Back to Journals » International Journal of General Medicine » Volume 16
Late Diagnosis in HIV with New and Old Definitions; Data from a Regional Hospital in Turkey
Authors Candevir A ![]() , Kuscu F, Kurtaran B, Kömür S, İnal AS, Ertürk D
, Kuscu F, Kurtaran B, Kömür S, İnal AS, Ertürk D ![]() , Taşova Y
, Taşova Y
Received 22 June 2023
Accepted for publication 12 September 2023
Published 18 September 2023 Volume 2023:16 Pages 4227—4234
DOI https://doi.org/10.2147/IJGM.S424561
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Aslıhan Candevir,1 Ferit Kuscu,1 Behice Kurtaran,1 Süheyla Kömür,1 Ayşe Seza İnal,1 Damla Ertürk,2 Yeşim Taşova1
1Infectious Diseases, Çukurova University, Adana, Türkiye; 2Infectious Diseases, Health Sciences University Izmir Tepecik Education and Research Hospital, İzmir, Türkiye
Correspondence: Aslıhan Candevir, Infectious Diseases Department, Çukurova University Medical School, Adana, Türkiye, Tel +90 5335775954, Email [email protected]
Background: Late presentation for HIV care, continues to be a challenge, leading to increased morbidity, mortality, and society costs. The study aimed to determine the rates of late diagnosis (LD) and patient characteristics in Turkey, utilizing the new definition excluding recently infected.
Methods: The study included patients admitted to the hospital between 1998 and 2023, with at least 1 year of follow-up. Patients without a CD4 count at their initial admission were excluded. Two definitions of presentation were used: LD, (CD4< 350 cells/mL or AIDS-defining event) and advanced disease (AD), (CD4< 200 cells/mL or AIDS-defining event). Individuals with recent evidence of infection were reclassified as “not late”.
Results: Out of the 914 patients meeting the criteria and the analysis focused on 794 treatment-naïve patients, with 90.6% being male and an average age of 36.0 ± 12.0 years. Using the previous definition, 48.9% were diagnosed as late, while the new definition identified 47.2%. A total of 183 patients (23%) were diagnosed with AD, and 25.9% of the diagnoses occurred during the COVID-19 Pandemic. The rate of LD increased during the pandemic compared to before (55.8% vs 44.2%, p=0.005), as did the rate of AD (30.1% vs 20.6%, p=0.007). There was no significant relationship between gender and LD. Patients with LD were older (median ages were 31 vs 36 in groups, p< 0.001), had poorer virological response, higher mortality rates (4.8% vs 1.2%, p=0.003), and shorter survival compared to those without (log rank=0.004).
Conclusion: HIV patients with LD have poorer prognosis with older age as well as disruption of health services during the pandemic as risk factors. To improve outcomes, multicenter studies should investigate missed opportunities and specific risk factors in our region, and we should screen at-risk populations, promote awareness among underdiagnosed populations, and advocate testing even in disastrous situations.
Plain Language Summary: Late diagnosis of HIV remains a challenge, leading to increased health problems, deaths, and societal costs. This study aimed to determine the rates of late diagnosis and patient characteristics in Turkey, using a new definition that excludes recently infected individuals. The study included 794 treatment-naïve patients, mostly male with an average age of 36 years. With the new definition, 47.2% were diagnosed late, and 23% had advanced disease. The pandemic period saw higher rates of late diagnosis (55.8% vs 44.2%) and advanced disease (30.1% vs 20.6%). Gender did not significantly affect late diagnosis. Patients with late diagnosis were older, had lower CD4 counts, poorer treatment response, higher mortality rates (4.8% vs 1.2%), and shorter survival. Older age and disruptions in healthcare during the pandemic were identified as risk factors for late diagnosis. To improve outcomes, multicenter studies should investigate missed opportunities and specific risk factors, while focusing on screening high-risk populations, raising awareness among underdiagnosed groups, and promoting testing even during challenging situations.
Keywords: human immunodeficiency virus, HIV, late diagnosis, new definition, risk factors
Introduction
More than 75 million people have been infected with HIV, and an estimated 37 million people are presently living with the virus. Globally, HIV infection is among the leading causes of morbidity and mortality.1 In Europe, roughly one-third of people who are HIV positive do not seek medical attention until a late stage in the course of their infection. In spite of efforts made to raise awareness about the importance of early HIV testing, the current state of affairs has remained unchanged for a number of years with little signs of improvement. A delayed presentation for treatment is not only hurtful to the person who is infected but also more expensive. Also, the spread of HIV is detrimental to society due to its impact on health, economy, stigma, loss of human capital, families, and communities, straining public health systems, and disrupting global health dynamics. Therefore, surveillance is crucial to determine the extent to which late presentation is occurring. The probability of getting an AIDS-defining illness increases exponentially in HIV-infected people who are not receiving treatment; the risk is particularly significant in those with a CD4 cell count of 200 cells/mL. Delaying therapy for a longer period of time results in a poorer outcome for the patient.2
There are over twenty distinct definitions of late presentation in the literature. Late presentation of HIV was defined in a 2010 consensus statement as “presenting with a CD4 count of 350 cells/L or with an AIDS-defining event”. This definition has been accepted by the World Health Organization (WHO) and the European Centre for Disease Prevention and Control (ECDC) and for more than a decade.2
HIV testing has been more widespread and frequent in various communities in Europe and areas in recent years as part of pre-exposure prophylaxis (PrEP) programs, resulting in a rise in the number of people diagnosed with HIV, notably men who have sex with men (MSM). According to the current definition of late HIV presentation, these people are wrongly classified as late because of their low CD4 counts at the time of acute HIV infection.3 This possible overestimation issue has been raised by some research groups and has led to the application of correction factors to the late diagnosis rates. The amount of these adjustment factors varies depending on the reclassification criteria, country, population, and study era, but in Belgium it has been estimated to be as high as 9%.4–6
As a result, a working committee formed as part of the EuroTEST Initiative and supported by the ECDC, the WHO Regional Office for Europe, and the European AIDS Clinical Society (EACS) resolved to reassess this criterion. After reviewing the data to make a better distinction to between people with a LD and people who have recently acquired HIV, persons with recent evidence of infection (ie diagnosed at the time of seroconversion) would be reclassified as “not late”. Some Western European countries reported adjusted national late HIV diagnosis rates for recent infection. The extent of these adjustments varies by country and subpopulation.7
The reclassification of newly infected persons can contribute to the reduction of an overestimation of the late HIV diagnosis estimates, as well as the improved identification of groups who are at risk for poor HIV outcomes and intervention areas in order to further expand and focus HIV testing.
There is very limited data on the epidemiology of LD in Turkey and no data with the new definition excluding recently infected people. In this study, it was planned to determine the LD rates and patient characteristics of patients admitted to our hospital, which is a regional HIV center.
Methods
From 1998 to 2023, patients who admitted to the outpatient clinic of Çukurova University Medical School Hospital in Adana, Turkey and who were followed up for at least 1 year were included in the study. Patients who did not have a CD4 count at their first admission were excluded from the study. The data collection form was filled out by analyzing the electronic data system and written documents of the patients. The data collection form included demographic data, diagnosis and treatment dates, details of the treatments received, baseline CD4 lymphocyte counts and HIV RNA levels, CD4 lymphocyte counts and HIV RNA levels at 6 months± 1 month and 1 year ±1 month of treatment. After data anonymization by the data expert, personal data were protected and statistical analysis was performed.
Two definitions for presentation were used as follows: 1. Late diagnosis: Presentation with a CD4 cell count fewer than 350 cells/mL and/or with an AIDS-defining event. 2. Advanced HIV disease: Presentation with a CD4 cell count below 200 cells/mL and/or with an AIDS-defining event. Persons with recent evidence of infection (ie diagnosed at the time of seroconversion) was reclassified as “not late”. The presence of at least one of the following characteristics was used to evaluate the evidence of recent infection: (i) negative HIV test within 12 months to HIV diagnosis or (ii) acute HIV infection (eg seroconversion illness). Persons having evidence of earlier diagnosis in another country or region were excluded from the study.
The data were transferred to the computer environment with SPSS v20.0 program and descriptive analyses were performed. Data were presented as mean (mean) ± standard deviation (SD), median, lower value (LV), upper value (UV), number (n) and percentage (%). The conformity of the variables to normal distribution was tested with the Shapiro–Wilks test. Student t-test was used in the analysis of continuous variables showing normal distribution. Mann–Whitney U-test and Kruskal–Wallis test were used to analyze continuous variables that did not show normal distribution. Chi-square or Fischer’s exact test was used to analyze categorical variables. In correlation analysis, Spearman correlation test was applied. A p value 0.05 was considered as statistically significant. Kaplan Meier test and log rank were used for survival analysis.
The study was approved by Çukurova University Medical School non-interventional studies Institutional Review Board (IRB) with the 130th meeting decision No: 18 dated February 4, 2023. The committee waived the requirement for informed consent due to the anonymization of patient data.
Results
Of the recorded 914 patients who met the inclusion and exclusion criteria, 120 patients had evidence of previous diagnosis abroad or elsewhere. Further analysis was made with 794 treatment naïve patients who admitted to our outpatient clinic; 90.6% were male and the mean±SD and median (min-max; IQR) ages were 36.0±12.0 and 33.0 (16–82; 18) years respectively.
When the previous definition used 48.9% was diagnosed as late while 47.2% was diagnosed as late with the new definition used. Only 13 patients were marked as “not late”. 183 patients (23%) were diagnosed as advanced disease (AD). 25.9% (n=206) of the patients were diagnosed during the pandemic period (March 1, 2020- April 1, 2022). While the LD rate was 44.2% before the pandemic, it was 55.8% during the pandemic period (P=0.005). The rate of AD was 20.6% before the pandemic and 30.1% during the pandemic (P=0.007).
There was no statistically significant relationship between gender and LD (p=0.546, OR=1.164 [0.723–1.873]). 46.9% (n=375) of men and 50.7% (n=388) of women had LD. Those with LD were statistically significantly older, p<0.001. Median ages (min-max, IQR) were was 36 (17–82,18) for LD and 31 (17–82, 16) for not LD.
CD4 counts before, during and after treatment were statistically significantly lower in patients with LD (Table 1) The virological response was statistically significantly worse in patients with LD compared to those without (Table 2).
 |
Table 1 The Relationship Between CD4 Counts and Late Diagnosis |
 |
Table 2 Virological Response of Patients with Late Diagnosis Vs Not Late Diagnosis |
Mortality rate was 2.9% (n=29) and was higher in patients with LD compared to those without (4.8% vs 1.2%, p=0.003, OR=4.175 [CI:1.534–11.358]). Survival of the patients with LD was significantly shorter than those without (Figure 1, log rank=0.004).
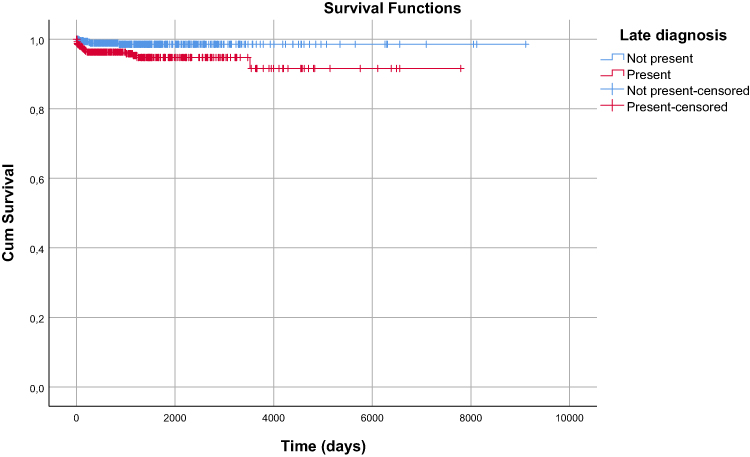 |
Figure 1 Survival of patients with late diagnosis. |
Discussion
In our study, 48.9% of cases were diagnosed as late with the previous definition, and, 47.2% with the new definition. Only 13 patients (1.7%) were designated as “not late” and advanced disease (AD) was diagnosed in 183 patients (or 23%). When we look at the published studies, late presenter rates were similar to us. Late Presentation Working Groups in EuroSIDA and COHERE estimated the burden of late presenters between 36.8% and 64.2%.8 According to the study by Gullón et al using old definitions, 158 (50%) of all newly diagnosed patients had LD and 30.7% of the patients (n=97) had AD.9 Similar to us, in the cohort including 2016 and 2017 from 13 of the 17 HIV centers in Poland, 88.9% of the 1522 patients were male, with a median age of 33.6 years. Late presenters accounted for 44.8% of the study group.10 In a study from 15 centers and 2953 patients in Turkey, similar with the literature, 46.7% presented with a CD4 T cell count of <350 cells/mm3.11 In a Turkish Cohort that was conducted in Istanbul, there were a total of 1673 patients (1440 males, with a median age of 35 years) and 49.4%, were diagnosed with the disease at a later stage, having a CD4 count that was lower than 350 cells/mm3. 427 people who were diagnosed late had advanced HIV illness, which accounts for 25.5% of all diagnoses and 51.7% of diagnoses.12
Data from the national Swedish InfCareHIV registry from 2017 to 2021 showed that LD decreased from 55% to 52% following reclassification of acute HIV infection as “not late”.7 In another study from the UK reclassifying LD based on RITA testing and/or using 24 months for a negative test, LD decreased by 7% in 2019, from 49% to 42%.4 As far as we know, there are no studies in Turkey using the new definition and we are first cohort reporting it. Our reclassification did not yield that much difference in the rates possibly because of patients’ admitting to hospitals lesser during the pandemic that led us underdiagnosing the acute HIV infection.
In our study, LD affected the patients’ response to treatment and prognosis. In an observational study, LD cases had greater short-term mortality than non-LD cases across the majority of socio-demographic and epidemiological parameters, and the mortality rate ratio (RR) was 5.37 (95% confidence interval [CI]: 3.49–8.2). The preponderance (88.8%) of the 98 fatalities that occurred within one year of HIV diagnosis were due to LD. HIV/AIDS-related causes accounted for 70.4% of all fatalities that occurred within the first year of diagnosis (non-LD 36.4% vs LD 74.7%), compared to 31.1% of deaths that occurred >1 year after diagnosis (non-LD 21.4% vs LD 35.5%).13 In another research that looked at the prevalence, epidemiological features, and survival probability of individuals newly diagnosed with HIV in Catania, Italy, from 1985 to 2010, late and very late presentation was related with a decreased survival probability. They believe that implementing methods centered on targeted preventive initiatives and HIV testing programs is critical to detecting and treating HIV infection as early as feasible.14 The Late Presentation Working Groups in COHERE and EuroSIDA estimate that, during 2010–2016, 12,050 excess AIDS-related events and/or deaths could have been avoided if people were diagnosed. This underestimates the therapeutic benefit of beginning ART sooner because their findings were based on cohort data from years when many patients did not start ART until their CD4 cell count was low, before the INSIGHT START research changed clinical treatment in Europe.15 They suggest that, if all were detected and treated immediately, many more events may have been prevented.8
A retrospective multicenter cohort study comprised of all the HIV patients diagnosed in 2019 in 27 Spanish hospitals included one hundred and fifty-five of 352 patients of which 42.9% had a CD4 count of less than 350 per mm3 at the time of HIV diagnosis. Sixteen percent of patients diagnosed had a missed opportunity in the 5 years before HIV diagnosis, highlighting the need to implement screening strategies in the emergency departments different from the current one to improve these outcomes.16 It is important to identify the reasons of missed opportunities and risk factors to reduce LD in order to improve prognosis.
In Jabłonowska’s study, the independent factors associated with LD were age (OR = 1.52) and mode of transmission (Heterosexual: OR = 1.73, intravenous drug use: OR = 2.24). To enhance early diagnosis and medical care, it was suggested that these patients be targeted.10 The review, which covered the years 2015–2021, older age was consistently associated with delayed presentation even it was variably defined, but usually ≥50 years.17 LD was also associated with older age and was more common among immigrants as well as intravenous drug users in Gullon’s study.9 A Polish study from 15 HIV centers in 2016–2017 also identified advanced age, heterosexuality and intravenous drug use as risk factors.10 Similarly, LD was identified as a risk factor for LD in our patients. In the study by Karaosmanoglu et al from Turkey, late presenters were older and less educated. Therewithal, the likelihood of LD was higher among married patients. Among early applicants, homosexuals which were diagnosed in screening studies and those with low HIV-RNA viral load were more likely.12 Heterosexuality also found to be a risk factor for LD in other studies. In a study, a greater proportion of heterosexual men had LD along with their short-term mortality rate. This could be due to differences in their risk perception, knowledge, and HIV testing frequency.13
A study from the Netherlands explored the experiences of 34 people with LD via semi-structured interviews. Reasons for LD were identified as “symptoms not attributed to HIV by a medical professional”, “feeling healthy” and “fear of the consequences of an HIV diagnosis”. It was usually a combination of not being aware of the fact that they were at risk of HIV infection and the absence of HIV-related symptoms prior to diagnosis.18
Immigrants and asylum seekers are another population at risk. A retrospective cohort study, between June 1, 2017 and October 31, 2018, Canada, of 1849 patients, 62% had LD, 22% were presented with AD, 25% of the patients had high viral load (> 100,000 copies/mL).19 Between 2004 and 2016, 9590 new HIV diagnoses registered in the Spanish cohort, with a higher rate of LD in migrants than in non-migrants (46.7% vs 51.4%, p < 0.001). Among migrants, the highest rates of LD were in sub-Saharan Africa (63.4%) and North Africa (62.8%), heterosexual men (66.4%), people who are illiterate or have not completed primary school (64.6%), and people over 50 (61.4%). The rate of LD was higher in women (57.1%) than in men (50.0%).20
On the other hand, the subsequent SARS-CoV-2 pandemic caused serious consequences for health services, particularly for the most vulnerable populations, such as people infected with HIV. These people may not have been able to reach a hospital for HIV testing and treatment, leading to delayed diagnosis and potentially increased mortality.21 A retrospective case series from four centers in Poland in a study examining COVID-19 and LD, 19/25 of patients were male (76%) and median age was 38.5 years (range 25–59) The median CD4 cell count was 72 cells/μL (range 3–382) and twenty-three patients (92%) had LD while 22 (88%) had AD. This was higher than the previous studies after 2015 where LD rates were between 43% and 53%.22 In a non-interventional, single-center retrospective cohort from Germany, LD in diagnoses made in 75 patients was found to be 83% during the COVID-19 period, compared to 59% before COVID-19.23 In a study from Turkey with 1071 patients, 36.4% of the patients had low CD4 counts (<350 cells/mm3) in the pre-pandemic period, while it was 47.9% patients during the pandemic phase (p<0.01).24 We made comparable observations, and LD and AD were statistically significantly higher during the pandemic period.
Our limitations in this study are being a single center study and not reporting many risk factors for late diagnoses. Because of being a regional hospital and serving a population representing the south-east of Turkey may overcome one of these limitations. However, we should perform a multicenter study investigating the missed opportunities and specific risk factors in our region in order to integrate our work to the field and disseminate scientific data.
As a conclusion, HIV patients with a LD had a poorer prognosis. Older age and heterosexuality seem to be the main risk factors for it and disruption of health services during the pandemic might have contributed the increase of late and advanced prognoses. In addition to screening groups who are at risk, promoting awareness among populations that are underdiagnosed and advocating testing even in disastrous situations appear to be the most effective ways forward.
Data Sharing Statement
If needed, data supporting the results will be shared.
Author Contributions
All authors made substantial contributions to conception and design, acquisition of data, or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval of the version to be published; and agree to be accountable for all aspects of the work.
Disclosure
Dr Yeşim Taşova reports personal fees, non-financial support from Gilead, personal fees, non-financial support from GSK, personal fees from Pfizer, personal fees from MSD, outside the submitted work. The authors report no other conflicts of interest financial or otherwise about this work.
References
1. Deeks SG, Overbaugh J, Phillips A, et al. HIV infection. Nat Rev Dis Primers. 2015;1(1):15035. doi:10.1038/nrdp.2015.35
2. Antinori A, Coenen T, Costagiola D, et al; European tter Consensus Working Group. Late presentation of HIV infection: a consensus definition. HIV Med. 2011;12(1):61–64. doi:10.1111/j.1468-1293.2010.00857.x
3. Lodi S, Fisher M, Phillips A, et al; CASCADE Collaboration in EuroCoord. Symptomatic illness and low CD4 cell count at HIV seroconversion as markers of severe primary HIV infection. PLoS One. 2013;8(11):e78642. doi:10.1371/journal.pone.0078642
4. Kirwan PD, Croxford S, Aghaizu A, et al. Re-assessing the late HIV diagnosis surveillance definition in the era of increased and frequent testing. HIV Med. 2022;23(11):1127–1142. doi:10.1111/hiv.13394
5. Sasse A, Florence E, Pharris A, et al; Belgian Research AIDS & HIV Consortium (BREACH). Late presentation to HIV testing is overestimated when based on the consensus definition. HIV Med. 2016;17(3):231–234. doi:10.1111/hiv.12292
6. Brännström J, Svedhem Johansson V, Marrone G, et al. Deficiencies in the health care system contribute to a high rate of late HIV diagnosis in Sweden. HIV Med. 2016;17(6):425–435. doi:10.1111/hiv.12321
7. Croxford S, Stengaard AR, Brännström J, et al; EuroTEST HIV Late Diagnosis Definition Working Group. Late diagnosis of HIV: an updated consensus definition. HIV Med. 2022;23(11):1202–1208. doi:10.1111/hiv.13425
8. Late Presentation Working Groups in EuroSIDA and COHERE. Estimating the burden of HIV late presentation and its attributable morbidity and mortality across Europe 2010–2016. BMC Infect Dis. 2020;20(1):728. doi:10.1186/s12879-020-05261-7
9. Gullón A, Verdejo J, de Miguel R, et al. Factors associated with late diagnosis of HIV infection and missed opportunities for earlier testing. AIDS Care. 2016;28(10):1296–1300. doi:10.1080/09540121.2016.1178700
10. Jabłonowska E, Szetela B, Bielecki M, et al. Acquired immune deficiency syndrome (AIDS) and late presentation in Poland - data from Test and Keep in Care (TAK) Polska project. HIV Med. 2021;22(5):387–396. doi:10.1111/hiv.13041
11. Erdinc FS, Dokuzoguz B, Unal S, et al; Multicentric Hiv Study Group. Temporal trends in the epidemiology of HIV in Turkey. Curr HIV Res. 2020;18(4):258–266. doi:10.2174/1570162X18666200427223823
12. Karaosmanoğlu HK, Mete B, Gündüz A, et al. Late presentation among patients with human immunodeficiency virus infection in Turkey. Cent Eur J Public Health. 2019;27(3):229–234. doi:10.21101/cejph.a5416
13. Ang LW, Toh MPHS, Wong CS, et al. Short-term mortality from HIV-infected persons diagnosed from 2012 to 2016: impact of late diagnosis of HIV infection. Medicine. 2021;100(26):e26507. doi:10.1097/MD.0000000000026507
14. Celesia BM, Castronuovo D, Pinzone MR, et al. Late presentation of HIV infection: predictors of delayed diagnosis and survival in Eastern Sicily. Eur Rev Med Pharmacol Sci. 2013;17(16):2218–2224.
15. Lundgren JD, Babiker AG, Gordin F, et al.; INSIGHT START Study Group. Initiation of antiretroviral therapy in early asymptomatic HIV infection. N Engl J Med. 2015;373(9):795–807. doi:10.1056/NEJMoa1506816
16. Salmerón-Béliz OJ, Pérez-Fernández E, Miró O, et al; Infectious Diseases in Emergency Medicine Working Group of the Sociedad Española de Medicina de Urgencias y Emergencias [Spanish Society of Emergency Medicine] (INFURG-SEMES). Evaluation of emergency department visits prior to an HIV diagnosis: missed opportunities. Enferm Infecc Microbiol Clin. 2022. doi:10.1016/j.eimce.2021.12.010
17. Justice AC, Goetz MB, Stewart CN, et al. Delayed presentation of HIV among older individuals: a growing problem. Lancet HIV. 2022;9(4):e269–e280. doi:10.1016/S2352-3018(22)00003-0
18. van Opstal SEM, van der Zwan JS, Wagener MN, et al. Late presentation of HIV infection in the Netherlands: reasons for late diagnoses and impact on vocational functioning. AIDS Behav. 2018;22(8):2593–2603. Erratum in: AIDS Behav. 2018 Aug 24. doi:10.1007/s10461-018-2082-9
19. Kronfli N, Linthwaite B, Sheehan N, et al. Delayed linkage to HIV care among asylum seekers in Quebec, Canada. BMC Public Health. 2019;19(1):1683. doi:10.1186/s12889-019-8052-y
20. Conway AS, Esteve A, Fernández-Quevedo M, et al; PISCIS Study Group. Determinants and outcomes of late presentation of HIV infection in migrants in Catalonia, Spain: PISCIS cohort 2004–2016. J Immigr Minor Health. 2019;21(5):920–930. doi:10.1007/s10903-018-0834-2
21. Brugnaro P, Morelli E, Cattelan F, et al. The serious threat of late presenters HIV-infected patients in the context of the COVID-19 pandemic. Infez Med. 2022;30(1):119–123. doi:10.53854/liim-3001-14
22. Suchacz MM, Krankowska D, Cybula A, et al. Delayed HIV diagnosis during the COVID-19 pandemic in Poland: a call for targeted HIV testing for those under suspicion of SARS-CoV-2. HIV Med. 2022;23(11):1173–1183. doi:10.1111/hiv.13437
23. van Bremen K, Monin M, Schlabe S, et al. Impact of COVID-19 on HIV late diagnosis in a specialized German centre. HIV Med. 2022;23(11):1209–1213. doi:10.1111/hiv.13426
24. Karaosmanoglu HK, Mete B, Gunduz A, et al. Changing characteristics of patients living with HIV/AIDS after the COVID-19 pandemic in Turkey. Curr HIV Res. 2022;20(3):236–241. doi:10.2174/1570162X20666220303103805
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Case Series of HIV-Associated Oral Lesions Across Different Clinical Stages in People Living with HIV
Permatasanti A, Sufiawati I
HIV/AIDS - Research and Palliative Care 2024, 16:289-299
Published Date: 26 July 2024
Population-Specific Predictors of Immunologic Reconstitution Following Initiation of Combined Antiretroviral Therapy in Children: A Retrospective Observational Study from a 15-Year Cohort of HIV-Positive Children and Adolescents in Eritrea
Ghebremeskel GG, Mengistu ST, Tsegai MT, Mehretab AG, Kidane HA, Abraham YT, Habte RA, Teklemariam HM
HIV/AIDS - Research and Palliative Care 2024, 16:433-453
Published Date: 6 November 2024