Back to Journals » Advances in Medical Education and Practice » Volume 17
Learning Needs Assessment Among Indonesian Dental Schools’ Teachers for Teaching Evidence-Based Practice
Authors Firman DR ![]() , de Jong PGM
, de Jong PGM ![]() , Dekker FW
, Dekker FW ![]()
Received 16 October 2025
Accepted for publication 5 March 2026
Published 25 April 2026 Volume 2026:17 566750
DOI https://doi.org/10.2147/AMEP.S566750
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Md Anwarul Azim Majumder
Dani R Firman,1,2 Peter GM de Jong,1 Friedo W Dekker1,3
1Center for Innovation in Medical Education, Leiden University Medical Center, Leiden, The Netherlands; 2Department of Oral Biology, Faculty of Dentistry, Universitas Padjadjaran, Kabupaten Sumedang, Jawa Barat, Indonesia; 3Department of Clinical Epidemiology, Leiden University Medical Center, Leiden, The Netherlands
Correspondence: Dani R Firman, Department of Oral Biology, Faculty of Dentistry, Universitas Padjadjaran, Jl. Raya Bandung-Sumedang Km. 21 Jatinangor, Kabupaten Sumedang, Jawa Barat, Indonesia, Tel +0227794120, Email [email protected]; [email protected]
Introduction: Evidence-based practice (EBP) in dentistry is considered the standard for achieving optimal patient outcomes, integrating the best scientific evidence, clinical expertise, and patient values. EBP implementation in most low-resource countries remains limited. To improve EBP education in Indonesian dental schools, it is necessary to explore their specific needs and their current capabilities, which were not yet available. Therefore, the aim of this study is to describe candidate teachers’ profile, attitudes toward EBP, self-reported use of evidence, learning needs, and willingness to support peers, providing a basis for developing a tailored training program.
Methods: A validated online questionnaire was distributed via email in June 2024 to 165 candidate teachers across 29 Indonesian dental schools.
Results: A nearly equal number of candidate teachers from public and private dental schools responded, (n=125; 75.8%). While most respondents received prior EBP training, 16% reported no exposure. Twenty-eight percent had experience teaching EBP, and just 3.2% had served as EBP instructor in continuing education. The average teachers’ attitude towards EBP score was moderately high positive 37.5 (SD=4.4; min=9; max=45). Textbook, original research, and review articles were the most used, and brochures of products, consulting colleagues, and the Cochrane Library were the least used. Regarding learning needs, 71.2% of teachers expressed their need to learn more, 58.8% need teaching materials support, and 14% were willing to share their knowledge or teaching materials.
Conclusion: This study revealed a widespread need for candidate teachers for further training and teaching material support and identified candidates that were willing to teach their colleagues. Both low-level and high-level evidence sources were utilized, and candidate teachers had positive attitudes towards EBP. These results reveal more explicit learning needs for EBP training and a potential collaboration among the teachers to develop a nation-wide faculty development program.
Keywords: evidence-based practice, national survey, faculty development, needs assessment
Introduction
Initially, evidence-based practice (EBP) was introduced in medicine, also known as evidence-based medicine (EBM) more than three decades ago.1 This approach has also been used by other health professionals, including in dentistry, which known as evidence-based dentistry (EBD). EBP as a general term is widely recognised as a standard of care to ensure the best possible patient outcomes, including the search for the best evidence, critical evaluation of the evidence, and integration of the evidence with practitioners’ experience and expertise based on patient preferences.2,3
Within the field of dental education, students are expected to have the skills to utilise research for clinical decision-making. Dental schools play a key role in training future dentists in EBP competencies. EBP teaching programs should begin during early education and provide students experience on practicing them as integrated clinical programs.4,5 This approach is expected to support the uptake of evidence-based treatments and practices in dentistry.6,7
The EBP approach is widely implemented in developed countries. Although the same principles are applied in developing countries, research reports of the implementation on EBP in middle- and low-income countries remain significantly less compared to developed countries.8 The World Health Organization (WHO) has actively promoted the implementation of EBP specifically for dental settings within developing regions such as Southeast Asia.9 This global strategy for oral health recommendations emphasises the EBP approach for better decision-making.10 Indonesia is one of the developing countries in Southeast Asia, with 32 dental schools spread across its archipelago, comprising private and public universities. In comparison with other countries in Southeast Asia, it has the largest number of dental schools, which is considered a significant asset in the region.11
In our previous study, we found that the deans and curriculum teams of Indonesian dental schools acknowledged their limited availability of EBP teachers and recognized the need to train more of them.12 As a follow up, to develop relevant training opportunities that align with candidate teachers’ needs, it is essential to conduct a needs assessment. This is particularly important given the potential diversity in backgrounds, attitudes, the use of evidence, learning experiences, learning needs, and prior involvement in implementing and teaching EBP. Therefore, this study aimed to describe the profile of candidate teachers, their attitudes toward EBP, self-reported evidence use, learning needs, and willingness to share the knowledge with other teachers of EBP.
The findings of such an assessment can provide critical evidence for the development and tailoring of teaching EBP training programs. These programs are expected to enhance EBP teaching at their own schools, potentially leading to a better implementation of EBP on a national scale and, ultimately, improve oral health care for patients.
Materials and Methods
Study Setting and Data Collection
In collaboration with the Association of Indonesian Dental Schools, which had 32 eligible dental schools at the time this study was conducted. A formal invitation letter was sent to the deans of all the schools. The letter was asking the deans to participate in a faculty development program of EBP teaching by nominating candidate teachers, with the criteria including having an active role in teaching EBP or EBP-related subjects (such as scientific literacy, research methodology, statistics, or epidemiology) or being projected to teach EBP in the future. Out of the 29 schools that responded, we received 165 candidate dental teachers nominated by the deans.
Candidates representing various disciplines in dentistry were identified as either prospective trainees or future trainers in EBP. The participating institutions included 15 private and 14 public dental schools, which provided a broad representation of the dental education sector across the country.
The survey was administered online via Google Forms in June 2024 and was distributed by email. The questionnaire was accessible for 1 month, and most participants completed the questionnaire within the first two weeks. Prior to participation, respondents were presented with an introductory statement outlining the objectives of the study, the voluntary nature of participation, and assurances of confidentiality and data protection. This information was explicitly included in the introduction section of the questionnaire where they were asked to provide informed consent. Participants were informed that individual identities and affiliated institutions would remain confidential and would not be linked to any survey responses. All analyses were performed on aggregated data, without reference to any specific institution.
Questionnaire and Variables
We used a translated and modified version of a validated questionnaire consisting of closed- and open-ended questions that was previously used in dental faculties in Iran, which is strongly relevant because it was validated specific for dental schools and it has a similar setting to Indonesia as an upper-middle-income-country.13 The questionnaire was translated by two person that having qualification in dental education and familiar with EBP. One of the aims of this study is to describe learning needs of the teachers, therefore the instrument was modified by replacing the actual knowledge test section as multiple-choice question items with a self-perceived needs about EBP specific topics as checklist. The EBP specific topics were based on the questionnaire of our previous study.12
The translated and modified questionnaire was pilot tested to examine clarity with teachers of the target population to assess clarity and comprehensibility. Participants provided feedback on item wording and interpretation, leading to minor revisions for improved clarity. Face validity was also evaluated by experts in EBP topic, who confirmed that the items appeared to adequately measure the intended constructs.
The questionnaire comprised five sections, each designed to capture a distinct aspect of participants’ background, experiences, and perspectives related to EBP. The first section gathers demographic information, including age, gender, professional background, and years of experience. This information provided context for interpreting participants’ responses in subsequent sections.
The second section focusses on participants’ experiences in learning and teaching EBP. Respondents were asked to report any formal or informal training they had received, as well as any involvement in teaching EBP to others. This section aims to reveal participants’ prior exposure to EBP education. In the third section, participants indicate the extent to which they rely on higher or lower-level sources of evidence in their professional practice. Low-level sources include textbooks, congresses and seminars, pharmaceutical brochures, and expert consultations, which are categorised as expert opinion as in the hierarchy of evidence pyramid.13,14 While high-level evidence sources include original research articles, systematic reviews, evidence-based guidelines, and the Cochrane Library as pre-appraised evidence.15,16 Responses were recorded using a Visual Analog Scale (VAS) ranging from 0 (not used at all) to 10 (used very frequently).
The fourth section assesses participants’ attitudes toward EBP using nine statements rated on a five-point Likert scale, ranging from 1 (strongly disagree) to 5 (strongly agree). This section aims to capture the level of agreement with statements reflecting beliefs, values, and perceptions about the importance and usefulness of EBP. Total scores could range from 9 to 45, with higher scores indicating more positive attitudes toward EBP.
The final section explores participants’ learning and teaching material needs and their willingness to share their teaching materials and knowledge, as multiple response items. This section is organized around key subtopics commonly included in EBP curricula, such as the introductory to EBP, the five steps of EBP (Ask, Acquire evidence, Critical appraisal and interpretation, Apply, and Evaluation), and EBP teaching strategies. The subtopic lists of EBP five-step was adapted from Gorgon (2013) to assess participants to indicate which specific topics they identified gaps in their knowledge or instructional ability.17
The survey was administered using Google Forms under a Google Workspace for Education account, which provides institutional-level data security and privacy controls. This setup complies with relevant data protection standards, including the General Data Protection Regulation (GDPR), by ensuring that identifying information is stored separately from survey responses and used exclusively for communication purposes related to the upcoming faculty development program.
Statistical Analysis
Data were analysed using R version 4.5.0 (R Foundation for Statistical Computing, Vienna, Austria). Descriptive statistics such as means, standard deviations, frequencies, and percentages were calculated as appropriate. Normality of continuous variables was assessed using the histogram. Data with approximately normal distribution are presented as mean and standard deviation, whereas non-normally distributed data are presented as median and interquartile range (IQR).
Results
Demographic
Of all the 165 candidate teachers from 29 Indonesian dental schools in total, 125 teachers responded to the survey (75.8%), and most of them completed it within the first two weeks. Most respondents were female (80%). The median age of respondents was 41 years (min = 30, max = 63), and the median duration of teaching experience in dental schools was 12 years. Respondents typically conducted 10 research projects during their tenure as lecturer, excluding research undertaken as part of their final assignments during formal education. Most respondents hold Master and/or Specialist educational background (60%), with a median of 11 years of clinical experience. Most respondents had prior experience with EBP learning, while 16% had no such experience. Thirty-five respondents (28%) had experience as EBP teachers, but only four (3.2%) had served as EBP instructors in continuing education or professional development. The demographic characteristics of participants are presented in Table 1. Respondents were affiliated with either a pre-clinic or a clinic department (see S1 in the supplementary files).
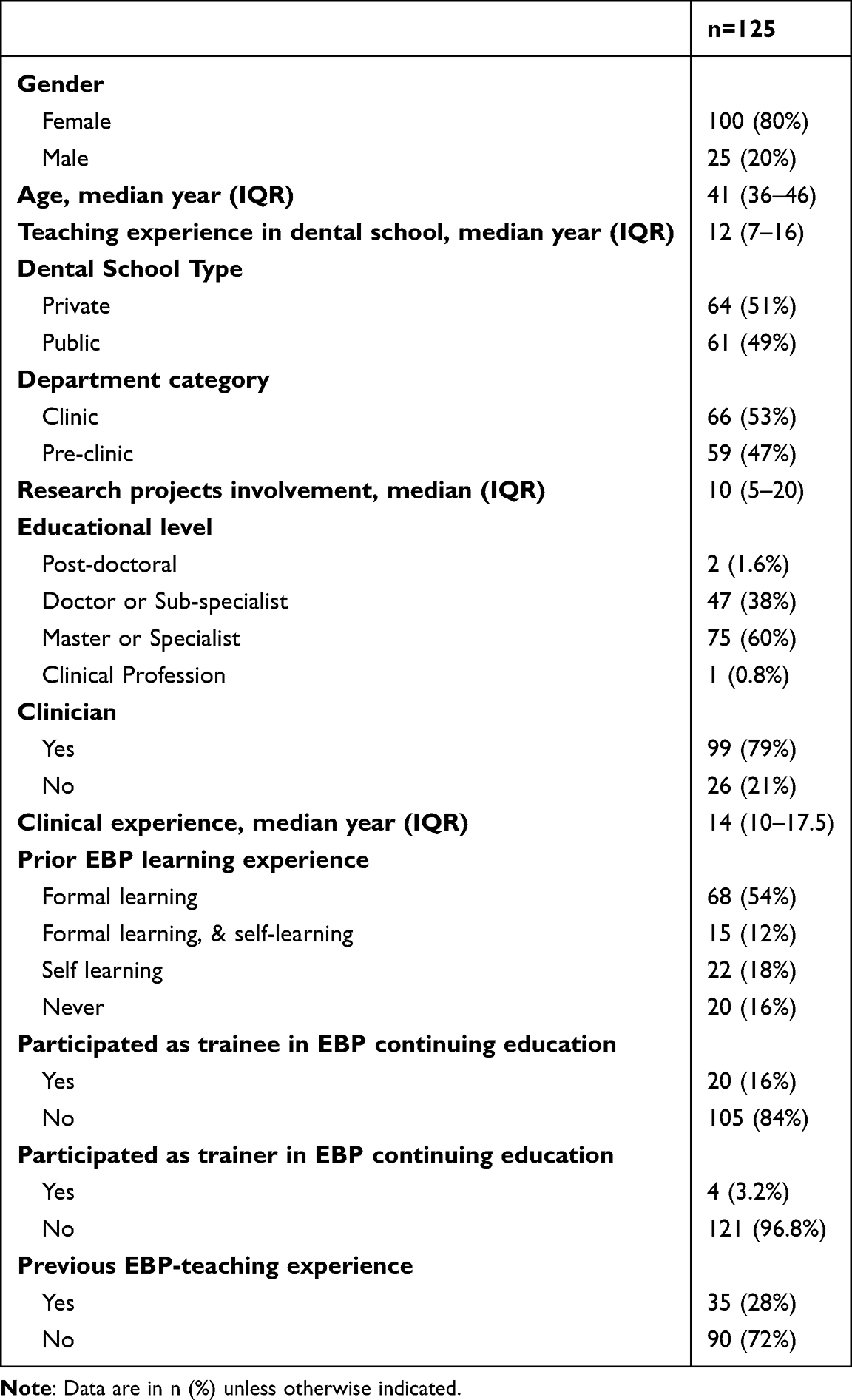 |
Table 1 Demographic of Respondents |
Attitudes Towards EBP
Overall, the responses reflect a generally positive attitude towards EBP. This is based on the distribution of responses to nine statement items, measured using a five-point Likert scale ranging from “Strongly Disagree=1” to “Strongly Agree=5” (see Figure 1). The respondents’ attitude towards EBP total score was 37.5 (SD=4.4; min=9; max=45). Most respondents either agreed or strongly agreed that EBP facilitates clinical decision-making (94.4%), promotes the quality of oral healthcare (97.6%), and that scientific evidence is an appropriate guide for clinical practice in dentistry (93.6%). Notably, the majority (92%) of the participants expressed a necessity for additional training in EBP.
 |
Figure 1 Candidate teachers’ attitude towards EBP. |
Items that were negatively worded and reverse-coded (indicated with’(r)’), such as the view that dental care can be delivered effectively without EBP, or that EBP is unnecessary due to the limited types of services, received lower levels of agreement. For instance, 87.2% of respondents disagreed or strongly disagreed with the statement that EBP is not necessary, and 79.2% rejected the notion that care can be provided perfectly without the EBP approach. For better interpretation (green color indicates positive attitude and red as negative attitude towards EBP), the score of these two items, and other negative items were reversed to align with other positive items (see Figure 1; and S2 in the supplementary files).
Frequency of Evidence Source Usage
The frequency of evidence source utilized by respondents, based on a scale ranging from 0 (not used at all) to 10 (used very frequently) was categorised into high-level and low-level evidence sources (see Table 2). Among the high-level evidence sources, original article journals had the highest use, followed closely by review articles and evidence-based guidelines. In contrast, the Cochrane Library, a reputable source of systematic reviews, had a relatively lower usage.
 |
Table 2 Evidence Sources Usage (0=Do Not Use at All, 10=use Very Frequently) |
By comparison, low-level evidence sources showed generally lower levels of use. Drug or product brochures and informal consultations with colleagues were among the least frequently used sources. An exception within this category was textbooks, which were the most used of the low-level evidence source category.
Learning Needs, Teaching Needs and Willingness to Share
The respondents’ self-reported learning needs, need for teaching material support, and willingness to share knowledge or materials across 30 subtopics of EBP were assessed and structured in seven domains of EBP topics, see Table 3 (Complete listing of items is available as S3 in the supplementary files). Overall, the majority of respondents self-reported that they need to learn more about several EBP topics, half of the respondents need teaching material supports, and less than 20% are willing to share knowledge or materials. The topic of teaching EBP strategies or methods scored highest on the list of learning needs (74.4–75.2%). In contrast, “Acquiring evidence” had the lowest percentage among all topics (62.4–70.4%).
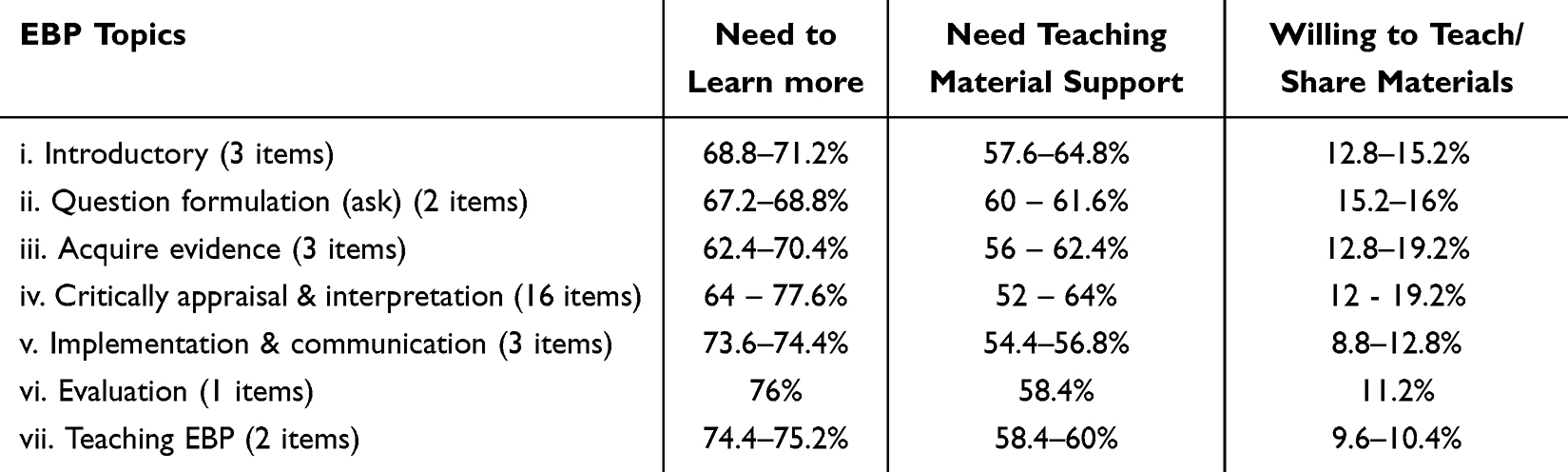 |
Table 3 Range of Self-Reported Learning Needs, Material Support Needs and Willingness to Teach based on EBP Topics Category |
As shown in Table 4, more than 50% of respondents indicated a need for further learning in all 30 listed EBP subtopics across all domains. In contrast, only six respondents expressed a willingness to share knowledge or materials in all 30 subtopics. In addition, more than two-thirds of respondents needed support in fewer than one-third of the EBP subtopics across all topics.
 |
Table 4 Cumulative Range of Chosen EBP Subtopics Items by Candidate Teachers |
Notably, the subtopics with the highest reported need for further learning included “Use of appraisal tools to assess validity” (77.6%), “Critical appraisal of systematic reviews and meta-analysis” (77.6%), and “Critical appraisal of studies about diagnosis and prognosis” (75.2%). The support for EBP teaching material in all subtopics across all domains is needed by 52% to 64.8% of the respondents (see S3 in the supplementary files).
Discussion
In this nationwide study involving faculty members from 29 dental schools across Indonesia, we found moderately high positive attitudes among candidate teachers towards EBP, and confirmation by the majority of their learning needs, and only a few teachers willing to share their knowledge to other colleagues in all the EBP subtopics. The willingness of candidate teachers to share may be related to their self-perception of competence, as in the Self Determination Theory.18 These findings reflect their potential contributions as future EBP educators in the country.
Another nationwide initiative of the EBP program among of 18 UK and Irish dental schools was also conducted as a national survey, by mapping statistics teaching across undergraduate dental programmes.19 The finding revealed wide variation in content and delivery of statistics teaching as part of EBP education. Although our study differs in scope, both studies share a common implication, is to increase faculty awareness to drive improvement, which we considered as key element for follow-up program.
One key modification to the instrument was replacing objective knowledge test items with self-assessment checklist items to create a lower-pressure environment during the initial phase of improving EBP education among teachers. In contrast to formal evaluations such as assessing actual knowledge of EBP, e.g. an evaluation of EBP knowledge, attitude, confidence and evidence access of dental hygienist teachers in the United States.20 Our approach focused on self-perceived needs and was considered more appropriate for encouraging broader teacher participation and engagement in follow-up programs, rather than positioning the study as a formal evaluation, as reflected in the high response rate.
A majority strongly agreed that EBP enhances clinical decision-making, promotes the quality of oral healthcare, and that scientific evidence is an appropriate guide for practice. Within the Classification Rubric for EBP Assessment Tools in Education (CREATE) framework, attitudes are considered as a fundamental and strong predictor of future EBP implementation in clinical decision-making.21 Therefore, examining candidate teachers’ attitudes toward EBP was considered essential in this phase. Overall, the cumulative responses reflect a positive attitude towards EBP, which may strengthen the advancement of EBP education within their schools.
Most participants rejected negatively worded statements that minimized the relevance of EBP, indicating a solid conceptual endorsement of its value. However, some concerns were evident, particularly regarding factors beyond the candidate teachers’ control. Most respondents agreed or strongly agreed that limited access to scientific information in Indonesian dental schools poses a significant obstacle to implementing EBP. This finding underscores that while individual readiness is crucial, structural and institutional support is equally necessary for sustainable EBP implementation. Without sufficient access to evidence and supportive infrastructure, even well-intentioned and well-informed educators may struggle to integrate EBP into teaching and clinical practice.22
Another key observation is the inconsistency in self-reported evidence utilisation among participants. This inconsistency reflects not only the varying levels of EBP competence but also potential barriers to accessing or utilising quality evidence sources. The findings indicate a preference for high-level evidence sources over low-level sources. However, among the high-level sources of evidence, the Cochrane Library was the least frequently used by candidate teachers. This finding aligns with a previous study by Sabounchi et al (2013) in Iran.13 One of the most relevant Cochrane groups for dentistry is Cochrane Oral Health, which publishes summaries of research evidence to help people (patients, carers, clinicians, researchers and funders) make better informed decisions about oral healthcare choices.23 A possible reason for its limited use could be the restriction imposed by its paywall system.
In contrast, while standard textbooks are generally regarded as low resource according to hierarchy of evidence pyramid, yet they remain the most frequently utilised resource among candidate teachers. Standard textbooks continue to be relevant for foundational knowledge, possibly due to the most current research advancement often take longer to be incorporated into these texts. Therefore, enhancing access to higher-quality evidence resources and offering practical training or providing access may help to promote the use of the best available evidence.
Encouragingly, many participants acknowledged their own learning needs, which reflects a degree of openness and self-awareness. This willingness to improve should be considered a positive foundation for future capacity-building measures. At the same time, a notable concern emerged; very few respondents felt confident teaching their peers to become EBP educators. This lack of confidence could hinder the dissemination of EBP principles within institutions and limit the sustainability of EBP integration in the curricula.24
These findings suggest that while the foundational attitudes towards EBP implementation are strong, there remains a significant need for further training, as indicated by more than half of the respondents. This highlights a gap between belief and perceived competence. The distinction between attitude and self-efficacy is crucial, although participants support EBP in principle, many do not yet feel fully capable of practicing or teaching it confidently.
Interestingly, a larger proportion of respondents expressed interest in learning more about EBP than in teaching it. This imbalance may reflect limited self-efficacy or perceived inadequacy in their current EBP skillset. Addressing this issue through comprehensive training aligned with the CREATE framework will increase knowledge and improve attitudes, self-efficacy, and behaviours, which might ultimately enhance both individual competence and institutional teaching capacity in EBP.
Strengths and Limitations
This study reflects a notably high level of nationwide participation by dental schools in the context of EBP education. Furthermore, by identifying specific areas of need, it offers actionable insights for the development of EBP training programs that are contextually relevant and aligned with institutional objectives.
However, several limitations must be acknowledged. First, this result might not reflect teachers in Indonesian dental schools in general, because the selection of candidate teachers was selected by their respective deans, which we have no control to ensure that the deans not missed any suitable candidates. Moreover, these individuals might already be high performers or more motivated, which could skew results toward more favourable self-assessments. We are also aware the results might be different in teachers of the three non-participating dental schools. Nevertheless, given that candidate teachers from approximately 90% of Indonesian dental schools participated, therefore the risk of sampling bias is minimal.
Second, the study did not include objective measures of EBP knowledge. This also limits our ability to compare perceived versus actual competencies, a common concern in self-reported studies. Future stage research of interventional study with pre- and post-test should consider incorporating multiple domains and sources on assessing the progress of EBP competence, as well as a longitudinal designs to evaluate the impact of faculty development interventions over time.
Conclusion
This study revealed a widespread need of candidate teachers in Indonesia for further training and teaching material support on the topic of EBP. It also identified only a few candidates that are willing to teach their colleagues. Both low-level and high-level evidence sources are being used, and in general candidate teachers have positive attitudes toward EBP. These results reveal more explicit learning needs for EBP training and a potential collaboration among the teachers to develop a nation-wide faculty development program.
Data Sharing Statement
Anonymized data are only available on reasonable request by email to the corresponding author.
Compliance with Ethical Standards
Research approval for this study was obtained from the Educational Research Review Board of the Leiden University Medical Center (OEC/ERRB/20230613-2). All prospective respondents were informed about the study’s objectives, the voluntary nature of their participation, the intended use of the collected data, and the measures taken to protect their anonymity in any resulting publications. Informed consent was obtained electronically prior to participation.
Acknowledgments
The authors would like to express sincere appreciation to all respondents; the deans of the participating schools for providing lists of candidate teachers; the Indonesian Dental Schools Association and its members for their support; and the research group of Center for Innovation in Medical Education, LUMC for their valuable and constructive feedback. The authors also acknowledge Vitri Darlene and Ahmad Haidar Baqir for their contribution to the questionnaire translation.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agreed to be accountable for all aspects of the work.
Funding
This research was funded by a PhD scholarship to the first author from Universitas Padjadjaran, Indonesia (3781/UN.6.WR2/KP.10/2021) and the open-access publishing charge was supported by Leiden University Medical Center (LUMC).
Disclosure
This research was previously presented at the Dutch Association for Medical Education conference in May 2025 or known as Nederlandse Vereniging voor Medisch Onderwijs (NVMO) Conference, in the Netherlands, as a scientific presentation with interim findings. The abstract, titled “Learning needs assessment of evidence-based practice among Indonesian dental faculty members to guide a nation-wide development training program” is available in the database of NVMO abstracts (https://nvmo.nl/abstract/learning-needs-assessment-of-evidence-based-practice-among-indonesian-dental-faculty-members-to-guide-a-nation-wide-development-training-program/).
The authors report no conflicts of interest in this work.
References
1. Sackett DL, Rosenberg WM, Gray JM, Haynes RB, Richardson WS. Evidence based medicine: what it is and what it isn’t. BMJ. 1996;312:71–10. doi:10.1136/bmj.312.7023.71
2. Kishore M, Panat SR, Aggarwal A, Agarwal N, Upadhyay N, Alok A. Evidence based dental care: integrating clinical expertise with systematic research. J Clin Diagn Res. 2014;8(2):259. doi:10.7860/JCDR/2014/6595.4076
3. Weyant RJ. Teaching evidence-based practice: considerations for dental education. Dental Clini North Ame. 2019;63(1):97–117. doi:10.1016/j.cden.2018.08.010
4. Lallier TE. Introducing evidence–based dentistry to dental students using histology. J Dental Educ. 2014;78(3):380–388. doi:10.1002/j.0022-0337.2014.78.3.tb05688.x
5. Kachabian S, Seyedmajidi S, Tahani B, Naghibi Sistani MM. Effectiveness of educational strategies to teach evidence-based dentistry to undergraduate dental students: a systematic review. Evidence Based Dentistry. 2024;25(1):53–54. doi:10.1038/s41432-023-00958-5
6. Kao RT. The challenges of transferring evidence-based dentistry into practice. J Evid Based Dental Prac. 2006;6(1):125–128. doi:10.1016/j.jebdp.2005.12.011
7. Azarpazhooh A, Mayhall JT, Leake JL. Introducing dental students to evidence-based decisions in dental care. J Dental Educ. 2008;72(1):87–109. doi:10.1002/j.0022-0337.2008.72.1.tb04457.x
8. Tiley C, Kyriakopoulos M. Evidence-based practice in a multicultural world: changing with the times. BJPsych Int. 2018;15(3):55–57. doi:10.1192/bji.2018.14
9. World Health Organization. Strategy for Oral Health in South-East Asia, 2013-2020. WHO Regional Office for South-East Asia; 2013.
10. Benzian H, Guarnizo-Herreño CC, Kearns C, Muriithi MW, watt RG. The WHO global strategy for oral health: an opportunity for bold action. Lancet. 2021;398(10296):192–194. doi:10.1016/S0140-6736(21)01404-5
11. He S, Wu S, Duangthip D, Chu CH, Lo ECM. Teaching of silver diamine fluoride for the management of dental caries and hypersensitivity – situation in the Southeast Asia dental schools. BMC Oral Health. 2023;23(1):815. doi:10.1186/s12903-023-03502-0
12. Firman DR, Dekker FW, Riyanti E, Widyaputra S, Jong PGM. Evidence-based practice teaching in Indonesian dental schools: a survey among faculty members. Asia Pacific Scholar. 2025;10(3):65–74. doi:10.29060/TAPS.2025-10-3/SC3251
13. Sabounchi S, Nouri M, Erfani N, Houshmand B, Khoshnevisan M. Knowledge and attitude of dental faculty members towards evidence-based dentistry in Iran. Euro J Dental Educ. 2013;17(3):127–137. doi:10.1111/eje.12019
14. Burns PB, Rohrich RJ, Chung KC. The levels of evidence and their role in evidence-based medicine. Plastic Reconstruct Surg. 2011;128(1):305. doi:10.1097/PRS.0b013e318219c171
15. Haynes RB. Of studies, syntheses, synopses, summaries, and systems: the “5S” evolution of information services for evidence-based healthcare decisions. BMJ Evidence Based Med. 2006;11(6):162–164. doi:10.1136/ebm.11.6.162-a
16. Alper BS, Haynes RB. EBHC pyramid 5.0 for accessing preappraised evidence and guidance. Evidence Based Med. 2016;21(4):123–125. doi:10.1136/ebmed-2016-110447
17. Gorgon EJR, Basco MDS, Manuel AT. Teaching evidence based practice in physical therapy in a developing country: a national survey of Philippine schools. BMC Med Educ. 2013;13(1):154. doi:10.1186/1472-6920-13-154
18. Ryan RM, Deci EL. Self-determination theory and the facilitation of intrinsic motivation, social development, and well-being. Am Psychologist. 2000;55(1):68–78. doi:10.1037/0003-066X.55.1.68
19. Leary S, Cook N, Kang J. Overview of statistics teaching within undergraduate programmes in UK and Ireland dental schools. Br Dent J. 2025;238(4):265–270. doi:10.1038/s41415-024-8232-8
20. Stanley JL, Hanson CL, Ness CJV, Holt L. Assessing evidence-based practice knowledge, attitudes, access and confidence among dental hygiene educators. Ame Dental Hygienists’ Assoc. 2015;89(5):321–329.
21. Tilson JK, Kaplan SL, Harris JL, et al. Sicily statement on classification and development of evidence-based practice learning assessment tools. BMC Med Educ. 2011;11(1). doi:10.1186/1472-6920-11-78
22. Feres MFN, Roscoe MG, Job SA, Mamani JB, Canto GDL, Flores-Mir C. Barriers involved in the application of evidence-based dentistry principles: a systematic review. J Ame Dental Assoc. 2020;151(1):16–25.e16. doi:10.1016/j.adaj.2019.08.011
23. Worthington HV, Glenny A-M, Clarkson JE. Twenty years of the cochrane collaboration. J Dent Res. 2013;92(8):680–681. doi:10.1177/0022034513491116
24. Young T, Esterhuizen TM, Volmink J, Clarke M. Attitude and confidence of undergraduate medical programme educators to practice and teach evidence-based healthcare: a cross-sectional survey. JBI Evid Implement. 2016;14(2):74. doi:10.1097/XEB.0000000000000068
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.