Back to Journals » International Journal of General Medicine » Volume 14
Knowledge, Attitude, Practice and Food Poisoning Associated Factors Among Parents in Bench-Sheko Zone, Southwest Ethiopia
Authors Mekonnen B ![]() , Solomon N
, Solomon N ![]() , Yosef T
, Yosef T ![]()
Received 22 January 2021
Accepted for publication 9 April 2021
Published 3 May 2021 Volume 2021:14 Pages 1673—1681
DOI https://doi.org/10.2147/IJGM.S294294
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 4
Editor who approved publication: Dr Scott Fraser
Besufekad Mekonnen,1 Nahom Solomon,1 Tewodros Yosef2
1Department of Public Health, Mizan-Tepi University, Mizan-Aman, Southern Nation Nationality and People Region, Ethiopia; 2Department of Epidemiology and Biostatistics, Mizan-Tepi University, Mizan-Aman, Southern Nation Nationality and People Region, Ethiopia
Correspondence: Besufekad Mekonnen
Department of Public Health, Mizan-Tepi University, P.O. Box: 260, Mizan-Aman, Southern Nation Nationality and People Region, Ethiopia
Email [email protected]
Background: Food poisoning is a food borne disease, mainly resulting from ingestion of food that contains a toxin, chemical or infectious microorganisms like bacteria, virus, parasite, or prion. On the other hand, avoiding food contamination during preparing and feeding is a key factor for reducing the prevalence of food poisoning. This study aimed to assess the knowledge, attitude, self-reported practice and food poisoning associated factors among parents in the selected health centers of Bench-Sheko Zone in Ethiopia.
Methods: An institution-based cross-sectional study was conducted among 408 systematically selected parents in Bench-Sheko zone, Ethiopia. The data were collected through face to face interview using a structured questionnaire.
Results: The median knowledge score was 8.0 with an interquartile range (IQR) of 8.0– 10.0. The median attitude score was 9.0 with an IQR of 6.0– 9.0. The median practice score was 12.0 with an IQR of 10.0– 13.0. A positive correlation was seen between knowledge and attitudes of parents with food poisoning (r= 0.321, P < 0.026), between knowledge and practices of parents towards food poisoning (r= 0.312, P < 0.001) and between attitude and practices result towards food poisoning (r= 0.224, p < 0.031). The parents with a higher education level, employed and who live in a city were the factors significantly associated with higher knowledge scores (p < 0.05). The improved attitude was seen as educational level increased (p < 0.05). The parents with female gender, employed and who live in a city were significantly associated with higher hygienic practices towards the prevention of food poisoning (p < 0.05).
Conclusion: The knowledge, attitude, and self-reported practices of parents regarding food poisoning prevention are associated with each other and are affected by socio-demographic variables. Therefore, adequate emphasis should be given by health sectors to designing strong strategies which address the specific contributing factors for the problem.
Keywords: knowledge, attitude, practices, parents, food poisoning, Ethiopia
Introduction
Food is a known vehicle for many pathogenic and toxigenic agents that cause what are known as food-borne diseases.1,2 Food borne diseases (FBDs) are diseases which are caused by the consumption of contaminated foods or water, with a variety of diseases causing agents ranging from infective organisms, poisonous chemicals, radioactive substances and other harmful substances.1,3 FBDs have increased over the years, and treacherously upset the health and economic well-being of many people in developed and developing countries.3–5
According to World Health Organization (WHO), contaminated food contributes to 1.5 billion cases of diarrhea in children each year, resulting in over three million premature deaths.6,7 Safe food is defined as not causing harm or illness to the consumer.8 Food safety is the processes of handling, preparing and storing of food in ways that prevent contamination by toxic chemicals9 or pathogenic microbes, which result in food-borne illness.1,10
Food poisoning occurs as a result of consuming food contaminated with microorganisms or their toxins; the contamination starting from inadequate preservation methods, unhealthy handling practices, cross-contamination from food contact surfaces, or from persons hiding the microorganisms in their nails and on the skin.11 The presence of poor hygienic practices during food preparation, handling and storage creates the conditions that allow the proliferation and transmission of disease causing organisms such as bacteria, viruses and other food-borne pathogens.2,15 The signs of toxigenic food poisoning mostly appear within 24 hours after eating of contaminated food. The symptoms include nausea, vomiting, diarrhea, abdominal pain, a headache and fever. The life-threatening neurologic, hepatic and renal syndromes may occur several days after intestinal, and may cause permanent disability or death depending upon which microbe is ingested.1,13–15
The incidence of FBDs depends on the hygienic measures implicated in food production and storage, but they could be ineffective if consumers have unhygienic practices and food handling approaches.16 It is recommended to apply different precaution techniques to keep safety of foods, including: to wash hands well and often, especially after using the bathroom, before touching food, and after touching raw food by using soap and warm water and scrub for at least 15 seconds; clean all utensils, cutting boards, and surfaces that you use to prepare food with hot, soapy water; wash all raw vegetables and fruits; keep raw foods (especially meat, poultry, and seafood) away from other foods until they are cooked; and cook all food from animal sources to a safe internal temperature.17 But different studies from Ethiopia have reported that people fail to be concerned of and/or properly apply the prevention techniques.7,17–19
It is known that the KAP of food poisoning are key factors for reducing the prevalence of food-borne diseases in food production and serving area.7,20 In addition, the issue demands more evidence, particularly in southwest Ethiopia. Therefore, this study aimed to assess the knowledge, attitude and self-reported practices related to food poisoning among parents in the selected four health centers of Bench-Sheko zone in southwest Ethiopia. The finding will contribute to devise an intervention of operative, effective and proper health intervention program regarding how to handle food safely and adds evidence in the area of interest.
Methods
Study Design, Setting and Period
An institution based cross-sectional study was conducted among parents attending health institutions from September 1 to December 30, 2019, in former Bench-Maji zone which is currently named as Bench-Sheko zone, Ethiopia. Bench-Sheko Zone is one of the 16 zones in Southern Nation Nationalities and Peoples Regional state (Figure 1), which is located at 585 km southwest of Addis Ababa, the capital city of Ethiopia. The zone has an estimated population of 829,493, and the primary health service coverage of the zone is 92.6%, covering a total catchment area of 19,965.8 km2 with majority (86%, 713,363.98) of the population living in the rural areas. A study was conducted in four randomly selected primary health centers, namely Bire (found in North Bench district), Kite, Debrework (found in South Bench district) and Biftu (found in Guraferda district).
 |
Figure 1 Map of the study area. |
The parents who had children aged less than 6 years old and attending the health centers were selected, interviewed and their responses were recorded. The inclusion criteria were age of 18 years old and above and agreed to participate in the study. Exclusion criteria included parents who were not resident in the study area, had not given birth, who had children over 6 years or who had difficulty in communication.
Sample Size Determination and Sampling Technique
The required sample size was determined using a single population proportion formula 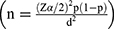 with the assumption of estimated proportions of knowledge, attitude and practice of food poisoning among parents to be 50% (since there is no previous study, the maximum sample size was achieved by taking 50% proportions), 5% margin of error, 95% confidence level, and 10% for non-response compensation. The final sample size calculated for knowledge, attitude and self-reported practice was 422. The total sample size was proportionally allocated for each health center based on the previous year’s cases. Then, a systematic random sampling was employed to select the potential study participants.
with the assumption of estimated proportions of knowledge, attitude and practice of food poisoning among parents to be 50% (since there is no previous study, the maximum sample size was achieved by taking 50% proportions), 5% margin of error, 95% confidence level, and 10% for non-response compensation. The final sample size calculated for knowledge, attitude and self-reported practice was 422. The total sample size was proportionally allocated for each health center based on the previous year’s cases. Then, a systematic random sampling was employed to select the potential study participants.
Data Collection Instrument and Procedures
A structured questionnaire, which was adapted from similar studies,1,21–23 was used. The questionnaire was composed of four parts socio-demographic variables (age, gender, educational status, residency, and number of family members including children, their ages, food preparation habit), food poisoning knowledge related questions including general statements about food poisoning causes (15 questions), food poisoning attitude related questions including statements about eating raw food and washing fruits and vegetables (15 questions), and food poisoning practices related questions regarding eating, drinking and washing hands (20 questions). Moreover, in the knowledge and attitude part, the questionnaire entails five options ranging from “strongly agree” to “strongly disagree”. In the practice section, the respondents had five choices: “always yes”; “most of the time”; ‘sometimes’; “rarely”; and “always no”.
The data were collected by BSc nurses and public health officers. Two days’ training was given for data collectors and supervisors about objectives of the study, contents of questionnaire, and approaches to interview. A pre-test was conducted on 5% of the sample in other primary health centers than the study set up, and necessary amendment of the questionnaires based on the result of the pre-test were considered. Finally data were collected through a face-to-face interview.
Ethical Consideration
Data collection was started after obtaining permission from Mizan-Tepi University Institutional Review Boards (MTU-IRB). Again, a support letter was obtained from the Bench Sheko Zone Health Bureau. All study participants were informed about the purpose of the study, their right to deny participation, anonymity, and confidentiality of the information. Moreover, the verbal informed consent was approved by the Mizan-Tepi University Ethical Review Board, and this study was conducted in accordance with the Declaration of Helsinki.
Data Processing and Analysis
The data were entered in to Epi data manager and analyzed using SPSS software version 22. The descriptive statistics (mean, standard deviation, median and interquartile range) were conducted to summarize the results. Some characteristics were consolidated into dichotomous (binary) variables for ease of analysis and interpretation. Normality test was made by using Kolmogorov Smirnov test. In addition, the Mann–Whitney U-test and the Kruskal–Wallis H-test were performed to determine significance difference between the mean values. Moreover, Pearson correlation coefficient was designed to examine a possible correlation between continuous variables (knowledge, attitude and practice scores). The level of significance was declared at p value <0.05.
Results
Socio-Demographic Profiles
Of the 422 sampled populations, 408 were interviewed and completed data were collected, giving a response rate of 96.7%. Almost all respondents were women (97.3%). The mean age of the study participants was 32.5 (SD±5.2) years. One hundred sixty-eight (41.2%) of them have achieved secondary educational level followed by 37% of parents who are able to read and write. Again 88% and 74.3% of participants were unemployed and rural residents respectively. Mothers were found to be the responsible body for preparing food for the family (98.8%) (Table 1).
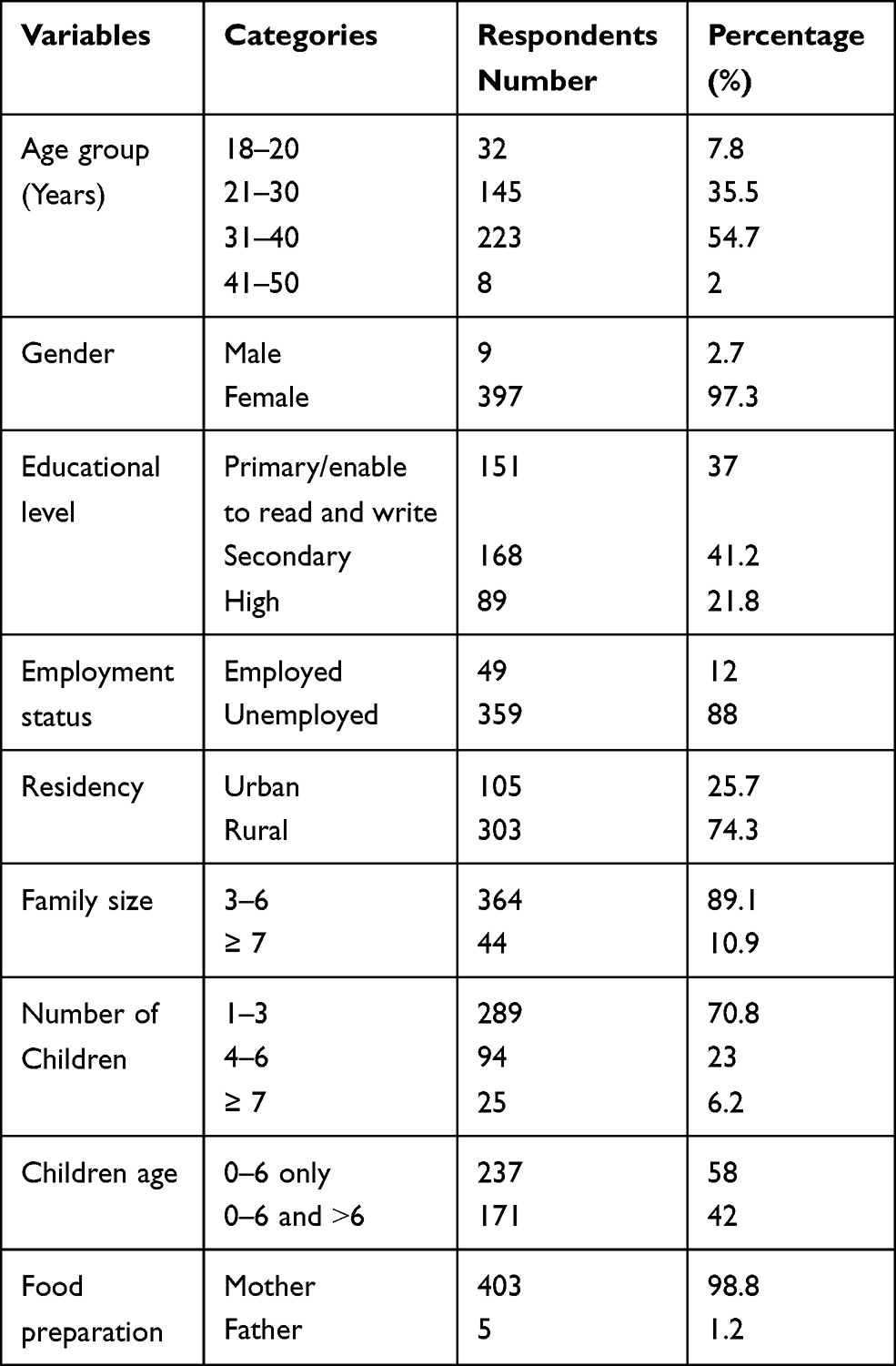 |
Table 1 Socio-Demographic Status of Parents in Bench-Sheko Zone, Ethiopia; 2019 (N= 408) |
Knowledge About Food Poisoning
The mean value of knowledge about food poisoning was 9±3.2 SD. When the respondents were asked about the highly risky foods for food poisoning, 42% of the study participants responded that eating raw meat is highly risky for food poisoning, 75% responded that eating raw unwashed vegetables is highly risky for food poisoning and 73.4% responded that drinking raw milk is highly risky for food poisoning. Furthermore, 78%, 74%, 75%, 78.4% and 74.5% of the respondents responded correctly that raw white cheese, unwashed not peeled fruits, uncovered leftover cooked food, untreated surface and rainwater, and raw eggs, respectively, were risky food. The majority of respondents (88%) responded that well cooked food is free from microbes that cause food poisoning and that keeping food in refrigerator will slow down the microbial growth and multiplication, so, prevent food poisoning (52%). Nearly half of the respondents (50.9%) said that there is no risk of food poisoning from eating leftover cooked food reserved in refrigerator for 2–3 days. Regarding hygienic condition of parents, 75% of the respondents said that poor hygienic practice of parents could be the source of food poisoning. Instead, only 38.7% of the respondents agreed that some toxins produced by microbes and cause food poisoning are resistant to heating temperature of food.
Attitude Regarding Food Poisoning
The mean value of attitude regarding food poisoning was 8±4.8 SD. Half of the respondents reported that washing hands with soap before preparing (51.2%) and eating food (50.2%), along with thorough washing of vegetables and fruits (50.4%) are necessary to prevent food poisoning. Concerning raw milk, 58.4% of the respondents correctly disagreed that there is no risk of disease from drinking raw cow milk right after milking, 59.7% disagreed that raw milk is more healthy and nutritious than pasteurized or boiled milk. Regarding raw eggs, half of respondents (51.2%) disagreed that raw eggs are more healthy and nutritious than cooked ones, while 22.7% disagreed that there is no risk of disease from drinking raw eggs. Regarding vegetables and fruits, 50.8% of the respondents disagreed that eating vegetation and fruits directly from the plant without wiping has no risk of disease occurrence. Instead, majority of the respondents agreed that baby feces are free from pathogenic microbes if he/she is not sick. Majority of the respondents (74.5%) agreed that rainwater collected in reservoir is safe to drink without any treatment and 49.6% agreed that there is no risk of disease from eating cooked food reserved at room temperature for 1 day if covered.
Practices About Food Poisoning
The mean practice score was 12±4.8 SD. Regarding practices questions, more than half of the respondents wash their hands with soap and water before eating and preparing food, after contact with animals (55.4%) and after using the toilet (55.6%). In addition, 58% of the respondents wash fresh vegetables and fruits before eating while 57.4% wash their hands with water and soap after handling raw unwashed vegetables. Likewise, 54.4% of the respondents may eat fresh vegetables and fruits after just wiping it, without washing it (56.3%) or pick it up from the plants during a field trip and eat it without washing (59.1%). Half of the respondents do not eat raw eggs and 55% of the respondents do not eat raw or half-cooked meat. Moreover, 60% of the respondents drink raw milk. A high percentage of respondents drink from rainwater collected without any treatment (78.4%) and 75% of parents do not eat foods out of their home (hotels, restaurants and cafeteria), 88% of parents may eat raw white cheese prepared from raw unpasteurized milk. Furthermore, 57.4% of the respondents were cooked food left at room temperature for over 6 h without sufficient heating.
The Kruskal–Wallis test was used to assess the association between socio-demographic variables and knowledge. The result revealed that educational level, residency and employment status were significantly associated with knowledge (P value < 0.05). However, no significant association was seen between age, gender, number of family member, number of children and food preparation habit with knowledge. It is observed that, parents with relatively highest level of education have good level of knowledge about food poisoning. In addition, respondents who live in urban setting have better knowledge than those who live in rural area (Table 2).
 |
Table 2 Association Between Socio-Demographic Variable and KAP of Food Poisoning, Among Parents in Bench Sheko Zone, 2019 |
According to Kruskal–Wallis test, there was significant association between gender, educational level and residency with attitude about food poisoning (p value < 0.005). On the other hand, age, employment status, number of children, number of family, age of the children and food preparation habit did not show any significant association with attitude (Table 2).
It is observed that gender, education and residency had significant association with practices or taking measures against food poisoning. Other socio-demographic variables such as age, employment status, family number, age of children and food preparation habit did not show any significant association with practice of food poisoning. The result revealed that female parents do have better hygiene practice than males. In addition, the respondents with high level of educational status had better hygienic practices than low educational level. Moreover, parents who live in urban area experience better hygienic practices than those who live in rural setting (Table 2).
The Correlations Between Knowledge, Attitude and Practice Towards Food Poisoning
Pearson’s correlation coefficient was used for testing the existence of any correlation between knowledge, attitude and self-reported practices of parents with food poisoning. Accordingly, positive correlation was seen between knowledge and attitudes of parents with food poisoning (r= 0.321, P value < 0.026). This shows that parents who had good knowledge were more likely to have good attitude regarding food poisoning. In addition, there was positive correlation between knowledge and practices of parents towards food poisoning (r= 0.312, P value 0.001). This implies that parents who had good knowledge were more likely to have good hygiene practices towards food poisoning. Moreover, there was positive correlation between attitude and self-reported practices result towards food poisoning (r= 0.224, p value 0.031). It is well expressed that parents who had good attitude were more likely to have good hygiene practices regarding food poisoning.
Discussion
This study assessed the knowledge, attitude, and self-reported practice and food poisoning associated factors among parents in the selected health centers of Bench-Sheko zone, southwest Ethiopia. In the developing world, females are more commonly responsible for food preparation; the female carries the responsibility for family care as a wife, from cleaning and arranging the house to preparing the food for all members of the family. In addition, the female, as a mother, takes care of her children.1,24,25 This is also clearly found in this study where mothers are the responsible body of preparing food, and since mothers have also other house work burdens, there could be gaps in following necessary precautions for keeping safety of food.
Recent studies asserted that knowledge, attitude and practice are key factors in reducing the prevalence of food-borne diseases in food processing and serving area.1,21,22,26 On the other hand, they themselves are also influenced by many factors including educational status, gender and age of food handlers.23,27–29 In the current study, it is revealed that educational level, residency and employment status were significantly associated with knowledge. Badrie et al30 and Zyoud et al1 have also reported similar findings, in which a significant association between educational level and knowledge was scored. Parents with a high level of education reported higher knowledge scores than those with a lower level. In addition, parents who live in the urban setting reported higher scores than those who live in the rural setting. This consistency might be explained by some close features of study population. Parents, who are educated, employed and who live in towns showed higher knowledge scores and attitude is also improved as educational level increased. Parents with female gender, employed and who live in town had higher hygienic practices towards the prevention of food poisoning. Therefore addressing educational gaps and accessing health information to rural community is demanding.
Educational level, gender and residency were also found to have significant influence on attitude about food poisoning. Although gender was found as one factor affecting parents’ attitude regarding food poisoning, opposing result was reported from a study conducted in Palestine,1 which revealed there was no significant association between gender and attitude regarding food poisoning. Of course, the difference might happen because in our study majority of respondents were women. Again, men in this study area could pass most of their time at field, and/or may contact many people and as a result may have more exposure to information, on the other hand, those who live in towns and/or who had achieved highest level of education may be influenced to experience good attitude. Parents with a high education level reported a good attitude compared to those with a lower level. Zyoud et al, Altekruse et al, and Ozilgen S. have reported comparably close result.1,31,32 Again, influence of health information and education status is found to be the most important factor affecting attitude of parents toward food poisoning, so working in filling these gaps would bring better change.
Regarding practice, again gender, level of education and residency were found to have significant association about taking measures against food poisoning. This result is consistent with a study conducted in Debark town and Palestine.1,7 Similarity may be explained by comparability of study population and setting. Parents who live in a town had better hygienic practice than those who live in rural area. In addition, female parents scored higher than males. A possible explanation for this result may be the lack of adequate experience in food preparation between female parents compared to males. Contrary to this, study reports from Henok et al and Zyoud et al1,7 revealed that female parents and village residences lack hygienic knowledge and practices regarding food poisoning. Whenever people live at a distance from towns where many health services and information are easily accessible, it is clear that health problems may occur and failing to keep safety of food is one of the areas which results in big health impact, mainly resulting in food poisoning.
Significant association was also shown between knowledge, attitude and practice. Accordingly; parents who had good knowledge have also demonstrated a good level of attitude and practice. This result is consistent with a study conducted in Iran, Palestine, China and West Indies.1,22,30 This implies knowledge is a primary and a very important potential for securing food safety and enabling people to take measures to reduce occurrence of food poisoning, as a result, it demands interventions targeting specific population group so as to empower them to prevent food poisoning.
Generally it is found that knowledge, attitude and practice towards taking measures against food poisoning are still limited and demands efforts to promote public health through applying different health interventions mainly health education targeting the main associated factors.
Conclusion and Recommendations
Two-thirds of the parents have good knowledge about food poisoning but only half of them have good attitude and experience of taking preventive measures to avoid food poisoning. The study also found that gender; educational status, occupation and place of residence were the main factors which showed significant effect and parents who had good knowledge have also demonstrated a good level of attitude and practice. Therefore, emphasis should be given to fill the gaps by applying necessary interventions which consider the major contributing factors as well. Consequently, health sectors in the local area shall give emphasis in fostering knowledge of parents regarding food poisoning and design strategy to change attitude of parents regarding poisoning, facilitate them to experience a good preventive measures and shall promote for good knowledge, attitude and taking preventive measures about food poisoning. Moreover, academic sectors and other sectors working in the area shall design strategies and implement for fostering knowledge, attitude and preventive measures concerning food poisoning and shall make advanced level study of both qualitative and quantitative method to identify the gaps and associated factors more. This study has come with important results but should be used without forgetting its limitation of social desirability bias.
Abbreviations
FBDs, food born diseases; IRB, internal review board; IQR, inter quartile range; KAP, knowledge, attitude and practice; MTU, Mizan-Tepi University; SD, standard deviation; SPSS, Statistical Package for Social Science; WHO, World Health Organization.
Data Sharing Statement
The data that support the findings of this study are available from the corresponding author upon reasonable request.
Acknowledgment
The authors acknowledge Mizan Tepi University for unreserved support. In addition, the authors express their appreciation and thanks to Mizan-Tepi University research and community service directorate for overall facilities during the survey. Lastly, the researchers would like to address their deepest thanks to all staff of College of Health Sciences in MTU for their valuable comments.
Funding
The Authors acknowledged Mizan-Tepi University for financial support.
Disclosure
The authors declare that they have no conflicts of interest for this work.
References
1. Zyoud S, Shalabi J, Imran K, et al. Knowledge, attitude and practices among parents regarding food poisoning: a cross-sectional study from Palestine. BMC Public Health. 2019;19(1):1–10. doi:10.1186/s12889-019-6955-2
2. Zeeshan M, Shah H, Durrani Y, Ayub M, Jan Z, Shah M. A questionnaire-based survey on food safety knowledge during food-handling and food preparation practices among university students. J Clin Nutr Diet. 2017;03(02):1–8. doi:10.4172/2472-1921.100052
3. Ulusoy BH, Çolakoğlu N. What do they know about food safety? A questionnaire survey on food safety knowledge of kitchen employees in Istanbul. Food Health. 2018;4(4):283–292. doi:10.3153/fh18028
4. Ismail KA. Assessment of the knowledge, attitude and practice about food safety among Saudi Population in Taif. Biomed J Sci Tech Res. 2018;8(2):4–10. doi:10.26717/bjstr.2018.08.001629
5. Akabanda F, Hlortsi EH, Owusu-Kwarteng J. Food safety knowledge, attitudes and practices of institutional food-handlers in Ghana. BMC Public Health. 2017;17(1):1–9. doi:10.1186/s12889-016-3986-9
6. Zvenyika F. The knowledge, attitudes and practices, and compliance regarding the basic prerequisite programmes (prps) of food safety management systems of food service workers in boarding schools and restaurants in Masvingo province, Zimbabwe; 2017 (November).
7. Dagne H, Raju RP, Andualem Z, Hagos T, Addis K. Food safety practice and its associated factors among mothers in debarq town, Northwest Ethiopia: community-based cross-sectional study. Biomed Res Int. 2019;2019:1–8. doi:10.1155/2019/1549131
8. Mohammed AFH. Food safety knowledge, attitude and self‐reported practices among food handlers in Sohag Governorate, Egypt. East Mediterr Heal J. 2019;25(9):1–5.
9. Mekonnen B, Siraj J, Negash S. Determination of pesticide residues in food premises using QuECHERS method in Bench-Sheko Zone, Southwest Ethiopia. Biomed Res Int. 2021;2021:1–13. doi:10.1155/2021/6612096
10. Yusuf TA, Chege PM. Awareness of food hygiene practices and practices among street food vendors in Nasarawa State, Nigeria. Int J Health Sci Res. 2019;9(7):156–164.
11. Ngoc T, Thanh C. Food safety behavior, attitudes and practices of street food vendors and consumers in Vietnam; 2015.
12. Warner K. Street food vending: vendor food safety practices and consumers’ behaviours, attitudes and perceptions; 2013.
13. Sharma S, Sangha JK. Relation between food safety awareness and disease incidence: a study of home food preparers in Punjab. Stud Ethnomed. 2015;9(2):255–261. doi:10.1080/09735070.2015.11905443
14. Malavi DN. Food Safety knowledge, attitude and practices of orange-fleshed sweetpotato puree handlers in Kenya. Food Sci Qual Manag. 2017;67(April2018):54–63.
15. Oladoyinbo CA, Akinbule OO, Awosika IA. Knowledge of food borne infection and food safety practices among local food handlers in Ijebu-Ode Local Government Area of Ogun State. J Public Health Epidemiol. 2015;7(9):268–273. doi:10.5897/jphe2015.0758
16. World Health Organization. Five keys to safer food manual safer food manual. Vol 3, 206AD. Available from: http://www.mdpi.com/1660-4601/6/11/2833/.
17. Eshetu D, Kifle T, Hirigo AT. Knowledge, attitudes, and practices of hand washing among aderash primary schoolchildren in Yirgalem Town, Southern Ethiopia. J Multidiscip Healthc. 2020;13:759–768. doi:10.2147/JMDH.S257034
18. Adane M, Teka B, Gismu Y, Halefom G, Ademe M. Food hygiene and safety measures among food handlers in street food shops and food establishments of Dessie town, Ethiopia: a community-based cross-sectional study. PLoS One. 2018;13(5):1–13. doi:10.1371/journal.pone.0196919
19. Tshipamba ME, Lubanza N, Adetunji MC, Mwanza M. Evaluation of the effect of hygiene practices and attitudes on the microbial quality of street vended meats sold in johannesburg, south- africa journal of food: microbiology, safety & hygiene. J Food Microbiol Saf Hyg. 2018;3(2):1–10. doi:10.4172/2476-2059.1000137
20. Adel HS, Ns M, Sm A-R. Assessment of the knowledge, attitude and practice towards food poisoning of food handlers in some Egyptian worksites. Egypt J Occup Med. 2014;38(1):79–94. doi:10.21608/ejom.2014.789
21. Zolfaghari H, Khezerlou A, Alizadeh-Sani M, Ehsani A. Food-borne diseases knowledge, attitude, and practices of women living in East Azerbaijan, Iran. J Anal Res Clin Med. 2019;7(3):91–99. doi:10.15171/jarcm.2019.017
22. Henson S, Reardon T. Private agri-food standards: implications for food policy and the agri-food system. Food Policy. 2005;30(3):241–253. doi:10.1016/j.foodpol.2005.05.002
23. Patil SR, Cates S, Morales R. Consumer food safety knowledge, practices, and demographic differences: findings from a meta-analysis. J Food Prot. 2005;68(9):1884–1894. doi:10.4315/0362-028X-68.9.1884
24. Aa MB. Knowledge, attitude and practice of female teachers regarding safe food handling; is it sufficient? An Intervention Study, Zagazig, Egypt. Egypt J Occup Med. 2017;41(2):271–287.
25. Omar BA, Shadia SM, Anas SD, Mohammed AE. Food hygiene knowledge, attitude and practices among hospital food handlers in Elmanagil City, Sudan. African Journal of Microbiology Research. 2020;14(4):106–111. doi:10.5897/AJMR2020.9323
26. Soon JM, Baines R, Seaman P. Meta-analysis of food safety training on hand hygiene knowledge and attitudes among food handlers. J Food Prot. 2012;75(4):793–804. doi:10.4315/0362-028X.JFP-11-502
27. Zanin LM, Thimoteo D, Vera V; GeQual Study Group of Food Quality. Centro de Desenvolvimento do Ensino SC. Food Res Int. 2017;100(Pt 1):53–62. doi:10.1016/j.foodres.2017.07.042
28. Barrie D. The provision of food and catering hospital services in. J Hosp Infect. 1996;33(1):13–33. doi:10.1016/S0195-6701(96)90026-2
29. Badrie N, Gobin A, Dookeran S, Duncan R. Consumer awareness and perception to food safety hazards in Trinidad, West Indies. Food Control. 2006;17(5):370–377. doi:10.1016/j.foodcont.2005.01.003
30. Altekruse SF, Street DA, Fein SB, Levy AS. Consumer knowledge of foodborne microbial hazards and food-handling practices. J Food Prot. 1995;59(3):287–294. doi:10.4315/0362-028X-59.3.287
31. Ozilgen S. Food safety education makes the difference: food safety perceptions, knowledge, attitudes and practices among Turkish university students. J Verbr Leb. 2011;6(1):25–34. doi:10.1007/s00003-010-0593-z
32. Ma L, Chen H, Yan H, Wu L, Zhang W. Food safety knowledge, attitudes, and behavior of street food vendors and consumers in Handan, a third tier city in China. BMC Public Health. 2019;19(1):1–13. doi:10.1186/s12889-019-7475-9
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.