Back to Journals » International Journal of Women's Health » Volume 13
Knowledge, Practice and Associated Factors Towards Medication Abortion Among Reproductive-Age Women in Sexual and Reproductive Health Clinics of Addis Ababa, Ethiopia, 2018: Cross-Sectional Study
Authors Yeshambel Wassie A ![]() , Berhe Lemlem S
, Berhe Lemlem S ![]() , Boka A
, Boka A ![]()
Received 16 December 2020
Accepted for publication 4 May 2021
Published 24 May 2021 Volume 2021:13 Pages 489—499
DOI https://doi.org/10.2147/IJWH.S297626
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Elie Al-Chaer
Addisu Yeshambel Wassie,1 Semarya Berhe Lemlem,2 Abdisa Boka2
1Department of Midwifery, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia; 2School of Nursing and Midwifery, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia
Correspondence: Addisu Yeshambel Wassie
Department of Midwifery, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia
Tel +251926725128
Email [email protected]
Background: Abortion rates following unintended pregnancies are increasing in developing countries, and unsafe abortion is a commonly neglected reproductive health-care problem. In Ethiopia, the number of women receiving treatment for complications from unsafe abortion is increasing. Improving the level of knowledge of reproductive-age women on medication abortion contributes to the prevention of unsafe abortion. Therefore, the purpose of this study was to assess knowledge, and practice of medication abortion and associated factors among women in SRH clinics of Addis Ababa, Ethiopia, 2018.
Methods: A cross-sectional quantitative study design was conducted to collect data from 30th February to March 30, 2018. Study participants were selected by using a convenient sampling technique. The data were coded and entered into EpiData version 4.2, and SPSS version 23 was used for analysis. Bivariate and multivariate analysis with 95% CI were employed. The strength of association was declared at a P value < 0.05.
Results: The overall knowledge and practice of medication abortion were 72.1%, and 33%, respectively. Participants level of education (AOR=3.54, 95% CI (1.02, 12.26)), father education (AOR=2.80, 95% CI (1.42, 5.52)), participants way of living (AOR=6.08, 95% CI (2.41, 15.33)), income (AOR=2.19, 95% CI (1.02, 4.75)), and history of unwanted pregnancy (AOR=11.7, 95% CI (1.11, 12.46)) were some of the factors associated with knowledge and practice of medication abortion.
Conclusion: This study provided that women were relatively knowledgeable but their practice on medication abortion was low. The low practice of medication abortion call health-care providers to give due attention to awareness creation and strengthened action to provide quality maternal care for childbearing mothers towards medication abortion and unsafe abortion in particular.
Keywords: knowledge, practice, medication abortion, reproductive-age women
Introduction
Abortion is a termination of pregnancy (spontaneous, therapeutic, or induced) before the stage of viability (fetal weight <500gm).1 Unsafe abortion is defined by WHO as a procedure for terminating an unwanted pregnancy either by persons lacking the necessary skills or in an environment lacking the minimal medical standards, or both.2 Medication abortion is the commonly performed safe abortion technology that uses medications (mifepristone and misoprostol) in place of traditional surgical interventions for terminating an early unintended pregnancy.3 Death and morbidity as a result of unsafe abortion are perhaps some of the least discussed health problems in the world.4 Maternal mortality will be achievable if unsafe abortion will be replaced by medication abortion since thousands of lives could be saved each year by implementing medication abortion.5 The study done by WHO and Guttmacher institute estimated 56 million abortions occurred every year worldwide, of this 25 million (45%) are unsafe abortions and the majority (97%), occurred in developing countries in Africa, Asia, and Latin America.6,7
The 2004 Ethiopian revised criminal code allows abortion under certain circumstances. When the pregnancy results from rape or incest, the woman’s or fetus’s lives are threatened, the fetus has severe abnormalities, the woman has physical or mental disabilities, and when a minor is physically or psychologically unprepared to raise a child. According to the new law, there is no need for proof of age or whether the pregnancy has resulted from rape or incest.8
Ethiopia has a high maternal mortality ratio, 412 deaths per 100,000 live births for the period 2009–20169 and an estimated 1.9 million (38%) Ethiopian women have unintended 4.9 million (62%) total pregnancies and 13% induced abortion were performed in 2014.10,11 The proportion of abortions occurring in facilities raises from 27% to 53%; nonetheless, an estimated 294,100 abortions occurred outside of health facilities.10 The number of women receiving treatment for complications from induced abortion nearly doubled.11,12
Medication abortion using drugs has recently come into focus as a plausible alternative to manual vacuum aspiration to induce abortion.13 A prospective study which was conducted on client preferences and acceptability for medical abortion and manual vacuum aspiration as an early pregnancy termination method in northwest Ethiopia showed that subjects undergoing medical abortions reported significantly greater satisfaction and more likely to choose the same method again than were subjects undergoing manual vacuum aspiration.14
In Ethiopia, death and disability due to unsafe abortion continue to occur against the backdrop of major advances in the medical profession, especially in terms of the availability of safe and effective technologies and skills for induced abortion. Barriers and challenges to accessing medication abortion exist at multiple levels which may deprive women of using safe medication abortion and exposing them to unsafe abortion and its devastating consequences of death and disability.15 Access to medication abortion is commonly restricted, not only by the law but also by social, religious, cultural impediments, lack of awareness, maternal perception contribute to delays in seeking an abortion to a time beyond the limit set by the law and thus when faced with an unintended pregnancy, women seek abortion and self-induce it or find providers, irrespective of the law and Unsafe abortions present a critical public health and human rights challenge of the present time.15,16
The combination of mifepristone and misoprostol has been shown by various studies to be a safe, effective, and well-established method for the termination of pregnancy. However, many women used less recognized and less effective abortive drugs.13 So, there seems to be a gap in non-use of MA, or wrong use of non-effective drugs. Therefore, this study will aim to assess the knowledge, and practice of medication abortion and associated factors among women in sexual and reproductive clinics of Addis Ababa, Ethiopia.
Methods
Study Area and Setting
The study was conducted in Addis Ababa, the capital of Ethiopia. Addis Ababa is set up into ten sub-cities. According to the 2007 population and housing census, the city has a total population of 2,739,551 (3.7%) and an annual growth rate of 2.1% between 1994 −2007. Out of these, female population accounted for 1,434,164 (52%). Women of reproductive age group among the total population are 947,855.17 According to the report from Addis Ababa FMHACA and Ethiopian MOH, in the city, seven stand-alone SRH-clinics existed and the outpatient service of SRH clinic shall provide services like adolescent reproductive health service, delivery service (optional), antenatal Care service, postnatal Care service (optional), removal of retained concepts products following miscarriage or abortion, family planning service, New-born resuscitation, Immunization, abortion care (as per law), PMTCT services, STIs and HTC and referral service.18
Study Design and Period
The facility-based cross-sectional quantitative study design was employed from 30th February–March 30, 2018.
Source Population
All reproductive age women attending sexual and reproductive health clinics of Addis Ababa, Ethiopia, in 2018.
Study Population
All reproductive-age women attending selected SRH clinics of Addis Ababa, Ethiopia in 2018.
Inclusion Criteria
All reproductive age women (18–49) coming for service in selected SRH clinics during the data collection period were included.
Exclusion Criteria
Reproductive age women coming for the service but involuntary, severely ill were excluded from the sample.
Sample Size Determination
The sample size required for the study was calculated based on a single population proportion formula by considering the anticipated proportion of women’s knowledge, attitude, and practice of medication abortion as 50%.

By adding a 10% non-response rate, the total sample size= 423.
Sampling Procedure
From the total seven SRH clinics, four clinics were selected by using simple random sampling, and then the total sample size was distributed to each selected SRH clinic proportionally. Finally, a convenient sampling technique was employed to select subjects.
Dependent Variable
Knowledge, attitude, and practice of medication abortion
Independent Variable
Socio-demographic and economic variables (Age, educational status, residence, religion, place of birth, marital status, occupation, income, parental educational status), Obstetric variables (parity), and RH service variables (contraceptive history, Friends or relative/family who has had an abortion, history of unwanted pregnancy)
Operational Definition
Medication Abortion
Is a method of pharmacologic termination of the early first trimester of pregnancy (meaning by using mifepristone, misoprostol, or both).
Knowledge
What a woman knows about medication abortion (Meaning: a place where it is done, drugs used for medication abortion, and gestational age medication abortion is used) and it consists of 16 knowledge item questions.
- Low knowledge: If the participant scores ≤2 on the total knowledge part questions.17
- Satisfactory knowledge: A score of 3 on the total knowledge part of the assessment17
- High knowledge: A score of ≥4 on the total knowledge part of the assessment.19
Practice
Is the habit of a woman related to medication abortion or those who have experienced or practiced medication abortion at least once in the past.
Methods of Data Collection and Tools
A pretested, structured interview questionnaire consisting of items with pre-coded response categories was used. The questionnaire was adapted and modified by reviewing the literature.20 The questionnaire was 1st designed in English and translated into the local Amharic language and then translated back to English by language experts to check its consistency.
Data Collection Procedure and Quality Control
Data were collected by face-to-face interviews using structured questionnaires. Five BSc nurses and three BSc midwives were selected to collect the data and two BSc midwives were selected for supervision. Before starting the actual data collection to assure the data quality, the high emphasis was given to designing a data collection instrument; first, the questionnaire was pre-tested on 10% of the sample size or 43 mothers on Gotera SRH clinics. The data entry format template was prepared and programmed by the principal investigator.
Data Analysis and Processing
The data was cleaned, stored and data template and entry was done using EpiData version 4.2, and then it was exported to SPSS version 23.0 software for analysis. Descriptive statistics like frequency, proportion, mean, and standard deviation were computed to describe study variables in relation to the population. Logistic regression was used to determine the effect of independent variables on the outcome variables. Variables with P <0.2 in binary logistic regression were entered into multiple logistic regression and the strength of association was declared at P value <0.05. Finally, results were compiled and presented using texts, tables, graphs.
Ethical Consideration
Ethical clearance and approval were obtained from Addis Ababa University ethical review committee. Informed written consent was taken from all study participants. All the participants were reassured of the anonymity, and personal identifiers were not used. Then, the data collectors have continued the job by giving due respect to the norms, values, beliefs, culture, and ensured the confidentiality of the data. Client informed consent was not required since all data were fully anonymized before data was accessed and that this study was conducted in accordance with the declaration of Helsinki.
Results
Socio-Demographic Characteristics of Study Participants and Their Parents
From a total of 423 mothers who were invited for an interview, 412 filled the questionnaires completely, resulting in a response rate of (97.4%). The mean age of the respondents was 25.0 (SD±5.11) years with a minimum and maximum age of 18 and 43, respectively. The majority of the respondents 133 (32.3%) fall in between the 24–27 years of age group. Out of the total respondents, 294 (71.4%) of them were born in Addis Ababa and the majority of 238 (57.8%) of the study participants were orthodox religious followers. From the total participants; 145 (35.2%) had attended up to secondary education followed by college/university 139 (33.7%). Regarding the marital status of the respondents, 132 (32%) were married, and almost all 386 (93.7%) were living in Addis Ababa where 88 (21.4%) were private employers, and out of the total respondents, 138 (33.5%) of them had a monthly income of <500 Ethiopian birrs (Table 1).
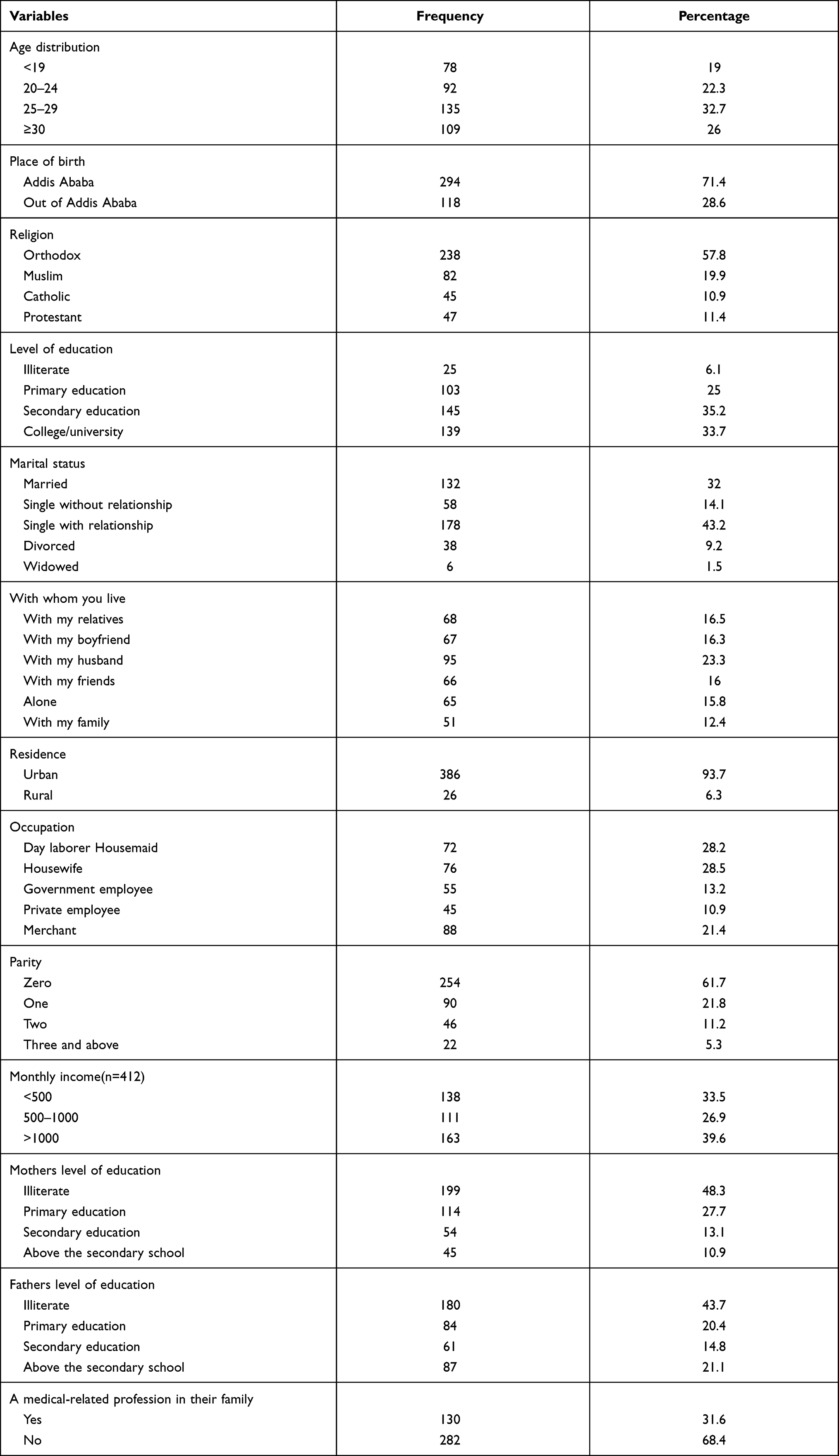 |
Table 1 Socio-Demographic Characteristics of Reproductive Age Women in SRH Clinics of Addis Ababa, 30th February–March 30, 2018 (n=412) |
Respondents General Knowledge on Abortion Law and Medication Abortion
More than one-third of the respondents 168 (40.8%) reported that abortion is legally allowed in Ethiopia. From those study participants who believe abortion is legally allowed in Ethiopia (n=168), most of the participants mentioned conditions as when the pregnancy results from rape or incest 131 (78%). More than half of the respondents, 247 (60%) support the government allowing abortion in Ethiopia. Three fourth 312 (75.7%) reported that as they knew what MA means. Among those respondents who claimed to know MA, 221 (70.8%), said MA means; abortion using abortion pill/drug. The majority of the respondents 199 (63.8%) did not know which drugs are used in the case of MA, however, some of the respondents mentioned misoprostol 86 (27.6%) followed by mifepristone 67 (21.5%). Most of the respondents 116 (37.2%) who claimed to know MA did not know the preferred gestational age to perform MA and only 185 (59.3%) of respondents mentioned as it was performed when their gestational age less than or equal to 9 weeks or 63 days (Table 2).
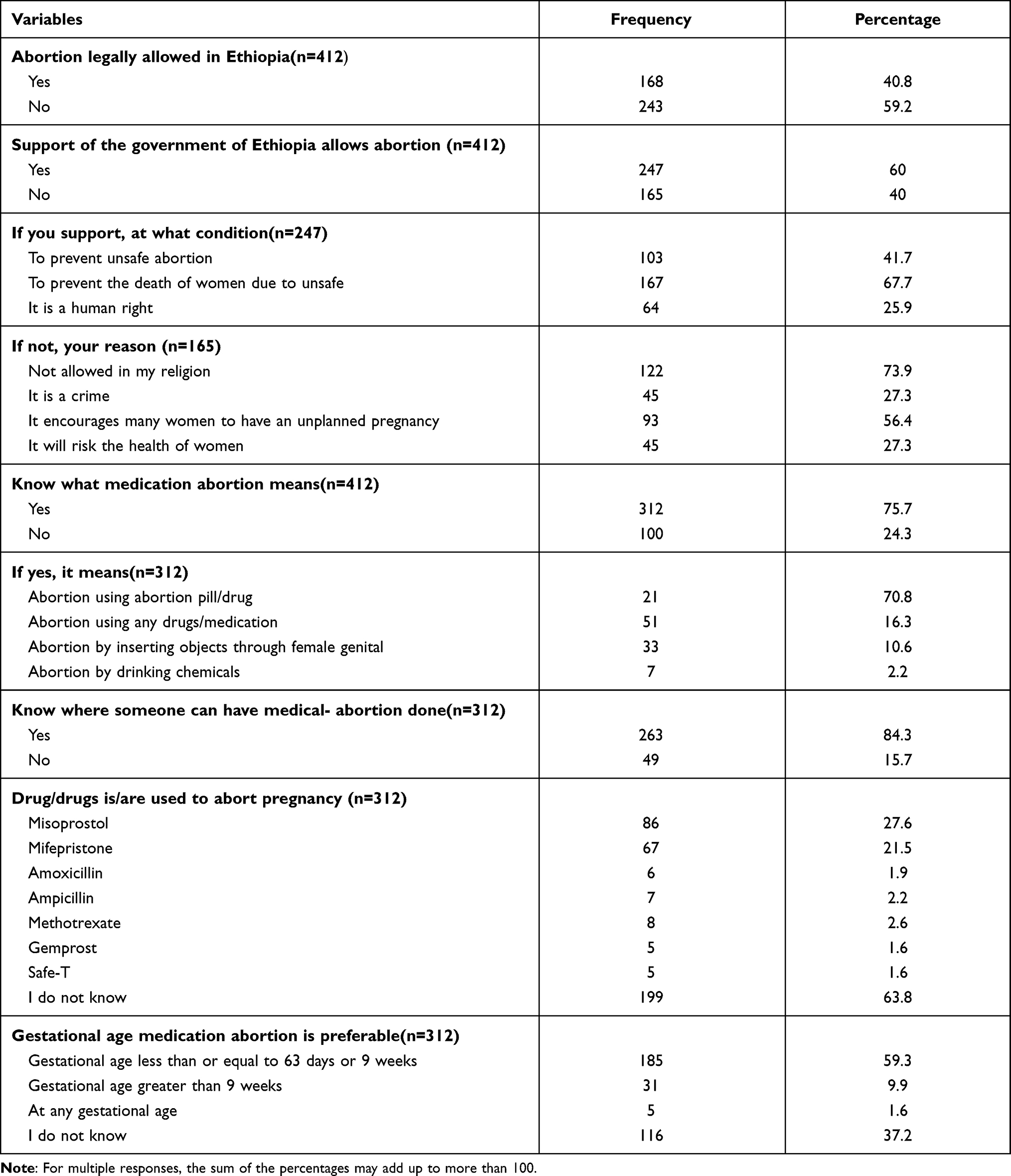 |
Table 2 Knowledge of Reproductive Age Women on Medication Abortion and on Abortion Law in SRH Clinics of Addis Ababa, 30th February–March 30, 2018 |
When the knowledge score was done from the knowledge questions, it was found that most of the study participants have high knowledge towards MA 159 (38.6%) followed by satisfactory knowledge 138 (33.5%).
Sexual and Medication Abortion Practice
Nearly half 201 (48.8%) of the respondents know a friend/neighbor who had terminated pregnancies and almost all 409 (99.3%) of the respondents had sexual intercourse experience, from those who had sexual intercourse before, 193 (46.8%) of them had a history of unwanted pregnancy. From those (n=206) respondents, majority 136 (66.2) used medication/drugs for termination followed by surgical abortion 35 (17.2%). Being easy to take 81 (39.71%) is the most given reason for MA preference (Table 3).
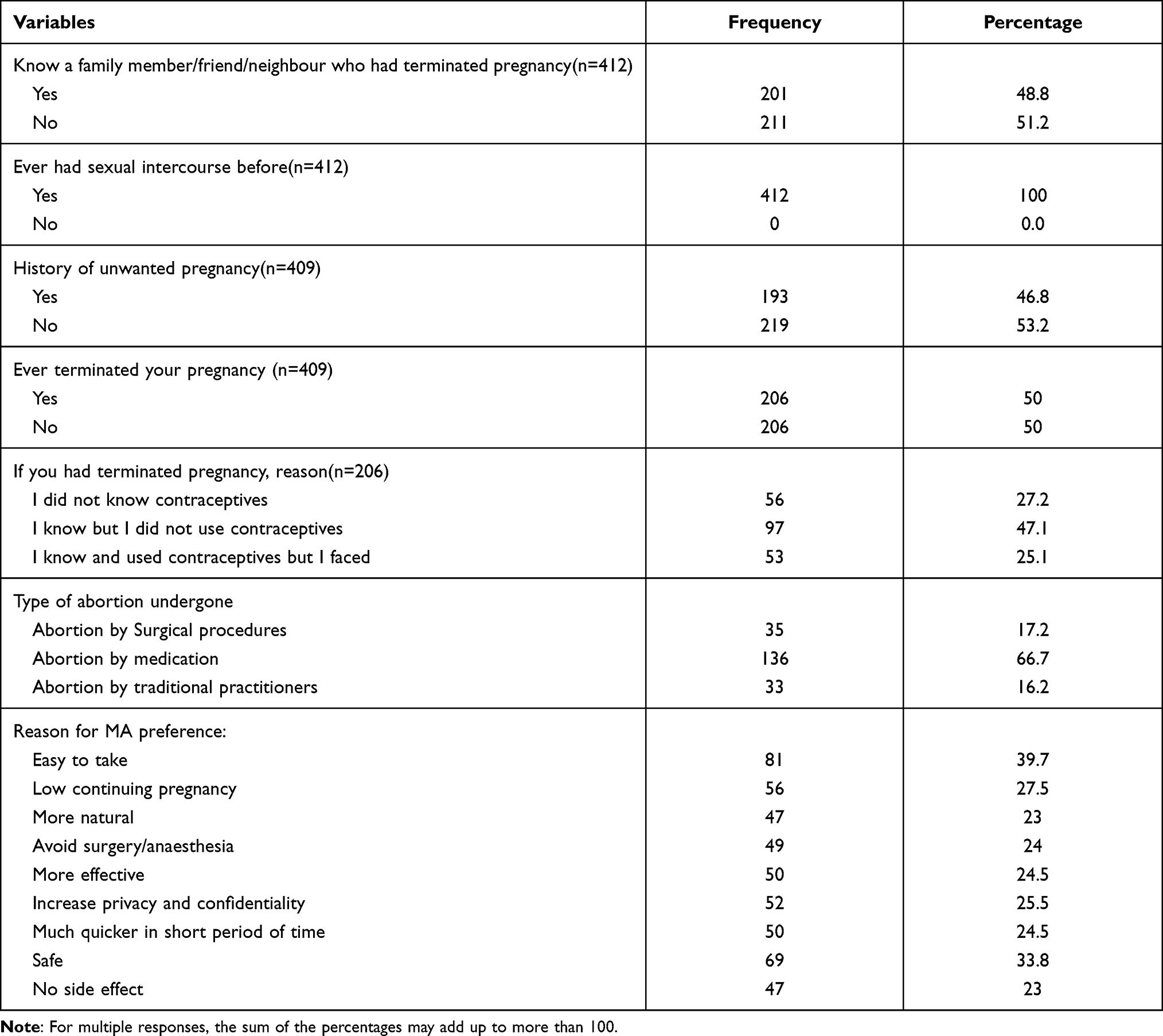 |
Table 3 Practice of Reproductive Age Woman Towards Medication Abortion in SRH Clinics of Addis Ababa, 30th February–March 30, 2018 |
Association of Explanatory Variables with Knowledge Medication Abortion
Binary Logistic regression was performed to assess the association of each independent variable with medication abortion knowledge. Fathers’ level of education and their way of living was significantly associated with medication abortion knowledge at a P-value of <0.05 (Table S1. Respondents who have a father who learned up to secondary education were 2.03 times more knowledgeable on the MA (AOR=2.03, 95% CI (1.01, 4.10)). Similarly, those respondents whose father learned some forms of college or university education were 2.80 times more likely knowledgeable on MA (AOR=2.80, 95% CI (1.42, 5.52)). In addition, respondents living with their relatives (2.34 times), with their boyfriends (6.08 times), and with their friends (5.35 times) were more likely to knowledge on MA compared with those living with their family (AOR=2.34, 95% CI (1.05, 5.25)), (AOR=6.08, 95% CI (2.41, 15.33)), and (AOR=5.35, 95% CI (2.18, 13.16)) respectively (Table S1).
Association of Explanatory Variables with Practice of Medication Abortion
As shown in Table S2, respondents who had learned secondary education (3.54 times) and college/university (3.49 times) were more likely to practice MA than illiterates (AOR=3.54, 95% CI (1.02, 12.26)), (AOR=3.49, 95% CI (1.02, 11.92)) respectively. Similarly, respondents who had a history of unwanted pregnancy were 11.7 times more likely to practice to MA than those respondents who had no history of unwanted pregnancy (AOR=11.7, 95% CI (1.11, 12.46)) In addition, respondents who get a monthly salary of greater than 1000 ETB were 2.19 times more likely to practice MA than those who get monthly salary less than 500 ETB (AOR=2.19, 95% CI (1.02, 4.75)) (Table S2).
Discussion
According to this study, more than half of the respondents have heard about safe abortion (58.3%) and unsafe abortion (57.3%) and this study were higher than the descriptive study carried out on 50 reproductive-age women in Lekhnath, Kaski, Nepal, on the assessment of the level of knowledge regarding safe abortion which showed that only 40% of the respondents knew safe abortion.21 This might be due to the study time difference or due to a small sample size carried out in Nepal.
In this study, most of the respondents who claimed to know MA reported when medication abortion was preferable. From those respondents, 185 (59.3%) said, when the pregnancy is less or equal to 9 weeks or 63 days, and a few 5 (1.6%) said at any gestational age. However, the majority of 116 (37.2%) did not know when medication abortion will be performed. This finding was slightly in line with the study done in India to assess the knowledge, attitude, and practice of MA which showed that the majority 53.3% taken abortifacient at less than 12 weeks gestation, and 26.6% of them did not know where MA will be given.22 These might be due to the educational level, technological dissemination, or maybe due to better health policy and program implementation currently across the world.
Regarding medication abortion practice, only 33% practiced medication abortion from the total study participants. Of the respondents, 46.8% had a history of unwanted pregnancy and 49.8% of them had a history of termination of pregnancy. From those who had terminated their pregnancy, the majority 66.7% used abortion pill/drugs for termination followed by abortion by surgical procedures 17.2% and by traditional Practitioners 16.2%. Many of them claimed the reason for termination was they know, but negligent to use contraceptives (47.1%), followed by lack of knowledge (27.2%) and some of them were claimed that as they become pregnant as they were on contraceptives (25.7%). This figure was higher than the study conducted in India which showed only 17.5% used MA23 and the study was slightly higher than the study done in Nigeria, which showed 49% had previous termination and 48% had used drugs for termination of pregnancy.13 This inconsistency might be due to the difference in health policy, implementation program, and small sample size used in the previous study.
In this study father’s educational level was significantly associated with medication abortion knowledge which shows that respondents who have a father who learned secondary education were 2.03 times more knowledgeable on MA than illiterate fathers. Similarly, those respondents whose father learned college/university were 2.80 times more knowledgeable on MA than respondents whose father is illiterate. This finding was consistent with the study done in India,23 Addis Ababa,20 which showed that respondents with fathers who are illiterate had low knowledge regarding MA compared to respondents having fathers who are educated (AOR=0.112 [0.013–0.969]). In addition to this, from this study ‘participant’s way of living was significantly associated with MA abortion. Those respondents living with their relatives [AOR=2.34, CI [1.05–5.25]], boyfriends [AOR= [6.08, CI [2.41–15.33]] and with their friends [AOR=5.35, CI [2.18–13.16]] had knowledge on MA compared with those living with their family, respectively. This finding was comparable to the study conducted in Dar Es Salaam, Tanzania, on unwanted pregnancy and induced abortion among females, which showed that majority 17 (65.4%) of the respondents living with their boyfriend and 3 (11.5) living with their friends had significant knowledge on abortion.4
In addition to this, respondents who had secondary education (3.54 times) and college/university (3.49 times) were more likely to practice MA than illiterates. This finding was similar to the study done in India23 and in Addis Ababa8 which showed that usage of MA drugs was significantly higher than in an educated group. Similarly, respondents who had a history of unwanted pregnancy were 11.7 times more likely to practice MA than those respondents who had no history of unwanted pregnancy. This finding was consistent with the study done on determinants of abortion practice in Addis Ababa, which showed that respondents with a history of unwanted pregnancy (p < 0.000) had a strong association with their unwanted pregnancy.24 In addition to the above factors, respondents who get a monthly salary of greater than 1000 ETB were 2.19 times more likely to practice MA than those who get less than 500ETB. This finding is comparable with the study conducted on evangelical women residing in Addis Ababa8 which showed that respondents’ income level was strongly associated with abortion practices. This might be due to the same socio-economic background of the country.
Study Limitations
Respondents may answer questions in a manner that would be viewed favorably by others (may under/inaccurately report their view towards medication abortion). Selection bias, recall bias, and white coat bias might not be minimized. Since the data is collected at a single point in time, the temporal relationship could not be established. Being a facility-based data, the finding from this study may not be generalizable to the whole population in Ethiopia or similar countries setting.
Conclusion
Generally, out of 78.9% of the study participants who heard about abortion, only 75.7% had aware of medication abortion and nearly one-third of the respondents (27.9%) were found to have low knowledge scores on medication abortion. Of all the respondents, 230 (55.8%) would consider abortion to terminate if they have an unplanned pregnancy and 33% of them had practiced medication abortion from the total participants. Respondents’ level of education, father’s educational level, way of living, history of unwanted pregnancies, a medical-related profession in the family, and monthly income were identified as major determinants (predictors) of medication abortion knowledge, attitude, and practice.
Recommendations
Both governmental and non-governmental organizations that were primarily involved in maternal health should address the issue of negative attitude to change the communities towards safe abortion services especially on medication abortion. The media should better disseminate the conditions under which abortion is currently permitted, the availability of medication abortion, and where the women can access information regarding medication abortion. Health workers, particularly health extensions should teach the community about the consequence of unsafe abortion and stigma.
Abbreviations
EDHS, Ethiopian Demographic Health survey; FMHACA, Food, Medicine and Health administrative and control authority; MA, Medication abortion; MCH, Maternal and Child Health; MOH, Ministry of Health; RH, Reproductive Health; STI, Sexually transmitted infections; SRH, Sexual and reproductive health.
Data Sharing Statement
The data sets used and/or analyzed during the current study are available from the corresponding author on reasonable request.
Ethics Approval and Consent to Participant
Ethical clearance was obtained from Addis Ababa University. Informed written consent was taken from all study participants. Personal patient information was not recorded, after finishing the data collection the patients’ document return to the card room, the information was used for study purposes only. Committee’s reference number was not given/number is not applicable and/or not available.
Acknowledgments
We would like to express our deepest heartfelt thanks to Addis Ababa University for allowing conduct this study. Our special thanks go to SRH clinic staff for their support during the data collection process.
Authors-Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Authors’ Information
- Addisu Yeshambel Wassie is a Lecturer in the Department of Midwifery, College of Health Science and Medicine, Wolaita Sodo University, Wolaita Sodo, Ethiopia.
- Semarya Berhe Lemlem is an Assistant professor in the School of Nursing and Midwifery, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia.
- Abdisa Boka is a Lecturer in the School of Nursing and Midwifery, College of Health Science, Addis Ababa University, Addis Ababa, Ethiopia.
Funding
No funding agencies were involved and the principal investigator has covered the fee for data collectors, and expenditure for translation and transcription of questionnaires and for hard copies.
Disclosure
The authors declare that there were no competing interests.
References
1. Organization WH. Safe and Unsafe Induced Abortion: Global and Regional Levels in 2008, and Trends During 1995–2008; 2012.
2. Clinic WLIHR. U.S. Foreign Policy as an Obstacle to the Implementation of Ethiopia’s Liberalized Abortion Law; 2010.
3. Borkowski L, Strasser J, Allina A, Wood S. Medication abortion: overview of research & policy in the United States-references by topic area. 2015.
4. Mamboleo N. Unwanted Pregnancy and Induced Abortion Among Female Youths: A Case Study of Temeke District. Muhimbili University of Health and Allied Sciences; 2012.
5. Baggaley RF, Burgin J, Campbell OMR, Gravenor MB. The potential of medical abortion to reduce maternal mortality in Africa: what benefits for Tanzania and Ethiopia? PLoS One. 2010;5(10):e13260. doi:10.1371/journal.pone.0013260
6. institute G. Induced Abortion Worldwide. September, 2017.
7. Sedgh G, Henshaw S, Singh S, Åhman E, Shah IH. Induced abortion: estimated rates and trends worldwide. Lancet. 2007;370(9595):1338–1345. doi:10.1016/S0140-6736(07)61575-X
8. Solomon H. Knowledge, Attitude, and Practice Assessment Towards Induced Abortion Among Evangelical Women Residing in Addis Ababa. 2015.academia.edu 2015.
9. Central Statistical Agency I. Ethiopia demographic and health survey 2016. BMC Public Health. 2016;15(1):139.
10. Gebrehiwot Y, Fetters T, Gebreselassie H, et al. Changes in morbidity and abortion care in Ethiopia after legal reform: national results from 2008 and 2014. Int Perspect Sex Reprod Health. 2016;42(3):121–130. doi:10.1363/42e1916
11. Singh S, Fetters T, Gebreselassie H, et al. The estimated incidence of induced abortion in Ethiopia, 2008. Int Perspect Sex Reprod Health. 2010;36(01):16–25. doi:10.1363/3601610
12. Moore AM, Gebrehiwot Y, Fetters T, et al. The estimated incidence of induced Abortion in Ethiopia, 2014: changes in the provision of services since 2008. Int Perspect Sex Reprod Health. 2016;42(3):111–120. doi:10.1363/42e1816
13. Adinma ED, Adinma JIB-D, Iwuoha C, Akiode A, Oji E, Okoh M. Knowledge and practices among medical abortion seekers in southeastern Nigeria. Southeast Asian J Trop Med Public Health. 2012;43(2):471.
14. Woldetsadik MA, Sendekie TY, White MT, Zegeye DT. Client preferences and acceptability for medical abortion and MVA as early pregnancy termination method in northwest Ethiopia. Reprod Health. 2011;8(1):19. doi:10.1186/1742-4755-8-19
15. Assifi AR, Berger B, Tuncalp O, Khosla R, Ganatra B. Women’s awareness and knowledge of abortion laws: a systematic review. PLoS One. 2016;11(3):e0152224. doi:10.1371/journal.pone.0152224
16. Alemu FF. Minors’ Awareness about the New Abortion Law and Access to Safe Abortion Services in Ethiopia: the Case of Marie Stopes International Ethiopia Centers in Addis Ababa [Unpublished thesis]. Addis Ababa: University of Amsterdam; 2010.
17. Samia Zekaria member and Secretary PCC. Population and Housing Census of Addis Ababa, Ethiopia; 2007.
18. Health FMo. Health and Health-Related Indicators; 2007.
19. Fernandes KG, Camargo RPS, Duarte GA, et al. Knowledge of medical abortion among Brazilian medical students. Int J Gynecol Obstet. 2012;118(S1):S10–S14. doi:10.1016/j.ijgo.2012.05.004
20. Thomas G. Assessment of Knowledge, Attitude, and Practices Regarding Medication Abortion Among Regular Undergraduate Female Students in College of Social Sciences, Addis Ababa University. Ethiopia: Addis Ababa University Addis Ababa; 2014.
21. Acharya A, Bhattarai S. Assessment of the level of knowledge regarding safe abortion among reproductive age group women, a short cross-sectional study in lekhnath, kaski. J Inst Med. 2017;39(1):105–109.
22. Namrata S, Sumitra Y. The study of knowledge, attitude and practice of medical abortion in women at a tertiary Centre. IOSR J Dent Med Sci. 2015;14(12):1–4.
23. Lakkawar N, Magon S, Alaganandam P. Attitude and experiences of young women towards medical abortion a hospital-based study. Sch J App Med Sci. 2014;2(6B):2034–2041.
24. Habte M. Determinants of Abortion Practice in Addis Ababa [MA Thesis Submitted to Population Studies]. Addis Ababa University. 2010.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.