Back to Journals » Journal of Multidisciplinary Healthcare » Volume 12
Knowledge, Beliefs, and Attitudes Concerning Genetic Testing Among Young Jordanians
Authors Altaany Z ![]() , Khabour OF
, Khabour OF ![]() , Al-Taani G
, Al-Taani G
Received 6 October 2019
Accepted for publication 15 November 2019
Published 11 December 2019 Volume 2019:12 Pages 1043—1048
DOI https://doi.org/10.2147/JMDH.S233614
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Zaid Altaany,1 Omar F Khabour,2 Ghaith Al-Taani3
1Department of Basic Medical Sciences, Faculty of Medicine, Yarmouk University, Irbid, Jordan; 2Department of Medical Laboratory Sciences, Jordan University of Science and Technology, Irbid, Jordan; 3Department of Pharmacy Practice, Faculty of Pharmacy, Yarmouk University, Irbid, Jordan
Correspondence: Zaid Altaany
Department of Basic Medical Sciences, Faculty of Medicine, Yarmouk University, P.O. Box 566, Irbid 21163, Jordan
Tel +962 2721111 Ext 7109
Email [email protected]
Background: Medical genetic testing is an evolving side of clinical care that helps people to make informed medical and lifestyle decisions. The source of knowledge, personal beliefs, and attitude towards genetic testing are the main determinative factors of getting optimal utilization of such technology in reducing/prevention of diseases.
Methods: A structured survey was used to assess the knowledge, beliefs, and attitude regarding genetic testing among 463 young adults aged 18 years or older living in the North of Jordan.
Results: More than three-quarters (77.1%) of the respondents were familiar with the term genetic testing. The most common sources of knowledge were: education they received (44.8%), the internet (37.5%), and social media (17.2%). Most (93.9%) of the respondents believed that genetic testing is a useful tool to diagnose and prevent genetic diseases. Almost three-quarters (72.7%) of the respondents believed that the health care system provides advice or genetic counseling to those with a genetic disease. A total of 9.6% of the respondents thought that genetic testing might cause a physical risk to their lives. In addition, 11.3% of the respondents believed that genetic testing is forbidden and not permissible and about 6.3% did not agree in performing genetic testing in the future. Finally, about half (53.4%) of the respondents consider genetic testing affordable and the remainder consider it costly.
Conclusion: Our findings emphasize the importance of acquiring knowledge about genetic testing among young individuals, Issues related to knowledge were identified and should be further improved, such as cost prediction, safety, and the legitimacy of genetic testing to get better outcomes in the Jordanian community.
Keywords: genetic testing, beliefs of genetic testing, source of knowledge of genetic testing
Introduction
Congenital/genetic disorders are common among children worldwide.1,2 The chance of having an affected child with a certain disease increases with a family history of genetic disorders3,4 People concern about the potential harm of their genomic risk for diseases and the appropriateness of genetic testing.5 Medical genetics involves the application of genetic knowledge and technology to specific clinical concerns.6,7 Therefore, genetic testing can be used to screen the presence of mutations or genetic variants that increase the risk of development of many diseases,8,9 or to predict the effectiveness/dose of therapeutics drugs,10 and to assess individual’s reaction to diet or allergen.11
Health literacy may influence the understanding of personal or familial genomic risk, and it is related to cultural, social, and individual factors.12 For example, it has been reported that individuals with weak health literacy recall little information about a genetic test to predict the recurrence of certain types of cancer. Likewise, genetic literacy can also affect public attitudes, interest, and understanding.13,14 Studies have reported low levels of public understanding of genetic concepts such as the location of genes and applications such as newborn screening.15–17 While other studies have investigated individuals’ attitudes toward genetic testing and their association with the interest in undergoing genetic testing.18,19 The individual’s attitudes toward genetic testing are important because of the efforts can be expended in establishing services that are accepted by the public and in concordance with people’s needs.20,21 The primary care physician’s knowledge, attitudes, and experience with genetic testing are important as well, and their lack of training and knowledge may limit their ability to advise patients or interpret the genetic test results.22 Lacking in self-knowledge in genetic testing may contribute to personal health management and familial decision. Therefore, the objective of this study was to evaluate the knowledge, beliefs, and attitude regarding genetic testing among young Jordanians.
Methods
A cross-sectional, descriptive survey study design was used to assess the knowledge, beliefs, and attitude regarding genetic testing among young adults aged 18 years or more living in Irbid, a large city in North of Jordan, between April 2019 and September 2019.
Data Collection
A self-administered, structured survey that assessed a number of issues related to genetic testing was developed. The survey addresses the personal knowledge, past experience of genetic testing, benefits, concerns of genetic testing, and social and health system-related factors affecting utilization of genetic testing. Published studies in the area were used to guide the content of the survey,23,24 and the face and content validity of the survey were confirmed by a review of the survey by faculty members within the research area. A pilot exercise was carried out and involved the distribution of the survey to 20 lay public persons. Minor modifications were carried out to the content of the survey to improve its validity and readability. The survey is available upon request from the corresponding author.
The survey was delivered to a convenience sample of university students from different universities in Irbid, Jordan. The distribution was carried out by a research assistant who was trained in the process via face to face approach. The research assistant meets the student between classes breaks and in the cafeterias to described the study to the respondents and gave appropriate information. After consideration, those who agreed to participate to take part in the study were asked to provide written informed consent. Those who did not provide informed consent were not included in the study. It was highlighted to them that it is voluntary and they can withdraw from the study at any time without providing any reasons or explanation. Also, they were informed that the survey was anonymous, in order to respect the confidentiality and privacy of the respondents. The survey was created in the Arabic language and was not translated from any other language. The protocol for the study was approved by the Institutional Review Boards of Jordan University of Science and Technology (Approval ID: 17/122/2019). The sample size calculation revealed that 184 responses are needed to achieve a representative sample of North Jordan, taking into consideration a 5% margin of error and at the 95% confidence level.
Data Analysis
Data were analyzed using the Statistical Package for Social Sciences software, SPSS (SPSS Inc., Chicago, IL, USA) version 20. The descriptive statistics of all items was examined in terms of means and percentages.
Results
A total of 463 surveys were completed. The sample was characterized by being approximately two thirds (68.7%) females with a mean of age of 20.7 years of old. Most (83.0%) of the respondents were insured. More than two-thirds (74.4%) of the respondents have large family sizes and consist of 6 or more individuals. The full details about the demographic characteristics are summarized in Table 1. Table 2 illustrated the knowledge and experience of genetic testing. The results demonstrated that most (77.1%) of the respondents are familiar with the term genetic testing. It seems that respondents used as a source of knowledge of genetic testing trustworthy and non-trustworthy resources. As the most common source of knowledge is the education they received and approximately one third (37.5%) obtained this information from the internet and 17.2% of the respondents from media, including social media. The majority of the responders (83.3%) think that genetic testing optimal time is pre-marriage, 4.2% of the responders think the optimal time during pregnancy, and 6% of the responders think that they can do the genetic test routinely at any time and there is no optimal time to perform genetic testing. Furthermore, 6.3% of the responders do not agree or think about performing genetic testing in the future. More than half (53.5%) of the responders think that genetic testing is expensive.
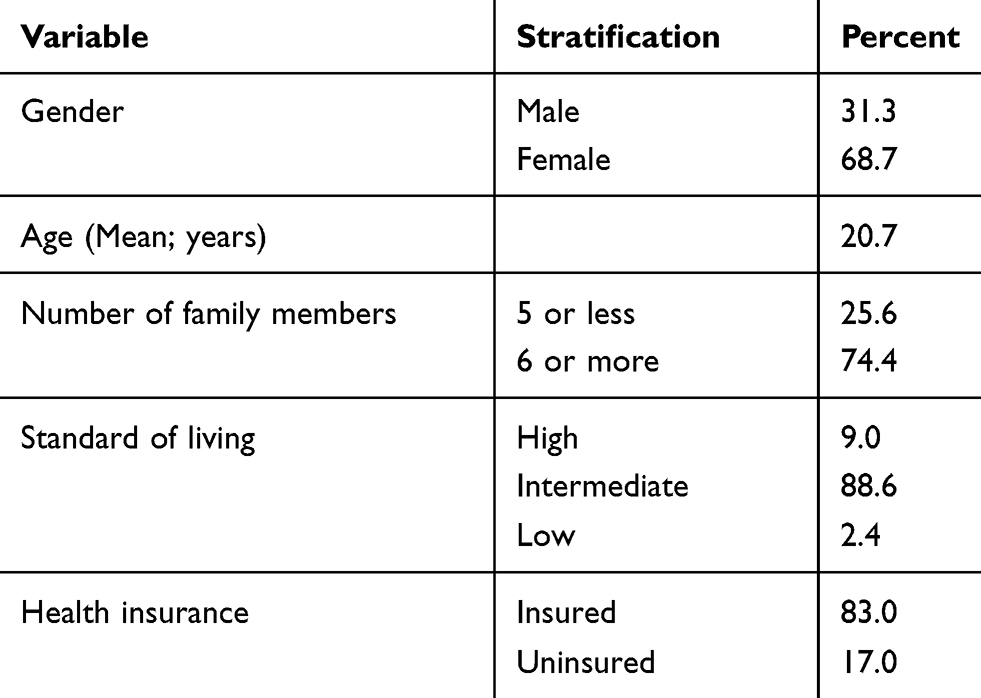 |
Table 1 Demographic Characteristic of Survey Respondents |
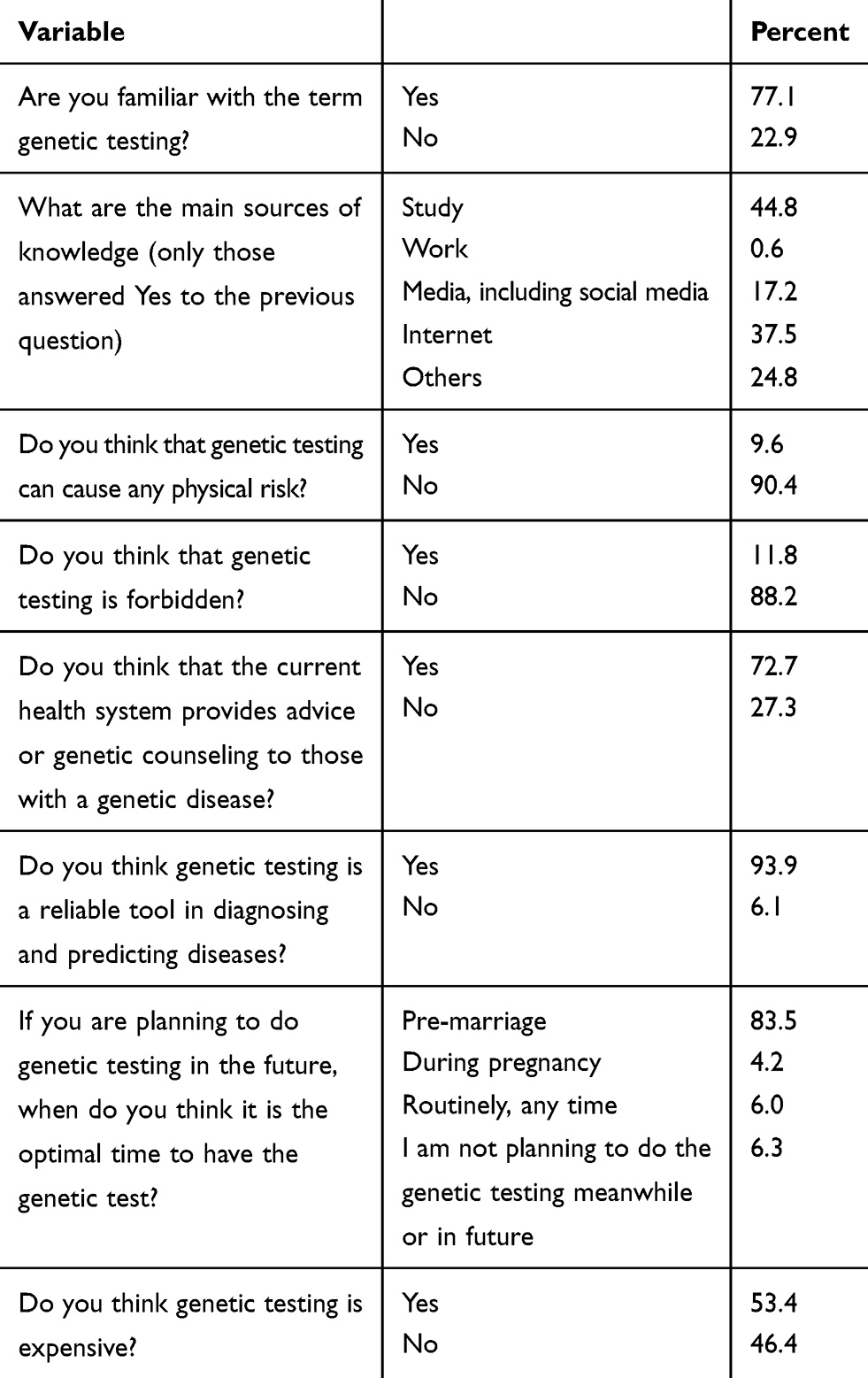 |
Table 2 Knowledge and Past Experience of Genetic Testing Among Young Jordanians |
To help in the uptake of genetic testing by subjects, it is important to determine the benefits and concerns that the subjects believe. In terms of benefits, the beliefs are in a positive direction, e.g., 93.9% of the respondents believe that genetic tests are a useful and reliable tool in diagnosing and prediction of genetic diseases. Also, when it comes to concerns the beliefs are in a positive direction, only a small minority (9.6%) worried and think that genetic testing can cause a physical risk to their lives. In contrast, the majority does not agree that genetic testing can cause any physical risk.
A snapshot of the social and health system-related factors affecting the utilization of genetic testing as reported by respondents are highlighted. Almost three-quarter (72.7%) of the respondents believe that the health care system in Jordan provides advice or genetic counseling to whom with a genetic disease. Only 11.8% of the respondents think genetic testing is forbidden, and 88.2% of the respondents think genetic testing is permissible. More than half (53.5%) of the responders think genetic testing is expensive.
Discussion
Genetic testing contributes to both medical management and personal decision making. The public understanding of the importance of genetic testing to decrease the susceptibility of having a hereditary disease is a major public health concern. Public attitudes towards genetic testing for the risk of diseases, including cancer, have been found to be generally positive.25–27 In a study conducted in the USA, 97% of participants indicated that they were at least somewhat interested in the topic of genetic testing and the majority had positive attitudes about genetic research and approved of the use of genetic testing in the detection of diseases.25 Positive attitudes towards genetic testing are also reported in a Dutch survey study that has been conducted in 2002 and 2010 and found that expectations of benefits and potential use of genetic testing have been raised among the public in 2010 compared to 2002, resulting in more positive opinions.27 An interesting systematic review published in 2017 that included a forty-one studies (39 studies from the US, and two from Australia) between 2000 and 2009 showed a low awareness and knowledge of genetic counseling/testing for cancer susceptibility among ethnic minority groups, including African Americans, Asian Americans, and Hispanics.28 Furthermore, negative attitudes were also evident, particularly the anticipated emotional impact of test results, and concerns about confidentiality, stigma, and discrimination.28
Here in the current study, a young Arab Jordanian respondent had a positive knowledge and awareness of genetic testing, this knowledge mostly derived from education and media sources. Informative and updated internet websites may provide both general and specific information, but may not target certain groups of people such as older individuals,29 or low-income individuals who might do not have the facility and internet access. Furthermore, information on the web or social media is not always of high quality and objective, and might not be picked up by the lay public. Knowledge deficiency may lead people to refrain from taking a genetic test when necessary. This may lead to poorer health, reduce the quality of life, and increase the medical costs when an easily preventable disorder requires later treatment.30,31
The newborn-screening services programs (NBS) are often carried out in the private sector and for those who can afford to pay for the test in many developing countries. A study has shown that in 2007 only 4 countries in the Middle East and North Africa (MENA) region had ongoing NBS programs. The MENA region consists of 21 countries with a population of about 440 million with 11 million annual births.32 Because there are high rates of consanguinity and first cousin marriages, genetic disorders are relatively common.33 Nowadays, many national NBS programs with extensive screening coverage are present in Bahrain, Egypt, Iran, Kuwait, Oman, Qatar, State of Palestine, Saudi Arabia, and the United Arab Emirates, and pilot screening projects have been completed in Jordan, Lebanon, and Tunisia.32 Genetic services are available to help individuals and families to understand their genetic status or risk, and ultimately improve health by reducing morbidity and mortality associated with these conditions. It’s necessary to introduce more awareness-raising programs for genetic testing services in Jordan, to get an early diagnosis for genetic disorders, and to provide the appropriate follow-up, management or treatment. Islamic teachings emphasize the importance of counseling and raising their awareness, and the available means of care and prevention of genetic diseases.34,35 An 88.2% of the respondents think that genetic testing is permissible and not forbidden and only a small minority of the respondents (11.3%) think it’s forbidden and not permissible. The proper understanding and implementation of Islamic principles, therefore, offer a significant framework in research and guidance for addressing social, ethical, and legal issues governing the organization and provision of genetic services in Arab communities.36–39
Medical genetics education assumes particular importance in Arab countries because of the high frequency of genetic disorders and the generally low level of genetic literacy.40 Genetic testing can serve different purposes such as predictive testing which indicate if early diagnosis or diagnostic testing to confirm or rule out a known or suspected genetic disorder in an asymptomatic person.
The majority of the responders believed that genetic testing should take place before marriage, keeping in mind that those responders are at a younger age and planning to get married. Nevertheless, a small minority of the responders decided that they are not planning to do the genetic testing meanwhile or in the future. A mandatory pre-marital screening program for thalassemia have been introduced by the Jordanian government in 2004, which requires all couples who are planning to get married to undergo thalassemia testing, the couple then is informed about the result of the tests in terms of their genetic risks and their choices are discussed. In an ideal situation, effective preventive measures can be put forward preventing the majority of affected births via wise use of the available resources. However, still some people in the Jordanian community make decisions about having children or getting married regardless of the result of the genetic test.
The genetic testing is offered to adults, newborns, preimplantation, or sometimes to families with aggressive disease. Individuals have to be aware that more genetic testing screening approaches may be considered to individuals with high risk and highly recommended before pregnancy. Here in Jordan preventive genetic services that include thalassemia, congenital hypothyroidism, phenylketonuria, and glucose-6-phosphate dehydrogenase deficiency tests are offered by the Ministry of Health.
The spreading of genetic testing is still a relatively slow and expensive process, but the genetic technology nowadays is advancing quickly. The cost and financing of genetic testing and counseling have had a profound impact on access to these services in developing countries. In developing countries, these services are often not implemented in a way that maximizes public access or cost-effectiveness; they are often available and accessible only to the wealthier individuals which account for nearly 20% of the population.41,42 Due to lack of expertise and specialized centers, the situation is similar and even more difficult in middle-income countries such as Jordan and many other developing countries. In our study, slightly more than half of all respondents (53.4%) consider genetic testing is cheap and affordable and (46.6%) consider genetic testing is expensive and not affordable which somehow need to give a second thought before performing the genetic testing if needed.
Regardless of a respectable number of research papers, there are many unanswered ethical issues have to be addressed, particularly the misuse of genetic information.43 How the genetic test is implemented, and what uses are made of its results after. If the genetic data released to third parties such as partners, employers or insurers. Should tested individuals have the decision or allowed to choose or refuse the genetic testing, or should it be mandatory, especially for the newborn screening? Should tested individuals be able to be in charge of access to the results of their tests? All of these areas are fertile ground for future research.
One limitation of our work that we used broad terms “genetic testing” and “cost of genetic testing”. Future studies should be more specific and investigate the knowledge and attitudes about different types of genetic tests such as carrier screening, prenatal testing, newborn screening, diagnoses of genetic conditions, and the presymptomatic detection of late-onset conditions. In addition, the cost and risk of genetic testing procedures vary, depending on a number of factors including the complexity and methodology of the testing procedure.
Conclusion
Jordan, like other Arab countries in the region, is faced with major challenges in providing comprehensive and up-to-date health services in a rapidly advancing field such as genetics testing. Prevention of genetic disorders at the population level depends on a combination of basic public health measures and the education and involvement of the primary health care network. The current study showed that the young Jordanians were familiar with genetic testing, however, intervention efforts are needed to improve awareness, with a special focus on accessibility with reasonable cost and religious awareness of the need and permissibility of genetic testing, to help the community in preventing many health problems related to genetic disorders.
Compliance with Ethical Standards
All procedures followed were in accordance with the ethical standards and with the Helsinki Declaration of 1975, as revised in 2000 (5). Informed consent was obtained from all patients for being included in the study. The study was approved by the Institutional Review Board Committee (17/122/2019) at Jordan University of Science and Technology.
Acknowledgments
The authors would like to thank the Research Ethics Education Program in Jordan and Jordan University of Science and Technology for funding the study (grant number: 2015/271). In addition, the authors would like to thank the Deanship of Research and Graduate Studies at Yarmouk University for its support.
Disclosure
The authors report no conflicts on interest in this work.
References
1. Bertini E, Zanni G, Boltshauser E. Nonprogressive congenital ataxias. Handb Clin Neurol. 2018;155:91–103.
2. Vatankhah S, Jalilvand M, Sarkhosh S, Azarmi M, Mohseni M. Prevalence of congenital anomalies in Iran: a review article. Iran J Public Health. 2017;46(6):733–743.
3. Gim J, Kim W, Kwak SH, et al. Improving disease prediction by incorporating family disease history in risk prediction models with large-scale genetic data. Genetics. 2017;207(3):1147–1155. doi:10.1534/genetics.117.300283
4. Lin J, Marcum CS, Myers MF, Koehly LM. Put the family back in family health history: a multiple-informant approach. Am J Prev Med. 2017;52(5):640–644. doi:10.1016/j.amepre.2016.11.018
5. McGowan M, Glinka A, Highland J, Asaad G, Sharp R. Genetics patients’ perspectives on clinical genomic testing. Per Med. 2013;10(4):339–347. doi:10.2217/pme.13.32
6. Thong MK, See-Toh Y, Hassan J, Ali J. Medical genetics in developing countries in the Asia-Pacific region: challenges and opportunities. Genet Med. 2018;20(10):1114–1121. doi:10.1038/s41436-018-0135-0
7. Mantere T, Kersten S, Hoischen A. Long-read sequencing emerging in medical genetics. Front Genet. 2019;7(10):426. doi:10.3389/fgene.2019.00426
8. Lalani SR. Current genetic testing tools in neonatal medicine. Pediatr Neonatol. 2017;58(2):111–121. doi:10.1016/j.pedneo.2016.07.002
9. Treff NR, Zimmerman RS. Advances in preimplantation genetic testing for monogenic disease and aneuploidy. Annu Rev Genomics Hum Genet. 2017;31(18):189–200. doi:10.1146/annurev-genom-091416-035508
10. Nowak-Sliwinska P, Scapozza L, Altaba ARI. Drug repurposing in oncology: compounds, pathways, phenotypes and computational approaches for colorectal cancer. Biochim Biophys Acta Rev Cancer. 2019;1871(2):434–454. doi:10.1016/j.bbcan.2019.04.005
11. Aruoma OI, Hausman-Cohen S, Pizano J, et al. Personalized nutrition: translating the science of genomics into practice: proceedings from the 2018 American college of nutrition meeting. J Am Coll Nutr. 2019;38(4):287–301. doi:10.1080/07315724.2019.1582980
12. Parker RM, Ratzan SC, Lurie N. Health literacy: a policy challenge for advancing high-quality health care. Health Aff. 2003;22(4):147. doi:10.1377/hlthaff.22.4.147
13. Lillie SE, Brewer NT, O’Neill SC, et al. Retention and use of breast cancer recurrence risk information from genomic tests: the role of health literacy. Cancer Epidemiol Biomarkers Prev. 2007;16(2):249–255. doi:10.1158/1055-9965.EPI-06-0525
14. Brewer NT, Tzeng JP, Lillie SE, Edwards AS, Peppercorn JM, Rimer BK. Health literacy and cancer risk perception: implications for genomic risk communication. Med Decis Making. 2009;29(2):157–166. doi:10.1177/0272989X08327111
15. DeLuca JM. Public attitudes toward expanded newborn screening. J Pediatr Nurs. 2018;38:e19–e23. doi:10.1016/j.pedn.2017.10.002
16. Tarini BA, Simon NJ, Payne K, Gebremariam A, Rose A, Prosser LA. An assessment of public preferences for newborn screening using best-worst scaling. J Pediatr. 2018;201:62–68.e1. doi:10.1016/j.jpeds.2018.05.035
17. Lea DH, Kaphingst KA, Bowen D, Lipkus I, Hadley DW. Communicating genetic and genomic information: health literacy and numeracy considerations. Public Health Genomics. 2011;14(4–5):279–289. doi:10.1159/000294191
18. Lim Q, McGill BC, Quinn VF, et al. Parents’ attitudes toward genetic testing of children for health conditions: a systematic review. Clin Genet. 2017;92(6):569–578. doi:10.1111/cge.2017.92.issue-6
19. Saylor KW, Ekunwe L, Antoine-LaVigne D, et al. Attitudes toward genetics and genetic testing among participants in the Jackson and Framingham heart studies. J Empir Res Hum Res Ethics. 2019;14(3):262–273. doi:10.1177/1556264619844851
20. Michie S, Marteau TM. Response to GIG’s response to the UK clinical genetics society report “the genetic testing of children”. J Med Genet. 1995;32(10):838. doi:10.1136/jmg.32.10.838
21. Ramirez AG, Chalela P, Gallion KJ, et al. Attitudes toward breast cancer genetic testing in five special population groups. J Health Dispar Res Pract. 2015;8(4):124–135.
22. Haga SB, Kim E, Myers RA, Ginsburg GS. Primary care physicians’ knowledge, attitudes, and experience with personal genetic testing. J Pers Med. 2019;9(2):E29. doi:10.3390/jpm9020029
23. Hamamy H, Al-Hait S, Alwan A, Ajlouni K. Jordan: communities and community genetics. Community Genet. 2007;10(1):52–60. doi:10.1159/000096282
24. Abdo N, Ibraheem N, Obeidat N, et al. Knowledge, attitudes, and practices of women toward prenatal genetic testing. Epigenet Insights. 2018;4(11):2516865718813122.
25. Haga SB, Barry WT, Mills R, et al. Public knowledge of and attitudes toward genetics and genetic testing. Genet Test Mol Biomarkers. 2013;17(4):327–335. doi:10.1089/gtmb.2012.0350
26. Etchegary H. Public attitudes toward genetic risk testing and its role in healthcare. Pers Med. 2014;11(5):509–522. doi:10.2217/pme.14.35
27. Henneman L, Vermeulen E, van El CG, Claassen L, Timmermans DR, Cornel MC. Public attitudes towards genetic testing revisited: comparing opinions between 2002 and 2010. Eur J Hum Genet. 2013;21(8):793–799. doi:10.1038/ejhg.2012.271
28. Hann KEJ, Freeman M, Fraser L, et al.; PROMISE study team. Awareness, knowledge, perceptions, and attitudes towards genetic testing for cancer risk among ethnic minority groups: a systematic review. BMC Public Health. 2017;17(1):503. doi:10.1186/s12889-017-4375-8
29. Baker L, Wagner TH, Singer S, Bundorf MK. Use of the internet and e-mail for health care information. Results from a national survey. J Am Med Assoc. 2003;289:2400–2406. doi:10.1001/jama.289.18.2400
30. Andrus MR, Roth MT. Health literacy: a review. Pharmacotherapy. 2002;22:282–302. doi:10.1592/phco.22.5.282.33191
31. Shahmoradi L, Safadari R, Jimma W. Knowledge management implementation and the tools utilized in healthcare for evidence-based decision making: a systematic review. Ethiop J Health Sci. 2017;27(5):541–558. doi:10.4314/ejhs.v27i5.13
32. Therrell BL, Padilla CD, Loeber JG, et al. Current status of newborn screening worldwide: 2015. Semin Perinatol. 2015;39(3):171–187. doi:10.1053/j.semperi.2015.03.002
33. Shawky RM. Newborn screening in the Middle East and North Africa-challenges and recommendations. Hamdan Med J. 2012;5(3):191–192. doi:10.7707/hmj.v5i3.192
34. El-Hazmi MA. Islamic teachings of bioethics in relation to the practice of medical genetics. Saudi Med J. 2007;28(12):1781–1787.
35. Albar MA. Counseling about the genetic disease: an Islamic perspective. East Mediterr Health J. 1999;5(6):1129–1133.
36. Al Aqeel AI. Islamic ethical framework for research into and prevention of genetic diseases. Nat Genet. 2007;39(11):1293–1298. doi:10.1038/ng.2007.14
37. Ghareeb BA. Human genetics and Islam: scientific and medical aspects. J IMA. 2011;43(2):83–90. doi:10.5915/43-2-7014
38. El Shanti H, Chouchane L, Badii R, Gallouzi IE, Gasparini P. Genetic testing and genomic analysis: a debate on ethical, social and legal issues in the Arab world with a focus on Qatar. J Transl Med. 2015;13:358. doi:10.1186/s12967-015-0720-9
39. Zayed H, Ouhtit A. Accredited genetic testing in the Arab Gulf region: reinventing the wheel. J Hum Genet. 2016;61(7):673–674. doi:10.1038/jhg.2016.22
40. Hamamy H, Bittles AH. Genetic clinics in Arab communities: meeting individual, family and community needs. Public Health Genomics. 2009;12(1):30–40. doi:10.1159/000153428
41. Penchaszadeh VB. Preventing birth defects in developing countries. Community Genet. 2002;5:61–69. doi:10.1159/000064632
42. Christianson A, Modell B. Medical genetics in developing countries. Annu Rev Genomics Hum Genet. 2004;5:219–265. doi:10.1146/annurev.genom.5.061903.175935
43. Wauters A, Van Hoyweghen I. Global trends on fears and concerns of genetic discrimination: a systematic literature review. J Hum Genet. 2016;61(4):275–282. doi:10.1038/jhg.2015.151
 © 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2019 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.