Back to Journals » Journal of Pain Research » Volume 18
Large-Channel Interlaminar Endoscopic Discectomy for Highly Migrated Lumbar Disc Herniation: Effectiveness and Safety
Authors Zheng S ![]() , Zhao Q, Hu Z, Li H, Wang B, Zhu Z, Qiu Y, Sun X
, Zhao Q, Hu Z, Li H, Wang B, Zhu Z, Qiu Y, Sun X
Received 28 April 2025
Accepted for publication 25 July 2025
Published 1 August 2025 Volume 2025:18 Pages 3821—3832
DOI https://doi.org/10.2147/JPR.S537181
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Andrea Tinnirello
Shicheng Zheng, Qinghua Zhao, Zongshan Hu, Haibo Li, Bin Wang, Zezhang Zhu, Yong Qiu, Xu Sun
Division of Spine Surgery, Department of Orthopedic Surgery, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China
Correspondence: Xu Sun, Division of Spine Surgery, Department of Orthopedic Surgery, Nanjing Drum Tower Hospital, Affiliated Hospital of Medical School, Nanjing University, Nanjing, Jiangsu, People’s Republic of China, Email [email protected]
Purpose: Highly migrated lumbar disc herniation (HM-LDH) presents a significant challenge for surgeons. This study aimed to assess the safety and clinical outcomes of large-channel interlaminar endoscopic discectomy for HM-LDH and compare it to open fenestration discectomy.
Patients and Methods: Patients who underwent large-channel interlaminar endoscopic discectomy (group A) or open fenestration discectomy (group B) for HM-LDH between January 2021 and December 2023 were included. Radiological and clinical outcomes were evaluated over at least one year. Operation time, intraoperative blood loss, postoperative drainage, postoperative hospital stay, patient-reported outcomes and complications were compared between groups, independent sample t-tests and Fisher’s exact probability test were performed for two groups.
Results: One hundred and thirty-six patients were retrospectively included in this study, with 84 in group A and 52 in group B, respectively. Although similar operative time was observed in group A and group B, group A was detected with significantly less intraoperative blood loss (17.6 ± 6.0 mL vs 101.7 ± 62.0 mL, P = 0.003) and shorter postoperative hospital stay (2.4 ± 0.6 days vs 5.2 ± 2.2 days, P < 0.001). Additionally, postoperative drainage was required in group B (35.9 ± 26.4 mL), but none in group A. Follow-up durations averaged 22.8 ± 4.9 months for group A and 20.2 ± 4.2 months for group B. Both groups achieved a significant improvement in VAS, ODI and EQ-5D scores without significant differences. No case experienced neurological deficits and reoperation after surgery in either group. The overall percentage of patients with good to excellent results according to modified MacNab criteria of group A was 95.2%, versus 92.3% of group B.
Conclusion: For the treatment of HM-LDH, large-channel interlaminar endoscopic discectomy is an effective and safe treatment.
Keywords: spine endoscopy, open fenestration discectomy, highly migrated disc herniation, clinical effectiveness
Introduction
Low back pain and leg pain are the leading causes of disability worldwide, with lumbar disc herniation (LDH) being one of the most common underlying causes.1,2 Migrated LDH represents a distinct subset of LDH, characterized with an upward or downward migration of the nucleus pulposus caused by complete rupture of the annulus fibrosus.3 When the nucleus pulposus extends beyond the height of the posterior disc margin, it is classified as highly migrated lumbar disc herniation (HM-LDH).4 Due to the nucleus pulposus breaking through the annulus fibrosus or the posterior longitudinal ligament into the spinal canal, this type of LDH typically presents with severe clinical symptoms, in which, conservative treatment usually fails and surgical intervention is commonly recommended.5
Conventional open fenestration discectomy used to be a standard procedure in treating LDH.6 For the treatment of HM-LDH, open fenestration discectomy typically requires dissecting of paraspinal muscles and removing substantial part of lamina either superiorly or inferiorly, which can lead to long-term complications such as chronic back pain and spinal instability.7–9 Additionally, open fenestration discectomy still has disadvantages of unclear vision, residual fragments, considerable blood loss, and the need of drainage.10
In recent years, percutaneous endoscopic lumbar discectomy (PELD) has been widely used to treat LDH.11 Generally, it can be divided into two approaches: transforaminal endoscopic lumbar discectomy (TELD) and interlaminar endoscopic lumbar discectomy (IELD).12 When employing TELD for the treatment of HM-LDH, extensive resection of the facet joints and pedicles is often required to achieve complete exposure due to the obstruction of the pedicles, facet joints, and ligaments of the intervertebral foramen.13–15 Nonetheless, residual fragments, incomplete decompression, and even the need for reoperation do occur occasionally after TELD treatment.16
Since Ruetten et al17 first proposed a minimally invasive approach via interlaminar window in treating LDH, IELD has experienced significant development and wide application, especially in L5/S1 segment. However, for HM-LDH, particularly at the L4/5 segment where the interlaminar space is relatively narrow, complete removal of the migrated disc may be rather challenging. Kim et al4 reported an 88.2% success rate (15/17) for IELD in a series of cases with HM-LDH and two patients with failed L4/5 IELD had to receive a second IELD procedure through the L5/S1 interlaminar window.
Large-channel interlaminar endoscopic discectomy, a IELD technique performed under a large channel, can achieve a similar decompression effect to conventional surgery.18,19 Due to its larger working channel, it can provide a larger surgical exploration area and ensure sufficient decompression.20 Additionally, it provides a wider range of swing, a broader field of view, and a more comprehensive exploration, facilitating the detection of residual migrated nucleus pulposus tissue, which makes this approach suitable for a wide range of indications in contrast to other endoscopic spinal surgery systems.21–23 Several studies reported that large-channel interlaminar endoscopic discectomy for treating LDH can achieve clinical outcomes similar to open fenestration discectomy,24,25 but no studies have compared the effectiveness of these two procedures in treating HM-LDH.
Evaluating the clinical outcomes of minimally invasive techniques in challenging cases such as HM-LDH is an important contribution to surgical practice, as a result of which, this study aimed to investigate the effectiveness and safety of large-channel interlaminar endoscopic discectomy in treating HM-LDH. Additionally, we intended to illustrate the minimum-one-year radiological and clinical outcomes of large-channel interlaminar endoscopic discectomy in treating HM-LDH in comparison with open fenestration discectomy. It was hypothesized that large-channel interlaminar endoscopic discectomy might take the advantages of less trauma and shorter hospital stay.
Methods
Study Design and Patient Population
The study was approved by our Institutional Ethics Review Board (Ethical number: 2025–0289-01). As shown in Figure 1, we reviewed a series of patients with HM-LDH who had undergone single-level L4/5 or L5/S1 large-channel interlaminar endoscopic discectomy or open fenestration discectomy between January 2021 and December 2023 in our center. To minimize clinical outcome variability due to surgical experience and professional skills, all surgeries were performed by a single surgeon (XS) who had at least ten years’ experience in spine surgery and at least two years of experience in PELD surgery.
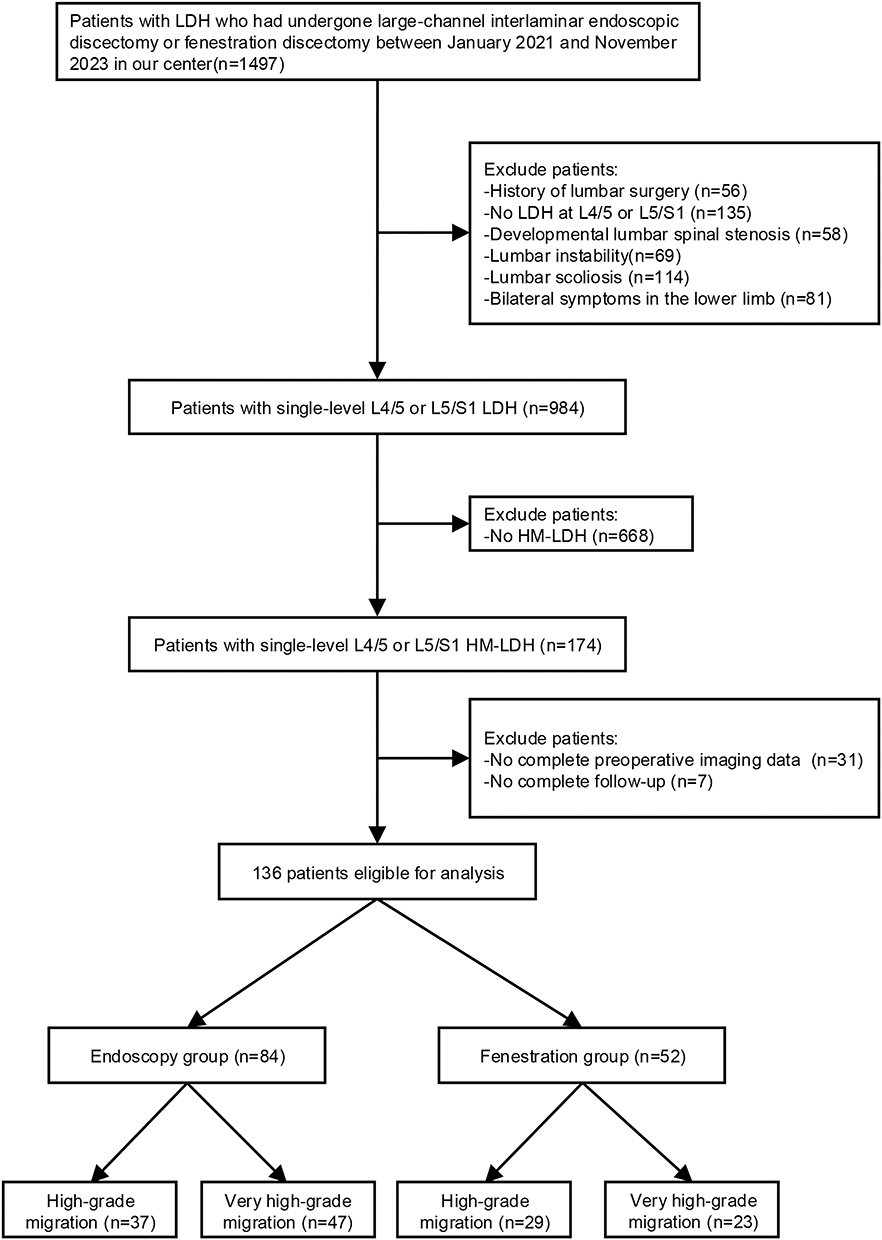 |
Figure 1 Study flow diagram showing the inclusion and exclusion of patients. |
Patients included in this study had to meet the following criteria: (1) MRI confirming L4/5 or L5/S1 single-segment HM-LDH, (2) unilateral radiating pain and numbness in the lower limb, and (3) had received conservative measures for more than 12 weeks but failed. Exclusion criteria were as follows: (1) history of lumbar surgery, (2) concomitant developmental spinal stenosis, instability, scoliosis, or inflammation of lumbar spine, and (3) inability to tolerate surgery due to other severe diseases. Written informed consent was obtained from each patient.
Enrolled patients who had undergone large-channel interlaminar endoscopic discectomy were assigned to group A, while those had undergone open fenestration discectomy were assigned to group B.
Assessment of HM-LDH
According to Ahn’s classification system,26 disc migration was classified into seven zones based on the direction and extent of migration observed on preoperative MRI imaging: very high-grade upward; high-grade upward; low-grade upward; disc level; low-grade downward; high-grade downward and very high-grade downward (Figure 2). The high-grade migration was characterized by the extent of migration beyond 3 mm below the inferior margin of the upper pedicle (high-grade upward) or below the middle of the lower pedicle (high-grade downward). Very high-grade migration was defined as a migration that beyond the inferior margin of the upper pedicle (very high-grade upward) or the inferior margin of the lower pedicle (very high-grade downward) (Figure 3).
 |
Figure 2 Schematic diagram illustrating migrated lumbar disc herniation, categorized into seven zones based on the direction and degree of migration. |
 |
Figure 3 Preoperative MRI of HM-LDH. (A) High‐grade upward migration; (B) Very high‐grade upward migration; (C) High‐grade downward migration; (D) Very high‐grade downward migration. The white arrow indicates the direction of the migrated herniated disc. |
Surgical Techniques
Each surgery was performed under general anesthesia. All patient was placed in the prone position on an arch-shaped operating table, and the lumbar region was maintained in an appropriate flexed position to widen the interlaminar window. The skin entry point and the lesion segments were confirmed with the assistance of anterior-posterior fluoroscopy. After regular disinfection and draping, we performed the following two types of surgeries.
Large-Channel Interlaminar Endoscopic Discectomy
The selection of the entry point is not at the traditional position directly facing the intervertebral space. Instead, the location of the migrated disc determines whether the puncture site is chosen to be on the cranial or the caudal side of the lateral margin of the interlaminar window. Once the entry point is determined, an 18-gauge spinal needle was carefully inserted into the target position. Subsequently, a 1.2-cm skin incision was made around the needle, followed by the sequential insertion of dilators until they reached the level of the ligamentum flavum. A working cannula was then introduced, and the final position was checked on the anteroposterior (AP) and lateral fluoroscopic images. The large channel-endoscope (iLESSYS-Delta, Joimax, Germany) was placed through the cannula, and the ligamentum flavum was exposed by dissecting the surrounding soft tissues. Throughout the procedure, a bipolar radiofrequency electrode (DTF-40, Elliquence, America) was employed for hemostasis. Under the endoscope, the upper and lower margins of the lamina, as well as the interlaminar window, were clearly visible. Based on the location of the migrated disc, either the cephalic or caudolateral portion of the lamina was meticulously removed using an endoscopic high-speed burr or a laminar rongeur. To improve the visibility of the spinal canal, a tiny section of the medial facet joint could be resected, with careful attention to preserving the stability of the facet joint and the integrity of the pars. Once the exposure was adequate, a portion of the ligamentum flavum was carefully dissected to reveal the dural sac and the nerve root. By adjusting the angle of the endoscope, the shoulder and axilla of the nerve root were thoroughly explored, ensuring that the compressed nerve root and the intervertebral disc were fully visible. With gentle retraction of the nerve root, the herniated disc fragment was identified and subsequently removed using forceps. Following this, an assessment of the distal end of the migrated disc was conducted to detect any residual disc tissue. The endpoint for endoscopic decompression was established by confirming the unobstructed movement of the exposed nerve root and the strong pulsation of the dural sac. Once this endpoint was verified, the surgical procedure was successfully concluded. Finally, the working cannula was carefully removed, and the incision was closed after hemostasis, with no need for drainage (Figure 4).
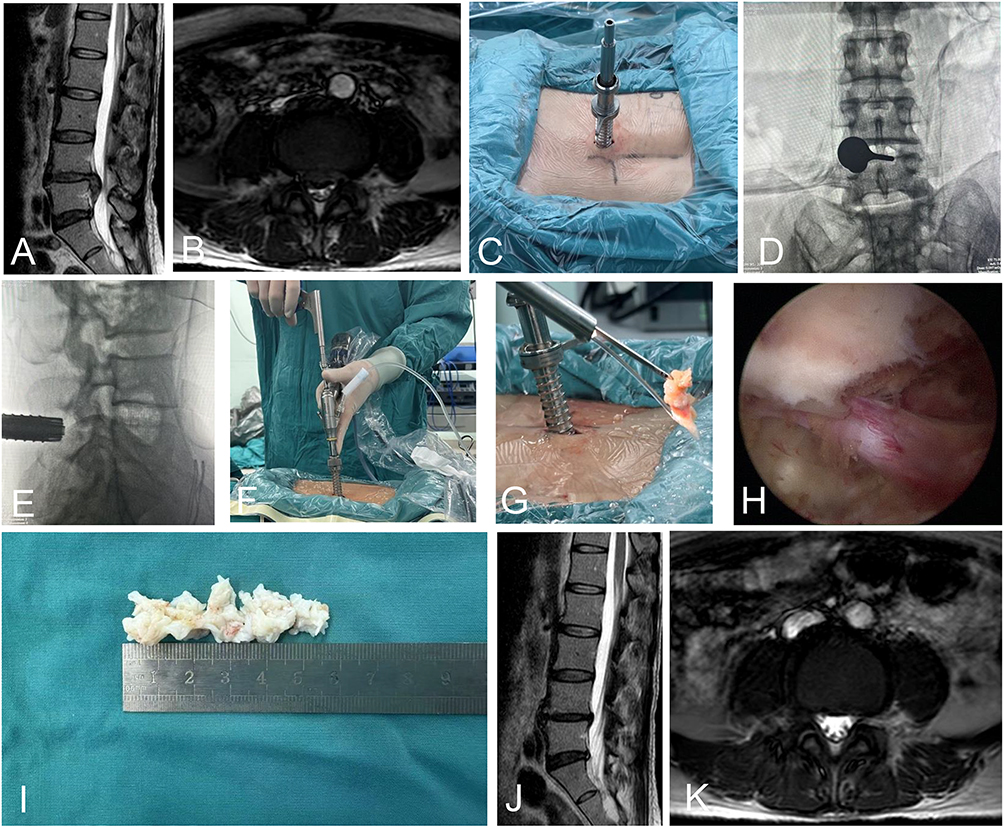 |
Figure 4 A 49‐year‐old female with very high‐grade downward migration underwent large-channel interlaminar endoscopic discectomy. (A and B) The preoperative MRI showed that the migrated intervertebral disc from the L4-L5 disc level to the L5 lower end plate. (C-G) Properly placed the large-channel endoscopy under the C-arm fluoroscope and perform endoscopic discectomy during surgery. (H) Under endoscopic visualization, thorough decompression was achieved. (I) The nucleus pulposus removed during surgery. (J and K) The MRI taken 15 months after the surgery showed no recurrence of disc herniation or migration. |
Open Fenestration Discectomy
A 4-cm longitudinal median skin incision was made and dissection was performed to fully expose the superior and inferior lamina and zygapophyseal joint of the target segment. By using Kerrison rongeur, lamina was partially removed to fully expose herniated disc and nerve roots. After herniated intervertebral disc tissues were exposed, migrated nucleus pulposus and residual diseased tissues in intervertebral disc were removed. Confirming that the dura sac and nerve root was completely decompressed, a drainage tube were introduced and the incision was sutured layer by layer to conclude the surgery.
Postoperative Management
Standard postoperative treatment was administered, including medication measures to alleviate pain and reduce swelling. After 24 hours of bed rest, patients in group A were encouraged to sit and walk while wearing a lumbar brace. In group B, drainage tube was routinely removed no later than 24 hours after surgery. All patients were advised to avoid excessive lifting, bending, and twisting for one month, and also to incorporate moderate lumbar and back muscle exercises into their daily routine activities. Quality of life (QOL) scores at 3, 6, and 12 months postoperatively were recorded to evaluate clinical efficacy, MRI examinations were conducted on postoperative 3 months and 12 months to assess the decompression effectiveness and identify the condition of the intervertebral discs at the surgical segment.
Clinical Data and QOL Measures
The hospital information system was used to collect clinical records. Follow-up data were collected via telephone interview or via electronic questionnaire at the outpatient clinic. Patient demographic characteristics, including baseline data, smoking history and comorbidities (diabetes and hypertension) were obtained.
Clinical records including level of migrated LDH (L4/5 or L5/S1), side of disc herniation (left or right), condition of disc migration (direction and degree), duration of disease, operation time, follow-up duration, intraoperative blood loss, postoperative drainage and postoperative hospital stay were collected. Visual Analog Scale (VAS) for pain on the back, buttock and legs, the Oswestry Disability Index (ODI) and the European Quality of Life-5 Dimensions (EQ-5D) were used to assess QOL of patients preoperatively and postoperatively. The modified MacNab criteria were used at 12 months postoperatively to assess patients’ satisfaction on the surgery.
Statistical Analysis
All data were analyzed using SPSS Statistics (SPSS Inc., Chicago, IL, USA). The Kolmogorov–Smirnov test was used to determine whether the variables followed a normal distribution. The continuous variables (age, BMI, duration of disease, follow-up time, clinical records, VAS, ODI, EQ-5D) were in accordance with approximate normal distribution and presented as mean ± standard deviation (x± SDs). Categorical variables (gender, smoking status, comorbidities, level of migrated LDH, side of disc herniation, direction of migration, degree of migrated LDH and modified MacNab were expressed as number (percentages). With regards to comparisons between group A and group B, independent sample t-test was used for continuous variables, and chi-square test or Fisher’s exact probability test was used to examine categorical ones. Histograms and line charts were generated through Prism 9 software (GraphPad Software, San Diego, California, USA). When p value < 0.05, it was considered statistically significant.
Results
Patient Demographic Data
This study finally enrolled a total of 136 patients (89 males and 47 females), with 84 in group A and 52 in group B respectively. As shown in Table 1, there were 37 patients with high-grade migration and 47 patients with very high-grade migration in group A while 29 with high-grade migration and 23 patients with very high-grade migration in group B. No statistically significant differences were observed between the two groups in terms of age, gender, BMI, smoking status, comorbidities, level of migrated LDH, side of disc herniation, direction of disc migration, degree of migrated LDH and follow-up time (P > 0.05).
 |
Table 1 Demographic Data in 136 Patients with Highly Migrated Lumbar Disc Herniation |
Surgical Results and Radiological Results
The surgeries of both groups were successfully completed. As shown in Table 2, the intraoperative blood loss was significantly less in group A than in group B (17.6 ± 6.0 mL vs 101.7 ± 62.0 mL, P = 0.003). The postoperative hospital stay was also significantly shorter in group A compared to group B (2.4 ± 0.6 days vs 5.2 ± 2.3 days, P < 0.001). The surgery time for group A was slightly shorter, but there was no significant difference. (P = 0.074). Patients in group B averagely had a drainage of 35.9 ± 26.4 mL, while none in group A needed a drainage tube. Except for one case of delayed wound healing in Group B, other patients’ wounds healed by primary intention. All patients in group A achieved primary healing of surgical wounds.
 |
Table 2 Surgical Data of the 136 Patients with Highly Migrated Lumbar Disc Herniation |
As shown in Table 3, complications such as dural tear, neurologic deterioration, symptomatic hematoma and surgical site infection were not observed. During the surgery, one case in group A experienced facet injury, while two cases in group B experienced facet injury. All of them received conservative treatment. No recurrence of herniation or migration was observed in group A and B. No significant difference in the complication rates was observed between two groups (P = 1.000).
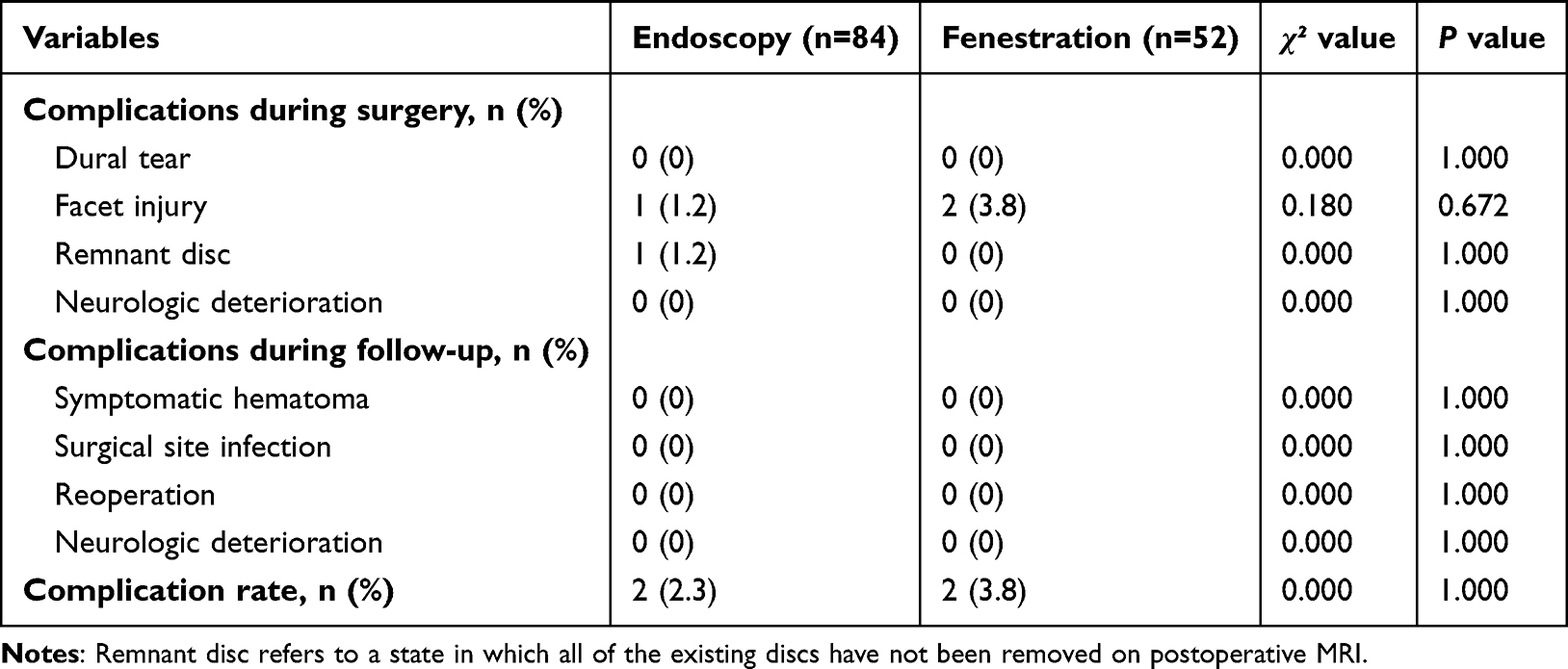 |
Table 3 Complications of the 136 Patients with Highly Migrated Lumbar Disc Herniation |
Clinical Results
As shown in Figure 5, the postoperative VAS and ODI scores significantly decreased compared with the preoperative scores (P < 0.05). The symptoms continued to improve at different time points after surgery in both groups. The mean VAS (back), VAS (buttock) and VAS (leg) scores in group A improved from 5.5 ± 3.0, 5.3 ± 3.3 and 7.10 ± 2.8 preoperatively to 2.2 ± 1.7, 1.6 ± 0.6 and 1.6 ± 0.6 at 3 months postoperatively, which further improved to 1.5 ± 0.7, 1.1 ± 0.6 and 1.1 ± 0.4 at the final follow-up, respectively. The mean ODI scores improved from 53.3 ± 24.1% preoperatively to 13.4 ± 2.7% at 3 months postoperatively, which further improved to 7.7 ± 2.4% at the final follow-up. The mean VAS (back), VAS (buttock), VAS (leg) scores and mean ODI scores in group A were comparative with group B. According to the modified MacNab criteria, the rate of excellent or good outcomes in group A was 95.2%, versus 92.3% in group B. At the final follow-up, the EQ-5D scores in both groups demonstrated significant increases, but no statistically significant differences were observed between the groups. Moreover, we found that there were no significant differences in clinical outcomes between patients with high-grade migration and those with very high-grade migration in either group.
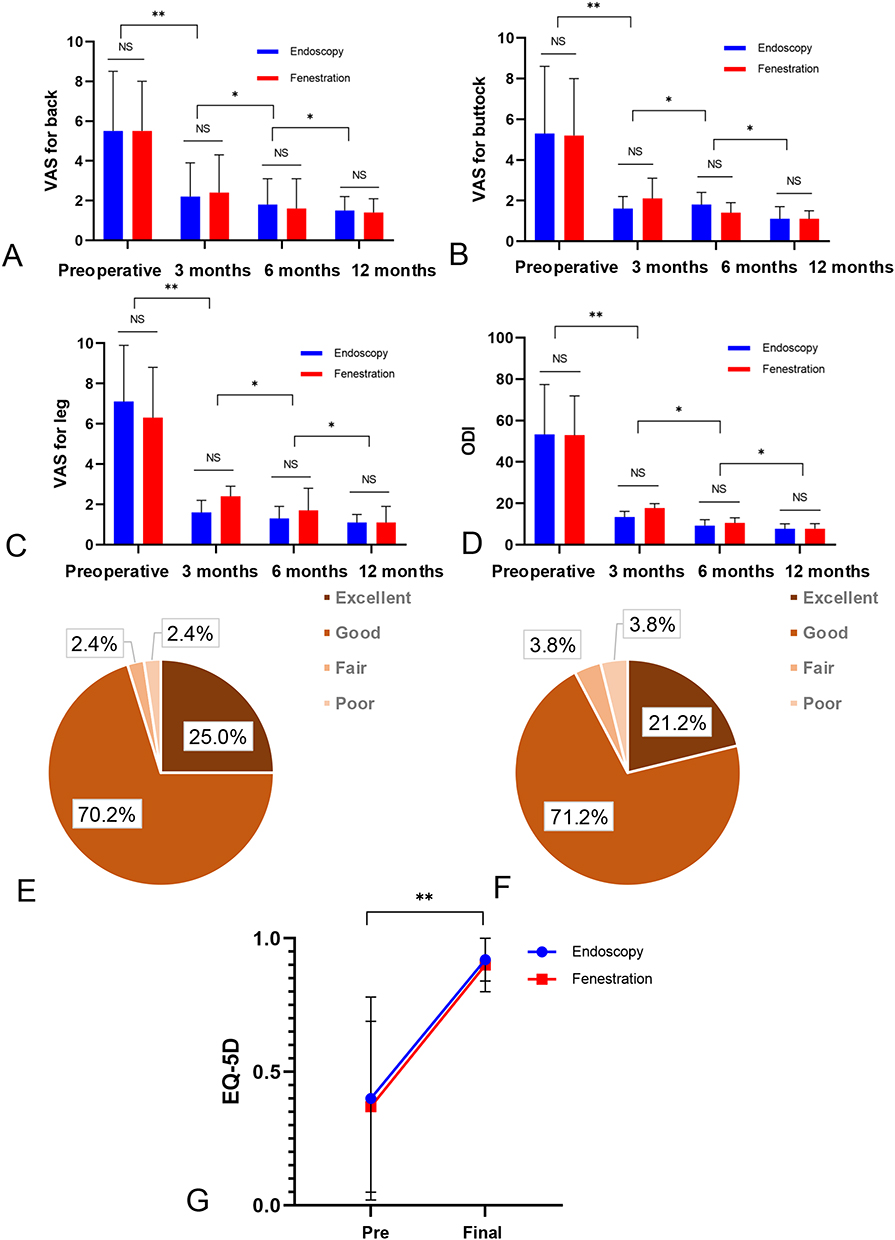 |
Figure 5 Patient-reported outcomes at different time points. (A-C) Changes in VAS scores during the follow-up between groups A and B. (D) Changes in ODI scores during the follow-up between groups A and B. (E) At the last follow-up, patient satisfaction in group A was evaluated according to the MacNab criteria. (F) At the last follow-up, patient satisfaction in group B was evaluated according to the MacNab criteria. (G) At the final follow-up, the improvement in EQ-5D scores was assessed for patients in groups A and B. Notes: NS, no significant difference; *P < 0.05, **P < 0.01, comparison within groups. |
Discussion
The present study was the first to investigate the safety and effectiveness of large-channel interlaminar endoscopic discectomy in treating patients with HM-LDH. In our study, open fenestration discectomy was used as a reference. Our results revealed that large-channel interlaminar endoscopic discectomy for the treatment of HM-LDH can achieve clinical effectiveness comparable to that of open fenestration discectomy with less blood loss and shorter hospital stay.
HM-LDH is a rather more severe type of LDH which often requires surgical treatment.3 Open fenestration discectomy is the classical surgical procedure for LDH and is widely accepted by spine surgeons because of its simplicity, low osteotomy rate, low impact on spinal stability, and validity,27 but it presents many technical challenges in the management of HM-LDH.7–9 In this study, we introduced the large-channel interlaminar endoscopic discectomy to manage HM-LDH. Compared to traditional spine endoscopy, the large-channel endoscopy has a larger working channel (1 cm in diameter), which supports the use of a larger Kerrison punch, grinding drill, and nucleus pulposus forceps for better decompression.20 Moreover, this endoscopy allows for a wider oscillating range, wider field of view, and more thorough exploration, allowing for the detection of residual prolapsed nucleus pulposus tissue. Under clear illumination, continuous saline irrigation, and a visual field magnification system, migrated nucleus pulposus can be detected, thereby reducing the risk of residual nucleus pulposus.21–23 In our study, group A had relatively shorter operation time. Moreover, no cases required reoperation during the follow-up. Therefore, large-channel endoscopy can serve as an alternative option for the treatment of HM-LDH.
As shown in our study, for HM-LDH, large-channel interlaminar endoscopic discectomy has several advantages. First, compared with group B, group A was associated with less intraoperative blood loss (17.6 ± 6.0mL vs 101.7 ± 62.0mL, P<0.001). This finding was consistent with the report by Fei et al.28 This may be due to the smaller incision (1.2cm) and lesser dissection of the paravertebral muscles. Moreover, bipolar radiofrequency allows precise haemostasis of the perineural tissue, resulting in less intraoperative blood loss.24 Second, patients in group A had a shorter postoperative hospital stay than group B (2.4 ± 0.6 days vs 5.2 ± 2.2 days, P<0.001), which was similar to the results reported by Sheng et al29 and Yang et al.30 This may be attributed to the minimal damage to the bony structures, muscles, and ligamentous complex caused by endoscopic discectomy, as well as the absence of drainage, all of which contribute to a faster postoperative recovery.31 Third, group A did not increase the incidence of complications (2.3% vs 3.8%, P = 1.000), which was similar to the 5% reported by Oertel.32 This was due to the clear endoscopic vision, precise decompression, and shorter operative time, reducing the possibility of accidental injury to vital tissues. Notably, endoscopic surgery can still achieve clinical efficacy comparable to open fenestration discectomy while possessing the aforementioned advantages.
Large-channel endoscopy is relatively wide and mainly used for the lower lumbar spine, since the spinal canal at the L4/5 and L5/S1 segments is relatively spacious, which allows the accommodation of such endoscopes. But it also carries the risk of injury to the facet joint or the pars, particularly during removal of migrated nucleus pulposus at the L4/5 level. In our study, group A remained a risk of facet joint injury (1.2% vs 3.8%, P = 0.672). Excessive bony resection or drilling to widen the narrow interlaminar window may inadvertently violate the medial facet capsule or articular surface. Additionally, excessive lateral inclination during fragment retrieval can lead to unintended abrasion or fracture of the facet joint. Therefore, when performing laminectomy under the endoscope, attention should be paid to protecting the pars and excessive oscillation should be avoided to prevent damage to the facet joint. Fortunately, none of the patients experienced pain due to facet joint injury after conservative treatment and lumbar and back muscle exercises. Moreover, the mean operation time was slightly shorter than that of open fenestration discectomy because of the small incision size, limited operating space and additional surgical steps required for endoscopic discectomy such as cannula installation and device connection. More time is needed to correctly identify anatomical structures, and surgeons need to be familiar with the instruments.24 As well as the need for the surgeon to operate without tactile sensation, the understanding of three-dimensional anatomy through two-dimensional imaging underneath, and the training cycle for manual dexterity, which caused the steeper learning curve.33 A research report34 states that the learning curve for IELD stabilizes after 50 cases. This has important implications for clinical practice, as the surgeon’s experience not only significantly affects the learning curve but also impacts the outcomes of these surgeries. Our study involved a surgeon with over 500 cases of endoscopic surgical experience, and the results demonstrate that proficiency in performing large-channel endoscopic discectomy can yield favorable clinical outcomes. However, it is important to acknowledge that novice surgeons may require more time to achieve consistent results with this technique, which may affect the success rate in real-world clinical settings.
This study has several limitations. First, it was a non-randomized retrospective study, and it was inevitable that there will be biases in the selection and collection of cases. Therefore, prospective randomized controlled trials need to be carried out to further verify our findings. Second, all the operations were performed by the same experienced surgeon, which may limit the generalizability of the results. In the future, multi-center studies involving surgeons with different levels of skills are needed to determine the clinical outcomes of these two techniques. Third, this study only enrolled patients with over-one-year follow-up, a long-term follow-up study is needed to further verify the results.
Conclusion
For the treatment of HM-LDH, large-channel interlaminar endoscopic discectomy can not only lessen blood loss, shorten postoperative hospital stay, but also achieve similar clinical outcome to open fenestration discectomy. Therefore, it is an effective and safe treatment for HM-LDH.
Ethics Statement
This study was approved by the ethics committee of Nanjing Drum Tower Hospital (2025-0289-01). The study was performed in accordance with the principles of the Helsinki Declaration of 1964 and its later amendments. All patients provided informed consent for participation in the study and research publication.
Acknowledgments
The authors acknowledge the Imaging Department and Operation Department of Nanjing Drum Tower Hospital, for their technical support and expertise in the radiological assessments.
Funding
This study was supported by the Clinical Research Project of Nanjing Drum Tower Hospital (2024-LCYJ-MS-04).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Özüdoğru A, Canlı M, Ceylan İ, Kuzu Ş, Alkan H, Karaçay B. Five times sit-to-stand test in people with non-specific chronic low back pain-a cross-sectional test-retest reliability study. Ir J Med Sci. 2023;192(4):1903–1908. doi:10.1007/s11845-022-03223-3
2. Zhang AS, Xu A, Ansari K, et al. Lumbar disc herniation: diagnosis and management. Am J Med. 2023;136(7):645–651. doi:10.1016/j.amjmed.2023.03.024
3. Fardon DF, Williams AL, Dohring EJ, Murtagh FR, Gabriel Rothman SL, Sze GK. Lumbar disc nomenclature: version 2.0: recommendations of the combined task forces of the North American spine society, the American society of spine radiology and the American society of neuroradiology. Spine J. 2014;14(11):2525–2545. doi:10.1016/j.spinee.2014.04.022
4. Kim CH, Chung CK, Woo JW. Surgical outcome of percutaneous endoscopic interlaminar lumbar discectomy for highly migrated disk herniation. Clin Spine Surg. 2016;29(5):E259–66. doi:10.1097/BSD.0b013e31827649ea
5. Rogerson A, Aidlen J, Jenis LG. Persistent radiculopathy after surgical treatment for lumbar disc herniation: causes and treatment options. Int Orthop. 2019;43(4):969–973. doi:10.1007/s00264-018-4246-7
6. Li T, Zhang J, Ding Z, Jiang Q, Ding Y. Percutaneous endoscopic lumbar discectomy versus open fenestration discectomy for lumbar disc herniation: a retrospective propensity score-matched study with more than 5 years of follow-up. J Orthop Surg Res. 2024;19(1):753. doi:10.1186/s13018-024-05239-0
7. Li X, Han Y, Di Z, et al. Percutaneous endoscopic lumbar discectomy for lumbar disc herniation. J Clin Neurosci. 2016;33:19–27. doi:10.1016/j.jocn.2016.01.043
8. Bokov A, Isrelov A, Skorodumov A, Aleynik A, Simonov A, Mlyavykh S. An analysis of reasons for failed back surgery syndrome and partial results after different types of surgical lumbar nerve root decompression. Pain Physician. 2011;14(6):545–557. doi:10.36076/ppj.2011/14/545
9. Fritsch EW, Heisel J, Rupp S. The failed back surgery syndrome: reasons, intraoperative findings, and long-term results: a report of 182 operative treatments. Spine. 1996;21(5):626–633. doi:10.1097/00007632-199603010-00017
10. Hamawandi SA, Sulaiman II, Al-Humairi AK. Open fenestration discectomy versus microscopic fenestration discectomy for lumbar disc herniation: a randomized controlled trial. BMC Musculoskelet Disord. 2020;21(1):384. doi:10.1186/s12891-020-03396-x
11. Ljungqvist O, Scott M, Fearon KC. Enhanced recovery after surgery: a review. JAMA Surg. 2017;152(3):292–298. doi:10.1001/jamasurg.2016.4952
12. Pan M, Li Q, Li S, et al. Percutaneous endoscopic lumbar discectomy: indications and complications. Pain Physician. 2020;23(1):49–56.
13. Li ZZ, Hou SX, Shang WL, Song KR, Zhao HL. Modified percutaneous lumbar foraminoplasty and percutaneous endoscopic lumbar discectomy: instrument design, technique notes, and 5 years follow-up. Pain Physician. 2017;20(1):E85–e98. doi:10.36076/ppj.2017.1.E85
14. Lee S, Kim SK, Lee SH, et al. Percutaneous endoscopic lumbar discectomy for migrated disc herniation: classification of disc migration and surgical approaches. Eur Spine J. 2007;16(3):431–437. doi:10.1007/s00586-006-0219-4
15. Gadjradj PS, van Tulder MW, Dirven CM, Peul WC, Harhangi BS. Clinical outcomes after percutaneous transforaminal endoscopic discectomy for lumbar disc herniation: a prospective case series. Neurosurg Focus. 2016;40(2):E3. doi:10.3171/2015.10.Focus15484
16. Krzok G. Transforaminal endoscopic surgery: outside-in technique. Neurospine. 2020;17(Suppl 1):S44–s57. doi:10.14245/ns.2040128.064
17. Ruetten S, Komp M, Merk H, Godolias G. Use of newly developed instruments and endoscopes: full-endoscopic resection of lumbar disc herniations via the interlaminar and lateral transforaminal approach. J Neurosurg Spine. 2007;6(6):521–530. doi:10.3171/spi.2007.6.6.2
18. Lee CH, Choi M, Ryu DS, et al. Efficacy and safety of full-endoscopic decompression via interlaminar approach for central or lateral recess spinal stenosis of the lumbar spine: a meta-analysis. Spine. 2018;43(24):1756–1764. doi:10.1097/brs.0000000000002708
19. Kim HS, Paudel B, Jang JS, et al. Percutaneous full endoscopic bilateral lumbar decompression of spinal stenosis through uniportal-contralateral approach: techniques and preliminary results. World Neurosurg. 2017;103:201–209. doi:10.1016/j.wneu.2017.03.130
20. Perez-Roman RJ, Basil GW, Boddu JV, Bashti M, Wang MY. Size matters - From the working channel to the wavelength of light: optimizing visualization in endoscopic spine surgery. J Clin Neurosci. 2022;105:73–78. doi:10.1016/j.jocn.2022.08.024
21. Lee CW, Yoon KJ, Ha SS. Comparative analysis between three different lumbar decompression techniques (microscopic, tubular, and endoscopic) in lumbar canal and lateral recess stenosis: preliminary report. Biomed Res Int. 2019;2019:6078469. doi:10.1155/2019/6078469
22. Lee CW, Yoon KJ, Jun JH. Percutaneous endoscopic laminotomy with flavectomy by uniportal, unilateral approach for the lumbar canal or lateral recess stenosis. World Neurosurg. 2018;113:e129–e137. doi:10.1016/j.wneu.2018.01.195
23. Middleton SD, Wagner R, Gibson JNA. Multi-level spine endoscopy: a review of available evidence and case report. EFORT Open Rev. 2017;2(7):317–323. doi:10.1302/2058-5241.2.160087
24. Zhu X, Zhao Y, Liu K, Zhang Y, Cheng L. Clinical outcomes of fenestration discectomy and iLESSYS-Delta interlaminar endoscopic system for treatment of LDH: a single-center retrospective cohort study. Sci Rep. 2024;14(1):20087. doi:10.1038/s41598-024-70973-8
25. Meng SW, Peng C, Zhou CL, et al. Massively prolapsed intervertebral disc herniation with interlaminar endoscopic spine system Delta endoscope: a case series. World J Clin Cases. 2021;9(1):61–70. doi:10.12998/wjcc.v9.i1.61
26. Ahn Y, Jeong TS, Lim T, Jeon JY. Grading system for migrated lumbar disc herniation on sagittal magnetic resonance imaging: an agreement study. Neuroradiology. 2018;60(1):101–107. doi:10.1007/s00234-017-1943-7
27. Alvi MA, Kerezoudis P, Wahood W, Goyal A, Bydon M. Operative approaches for lumbar disc herniation: a systematic review and multiple treatment meta-analysis of conventional and minimally invasive surgeries. World Neurosurg. 2018;114:391–407.e2. doi:10.1016/j.wneu.2018.02.156
28. Zhang F, Ye D, Zhang W, Sun Y, Guo L, Li J. Efficacy of lumbar decompression under large-channel spinal endoscope in elderly patients with segmental lumbar spinal stenosis. J Orthop Surg Res. 2024;19(1):16. doi:10.1186/s13018-023-04389-x
29. Sheng Y, Li J, Chen L, et al. Delta large-channel technique versus microscopy-assisted laminar fenestration decompression for lumbar spinal stenosis: a one-year prospective cohort study. BMC Musculoskelet Disord. 2023;24(1):43. doi:10.1186/s12891-023-06143-0
30. Yang F, Ren L, Ye Q, et al. Endoscopic and microscopic interlaminar discectomy for the treatment of far-migrated lumbar disc herniation: a retrospective study with a 24-month follow-up. J Pain Res. 2021;14:1593–1600. doi:10.2147/jpr.S302717
31. Ma C, Li H, Zhang T, et al. Comparison of percutaneous endoscopic interlaminar discectomy and open fenestration discectomy for single-segment huge lumbar disc herniation: a two-year follow-up retrospective study. J Pain Res. 2022;15:1061–1070. doi:10.2147/jpr.S352595
32. Oertel JM, Burkhardt BW. Endoscopic intralaminar approach for the treatment of lumbar disc herniation. World Neurosurg. 2017;103:410–418. doi:10.1016/j.wneu.2017.03.132
33. Gadjradj PS, Vreeling A, Depauw PR, Schutte PJ, Harhangi BS. Surgeons learning curve of transforaminal endoscopic discectomy for sciatica. Neurospine. 2022;19(3):594–602. doi:10.14245/ns.2244342.171
34. Jamaleddine Y, Haj Hussein A, Honeine MO, et al. Evaluating the learning curve and operative time of interlaminar and transforaminal endoscopic lumbar discectomy. Brain Spine. 2025;5:104225. doi:10.1016/j.bas.2025.104225
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.