Back to Journals » Advances in Medical Education and Practice » Volume 11
“Turning Point”: Evaluating the Impact of a Three-Month UK-Based Clinical Education Training Programme for Physicians from a Chinese Medical School
Authors Rashid MA ![]() , Nicholson J
, Nicholson J ![]() , Fazal F, Gallivan S, Thomas D, Xu L, Gill D
, Fazal F, Gallivan S, Thomas D, Xu L, Gill D
Received 8 April 2020
Accepted for publication 29 July 2020
Published 28 August 2020 Volume 2020:11 Pages 601—607
DOI https://doi.org/10.2147/AMEP.S257384
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Mohammed A Rashid,1 John-george Nicholson,1 Faruq Fazal,1 Samantha Gallivan,1 Daphne Thomas,2 Leiting Xu,3 Deborah Gill1
1UCL Medical School, University College London, London, UK; 2UCL Centre for Language and International Education, University College London, London, UK; 3School of Medicine, Ningbo University, Ningbo, Zhejiang, People’s Republic of China
Correspondence: Mohammed A Rashid
UCL Medical School, University College London, Room GF664, Royal Free Hospital, London, UK
Tel +44 7976 829515
Email [email protected]
Purpose: Transnational faculty development programmes are increasingly popular in medicine, although evaluation of such activities rarely considers longer-term outcomes or the impact of language training. This study attempts to fill this gap by evaluating the lasting impacts of a three-month clinical education and English language training programme at University College London Medical School, UK, for medical educators from Ningbo University, China.
Methods: In-depth, semi-structured interviews were conducted in China with 41 participants who had completed the programme between 2013 and 2018. Interview data were analysed using an inductive thematic analysis, and themes were categorised using the four primary components of the faculty development model outlined by Irby and O’Sullivan (2011) – context, facilitator, programme, and participant.
Results: Contextual impacts included the importance of participants learning in the familiar environment of their own clinical discipline, the cultural enrichment gained by spending time overseas, reflecting on differences in health-care systems, and attempts to implement and disseminate learning on return to China. Facilitator-related factors included new insights into the student–educator relationship and valuing the support of programme mentors. Programme-related factors included exposure to new teaching methods and technical presentation skills, the challenges of navigating observership placements, spoken English language and pronunciation issues, and establishing a peer network of medical educators. Participant-related factors included improved confidence and self-reflection, adjusting educational approaches for different student groups, and career development in medical education.
Conclusion: Participants gained teaching confidence from their engagement in the programme and many described it as a turning point in their careers as educators. Although in the period after attending, individuals changed their own practices and influenced colleagues within their organisation, often through taking on senior roles, and systematic education changes were generally not implemented. Dedicated English language classes and clinical placements were considered the most positive features of the programme.
Keywords: international, globalisation, faculty development, clinical education, language
Introduction
Although the globalisation of medical education has contributed to improved scholarship, the formation of professional communities and the sharing of good practice,1,2 improvements in the standards of training for physicians have not been consistent around the world. In response to a call for reform,3 an increasing number of medical schools have sought to raise standards by partnering with well-established institutions4. These collaborations have varied from joint degree programmes5 to lower intensity relationships that provide advisory support,6 and have variously been labelled partnerships, networks, coalitions, alliances, consortia, task forces, joint-working, and twinning.7 Faculty development activities have been a popular feature of such international collaborations.
Evaluations of transnational faculty development programmes in developing countries have suggested that participants typically augment their knowledge and skills in education leadership, management, and methodology, and apply that knowledge at their home institutions.8 Features that have been noted to be linked to success in the faculty development elements of wider collaborations include a focus on local needs, encouraging the diffusion of ideas, and recognising the importance of personal relationships to build trust between organisations.9
China has a vast, complex medical education system, which continues to evolve and transform to meet the needs of its faculty, students and patients.10 Surveys of medical faculty members in China have demonstrated concerns about burnout and low job satisfaction levels in Chinese physicians and medical educators11 with studies describing a significant need for faculty development in medical education.12 One recent transformation that reflects a global trend in higher education, is the adoption of English as the language of tuition13 with Chinese universities developing English-language undergraduate medical programmes to accommodate an increasingly mobile student population in Asia. Faculty development courses at these institutions therefore need to address the need for medical educators to be able to teach in English alongside training in clinical teaching methods, although support in language education alongside professional training for medical educators working in such settings has yet to be explored in an in-depth way in the medical education literature.
The Ningbo University-University College London Medical School (NBU-UCLMS) Programme
The NBU-UCLMS programme involves physicians from China spending three months observing clinical teaching in the UK. The participants are physicians who have completed postgraduate training and are eligible to be appointed as senior teachers on the NBU MBBS programme, an English language medical degree at Ningbo University aimed at international students, with clinical training provided at affiliated hospitals in Ningbo. Most participants are early-career professionals in the first five years of completing clinical training, although a small minority have been mid-career.
Between October 2013 and June 2019, a total of 132 physicians, in eight cohorts have completed the UCLMS-NBU programme. The programme has evolved in response to feedback: it was shortened from four to three months as participants struggled to take leave from their clinical roles and changes were made to the content and duration of the programme from the second cohort onwards. Formal English lessons are now delivered by the UCL Centre for Languages and International Education with a reflective journal used to record new vocabulary and learning points. Although there are no formal English requirements set by UCLMS, participants are required to take English lessons in Ningbo in the months before travelling to London for the programme.
The programme includes an initial eight weeks of general medical education training combining small group work and seminars, along with observations of campus-based teaching at UCLMS and placement-based teaching at a UCLMS teaching hospital. The final 4 weeks are spent observing in clinical placements in the physicians’ own specialty. During the first eight weeks, participants are intentionally placed on attachments away from their own discipline so that they can focus on learning about medical education rather than their specialist clinical interests. During their time in London, participants are assigned a UCLMS mentor, who meets weekly with the NBU physicians for pastoral support. Participants also have a clinical supervisor in each of their two placements.
Given the paucity of evaluations that consider the long-term impacts of such faculty development programs, and particularly the lack of focus on English language training in transnational medical education faculty development, this study sought to evaluate the NBU-UCLMS programme by interviewing participants between one and six years after returning to NBU. The research questions were: what were participants’ experiences of the programme and to what extent did it influence their educational practices and careers when they returned to NBU?
A review of the empirical and theoretical literature14–16 suggested that a framework devised by O’Sullivan and Irby14 and that foregrounds the sociocultural aspects of faculty development was considered a useful lens through which to approach data generation and subsequent analysis given the research question and context described above.
Methods
Ethical Approval
This study was approved by the Research Ethics Committee at University College London (15,443/002). Written informed consent was obtained from all study participants who were recruited by the NBU senior leadership team by contacting all physicians who had participated in the programme (up to March 2019). Interviews were conducted at the NBU campus in April 2019. No incentives were given to participate in the interviews and the participants had written information sheets.
Interviews
In-depth, semi-structured interviews were jointly conducted in English by two authors (AR & JN) to ensure consistency. Although both interviewers had been involved in the development of the programme, neither are involved in the current delivery of the programme. Participants were invited to attend interviews by email, distributed by NBU administrators. An NBU academic representative, who was not part of the NBU-UCLMS project, was present during the interviews to help with English-Mandarin translations and was called upon regularly to help explain words or sentences that were challenging to understand. Mindful of both the possibility of social desirability bias and the cultural phenomenon of losing face, participants were encouraged at the start of interviews to share both positive and negative experiences and were probed further when they showed hesitancy to encourage full and candid responses to questions. No participants dropped out of the study. Interviews were conducted at the NBU medical school campus.
Data Analysis
Audio recordings and field notes during interviews were used to create annotated transcripts for each interview, which were stored and managed on Microsoft Excel. Data were analysed using an inductive thematic analysis and continued until data saturation was reached. The first step of analysis was for the authors to check the accuracy of all transcripts and to read and re-read the data to become familiar with it. Two team members analysed transcripts independently (AR and JN), noting key views, issues and themes, before agreeing a thematic index and descriptors that were then applied to the full data set and shared with the author team. This involved some expanding and collapsing of themes and the refinement of descriptors. The authors dealt with any areas of discrepancy by consensus meetings. The four primary components of faculty development that have been identified from previous theoretical work (context, facilitator, programme, participants) by Irby and O’Sullivan14 were used as a framework to categorise and synthesise themes, as described above.
Results
A total of 41 interviews were conducted, which included at least one participant from each of the eight cohorts to have completed the programme between 2013 and 2019. Participants were from a variety of clinical disciplines, including medical and surgical specialties, paediatrics, gynaecology, and radiology. After completing the NBU-UCLMS programme, all participants were involved in teaching on the NBU English-language MBBS programme.
A table of overall themes, categorised according to the four component domains of faculty development, is presented in Table 1.
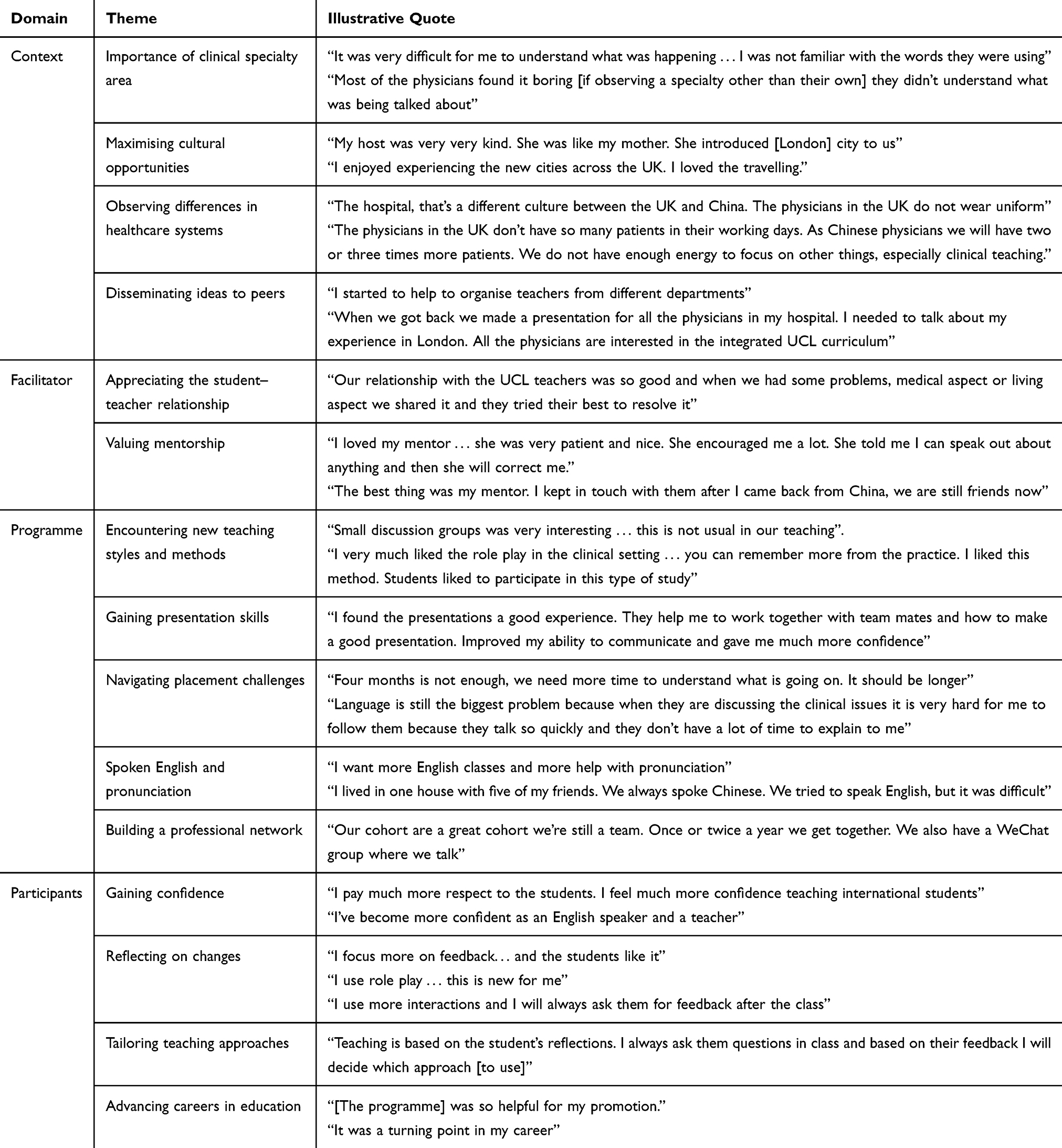 |
Table 1 Themes from Participant Interviews |
Context Factors
In this domain, themes relate to the sociocultural environment that shaped both the training programme and the period of time after participants returned to NBU.
Participants consistently highlighted the value of the clinical placements in their own learning experience. Although they found it challenging to be observers in specialties other than their own, as was the case for the first eight weeks of the programme, they mostly recognised the rationale for this decision. Some participants expressed a frustration at their perceived lack of ability to maximise the learning opportunities available through not being able to understand technical vocabulary in disciplines other than their own.
Although many physicians remarked on the person-centred care, shared decision-making, and multidisciplinary team meetings they observed, it was considered unrealistic to implement these in the Chinese context due to time pressures and cultural professional differences. Some physicians felt the Chinese system was more efficient and were unimpressed by the UK National Health Service overall, observing that Chinese physicians see more patients per clinic or day.
Almost all participants talked about the value of utilising free time during the programme to travel around the UK to historic places and visit museums and galleries in London. There was widespread recognition for the enrichment that came from these activities, both linguistically in terms of practising spoken English, but also in terms of broadening horizons and understanding different cultural traditions.
All participants described at least some level of implementing ideas they had encountered in London on their return. These included novel teaching methods, role-play, providing structured feedback, and using more interactive and case-based approaches. Participants also described teaching topics such as professionalism and cultural psychiatry that have traditionally been less of a focus in Chinese medical education. Of note, many participants talked of a phased approach to implementing ideas in the months and years after the programme, as they built up the confidence to be more experimental.
Sharing ideas with peers from China on return was challenging. Although there was some interest in the UK healthcare system, there was less interest in the practical teaching skills that were taught in London, as Chinese physicians generally consider themselves too busy to engage. Many described an inability to influence curriculum change at NBU. Although they had ideas and passion to do so, they did not have the necessary power or influence. A small number of participants stated that they had made suggestions for amendments to the curriculum, but that these had not been pursued.
Facilitator Factors
Many elements of the teacher–student relationship were important to participants, relating both to their own relationships with UCLMS facilitators, and the relationships between clinical teachers and medical students that they observed. They were influenced by the “student centred” ethos and the idea of inspiring students rather than imparting knowledge upon them. Some participants noted that they bonded with their own students differently after the programme.
Personal mentors from UCLMS were frequently discussed, universally positively. Participants liked having a named person who could be a first point of contact to offer pastoral and social support.
Programme Factors
Although participants were not always able to implement new teaching methods on returning to NBU, there was a sense that it was still useful to have observed and encountered them. Participants gained technical presentation skills and gave examples of how they had improved their use of PowerPoint, both in terms of overall structure and individual slide layout and design.
Some participants expressed that the programme was not long enough. Others, however, said it was “just right” in duration. There were some examples of challenges in clinical placements, including, a feeling of the service being too busy to provide any training, and a frustration at not having access to electronic health records. The majority of participants, though, felt the clinical placements were the single most valuable aspect of the programme.
Although a few participants felt that being in a group of 12 to 16 participants limited the amount of time speaking in English, there was a strong sense of camaraderie, and almost all participants said they were still in touch with this group. Some participants used this group as a medical educator network to exchange ideas with, whilst others said it was now simply a social engagement group.
The English language lessons, delivered by the UCL Centre for Languages and International Education, were universally popular amongst participants with their focus on academic reading and writing. Many highlighted that there was also a personal responsibility to engage with learning and practising English, but the supportive environment of the English classes was paramount.
Participant Factors
A prominent theme to emerge was that the programme helped participants increase their confidence as medical teachers and as English speakers. Linked to this was an increased awareness of reflective practice, as prompted by the completion of a reflective journal during the UCLMS programme. Many participants commented that they believe their teaching was poor prior to coming on the programme and participants now engage in seeking and responding to student feedback. Participants also felt able to tailor teaching according to student groups, for example using role-play with international medical students and not with local Chinese students, due to cultural differences to learning between the groups.
Many participants valued the exposure to novel educational resources such as simulation centres and online resources, although they noted that some internet sites for medical education are not available in China.
Although many felt that the programme was a critically important “turning point” in their lives, others said that although it had professional influence, there was minimal or no impact on their personal self. A number of participants secured new roles in education following their return from the programme varying from departmental teaching secretary roles to more senior roles, such as hospital coordinator or director for medical education. A number of participants described having pursued short courses in medical education in China and some have since won prestigious educational prizes.
Discussion
This study evaluated the impact of a three-month medical education training programme in a UK medical school on physicians from China. They described outcomes and experiences that can be categorised according to the four aspects of faculty development outlined by O’Sullivan and Irby.14
A number of features of this programme made it popular with participants. The exposure to a variety of clinical teaching methodologies was felt to be particularly important. The programme included dedicated, weekly English lessons delivered by specialists in academic English language instruction resulting in increased teaching confidence and improved perceived performance in spoken English. Previous studies on English-medium instruction in Chinese higher education also found that collaboration between subject and language specialists was critically important15 alongside a perceived need for a safe learning environment when delivering international faculty development in a non-native language.16
Many participants in this study deeply valued the time and opportunity to engage with UK history and culture, and commented on the inclusion of topics in clinical teaching that are influenced by scholarship from the medical humanities. Previous studies have suggested that the focus on science subjects from high school onwards typically experienced by Chinese physicians may reduce their opportunities to engage with the empathetic and human aspects of medical education.17
Despite the fact that all participants framed their responses favourably about the overall impact of the programme, a number of themes linked naturally to recommendations for changes to the programme. One important area was the desire to spend more time in a participant’s own specialty. Participants believed they would find it easier to understand clinical terminology that they are already familiar with. Other suggestions from this study have already been adopted, such as the centralisation of all placements to a single teaching hospital site.
Many participants have gained senior and supervisory roles in clinical education. However, there is currently no defined mechanism for this programme to make a structural difference to the NBU MBBS course, which like the majority of Chinese medical degree courses,17 adopts a traditional, disciplinary structure and not a modular, systems-based approach. Given that participants highlighted that the ability to influence medical school leaders was needed to realise structural changes, a parallel training programme focused on leadership may be of benefit, if developed by NBU staff as to reflect a local cultural understanding of hierarchy and respect in the medical workplace.
Strengths and Weaknesses
An important limitation of this work is that participants were not conversing in their primary language and may have therefore been unable to provide nuanced insights into their experiences, although this effect was minimised by the availability (and regular use) as a translator of a Mandarin-speaking NBU member of staff. A strength of the work is the variety of backgrounds of the research team, including clinician educators with formal medical education training (MAR, FF, SG, LX, DG), a language education specialist (DT), and a higher education professional services specialist (JN). It also included perspectives from those in leadership roles at the respective institutions (LX and DG) as well as more junior team members.
The findings from this study were consistent with other studies on faculty development, both from this world region, and more broadly across the globe. A significant sample of total participants in the programme took part in this study with representatives from each cohort of participants interviewed. Despite the evolution of the programme, persistent themes were identified across all years suggesting some stability in the experiences and observations of the participants.
Conclusion
This study demonstrates that a three-month London-based medical education training programme helped physicians from China to implement new clinical teaching methodologies into their roles teaching on an English-language undergraduate medical course, and was often a turning point in their medical education careers. Language training has not been previously evaluated in the context of medical education faculty development, and formal English lessons were perceived to be critically important to the success of this programme. Some more unexpected consequences of the programme included cultural enrichment, especially linked to travelling around the UK, and the importance of the network of professionals in each cohort, which still remain active many years after the programme. Influencing medical school leadership teams and prompting changes at course and curriculum level was not achieved, although this was not an explicit aim of the programme. This programme and study could help faculty developers engaged in planning activities across two divergent cultures and particularly, those that have a focus on improving linguistic as well as educational competence.
Acknowledgment
UCL Medical School has a consultancy agreement with Ningbo Medical School to provide faculty development support programmes.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Prideaux D. The global–local tension in medical education: turning ‘think global, act local’ on its head? Med Edu. 2019;53(1):25–31. doi:10.1111/medu.13630
2. van der Vleuten CP. Medical education research: a vibrant community of research and education practice. Med Edu. 2014;48(8):761–767. doi:10.1111/medu.12508
3. Frenk J, Chen L, Bhutta ZA, et al. Health professionals for a new century: transforming education to strengthen health systems in an interdependent world. lancet. 2010;376(9756):1923–1958. doi:10.1016/S0140-6736(10)61854-5
4. Kolars JC, Cahill K, Donkor P, et al. Perspective: partnering for medical education in Sub-Saharan Africa: seeking the evidence for effective collaborations. Acad Med. 2012;87(2):216–220. doi:10.1097/ACM.0b013e31823ede39
5. Williams RS, Casey PJ, Kamei RK, et al. A global partnership in medical education between Duke University and the National University of Singapore. Acad Med. 2008;83(2):122–127. doi:10.1097/ACM.0b013e318160b8bc
6. Sherer R, Dong H, Yunfeng Z, et al. Medical education reform in Wuhan University, China: a preliminary report of an international collaboration. Teach Learn Med. 2013;25(2):148–154. doi:10.1080/10401334.2013.770745
7. Friedman S, Cilliers F, Tekian A, Norcini J. International faculty development partnerships. In: Faculty Development in the Health Professions. Dordrecht: Springer; 2014:311–329.
8. Burdick WP, Diserens D, Friedman SR, et al. Measuring the effects of an international health professions faculty development fellowship: the FAIMER institute. Med Teach. 2010;32(5):414–421. doi:10.3109/01421590903394587
9. Burdick WP. Global faculty development: lessons learned from the foundation for advancement of international medical education and research (FAIMER) initiatives. Acad Med. 2014;89(8):1097–1099. doi:10.1097/ACM.0000000000000377
10. Hou J, Michaud C, Li Z, et al. Transformation of the education of health professionals in China: progress and challenges. Lancet. 2014;384(9945):819–827. doi:10.1016/S0140-6736(14)61307-6
11. Lo D, Wu F, Chan M, Chu R, Li D. A systematic review of burnout among doctors in China: a cultural perspective. Asia Pac Fam Med. 2018;17(1):3. doi:10.1186/s12930-018-0040-3
12. Guo Y, Sippola E, Feng X, et al. International medical school faculty development: the results of a needs assessment survey among medical educators in China. Adv Health Sci Educ. 2009;14(1):91–102. doi:10.1007/s10459-007-9093-z
13. Yuan R, Li S, Neither YB. “local” nor “global”: chinese university students’ identity paradoxes in the internationalization of higher education. High Educ. 2018;
14. O’sullivan PS, Irby DM. Reframing research on faculty development. Acad Med. 2011;86(4):421–428. doi:10.1097/ACM.0b013e31820dc058
15. Plack MM, Goldman EF, Wesner M, Manikoth N, Haywood Y. How learning transfers: a study of how graduates of a faculty education fellowship influenced the behaviors and practices of their peers and organizations. Acad Med. 2015;90(3):372–378. doi:10.1097/ACM.0000000000000440
16. Kim DH, Lee JH, Park J, Shin JS. Process-oriented evaluation of an international faculty development program for Asian developing countries: a qualitative study. BMC Med Educ. 2017;17(1):260. doi:10.1186/s12909-017-1101-2
17. Jiang L, Zhang LJ, May S. Implementing english-medium instruction (EMI) in China: teachers’ practices and perceptions, and students’ learning motivation and needs. Int J Biling Educ Biling. 2019;22(2):107–119. doi:10.1080/13670050.2016.1231166
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.