Back to Journals » Patient Preference and Adherence » Volume 19
Knowledge, Practices, and Barriers to Diabetes Self-Management Among Patients with Type 2 Diabetes in a Rwandan Referral Hospital
Authors Munezero MC ![]() , Bagweneza V, Kubahoniyesu T
, Bagweneza V, Kubahoniyesu T ![]() , Collins A
, Collins A
Received 7 July 2025
Accepted for publication 30 October 2025
Published 3 November 2025 Volume 2025:19 Pages 3409—3419
DOI https://doi.org/10.2147/PPA.S552026
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 5
Editor who approved publication: Dr Ramón Morillo-Verdugo
Marie Colombe Munezero,1 Vedaste Bagweneza,1 Theogene Kubahoniyesu,2 Anita Collins3
1School of Nursing and Midwifery, College of Medicine and Health Sciences, University of Rwanda, Kigali, Rwanda; 2African Centre of Excellence in Data Science, University of Rwanda, Kigali, Rwanda; 3Rory Meyer’s College of Nursing, New York University, New York, NY, USA
Correspondence: Marie Colombe Munezero, Email [email protected]
Background: Effective self-management is essential for controlling type 2 diabetes mellitus (T2DM) and preventing complications. However, patients often encounter barriers that compromise adherence to recommended care practices. This study aimed to assess the level of knowledge, self-care practices, and barriers to diabetes self-management among patients attending a Rwandan referral hospital.
Methods: This quantitative study was conducted at University Teaching Hospital of Kigali (CHUK) using a cross-sectional design. Data were collected from 140 patients with type 2 diabetes mellitus (T2DM) through a self-administered structured questionnaire. Participants were recruited using a systematic sampling technique. Data analysis was performed using the Statistical Package for the Social Sciences (SPSS) version 20, employing both descriptive statistics and logistic regression to identify factors associated with barriers to diabetes self-management.
Results: The majority of participants (73.6%) reported regularly engaging in diabetes self-care practices, with 74.3% demonstrating an adequate understanding of the condition. Despite positive self-care behaviors, 60.7% of participants reported facing significant barriers, primarily related to financial constraints and lack of adequate information from healthcare providers. Multivariate analysis revealed that certain sociodemographic factors were significantly associated with the presence of self-management barriers. Patients aged 50– 59 years (Adjusted Odds Ratio (AOR) = 1.235, p = 0.025), married patients (AOR = 1.32, p = 0.019), and those in Ubudehe Category 1 (AOR = 1.934, p = 0.032) were more likely to report barriers. In contrast, having university-level education (AOR = 0.527, p = 0.023) and residing in urban areas (AOR = 0.304, p = 0.041) were protective factors.
Conclusion: While many patients demonstrated regular self-care and fair knowledge of T2DM, a significant number still face barriers, especially those related to financial hardship and limited health education. Tailored interventions that improve diabetes literacy and reduce socioeconomic inequalities are essential to enhance effective self-management and long-term outcomes for patients living with diabetes in Rwanda.
Keywords: type two diabetes, self-care management, barriers, Rwanda
Background
Diabetes mellitus, particularly type 2, has become one of the most pressing public health challenges of our time.1 Across the globe, millions of people live with this chronic condition, which not only demands lifelong treatment but also requires consistent, daily self-management. In 2024, the International Diabetes Federation (IDF) estimated that about 589 million adults aged between 20 and 79 were living with diabetes worldwide, and this number is expected to rise significantly in the coming decades.2 If current trends continue, global prevalence could reach 783 million by 2045. Much of this increase is anticipated in low- and middle-income countries, where health systems are often less equipped to handle the long-term needs of patients with chronic diseases.
In sub-Saharan Africa, the diabetes burden is growing quickly. The region recorded approximately 24 million people with diabetes in 2021, and projections indicate this figure could more than double by 2045.3 Rwanda, like many African countries, has not been immune to this trend. Recent national assessments highlight a rising Non-communicable diseases (NCD) burden and growing service demand for diabetes care in Rwanda.4 The World Health Organization (WHO) STEPS survey conducted in 2021 estimated the national diabetes prevalence at around 12%. However, programmatic and hospital-based reports suggest that urban areas may be seeing a higher and more complex burden.5 Rwanda’s health financing context, including the community-based health insurance (Mutuelle de Santé) and cost-sharing policies, shapes patient access to diagnostics, medicines, and routine follow-up, As Rwanda continues to make strides in controlling infectious diseases, non-communicable conditions like diabetes are beginning to take center stage in the country’s public health agenda.
Living with diabetes involves much more than taking medication. It requires individuals to develop a deep understanding of their condition and consistently practice self-care behaviors such as monitoring blood glucose, adhering to diet, exercising, and attending regular follow-up.6 Studies have shown that people who are actively engaged in their own care have better blood glucose control and a lower risk of complications. Yet for many patients, especially those in low-resource settings, managing diabetes day-to-day is not straightforward.7 They often face a host of challenges some related to knowledge gaps, others to financial hardship or limited access to support and health education.
Several studies from different African contexts have emphasized these barriers. In Ethiopia, research conducted at the University of Gondar Hospital found that while general knowledge about diabetes was relatively high, patients still struggled with understanding chronic complications and how to prevent them.8 Similar findings were reported in Ghana and South Africa, where economic stress, medication shortages, and gaps in health communication were cited as key obstacles.9,10 In Mexico, patients spoke about the strain of managing their condition in environments where both resources and social support were lacking. These examples reflect a broader pattern of motivated patients constrained by structural and informational barriers.
In Rwanda, published evidence on patient-reported self-management barriers remains limited, despite recent national assessments of the diabetes care cascade. Most existing studies have focused on prevalence or biomedical aspects, leaving a gap in our understanding of the social and behavioral factors that influence diabetes management.11 Understanding barriers within Rwanda’s referral pathway (health posts/centers - district hospitals - national referral hospitals such as CHUK) and within insurance and cost-sharing arrangements is essential to interpret whether obstacles are primarily individual or system-level.
To frame these interactions, we draw on the Capability, Opportunity, and Motivation (COM-B model) as proximal drivers of Behavior and the WHO Innovative Care for Chronic Conditions (ICCC) framework. COM-B emphasizes patient knowledge/skills (capability), environmental/resources and service access (opportunity), and beliefs/intentions (motivation) as levers for sustained self-care. The ICCC framework complements this by situating patient behaviours within health-system organization and community support, clarifying where barriers may arise and where interventions should target.12
With this context, the present study examines patient knowledge, self-care practices, and perceived barriers among adults with T2DM attending at CHUK, anchoring findings within the country’s referral and financing architecture.
Materials and Methods
Study Design
This study employed a cross-sectional design to assess the level of knowledge, self-care practices, and perceived barriers to self-management among patients with type 2 diabetes mellitus (T2DM). The design was chosen as it allows the collection of data at a single point in time, which is appropriate for understanding the current experiences and behaviors of patients within the clinical setting. We prespecified outcomes (presence of ≥1 self-management barrier versus none) and analytic covariates, and documented procedures in a study operations manual.
Study Setting
The study was conducted at University Teaching Hospital of Kigali(CHUK), a national referral and teaching hospital located in Kigali, Rwanda. CHUK provides specialized care to patients from across the country, including those with chronic conditions such as diabetes. The diabetic outpatient clinic at CHUK served as the primary site for data collection, as it provides routine follow-up and education to T2DM patients. The diabetic clinic at CHUK operates every day with for T2DM follow-ups, providing medications, glucose strips where eligible, and education per national guidelines.
Study Population and Sample
The study population comprised adult patients diagnosed with type 2 diabetes mellitus who were receiving follow-up care at the CHUK diabetic clinic. A total of 140 participants were recruited using a systematic sampling technique. Recruitment occurred April 1–May 31, 2019, whereby eligible and available patients during clinic visits were invited to participate.
Inclusion and Exclusion Criteria
Inclusion criteria were age ≥18 years, confirmed T2DM per [WHO 2019 / ADA 2022] diagnostic criteria (FPG ≥7.0 mmol/L [126 mg/dL], 2-h OGTT ≥11.1 mmol/L [200 mg/dL], random plasma glucose ≥11.1 mmol/L with symptoms, or HbA1c ≥6.5%; confirmation on a separate day when required, and the ability to complete the questionnaire in Kinyarwanda or English. Exclusion criteria were type 1 diabetes, critical illness, cognitive impairment precluding consent, or refusal to participate. Eligibility was verified from clinic records.
Study Instrument
Data were collected using a structured, self-administered questionnaire adapted from the Self-Care Inventory (SCI) for the Rwandan context. The instrument comprised 62 items across four domains: (i) sociodemographics (12 items), (ii) diabetes knowledge (18 items, true/false/do not-know; sample items include risk factors, treatment, complications), (iii) self-care practices (20 items, 5-point Likert: never/rarely/sometimes/often/always; domains include glucose monitoring, diet, physical activity, medication adherence, and clinic attendance), and (iv) perceived barriers (12 items, yes/no plus open-ended prompts covering affordability, transport, information, time, and supplies).
Scoring
Knowledge items were scored 1 for correct and 0 for incorrect/do not-know (range 0–18); “knowledgeable” was defined a priori as ≥70% correct (≥13/18). Self-care items were scored 1–5 (higher indicates better adherence), with subscale means reported. The primary outcome (any barrier) was coded 1 if ≥1 barrier was endorsed, else 0.
Adaptation and Validation
The instrument underwent forward–back translation (Kinyarwanda-English) by independent translators with reconciliation by a third reviewer. A panel of 5–7 experts (endocrinology, nursing, public health, behavioral science) rated item relevance (4-point scale); item-level content validity indices (I-CVI) and the scale-level S-CVI/Ave were computed, and items with I-CVI <0.78 were revised or removed (S-CVI/Ave = [value]). Cognitive debriefing with 8–12 clinic patients assessed clarity and cultural appropriateness, prompting minor wording adjustments.
Reliability
Internal consistency was acceptable to excellent. Cronbach’s α was 0.90 for the overall instrument, 0.78 for the knowledge domain (KR-20 for dichotomous items), 0.88 for self-care practices, and 0.74 for barriers. In a pilot subsample (n = 14) reassessed after 14 days, test–retest reliability showed ICC (2, 1) of 0.86 (95% CI 0.72–0.93) for the total score; domain ICCs were 0.82 (95% CI 0.63–0.91) for knowledge, 0.88 (95% CI 0.76–0.94) for self-care, and 0.79 (95% CI 0.56–0.90) for barriers (Appendix/Supplement Table S1).
Data Collection Process
The principal researcher, trained in human subjects’ protection and standardized instrument administration, approached potential participants in the clinic waiting area, obtained written informed consent, and supervised self-administration using a standardized script. Clarifications were limited to neutral explanations. Questionnaires were completed in a private area and returned the same day. We tracked item-level missingness; for subscales with ≤10% missing items, scores were prorated; otherwise, the subscale was set to missing. “Don’t know” responses were coded incorrect in the knowledge scale.
Sample Size and Power
We aimed to estimate the prevalence of any self-management barrier with a [desired precision ±d at 95% CI] and to model associations with key covariates. A priori, assuming a barrier prevalence of [p≈0.60], [Z=1.96], and margin of error [d], the minimum sample was 140. Ultimately, 140 participants were enrolled; with ~85 events (60.7%), the events-per-variable (EPV) for ~8 predictor groups are ≈10–11, at the lower recommended threshold. We therefore (i) collapsed categories for sparse variables, (ii) limited parameters, and (iii) performed Firth-penalized logistic regression as sensitivity. We acknowledge the risk of imprecise odds ratios due to limited EPV.
Data Analysis
The continuous variables were summarized with means (SD) or medians (IQR) and categorical variables with counts (percentages). For the primary outcome (any barrier vs none), we fit multivariable logistic regression including prespecified covariates: age group, sex, marital status, education, occupation (collapsed), residence (urban/rural), and Ubudehe category. We assessed multicollinearity (VIF<5), linearity in the logit (for any continuous predictors), and model fit (Hosmer–Lemeshow; calibration plot). Missing data were handled primarily by complete-case analysis; m=20 was used in sensitivity analyses with similar inferences. Two-sided α=0.05. Analyses were conducted in SPSS v20.
Ethical Considerations
Ethical approval for this study was secured from the University Teaching Hospital of Kigali (CHUK) (Reference: EC/CHUK/044/2019) and the University of Rwanda College of Medicine and Health Sciences (CMHS) (Reference: CMHS/IRB/016/2019) before data collection. The study was conducted in full compliance with the ethical principles of the Declaration of Helsinki. All participants provided written informed consent after being fully informed about the study’s purpose, their rights, and the confidentiality protocols. The research strictly adhered to fundamental ethical principles, ensuring voluntary participation, respect for privacy, and the protection of participant identity throughout the entire process.
Results
Socio-Demographic Characteristics of Diabetic Patients
The study included 140 participants, most of whom were middle-aged and older adults. The majority were aged between 40 and 49 years (26.4%), followed closely by those aged 60 and above (25.7%) and those between 50 and 59 years (22.9%). Women made up the majority of respondents, accounting for nearly 68% of the total. Over half of the participants (50.7%) were married, while others were either single, divorced, widowed, or cohabiting.
When it came to education, about a third had completed secondary school (33.6%), while nearly 28% had only primary education, and around 23% had reached university level. A small portion roughly 9% had no formal education at all. In terms of occupation, a large number (60.7%) reported jobs that did not fall under common categories like farming or teaching, the rest were mostly crop farmers, educators, or cattle keepers.
The majority of participants (70%) were from urban areas, indicating easier access to the referral hospital where the study was conducted. In terms of socioeconomic classification, most belonged to Ubudehe Category 3 (82.9%), which typically includes individuals who are relatively better off economically (Table 1).
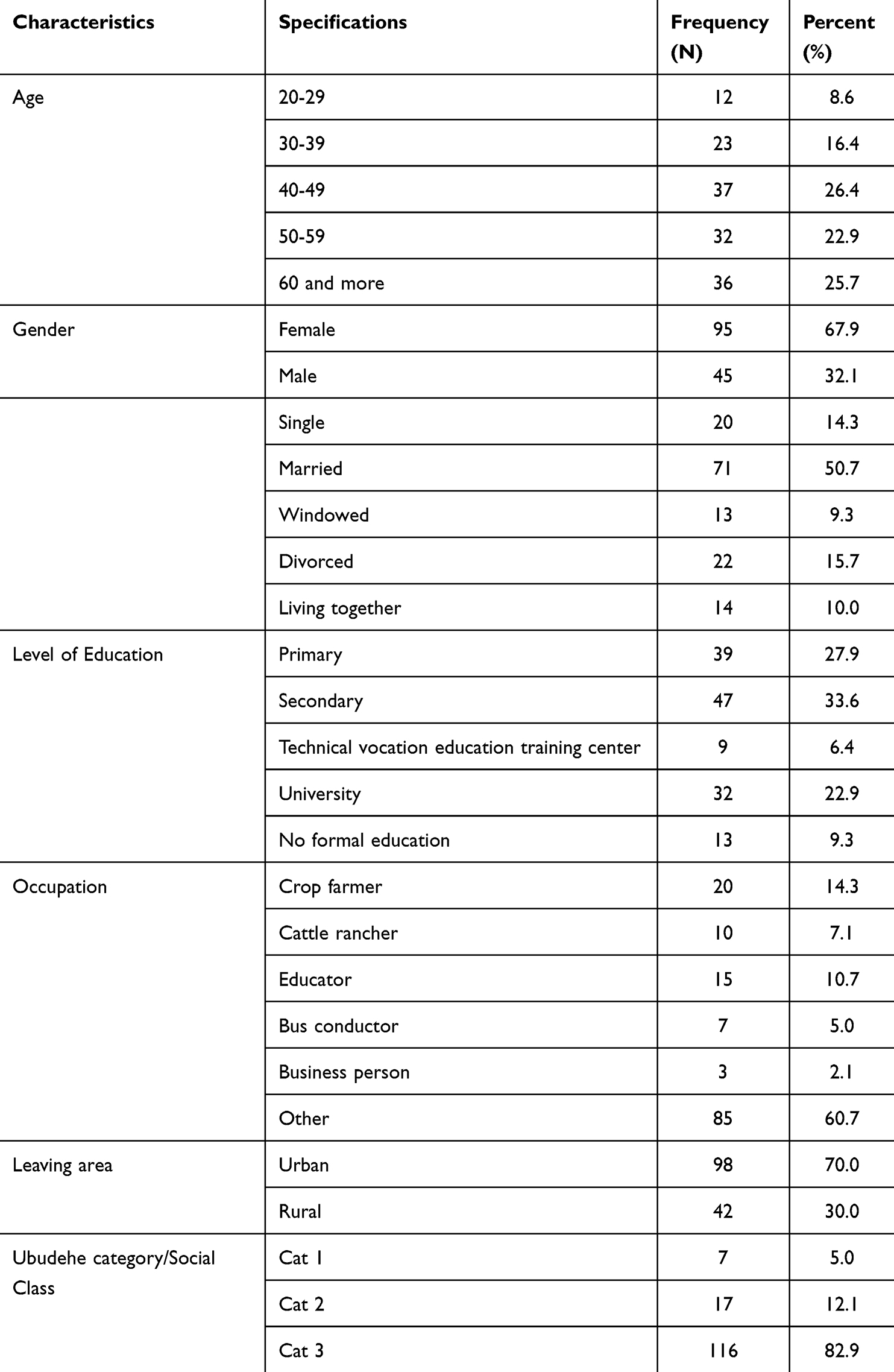 |
Table 1 Socio-Demographic Characteristics of Respondents |
Respondents’ Knowledge Regarding Type 2 Diabetes Mellitus
The findings reveal a varied understanding of type 2 diabetes among respondents across several domains (Table 2).
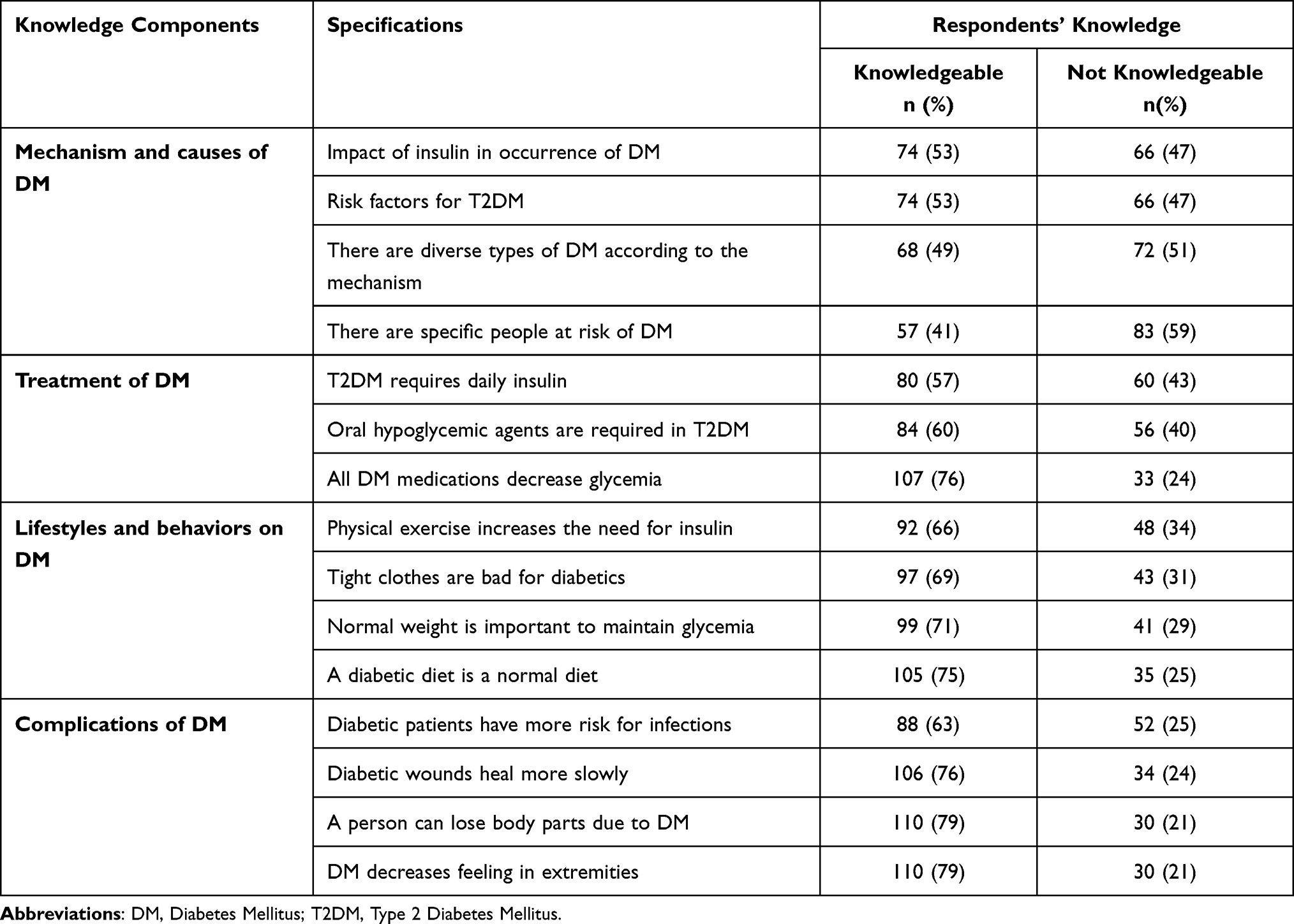 |
Table 2 Respondents’ Knowledge Regarding Type 2 Diabetes Mellitus |
In terms of disease mechanisms and causes, just over half (53%) correctly understood the role of insulin and common risk factors. However, fewer participants recognized that there are different types of diabetes based on mechanisms (49%) or that certain individuals are more at risk (41%). Knowledge regarding treatment was moderate. While 57% were aware that type 2 diabetes may require daily insulin, 60% understood the use of oral hypoglycemic agents, and a notable 76% correctly identified that all diabetes medications aim to lower blood sugar levels.
Respondents demonstrated stronger knowledge in lifestyle and behavioral aspects. A significant number acknowledged that physical exercise influences insulin needs (66%), tight clothing may be harmful for diabetics (69%), maintaining a healthy weight is essential for blood sugar control (71%), and a diabetic diet is essentially a normal healthy diet (75%). Awareness of diabetes-related complications was relatively high. About 79% recognized that diabetes can cause loss of sensation in extremities and potentially lead to amputation. Similarly, 76% knew that diabetic wounds heal more slowly, and 63% understood the increased risk of infections among diabetic patients.
Overall, 104 respondents (74.3%) were classified as knowledgeable. Knowledge was strongest in lifestyle and complication awareness but weaker in mechanisms and at-risk groups (Table 2). These knowledge levels are likely influenced by the sample: clinic-attending patients may have greater exposure to health education than the broader T2DM population, limiting generalizability.
Level of Diabetes Self-Care Management Among Respondents
Most participants (73.6%) reported regular engagement in self-care, while 26.4% practiced it only sometimes. Figure 1 shows the distribution, illustrating a substantial minority with irregular practices despite clinic follow-up (Figure 1).
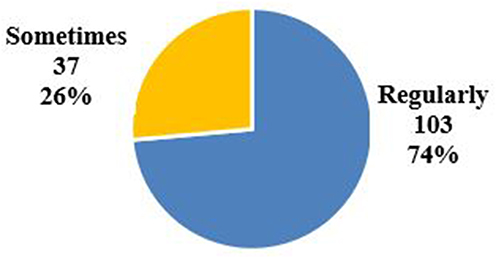 |
Figure 1 Distribution of diabetes self-care management practices among 140 respondents. Slices indicate proportion reporting “regular” versus “occasional” self-care across core domains. |
Respondents’ Barriers Regarding Type 2 Diabetes Mellitus Self-Management, with the Overall Barrier Level
The results highlight several barriers that patients face in managing their type 2 diabetes. One of the most common challenges was the lack of money, particularly for monitoring blood glucose at home, reported by 35% of respondents. Time constraints also emerged as a significant barrier to engaging in physical activity (40.7%), followed by a lack of understanding about the role of exercise in blood sugar control (20%). Regarding dietary adherence, financial limitations were again noted by 26.4%, and 21.4% of participants indicated that they had not received adequate information from healthcare providers about proper diabetic diets. Similarly, lack of guidance from healthcare personnel was reported as a barrier to medication adherence by 14.3% of respondents, and a small group (7.1%) mentioned missing meals around medication times as a challenge.
For attending follow-up appointments, 13.6% reported not having money for transportation, and a few noted long waiting times (5.7%) as a deterrent. In terms of skin care, an often-overlooked aspect of diabetes management, 9.3% admitted lacking knowledge about the potential complications’ diabetes can cause to the skin.
Overall, only 60.7% of the respondents were found to face significant barriers to diabetes self-management, suggesting that while a majority are relatively unhindered, a notable minority still experience challenges especially financial constraints and information gaps—that could compromise effective disease control (Table 3).
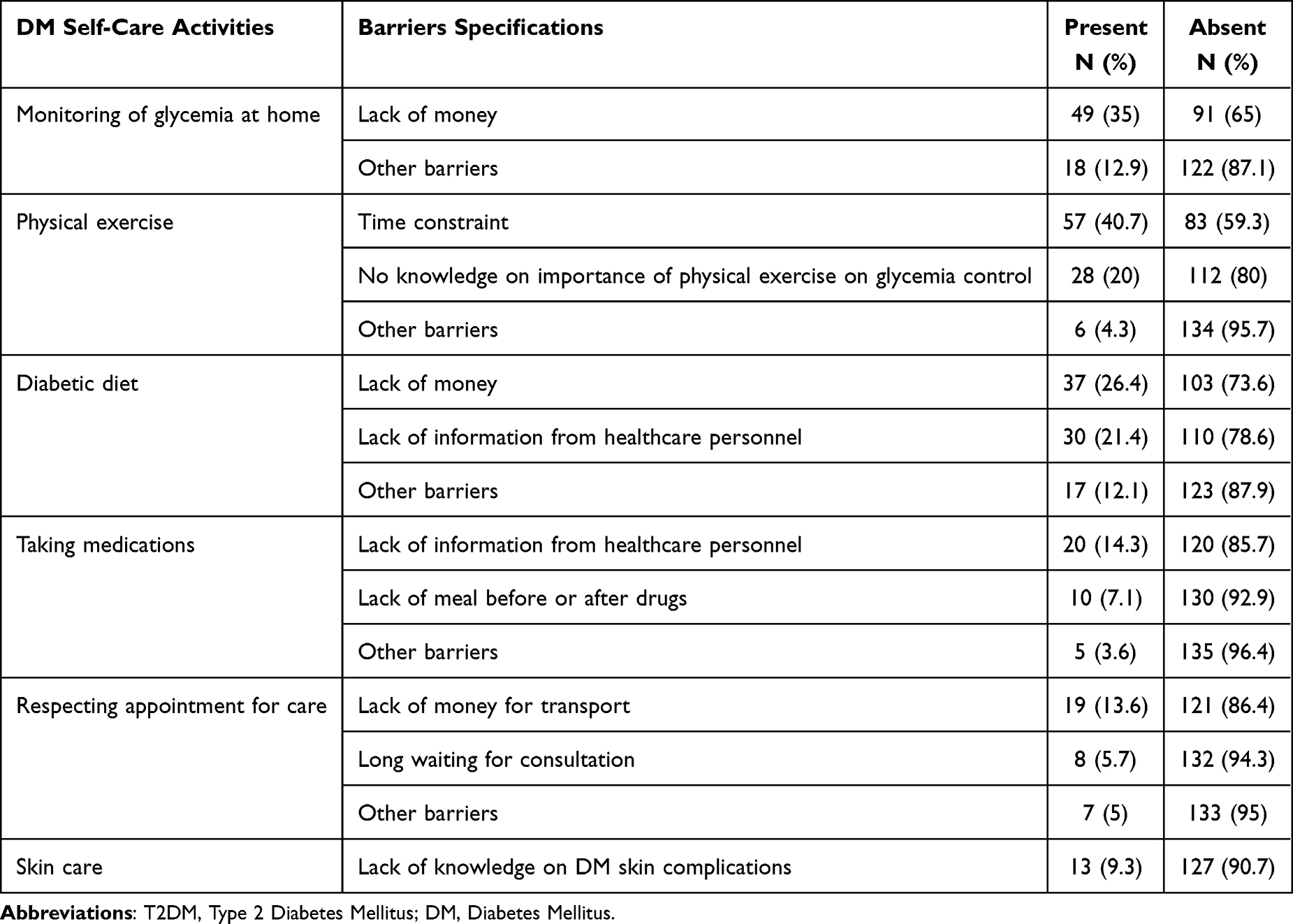 |
Table 3 Respondents’ Barriers Regarding Type 2 Diabetes Mellitus Self-Management |
Factors Associated with Barriers to Type 2 Diabetes Mellitus Self-Management
In the multivariate analysis, several sociodemographic characteristics were found to be significantly associated with barriers to type 2 diabetes mellitus self-management. Participants aged 50–59 years were significantly more likely to report barriers compared to those aged 60 and above (AOR = 1.235, 95% CI: 1.041–3.888, p = 0.025). Marital status was also a significant factor, with married respondents more likely to experience barriers than those living together (AOR = 1.32, 95% CI: 1.028–16.433, p = 0.019).
Education level appeared to play a protective role; those with university education were significantly less likely to encounter barriers compared to participants with no formal education (AOR = 0.527, 95% CI: 0.054–0.819, p = 0.023). In addition, place of residence was associated with differences in barriers: individuals residing in urban areas were significantly less likely to report barriers than those in rural areas (AOR = 0.304, 95% CI: 0.171–0.735, p = 0.041).
Lastly, socioeconomic status, as measured by the Ubudehe categorization, was a significant predictor. Respondents in Category 1 the most socioeconomically vulnerable were more likely to face barriers compared to those in Category 3 (AOR = 1.934, 95% CI: 1.083–10.501, p = 0.032) (Table 4).
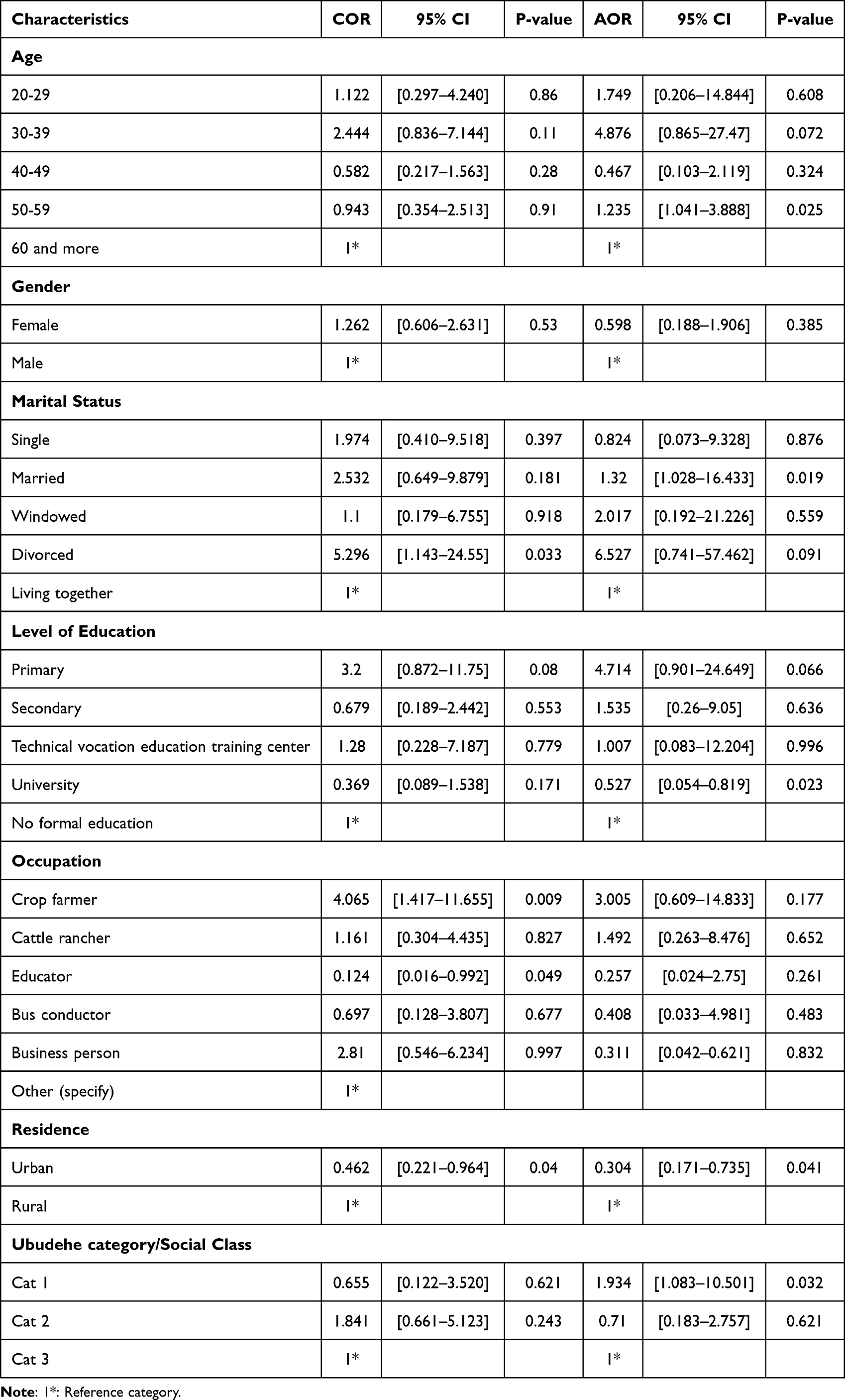 |
Table 4 Multivariate Analysis of Sociodemographic Factors Associated with Barriers to Type 2 Diabetes Mellitus Self-Management |
Discussion
This study examined knowledge, self-care practices, and barriers to T2DM self-management among patients attending Rwanda’s largest referral hospital. While the majority demonstrated regular self-care and moderate knowledge, a substantial proportion still reported barriers, particularly financial constraints and insufficient information from healthcare providers.
Findings revealed that while a majority of participants (73.6%) reported regularly engaging in diabetes self-care practices and 74.3% demonstrated a fair level of knowledge, a significant portion (60.7%) still faced notable barriers that could compromise effective diabetes control.
The overall knowledge level observed in our study is comparable to a study conducted in Ethiopia,13 where 85.6% of diabetic patients demonstrated good knowledge about the disease, though only 58.8% were knowledgeable about its chronic complications. In contrast, a study conducted in Thailand14 reported poor diabetes knowledge among 96.7% of patients, particularly in areas related to insulin use and general understanding of diabetes. Similarly, in Portugal,15 found that certain aspects of diabetes management such as recognizing signs of ketoacidosis and understanding dietary choices were poorly understood even among insulin-treated patients. These findings underscore that while general awareness may be moderate to high in some contexts, critical gaps in knowledge still persist globally.
In this study, financial constraints and lack of information from healthcare providers were the most commonly reported barriers to self-management. This aligns with findings from Ghana, where10 identified economic hardship, insufficient medication dosages, and limited diabetes education as major challenges. Similar barriers were reported in Mexico, where16 found that patients often struggled with cultural beliefs, limited family support, and healthcare system limitations. In South Africa,9 highlighted inadequate patient-provider communication and a disconnect between facility-based education and patients’ real-life experiences as major obstacles to self-management.
The findings of this study further revealed that certain sociodemographic factors were significantly associated with reported barriers. Participants aged 50–59 years, those who were married, and individuals from the most vulnerable economic group (Ubudehe Category 1) were more likely to experience difficulties in managing their diabetes. In contrast, university education and urban residence were associated with fewer barriers. This pattern mirrors the findings from India,17 where age and being employed in the medical field were associated with greater knowledge and likely better self-management. Similarly,14 in Thailand noted that individuals with at least a secondary education or employment had significantly better diabetes knowledge.
The protective role of education and urban residence may be attributed to better access to health information, stronger health literacy, and closer proximity to health services. This was also supported by findings from Gondar, Ethiopia,13 where individuals with higher education levels and longer disease duration had better awareness of complications, and from Portugal, where education correlated positively with knowledge in insulin-treated patients.
Despite the encouraging levels of knowledge and self-care practices in our study, the high proportion of respondents facing barriers points to a crucial gap between awareness and action. As emphasized by18 in a multi-national study, addressing self-management challenges requires a multidimensional approach combining education, socioeconomic support, and contextualized healthcare services. Without targeted interventions to bridge this gap, knowledge alone may not translate into sustained behavior change.
These findings have important implications. Addressing financial barriers will require revisiting the benefits package of Rwanda’s Mutuelle de Santé, particularly expanding coverage for essential supplies such as glucose-monitoring strips and dietary counseling. To overcome knowledge gaps, task-shifting should be considered: nurses and community health workers could be trained to deliver structured diabetes education sessions, supported by culturally adapted materials. Peer-support groups and family-centered programs could also mitigate the paradoxical barrier associated with marriage by engaging spouses and caregivers as allies in diabetes care.
Ultimately, knowledge alone is insufficient without system-level support. Policies that integrate financial protection, structured education, and workforce strengthening will be essential for reducing complications and improving the long-term quality of life of Rwandans living with diabetes.
Study Limitation
This study has some limitations. Its cross-sectional design limits causal interpretations, and being conducted in a single referral hospital reduces generalizability. the self-reported data are subject to recall and social desirability bias. Despite these limitations, the study provides valuable insights into diabetes self-management challenges in Rwandan context.
Conclusion
This study demonstrated that although many patients with type 2 diabetes mellitus showed moderate knowledge and consistent self-care practices, a large proportion still encountered barriers that threaten effective management. Financial hardship and insufficient information from healthcare providers were the most frequently reported obstacles. Importantly, higher education and urban residence emerged as protective factors, while socioeconomic vulnerability and rural residence increased the likelihood of facing barriers.
These findings highlight the dual need to address systemic constraints such as gaps in insurance coverage, limited workforce capacity, and unequal access to resources and patient-level challenges linked to knowledge and socioeconomic status. Policies that expand Mutuelle de Santé coverage for essential diabetes supplies, strengthen structured education and counseling through task-shifting to nurses and community health workers, and target rural and low-income populations with tailored support are particularly critical. By integrating both health-system and individual-level strategies, Rwanda can reduce disparities in diabetes self-management and improve long-term outcomes for people living with T2DM.
Acknowledgment
The authors acknowledge the management and staff of Kigali University Teaching Hospital for their support during the research process. Special appreciation goes to all patients who voluntarily participated in the study and provided valuable insights. The authors also acknowledge the contribution of data collectors and field assistants for their dedication and professionalism.
Author Contributions
MCM conceptualized the study, designed the methodology, and drafted the manuscript. TK led the data analysis and interpretation, and manuscript revision. Both VB and CA contributed to the literature review and critical revision of the manuscript. All authors made a significant contribution to the work reported, whether in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflict of interest regarding the publication of this manuscript.
References
1. World Health Organization. Diabetes. 2024. Available from: https://who.int/health-topics/diabetes.
2. IDF. Diabetes facts and figures. 2024. Available from: https://idf.org/about-diabetes/diabetes-facts-figures/.
3. Hossain MDJ, Al‐Mamun MD, Islam MDR. Diabetes mellitus, the fastest growing global public health concern: early detection should be focused. Health Sci Rep. 2024;7(3):e2004. doi:10.1002/hsr2.2004
4. MoH. National strategy and costed action plan for the prevention and control of non-communicable diseases in Rwanda. 2020.
5. Dukunde A, Marie Ntaganda J, Kasozi J, Nzabanita J. Prediction of prevalence of type 2 diabetes in Rwanda using the metropolis-hasting sampling. Afr H Sci. 2021;21(2):702–709. doi:10.4314/ahs.v21i2.28
6. Ahmad F, Joshi SH. Self-care practices and their role in the control of diabetes: a narrative review. Cureus. 2023;15(7). doi:10.7759/cureus.41409
7. Adhikari M, Devkota HR, Cesuroglu T. Barriers to and facilitators of diabetes self-management practices in Rupandehi, Nepal- multiple stakeholders’ perspective. BMC Public Health. 2021;21(1):1269. doi:10.1186/s12889-021-11308-4
8. Aschalew AY, Yitayal M, Minyihun A. Health-related quality of life and associated factors among patients with diabetes mellitus at the University of Gondar referral hospital. Health Qual Life Outcomes. 2020;18(1):62. doi:10.1186/s12955-020-01311-5
9. Masupe T, Onagbiye S, Puoane T, Pilvikki A, Alvesson HM, Delobelle P. Diabetes self-management: a qualitative study on challenges and solutions from the perspective of South African patients and health care providers. Global Health Action. 2022;15(1):2090098. doi:10.1080/16549716.2022.2090098
10. Tetteh C, Saah FI, Amu H. Diabetes self-management: a qualitative study of education needs, practices and caregiver support in the Keta Municipality of Ghana. BMJPH. 2024;2(2):e000640. doi:10.1136/bmjph-2023-000640
11. Kabeza CB, Harst L, Schwarz PEH, Timpel P. Assessment of Rwandan diabetic patients’ needs and expectations to develop their first diabetes self-management smartphone application (Kir’App). Therapeutic Adv Endocrinol. 2019;10:2042018819845318. doi:10.1177/2042018819845318
12. Michie S, Van Stralen MM, West R. The behaviour change wheel: a new method for characterising and designing behaviour change interventions. Implementation Sci. 2011;6(1):42. doi:10.1186/1748-5908-6-42
13. Kifle ZD, Adugna M, Awgichew A, Chanie A, Sewnet G, Asrie AB. Knowledge towards diabetes and its chronic complications and associated factors among diabetes patients in University of Gondar comprehensive and specialized hospital, Gondar, Northwest Ethiopia. Clin Epidemiol Global Health. 2022;15:101033. doi:10.1016/j.cegh.2022.101033
14. Phoosuwan N, Ongarj P, Hjelm K. Knowledge on diabetes and its related factors among the people with type 2 diabetes in Thailand: a cross-sectional study. BMC Public Health. 2022;22(1):2365. doi:10.1186/s12889-022-14831-0
15. Ferreira PL, Morais C, Pimenta R, et al. Knowledge about type 2 diabetes: its impact for future management. Front Public Health. 2024;12:1328001. doi:10.3389/fpubh.2024.1328001
16. Whittemore R, Vilar-Compte M, De La Cerda S, et al. Challenges to diabetes self-management for adults with type 2 diabetes in low-resource settings in Mexico City: a qualitative descriptive study. Int J Equity Health. 2019;18(1):133. doi:10.1186/s12939-019-1035-x
17. Kumar R, Itumalla R, Perera B, Tharwat Elabbasy M, Singh M. Patient knowledge about diabetes: illness symptoms, complications and preventive personal lifestyle factors. Health Psychol Res. 2022;10(3):1. doi:10.52965/001c.37520
18. Adu MD, Malabu UH, Malau-Aduli AEO, Malau-Aduli BS. Enablers and barriers to effective diabetes self-management: a multi-national investigation. PLoS One. 2019;14(6):e0217771. doi:10.1371/journal.pone.0217771
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.