Back to Journals » Pediatric Health, Medicine and Therapeutics » Volume 12
Knowledge, Attitude, and Practices of Parents About Immunization of Infants and Its Associated Factors in Wadla Woreda, North East Ethiopia, 2019
Authors GebreEyesus FA ![]() , Tarekegn TT, Amlak BT, Shiferaw BZ
, Tarekegn TT, Amlak BT, Shiferaw BZ ![]() , Emeria MS
, Emeria MS ![]() , Geleta OT
, Geleta OT ![]() , Mewahegn AA
, Mewahegn AA ![]() , Feleke DG
, Feleke DG ![]() , Chanie ES
, Chanie ES ![]()
Received 22 December 2020
Accepted for publication 8 April 2021
Published 10 May 2021 Volume 2021:12 Pages 223—238
DOI https://doi.org/10.2147/PHMT.S295378
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Roosy Aulakh
Fisha Alebel GebreEyesus,1 Tadesse Tsehay Tarekegn,1 Baye Tsegaye Amlak,1 Bisrat Zeleke Shiferaw,1 Mamo Solomon Emeria,1 Omega Tolessa Geleta,1 Agerie Aynalem Mewahegn,1 Dejen Getaneh Feleke,2 Ermias Sisay Chanie2
1Department of Nursing, College of Medicine and Health Sciences, Wolkite University, Wolkite, Ethiopia; 2Department of Pediatrics and Neonatal Nursing, College of Health Sciences, Debre Tabor University, DebreTabor, Ethiopia
Correspondence: Fisha Alebel GebreEyesus
Department of Nursing, College of Medicine and Health Sciences, Wolkite University, PO Box 07, Wolkite, Ethiopia
Tel +251 918644178/94286581
Email [email protected]
Introduction: Improving infant immunization coverage and timeliness is a key health policy objective in many developing countries such as Ethiopia. Despite this, full immunization coverage in Ethiopia becomes low with the concurrent significant burden of vaccine-preventable diseases among infants. A previously published study acknowledged that parental knowledge, attitude, and practice towards infant immunization are vital issues to improve coverage and influence uptake.
Objective: To assess parents’ knowledge, attitude, practice, and its associated factors regarding immunization of infants at Wadla Woreda, North East Ethiopia, 2019.
Material and Methods: A community-based cross-sectional study was employed among 418 parents from March to April 2019 in Wadla Woreda, North East Ethiopia. A stratified sampling technique was used to approach the study subjects. An interviewer-administered structured questionnaire was used. The collected data were cleaned, coded, and entered in EPI-Info 7.2 and transferred to SPSS version 25.0 for analysis. Binary logistic regression analyses were performed to identify variables having a significant association with parental knowledge, attitude, and practice. Variables with a p-value of ≤ 0.05 and AOR with 95% CI were declared as having a statistically significant association during multivariable logistic regression analysis.
Results: In this study, 65.1%, 57.3%, and 55.3% of the parents had good knowledge, a favorable attitude, and good practice towards infant immunization, respectively. Parent’s educational status (AOR=5.330), urban residency (AOR=2.788), favorable attitude (AOR=4.308) and got immunization service two–three times (AOR=3.227) and four–five times (AOR=2.254) were statistically associated with knowledge of parents. Parents who attend primary school [AOR=0.451) and secondary school [AOR=0.320), parents who were mothers of the child [AOR=3.813), and respondents who had good knowledge about infant immunization (AOR= 4.592) were significantly associated with a favorable parental attitude. Infant immunization practice was significantly associated with parental education who attend primary school (AOR=2.513), secondary school (AOR=2.546) and higher education (AOR=11.988), parents who had good knowledge of infant immunization (AOR= 4.206), and short waiting time (AOR=3.881).
Conclusion and Recommendation: Parental KAP towards infant immunization was found to be lower than most of the study findings quoted in this study. Improving the knowledge, attitude, and practice of parents about immunization and vaccine-preventable diseases was recommended by providing health education and health promotion interventions.
Keywords: knowledge, attitude, practice, parents, mothers, childhood immunization, vaccination
Introduction
Immunization is unquestionably one of the most indispensable public health interventions to reduce major illnesses that lead to child mortality and morbidity.1 The extermination, elimination, and considerable minimization of childhood vaccine-preventable diseases (VPDs), as well as the extending of life expectancy in many countries, are an important output of immunization achievement.2
Globally, it is estimated that around 22.6 million infants were partially protected.3 In 2016, routine immunization services such as the DTP3 vaccine did not reach about 19.5 million children under 1 year of age worldwide.4 About 70% of these children are in 10 countries, and more than 50% of them are living in Africa including Ethiopia, Kenya, and South Africa.5
Previous studies carried out worldwide showed that the death of children is more common in underdeveloped countries. Among 9 million deaths of children worldwide as a result of VPDs, a higher proportion happened in sub-Saharan Africa, which was 4.4 million, from this about 472,000 children passed away every year before their fifth birthday largely from VPDs in Ethiopia.6,7
Various reports revealed that VPDs are still responsible for about one-fourth of deaths occurring annually among children less than 5 years of age. Thus, VPDs put a significant economic and social crisis among individuals, families, and communities as a whole. Children who are exposed to these preventable diseases usually suffer from numerous growth and developmental squeals.5,8
In Ethiopia, the Expanded Program on Immunization was launched by providing six traditional antigens in 1980. The Program was reset subsequently and was capable of providing 10 vaccines to under 1 year of age at the moment5. These vaccines are financed by the GAVI, the National and subnational Government, UNICEF, and WHO and are given without payment in immunization clinics nationwide.9 However, several factors are related to low immunization status. Rural residence, wealth status, child sex and age, long-distance to a health facility, low access to immunization service, poor health infrastructure, inadequate awareness of mothers/caregivers, mothers’ perception to the accessibility of vaccines, missed opportunity, place of delivery, living altitude, lower number of trained manpower, and high staff turnover.5,10–13.
Optimal vaccination coverage is one of the most essential indicators of immunizations success and children’s better health outcome.2 To attain the required outcome in terms of vaccination coverage for most of the VPDs,
the Global Vaccine Action Plan 2011–2020 declared by the World Health Assembly in 2012, calls on all countries to reach >90% national coverage for all vaccines in the respective countries’ routine immunization schedule by 2020.
Considering this, Ethiopia has envisioned to -end all preventable newborn and child deaths by 2035. To this end in 2012, Ethiopia has led the development of the “Promise Renewed Child survival Roadmap” with a commitment to end preventable child death to drop the under-five mortality rate to less than 20/1000 live births by 2035.14,15
Despite the implementation of these strategies, to accomplish universal coverage in the EPI and reduce under-five mortality, vaccination coverage in Ethiopia was found to be less than the expected one and under-five mortality is also higher. According to the Ethiopian Mini Demographic and Health Survey (EMDHS) report, in 2019 showed that under-five mortality rate was 55 deaths per 1000 live births, close to 2 in 10 children (19%) have not received any vaccinations at all and only 4 out of 10 children (43%) have received all basic vaccinations.16
Parents’ knowledge, attitude, and practices regarding immunization are the most important factors that could contribute to their immunization decisions.17 Thus, parents’ decisions about immunization are very crucial for enhancing the immunization rate and compliance. Their compliance, in turn, leads to full immunizations of children, which prevents VPDs in children and for inhibiting any possible immunization errors.18,19
Moreover, some studies have been published globally regarding parents’ knowledge, attitude, and practices about infant immunizations.20,21 There is only a single study published nationally and no studies have been reported in the study area and the Woreda is known for frequent outbreaks of vaccine-preventable diseases, especially measles. Therefore, this study aims to assess the knowledge, attitude, and practices of parents regarding immunization of infants at Wadla Woreda, North East Ethiopia, 2019. It will also help policymakers, program implementers, and service providers in identifying the obstacles to utilization of EPI service and enhance infant immunization status to attain the goals of universal immunization. It also helps as a foundation for future studies.
Materials and Methods
Study Design
A community-based quantitative cross-sectional study was employed.
Study Period and Area
The study was carried out in Wadla Woreda, the Amhara Regional State of Ethiopia from March 6 to April 6, 2019. Wadla Woreda is found 250 km away from Bahir Dar, the capital city of Amhara Regional State, and 642 km from Addis Ababa.22
Wadla is bordered on the southeast by Delanta, on the southwest by Dawunt, on the north by Meket, and on the northeast by GubaLafto. The major town in Wadla is Kone. There are 23 kebeles with a total population size of 132,545 people of which 66,935 are female (50.5%), and 65,610 are male,17, 947 children of 0–59 months (13.5%), 6693 <2 years (5%) and 4122 infants (3%). The health institutions located in Wadla Woreda provide currently available vaccine in Ethiopia including measles second dose without charge to succeed the second comprehensive multiyear plan set by the Federal Ministry of Health.22
Source Populations
The source population was all mothers–infants pair aged less than 1 year in Wadla Woreda.
Study Population
Randomly selected mothers who live in the selected kebeles for at least 1 year. The study participants have been interviewed in their own houses.
Inclusion Criteria
Mothers who were voluntary to be involved in the study and those who had children aged under 1 year’s lives in the selected kebeles were included in the study.
Exclusion Criteria
Those mothers who were mentally/critically ill and not voluntarily participate in the study.
Sample Size
The sample size for this study was determined by using a single population proportion formula [n = [(Za/2)2.P (1-P)]/d2] by assuming a 95% confidence level (Z a/2 = 1.96), a margin of error of 5%, P=proportion of clients who are knowledgeable about immunization in Addis Ababa (55%),23 and a 10% addition for non-response rate. The final sample size will be 418.
Sampling Technique and Procedure
First, the total kebeles in the district was stratified into 20 rural kebeles and 3 urban kebeles. Then, seven rural and two urban kebeles were selected by lottery method from the total 23 kebeles in the district. Proportional allocation method was used to select the required amount of infants from the selected household. The first sampled infant in each household was selected by randomly choosing a direction from a central location in the kebele, and then counting the household along that directional line to the edge of the kebele area till the required number of infants has been fulfilled. For those households with more than one eligible infant, only one infant was included by the lottery method. When the selected household is locked, or the parents did not volunteer, the nearest household with an eligible infant was included in the study (Figure 1).
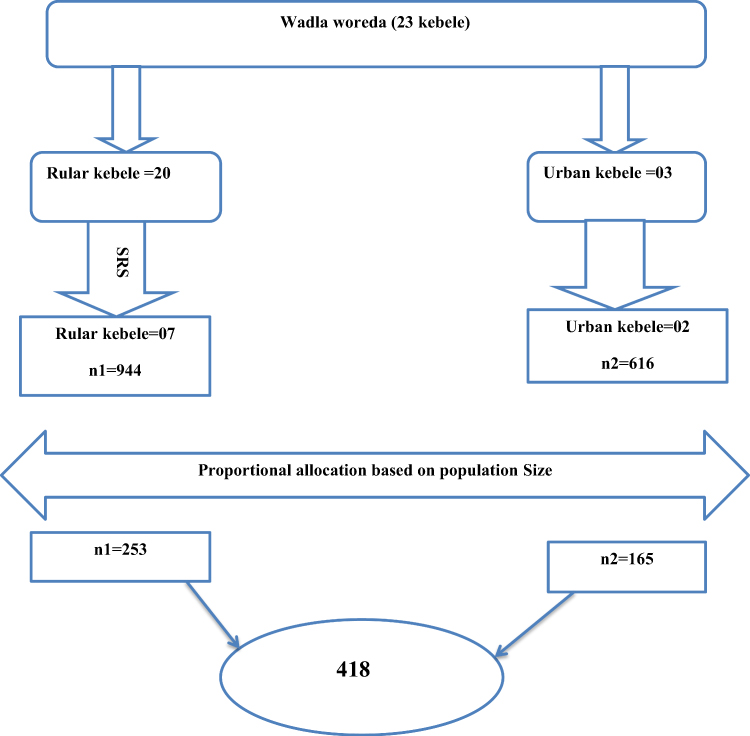 |
Figure 1 The schematic presentation of the sampling procedure to select the study participants in Wadla Woreda, North East Ethiopia, 2019 (n=418). |
Variables
Dependent Variable
- Knowledge, attitude, practice.
Independent Variable
Age, gender, religion, ethnicity, educational status, marital status, residence, occupation, means of transport, time is taken to reach health institution, waiting time.
Data Collection Instrument (Tools) and Procedure
Data were collected through a pretested, structured, and interviewer-administered questionnaire developed from an extensive literature search.
Data were collected by six clinical nurses who are fluent in the local language and supervised by two bachelor of science nurses. Following this, the collected questionnaire was checked for completeness and consistency of the data by the principal investigator on a daily basis.
Most of the questionnaire were adapted from previously conducted studies with some changes based on the local context and it consisted of five main themes: (1) demographics, which surveyed parents socio-demographic information, including gender, age, educational status, marital status, occupation, residence, religion, ethnicity, and monthly income, as well as the demographic data of the child (age, gender, birth order): (2) source of Information: (3) knowledge about immunization; (4) attitudes toward immunization and (5) practices relevant to immunization.
The knowledge status of the participants was measured by eight knowledge-related questionnaires. Participants were given “true,” “false,” or “I don’t know” response options to these items. A correct response to an item was assigned 1 point, while an incorrect/do not know the response was assigned 0 points. Study participants who scored the median and above were considered to have a “good knowledge” and those who scored below were considered as having a “poor knowledge” about infant immunization.
The attitude of the participants towards infant immunization was measured using nine items rated on a three-point Likert scale as “Agree”, “Disagree” and “Neutral”. Study participants who scored the median and above on attitude measuring item were considered to have a “favorable attitude” and those who scored below the median were considered as having “unfavorable attitude”
To measure practices, participants were asked how often they visit the health center to receive immunization service for their infant. Besides this, they were asked yes/no questions on whether the health team greets you; the health care worker tells you the type of the vaccine, a dose of vaccine, next immunization schedule.
Participants were given “yes” or “no” response options to these items. A correct response to an item was assigned 1 point, while an incorrect response was assigned 0 points. Study participants who scored the median and above were considered to have a “good practice” and those who scored below were considered as having a “poor practice” towards childhood immunization.
Data Quality Assurance and Control
The quality of data was ensured through training of data collectors and pretesting of the questionnaire. The principal investigator along with data collectors made frequent checks on the data collection process to ensure the completeness and consistency of the gathered data and daily-based corrections were made accordingly.
The questionnaire was translated initially from English to Amharic (The local language of the respondents) by an expert translator and then back to English to ensure consistency of the questionnaire and for the sake of analysis. The questionnaire was pretested on 5% of the mothers or caregivers of children in kebele which are not primarily selected for the study, and the findings were excluded from the main study. Based on the pretest, the time needed to complete an interview, and the total number of days needed for data collection were estimated. The necessary amendments were made upon the identification of ambiguities of the tools in the wording and logic. In addition to this, the instrument for KAP was tested for reliability and validity and accordingly; the Cronbach’s alpha coefficient was found to be 0.703.
Data Processing and Analysis
The data were cleaned, coded, and entered into EPI-Info version 7.2.2.2 and transferred to SPSS version 25.0 statistical package for further analysis. Data cleaning was performed to check for accuracy, consistencies, and missing values and variables.
The results of the analysis were mainly presented using frequency, tables, and graphs. A bi-variable logistic regression was carried out to determine candidate variables for the multivariable logistic regression model. Those variables which revealed a statistically significant value at a p-value of ≤0.25 in the bivariable analysis were selected for multivariable logistic regression.
For model fit, Hosmer and Lemeshow test was carried out and found to be t (p=0.249, 0.997, and 0.603 for knowledge, attitude, and practice, respectively) which indicated the final model was well fitted. The multicollinearity effect among candidate variables was carried out (checked) using variance inflation factor (VIF) and tolerance test between independent variables and found to be in a normal range. Variables with a p-value of 0.05 with 95% CI for AOR in multivariable logistic regression were used to determine the statistically significant association between independent and dependent variables.
Ethical Considerations
“This study and the verbal informed consent process was approved by the University of Gondar Institutional Review Board. All participants provided verbal informed consent, participants under the age of 18 years were approved to provide informed consent on their own behalf. Official letters were obtained from the district health office to collect the data. The purpose of the study was explained to the study participants, anonymity, privacy, and confidentiality were ensured. This study was conducted in accordance with the Declaration of Helsinki.”
Result
Socio-Demographic Characteristics of the Respondents
Four hundred and eighteen study participants enrolled in the study with a response rate of 100%. The highest proportion of respondents 128 (30.6%) were within the age group of 25–29 years with a median age of 28.00 (24.00–33.00 IQR) years. It showed that 388 (92.8%) parents who participated in this study were mothers of the children and 362 (86.6%) were married. Two hundred and twelve (50.7%) of the infants who received immunization services were males.
Majority of the respondents (90.9%) were orthodox Christian followers and 264 (63.2%) of the parents were housewives. Regarding the educational status of the respondents, 189 (45.2%) had not attended formal education while three-fifths (60.5%) of the respondents were residing in rural areas (Tables 1 and 2).
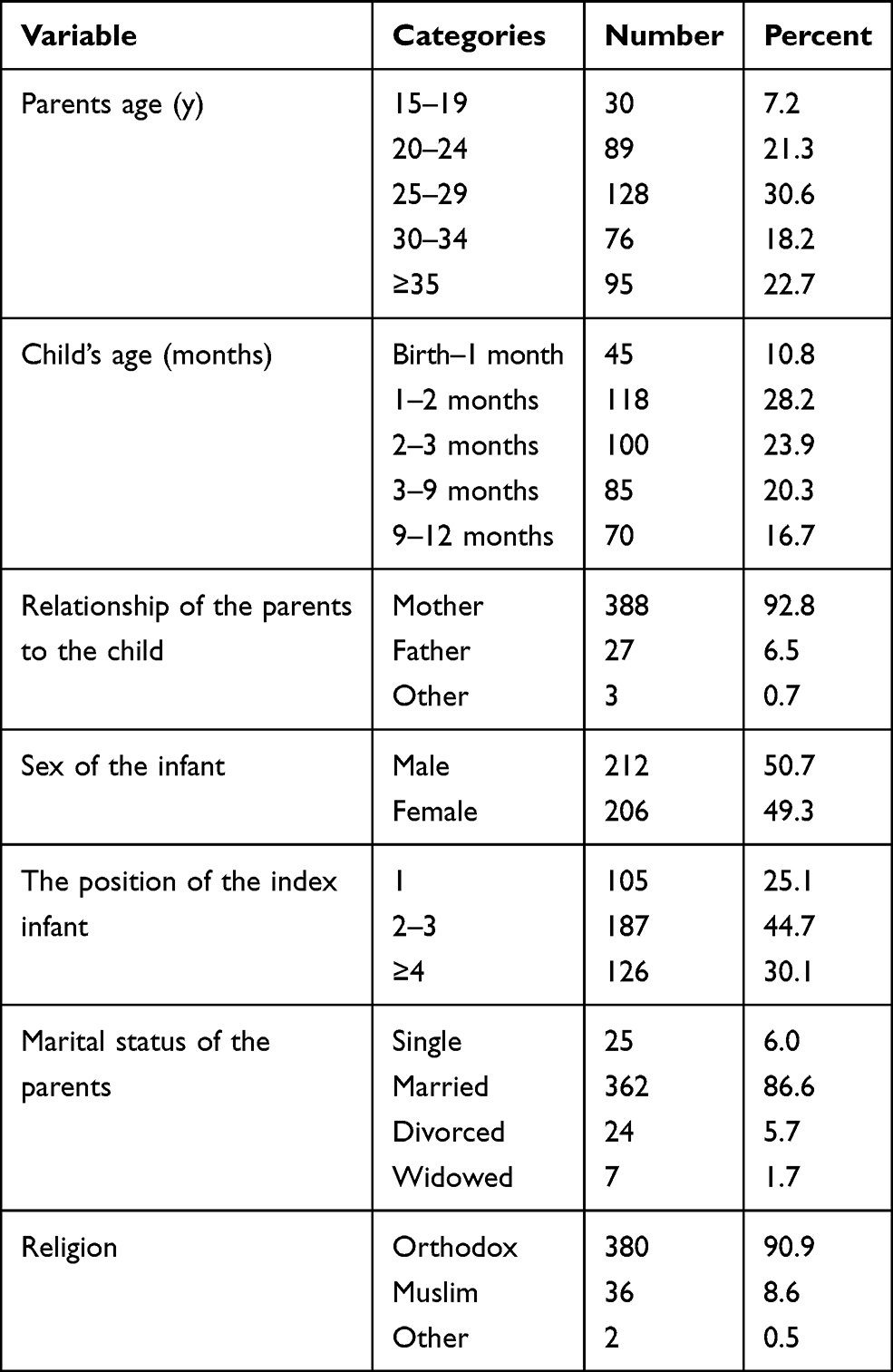 |
Table 1 Socio-Demographic Characteristics of Parents Whose Children Receiving Immunization Service in Wadla Woreda, North East Ethiopia, 2019 (n=418) |
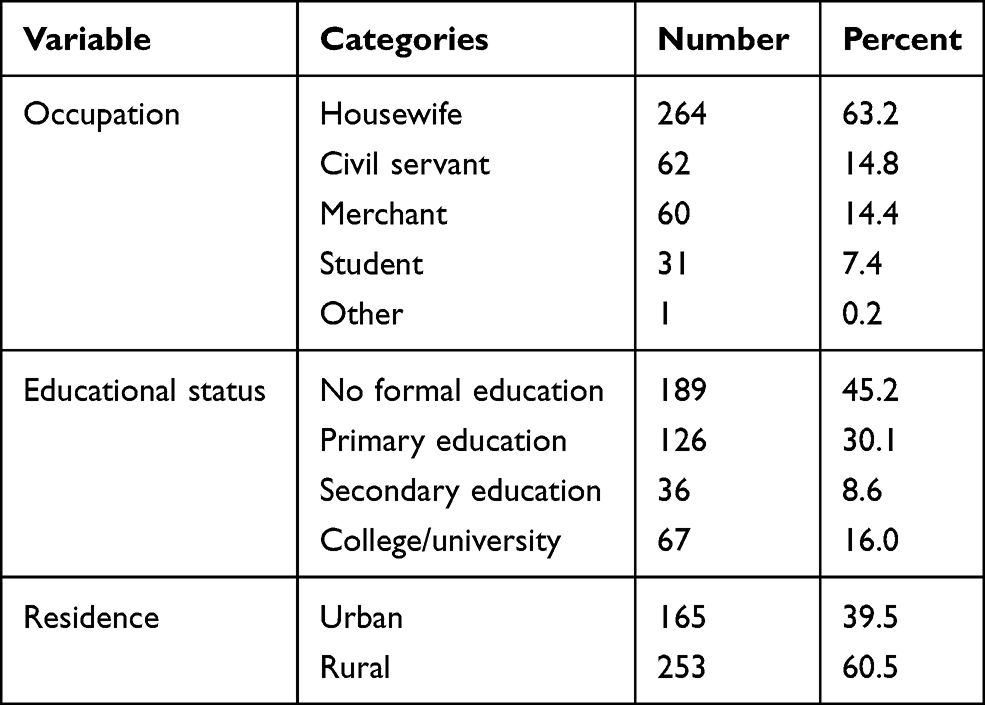 |
Table 2 Continued Socio-Demographic Characteristics of Parents Whose Children Receiving Immunization Service in Wadla Woreda, North East Ethiopia, 2019 (n=418) |
Knowledge of Parents About Infant Immunization
Based on the knowledge item assessed, around four-fifths of the study participants (80.4%) were aware of EPI target diseases and 367 (87.8%) of respondents replied that vaccination prevents infectious disease.
Of the study participants, 57.7% of the parents utilized health workers as the major source of information followed by radio while only 13.19% seek information from neighbors and friends (Figure 2).
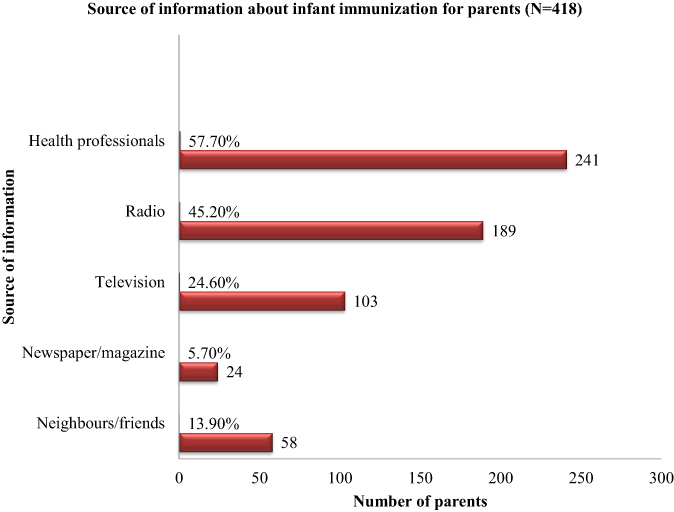 |
Figure 2 A source of information about infant immunization to parents in Wadla Woreda, North East Ethiopia, 2019 (n=418). |
The majority of the respondents 364 (87.1%) said that it is important to vaccinate breastfeeding infants and 317 (75.8%) vaccination is not harmful. Around 90% of the parents were agreeing to immunize their baby full dose while three-fifths of them thought infants should begin an immunization program just after birth 301 (72%) of parents were knowledgeable about when they should return for vaccination. And only 148 (35.4%) of the parents understand the side effects of vaccination (Table 3). And, 65.1% of the parents had good knowledge (Figure 3).
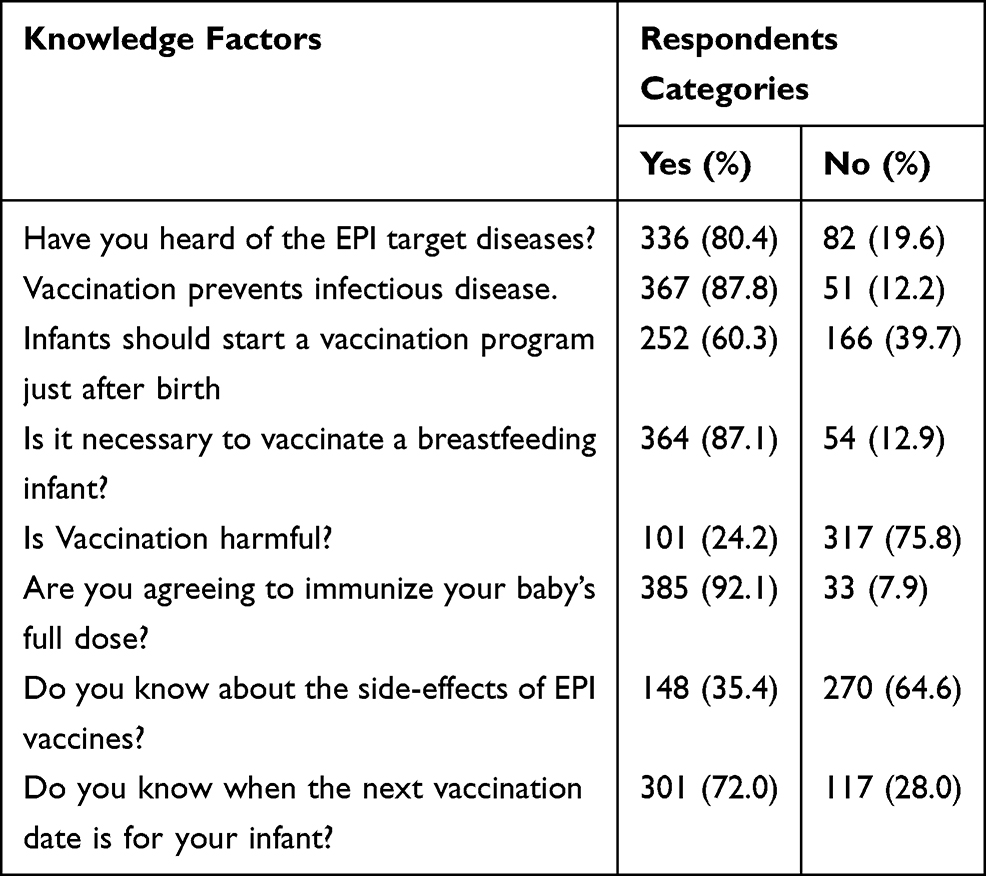 |
Table 3 Knowledge of Respondent Parents Regarding Infants’ Immunization in Wadla Woreda, North East Ethiopia, 2019 (n=418) |
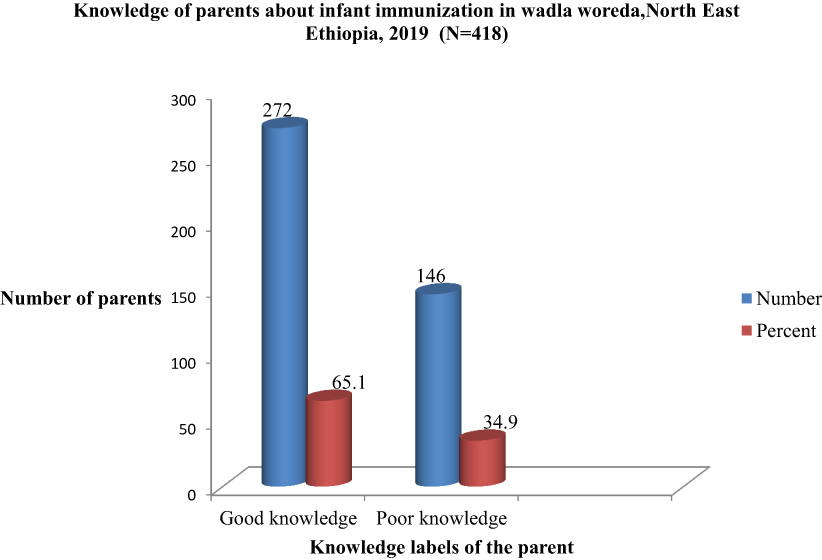 |
Figure 3 Knowledge of parents about immunization in Wadla Woreda, North East Ethiopia, 2019 (n=418). |
Factors Affecting Knowledge of Parents About Their Infants’ Immunization
To assess the association of different independent variables with the outcome, bivariable logistic regression analysis was carried out and for a crude association, all variables with a p-value <0.25 were candidates for multivariable logistic regression. Due to this, parental age, child age, the position of index child, marital status, educational status, residence, frequency of visit, means of transport, service waiting time, traveling time, time spent on immunization, levels of attitude and practice were found to have an association and become eligible for multivariable analysis. Then, the multivariable logistic regression analysis indicated that educational status, residence, attitude, and frequency of visit were found to be statistically significant predictors of parents’ knowledge (Table 4).
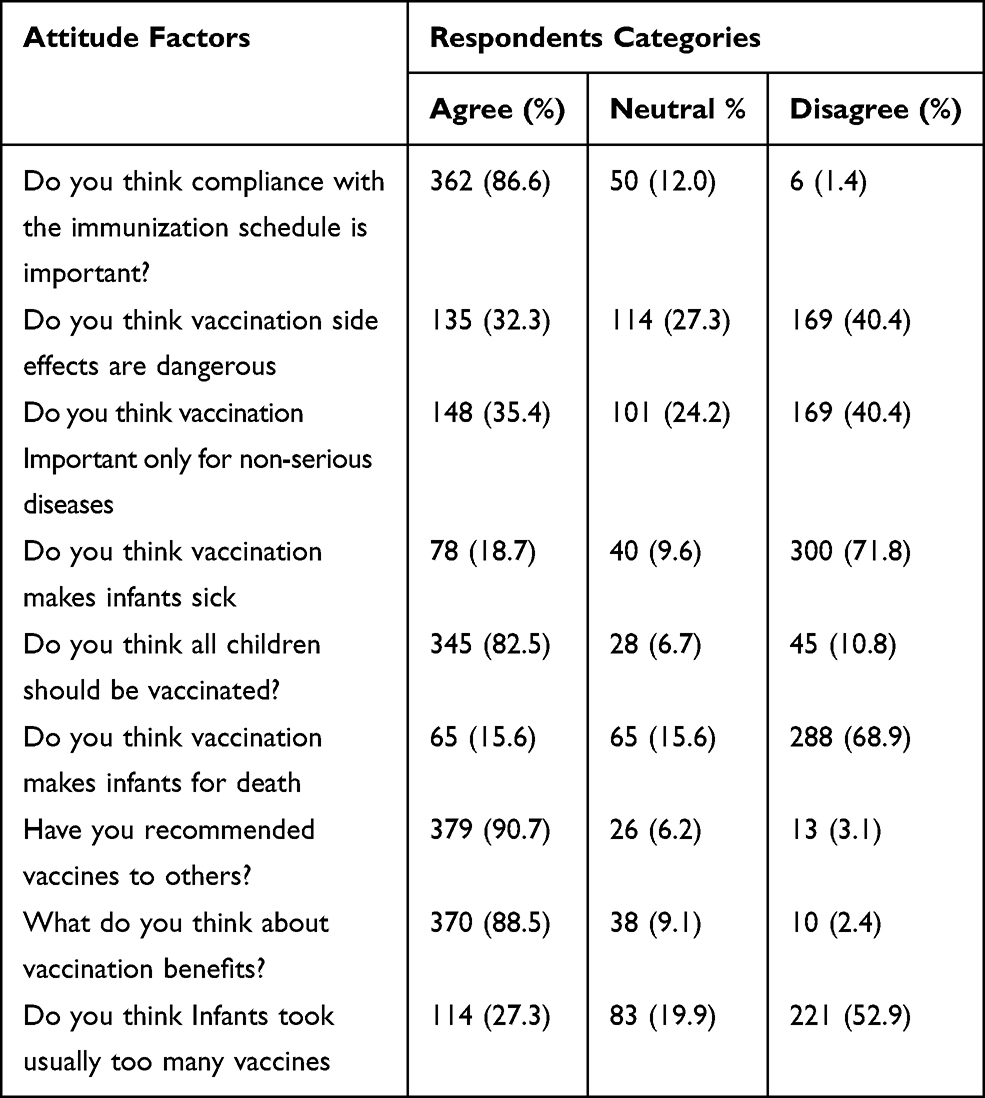 |
Table 4 Attitude of Respondent Parents’ Towards Infants’ Immunization in Wadla Woreda, North East Ethiopia, 2019 (n=418) |
Literate parents who attend higher education were about five times (AOR=5.330, 95% CI: (1.919–14.803)) more likely to be knowledgeable than illiterate respondents.
Parents who reside in an urban area were about two folds (AOR=2.788, 95% CI: (1.617–4.807) more likely to be knowledgeable than rural residents.
This study also shows parents who had a favorable attitude towards infant vaccination were four times (AOR=4.308, 95% CI: (2.609–7.111) more likely to be knowledgeable than their counterparts. Besides, parents who got immunization service two-three times and four-five times were three times (AOR=3.227, 95% CI: (1.543–6.748) and two times (AOR=2.254, 95% CI: (1.029–4.938) more likely to be knowledgeable respectively than parents who get the service at one occasion.
Attitude of Parents About Infant Immunization
Based on the attitude item assessed, the majority of the respondents 362 (86.6%) thought that compliance to immunization schedule is important and 370 (88.5%) Immunization is crucial for the health of the infant. On the other hand, 78 (18.7%) of respondents believed that immunization makes infants sick, and 65 (15.6%) leads to death.
Around 90% of the parents were recommended vaccines to others and 345 (82.5%) thought that all infants should be vaccinated.
Over one-third of the parents thought that vaccination side effects are dangerous and important only for non-serious diseases. Similarly, around one-fourth of the parents believed that infants took usually too many vaccines (Table 5). And, 57.1% of the parents had a favorable attitude (Figure 4).
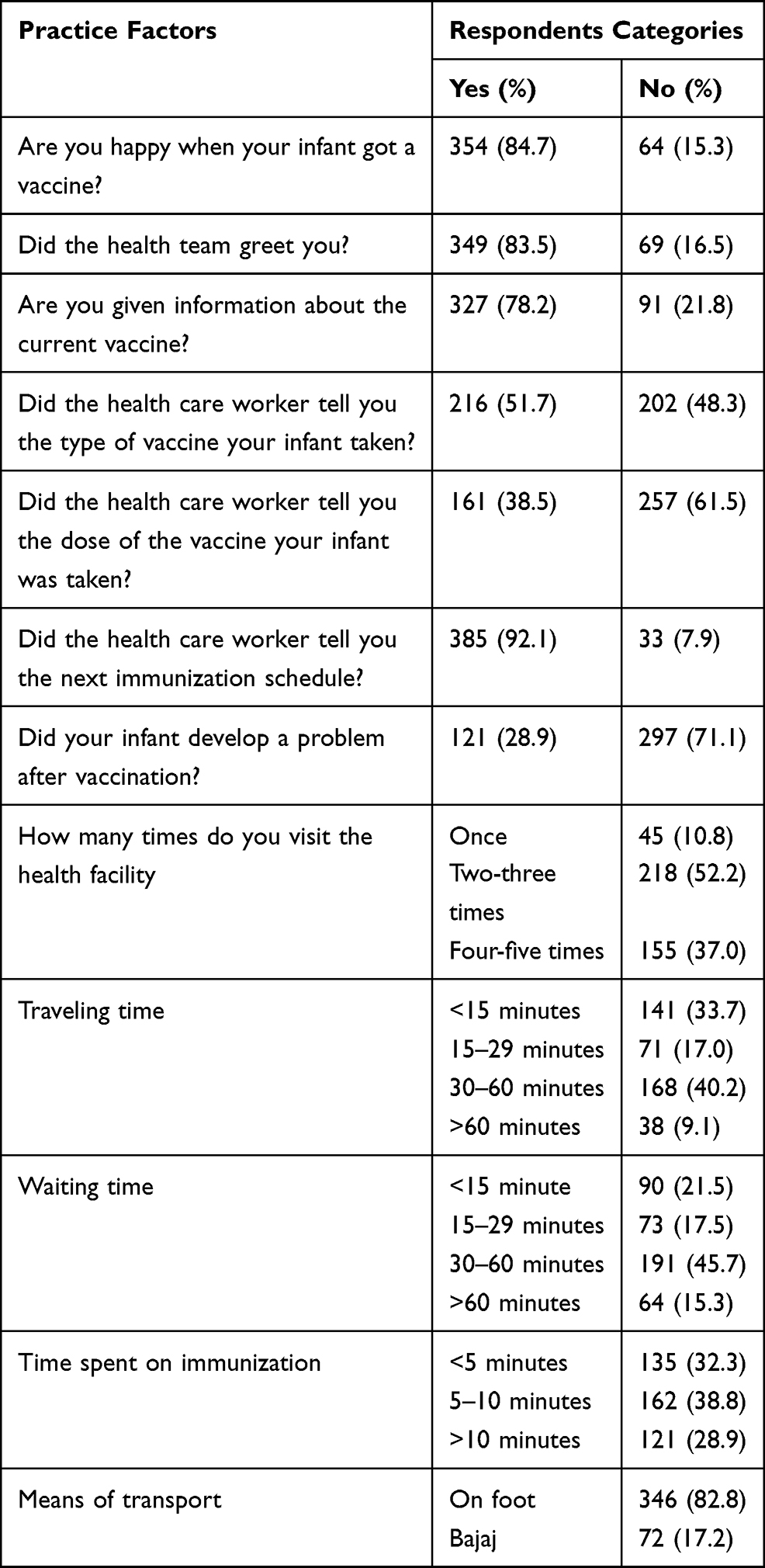 |
Table 5 Practice and Access-Related Factors Regarding Immunization of Infants in Wadla Woreda, North East Ethiopia, 2019 (n=418) |
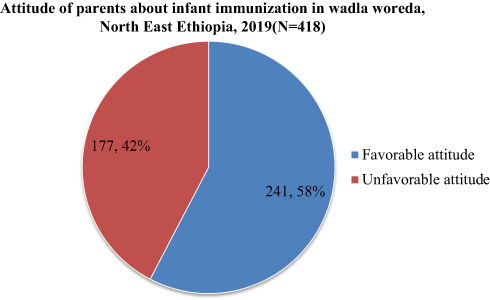 |
Figure 4 Parent’s attitude towards immunization service in Wadla Woreda, North East Ethiopia, 2019 (n=418). |
Factors Affecting Attitude of Parents About Infants’ Immunization
Literate respondents who attend primary school and secondary schools were 55% [AOR=0.451, 95% CI: (0.205–0.994) and 68% [AOR=0.320, 95% CI: (0.112–0.916) less likely to had a favorable attitude towards infant immunization than parents who attend higher education, respectively.
Similarly, the analysis revealed that parents who were mothers of the child were three times [AOR=3.813, 95% CI: (1.185–12.266) more likely to had a favorable attitude towards infant immunization than their counterparts. In addition to this, respondents who had good knowledge about infant immunization were four folds (AOR= 4.592, 95% CI: (2.709–7.786) more likely to had a favorable attitude towards infant immunization than their counterparts (Table 6).
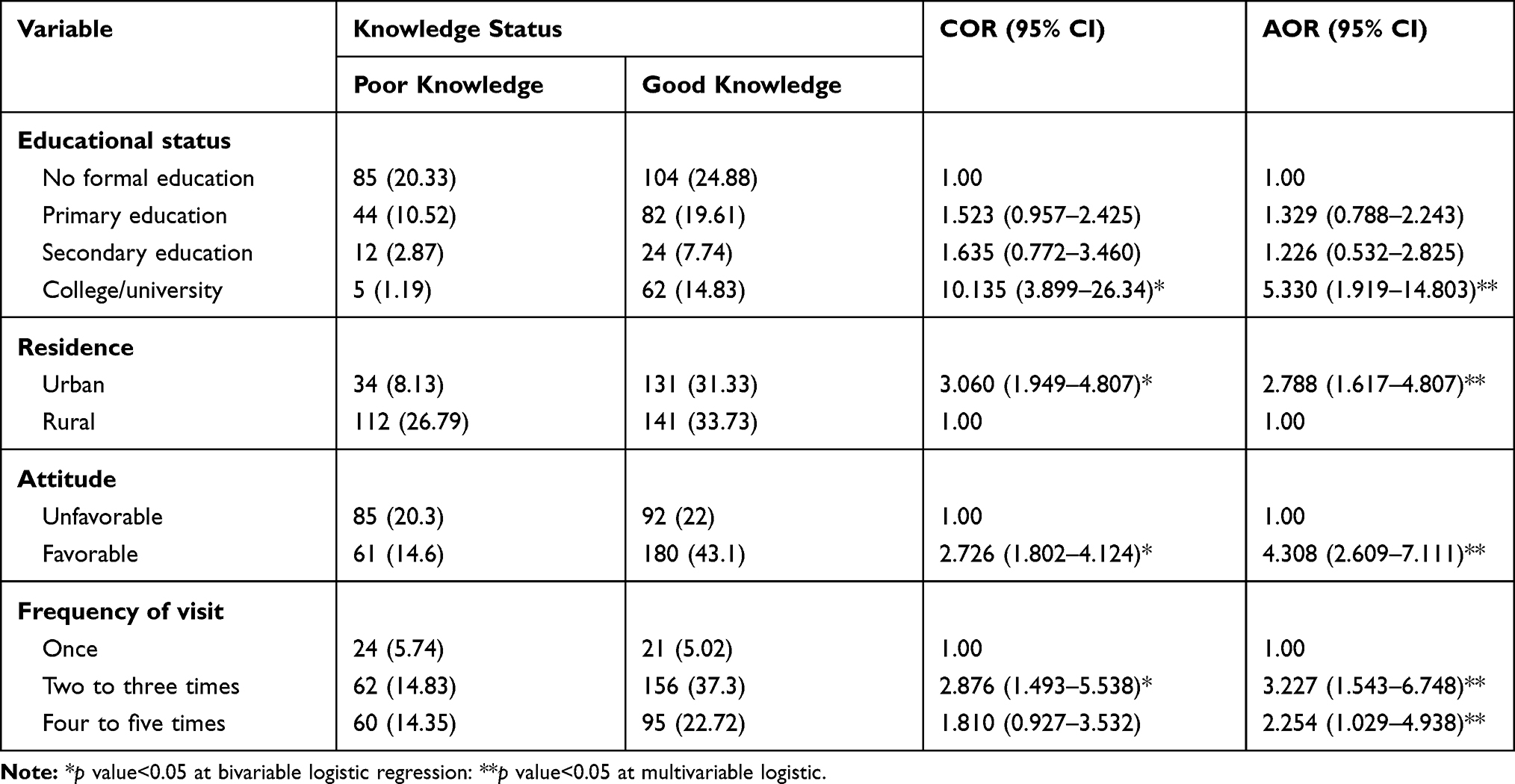 |
Table 6 Factors Associated with Respondent Parents’ Knowledge Regarding Immunization of Infants in Wadla Woreda, North East Ethiopia, 2019 (n=418) |
Practice and Access Related Factors Regarding Immunization of Infants
Regarding the number of visits to the centers, 45 (10.8%) parents visited the health facility one time, whereas 218 (52.2%) and 105 (37%) of the parents visited the health facility two to three times and four to five times, respectively.
Among the study participants, the majority of parents were 83.4% happy when their children got the vaccine and 81.7% of them got greeting from the health care providers. Moreover, 77.9% of the parents were informed about the current vaccine, 55% of the parents were getting information about the type of vaccine their infant took whereas only 35.3% of the parents informed about the dose of the vaccine.
Among the study participants, 91.2% of the parents were informed about the next immunization schedule of their infant and 27% of the infants developed problems after vaccination.
One-third (33.7%) of the parents reach the health facility within <15 minutes, 71 (17.0%) within 15–30 minutes, 168 (40.2%) within 30–60 minutes, and 38 (9.1%) travels more than an hour. By considering waiting time, 212 (50.7%) wait <30 minutes and the remaining 206 (49.3%) wait for >30 minutes. Regarding time spent in vaccination. One hundred and thirty-five (32.3%) of the parents spent <5 minutes, 162 (38.8%) spent 5–10 minutes, and 121 (28.9%) spent >10 minutes. And, 82.8% of the parents traveling through their foot to reach the health facility and the rest uses Bajaj (Table 7), whereas 231 (55.3%) of the parents had Good practices of infant immunization (Figure 5).
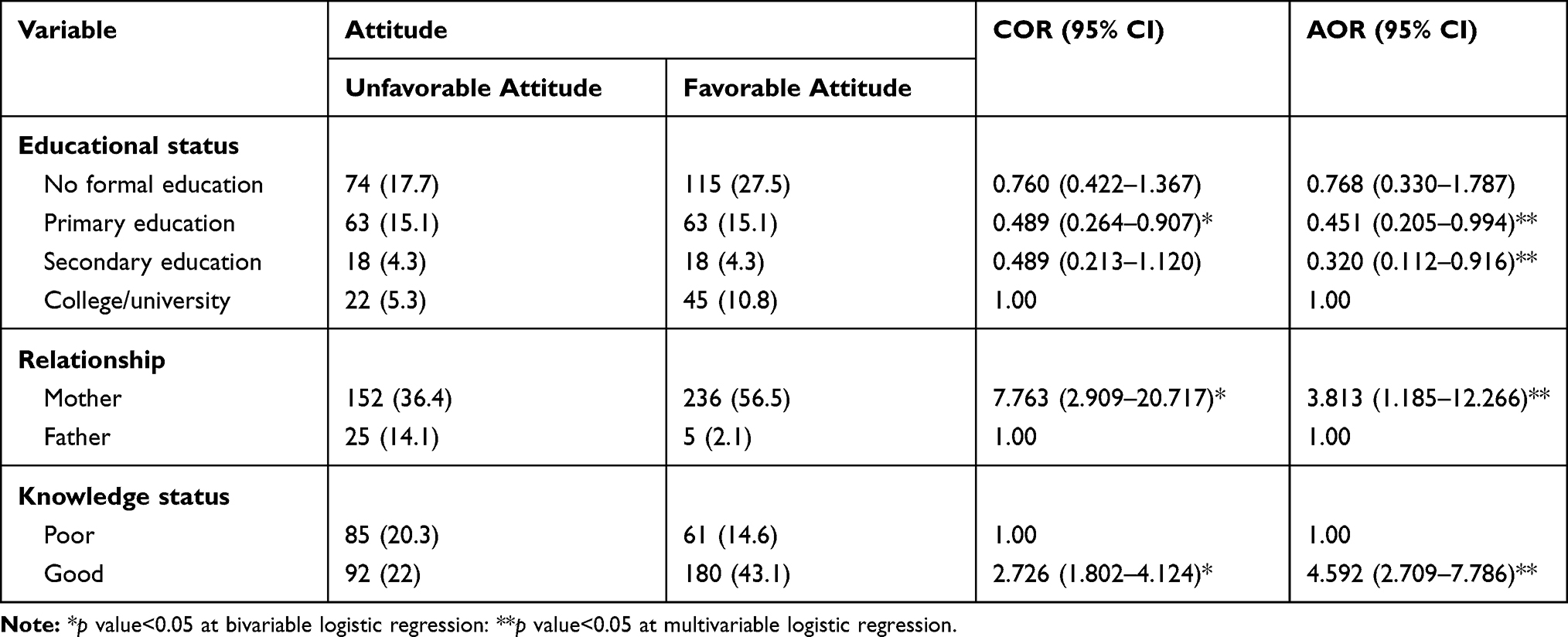 |
Table 7 Factors Associated with Respondent Parents’ Attitude Regarding Immunization of Infants in Wadla Woreda, North East Ethiopia, 2019 (n=418) |
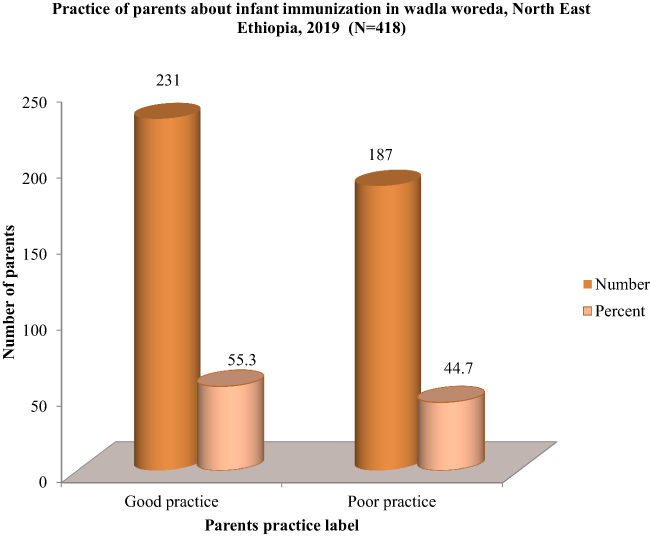 |
Figure 5 Parent’s practice towards immunization service in Wadla Woreda, North East Ethiopia, 2019 (n=418). |
Generally, 65.1%, 57.3%, and 55.3% of the parents in the Wadla district had good knowledge, a favorable attitude, and good practice about infant immunization, respectively (Figure 6).
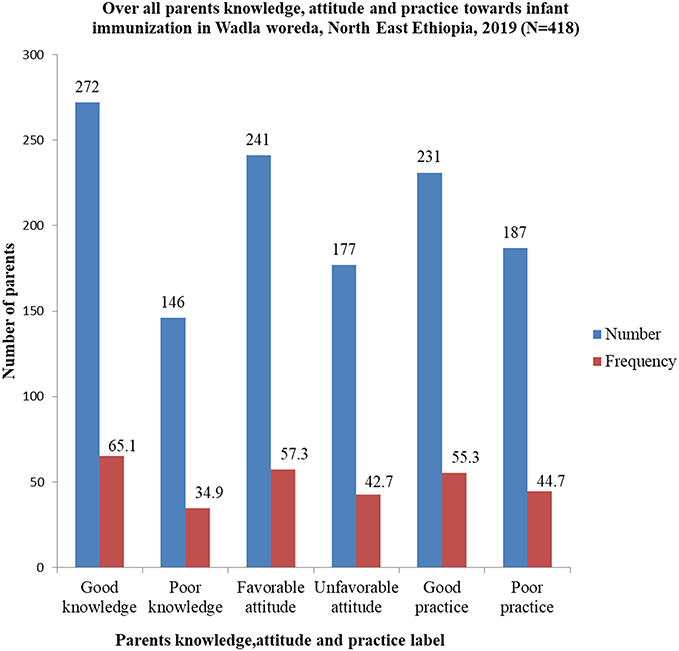 |
Figure 6 Overall knowledge, attitude, and practice of parents about immunization in Wadla Woreda, North East Ethiopia, 2019 (n=418). |
Factors Affecting Practices of Parents Towards Their Infants Immunization
Literate parents who attend primary school, secondary school, and higher education were about two times (AOR=2.513,95% CI: (1.526–4.136), two times (AOR=2.546, 95% CI: (1.159–5.9590) and twelve times (AOR=11.988, 95% CI: (4.470–32.147), respectively, more likely to practice infant immunization than illiterate respondents. Besides this, parents who had good knowledge of infant immunization were fourfold (AOR= 4.206, 95% CI: (2.597–6.811) more likely to practice than their counterparts.
This study also revealed that parents who wait a shorter time to get immunization service were three folds [AOR=3.881, 95% CI: (1.769–8.515) more likely to practice infant immunization than parents who wait a long time to get immunization service (Table 8).
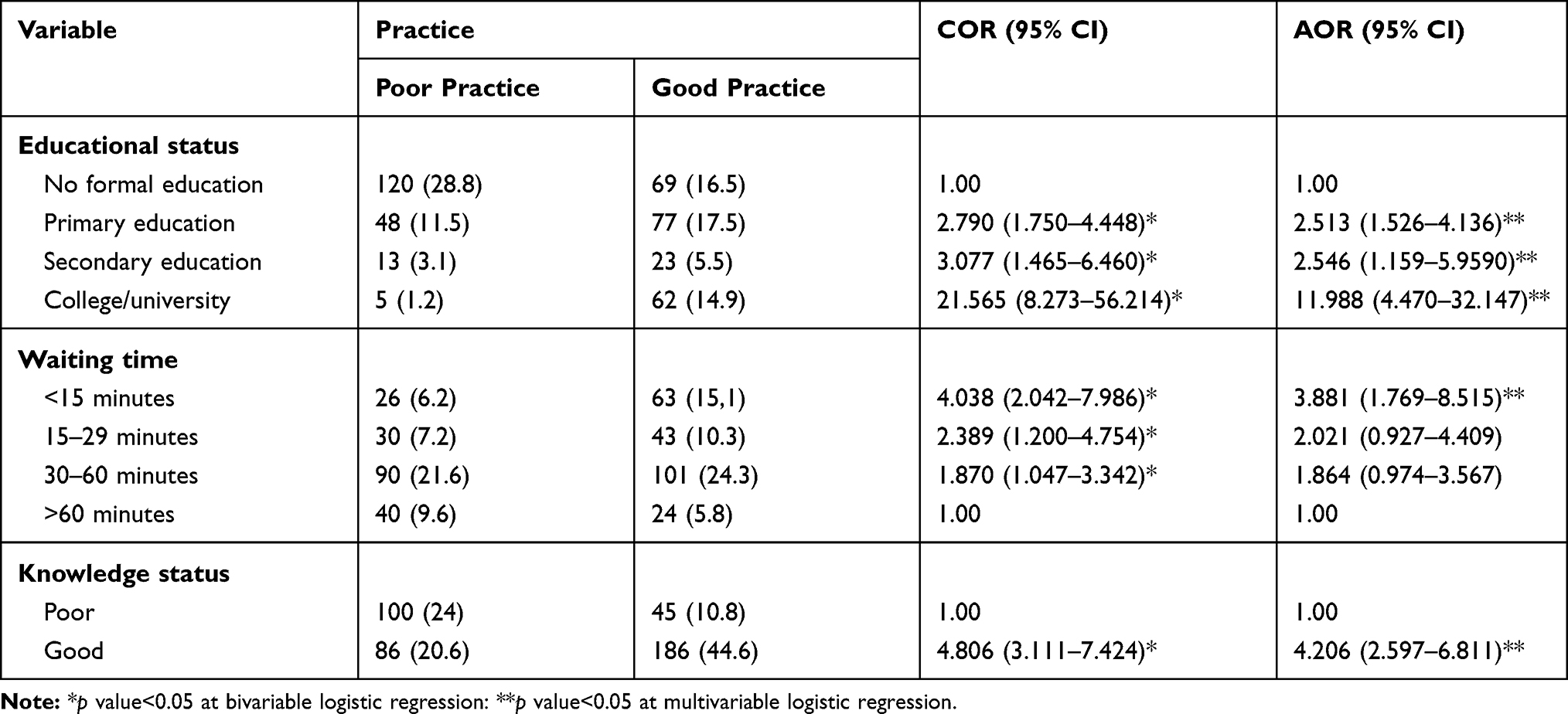 |
Table 8 Factors Associated with Respondent Parents’ Practice Regarding Immunization of Infants in Wadla Woreda, North East Ethiopia, 2019 (n=418) |
Discussion
In this study, 336 (80.4%) of mothers have heard information about infant immunization and 241 (57.7%) of them have access to information from health workers followed by 189 (45.2%) radio and 103 (24.6%) television. This is similar to a study carried out in Addis Ababa,23 Nigeria,24 Saudi Arabia,25,26 Pakistan,27 India,28–31 Nepal,32 Afghanistan,33 Lithuania,34 and Georgia,35 and health care workers were the major source of information. This might be due to nowadays most of the parents got delivery service at a health facility with skilled birth attendants and health care worker plays an indispensable role, during ANC and PNC period by convincing parents to link the newborn baby to Immunization unit to acquire immunization service as well as the intimate relationship between a service provider and the parents at primary health care levels and these health facilities seem to be most readily available and accessible to the people. This is, however, contrary to studies carried out in Minia city, Egypt,36 Libya,37 and Nigeria,38,39 television, paramedical workers, and antenatal clinics were the main source of information about infant immunization, respectively.
This study showed that 65.1% of the parents at 95% CI (60.8–69.4%) had good knowledge about infant vaccination which is higher than in study carried out in Addis Ababa (55%),40 Egypt (31.2%),41 Alma Dinah, Saudi Arabia (50.5%),26 south India (50.43%),29 Kerala, India (39.5%)42 and Lithuania (36.3%).34 But it is low compared with studies conducted in Minia city, Egypt 89.2%,36 Nigeria, Lagos state (72%).39 Edo State, Nigeria (87%)43 Jos North, Nigeria, 89.6%,44 Saudi Arabia (87.2%),45 Nepal (72.7%)32 and India (72.7%).46,47 The inconsistency may be due to differences in socio-demographic characteristics, sample size, study setting, and/or educational backgrounds of the participants.
Our study showed that Literate parents who attend higher education were about five times (AOR=5.330, 95% CI: (1.919–14.803)) more likely to be knowledgeable than illiterate respondents. This finding is comparable with the study findings from Addis Ababa,40 Minia City, Egypt,36 Nigeria,39,44 Saudi Arabia,17,18,25 Nepal,32 India,28,47,48 Lebanon49 and Lithuania.34 This was due to higher educational levels, of no doubt, have a good understanding of children’s health and understand the educational messages and vaccination policy much more easily. Moreover, being more educated allows better communication with health care providers and fewer chances of acquiring wrong beliefs regarding vaccines.
This study revealed that Parents who reside in an urban area were about two folds (AOR=2.788, 95% CI: (1.617–4.807) more likely to be knowledgeable than regular residents. This finding is congruent with the study conducted in Minia city, Egypt,36 Jos North, Nigeria,44 Saudi Arabia,17,18 Malaysia,50 and India.28 This may probably be attributed to the fact that parents living in urban were more likely to be educated which may increase their knowledge towards the advantages of infant immunization uptake compared to a parent living in the rural side or maybe due to variation in the provided health services in terms of availability and accessibility of immunization service. Since the people resident of the urban area has good availability and easy to get access to all the healthcare facilities and social media which makes them advantageous over people living in urban areas.
This study also investigated that Parents who had a favorable attitude towards infant vaccination were four times (AOR=4.308, 95% CI: (2.609–7.111) knowledgeable than their counterparts. This finding is in line with the study finding from Saudi Arabia25,26 and Bangalore, India.46 This might be due to peoples were more interested to have information about the vaccine and VPDs from health care professionals, social media, friends, and neighbors to improve their awareness which in turn change parents’ perception of the importance of immunization in the care of their infant.
Our study indicated that parents who got immunization service two-three times and four-five times were three times (AOR=3.227, 95% CI: (1.543–6.748) and two times (AOR=2.254, 95% CI: (1.029–4.938) more likely to be knowledgeable respectively than parents who get the service at one occasion. This might be attributed to the health education received by parents towards the advantage of timely infant immunization uptake during their frequent visit and the content for the health education provided to the parents focus more on emphasizing the benefits of infant immunization uptake and its compliance, immunization schedule, and how to manage its side effects also continuous educational programs for parents about the types and availability of other vaccines.
This study also revealed that 241 (58%) of the parents at 95% CI (52.6%-62.4%) had a favorable attitude towards infant vaccination which is in line with the study conducted in Addis Ababa (53.8%)40 and Alma Dinah, Saudi Arabia (56.4%).26 But lower than the study carried out in Egypt (70%),41 Libya (80.5%),37 Jos North, Nigeria, (97%),44 (100%),39 Edo State, Nigeria (99.1%),43 Saudi Arabia (80%),25 India (64.33%),29 (85.4%),46 (90%),47 Lithuania (83.2),34 and Georgia (97%).35 The inconsistency may be due to differences in socio-demographic characteristics, and/or educational backgrounds of the participants.
In this study, Literate respondents who attend primary school and secondary schools were 55% [AOR=0.451, 95% CI: (0.205–0.994) and 68% [AOR=0.320, 95% CI: (0.112–0.916) less likely to had a favorable attitude towards infant immunization than parents who attend higher education respectively. The results of the current study are supported by the study in Addis Ababa,40 Saudi Arabia,18,51 India,47 Malaysia,52 Europe53, and America.54 The reason behind this association might be that educated parents may have more opportunities to understand vaccination and its benefit than illiterate parents and this may create a favorable attitude towards infant immunization than illiterates. Besides this education level has an impact on parents’ beliefs and their attitude and the higher the education level, the higher is the acceptance level among the parents and the more positive their attitude in acceptance of vaccination.
Our study showed that respondents who had good knowledge about infant immunization were four folds (AOR= 4.592, 95% CI: (2.709–7.786) more likely to had a favorable attitude towards infant immunization than their counterparts. This is in line with studies conducted in Saudi Arabia,25,26 Bangalore, India,46 Lebanon,49 Lithuania,34 and Italy.55 This might be due to good knowledge was the most crucial and tangible factor that helps to attain a favorable attitude towards infant immunization and mothers who had better knowledge and understanding about EPI were more likely to adhere and less likely to refuse their infant’s immunization.
Our finding also revealed that Parents who were mothers of the child were three times [AOR=3.813, 95% CI: (1.185–12.266) more likely to had a favorable attitude towards infant immunization than their counterparts. This is in line with the study done in Taif, Saudi Arabia18, and Malaysia.52
This might be due to mostly mothers are responsible to bring their children to immunization visits and the degree of intimacy with health care workers may be responsible for the observed difference in mothers’ attitudes compared to fathers’ attitudes. In addition to this as most mothers are the primary caretakers, and the ultimate decision-makers about immunization.
The finding indicated that 231 (55.3%) of the parents at 95% CI: (50.4–60.4%) had good practice towards infant vaccination, which is lower than studies done in Addis Ababa (84%),40 Libya (81%),37 Edo State (Nigeria) (69.7%),43 Jos North (Nigeria) (76.6%),44 (86.4%),39 Saudi Arabia (77.7%),25 Al Madinah (Saudi Arabia) (92.8%),26 and India (90.20%),29 and rural areas (68.2%).46 The inconsistency may be due to variation in socio-demographic characteristics, low levels of awareness, and unfavorable attitude towards immunization, and immunization is not mandatory and is not needed for school registration in our setup made immunization practice poor.
Our study indicated that literate parents who attend primary school, secondary school, and higher education were about two times (AOR=2.513, 95% CI: (1.526–4.136), two times (AOR=2.546, 95% CI: (1.159–5.9590) and twelve times (AOR=11.988, 95% CI: (4.470–32.147), respectively, more likely to practice infant immunization than illiterate respondents. A similar result between the mother’s educational level and vaccination status was observed in other studies as well in Arba Minch town and Zuria District,10 Mizan Aman Town (Ethiopia),56 Sinan District,57 Tehulederie district,58 Taif (Saudi Arabia),18 Kama District (Afghanistan),33 Nepal,32 Bengaluru (India),48 urban slums of Varanasi (India),59 Lebanon,49 and Georgia.35 This might be related to the improvement of maternal educational status which enhances parental health-seeking behavior and it had a positive influence on infant immunization uptake. Moreover, this might be due to recent advancements in parental education such as changes in attitudes, customs, and beliefs, increased autonomy, and control over household resources, which promote healthcare-seeking behavior.
This study also found that parents who had good knowledge of infant immunization were four folds (AOR= 4.206, 95% CI: (2.597–6.811) more likely to practice than their counterparts. The result is in line with Arba Minch town and Zuria District,10 Mizan Aman Town (Ethiopia),56 Sinana District,57 Edo State (Nigeria),43 and Malaysia.50 This might be due to better knowledge of VPDs and the significance of immunization can alter parents’ health-seeking behavior which helps to promote immunization practice. In addition to this, as the knowledge of mothers improved on immunization, they could also develop a favorable attitude too. Then, they were encouraged to complete the immunization as well as the more knowledge they acquired, the more capable of increasing their practice, the more confidence towards infant immunization uptake.
Our finding also showed that shorter service waiting time to receive immunization service was another significant predictor for the parental practice of infant vaccination. The result is comparable with the study finding from Tehulederie district, Ethiopia,58 since long waiting times at health institutions were the main reasons mentioned for not fully immunizing their children in several studies conducted across the globe.
As a strength, since there were limited data related to parents knowledge, attitude, and practice towards infant immunization and associated factors nationally, this study might be a supplementary issue for those stakeholders who want to undertake any further intervention. Being community-based study and utilization of a valid and standardized instrument for assessing parents KAP towards infant immunization could also be another strength of the current study. This study cannot show cause-and-effect relationship since it is a cross-sectional type, it does not include children aged 12–23 months, which helps to measure immunization completion rate and overall immunization coverage could be listed as a potential limitation of the study.
Conclusion
In this study, parental knowledge, attitude, and practice towards infant immunization were found to be lower than most of the study findings quoted in this study.
The finding also revealed that educational status, residence, parental attitude, and frequency of visits were found to be statistically significant predictors of parental knowledge. Parental knowledge status, educational status, and r/n ship of parents to the infant showed a statistically significant association with the attitude of parents. Waiting time, educational status, and knowledge status of parents was also a statistically significant association with immunization practice.
According to this study, massive public health education must be intensified through the provision of Information, Education, and Communication materials to enhance the knowledge, attitude, and practice of parents about immunization and vaccine-preventable diseases.
It is also recommended to improve the accessibility of general care provided at the units, especially the service waiting time. The role of media in the form of advertisements on radio and television should take the lion’s share to encourage people for immunization activities.
Abbreviations
AOR, adjusted odds ratio; BCG, Bacillus Calmette Guérin; CI, confidence interval; COR, crude odds ratio; DPT, diphtheria, pertussis, and tetanus; EDHS, Ethiopian Demographic and Health Survey; EMDHS, Ethiopian Mini Demographic and Health Survey; EPI, expanded program on immunization; GAVI, Global Alliance for Vaccine and Immunization; Hib, Haemophilus influenza type B; IEC, information, education, and communication; IPV, inactivated polio vaccine; IQR, interquartile range; IRB, Institutional Review Board; KAP, knowledge attitude and practice; NGO, non-governmental organization; OPV, oral polio vaccine; PCV, pneumococcus vaccine; SNNP, South Nation Nationality and People; SPSS, Statistical Product and Service Solution; UNICEF, United Nations Children Fund; VPDs, vaccine-preventable diseases; WHO, World Health Organization.
Data Sharing Statement
All data will be shared upon request from the corresponding author.
Ethics Approval and Consent to Participate
Before conducting the study, the proposal was presented, defended and a letter of ethical clearance was obtained from the school of nursing ethical review committee on behalf of the University of Gondar. The purpose of the study was explained to the study participants; privacy and confidentiality were ensured. Before data collection, informed verbal consent was obtained from the study participants. The respondents’ right to refuse or withdraw from participating in the study was fully acknowledged.
Consent for Publication
The study does not include images or videos relating to an individual. But concerning other collected and used data in this study, while obtaining consent from each participant, information related to publishing the study finding was addressed and participants were agreed on that.
Acknowledgments
First and foremost we would like to thank Wolkite University for funding this research project. Secondly, our heartfelt gratitude goes to the wadla district health office administration staff and health care workers for their valuable supports while collecting the data. Our thanks also go to data collectors and supervisors for their endeavors.
Author Contributions
FA, TT, BT, BZ, MS, OT AA, DG, and ES: All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted, and agree to be accountable for all aspects of the work.
Funding
Funding for this research project was gained from Wolkite University.
Disclosure
The authors declare that they have no financial or non-financial competing interests.
References
1. Mahalingam S, Soori A, Ram P, Achappa B, Chowta M, Madi D. Knowledge, attitude and perceptions of mothers with children under five years of age about vaccination in Mangalore, India. Asian J Med Sci. 2014;5(4):52–57. doi:10.3126/ajms.v5i4.10306
2. Yu H, Luo S, Lou L, Zhang B, Li Q. Knowledge, attitude and practice on immunization among migrant mothers: a questionnaire development and field application. Int J Vaccine Immunization. 2016;2(1). doi:10.16966/2470-9948.106
3. World Health Organization. Global routine vaccination coverage; 2013.
4. Casey RM, Dumolard L, Danovaro-Holliday MC, et al. Global routine vaccination coverage, 2015. Morbidity and Mortality Weekly Report. 2016;65(45):1270–1273.
5. Yenit MK, Assegid S, Abrha H. Factors associated with incomplete childhood vaccination among children 12–23 months of age in Machakel Woreda, East Gojjam Zone: a case-control Study. J Pregnancy and Child Health. 2015;2(4). doi:10.4172/2376-127X.1000180
6. Berhane Y. Universal childhood immunization: a realistic yet not achieved goal. Ethiop J Health Dev. 2008;22(2):146–147.
7. World Health Organization. Progress towards measles control in WHO’s African region, 2001–2008. Wkly Epidemiol Rec. 2009;39(84):397–404.
8. Sharma S, Kohli C, Sharma N, Mehra D. Incomplete immunization coverage in Delhi: reasons and Solutions. Prim Health Care. 2016;6(4). doi:10.4172/2167-1079.1000240
9. Health FMo. Ethiopia national expanded program on immunization comprehensive multi-year plan 2016–2020; April 2015.
10. Animaw W, Taye W, Merdekios B, Tilahun M, Ayele G. Expanded program of immunization coverage and associated factors among children age 12–23 months in Arba Minch town and Zuria District, Southern Ethiopia, 2013. BMC Public Health. 2014;14(1):464. doi:10.1186/1471-2458-14-464
11. World Health Organization. Control CfD prevention, “Epidemiology of the unimmunized child: findings from the peer-reviewed published literature, 1999–2009”; 2009.
12. Ebrahim T, Salgedo W. Childhood immunization coverage in tehulederie district, northeast of Ethiopia: a Community-Based Cross-Sectional Study. Int J Curr Res. 2015;7(09):20234–20240.
13. Gualu T, Dilie A. Vaccination coverage and associated factors among children aged 12–23 months in Debre Markos Town, Amhara Regional State, Ethiopia Hindawi. Adv Public Health. 2017;2017(6). doi:10.1155/2017/5352847
14. World Health Organization. Global vaccine action plan 2011–2020. Geneva, Switzerland: WHO; 2013. Available from: http://www.who.int/immunization/global_vaccine_action_plan/en/.
15. Directorate Mach, Health FMo. National strategy for newborn and child survival in Ethiopia, 2015/16 – 2029/20; June 2015.
16. EPHIEE, ICF. Ethiopia Mini Demographic and Health Survey 2019: Key Indicators. USA: EPHI and ICF; 2019.
17. Alagsam EH, Alshehri AA. Knowledge, attitude, and practice of parents on childhood immunization schedule in Saudi Arabia. IJMDC. 2019;3(5):457–461. doi:10.24911/IJMDC.51-1547400699
18. Yousif MA, Albarraq AA, Abdallah MAA, Ai E. Parents′ knowledge and attitudes on childhood immunization, Taif, Saudi Arabia. J Vaccines Vaccin. 2013;5:215.
19. Mphaka MR, Moshime M, Reddy C. A cross-sectional study on caregivers’ knowledge, attitudes, and practices about the routine immunisation program in Tshwane Sub-District 2, Gauteng, South Africa. J Environ Sci Public Health. 2018;2(04):221–231. doi:10.26502/jesph.96120041
20. Awadh AI, Hassali MA, Al-Lela OQ, Siti Halimah Bux SH, Elkalmi RM, Hadi H. Immunization knowledge and practice among Malaysian parents: a questionnaire development and pilot-testing. BMC Public Health. 2014;14(1):1107. doi:10.1186/1471-2458-14-1107
21. Adhikari P, Dhungel S, Shrestha R, S Khanal. Knowledge attitude and practice (KAP) study regarding facts for life. Nepal Med Coll J. 2006;8(2):93.
22. Zekaria S. Summary and statistical report of the 2007 population and housing census (Doctoral dissertation, United Nations Population Fund (UNFPA)). Available from: http://196.189.45.87/handle/123456789/88805.
23. Birhanu S, Anteneh A, Kibie Y, Jejaw A. Knowledge, attitude and practice of mothers towards immunization of infants in health centres at Addis Ababa, Ethiopia. Am J Health Res. 2015;4(1):6–17. doi:10.11648/j.ajhr.20160401.12
24. Awosan KJ, Ibrahim MTO, Yunusa EU, Isah BA, Raji MO, Abubakar N Abubakar. N. Knowledge, attitude and compliance with full immunization of children against vaccine-preventable diseases among pregnant mothers in Sokoto, Nigeria. Int J Contemp Med Res. 2018;5(6):F10–F6.
25. Majmaah JZ. Kap of parents towards childhood vaccination. J Health Sci. 2013;1(1).
26. Lharbi KM. A parents’ knowledge, attitude and practice towards childhood vaccination, Al Madinah, Saudi Arabia. Neonat Pediatr Med. 2017;3:126.
27. Qidwai W, Ali SS, Ayub S, Ayub S. Knowledge, attitude and practice regarding immunization among family practice patients. JDUHS. 2007;1(1):15–19.
28. Mugada V, Chandrabhotla S, Kaja DS, SG Machara. Knowledge towards childhood immunization among mothers & reasons for incomplete immunization. J App Pharm Sci. 2017;7(10):157–161.
29. Sankar BK, Rameh S, Sunny A. A study to assess and correlate the knowledge, attitude, and practices of vaccination among mothers with educational status in a teaching hospital in South India.. Prim Health Care. 2018;8(01):290. doi:10.4172/2167-1079.1000290
30. Hedaoo SS, Deshpande SR, Badge VL. Determinants of awareness regarding immunization among parents of children residing in an urban slum of a metro city.. Int J Community Med Public Health. 2018;5(9):4037–4042. doi:10.18203/2394-6040.ijcmph20183592
31. Patil R, Maheshwari M, Patel B. Knowledge and awareness of parents about universal immunization program and optional vaccines: a cross-sectional study in Central India. Indian J Basic Med Res. 2018;7(2):585–593.
32. Devkota S, Simkhada P, vanTeijlingen E, Rai LD. Parents’ knowledge and practices to childhood immunisation in Nepal: implications for health policy. Health Sci J. 2013;7(4).
33. Sherzai DMI Routine vaccination coverage and related factors among children aged 12–23 months in one rural area of Nangarhar province-Afghanistan, Hacettepe University; 2014.
34. Šeškute M, Tamuleviˇciene E, Levine G. Knowledge, and attitudes of postpartum mothers towards immunization of their children in a Lithuanian Tertiary Teaching Hospital. Medicine. 2018;54(2). doi:10.3390/medicina54010002
35. Verulava T, Jaiani M, Lordkipanidze A, Jorbenadze R, Dangadze B. Mothers’ knowledge and attitudes towards child immunization in Georgia. Open Public Health J. 2020;13:1874–9445.
36. Ahmed SM, Rahman TAA-E, Masoed ES. Mothers’ awareness and knowledge of under five years children regarding immunization in Minia city Egypt. Life Sci J. 2013;10(4):1224–1232.
37. Bofarraj MAM. Knowledge, attitude and practices of mothers regarding immunization of infants and preschool children at Al-Beida City, Libya. J Pediatr Allergy Immunol. 2011;9(1):29–34.
38. Adeyinka DA, Oladimeji O, Adeyinka FE, Aimakhu C. Uptake of childhood immunization among mothers of under‑five in South-Western Nigeria.. Internet J Epidemiol. 2009;7(1–5).
39. Adefolalu OA, Kanma‑Okafor OJ, Balogun M. Maternal knowledge, attitude, and compliance regarding immunization of under-five children in primary health care centers in Ikorodu Local Government Area, Lagos State. J Clin Sci. 2019;16(1):7–14. doi:10.4103/jcls.jcls_55_18
40. Birhanu S, Anteneh A, Kibie Y, Jejaw A. Knowledge, attitude and practice of mothers towards immunization of infants in health centres at Addis Ababa, Ethiopia. Am J Health Res. 2016;4(1):6–17.
41. Ramadan HA, Soliman SM, El-kader RGA. Knowledge, attitude and practice of mothers toward children’s obligatory vaccination. IOSR-JNHS. 2016;5(4):22–28. doi:10.9790/1959-0504022228
42. Aslami AN, Athira TK, Salim AK, et al. Assessment of knowledge about immunization of under five children among mothers attending outpatient department of pediatrics in a tertiary care hospital in Kollam, Kerala. Int J Evid Based Healthc. 2015;2(29):4191–4200. doi:10.18410/jebmh/2015/595
43. Odusanya OO, Alufohai EF, Meurice FP, Ahonkhai VI. Determinants of vaccination coverage in rural Nigeria. BMC Public Health. 2008;8(1):381. doi:10.1186/1471-2458-8-381
44. Chris-Otubor GO, Dangiwa DA, Ior LD, Anukam NC. Assessment of knowledge, attitudes, and practices of mothers in Jos North regarding immunization.. IOSR J Pharm. 2015;5(6):34–45.
45. Habib RF, Alsubhi RA, Saadawi DW, Hatim R, Saleh A, Alrashidi AA. Assessment of knowledge, attitude, and practice of parents towards immunization of children in Saudi Arabia, 2018. Egypt J Hosp Med. 2018;71(2):2585–2589. doi:10.12816/0045660
46. Trushitkumar BP, Pathak R, Singh R, Alves V, Mahesh NM, Chaluvaraj TS. Assessment of parents’ knowledge, attitude and practice about child vaccination in rural areas. J Pharm Res. 2017;16(3):235.
47. Kumar PRT, Kavinprasad M. A study to assess the parent’s knowledge and attitudes on childhood immunization. Int J Community Med Public Health. 2018;5(11):4845–4848. doi:10.18203/2394-6040.ijcmph20184582
48. Joseph J, Devarashetty V, Reddy SN. Parents’ knowledge, attitude and practice on childhood immunization. Int J Basic Clin Pharmacol. 2015;4:1201–1207. doi:10.18203/2319-2003.ijbcp20151359
49. Matta P, Mouallem RE, Akel M, Hallit S, Khalife M-CF. Parents’ knowledge, attitude and practice towards children’s vaccination in Lebanon: role of the parent-physician communication. BMC Public Health. 2020;20(1):1439. doi:10.1186/s12889-020-09526-3
50. Awadh AI, Hassali MA, Al-Lela OQ, et al. Immunization knowledge and practice among Malaysian parents: a questionnaire development and pilot-testing. BMC Public Health. 2014;14(1):1107.
51. Alagsam EH, Alshehri AA, Alagsam EH, et al. Knowledge, attitude, and practice of parents on childhood immunization schedule in Saudi Arabia. IJMDC. 2019;3(5):457–461.
52. Aziz S, Iqbal MZ, Iqbal MS, et al. Attitude towards vaccination: a cross-sectional study among the parents in Sungai Petani, Kedah, Malaysia. Int J Pharm Sci Res. 2019;10(5):2465–2472.
53. Stefanoff P, Mamelund SE, Robinson M, et al. Working group on the standardization of attitudinal studies in Europe. Tracking parental attitudes on vaccination across European countries: the vaccine safety, attitudes, training, and communication project (VACSATC). Vaccine. 2010;28(35):5731–5737.
54. Prislin R, Dyer JA, Blakely CH, Johnson CD. Immunization status and sociodemographic characteristics: the mediating role of beliefs, attitudes, and perceived control. Am J Public Health. 1998;88(12):1821–1826. doi:10.2105/AJPH.88.12.1821
55. Rosso A, Massimi A, Vito CD, et al. Knowledge and attitudes on pediatric vaccinations and intention to vaccinate in a sample of pregnant women from the City of Rome. Vaccine. 2019;37(14):1954–1963. doi:10.1016/j.vaccine.2019.02.049
56. Meleko A, Geremew M, Birhanu F. Assessment of Child immunization coverage and associated factors with full vaccination among children aged 12–23 months at Mizan Aman Town, Bench Maji Zone, Southwest Ethiopia Hindawi. Int J Pediatr. 2017;2017:11. doi:10.1155/2017/7976587
57. Legesse E, Dechasa W. An assessment of child immunization coverage and its determinants in Sinana District, Southeast Ethiopia. BMC Pediatr. 2015;15(1). doi:10.1186/s12887-015-0345-4
58. Ebrahim TY, Salgedo WB. Childhood immunization coverage in Tehulederie district, Northeast of Ethiopia: a community-based cross-sectional study. Int J Curr Res. 2015;7(9):20234–20240.
59. Awasthi A, Pandey CM, Singh U, Kumar S. Maternal determinants of the immunization status of children aged 12–23 months in urban slums of Varanasi, India. Clin Epidemiol Glob Health. 2015;3:10–1 6.
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.