Back to Journals » Journal of Healthcare Leadership » Volume 18
Leadership Perspectives on Criteria-Based Dispatch and Prehospital Triage in Thailand’s Emergency Medical Services: A 10-Year National Trend Analysis and Policy Implications
Authors Kongwitseranee P ![]() , Rojsaengroeng R
, Rojsaengroeng R ![]() , Sri-On J, Piyachan P, Huabbangyang T
, Sri-On J, Piyachan P, Huabbangyang T ![]() , Thepmanee D, Chansomboon P
, Thepmanee D, Chansomboon P ![]() , Buaprasert P
, Buaprasert P ![]()
Received 20 February 2026
Accepted for publication 19 May 2026
Published 29 June 2026 Volume 2026:18 604314
DOI https://doi.org/10.2147/JHL.S604314
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Pavani Rangachari
Ponlakrit Kongwitseranee,1 Rapeeporn Rojsaengroeng,1 Jiraporn Sri-On,1 Pacharee Piyachan,1 Thongpitak Huabbangyang,2 Duangpon Thepmanee,2 Pit Chansomboon,3 Phudit Buaprasert,4
1Department of Emergency Medicine, Faculty of Medicine Vajira Hospital, Navamindradhiraj University, Bangkok, Thailand; 2Department of Disaster and Emergency Medical Operation, Faculty of Science and Health Technology, Navamindradhiraj University, Bangkok, Thailand; 3Department of Emergency Medicine, Udonthani Hospital, Mueang, Udonthani Province, Thailand; 4Department of Emergency Medicine, Emory University School of Medicine, Atlanta, GA, USA
Correspondence: Rapeeporn Rojsaengroeng, Email [email protected]
Introduction: Criteria-Based Dispatch (CBD) is Thailand’s national telephone-based prehospital triage system used to prioritize emergency response and allocate resources. However, long-term national trends in CBD utilization and their implications for healthcare leadership remain limited.
Purpose: This study aimed to analyze 10-year trends in CBD utilization in Thailand (2012– 2022), focusing on overall patterns, age groups, and geographic variations to inform policy and EMS planning.
Methods: This retrospective descriptive study analyzed 14,763,882 emergency calls recorded in the national EMS database. Trend analyses were conducted to assess temporal changes across CBD categories, demographic subgroups, and regions.
Results: Of 14,758,415 eligible calls, CBD 25 (motor vehicle accident) was the most common category (23.6%) and showed a significant increasing trend with seasonal peaks during the New Year period (p < 0.001). Adults aged 18– 59 years accounted for the largest proportion of calls (52.4%), with CBD 25 predominating (31.5%). Among older adults (≥ 60 years), CBD 17 (sick [unknown]/other) was most frequent (33.3%). Regionally, the Northeast had the highest call volume (46.7%), where CBD 17 predominated, while CBD 25 was most common in other regions.
Conclusion: These findings describe important variations in EMS demand across population groups and regions and may inform workforce planning, resource allocation, and targeted prevention strategies.
Keywords: emergency medical services, triage, emergency medical dispatch, criteria-based dispatch, emergency care policy
Introduction
The Emergency Medical Act B.E. 2551 2008,1 represents a landmark policy framework that governs emergency medical operations and ensures equitable access to emergency care in Thailand. Under Section 28,1 operational units, hospitals, and healthcare providers are required to assess and prioritize patients based on clinical severity. In the prehospital setting, this prioritization depends on effective emergency dispatch and triage systems, which are essential for guiding timely response, optimizing resource allocation, and supporting coordinated care delivery. These processes reflect key leadership responsibilities in emergency medical services (EMS), including decision-making under uncertainty, strategic management, and system governance.
Globally, emergency dispatch systems are broadly classified into two models: the Medical Priority Dispatch System (MPDS), which follows standardized scripted protocols, and the Criteria-Based Dispatch (CBD) system, which integrates structured criteria with dispatcher experience and clinical judgment.2 In the Thai EMS system, CBD is the standardized symptom-based telephone triage framework used through the national EMS hotline (1669) to prioritize emergency response and allocate resources according to patient urgency. MPDS has been widely implemented as a universal standard in many high-income countries to improve consistency, quality, and patient safety.3,4 In contrast, Thailand has adopted the CBD model, which was initially piloted in selected provinces in 2009 and later expanded nationwide.5 This model reflects the need for adaptable and context-specific approaches in low- and middle-income countries (LMICs), where variations in workforce capacity, infrastructure, and resource availability require flexible yet structured decision-support systems.
To strengthen national EMS governance and enhance accountability, the National Institute for Emergency Medicine (NIEM) developed the Information Technology for Emergency Medical System (ITEMS) database, enabling centralized and computerized data collection across the country. This system, currently known as ITEMS 4.0, has served as the national standard since 2013 and supports performance monitoring, quality improvement, and evidence-based policy development.5 The integration of digital health infrastructure into emergency systems is increasingly recognized as a strategic leadership priority, particularly in LMICs, where data-driven decision-making can reduce disparities in access to care and improve system resilience.
Within the Thai EMS system, CBD functions as a telephone-based prehospital triage approach that classifies patients into five levels of emergency (red, yellow, green, white, and black) to ensure that critically ill patients receive priority care.1,5 In addition, patients are categorized into 25 CBD groups according to their presenting symptoms, which helps identify potential life-threatening conditions and supports early clinical and operational decision-making.5,6 This structured framework facilitates interdisciplinary coordination among dispatchers, EMS providers, emergency physicians, and hospital administrators, thereby enhancing communication and system preparedness.
Despite the growing importance of dispatch systems in emergency care, most international research has focused on MPDS implementation in high-income settings, while evidence regarding CBD systems remains limited, particularly in LMIC contexts.7,8 Challenges in these settings include workforce shortages, geographic disparities, variability in training and protocol adherence, and increasing EMS demand due to demographic and epidemiological transitions. Thailand is experiencing rapid population aging and rising prevalence of noncommunicable diseases, which are expected to increase emergency service utilization and complexity. These trends highlight the need for healthcare leaders to adopt data-driven and system-oriented approaches to improve service delivery and resource prioritization.
A previous national study by Thepmanee et al9 analyzed more than 8 million emergency call records between 2016 and 2020, focusing primarily on the causes of emergency calls and temporal variations. However, long-term national evidence examining trends in the utilization of CBD categories, as well as their implications for healthcare leadership, strategic planning, and policy development, remains limited. Understanding these trends is important for strengthening emergency preparedness, improving workforce planning, and supporting injury prevention and chronic disease management strategies.
Therefore, this study analyzed 10-year trends in the utilization of CBD categories in Thailand from 2012, the first year of data availability in the ITEMS database, to 2022. By examining variations over time, across age groups, and between geographic regions, this study aimed to provide national descriptive evidence to support healthcare leadership, EMS policy, and strategic system planning.
Methods
Study Design
This retrospective descriptive study analyzed emergency call data recorded through the Thai national EMS dispatch system (hotline 1669) from January 1, 2012 to December 31, 2022. The study was designed to generate system-level evidence to support healthcare leadership, strategic planning, and policy development in emergency care delivery.
Data were obtained in electronic format from two main national sources: the Bangkok Emergency Medical Service Center, which manages emergency calls originating from Bangkok, and the NIEM, which oversees dispatch data from all other provinces. Access to these national EMS dispatch data was granted through formal institutional approval and data-sharing authorization for research purposes. These databases represent the centralized national EMS information infrastructure and are routinely used for service monitoring, performance evaluation, and quality improvement.
The use of large-scale national data provides an opportunity to examine long-term trends in emergency demand and dispatch patterns. Such insights are critical for healthcare leaders to inform workforce planning, resource allocation, regional service development, and system resilience, particularly in the context of increasing EMS demand and evolving population health needs.
Study Population
A total of 14,763,882 emergency call records were initially identified from the national EMS dispatch databases during the study period. To ensure data quality and reliability for system-level analysis, records with missing information on the CBD category or date of the event were excluded from the overall analysis, resulting in 14,758,415 eligible calls. For subgroup analyses, records with missing information on patient age group were excluded from the age-group analysis, while records with missing information on geographic region were excluded from the regional analysis. Thus, records with missing data were excluded only from the relevant analysis.
The use of comprehensive national EMS data provides a robust foundation for understanding patterns of emergency demand and dispatch utilization. Ensuring data completeness and accuracy is essential for supporting healthcare leadership, strengthening system governance, and promoting evidence-based decision-making. High-quality data are particularly important in low- and middle-income country settings, where resource constraints require effective prioritization and strategic planning to optimize emergency care delivery.
CBD Categories
In Thailand, the CBD system provides a structured and standardized framework for symptom-based triage during emergency calls. Each emergency call to the national EMS hotline (1669) is assessed in real time by trained EMS dispatch personnel using standardized National Institute for Emergency Medicine (NIEM) criteria-based dispatch protocols. CBD category assignment is based on callers’ reported symptoms and clinical information obtained during the call, rather than through automated chatbot or artificial intelligence systems. This process supports clinical prioritization, operational coordination, and efficient resource allocation within the EMS network.
The CBD system consists of 25 symptom-based categories that reflect common medical and trauma-related emergencies encountered in the prehospital setting. These categories facilitate communication between dispatchers and EMS providers, promote data standardization, and support national monitoring of EMS utilization and performance. From a healthcare leadership perspective, the use of standardized dispatch criteria enables system benchmarking, quality improvement, workforce planning, and evidence-based policy development.
For the present study, CBD categories recorded in the national EMS database were used to analyze long-term trends in emergency call utilization. The definitions of these categories are summarized in Table 1.
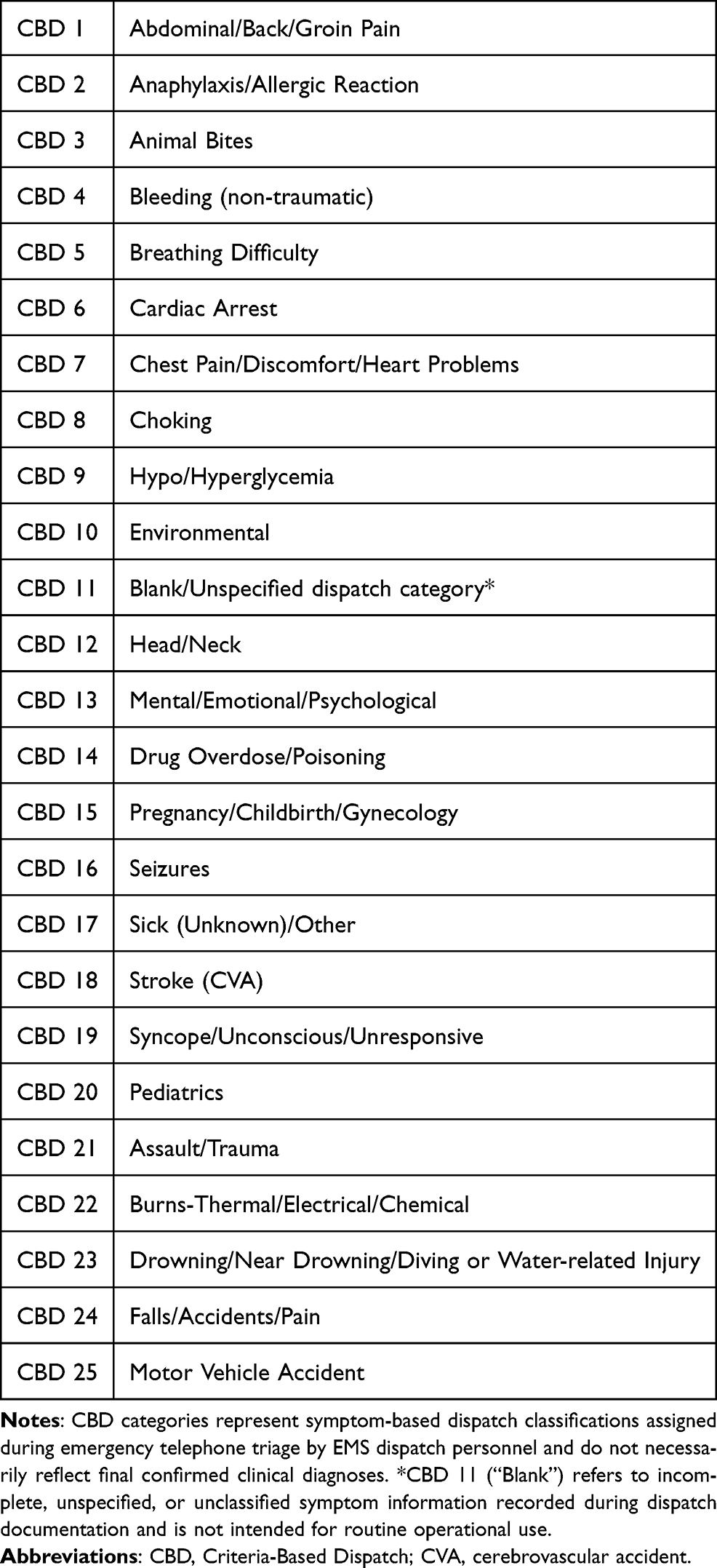 |
Table 1 Description of the 25 CBD Categories Used in Thailand’s Dispatching System |
Statistical Analysis
Demographic characteristics and emergency call profiles were described using frequencies and percentages for categorical variables. Monthly counts of emergency calls were summarized for each CBD category over the study period from 2012 to 2022, with particular focus on the five most frequently utilized CBD categories, in order to identify priority areas for EMS planning and resource allocation.
Long-term temporal trends in annual emergency call counts and category-specific proportions were assessed using linear regression models, with calendar year entered as a continuous independent variable to evaluate temporal changes over time. Trend analyses were based on absolute call volumes and proportions derived from the national EMS dispatch database and were not adjusted for population growth or demographic changes during the study period. This approach enabled the assessment of changes in EMS demand over time and supported data-driven insights for healthcare leadership and strategic system planning.
Seasonal patterns were examined using seasonal decomposition of monthly time-series data to assess recurrent temporal trends and periodic fluctuations in call volumes. Formal hypothesis testing was performed to detect significant seasonal variation. Understanding these seasonal trends is essential for improving emergency preparedness, workforce planning, and operational resilience.
Results are presented as total annual counts of emergency calls, along with corresponding p-values for trend and seasonality. All p-values were two-sided, and statistical significance was defined as p < 0.05. Statistical analyses were performed using Stata version 19.5 (StataCorp, College Station, TX, USA).
Results
Characteristics of Emergency Calls
A total of 14,763,882 emergency calls were recorded during the study period. Of these, 14,758,415 calls had complete information on the CBD category and the date of the event and were included in the overall analysis. The annual number of emergency calls increased significantly from 1,036,936 in 2012 to 1,481,629 in 2022 (p for trend = 0.001; Table 2).
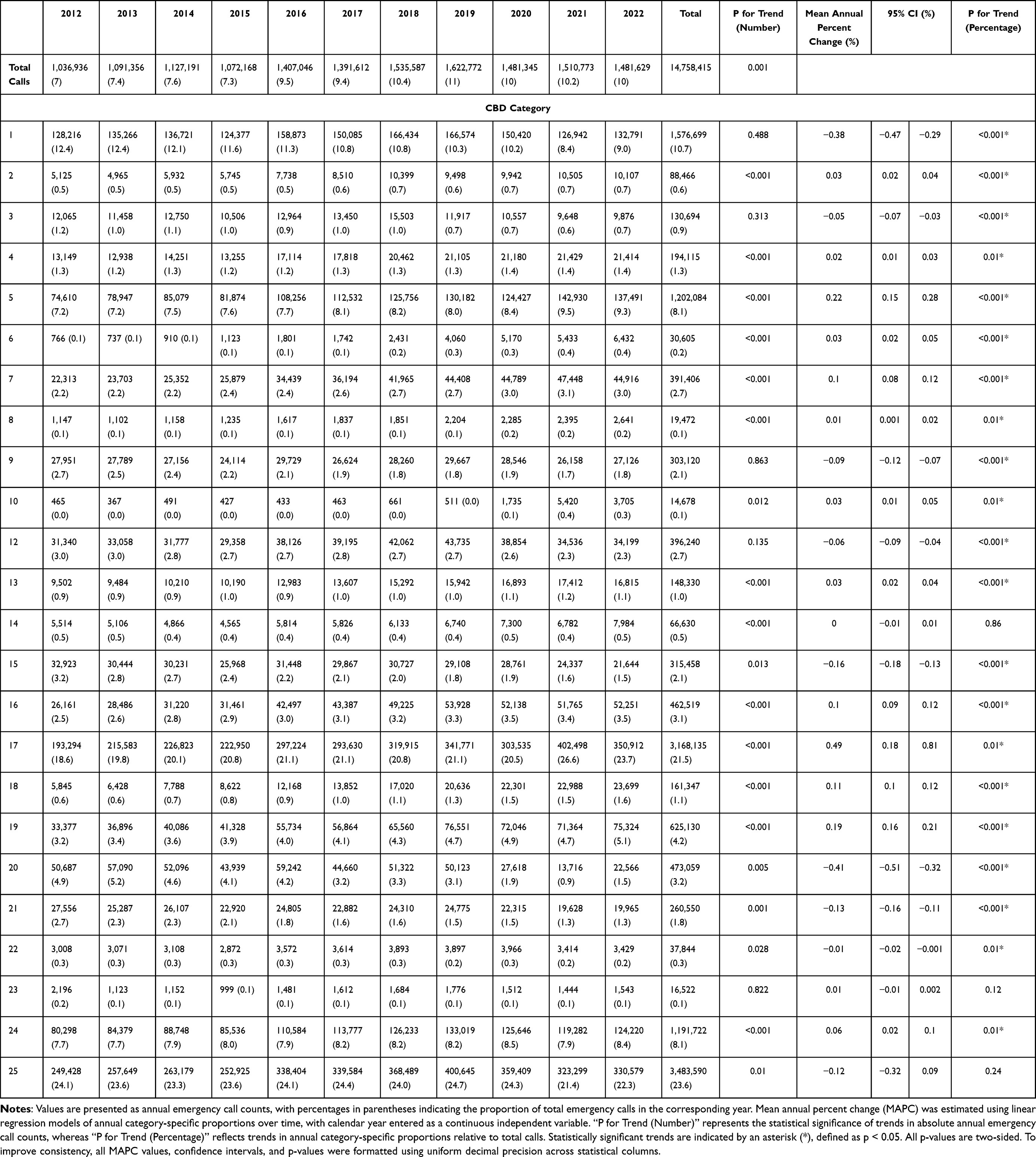 |
Table 2 Distribution of Total Emergency Calls by CBD Categories From 2012 to 2022 with Long-Term Trend Analyses |
For subgroup analyses, 13,982,898 calls with complete data on the CBD category and patient age group were included in the age-group analysis. Additionally, 14,758,415 calls with complete data on the CBD category, event date, and geographic region were included in the regional analysis. These percentages are presented based on the relevant analysis dataset.
CBD Categories with the Most Frequent Emergency Calls
The five most frequently utilized CBD categories in the overall analysis dataset were CBD 25 (Motor Vehicle Accident) (3,483,590 calls, 23.6%), CBD 17 (Sick [Unknown]/Other) (3,168,135 calls, 21.5%), CBD 1 (Abdominal/Back/Groin Pain) (1,576,699 calls, 10.7%), CBD 5 (Breathing Difficulty) (1,202,084 calls, 8.2%), and CBD 24 (Falls/Accidents/Pain) (1,191,722 calls, 8.1%). The overall number of calls is presented in Table 2, and annual call volumes are shown in Figure 1.
 |
Figure 1 Annual number of emergency calls by the five most frequently utilized CBD categories in Thailand, 2012–2022. This figure presents annual emergency call volumes for the five most frequently utilized Criteria-Based Dispatch (CBD) categories recorded in the national EMS dispatch database from 2012 to 2022. CBD 25 (Motor Vehicle Accident) and CBD 17 (Sick [Unknown]/Other) consistently accounted for the highest annual call volumes. |
Among these categories, CBD 25 and CBD 17 had the highest monthly call volumes, with approximately 26,390 and 24,001 calls per month, respectively. From 2012 to 2022, the annual number of calls increased significantly for both CBD 25 (249,428 to 330,579 calls; p for trend = 0.043) and CBD 17 (193,294 to 350,912 calls; p for trend < 0.001).
When annual category-specific proportions were analyzed using linear regression models, only CBD 17 showed a statistically significant increase over time (18.6% to 23.7%; mean annual percent change = 0.49, 95% CI 0.18 to 0.81), whereas CBD 25 showed no statistically significant proportional change (24.1% to 22.3%; mean annual percent change = −0.12, 95% CI −0.32 to 0.09).
Seasonal trend analysis demonstrated significant temporal variation in monthly call volumes across all five most frequently utilized CBD categories, with pronounced peaks during the New Year festival period compared with other times of the year (p < 0.001 for all categories; Figure 2).
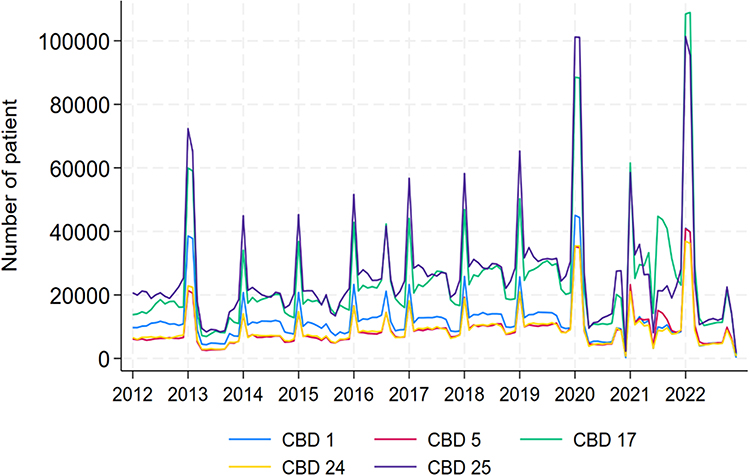 |
Figure 2 Seasonal patterns of monthly emergency call volumes for the five most frequently utilized CBD categories, 2012–2022. This figure presents absolute monthly emergency call counts for the five most frequently utilized CBD categories from January 2012 to December 2022. Seasonal patterns were analyzed using monthly time-series data. Pronounced peaks were observed during the New Year festival period across all five categories. |
Age Group Analysis
Patients were classified into three age groups: children and adolescents (≤18 years), adults (18–59 years), and older adults (≥60 years).10 Among the age-group analysis dataset, adults accounted for the highest proportion of emergency calls (7,320,875 calls, 52.3%), followed by older adults (4,819,247 calls, 34.5%), and children/adolescents (1,842,776 calls, 13.2%).
The most frequently utilized CBD category among children/adolescents and adults was CBD 25 (Motor Vehicle Accident), accounting for 580,728 calls (31.5%) and 2,385,384 calls (32.6%), respectively. In contrast, CBD 17 (Sick [Unknown]/Other) was the most common category among older adults, accounting for 1,605,963 calls (33.3%). Detailed age-specific distributions are presented in Figure 3 and Supplementary Material Table 1.
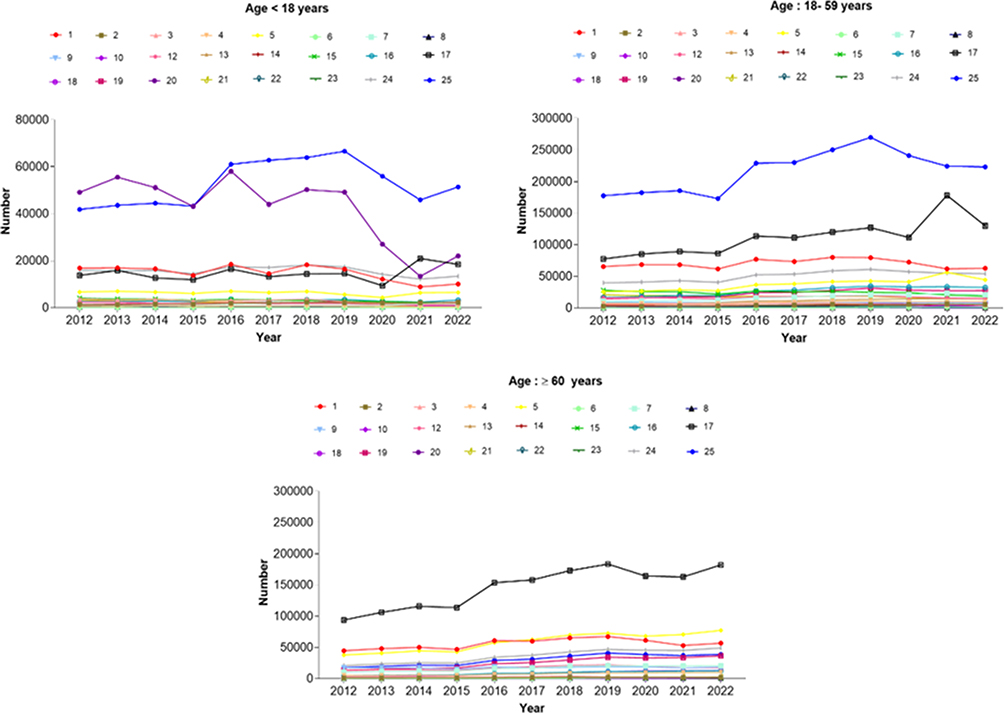 |
Figure 3 Annual emergency call trends by age group and CBD category, 2012–2022. This figure presents age-stratified annual emergency call distributions for the most frequently utilized CBD categories. Age groups were categorized as children and adolescents (≤18 years), adults (18–59 years), and older adults (≥60 years), based on prior demographic and EMS-related literature.10 |
Long-term trend analyses of annual emergency call counts stratified by age group from 2012 to 2022 showed statistically significant increases among adults (289,956 to 546,861 calls; p for trend = 0.001) and older adults (44,419 to 92,319 calls; p for trend < 0.001), whereas no statistically significant change was observed among children and adolescents (167,357 to 142,066 calls; p for trend = 0.207). Detailed age-stratified trend analyses are presented in Supplementary Material Tables 2–4.
Geographic Region Analysis
Thailand was categorized into six geographic regions: Central, North, Northeast, Eastern, Western, and South.11 In the regional analysis dataset, the Northeast region accounted for the highest volume of emergency calls (6,885,828 calls, 46.7%), whereas the Western region had the lowest volume (546,146 calls, 3.7%).
CBD 25 (Motor Vehicle Accident) was the most frequently utilized category in the Central, North, Eastern, Western, and Southern regions. In contrast, CBD 17 (Sick [Unknown]/Other) was the most common category in the Northeast region, accounting for 1,734,890 calls (25.2%). Detailed region-specific distributions are presented in Figure 4 and Supplementary Material Table 5.
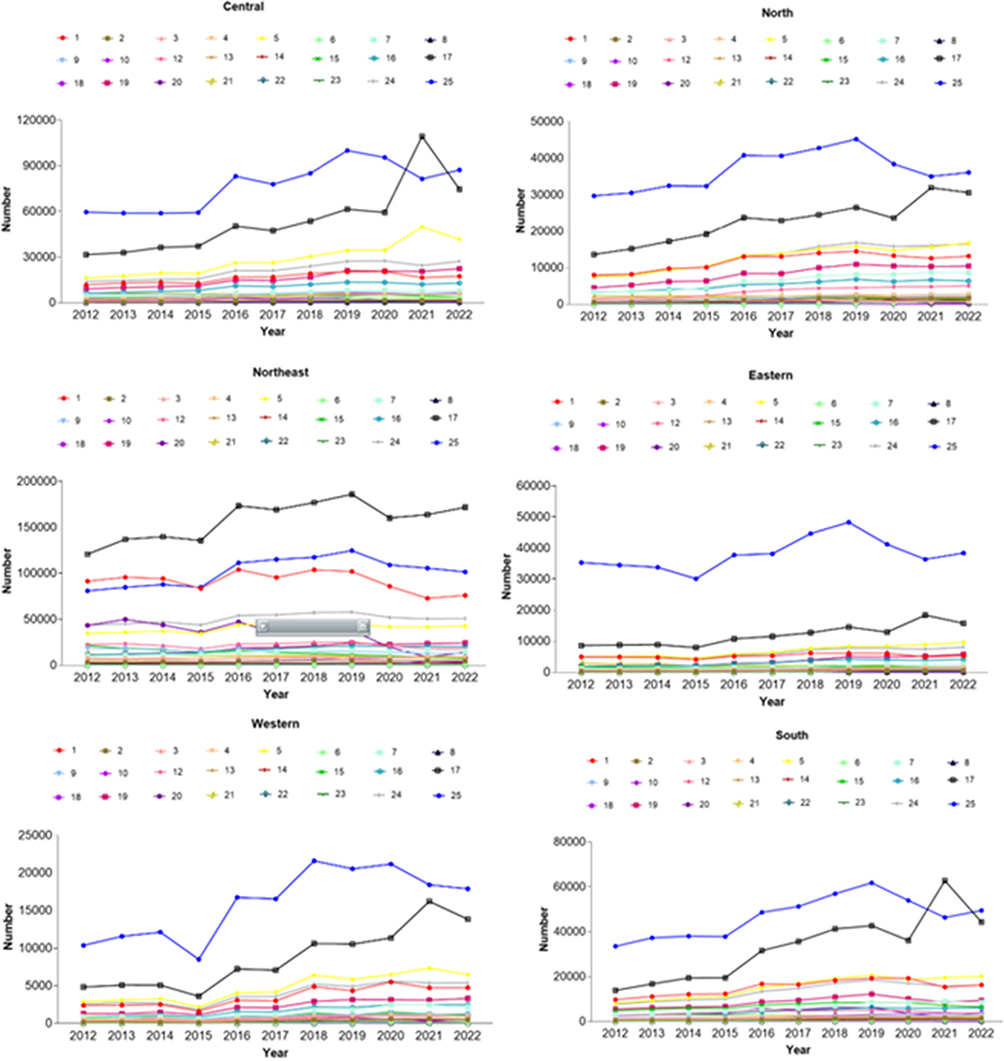 |
Figure 4 Regional distribution of emergency call volumes by CBD category in Thailand, 2012–2022. This figure presents regional trends in emergency call volumes for the most frequently utilized CBD categories across Thailand. Geographic regions were defined according to Thailand’s standard six-region administrative classification used in national health system analyses.11 |
Long-term trend analyses of annual emergency call counts stratified by geographic region from 2012 to 2022 showed statistically significant increases across all regions (p for trend = 0.001 in the Eastern region and p for trend < 0.001 in all other regions). Detailed region-stratified trend analyses are presented in Supplementary Material Tables 5–11.
Discussion
This study analyzed 14,758,415 emergency calls in Thailand over a 10-year period and provides comprehensive national insights into trends in the utilization of CBD categories. The findings have important implications for healthcare leadership, system governance, and policy development in EMS, particularly in LMIC settings where resource optimization and equitable access to care remain key priorities.
At the national level, CBD 25 (Motor Vehicle Accident) was consistently the most frequently utilized category. Although the absolute number of calls increased significantly over time, its proportional distribution remained relatively stable, suggesting that the observed increase was likely related to overall growth in EMS demand rather than a major shift in injury patterns. The clear seasonal peak during the New Year festival is consistent with increased traffic volume, interprovincial travel, and higher accident rates reported during this period in Thailand.12 In addition, the temporal spikes observed in monthly call volumes during peak holiday periods may reflect short-term increases in travel-related exposure, seasonal mobility, and fluctuating emergency service demand. This pattern also aligns with Thailand’s substantial road traffic injury burden and previous national EMS studies.9,13–19
The predominance of traffic-related emergencies in Thailand, an upper-middle-income country,13 differs from patterns reported in many high-income countries, where geriatric and non-specific complaints are more commonly observed in EMS dispatch systems.14–17 These differences may reflect variations in population demographics, burden of injury, injury prevention systems, healthcare accessibility, and health policy priorities.
CBD 17 (Sick [Unknown]/Other) also accounted for a substantial proportion of emergency calls and demonstrated a statistically significant increase in annual proportional trends. This pattern may reflect increasing complexity of non-specific symptom presentations, particularly among older adults and patients with chronic conditions. In addition, telephone-based triage may be influenced by limitations in symptom communication, caller uncertainty, time constraints, and variation in dispatcher interpretation. These findings underscore the importance of ongoing dispatcher training, standardized questioning protocols, and dispatch quality monitoring systems.
Age-stratified analyses showed that adults accounted for the largest proportion of emergency calls, followed by older adults, while children and adolescents represented the smallest group. Trauma-related emergencies predominated among younger populations, whereas non-specific or undifferentiated medical conditions were more common among older adults.20,21 This pattern is consistent with Thailand’s demographic transition and ongoing population aging,20 which are expected to increase EMS demand and complexity.
Regional variations in EMS utilization were also observed. The Northeast region had the highest emergency call volume, while the Western region had the lowest. These differences may reflect population distribution, socioeconomic factors, healthcare accessibility, and variation in health-seeking behavior.20 Although CBD 25 remained one of the most frequently utilized categories across all regions, the relative predominance of CBD 17 in the Northeast region may also be influenced by differences in symptom expression, health literacy, communication practices during emergency calls, and local patterns of chronic disease burden.
A health communication framework may provide a useful approach to understanding these regional differences. Effective emergency dispatch relies on clear, structured, and culturally sensitive communication between callers and dispatchers. Variations in language, cultural context, and health literacy may affect symptom description, triage accuracy, and subsequent care pathways. Healthcare leaders should consider integrating culturally adaptive communication strategies, standardized questioning techniques, and training programs that address linguistic diversity and community engagement.
From a policy and leadership perspective, this study highlights several system planning implications. First, national EMS leaders may use long-term dispatch trend data to support workforce planning, demand forecasting, and strategic ambulance deployment, particularly during predictable seasonal peaks such as the New Year festival. Second, the increasing proportion of nonspecific medical complaints, particularly among older adults and in certain regions, may support targeted dispatcher training, standardized telephone triage protocols, and improved coordination with community and chronic care services. Third, regional variations in EMS demand may help inform context-specific service planning and equitable resource allocation. Fourth, strengthening digital health infrastructure, dispatch quality monitoring systems, and data transparency may support evidence-based EMS governance and operational resilience. Recent evidence also suggests that strengthening evidence-based management through research-informed decision-making, data transparency, managerial training, economic evaluation, cost management, and digital transformation is important for sustaining effective healthcare leadership. Finally, equity-focused policies may prioritize underserved regions, aging populations, and vulnerable groups to support equitable access to emergency care. These findings may help guide future EMS performance evaluation and adaptive system planning in Thailand.
Overall, these findings provide useful national descriptive evidence on EMS demand patterns and may support data-informed leadership, policy development, and strategic planning in EMS systems. These findings may also offer insights for other LMICs facing similar challenges in emergency system development.
Future research should evaluate the relationship between dispatch patterns and patient outcomes, system efficiency, regional equity, and cost-effectiveness. In addition, implementation research is needed to assess strategies that improve dispatch accuracy, operational efficiency, and emergency care quality.
Limitations
This study has several limitations. First, emergency call records from Bangkok between 2012 and 2017 were partially incomplete due to the use of earlier paper-based data collection systems. However, given the very large national sample size and the consistency of trends observed across regions, this limitation is unlikely to substantially affect the overall findings. Nevertheless, this issue highlights the importance of strengthening digital health infrastructure and standardized data governance as key priorities for healthcare leadership in emergency systems.
Second, as a descriptive study, this analysis can identify temporal trends in emergency call utilization but cannot determine the underlying causal mechanisms. In addition, the analyses were based on absolute call counts and proportions rather than population-adjusted rates, which may affect interpretation of temporal and regional trends. Future research should explore potential drivers of increasing EMS demand, including demographic transitions, aging populations, rising chronic disease burden, improved public awareness, and expanded access to emergency services.
Third, this study was conducted within Thailand’s EMS system, and the findings may not be fully generalizable to other countries with different dispatch systems, healthcare infrastructures, and epidemiologic profiles.
Fourth, the frequently utilized CBD categories may not fully reflect patients’ true clinical conditions because of potential misclassification.21 This limitation may be related to the inability of the system to capture multiple complaints, reliance on caller-reported information, variability in dispatcher judgement, time constraints during emergency calls, and the inherent limitations of telephone-based triage, which precludes direct clinical assessment. These challenges are particularly relevant in LMIC settings and highlight the need for continuous dispatcher training, standardized questioning protocols, and the integration of decision-support technologies.
Finally, changes over time in EMS utilization behavior, public awareness, healthcare-seeking behavior, access to emergency services, and dispatch utilization practices may also have influenced call volumes. In addition, this study did not evaluate patient outcomes, clinical effectiveness, or cost-effectiveness of dispatch practices. Future research should examine the relationship between dispatch classification, patient outcomes, and resource utilization. Such evidence will be critical to guide policy development, improve quality of care, and strengthen accountability and performance monitoring in EMS systems.
Conclusion
These findings provide national descriptive evidence on EMS demand patterns in Thailand and may support data-informed leadership, policy development, and strategic planning in emergency medical services. The observed trends may help inform workforce planning, seasonal surge preparedness, region-specific service allocation, and strengthening of dispatch quality monitoring systems. The observed trends may also offer cautious contextual insights for other low- and middle-income countries with similar EMS structures and resource settings.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Ethics Approval and Consent to Participate
The study was conducted in accordance with the ethical principles outlined in the Declaration of Helsinki (1975) and its subsequent revisions. Ethical approval was obtained from the Institutional Review Board of the Faculty of Medicine Vajira Hospital, Navamindradhiraj University (COA No. 069/2567), and the Human Research Ethics Committee of the Bangkok Metropolitan Administration (Protocol No. U013hc/68_EXP). The requirement for informed consent was waived due to the retrospective design of the study and the use of de-identified secondary data. All data were analyzed anonymously to ensure the confidentiality and privacy of patients.
Acknowledgments
The authors would like to acknowledge the National Institute for Emergency Medicine and the Bangkok EMS Center for providing access to the data that supported this study. The authors also gratefully acknowledge the financial support provided by the Navamindradhiraj University Fund.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
Navamindradhiraj University Research Fund.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Royal Thai Government. Emergency Medical Act B.E. 2551 (2008). Royal Thai Government Gazette. 2008;125(39A):1–13.
2. Nicoletta V, Robitaille-Fortin M, Bélanger V, Mercier É, Harrisson J. Performance measures of the medical priority dispatch system in an urban basic life support system. Scand J Trauma Resusc Emerg Med. 2025;33(1):94. doi:10.1186/s13049-025-01410-6
3. International Academies of Emergency Dispatch. Medical priority dispatch system: emergency medical protocol [Internet]. 2025. Available from: https://www.emergencydispatch.org/what-we-do/emergency-priority-dispatch-system/medical-protocol.
4. Dong X, Ding F, Zhou S, et al. Optimizing an emergency medical dispatch system to improve prehospital diagnosis and treatment of acute coronary syndrome: nationwide retrospective study in China. J Med Internet Res. 2022;24(11):e36929. doi:10.2196/36929
5. National Institute for Emergency Medicine. Emergency Medical Triage Protocol and Criteria-Based Dispatch.
6. National Institute for Emergency Medicine. Notification of the national institute for emergency medicine: criteria for telecommunication emergency triage, B.E. 2568 (2025). Royal Thai Government Gazette. 2025;142(Special Part 193D):1–33.
7. Bohm K, Kurland L. The accuracy of medical dispatch - a systematic review. Scand J Trauma Resusc Emerg Med. 2018;26(1):94. doi:10.1186/s13049-018-0528-8
8. Baabdullah M, Faden H, Alsubhi R, Almalki A, Masri B, Alharbi A. The efficiency of the medical priority dispatch system in improving patient outcomes. Saudi J Emerge Med. 2020;1(2):110–120. doi:10.24911/SJEMed/72-1586163179
9. Thepmanee D, Tanaka H, Takyu H. Trends in pre-hospital emergency calls and transportation data for emergency medical services in Thailand. J EMS Med. 2023;2(2):45–54. doi:10.35616/jemsm.2022.00017
10. United Nations Population Fund (Thailand). Impact of Demographic Changes in Thailand. Bangkok: UNFPA; 2011.
11. Boontaeng N. Geographic regionalization [Internet]. Royal Society of Thailand; 2025. Available from: https://thaifarmer.lib.ku.ac.th/f/f6a5e2130eb93fa82212322900a09fe103853e11b33fa7830b0f072b7b4860d1.pdf.
12. Aroonsrimorakot S, Bovornkitti S. Forecasting incidence of road accidents during the 2019 New Year holiday season. Thammasat Med J. 2019;19(4):620–626.
13. World Bank. World Bank country and lending groups [Internet]. Washington (DC): World Bank Data Help Desk; 2025. Available from: https://datahelpdesk.worldbank.org/knowledgebase/articles/906519-world-bank-country-and-lending-groups.
14. Møller TP, Ersbøll AK, Tolstrup JS, et al. Why and when citizens call for emergency help: an observational study of 211,193 medical emergency calls. Scand J Trauma Resusc Emerg Med. 2015;23(1):88. doi:10.1186/s13049-015-0169-0
15. Salminen T, Kaartinen K, Palonen M, Setälä P, Paavilainen E, Hoppu S. Correlation between the accuracy of the emergency response centre’s urgency assessment and emergency medical services non-conveyance: a retrospective register-based study in Finland. BMC Emerge Med. 2024;24(1):193. doi:10.1186/s12873-024-01108-5
16. Herr D, Bhatia S, Breuer F, et al. Increasing emergency number utilisation is not driven by low-acuity calls: an observational study of 1.5 million emergency calls (2018–2021) from Berlin. BMC Med. 2023;21(1):184. doi:10.1186/s12916-023-02879-7
17. Brady M, Fivaz MC, Noblett P, Olola CHO, Scott G. Emergency communication nurse system outcomes of advanced medical priority dispatch codes in a UK ambulance service: a descriptive analysis. Ann Emerg Dispatch Response. 2024;12(1):11–18.
18. Bhattarai HK, Bhusal S, Barone-Adesi F, Hubloue I. Prehospital emergency care in low- and middle-income countries: a systematic review. Prehosp Disaster Med. 2023;38(4):495–512. doi:10.1017/S1049023X23006088
19. World Health Organization. Global Status Report on Road Safety 2018. Geneva: World Health Organization; 2018.
20. National Statistical Office. Statistical Yearbook Thailand 2023. Bangkok: National Statistical Office; 2023.
21. Bhalla MC, Wilber ST, Stiffler KA, Ondrejka JE, Gerson LW. Weakness and fatigue in older ED patients in the United States. Am J Emerg Med. 2014;32(11):1395–1398. doi:10.1016/j.ajem.2014.08.027
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Accuracy of Trauma on Scene Triage Screening Tool (Shock Index, Reverse Shock Index Glasgow Coma Scale and National Early Warning Score) to Predict the Severity of Emergency Department Triage: A Retrospective Cross-Sectional Study
Yuksen C, Angkoontassaneeyarat C, Thananupappaisal S, Laksanamapune T, Phontabtim M, Namsanor P
Open Access Emergency Medicine 2023, 15:79-91
Published Date: 21 March 2023