Back to Journals » Journal of Pain Research » Volume 16
Lasmiditan in Japanese Patients with Common Migraine Comorbidities or Concomitant Medications: A Post Hoc Safety and Efficacy Analysis from the MONONOFU Study
Authors Kitamura S ![]() , Imai N
, Imai N ![]() , Tanji Y, Ozeki A
, Tanji Y, Ozeki A ![]() , Komori M
, Komori M ![]()
Received 2 December 2022
Accepted for publication 8 May 2023
Published 25 May 2023 Volume 2023:16 Pages 1725—1738
DOI https://doi.org/10.2147/JPR.S399567
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Alexandre F DaSilva
Shigekazu Kitamura,1 Noboru Imai,2 Yuka Tanji,3 Akichika Ozeki,3 Mika Komori3
1Department of Neurology, Konan Kakogawa Hospital, Hyogo, Japan; 2Department of Neurology, Japanese Red Cross Shizuoka Hospital, Shizuoka, Japan; 3Japan Drug Development and Medical Affairs, Eli Lilly Japan K.K., Kobe, Japan
Correspondence: Mika Komori, Japan Drug Development and Medical Affairs, Eli Lilly Japan K.K., 5-1-28, Isogamidori, Chuo-Ku, Kobe-Shi, 651-0086, Japan, Tel +81-78-242-8391, Fax +81-78-242-9939, Email [email protected]
Background: Migraine is often comorbid with other disorders. People with migraine may be prescribed one or more concomitant medications. This post hoc analysis assessed the safety and efficacy of lasmiditan in Japanese people with migraine comorbidities or using concomitant medications.
Patients and Methods: The MONONOFU study was a Phase 2, randomized, placebo-controlled, multicenter study of lasmiditan for acute migraine treatment in Japanese adults. Patients reported comorbidities (pre-existing or coexisting conditions) during screening. Concomitant medications (any drugs taken ± 48 hours of the study drug) and treatment-emergent adverse events (TEAEs) were recorded in a paper diary. Study drug efficacy (pain freedom 2 hours after administration of study drug) was reported in an eDiary. Logistic regression models were used for subgroup analyses of safety (incidence of TEAEs) and efficacy (pain freedom at 2 hours post dose) of lasmiditan in relation to presence/absence of comorbidities, and safety in relation to concomitant medications.
Results: Common comorbidities (occurring in ≥ 10% of any lasmiditan dose group) were seasonal allergies, allergic rhinitis, tension-type headache, cervicobrachial syndrome, dysmenorrhea, nasopharyngitis, musculoskeletal stiffness, chronic gastritis, constipation, and insomnia. There was no significant interaction of treatment with comorbidity for safety or efficacy. There was also no significant interaction between treatment and concomitant medication groups of special interest (acetaminophen/nonsteroidal anti-inflammatory drugs, triptans, antiemetics, central nervous system depressant medications, serotonergic medications, antiepileptics, antihypertensive medications, Chinese herbal medicines, and contraceptives) for incidence of TEAEs.
Conclusion: In Japanese people with migraine, the safety of lasmiditan appeared to be independent of common comorbidities and concomitant medications; efficacy appeared to be independent of comorbid conditions.
Clinical Trials Registration: NCT03962738 (ClinicalTrials.gov).
Keywords: comorbidity, drug therapy, headache, Japan, migraine disorders, safety
Introduction
Migraine is a highly prevalent disorder globally and causes substantial disability.1 In Japan, the prevalence of migraine is estimated at around 8.5% of the population.2,3
Migraine is often comorbid with other highly prevalent disorders.4 Common comorbidities of migraine include cardiovascular conditions, gastrointestinal disorders, obesity, anxiety, depression, panic disorder, bipolar disorder, asthma, sleep disorders, arthritis and chronic pain, and fatigue.4 People with migraine may therefore be prescribed one or more concomitant medications to treat comorbid disorders, in addition to medication(s) prescribed for their migraine. Migraine treatment itself may also involve multiple medications, whether by combination of prescription and over-the-counter treatments, or by combination of preventive and acute migraine treatments.2,5
Effective acute treatment of migraine is required to quickly resolve or improve migraine symptoms in order to reduce impacts on day-to-day functioning and quality of life.
However, acute treatment options may be limited by drug contraindications for comorbidities.6 Lasmiditan is a selective 5-HT1F (serotonin) receptor agonist that acts at the trigeminal nerve system to inhibit release of neurotransmitters and at the central nervous system (CNS) to inhibit pain transmission, without causing vasoconstriction.4,7 The efficacy and safety of lasmiditan have been confirmed in global Phase 3 studies in non-Japanese patients8–10 and in a Phase 2 study of Japanese adults (the MONONOFU study).11–14 Lasmiditan was approved as an oral treatment for migraine in the USA in 201915 and in Japan in January 2022.
In a post hoc analysis of the global Phase 3 studies of lasmiditan, the efficacy and safety of lasmiditan appeared to be independent of comorbidities4 and concomitant medications.5 The impact of concomitant medications other than migraine preventives and of comorbidities common in Asian populations on the efficacy and safety of lasmiditan has not previously been assessed. In this post hoc analysis, data from the MONONOFU study were used to assess the impact of comorbidities on the safety and efficacy of lasmiditan, and the impact of concomitant medications (not limited to migraine preventives) on lasmiditan safety, in Japanese people with migraine.
Materials and Methods
Study Design, Study Population, and Treatment Protocol
The MONONOFU study design has been described previously.11 Briefly, MONONOFU was a prospective, multicenter, randomized, double-blind, placebo-controlled, Phase 2 study of lasmiditan in Japanese people with migraine (ClinicalTrials.gov identifier: NCT03962738). The primary objective was to evaluate the efficacy of lasmiditan 200 mg for achieving freedom from pain versus placebo. Included patients were aged ≥18 years and had migraine with or without aura fulfilling the International Headache Society diagnostic criteria,16 a history of disabling migraine for ≥1 year, a history of 3–8 migraine attacks/month and <15 headache days/month during the past 3 months, and a Migraine Disability Assessment score ≥11.17,18 The study protocol was approved by the Institutional Review Board for each study site (Supplementary Table 1). All participants provided written informed consent. The study was conducted in accordance with the Declaration of Helsinki and the Council for International Organizations of Medical Sciences International Ethical Guidelines, and in compliance with the International Council for Harmonisation Guideline for Good Clinical Practice and related laws and regulations.
Eligible patients were randomized to oral placebo or lasmiditan 50, 100, or 200 mg (7:3:7:6); the study drug was self-administered within 4 hours of onset of a single migraine attack (moderate-to-severe).11 Efficacy data were collected in an electronic diary. Study participants recorded the date and time of the migraine attack, the time at which the study drug was taken, and migraine severity using the 4-point International Headache Society headache severity rating scale (0 = no pain, 1 = mild pain, 2 = moderate pain, and 3 = severe pain). Migraine severity was rated prior to taking the study drug and at 0.5, 1, 1.5, 2, 3, 4, 24, and 48 hours post dose. Patients recorded adverse events (AEs) in a paper diary.
The medical history of each patient, including comorbidities and concomitant medications, was collected at the screening visit. Comorbidities were coded as System Organ Classes (SOCs) and Preferred Terms (PTs) using the international Medical Dictionary for Regulatory Activities (MedDRA) Version 23.0. During the study, patients recorded concomitant medication use (including use of rescue or recurrence medications during the migraine attack) in the paper diary. Medications prohibited from 24 hours prior to 2 hours after administration of the study drug were acetaminophen (ACE), nonsteroidal anti-inflammatory drugs (NSAIDs), caffeine, antiemetics, triptans, ergots, opioids, and barbiturates. From 2 hours post dose, ACE, NSAIDs, caffeine, and antiemetics were allowed as rescue medications. From 24 hours post dose, triptans, ergots, opioids, and barbiturates were allowed for recurrence of a migraine attack. Migraine preventive medications were allowed if treatment was stable for 3 months prior to baseline.
Post Hoc Analysis
This post hoc analysis examined the safety and efficacy of lasmiditan in patient groups defined by comorbidities and concomitant medications. The safety endpoint for this analysis was any treatment-emergent adverse event (TEAE). TEAEs were defined as AEs that occurred or worsened in severity within 48 hours after administration of the study drug, regardless of a causal relationship to the study drug. SOCs and PTs of TEAEs were coded using MedDRA Version 23.0.
The efficacy endpoint for this analysis was pain freedom 2 hours after administration of the study drug. Pain freedom was defined as moderate or severe headache pain (severity rating ≥2) becoming none (severity rating = 0).
The statistical procedure and analysis software used for the post hoc analysis is described in the Statistical Analysis section.
Comorbidities
Comorbidities were defined as pre-existing or coexisting conditions at baseline. Common comorbidities were defined as those that occurred in ≥10% of any treatment group.
Concomitant Medications
For this analysis, concomitant medications were defined as any drugs taken within 48 hours of the study drug (before or after), including rescue or recurrence medications. Concomitant medications were categorized into nine groups of special interest: ACE/NSAIDs (subgroups: ACE only, NSAIDs only), triptans, antiemetics, CNS depressant medications (subgroups: CNS depressants except antihistamines, antihistamines only), serotonergic medications, antiepileptics, antihypertensive medications, Chinese herbal medicines, and contraceptives. These medication groups were selected because they are common medications that are frequently used for migraine and/or headache treatment (eg, ACE, NSAIDs, triptans, antiemetics, Chinese herbal medicines); are specifically listed within the “precautions for co-administration” section of the package insert for lasmiditan (CNS depressants, serotonergic medications, and specific antihypertensive medications);19 and/or are used to treat conditions that may be comorbid with migraine (eg, serotonergic medications, contraceptives [for menstruation-linked migraine], CNS depressants, antihypertensive medications).
For five of the concomitant medication groups, a set of special interest TEAEs were defined per the descriptions in the package insert for lasmiditan.19 In the triptan and serotonergic medication groups, special interest TEAEs were those that could potentially be symptoms of serotonin syndrome (according to either the Hunter20 or Sternbach21 criteria). These included the PTs agitation, anxiety, chills, clonus, confused state, diarrhea, hyperhidrosis, hyperreflexia, hypomania, myoclonus, muscle rigidity, pyrexia, oculoclonus myoclonus, and tremor. In the CNS depressant group, special interest TEAEs were any TEAEs in the SOCs nervous system disorder, psychiatric disorder, or general disorder that occurred in ≥2% of the patients in any treatment group. In the antiemetic group, special interest TEAEs were nausea and vomiting. In the antihypertensive medication group, special interest TEAEs were any TEAEs in the cardiac disorder SOC that occurred in ≥2% of the patients in any treatment group. Special interest TEAEs were not defined for the ACE/NSAIDs, antiepileptics, Chinese herbal medicines, or contraceptives subgroups.
Statistical Analysis
All safety analyses were conducted using the safety analysis set (all randomized patients who received the study drug). TEAE incidence was calculated according to the presence or absence of comorbidities (or use of concomitant medications), and odds ratios (ORs) were calculated for the all-lasmiditan group (All LTN, which consisted of the lasmiditan 50-, 100-, and 200-mg arms combined) versus the placebo group. Logistic regression models were used for subgroup analyses of comorbidities (presence/absence) and concomitant drugs (presence/absence). The objective variable was the incidence of TEAEs. Covariates in the logistic regression models were treatment group (All LTN vs placebo), subgroup, and treatment-by-subgroup interaction. Results are presented as ORs with 95% confidence intervals (CIs). OR and treatment-by-subgroup interaction p-values were calculated with a significance level of 0.05 (2-sided test).
Efficacy analyses were conducted on data from the modified intent-to-treat (mITT) population (all randomized patients who took ≥1 dose of study drug within 4 hours of onset of the migraine attack and had any post-dose efficacy assessments). A logistic regression model was used for a subgroup analysis of efficacy in relation to comorbidities (presence/absence). The objective variable was pain freedom at 2 hours post dose. Because many concomitant drugs may have been taken >2 hours after the lasmiditan dose (eg, ACE/NSAIDs, caffeine, and antiemetics were allowed as rescue drugs 2–24 hours post dose), we did not model the influence of concomitant medication on the efficacy endpoint of pain freedom at 2 hours. Covariates in the logistic regression model were treatment group (All LTN vs placebo), baseline usage of preventive migraine medications (Yes/No), subgroup, and treatment-by-subgroup interaction. OR and treatment-by-subgroup interaction p-values were calculated with a significance level of 0.05 (2-sided test). All analyses were conducted using SAS 9.4 (SAS Institute Inc., Cary, NC, USA).
Results
Patient Disposition and Characteristics
The patient disposition and baseline characteristics for the MONONOFU study have been described previously.11 Briefly, 846 patients were randomized and 691 took the study drug (safety population); the mITT population was 682 patients.11 Most patients were female (83.1%) and the mean age was 45.2 years.11 Baseline migraine characteristics of the study population included a mean migraine history duration of 24.2 years and a mean baseline Migraine Disability Assessment total score of 22.3.11 Overall, 37.5% of the patients reported taking preventive migraine medication.11
Safety and Efficacy of Lasmiditan in Relation to Common Comorbidities
Comorbidities were very common in the safety population (Table 1; Supplementary Table 2). Among the patients who received any dose of lasmiditan (All LTN group, N=477), 444 (93.1%) had ≥1 comorbidity. The most common comorbidities (occurring in >15% of the patients) in the All LTN group were seasonal allergies, allergic rhinitis, tension-type headache, and cervicobrachial syndrome (26.6%, 23.1%,19.1%, and 16.8% of the All LTN group, respectively).
 |
Table 1 Most Common Comorbidities (Occurring in ≥10% of Any Lasmiditan Dose Group) by MedDRA Preferred Term (Safety Population) |
Safety
Overall, TEAEs were common in patients treated with lasmiditan (Table 2). In the All LTN group, the overall incidence of patients with ≥1 TEAE was 70.9%. Among the common comorbidity groups, the nasopharyngitis group reported the highest incidence of TEAEs, with 82.8% (53/64) of patients with nasopharyngitis in the All LTN group reporting ≥1 TEAE. The ORs for the incidence of TEAEs in the All LTN group with and without each comorbidity (vs placebo) were generally similar (Figure 1). There was no statistically significant treatment-by-subgroup interaction for any comorbidity.
 |
Table 2 Incidence of TEAEs in Patients Who Reported Comorbiditiesa (Safety Population) |
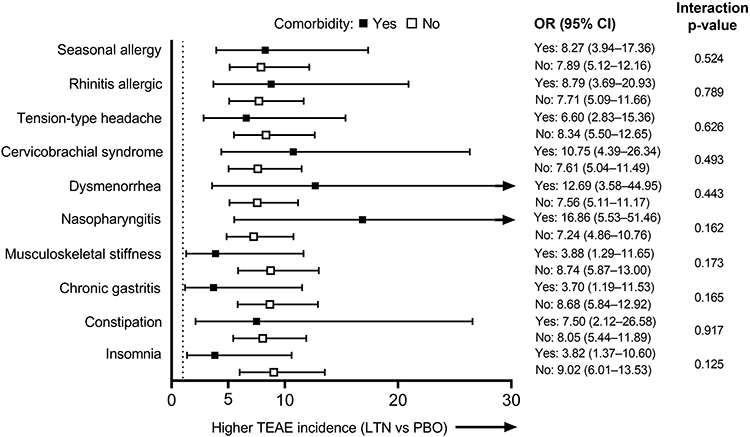 |
Figure 1 TEAE incidence: Forest plot of ORs (All LTN group vs PBO) for each of the most common comorbidity groups (safety population). Larger ORs indicate a higher incidence of TEAEs in the All LTN group compared with PBO. Dotted line indicates OR = 1. The interaction p-values shown are for the treatment-by-comorbidity interaction. Abbreviations: CI, confidence interval; LTN, lasmiditan; OR, odds ratio; PBO, placebo; TEAE, treatment-emergent adverse event. |
Efficacy
Regardless of comorbidity status, the proportion of patients who achieved pain freedom at 2 hours was higher for All LTN than placebo (Figure 2; Supplementary Table 3). However, the OR of All LTN versus placebo was significant among patients with a comorbidity only for the seasonal allergy group (OR [95% CI]: 3.29 [1.43–7.57], p=0.005; Figure 2; Supplementary Table 3). Among the common comorbidity groups, the insomnia group reported the highest proportion of patients who achieved pain freedom at 2 hours (18/43; 41.9%). The lowest proportion of patients who achieved pain freedom at 2 hours was in the dysmenorrhea comorbidity group (15/56; 26.8%). There was no statistically significant treatment-by-subgroup interaction for any comorbidity.
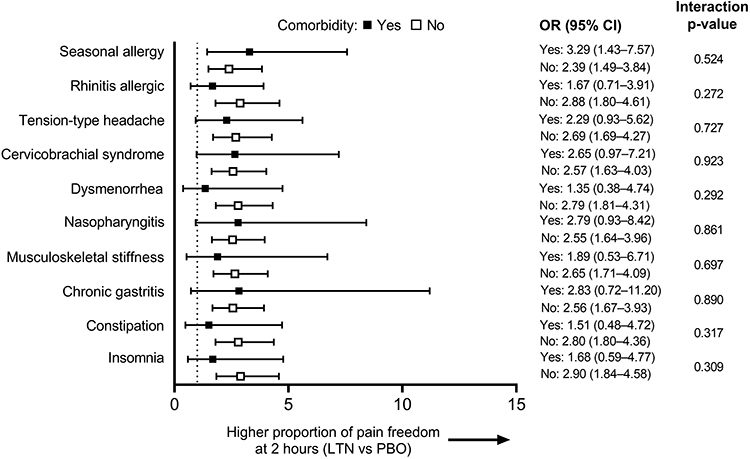 |
Figure 2 Efficacy: Forest plot of ORs (All LTN group vs PBO) for each of the most common comorbidity groups (mITT population). Larger ORs indicate a higher proportion of patients with pain freedom at 2 hours in the All LTN group compared with PBO. Dotted line indicates OR = 1. Abbreviations: CI, confidence interval; LTN, lasmiditan; mITT, modified intent-to-treat; OR, odds ratio; PBO, placebo. |
Safety of Lasmiditan in Relation to Concomitant Medications
The most commonly reported concomitant medications (taken by >40% of the patients in the All LTN group) were within the groups ACE/NSAIDs and triptans (53.0% and 42.3% of the All LTN group, respectively; Table 3). Antihypertensive medications (19.7%), CNS depressants (18.4%), and antiemetics (17.6%) were the next most common groups of concomitant medications.
 |
Table 3 Concomitant Medicationa Groups of Special Interest (Safety Population) |
Safety
At least 1 TEAE was reported by approximately two-thirds to three-quarters of patients who received lasmiditan in the concomitant medication groups (Figure 3). TEAE incidence was higher in the groups taking antiepileptics, Chinese herbal medicines, and contraceptives (incidence of ≥1 TEAE: 73.2%, 72.7%, and 77.8%, respectively) versus the overall All LTN group.
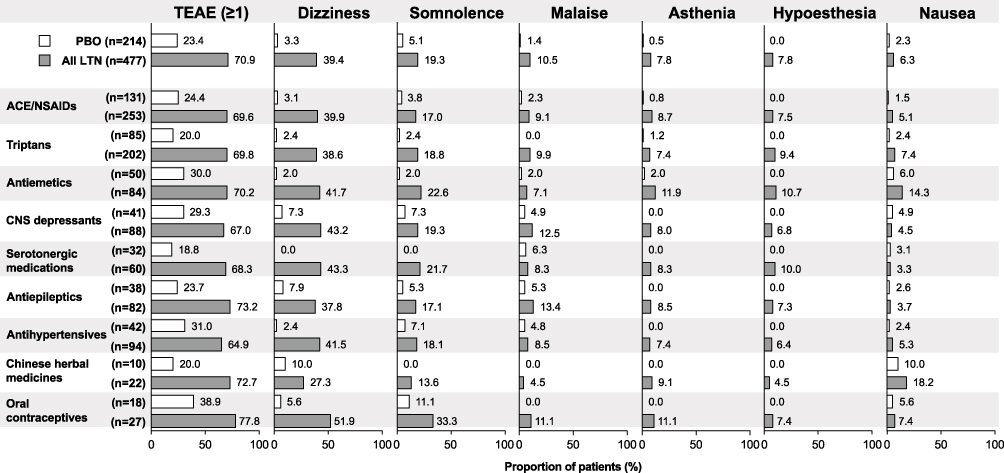 |
Figure 3 Most common TEAEs (≥5% in the All LTN group) in the MONONOFU study11 and their incidence in the concomitant medication groups (safety population). Abbreviations: ACE, acetaminophen; CNS, central nervous system; LTN, lasmiditan; NSAID, nonsteroidal anti-inflammatory drug; PBO, placebo; TEAE, treatment-emergent adverse event. |
As previously reported, the six most common TEAEs (≥5% in the All LTN group) in the MONONOFU study were dizziness, somnolence, malaise, asthenia, hypoesthesia, and nausea.11 The incidence of these TEAEs varied between the concomitant medication groups (Figure 3). The contraceptives group reported the highest incidences of dizziness (51.9%, 14/27 patients) and somnolence (33.3%, 9/27 patients) in All LTN patients. Malaise was highest in the antiepileptic–All LTN group (13.4%, 11/82 patients), while asthenia and hypoesthesia were highest in the antiemetic–All LTN group (11.9%, 10/84 patients and 10.7%, 9/84 patients, respectively). The Chinese herbal medicines group reported the highest incidence of nausea in All LTN patients (18.2%, 4/22 patients).
Within each of the concomitant medication groups, the ORs for the incidence of ≥1 TEAE in the All LTN group with and without each medication (vs placebo) were generally similar (Figure 4). The highest ORs were seen for patients who took Chinese herbal medicines (OR for All LTN vs placebo [95% CI]: 10.67 [1.74–65.27]), serotonergic medications (9.35 [3.30–26.48]), and triptans (9.25 [5.02–17.02]). The treatment-by-subgroup interaction was not significant for any of the concomitant medication groups.
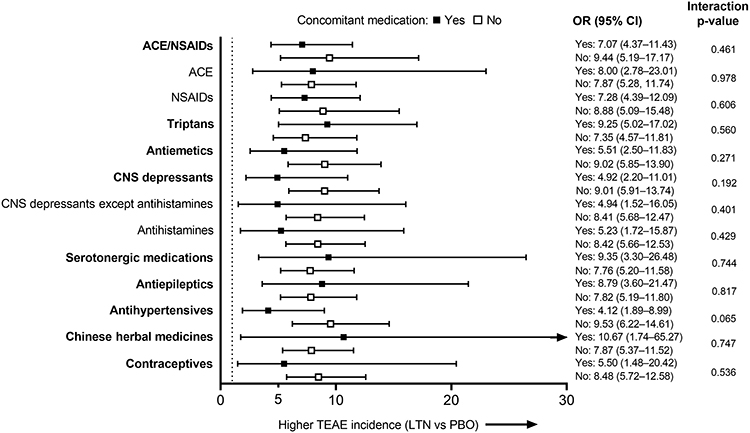 |
Figure 4 TEAE incidence: Forest plot of ORs (All LTN group vs PBO) for each of the concomitant medication groups (safety population). Larger ORs indicate a higher incidence of TEAEs in the All LTN group compared with PBO. Dotted line indicates OR = 1. The interaction p-values shown are for the treatment-by-concomitant medication interaction. Bold indicates concomitant medication groups and plain type indicates subgroups. Abbreviations: ACE, acetaminophen; CI, confidence interval; CNS, central nervous system; LTN, lasmiditan; NSAID, nonsteroidal anti-inflammatory drug; OR, odds ratio; PBO, placebo; TEAE, treatment-emergent adverse event. |
In patients who took CNS depressant medications and received lasmiditan as the study drug, around two-thirds reported ≥1 TEAE (59/88 patients, 67.0%; Table 4). The most common special interest TEAE in this group was dizziness (43.2% of the All LTN group with CNS depressants; 38/88 patients). There was no statistically significant interaction between lasmiditan treatment and CNS depressants for the incidence of CNS TEAEs.
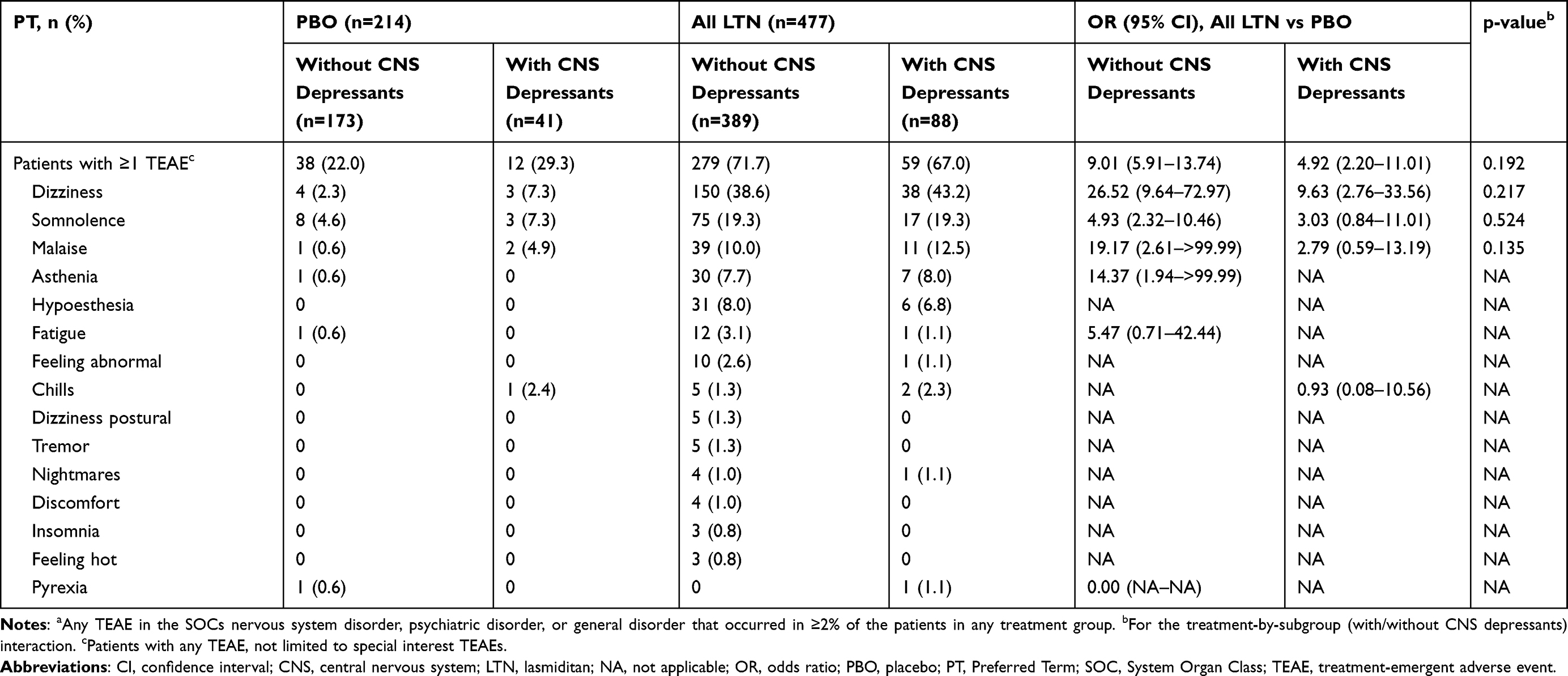 |
Table 4 Occurrence of Special Interest TEAEsa with and without CNS Depressant Use (Safety Population) |
There was no evidence of increased risk of serotonin syndrome symptoms in patients who received lasmiditan and either triptans or serotonergic medications (Table 5). Symptoms of confused state, hypomania, agitation, myoclonus, hyperreflexia, clonus, muscle rigidity, or oculoclonus myoclonus were not observed. Diarrhea, chills, tremor, pyrexia, and anxiety were reported at low incidence (0.5–2.5%) in triptan users; hyperhidrosis was not present in this group. In users of serotonergic medications, diarrhea, pyrexia, tremor, and hyperhidrosis were reported at low incidence (1.7% for each), while chills and anxiety were not reported. There was no statistically significant interaction between lasmiditan treatment and triptans or serotonergic medications for the incidence of these TEAEs.
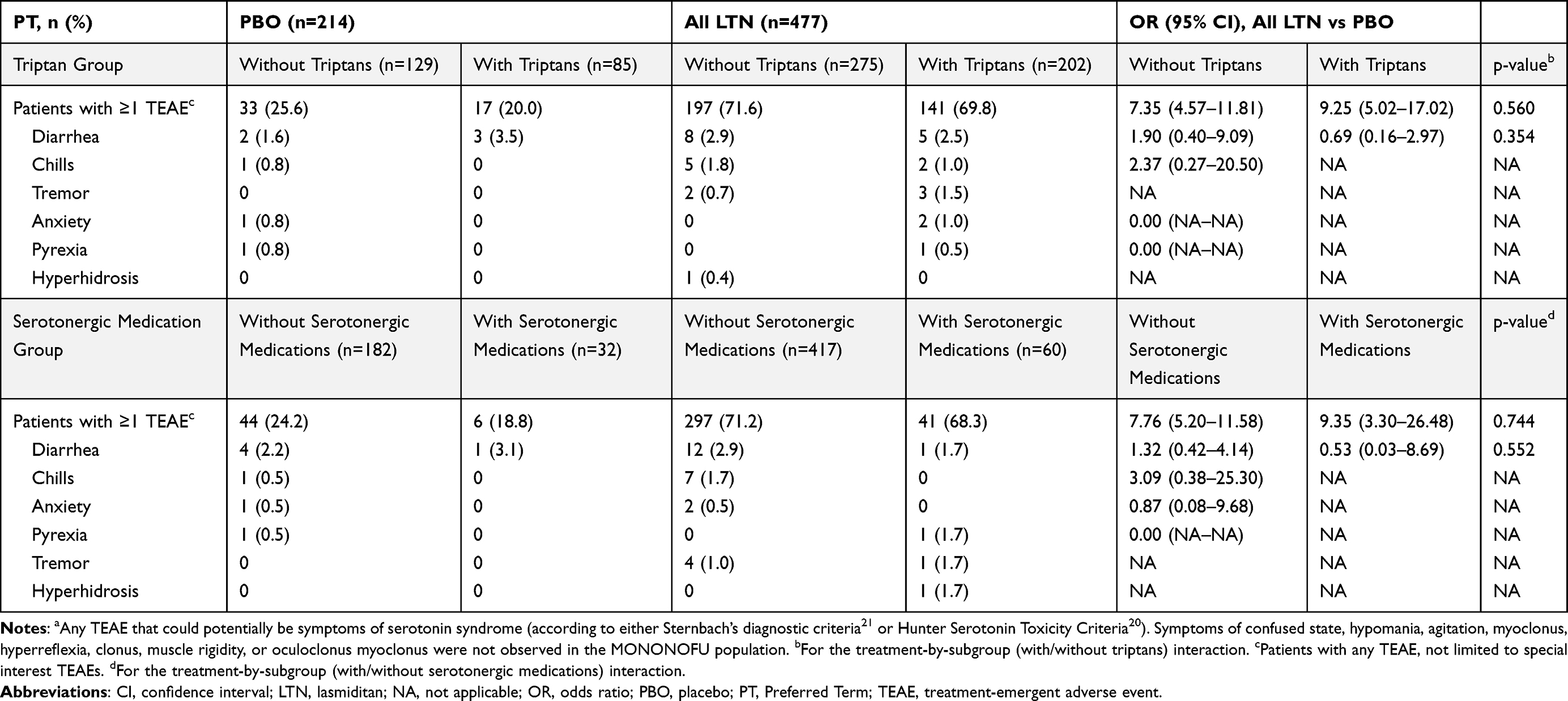 |
Table 5 Occurrence of Special Interest TEAEsa with or without Triptan or Serotonergic Medication Use (Safety Population) |
For patients who took antiemetics, the OR (All LTN vs placebo) for nausea was lower than for those who did not take antiemetics (2.61 vs 3.89, respectively; Table 6). However, the interaction between lasmiditan treatment and antiemetic use was not significant.
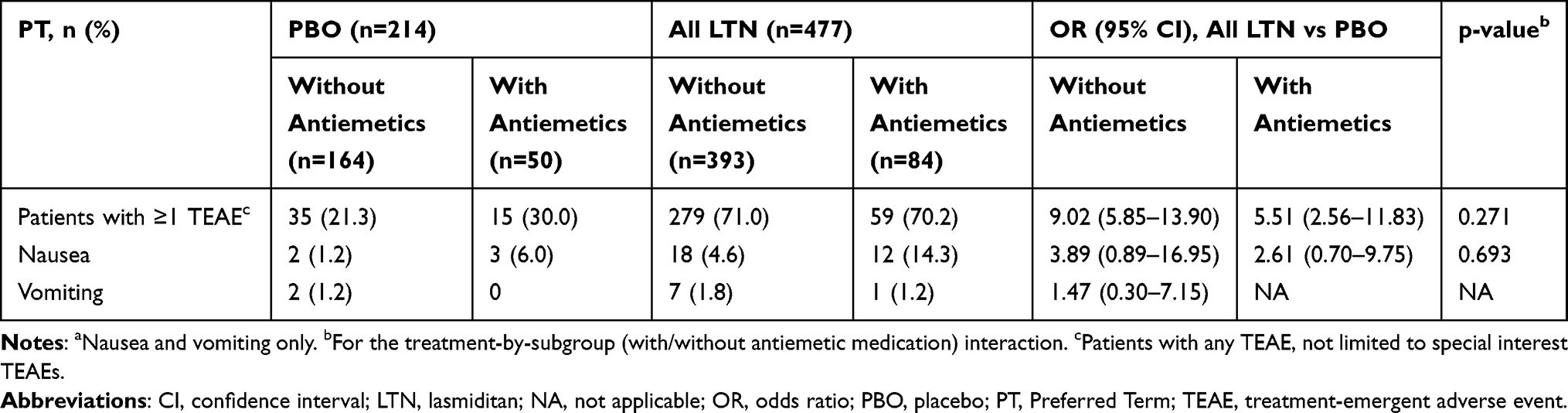 |
Table 6 Occurrence of Special Interest TEAEsa with and without Antiemetic Medication Use (Safety Population) |
In patients who took antihypertensive medications, the OR for palpitations was lower than in patients who did not take antihypertensive medications (0.89 vs 3.46, respectively; Table 7), but the interaction between lasmiditan and antihypertensive medications was not significant.
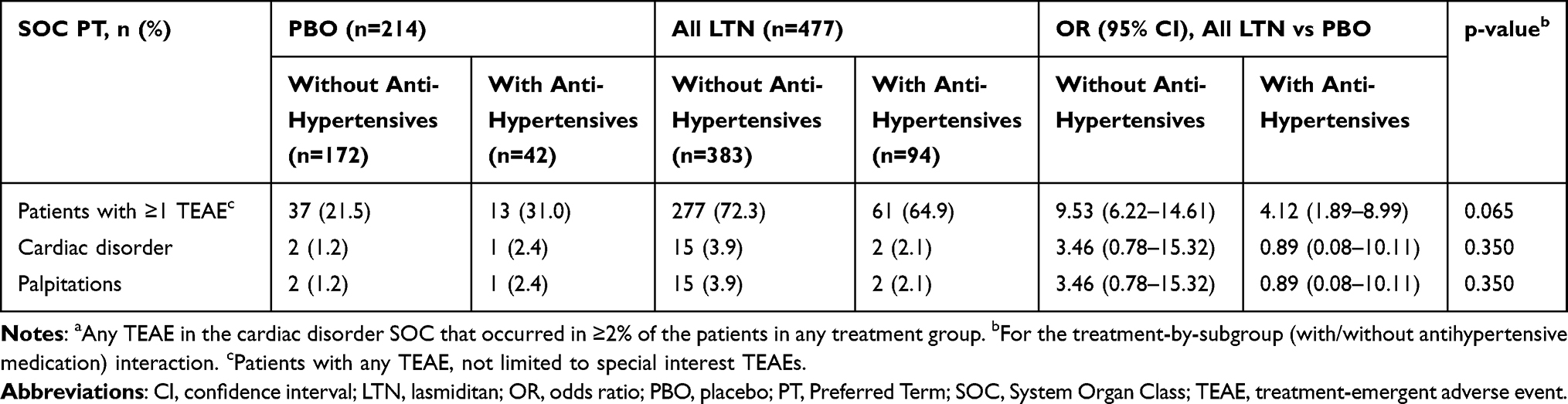 |
Table 7 Occurrence of Special Interest TEAEsa with and without Antihypertensive Medication Use (Safety Population) |
Discussion
This post hoc analysis of data from the MONONOFU study evaluated the safety and efficacy of lasmiditan for treatment of a single migraine attack among patients with and without common comorbidities, and safety of lasmiditan with and without concomitant medications. This is the first such analysis in an Asian patient population. In Japanese patients with migraine, comorbidities and concomitant medications did not affect the safety of lasmiditan. In general, the efficacy of lasmiditan was not affected by comorbidities. These results confirm the safety and efficacy of lasmiditan for migraine in patients with common comorbidities and/or using common concomitant medications.
In the current analysis, we evaluated safety and efficacy in relation to the most common comorbidities (defined as comorbidities that occurred in ≥10% of any lasmiditan dose group). The incidence of TEAEs was similar across all the common comorbidity groups, and the treatment-by-subgroup interaction was not significant for any comorbidity. Similarly, the proportion of patients who achieved pain freedom at 2 hours did not show any significant treatment-by-subgroup interaction for any comorbidity. These results are consistent with the results of a similar post hoc analysis of global Phase 3 trial data for lasmiditan.4 In the global post hoc analysis, the comorbidity groups were 13 categorical groups based on common migraine comorbidities. Despite this difference in approach, both our analysis and the global analysis found no evidence of a differential treatment effect (lasmiditan vs placebo) dependent on subgroup (ie, comorbidity “yes” vs comorbidity “no”) on the safety or efficacy of lasmiditan.
We examined a broader range of concomitant medications in our analysis than in the post hoc analysis of 2 global Phase 3 trials, which examined only medications often prescribed as migraine preventive treatments (even if taken for other reasons).5 Overall incidence of TEAEs was similar across all the concomitant medication groups in our analysis, and the treatment-by-subgroup interaction was not significant for any concomitant medication. This was similar to the pattern seen in the global study population.5 However, our results suggest this may be a broader pattern across a larger range of medications. This is important given that migraine is comorbid with multiple diseases, many of which require regular medication.
Several of the concomitant medication groups may be associated with specific TEAEs or groups of TEAEs. Because lasmiditan is a centrally penetrant drug,7,22 we hypothesized that lasmiditan may interact with CNS depressants to make CNS-specific TEAEs more common. However, in this study in Japanese patients, we found that this was not the case, and there was no significant interaction between lasmiditan and CNS depressants for any CNS-specific TEAE. As lasmiditan can be associated with nausea,11 we expected that there might be lower rates of nausea in patients who received lasmiditan plus antiemetics than in those receiving lasmiditan without antiemetics. However, we also found no interaction between lasmiditan and antiemetics in the incidence of nausea or vomiting. Our results suggest that patients took antiemetics because they experienced nausea, resulting in a relatively high proportion of patients with nausea among antiemetic users regardless of treatment group. Finally, we also checked for an interaction between antihypertensive medications and lasmiditan, as both can be associated with bradycardia.19,23,24 We found no interaction between lasmiditan and antihypertensive drugs in the incidence of cardiac TEAEs generally. The only cardiac disorder TEAE that occurred in ≥2% of the patients receiving lasmiditan was palpitations, which was more common in patients who were not using antihypertensive medications.
Because lasmiditan is a serotonin receptor agonist, we also assessed whether TEAEs potentially indicative of serotonin syndrome were impacted by the interaction of lasmiditan with triptans (also serotonergic) or general serotonergic medications. The serotonin syndrome symptoms of confused state, hypomania, agitation, myoclonus, hyperreflexia, clonus, muscle rigidity, or oculoclonus myoclonus were not observed in the MONONOFU study. Other TEAEs that may be related to serotonin syndrome (anxiety, chills, diarrhea, hyperhidrosis, tremor, and pyrexia) were observed only at low incidence. We found no significant interactions between lasmiditan treatment and triptans or serotonergic medications for the incidence of these TEAEs. These results are consistent with an earlier safety analysis of the whole MONONOFU population, in which none of the participants met the Hunter or Sternbach criteria for serotonin syndrome (based on medical review).13
Because of the study design, some concomitant medications may have been taken >2 hours after the lasmiditan dose as rescue medication (eg, ACE/NSAIDs, caffeine, and antiemetics). As a result, we were unable to model the influence of concomitant medication on the efficacy endpoint of pain freedom at 2 hours. Headache treatment guidelines in several countries advise the addition of an NSAID if a single dose of a triptan provides insufficient pain relief.25–29 The effectiveness of combining lasmiditan with other acute medications, particularly those that also target 5-HT receptors such as triptans and ergots, is an area that warrants further investigation.
The strengths of this post hoc analysis included the use of data from a randomized, placebo-controlled, multicenter clinical trial. In addition, these are the first assessments of the efficacy and safety of lasmiditan in relation to comorbidities or concomitant medications in an Asian population. Our analysis of concomitant medications was broad, including not only medications commonly used as migraine preventives but also other concomitant medications in frequent use. We also considered comorbidities within the framework of disease type rather than the SOC affected.
Limitations of our analysis include that our findings are based on post hoc analyses from a study that was limited to a single dose of lasmiditan and was not designed to investigate relationships between lasmiditan and comorbidities or concomitant medications. Because concomitant medications were taken at any time within 48 hours of the study drug, it is possible that the onset of some TEAEs was prior to the use of concomitant medications. In addition, we cannot rule out the effects of polypharmacy; in cases where a patient used lasmiditan and >1 category of concomitant medication, there was the potential for TEAEs to be associated with an interaction between lasmiditan and multiple categories of concomitant medications. In general, the small sample sizes in the comorbidity “yes” versus “no” and concomitant medication “yes” versus “no” subgroups meant that interaction hypothesis tests were unlikely to be rejected due to wider CIs (eg, as seen for the Chinese medication subgroup). In addition, our post hoc analyses were performed without multiplicity adjustment, which potentially inflated the overall Type 1 error rate.
Conclusion
In Japanese patients with migraine, comorbidities and concomitant medications did not affect the safety of lasmiditan. The efficacy of lasmiditan appeared to be independent of comorbid conditions.
Abbreviations
ACE, acetaminophen; AE, adverse event; CI, confidence interval; CNS, central nervous system; LTN, lasmiditan; MedDRA, Medical Dictionary for Regulatory Activities; mITT, modified intent-to-treat; NSAID, nonsteroidal anti-inflammatory drug; OR, odds ratio; PT, Preferred Term; SOC, System Organ Class; TEAE, treatment-emergent adverse event.
Data Sharing Statement
Eli Lilly and Company provides access to all individual participant data collected during the trial, after anonymization, with the exception of pharmacokinetic or genetic data. Data are available to request 6 months after the indication studied has been approved in the United States and the European Union and after primary publication acceptance, whichever is later. No expiration date of data requests is currently set once data are made available. Access is provided after a proposal has been approved by an independent review committee identified for this purpose and after receipt of a signed data sharing agreement. Data and documents, including the study protocol, statistical analysis plan, clinical study report, blank or annotated case report forms, will be provided in a secure data sharing environment. For details on submitting a request, see the instructions provided at www.vivli.org.
Acknowledgments
The authors would like to thank all study participants. Medical writing assistance was provided by Koa Webster, PhD, and Prudence Stanford, PhD, CMPP, of ProScribe – Envision Pharma Group, and was funded by Eli Lilly Japan K.K. and Daiichi Sankyo Company, Limited. ProScribe’s services complied with international guidelines for Good Publication Practice.
Author Contributions
All authors made a significant contribution to the work reported, either in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas. All authors took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This study was sponsored by Eli Lilly Japan K.K. (Kobe, Japan), manufacturer of lasmiditan. Eli Lilly Japan K.K. was involved in the study design, data collection, data analysis, and preparation of the manuscript.
Disclosure
SK reports lecture fees from Daiichi Sankyo Company, Limited and Otsuka Pharmaceutical Co., Ltd., outside the submitted work. NI reports payments or honoraria for lectures and presentations from Eli Lilly Japan K.K. and Daiichi Sankyo Company, Limited, during the conduct of the study; personal fees from Otsuka Pharmaceutical, Amgen, and Sawai Pharmaceutica, outside the submitted work. YT, AO, and MK are employees of Eli Lilly Japan K.K. and have minor shareholdings in Eli Lilly and Company. The authors report no other conflicts of interest in this work.
References
1. GBD 2016 Headache Collaborators. Global, regional, and national burden of migraine and tension-type headache, 1990–2016: a systematic analysis for the global burden of disease study 2016. Lancet Neurol. 2018;17(11):954–976. doi:10.1016/S1474-4422(18)30322-3
2. Sakai F, Igarashi H. Prevalence of migraine in Japan: a nationwide survey. Cephalalgia. 1997;17(1):15–22. doi:10.1046/j.1468-2982.1997.1701015.x
3. Hirata K, Ueda K, Komori M, et al. Comprehensive population-based survey of migraine in Japan: results of the ObserVational Survey of the Epidemiology, tReatment, and Care Of MigrainE (OVERCOME [Japan]) study. Curr Med Res Opin. 2021;37(11):1945–1955. doi:10.1080/03007995.2021.1971179
4. Clemow DB, Baygani SK, Hauck PM, Hultman CB. Lasmiditan in patients with common migraine comorbidities: a post hoc efficacy and safety analysis of two phase 3 randomized clinical trials. Curr Med Res Opin. 2020;36(11):1791–1806. doi:10.1080/03007995.2020.1808780
5. Loo LS, Ailani J, Schim J, et al. Efficacy and safety of lasmiditan in patients using concomitant migraine preventive medications: findings from SAMURAI and SPARTAN, two randomized phase 3 trials. J Headache Pain. 2019;20(1):84. doi:10.1186/s10194-019-1032-x
6. González-Hernández A, Marichal-Cancino BA, MaassenVanDenBrink A, Villalón CM. Side effects associated with current and prospective antimigraine pharmacotherapies. Expert Opin Drug Metab Toxicol. 2018;14(1):25–41. doi:10.1080/17425255.2018.1416097
7. Nelson DL, Phebus LA, Johnson KW, et al. Preclinical pharmacological profile of the selective 5-HT1F receptor agonist lasmiditan. Cephalalgia. 2010;30(10):1159–1169. doi:10.1177/0333102410370873
8. Kuca B, Silberstein SD, Wietecha L, et al. Lasmiditan is an effective acute treatment for migraine: a phase 3 randomized study. Neurology. 2018;91(24):e2222–e2232. doi:10.1212/wnl.0000000000006641
9. Goadsby PJ, Wietecha LA, Dennehy EB, et al. Phase 3 randomized, placebo-controlled, double-blind study of lasmiditan for acute treatment of migraine. Brain. 2019;142(7):1894–1904. doi:10.1093/brain/awz134
10. Shapiro RE, Hochstetler HM, Dennehy EB, et al. Lasmiditan for acute treatment of migraine in patients with cardiovascular risk factors: post-hoc analysis of pooled results from 2 randomized, double-blind, placebo-controlled, phase 3 trials. J Headache Pain. 2019;20(1):90. doi:10.1186/s10194-019-1044-6
11. Sakai F, Takeshima T, Homma G, Tanji Y, Katagiri H, Komori M. Phase 2 randomized placebo-controlled study of lasmiditan for the acute treatment of migraine in Japanese patients. Headache. 2021;61(5):755–765. doi:10.1111/head.14122
12. Komori M, Mimura H, Tsai M, Ozeki A, Takaichi G, Wilbraham D. Safety, tolerability, and pharmacokinetics of lasmiditan in healthy Japanese and caucasian subjects. Jpn J Clin Pharmacol Ther. 2020;51(3):119–127. doi:10.3999/jscpt.51.119
13. Hirata K, Matsumori Y, Tanji Y, Khanna R, Ozeki A, Komori M. Safety profile of lasmiditan in patients with migraine in an Asian population. Expert Opin Drug Saf. 2022;22(1):91–101. doi:10.1080/14740338.2022.2087630
14. Hashimoto Y, Komori M, Tanji Y, Ozeki A, Hirata K. Lasmiditan for single migraine attack in Japanese patients with cardiovascular risk factors: subgroup analysis of a phase 2 randomized placebo-controlled trial. Expert Opin Drug Saf. 2022;21(12):1495–1503. doi:10.1080/14740338.2022.2078302
15. Lamb YN. Lasmiditan: first approval. Drugs. 2019;79(18):1989–1996. doi:10.1007/s40265-019-01225-7
16. Headache Classification Subcommittee of the International Headache Society. The international classification of headache disorders: 2nd edition. Cephalalgia. 2004;24(Suppl 1):9–160. doi:10.1111/j.1468-2982.2003.00824.x
17. Lipton RB, Stewart WF, Sawyer J, Edmeads JG. Clinical utility of an instrument assessing migraine disability: the Migraine Disability Assessment (MIDAS) questionnaire. Headache. 2001;41(9):854–861. doi:10.1111/j.1526-4610.2001.01156.x
18. Stewart WF, Lipton RB, Dowson AJ, Sawyer J. Development and testing of the Migraine Disability Assessment (MIDAS) Questionnaire to assess headache-related disability. Neurology. 2001;56(6 suppl 1):S20–S28. doi:10.1212/wnl.56.suppl_1.s20
19. Lasmiditan succinate tablet [package insert; in Japanese]. Tokyo: Eli Lilly Japan K.K.; 2022.
20. Dunkley EJC, Isbister GK, Sibbritt D, Dawson AH, Whyte IM. The Hunter serotonin toxicity criteria: simple and accurate diagnostic decision rules for serotonin toxicity. QJM. 2003;96(9):635–642. doi:10.1093/qjmed/hcg109
21. Sternbach H. The serotonin syndrome. Am J Psychiatry. 1991;148(6):705–713. doi:10.1176/ajp.148.6.705
22. Hirata K, Ueda K, Ye W, et al. Factors associated with insufficient response to acute treatment of migraine in Japan: analysis of real-world data from the Adelphi migraine disease specific programme. BMC Neurol. 2020;20(1):274. doi:10.1186/s12883-020-01848-4
23. Ram CVS. Antihypertensive drugs: an overview. Am J Cardiovasc Drugs. 2002;2(2):77–89. doi:10.2165/00129784-200202020-00002
24. Wiysonge CS, Bradley HA, Volmink J, Mayosi BM, Opie LH. Beta-blockers for hypertension. Cochrane Database Syst Rev. 2017;1(1):CD002003. doi:10.1002/14651858.CD002003.pub5
25. Diener H-C, Holle-Lee D, Nägel S, et al. Treatment of migraine attacks and prevention of migraine: guidelines by the German Migraine and Headache Society and the German Society of Neurology. Clin Transl Neurosci. 2019;3(1):1–40. doi:10.1177/2514183X18823377
26. Lanteri-Minet M, Valade D, Geraud G, Lucas C, Donnet A. Revised French guidelines for the diagnosis and management of migraine in adults and children. J Headache Pain. 2014;15(1):2. doi:10.1186/1129-2377-15-2
27. Steiner TJ, Jensen R, Katsarava Z, et al. Aids to management of headache disorders in primary care (2nd edition): on behalf of the European Headache Federation and Lifting The Burden: the Global Campaign against Headache. J Headache Pain. 2019;20(1):57. doi:10.1186/s10194-018-0899-2
28. Worthington I, Pringsheim T, Gawel MJ, et al. Canadian Headache Society guideline: acute drug therapy for migraine headache. Can J Neurol Sci. 2013;40(suppl 3):S1–S80. doi:10.1017/S0317167100118943
29. Headache Clinical Practice Guideline Development Committee. Clinical Practice Guideline for Headache Disorders 2021. Tokyo: Igaku-Shoin; 2021. Japanese.
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.