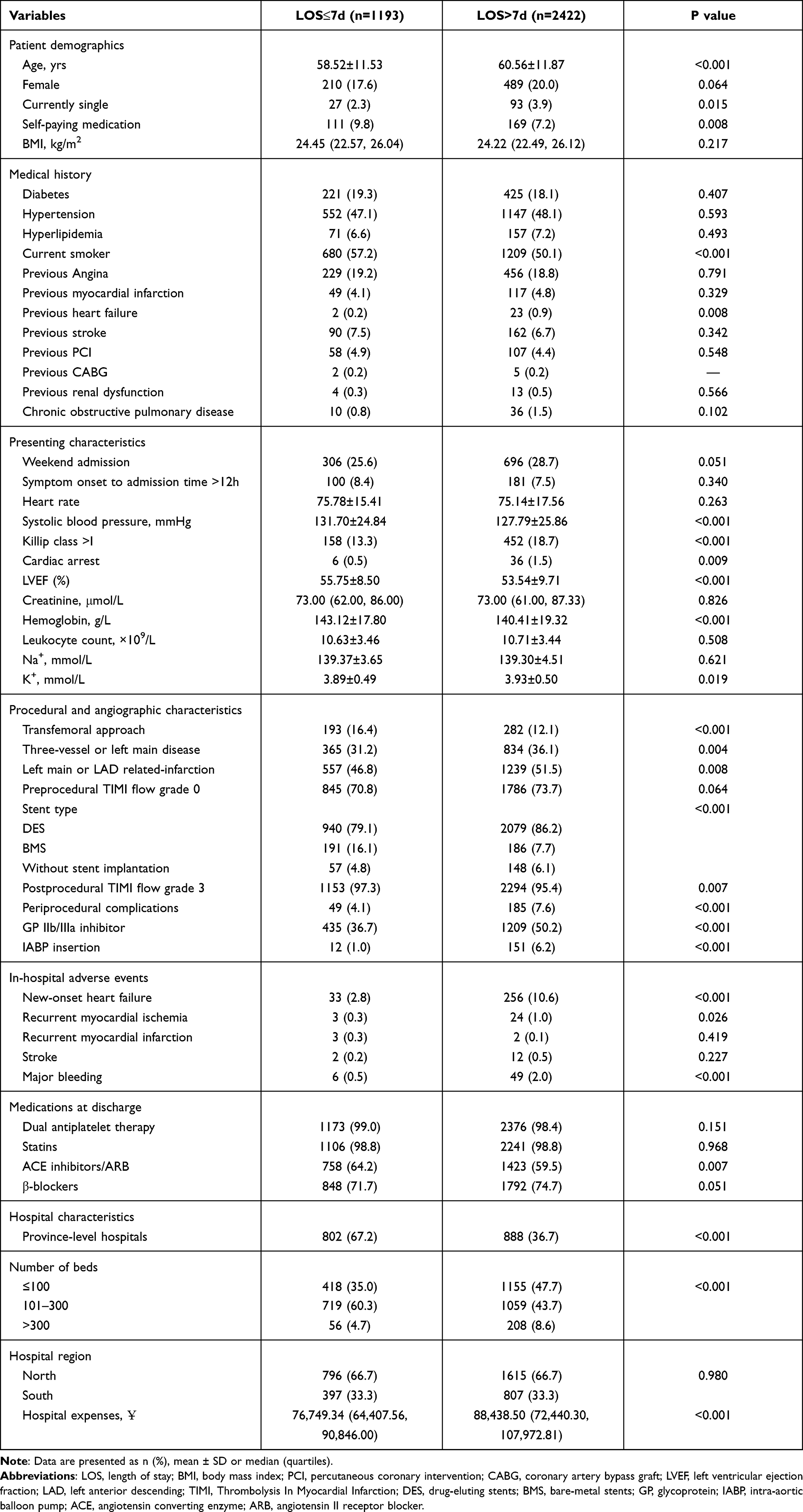 |
Table 1 Baseline Characteristics for Patients Stratified by LOS |
As for hospital characteristics and expenses, patients in province-level hospitals experienced significantly shorter LOS than those in lower-level hospitals (P<0.001), while there was no difference between hospitals in the North and South (P=0.103) (Supplementary Figures 4 and 5). Not surprisingly, expenses were significantly higher in longer LOS patients (Table 1).
Associated factors of LOS
In multivariate analysis, age, body mass index, prior heart failure, weekend admission, Killip class, systolic blood pressure, left ventricular ejection fraction, leukocyte count, cardiac arrest at admission, left main or left anterior descending related infarction, GPIIb/IIIa inhibitor, intra-aortic balloon pump insertion, hospital levels, and number of beds in department of cardiology were independent associated factors of LOS (Table 2). It should be noted that self-paying lost statistical significance in the multivariate analysis (OR: 0.773, 95% CI: 0.567–1.054, P=0.104). Among hospital-related factors, hospital level was strongly associated with LOS (OR: 5.979, 95% CI: 3.308–10.807, P<0.001).
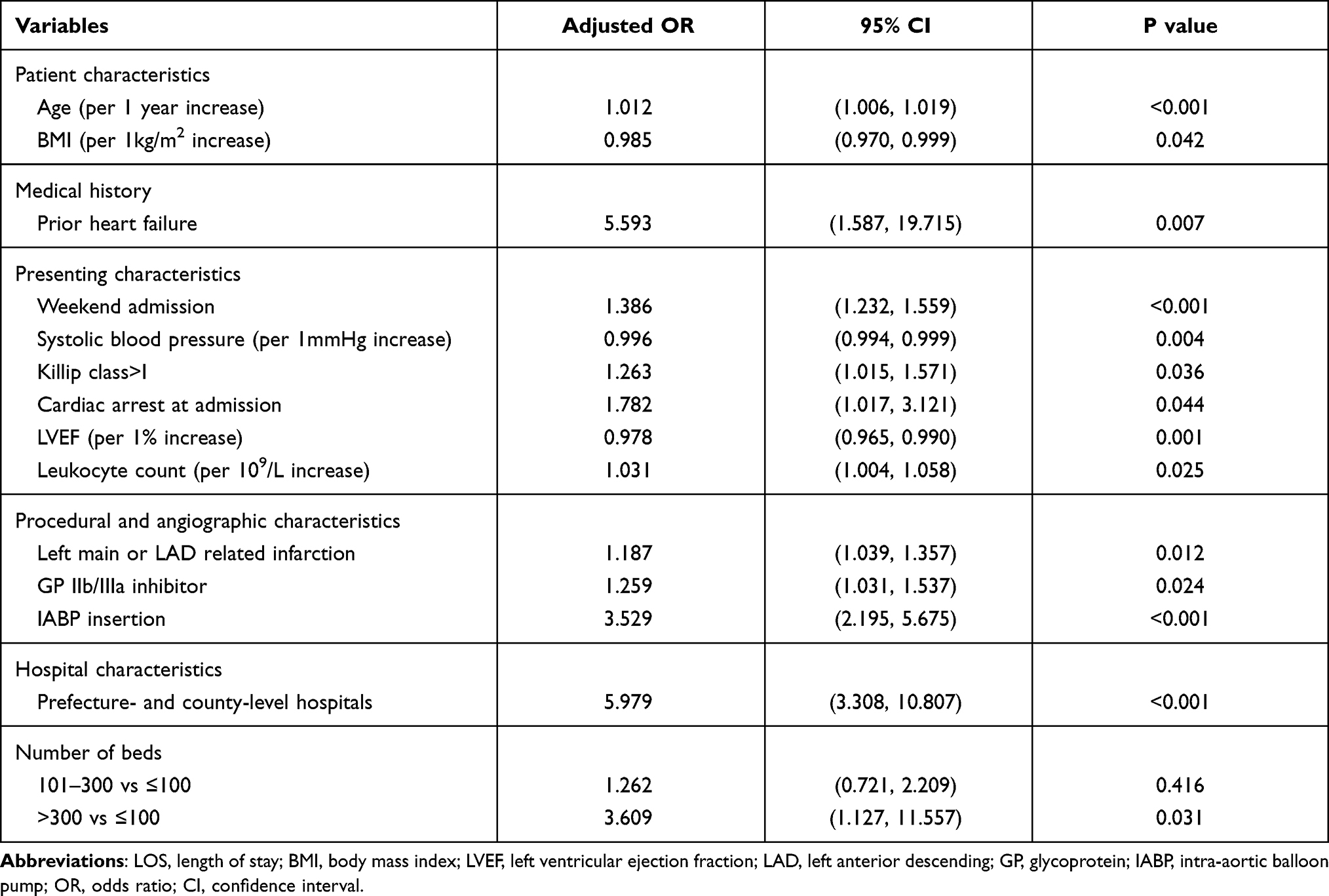 |
Table 2 Independent Predictors of Prolonged Length of Stay (LOS>7d) |
Association Between LOS and 30-Day Outcomes
MACCE, all-cause readmission, and functional status in different LOS groups are depicted in Figure 1A–C. The overall rates of MACCE, all-cause readmission, and resting at home were 4.0%, 4.1%, and 60.5%, respectively. Patients in longer LOS group had significantly higher rates of poor functional recovery compared with those with short LOS (63.2% and 55.0%, P<0.001). The rates of MACCE and all-cause readmission only showed a higher trend in patients with LOS>7d as compared with those with LOS≤7d (MACCE: 4.0% and 3.3%; all-cause readmission: 4.3% and 3.6%, respectively, both P>0.05). Table 3 shows association between LOS and 30-day outcomes. Longer LOS did not affect the risk of 30-day MACCE (adjusted OR: 1.085, 95% CI: 0.710–1.657, P=0.706) and all-cause readmission (adjusted OR: 1.060, 95% CI: 0.704–1.594, P=0.781) after multivariate adjustment. Furthermore, no difference was observed after propensity score matching (MACCE, OR: 1.541, 95% CI: 0.971–2.445, P=0.067; all-cause readmission, OR: 1.299, 95% CI: 0.828–2.037, P=0.255). Similar results were obtained after adjusting for stent type in the propensity-matching cohort (MACCE, OR: 1.565, 95% CI: 0.985–2.486, P=0.058; all-cause readmission, OR: 1.336, 95% CI: 0.850–2.099, P=0.210).
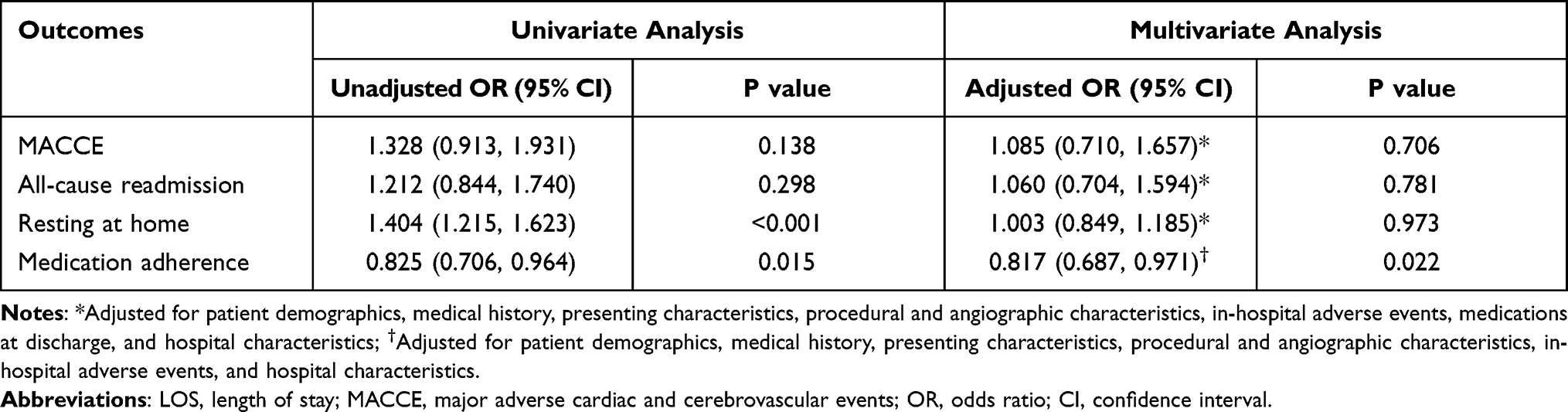 |
Table 3 Association Between LOS and 30-Day Outcomes |
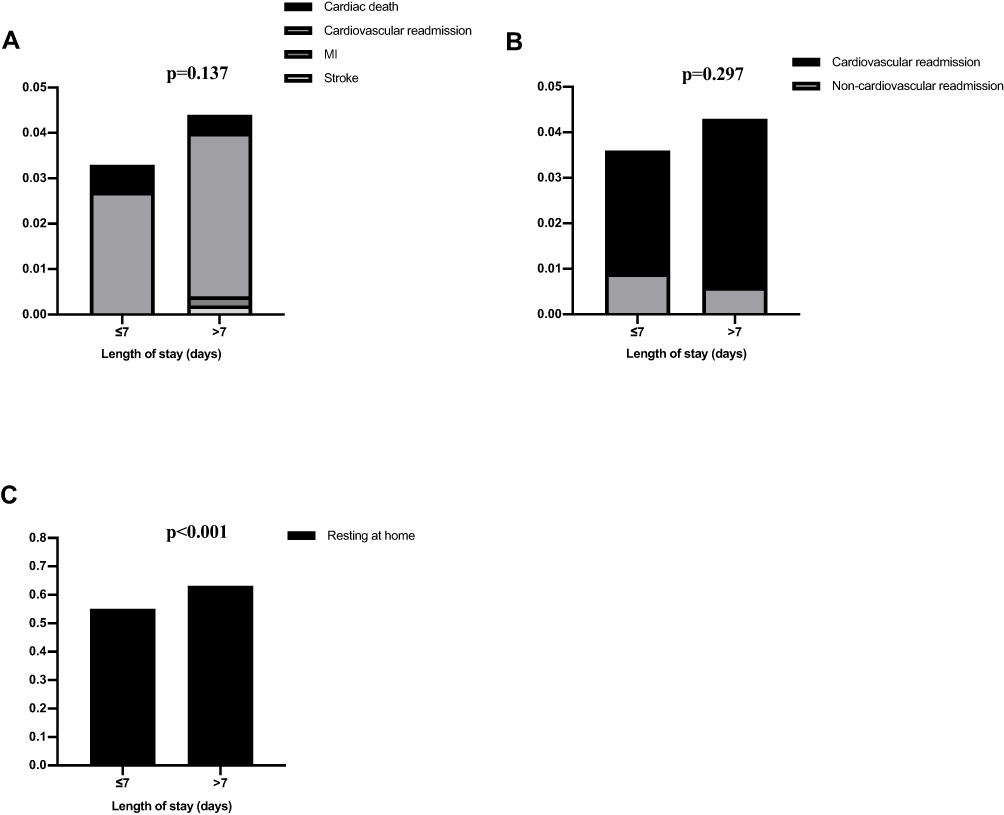 |
Figure 1 30-day clinical outcomes in different LOS groups. (A) MACCE. (B) Readmission. (C) Functional status. MACCE was defined as the composite of cardiac death, cardiovascular readmission, recurrent myocardial infarction, and stroke. Abbreviations: MACCE, major adverse cardiac and cerebrovascular events; LOS, length of stay; MI, myocardial infarction. |
Medication adherence was examined by comparing medications at different time points between LOS groups (Figure 2A–D). Within 30 days after discharge, proportion of patients not taking at least one drug prescribed at discharge was 26.2% (948 patients). In multivariate analysis, patients with longer LOS displayed significantly better medication adherence (OR: 0.817, 95% CI: 0.687–0.971, P=0.022). Similar result was gained from propensity-matching analysis (OR: 0.815, 95% CI: 0.671–0.989, P=0.038), even after further adjusting for stent type (OR: 0.815, 95% CI: 0.670–0.990, P=0.040).
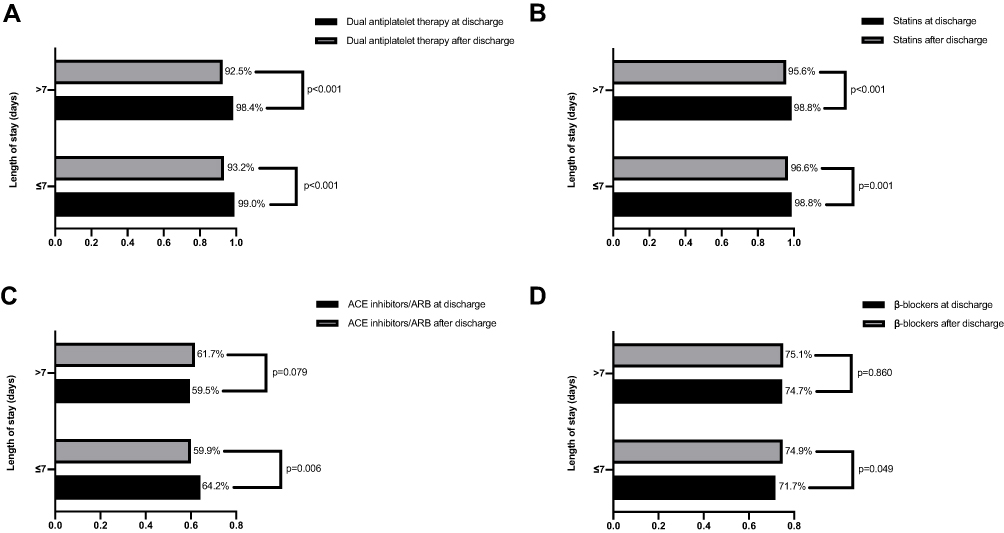 |
Figure 2 Comparison of medication usage between at and after discharge in different LOS groups. (A) Dual antiplatelet therapy. (B) Statins. (C) ACE inhibitors/ARB. (D) β-blockers. Abbreviations: LOS, length of stay; ACE, Angiotensin Converting Enzyme; ARB, angiotensin receptor blockers. |
Subgroup Analysis
The impact of LOS was further evaluated in different subgroups (Supplementary Figure 6). For patients meeting PAMI-II criteria or with CADILLAC RS 0–2, median LOS were both 8 (7, 11) days. There were no significant interactions between factors (hospital level, age, gender, PAMI-II criteria, and CADILLAC risk score) and LOS in 30-day MACCE, all-cause readmission, and functional status (Pinteraction>0.05). However, we observed a significant interaction between gender and LOS on medication adherence (Pinteraction=0.038).
Discussion
In this study, we found a relatively long LOS in patients with STEMI undergoing PPCI in China, even in low-risk patients selected by validated tools. Fourteen variables were identified as independent associated factors of LOS. Longer LOS had no improvement on primary outcome. However, our result revealed an unexpected impact of LOS on medication compliance.
Nationwide data showed that the median LOS of patients with STEMI in China was 7 days in 2018, and mean LOS was significantly shorter than that in 2017 (7.66d vs 9.09d).19 For patients undergoing PPCI, previous study showed that the median LOS was 9 days during 2007–2010,20 which was in line with our result. Additionally, our analysis indicated significantly more expenses of patients with longer LOS. The post hoc analysis of the Assessment of Pexelizumab in Acute Myocardial Infarction study that enrolled patients from July 2004 to May 2006 showed short median LOS in the United States (3 days), New Zealand (4 days), and Australia (4 days).21 There are several potential reasons for the relatively long LOS in China. First, limitations in medical efficiency including management processes deviated from standard still exist in China, particularly in lower-level hospitals.22,23 Second, patients with STEMI still have the certain risk of short-term adverse events following PPCI. Thus, early discharge forces doctors to face more concern. Third, the proportion of in-hospital reimbursement is higher than that of outpatient reimbursement in some regions, which may lead to the longer LOS as the wish of patients.24
In this study, weekend admission was an independent predictor of prolonged LOS, which was similar with result from Chin and colleagues,25 reflecting gaps of medical care quality between weekday and weekend. Our result indicated that patients with LOS>7d had more serious presenting characteristics at admission, including lower systolic blood pressure, higher Killip class, and cardiac arrest, which could be used to identify patients at higher probability of prolonged LOS. Lower LVEF was also an important predictor of longer LOS. Previous studies have demonstrated prognostic value of renal function in patients with STEMI.26–28 In present study, we found no significant impact of chronic renal dysfunction or creatinine on LOS. Interestingly, although numerous studies proved more advantages of transradial approach than transfemoral access in percutaneous coronary intervention (PCI),29 even for STEMI patients with cardiogenic shock,30 transradial approach was not an independent associated factor of LOS in this analysis. This result might reflect serious LOS redundancy in a different way. That is to say, despite lower risk of bleeding complications and periprocedural death, patients who underwent PPCI with transradial approach experienced excessive in-hospital observation in current situation. We also found that usage of drug-eluting stents, which had shown more benefits in patients with STEMI over bare-metal stents,31,32 was not associated with LOS. For the hospital-related factors, our work showed that prefecture- and county-level hospitals, instead of hospital locations, were strongly associated with longer LOS, which was opposite to the results from others.2,25 The disparity of LOS in different level hospitals may be influenced by various factors such as care capability and quality, care efficiency and philosophy of disease management.
Early study suggested that shortening LOS in patients with myocardial infarction had no impact on prognosis, and significantly saved medical expenses.10 Subsequently, some small randomized control trials supported the early discharge strategy.11,12 However, a few studies showed that shorter LOS was related to a higher rate of readmission,21 and for older patients, very early discharge strategy was associated with an increase in 30-day mortality.2 In European Society of Cardiology Guidelines for the management of STEMI, only low-risk patients identified using appropriate criteria were recommended to discharge within 48-72 hours.15 For countries with limited medical resources, clinical decisions for early discharge should be made more cautiously to balance the benefit and risk. Chinese patients experienced longer LOS, and the consequences of reducing LOS within a short period of time are unknown. To date, this is the largest study to assess association between LOS and prognosis in a developing country. This “real world” study showed that shorter LOS had no impact on 30-day MACCE or readmission.
Unexpectedly, our results showed that patients discharged within one week had poorer medication compliance. Moreover, there was difference in subgroup analysis stratified by gender. Prior to this study, only Safe-Depart trial enrolled 54 patients who underwent primary or rescue PCI examined the effect of early discharge on 6-week medication compliance.11 In this small, single-center, randomized controlled trial, no difference in medication compliance were observed. The opposite conclusions can be partly explained by sample size, and type of study which may affect the facilitation of health education. More importantly, a number of patients lack correct cognition of their own health status and related knowledge. Data from the China Patient-Centered Evaluative Assessment of Cardiac Events (China PEACE)-Retrospective CathPCI study showed that in the first month after discharge, nearly 30% of patients did not take the medicine as prescribed.33 They analyzed the main reason was that patients considered their condition had improved significantly. For patients with shorter LOS, this misunderstanding may be more common. Health education and medical transition from hospital to home should be further improved. Previous studies also indicated gender disparity in medication adherence.34,35 One of important reasons for this phenomenon is that women are more likely to serve as caregivers among family members.35 Therefore, the interaction between gender and LOS in medication adherence might be explained by women’s tendency to work for family earlier.
The Coronavirus Disease 2019 (COVID-19) Pandemic has become a serious public health crisis worldwide. Previous study showed that the pandemic had significant impact on STEMI care, even in a non-COVID-19 epicenter.36 During the early part of 2020, many hospitals in China adopted a fibrinolysis-first strategy considering the in-hospital delay to exclude coronavirus infection.37 Data from our institution showed that usage of PPCI for patients with STEMI decreased markedly, and LOS of patients with STEMI was significantly longer than that in 2019,37 and LOS in this work. More studies are needed to investigate associated factors of LOS and its impact on clinical outcomes during the pandemic, while the present work aims to explore these issues under normal mode of STEMI management.
Limitations
The study has several important limitations. First, this analysis is based on a cohort from observational study. Therefore, despite using multivariate analysis, confounding factors may exist. Large-scale randomized controlled trials are further needed.16 Second, compared with those in western countries, a significantly smaller proportion of patients discharged within 72 hours. Thus, we cannot evaluate the effect of very early discharge. Third, experience of invasive cardiologists and hospital volume were not included in the CAMI registry. Previous studies have found significant expertise-outcome and volume-outcome relationships for PCI.38–40 However, it should be noted that the requirements of operator and hospital volume were different in different countries. According to European Society of Cardiology Guidelines on myocardial revascularization, PCI for acute coronary syndromes should be performed by operators with volumes of ≥75 per year at high-volume institutions (≥400 per year),41 while Chinese Society of Cardiology guidelines recommended PPCI should be performed by operators with annual volumes of ≥50 procedures in cardiac catheterization laboratory with volumes of ≥100 PCIs per year.42 More efforts are still needed to clarify the threshold and the impact of hospital volume on clinical outcomes of PCI. Finally, since the study population is entirely composed of Chinese patients, it is uncertain that this conclusion can be applied to other countries. Nevertheless, few studies examined the association between LOS and prognosis in “real-world” practice comprehensively, particularly for developing countries. In this perspective, we think this study is an important supplement.
Conclusions
Our study showed that the LOS was relatively long against growing number of STEMI patients in China. Prolonging LOS brought no significant improvement in main adverse outcomes. Poorer medication adherence in patients discharged within one week called for raising health awareness of patients and better management after discharge. More efforts should be made to reduce LOS without affecting disease management quality. Health education and medical transition from hospital to home are needed to be highlighted.
Data Sharing Statement
Data are available on reasonable request from the corresponding authors.
Ethics Approval and Informed Consent
The study protocol conformed to the ethical guidelines of the Declaration of Helsinki and was approved by the institutional review board central committee at Fuwai Hospital, National Center for Cardiovascular Diseases of China (No. 2012-431). Written informed consent was obtained from eligible patients before registration.
Acknowledgments
We express our great gratitude to all staff and investigators for the China Acute Myocardial Infarction registry. In addition, we thank Zhengyang Niu for his assistance in statistical analysis. Haiyan Xu and Yuejin Yang contributed equally to this work as co-correspondence authors.
Funding
This study was supported by the Twelfth Five-Year Planning Project of the Scientific and Technological Department of China [Grant No. 2011BAI11B02].
Disclosure
The authors have no conflicts of interest to declare in this work.
References
1. Newby LK, Eisenstein EL, Califf RM, et al. Cost effectiveness of early discharge after uncomplicated acute myocardial infarction. N Engl J Med. 2000;342(11):749–755. doi:10.1056/NEJM200003163421101
2. Swaminathan RV, Rao SV, McCoy LA, et al. Hospital length of stay and clinical outcomes in older STEMI patients after primary PCI: a report from the National Cardiovascular Data Registry. J Am Coll Cardiol. 2015;65(12):1161–1171. doi:10.1016/j.jacc.2015.01.028
3. Rogers WJ, Canto JG, Lambrew CT, et al. Temporal trends in the treatment of over 1.5 million patients with myocardial infarction in the US from 1990 through 1999: the National Registry of Myocardial Infarction 1, 2 and 3. J Am Coll Cardiol. 2000;36(7):2056–2063. doi:10.1016/s0735-1097(00)00996-7
4. Abu-Assi E, Bernal JL, Raposeiras-Roubin S, et al. Temporal trends and prognostic impact of length of hospital stay in uncomplicated ST-segment elevation myocardial infarction in Spain. Rev Esp Cardiol. 2020;73(6):479–487. doi:10.1016/j.rec.2019.09.016
5. Velagapudi P, Kolte D, Ather K, et al. Temporal trends and factors associated with prolonged length of stay in patients with ST-elevation myocardial infarction undergoing primary percutaneous coronary intervention. Am J Cardiol. 2018;122(2):185–191. doi:10.1016/j.amjcard.2018.03.365
6. Li J, Li X, Wang Q, et al. ST-segment elevation myocardial infarction in China from 2001 to 2011 (the China PEACE-Retrospective Acute Myocardial Infarction Study): a retrospective analysis of hospital data. Lancet. 2015;385(9966):441–451. doi:10.1016/S0140-6736(14)60921-1
7. Yang J, Yang X, Yang Y. Analysis of hospitalization expenses of patients with acute myocardial infarction in basic medical insurance of urban population. Chin Circ J. 2018;33(11):1094–1097. doi:10.3969/j.issn.1000-3614.2018.11.012
8. Hu S, Gao R, Liu L, et al. Summary of the 2018 report on cardiovascular diseases in China. Chinese Circ J. 2019;34(3):209–220. doi:10.3969/j.issn.1000-3614.2019.03.001
9. Jones DA, Rathod KS, Howard JP, et al. Safety and feasibility of hospital. discharge 2 days following primary percutaneous intervention for ST-segment elevation myocardial infarction. Heart. 2012;98(23):1722–1727. doi:10.1136/heartjnl-2012-302414
10. Grines CL, Marsalese DL, Brodie B, et al. Safety and cost-effectiveness of early discharge after primary angioplasty in low risk patients with acute myocardial infarction. PAMI-II Investigators. Primary angioplasty in myocardial infarction. J Am Coll Cardiol. 1998;31(5):967–972. doi:10.1016/s0735-1097(98)00031-x
11. Kotowycz MA, Cosman TL, Tartaglia C, et al. Safety and feasibility of early hospital discharge in ST-segment elevation myocardial infarction–a prospective and randomized trial in low-risk primary percutaneous coronary intervention patients (the Safe-Depart Trial). Am Heart J. 2010;159(1):
12. Melberg T, Jørgensen M, Ørn S, et al. Safety and health status following early discharge in patients with acute myocardial infarction treated with primary PCI: a randomized trial. Eur J Prev Cardiol. 2015;22(11):1427–1434. doi:10.1177/2047487314559276
13. Novobilsky K, Stipal R, Cerny P, et al. Safety of early discharge in low risk patients after acute ST-segment elevation myocardial infarction, treated with primary percutaneous coronary intervention. Open label, randomized trial. Biomed Pap. 2019;163(1):61–66. doi:10.5507/bp.2018.041
14. Halkin A, Singh M, Nikolsky E, et al. Prediction of mortality after primary percutaneous coronary intervention for acute myocardial infarction: the CADILLAC risk score. J Am Coll Cardiol. 2005;45(9):1397–1405. doi:10.1016/j.jacc.2005.01.041
15. Ibanez B, James S, Agewall S, et al. 2017 ESC Guidelines for the management of acute myocardial infarction in patients presenting with ST-segment elevation: the Task Force for the management of acute myocardial infarction in patients presenting with ST-segment elevation of the European Society of Cardiology (ESC). Eur Heart J. 2018;39(2):119–177. doi:10.1093/eurheartj/ehx393
16. Sharkawi MA, McMahon S, Al Jabri D, et al. Current perspectives on location of monitoring and length of stay following PPCI for ST elevation myocardial infarction. Eur Heart J Acute Cardiovasc Care. 2019;8(6):562–570. doi:10.1177/2048872619860217
17. Xu H, Li W, Yang J, et al. The China Acute Myocardial Infarction (CAMI) Registry: a national long-term registry-research-education integrated platform for exploring acute myocardial infarction in China. Am Heart J. 2016;175:193–201. doi:10.1016/j.ahj.2015.04.014
18. Thygesen K, Alpert JS, Jaffe AS, et al. Third universal definition of myocardial infarction. Circulation. 2012;126(16):2020–2035. doi:10.1161/CIR.0b013e31826e1058
19. Working Group on coronary Artery Disease, National Center for Cardiovascular Quality Improvement (NCCQI). 2019 clinical performance and quality measures for adults with acute ST-elevation myocardial infarction in China. Chin Circ J. 2020;35(4):313–325. doi:10.3969/j.issn.1000-3614.2020.04.001
20. Han H, Wei X, He Q, et al. Comparison of in-hospital mortality and length of stay in acute ST-segment-elevation myocardial infarction among urban teaching hospitals in China and the United States. J Am Heart Assoc. 2019;8(22):e012054. doi:10.1161/JAHA.119.012054
21. Kociol RD, Lopes RD, Clare R, et al. International variation in and factors associated with hospital readmission after myocardial infarction. JAMA. 2012;307(1):66–74. doi:10.1001/jama.2011.1926
22. Xu H, Yang Y, Wang C, et al. Association of hospital-level differences in care with. outcomes among patients with acute ST-segment elevation myocardial infarction in China: insights from China Acute Myocardial Infarction Registry. JAMA Network Open. 2020;3(10):e2021677. doi:10.1001/jamanetworkopen.2020.21677
23. Leng W, Yang J, Fan X, et al. Contemporary invasive management and. in-hospital outcomes of patients with non-ST-segment elevation myocardial infarction in China: findings from China Acute Myocardial Infarction (CAMI) Registry. Am Heart J. 2019;215:1–11. doi:10.1016/j.ahj.2019.05.015
24. Li Q, Lin Z, Masoudi FA, et al. National trends in hospital length of stay for acute myocardial infarction in China. BMC Cardiovasc Disord. 2015;15:9. doi:10.1186/1471-2261-15-9
25. Chin CT, Weintraub WS, Dai D, et al. Trends and predictors of length of stay after primary percutaneous coronary intervention: a report from the CathPCI registry. Am Heart J. 2011;162(6):1052–1061. doi:10.1016/j.ahj.2011.09.008
26. Hayıroğlu Mİ, Keskin M, Uzun AO, et al. Predictors of in-hospital mortality in patients with ST-segment elevation myocardial infarction complicated with cardiogenic shock. Heart Lung Circ. 2019;28(2):237–244. doi:10.1016/j.hlc.2017.10.023
27. Wadie M, Samaan E, Nassar MK, et al. Estimated glomerular filtration rate as one of the main predictors of in-hospital mortality in Egyptian patients with ST elevation myocardial infarction: a two-year retrospective study. Egypt Heart J. 2020;72(1):32. doi:10.1186/s43044-020-00067-z
28. Hayıroğlu Mİ, Bozbeyoglu E, Yıldırımtürk Ö, et al. Effect of acute kidney injury on long-term mortality in patients with ST-segment elevation myocardial infarction complicated by cardiogenic shock who underwent primary percutaneous coronary intervention in a high-volume tertiary center. Turk Kardiyol Dern Ars. 2020;48(1):1–9. doi:10.5543/tkda.2019.84401
29. Siudak Z, Tokarek T, Dziewierz A, et al. Reduced periprocedural mortality and bleeding rates of radial approach in ST-segment elevation myocardial infarction. Propensity score analysis of data from the ORPKI Polish National Registry. EuroIntervention. 2017;13(7):843–850. doi:10.4244/EIJ-D-17-00078
30. Tokarek T, Dziewierz A, Plens K, et al. Radial approach reduces mortality in patients with ST-segment elevation myocardial infarction and cardiogenic shock. Pol Arch Intern Med. 2021;131(5):421–428. doi:10.20452/pamw.15886
31. Kalesan B, Pilgrim T, Heinimann K, et al. Comparison of drug-eluting stents with bare metal stents in patients with ST-segment elevation myocardial infarction. Eur Heart J. 2012;33(8):977–987. doi:10.1093/eurheartj/ehs036
32. Siudak Z, Dziewierz A, Rakowski T, et al. Borderline trend towards long-term mortality benefit from drug eluting stents implantation in ST-elevation myocardial infarction patients in Poland-data from NRDES registry. Catheter Cardiovasc Interv. 2014;83(3):436–442. doi:10.1002/ccd.25169
33. Shang P, Liu GG, Zheng X, et al. Association between medication adherence and 1-year major cardiovascular adverse events after acute myocardial infarction in China. J Am Heart Assoc. 2019;8(9):e011793. doi:10.1161/JAHA.118.011793
34. Hussain S, Jamal SZ, Qadir F. Medication adherence in post myocardial infarction patients. J Ayub Med Coll Abbottabad. 2018;30(4):552–557.
35. Lewey J, Shrank WH, Bowry AD, et al. Gender and racial disparities in adherence to statin therapy: a meta-analysis. Am Heart J. 2013;165(5):665–678. doi:10.1016/j.ahj.2013.02.011
36. Hammad TA, Parikh M, Tashtish N, et al. Impact of COVID-19 pandemic on ST-elevation myocardial infarction in a non-COVID-19 epicenter. Catheter Cardiovasc Interv. 2021;97(2):208–214. doi:10.1002/ccd.28997
37. Leng WX, Yang JG, Li XD, et al. Impact of the shift to a fibrinolysis-first strategy on care and outcomes of patients with ST-segment-elevation myocardial infarction during the COVID-19 pandemic-The experience from the largest cardiovascular-specific centre in China. Int J Cardiol. 2021;329:260–265. doi:10.1016/j.ijcard.2020.11.074
38. Hannan EL, Wu C, Walford G, et al. Volume-outcome relationships for percutaneous coronary interventions in the stent era. Circulation. 2005;112(8):1171–1179. doi:10.1161/CIRCULATIONAHA.104.528455
39. Tokarek T, Dziewierz A, Plens K, et al. Radial approach expertise and clinical outcomes of percutanous coronary interventions performed using femoral approach. J Clin Med. 2019;8(9):1484. doi:10.3390/jcm8091484
40. Post PN, Kuijpers M, Ebels T, et al. The relation between volume and outcome of coronary interventions: a systematic review and meta-analysis. Eur Heart J. 2010;31(16):1985–1992. doi:10.1093/eurheartj/ehq151
41. Neumann FJ, Sousa-Uva M, Ahlsson A, et al. 2018 ESC/EACTS Guidelines on myocardial revascularization. Eur Heart J. 2019;40(2):87–165. doi:10.1093/eurheartj/ehy394
42. Chinese Society of Cardiology of Chinese Medical Association, Editorial Board of Chinese Journal of Cardiology. 2019 Chinese Society of Cardiology (CSC) guidelines for the diagnosis and management of patients with ST-segment elevation myocardial infarction. Chin J Cardiol. 2019;47(10):766–783. doi:10.3760/cma.j.issn.0253-3758.2019.10.003
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.