Back to Journals » Drug, Healthcare and Patient Safety » Volume 17
Knowledge, Attitude, and Practice Towards Responsible Self-Medication Among Pharmacy Students: A Web-Based Cross-Sectional Survey in Uganda
Authors Brian B, Goruntla N, Bommireddy BR ![]() , Mopuri BM
, Mopuri BM ![]() , Easwaran V
, Easwaran V ![]() , Mantargi MJS
, Mantargi MJS ![]() , Thammisetty DP
, Thammisetty DP ![]() , Bukke SPN
, Bukke SPN ![]() , Yadesa TM, Ayogu EE
, Yadesa TM, Ayogu EE ![]()
Received 3 October 2024
Accepted for publication 20 December 2024
Published 7 January 2025 Volume 2025:17 Pages 7—23
DOI https://doi.org/10.2147/DHPS.S496924
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Professor Siew Siang Chua
Bukoli Brian,1 Narayana Goruntla,1 Bhavana Reddy Bommireddy,2 Bhavani M Mopuri,2 Vigneshwaran Easwaran,3 Mohammad Jaffar Sadiq Mantargi,4 Durga Prasad Thammisetty,5 Sarad Pawar Naik Bukke,6 Tadele Mekuriya Yadesa,1 Ebere Emilia Ayogu7
1Department of Clinical Pharmacy and Pharmacy Practice, School of Pharmacy, Kampala International University, Western Campus, Ishaka, Uganda; 2Research Scholar, Department of Pharmacy Practice, Raghavendra Institute of Pharmaceutical Education and Research (RIPER) – Autonomous, Anantapur, AP, India; 3Department of Clinical Pharmacy, College of Pharmacy, King Khalid University, Abha, Kingdom of Saudi Arabia; 4Department of Pharmacology, Pharmacy Program, Batterjee Medical College, Jeddah, Saudi Arabia; 5Department of Pharmacy Practice, Sri Padmavathi School of Pharmacy, Tiruchanoor, Tirupathi, AP, India; 6Department of Pharmaceutics and Pharmaceutical Technology, School of Pharmacy, Kampala International University, Western Campus, Ishaka, Uganda; 7Department of Clinical Pharmacy and Pharmacy Management, Faculty of Pharmaceutical Sciences, University of Nigeria, Nsukka, Nigeria
Correspondence: Narayana Goruntla; Bukoli Brian, Department of Clinical Pharmacy and Pharmacy Practice, School of Pharmacy, Kampala International University, Western Campus, Ishaka, Uganda, Tel +256760060453, Email [email protected]; [email protected]; [email protected]
Purpose: Rational self-medication (SM) practice among healthcare students is essential to promote the safe, effective, and economical use of medicines for self-diagnosed conditions. The study aimed to assess pharmacy students’ knowledge, attitude, and practice about responsible self-medication.
Methodology: A cross-sectional online survey was conducted among Ugandan pharmacy students for one month from March 1 to March 31, 2024. The study included students enrolled in diploma, bachelor, and master of pharmacy programs in Uganda. Informed consent was obtained online by asking a question regarding willingness to participate. A non-probable snowball sampling technique was used to recruit students. A pre-validated questionnaire was used to obtain socio-demographics, self-medication practices, knowledge, attitudes, and practices about responsible self-medication. We used binary and multivariable logistic regression analysis to identify the factors associated with KAP regarding responsible self-medication.
Results: The prevalence of self-medication practice among pharmacy students was 96.73%. The self-medication is most common in headache (78.97%), cold, and cough (79.91%) illnesses. Painkillers (90.19%) and antibiotics (53.97%) are the most common medicines used for self-medication. Most pharmacy students have good knowledge (87.38%) and a positive attitude (96.03%) toward responsible self-medication. However, only 27.34% of students practice rational self-medication. Participants’ university and parents’ professions were significantly associated with good knowledge of responsible self-medication. Whereas factors such as gender, residence, and type of illness were significantly associated with rational self-medication practice.
Conclusion: The prevalence of self-medication was high among pharmacy students in Uganda. Painkillers and antibiotics are the most preferred drugs for self-medication. About 87.38% of pharmacy students have good knowledge, and 96.03% have a positive attitude toward responsible self-medication. Rational self-medication practice was low among students. We recommended training sessions to enhance safe self-medication practices among pharmacy students.
Keywords: attitude, knowledge, pharmacy students, practices, self-medication, Uganda
Introduction
According to the World Health Organization (WHO), the consumption of medicines to treat self-diagnosed diseases or symptoms or the reuse of prescribed medicines for recurrent disease conditions is called self-medication (SM).1 It involves using over-the-counter (OTC) medicines, prescription-only medicines, and complementary and alternative medicines (CAM).2 Different forms of SM practices include taking medicines without a prescription, using a previous prescription for a similar illness, using medicines available at home without a doctor’s advice, and sharing medicines with relatives or friends having similar conditions.3
Globally, SM practice is a major public health concern that was triggered by cultural, economic, and political factors.4 SM is one of the more common practices observed in developing countries (12.7% to 95%) than in developed countries (3%).5 The wide difference in SM practices between developed and developing nations is due to variations in cultural and socioeconomic factors, as well as differences in healthcare systems, including compensation rules, healthcare accessibility, and medicine dispensing policies.6,7 In low- and middle-income countries (LMICs), most of the illnesses are treated by SM, which increases the burden of irrational drug use.8 Nowadays, SM is becoming an unavoidable option to reduce the healthcare costs associated with the majority of illnesses in developing nations.7 Evidence shows that the most common reasons for raising SM practice include lack of time to visit a doctor, inexpensiveness of practice, easy accessibility of drugs, mild symptoms, having previous prescriptions for the same illness, suggestions from peers or friends, and knowledge about the use of medicines.7–10
SM cannot be considered a completely safe practice, and it may cause many problems, such as wastage of resources, antibiotic resistance, drug interactions, adverse drug reactions, polypharmacy, the wrong diagnosis, prolonged use of medicine, and prolonged suffering.3,7,9 Though SM is not considered safe, responsible SM has several advantages, such as saving time and money, avoiding unnecessary consultations, saving patients’ lives in certain acute conditions, saving scarce medical resources from being wasted on minor conditions, and active involvement of the patient for his/her health.11
The previous studies’ findings indicate that the most common symptoms and illnesses for self-medication practices are headache, abdominal pain, cold, cough, fever, sore throat, cramps, and diseases such as respiratory infections, urinary tract infections, eye infections, malaria, and gastrointestinal disorders.10,12,13
Several studies have been published worldwide investigating the prevalence of SM practices. The prevalence of SM practices varied in different countries, in Bangladesh (88%), Jordan (86.7%), Egypt (52.7%), Ethiopia (72.2%), India (71%), Spain (12.7%), Chile (75%), Iran (76%), China (47.9%), and Vietnam (83.3%).12–17 Studies conducted among pharmacy and medical students in various countries show a diverse range of self-medication practices, ie, Bangladesh (88.0), Jordan (86.7%), Saudi Arabia (63.9%), Ghana (55.2%), Turkey (79.0%), Iran (57.1%), Serbia (81.3%), and Kabul (38.0%).3,18–24 The prevalence of SM among university students in Mbarara (63.5%), Lira (74.2%), and Busitema (93.8%) was found to be very high in Uganda.25–27 The participants in these studies were either university-enrolled or medical students. It demonstrates an evidence gap in self-medication practice among Ugandan pharmacy students.
Pharmacy students differ from other non-healthcare university students in terms of exposure to knowledge about medicines and diseases, which enables them to practice SM. Therefore, it is essential to assess pharmacy students’ knowledge, attitude, and practices (KAPs) regarding safe SM practice. Upon graduation, pharmacy students who become practicing pharmacists can offer patients suitable guidance about responsible SM. The current study addresses the gaps among pharmacy students about KAP toward responsible SM. As a result, the study can be used to develop and implement educational interventions to improve responsible SM practice among pharmacy students directly and patients indirectly in the coming years through practicing pharmacists. To the best of our knowledge, no study was conducted to assess the knowledge, attitude, and practice (KAP) toward self-medication (SM) among pharmacy students in Uganda. The study aimed to assess the KAP towards self-medication among pharmacy students and to examine the predictors of responsible SM in terms of KAP.
Materials and Methods
Study Design and Ethical Considerations
A cross-sectional online survey was conducted among Ugandan pharmacy students for one month from March 1 to March 31, 2024. The Kampala International University School of Pharmacy Research Committee (KIU SPRC/004/24) approved the research protocol, questionnaire, and informed consent procedure. This online study followed the ethical principles outlined in the Declaration of Helsinki for research involving human participants.
Study Participants
The study included students enrolled in diploma, bachelor’s, and master’s pharmacy programs at three Ugandan universities: Kampala International University (KIU), Mbarara University of Science and Technology (MUST), and Makerere University (MU). Before initiating the online survey, we sought permission from the deans or heads of the pharmacy schools or departments in the respective universities. Informed consent was obtained online. Before taking the survey, students must read the study background and objectives on the first page and select “yes” to the first two questions in the online form: 1. Are you a pharmacy student? 2. Are you willing to participate in this online self-medication survey among pharmacy students?
Sample Size and Sampling Technique
The number of pharmacy students to participate in this online survey was determined using a single-population proportion formula. It was assumed that 50% of students practice responsible self-medication, with a margin of error of 5%, a design effect of 1%, and a power of 80%. The calculated number of students required for the survey was 384. After considering a non-response rate of 5%, the total sample size was calculated to be 403. A non-probability snowball sampling method was employed to recruit pharmacy students, whereby invited participants were requested to disseminate the invitation to their familiar contacts. Although this sampling technique has limitations in terms of generalizing the findings, it can capture the maximum sample size as required by the study.
Questionnaire
The questionnaire consists of five sections: 1) Socio-demographics of pharmacy students; 2) Knowledge of responsible self-medication; 3) Attitude toward responsible self-medication; 4) Practice of responsible self-medication; and 5) Self-medication practices among pharmacy students.
Socio-Demographics of the Pharmacy Students
The socio-demographic characteristics, such as age, gender, pharmacy division, name of the educational institute/university, location, marital status, type of accommodation, parent’s profession, presence of any medical illness, and monthly household income, were included in this section.
Knowledge of Responsible Self-medication
The knowledge regarding responsible self-medication among pharmacy students was assessed by using seven questions: one regarding SM definition (K1), four regarding the safety of SM (K2-K5), one regarding the interference of SM with other medications prescribed by the doctor (K6), and one on how SM can mask the symptoms of other disease conditions (K7). These questions had two options (True/False or Yes/No) for answers. A correct response received one point, whereas an incorrect answer received zero points. Everyone’s total points ranged from 0 to 7. After assessment of the knowledge points, Bloom’s cut-off criteria were used to categorize knowledge levels into good (80–100% correct response; score 6–7), moderate (60–79% correct response; score 4–5), and poor (<60% correct response; score <4) knowledge toward responsible self-medication.28
Attitude Toward Responsible Self-medication
Attitude toward responsible self-medication among pharmacy students was assessed by using 10 statements: one regarding SM as a component of self-care (A1), two regarding SM-induced ADRs and monitoring (A2 and A3), one regarding long-term use of SM (A4), one regarding use of OTC medicines (A5), one regarding training for SM (A6), one regarding SM advice in all age groups (A7), one regarding SM advice during pregnancy (A8), one regarding the role of professional advice in SM (A9), and one regarding the influence of access to information on SM (A10). Each statement was rated on a 5-point Likert scale, with positive and negative responses such as strongly agree 5, agree 4, neutral 3, disagree 2, and strongly disagree 1. Statements 5 and 6 were reversely scored. The maximum expected score for all statements was 50, with a minimum of 10. Students with scores above or equal to 25 were deemed positive, while those with scores <25 were deemed negative towards responsible self-medication practices.10
Practice of Responsible Self-Medication
Practice toward responsible self-medication among pharmacy students was assessed by using six questions: one about the practice of reading leaflets or package inserts before self-medication (P1); one about sharing medicines with others having similar symptoms (P2); one about self-medicating without professional advice (P3); one about self-medication practice for a long period without medical advice (P4); one about the practice of self-medication in all types of illnesses (P5); and one about having undergone responsible self-medication training (P6). These questions had two options (True/False or Yes/No) for answers. A correct response received one point, whereas an incorrect answer received zero points. Everyone’s total points ranged from 0 to 6. Students who scored 5 or more in the practice domain were considered to have responsible self-medication practice, and those who scored less than 5 were considered to have irrational self-medication practice.
Self-medication Practices Among Pharmacy Students
Under this section, questions were asked about the frequency of SM per annum, preferred medical system for SM, the specific medical problems for which SM is practiced, drugs used for SM, reasons for choosing SM, the sources of information relied upon for SM practice, and side effects encountered with SM.
Development and Validation Of Questionnaire
A suitably designed, self-administered English version KAP questionnaire on self-medication was developed based on the previous studies conducted on self-medication among pharmacy and healthcare students.3,10,18,29 Then the questionnaire was subjected to face validity and reliability assessment. Face validation was done by a panel of experts comprising; clinical pharmacist (1), community pharmacist (1), physician (1), clinical pharmacologist (1), and epidemiologist (1). A total of 30 questions (knowledge = 7; attitude = 10; practice = 6; self-medication details = 7) are present in the questionnaire. Expert judgment of the inclusion of each statement or question in the survey instrument was rated on a four-point Likert scale in the ranges of strongly agree (4), agree (3), disagree (2), and strongly disagree (1). Finally, scale-level content validity index (S-CVI) indicators such as S-CVI/average number and S-CVI/utility agreement were calculated for the questionnaire’s knowledge (0.86, 0.9), attitude (0.9, 1), practice domains (0.9, 1), and self-medication details (0.94, 0.9). The S-CVI indicators that are equal to or greater than 0.8 represent the minimum criteria for accepting the content included in the questionnaire. A pilot sample survey’s reliability test results showed acceptable internal consistency with Cronbach’s alpha coefficients of 0.78 for the knowledge domain, 0.8 for the perception domain, and 0.76 for the practice domain.
Data Collection
Data were collected online by sending pharmacy students a link to a Google Forms questionnaire. The online questionnaire was distributed via various messenger groups (WhatsApp, WeChat, and IMO) and social media networks (Twitter, Instagram, and LinkedIn). The first page of the form provided information about the survey’s background, core objectives, expected results, and time (5–10 minutes) taken to fill out the online form for the enrollment of participants. Of 1160 pharmacy students (KIU = 650, MUST = 235, and MU = 275), 497 pharmacy students participated in this online survey with a response rate of 42.8%. After removing 69 incomplete responses, the final analysis included 428 responses (KIU = 288, MUST = 59, and MU = 81).
Data Analysis
To analyze the data collected from the pharmacy students, IBM SPSS Statistics for Windows, version 22.0 (IBM Corp., Armonk, NY, USA) was used. Before commencing the analysis, the data underwent cleaning, sorting, and processing within an Excel spreadsheet. Descriptive statistics such as frequency, percentages, mean, and standard deviation were used to represent the socio-demographics, knowledge, attitudes, and practices toward responsible self-medication and the adequacy level of KAP toward self-medication.
We used a bivariate and then a multivariate logistic regression analysis to investigate the relationship between the independent variables (socio-demographics) and the dependent variable (good knowledge, positive attitude, rational practice toward responsible self-medication, and prevalence of self-medication). Furthermore, good knowledge, a positive attitude, and rational practice of responsible self-medication among pharmacy students were linked to self-medication practice. Variables with a P value ≤ 0.2 in bivariate analysis were subjected to multivariate logistic regression analysis to adjust for potential confounders associated with the dependent variable. A two-way p-value of <0.05 was considered statistically significant.
Results
A total of 497 pharmacy students participated in this online survey. After removing 69 incomplete responses, the final analysis included 428 responses. The mean age of the study participants was 24.8 ± 2.92. Most of the students were Christians (85.75%), not suffering from any type of medical illnesses (75.70%), and their parents were in non-medical professions (84.11%). The socio-demographic profile of the pharmacy students is represented in Table 1.
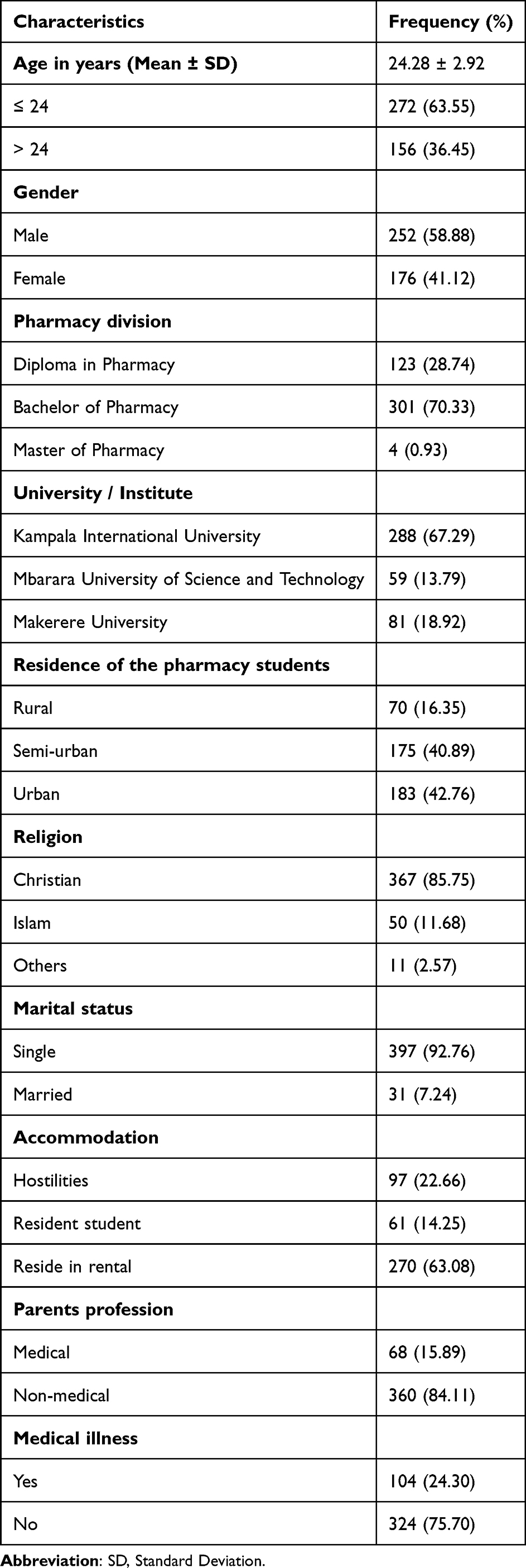 |
Table 1 Socio-Demographic Characteristics of the Pharmacy Students (n=428) |
The prevalence of self-medication practice among pharmacy students was found to be 96.73%. It was observed that self-medication is most common in headache (338), cold, and cough (342) illnesses. Painkillers (386) and antibiotics (231) are the common categories of medicine that are preferred for self-medication purposes. Students believe that the disease is not very serious (346) and is the most common reason to prefer self-medication. Distribution of the self-medication practices among pharmacy students is represented in Table 2.
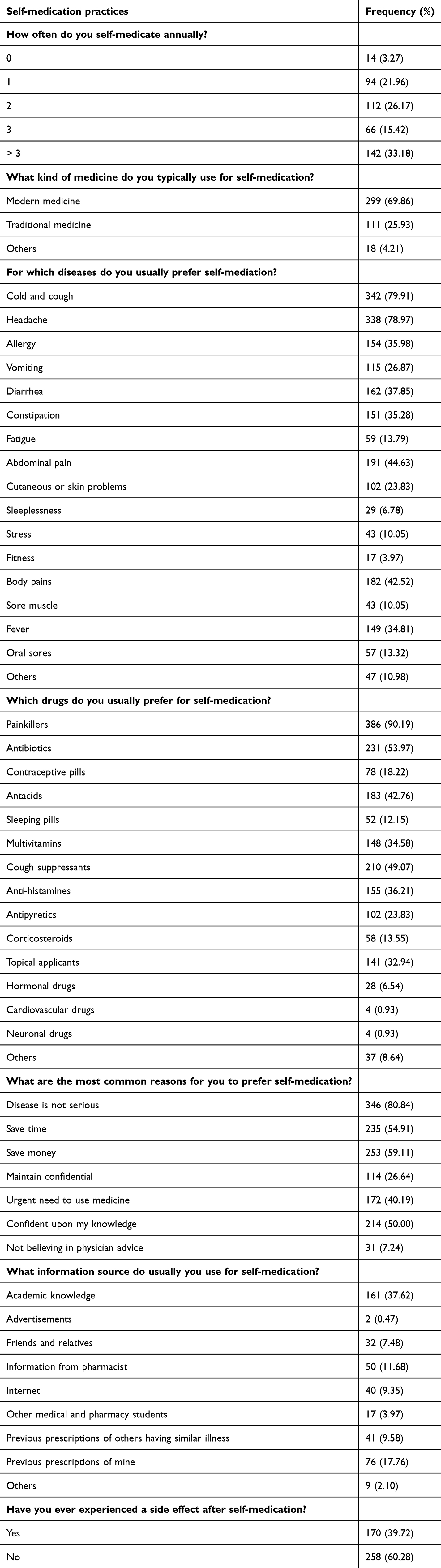 |
Table 2 Self-Medication Practices of Pharmacy Students |
The majority of students were aware of self-medication, and its safety. Students know that all types of medicines and medicines possess adverse effects and require medical attention upon experience of adverse effects during self-medication. Students are also aware that SM interferes with other medication prescribed by doctors, sometimes it will mask the symptoms of another disease. The distribution of pharmacy student’s knowledge about self-medication is presented in Table 3.
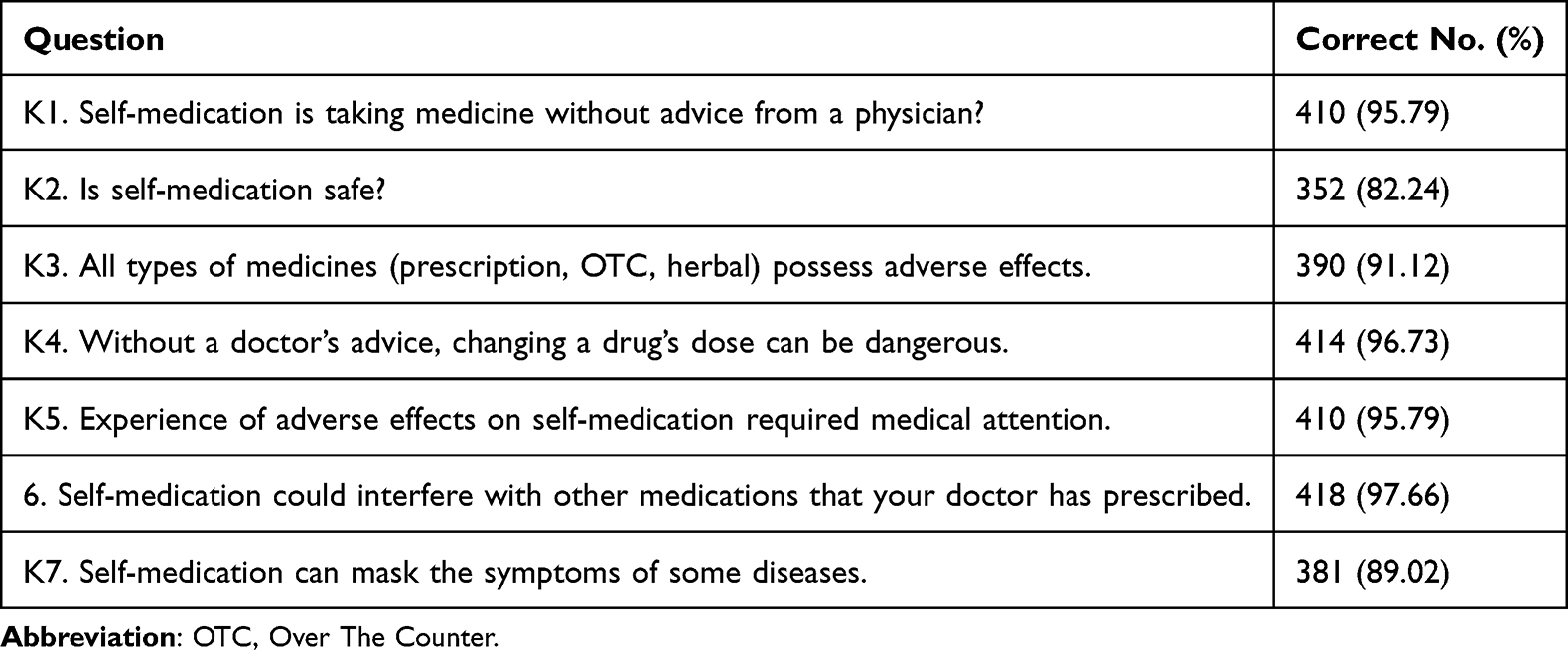 |
Table 3 Knowledge of Responsible Self-Medication Among Pharmacy Students |
The majority of the pharmacy students perceived positively toward all attitude statements of responsible self-medication. The distribution of pharmacy student’s attitudes toward responsible self-medication is presented in Table 4. The majority of pharmacy students practice self-medication for all types of illnesses (381), over a longer period (335). More the half of the students have a habit of reading leaflets or package inserts (251) while SM. One-third of the students have a practice of sharing medicines for similar symptoms (164), SM without professional advice (177), and have undergone training for responsible SM (141). The distribution of self-medication practices among pharmacy students is presented in Table 5.
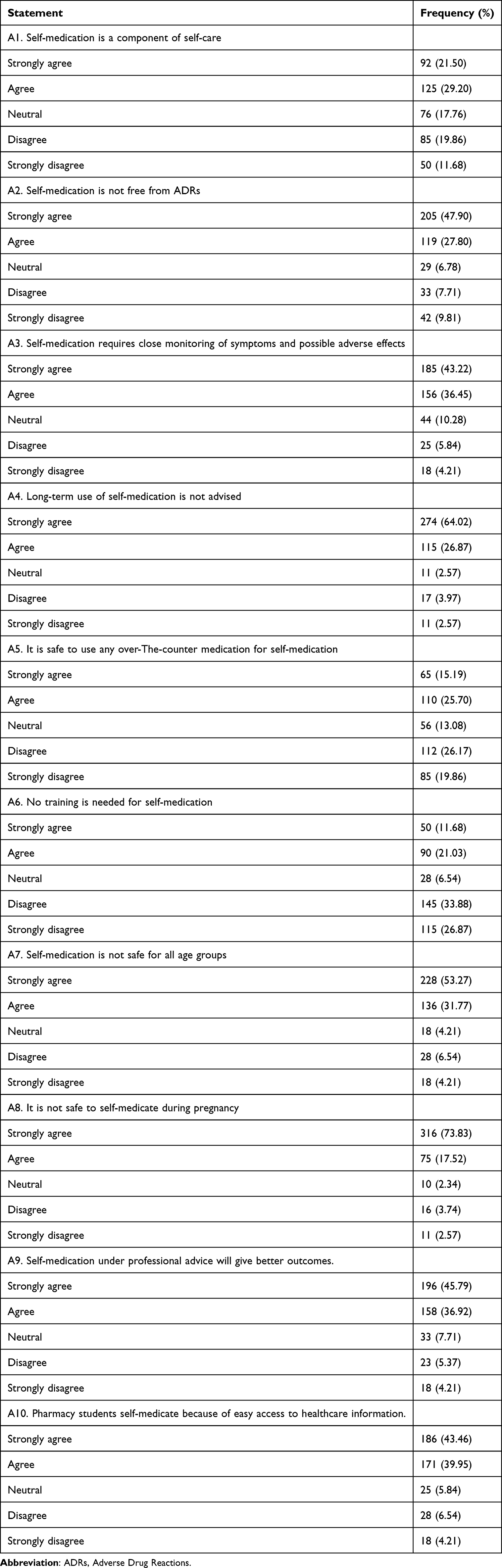 |
Table 4 Attitude Toward Responsible Self-Medication Among Pharmacy Students |
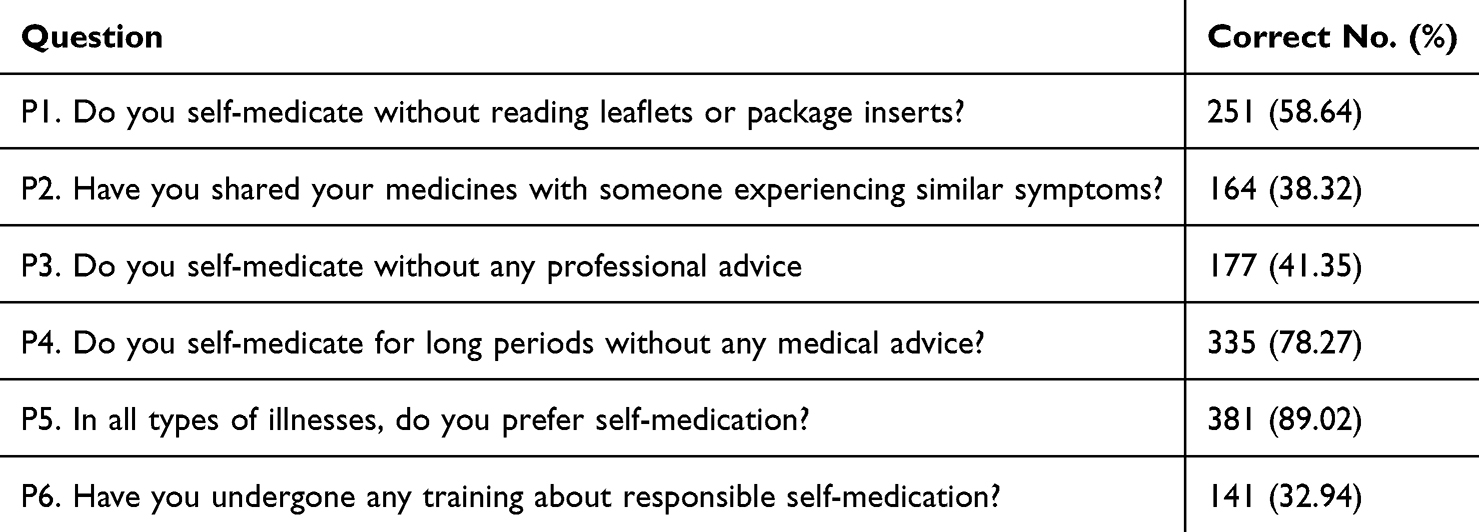 |
Table 5 Practice Toward Responsible Self-Medication Among Pharmacy Students |
The findings of the adequacy of KAP show that the majority of the pharmacy students have good knowledge (374), and a positive attitude (411) toward responsible self-medication. Whereas, very few students have a rational practice (117) toward self-medication. The distribution of adequacy levels of KAP toward responsible self-medication was presented in Table 6.
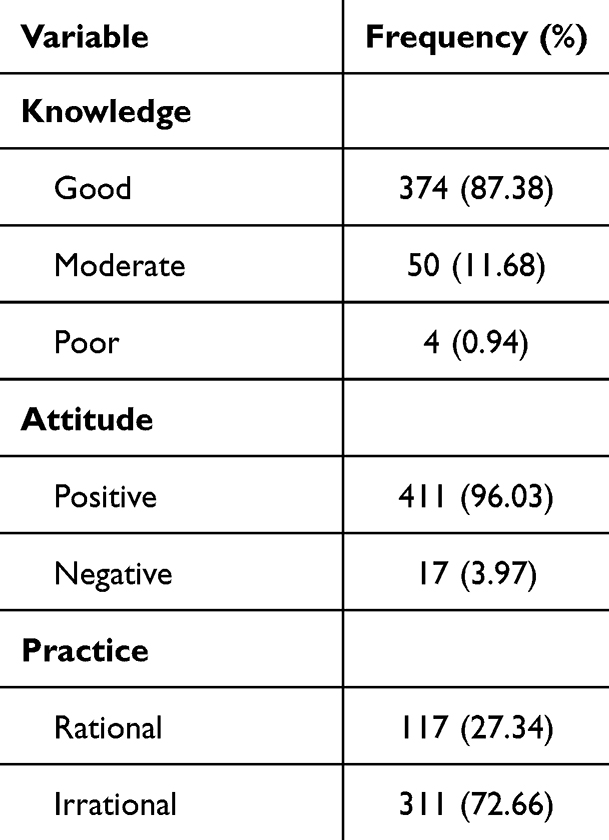 |
Table 6 Adequacy of KAP Toward Responsible Self-Medication Among Pharmacy Students |
Logistic regression analysis findings revealed that studying university (AOR = 2.76; 95% CI = 1.08–7.08), and parent’s profession (AOR = 0.28; 95% CI = 0.14–0.57) were significantly associated with pharmacy student’s knowledge of responsible self-medication. Whereas, factors such as gender (AOR = 0.55; 95% CI = 0.35–0.88), residence of the students (Rural: AOR = 0.48; 95% CI = 0.24–0.96, Semi-urban: AOR = 0.54; 95% CI = 0.32–0.89) and not suffering from any medical illness (AOR = 2.20; 95% CI = 1.18–4.11) were significantly associated with rational self-medication practice. Multivariate regression findings revealed that no factor was associated with positive attitude toward responsible self-medication among pharmacy students. Factors associated with good knowledge, positive attitude, and rational practice toward responsible SM are presented in Table 7. Bivariate and Multivariate Logistic Regression analyses of variables predicting good knowledge, positive attitude, and rational practices toward responsible self-medication among pharmacy students were presented with their P values in (Supplementary Tables 1-3).
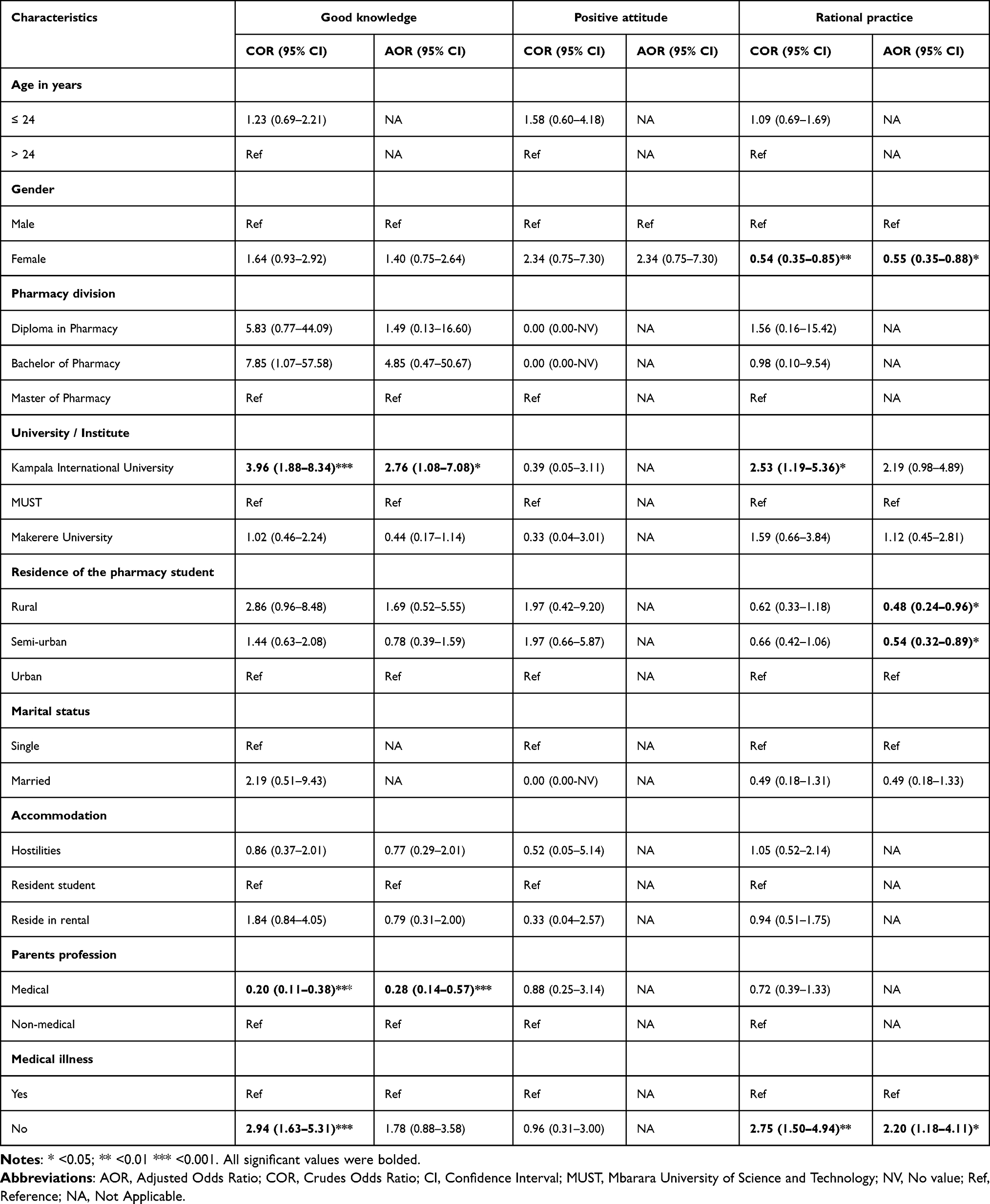 |
Table 7 Bivariate and Multivariate Logistic Regression Analysis of Variables Predicting Good Knowledge, Positive Attitude, and Rational Practice Toward Responsible Self-Medication Among Pharmacy Students (n=415) |
Discussion
Our study shows that the prevalence of self-medication practice among pharmacy students was 96.73%. In contrast with our findings, studies conducted in Ethiopia (38.5%), India (78.6%), Malaysia (57.2%) and Egypt (62.9%) show less prevalence of self-medication among medical students.30–33 Few studies conducted in developed countries such as the Netherlands (59.4%) and Colombia (34.3%) also reported a very low prevalence of self-medication.34,35 Studies conducted in Saudi Arabia revealed the prevalence of self-medication among university students of Riyadh (55.2%), and Najran (60.0%).36,37 The findings of our study were nearly similar to those of a study conducted among Palestinian students (98.0%).38 Overall, we observed a higher practice of self-medication among developing nations compared to developed nations. This could be attributed to the availability of higher-quality healthcare services, increased financial capacity to cover healthcare costs, and more efficient drug supply chain monitoring programs tailored to the specific needs of developed nations.
Previous studies conducted in Uganda about self-medication reported a prevalence of 63.5% at the Mbarara University of Science Technology (MUST), 74.2% at Lira University, and 79% of internet-enabled self-antibiotic use among patients of Kawempe private clinics.25,26,39 The variations observed in self-medication practice within the country are due to differences in the design, data collection techniques, type of medication assessed, location, and participants enrolled. Our study is a self-administered, online survey that was conducted among pharmacy students of three universities. Self-medication practices are higher among students than the general population. In the student category, pharmacy students have more chances to go for self-medication because of their clinical knowledge, exposure to more information about medications, and access to medicines. Additionally, students have better access to the internet and media advertising pharmaceutical products, which in turn promotes self-medication practice. The current study reveals that pharmacy students most commonly prefer headache relievers, cough and cold remedies, and antibiotics for self-medication. Similar findings are also observed in studies conducted in Uganda, Nigeria, Pakistan, and India. The rate of antibiotic self-medication use was reported to be 53.97% in our study, which was higher than the studies conducted in Ethiopia (35.2%), Serbia (44.0%), Palestine (50.0%), and Malaysia (39.3%).29,38,40,41 Self-antibiotic use is more common in developing nations than in developed nations. Ugandan standard treatment guidelines dictate that antibiotics are only available with a prescription from a licensed healthcare provider. These are inadequately enforced due to a variety of socioeconomic factors that may allow for indiscriminate access to antibiotics throughout the country.42 Evidence supports that using antibiotics for self-medication was higher among healthcare students and professionals than the general population.43 Antibiotic use without an appropriate diagnosis and prescription from authorized medical practitioners can increase the risk of antibiotic resistance in the country. In addition to traditional teaching modules in the coursework, we recommend providing educational interventions like workshops, seminars, and symposiums that highlight the role of pharmacists in combating antimicrobial resistance.
Many pharmacy students informed that the disease is not very serious (80.8%), saving time (54.9%), and saving money (59.11%) are the most common reasons for self-medication. Contrary to our study findings, a Nigerian study reveals that university students cite the behavior of healthcare providers, the distance of the clinics from the location, and the ineffectiveness of prescribed medicines as reasons for self-medication.6 An Iranian study revealed that the availability of stored medicines at home and having a history of the same illness were possible reasons for self-medication.12 Like our study’s findings, studies conducted in Iran, China, Brazil, and Rwanda also highlighted financial constraints, early management of the condition, and the disease’s lack of seriousness as major reasons for self-medication.44–46 In a Brazilian study, unawareness about possible consequences or side effects of the medicines was a reason for self-medication among nursing students.45 Though the symptoms expressed in acute conditions are limited by self-medication, it is very important to sensitize the students to consult medical practitioners if the symptoms are long-lasting. This will facilitate a rational approach to diagnosing and managing diseases among the student community.
The important finding of our study is that many students are using their academic knowledge as a resource of information for safe self-medication. Though the students have greater exposure to knowledge about diseases and medication management, students need to take advice from a registered medical practitioner or pharmacist while taking self-medication. During self-medication, there is a risk of taking excessive dosages, not following instructions in the use of medicines, and simultaneous administration of both prescription and non-prescription medicines that have potential interactions that can enhance the health-threatening complications. So, all medical and pharmacy students must be aware of responsible self-medication practices.
The findings of the adequacy level of KAP revealed that most pharmacy students have good knowledge and positive attitudes toward responsible self-medication. Whereas rational practice of self-medication is very low among pharmacy students. Similar findings, such as a high level of positive attitude about responsible self-medication and a low level of rational self-medication practice, were observed in a study conducted among pharmacy students in India.10 There is a wide gap in transforming good knowledge and a positive attitude into rational practices of self-medication in pharmacy students. The study recommends providing training modules and workshops on safe self-medication practice to pharmacy students. Thereby, the gap can be filled and students can acquire a high level of KAP about responsible self-medication.
Participants studying at KIU university were significantly associated with good knowledge about responsible self-medication. The higher odds of good knowledge among KIU students can be attributed to the greater number of responses from final-year pharmacy students compared to those from other universities. Factors such as gender, residence, and type of medical illnesses were significantly associated with rational self-medication practice among pharmacy students. Evidence about lower odds of rational self-medication practice in females was justified in a systematic review conducted on self-medication among university students.47 This review shows higher odds of self-medication in females compared to males. This could be due to females using more medications for their menstrual and gynecological illnesses, which in turn lessens the rational self-medication practice. Students from rural areas lack access to medical facilities, so these students try to self-medicate before getting initial medical care in the health facility.48 This could explain the high rate of rational self-medication among urban residents. An Indian study also found a connection between the residence and self-medication practices.10 Student parents who are practicing medical professionals can give appropriate guidance on conditions that can be self-diagnosed and require a medical practitioner’s attention for the diagnosis. This parental guidance can promote safe self-medication practices among pharmacy students. However, we found contrasting results in our study that students whose parents are non-medical-related have higher odds of good knowledge than those with medical-related parents. The factors identified in our study help in preparing targeted educational interventions to improve rational self-medication practices among pharmacy students.
Strengths and Limitations
The primary strength of our study is that the sample represented students from three top universities in Uganda with different socio-demographic backgrounds. Thus, the findings can be generalizable to similar settings. One more notable advantage of our study lies in the utilization of an online survey, which facilitated a heightened response rate and enabled us to obtain a substantial sample size.
The potential limitation of this study is using an online platform for data collection, which may have unknowingly excluded students residing in areas with limited social media and Internet accessibility. Again, the voluntary nature of the online survey has introduced selection bias, because the sample is not a representation of the targeted population. One of the researchers and the study participants were from the same university. This could have created some bias, especially in responses given by friendly participants from that university. Due to the cross-sectional nature of the survey, a temporal relationship cannot be established between factors and KAP levels of responsible self-medication. The knowledge, attitude, and practices of students can change with time and experience. So, it is advised to carry out prospective longitudinal studies to investigate the trends of student’s tendency towards self-medication practices and factors associated. The study used a non-probable snowball technique to capture the required participants, which can affect the generalizability of the findings. Furthermore, it is important to note that the data collected in this study were obtained through a self-administered online questionnaire rather than through interviews. This method of data collection may have introduced a potential bias, as participants may have provided information that is not entirely accurate or reflective of their true beliefs and intentions regarding self-medication practice. In any study, only subjective-based measures will introduce bias, it can be ruled out by including using objective-based measures, obtaining medicines left over in their home, and collecting of data at community pharmacy settings. The study captured self-medication practice for the past one year, this might have introduced recall bias in the study.
Conclusion
The study concludes that the prevalence of self-medication was very high among pharmacy students of three universities in Uganda. Painkillers and antibiotics are the most common drugs preferred for self-medication. It was observed that 87.38% of pharmacy students have good knowledge and 96.03% have a positive attitude toward responsible self-medication. However, the level of rational self-medication practice among students is very low. We recommended preparing training modules on safe self-medication practice, addressing the factors identified in our study, and implementing them among pharmacy students in Uganda to enhance their rational self-medication practices. Though they have heightened knowledge and positive attitudes that were acquired through their educational curriculum, transforming this into rational practice requires didactic training programs.
Ethical Considerations
The study protocol, data collection tools, and informed consent procedure were approved by the KIU-Research and Ethics Committee (KIU SPRC/004/24). This study was conducted following the provisions of the Declaration of Helsinki for research on human subjects. All subjects were informed of the study and its objectives, and informed consent was obtained from each participant.
Acknowledgments
The authors would like to thank all pharmacy university students for providing data regarding self-medication for the successful completion of the study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no conflict of interest and no affiliations with or involvement in any organization or entity with any financial interest (such as honoraria, educational grants, participation in speakers’ bureaus, membership, employment, consultancies, stock ownership, or other equity interest; and expert testimony or patent-licensing arrangements) or non-financial interest (such as personal or professional relationships, affiliations, knowledge, or beliefs) in the subject matter or materials discussed in this manuscript.
References
1. Organization WH. Guidelines for the regulatory assessment of medicinal products for use in self-medication. Published online 2000. Available from: https://iris.who.int/handle/10665/66154.
2. Torres NF, Chibi B, Middleton LE, Solomon VP, Mashamba-Thompson TP. Evidence of factors influencing self-medication with antibiotics in low and middle-income countries: a systematic scoping review. Public Health. 2019;168:92–101. doi:10.1016/j.puhe.2018.11.018
3. Alduraibi RK, Altowayan WM. A cross-sectional survey: knowledg e, attitudes, and practices of self-medication in medical and pharmacy students. BMC Health Serv Res. 2022;22(1):352. doi:10.1186/s12913-022-07704-0
4. Filho AI de L, Lima-Costa MF, Uchôa E. Bambuí Project: a qualitative approach to self-medication. Cad Saude Publica. 2004;20(6):1661–1669. doi:10.1590/s0102-311x2004000600025
5. Saha A, Zam D, Khan AA, Dutta P, Mannan A, Alam N. Prevalence and determinants of self-medication practices among general population: a cross-sectional study in Thimphu, Bhutan and Chattogram, Bangladesh. J Public Health Res. 2023;12(1):22799036231152327. doi:10.1177/22799036231152327
6. Osemene K, Lamikanra A. A study of the prevalence of self-medication practice among university students in Southwestern Nigeria. Trop J Pharm Res. 2012;11(4):683–689. doi:10.4314/tjpr.v11i4.21
7. Araia ZZ, Gebregziabher NK, Mesfun AB. Self medication practice and associated factors among students of Asmara college of health sciences, Eritrea: a cross sectional study. J Pharm Policy Pract. 2019;12(1):3. doi:10.1186/s40545-019-0165-2
8. Gelayee DA. Self-medication pattern among social science university students in Northwest Ethiopia. J Pharm. 2017;2017:8680714. doi:10.1155/2017/8680714
9. Abdelwahed RNK, Jassem M, Self-Medication Practices AA. Prevalence, and associated factors among Syrian adult patients: a cross-sectional study. In: Okosun IS, editor. J Environ Public Health. 2022; 2022. 1–7. doi:10.1155/2022/9274610
10. Susheela F, Goruntla N, Bhupalam PK, Veerabhadrappa KV, Sahithi B, Ishrar SMG. Assessment of knowledge, attitude, and practice toward responsible self-medication among students of pharmacy colleges located in Anantapur district, Andhra Pradesh, India. J Educ Health Promot. 2018;7(1):96. doi:10.4103/jehp.jehp_175_17
11. Hughes CM, McElnay JC, Fleming GF. Benefits and risks of self medication. Drug Safety. 2001;24(14):1027–1037. doi:10.2165/00002018-200124140-00002
12. Karimy M, Rezaee-Momtaz M, Tavousi M, Montazeri A, Araban M. Risk factors associated with self-medication among women in Iran. BMC Public Health. 2019;19(1):1033. doi:10.1186/s12889-019-7302-3
13. Mohammed SA, Tsega G, Hailu AD. Self-medication practice and associated factors among health care professionals at debre markos comprehensive specialized hospital, northwest Ethiopia. DHPS. 2021;13:19–28. doi:10.2147/DHPS.S290662
14. Figueiras A, Caamaño F, Gestal-Otero JJ. Sociodemographic factors related to self-medication in Spain. Eur J Epidemiol. 2000;16(1):19–26. doi:10.1023/a:1007608702063
15. Fuentes Albarrán K, Villa Zapata L. Analysis and quantification of self-medication patterns of customers in community pharmacies in southern Chile. Pharm World Sci. 2008;30(6):863–868. doi:10.1007/s11096-008-9241-4
16. Zhu X, Pan H, Yang Z, Cui B, Zhang D, Ba-Thein W. Self-medication practices with antibiotics among Chinese university students. Public Health. 2016;130:78–83. doi:10.1016/j.puhe.2015.04.005
17. Ha TV, Nguyen AMT, Nguyen HST. Self-medication practices among Vietnamese residents in highland provinces. J Multidiscip Healthc. 2019;12:493–502. doi:10.2147/JMDH.S211420
18. Seam MOR, Bhatta R, Saha BL, et al. Assessing the Perceptions and Practice of Self-Medication among Bangladeshi Undergraduate Pharmacy Students. Pharmacy. 2018;6(1):6. doi:10.3390/pharmacy6010006
19. Alsous M, Elayeh E, Abdel Jalil M, Alhawmdeh E. Evaluation of self-medication practice among pharmacy students in Jordan. Jordan J Pharm Sci. 2018;11:15–19.
20. Amponsah SK, Odamtten G, Adams I, Kretchy IA. A comparative analysis of pattern and attitude towards self-medication among pharmacy and non-pharmacy students in University of Ghana. Pan Afr Med J. 2022;41:254. doi:10.11604/pamj.2022.41.254.31013
21. Albayrak A. Assessment of pharmacy students’ knowledge, attitudes and practices on self medication. Bezmialem Science. 2024;12(1):38–45. doi:10.14235/bas.galenos.2023.70446
22. Hashemzaei M, Afshari M, Koohkan Z, Bazi A, Rezaee R, Tabrizian K. Knowledge, attitude, and practice of pharmacy and medical students regarding self-medication, a study in Zabol university of medical sciences; Sistan and Baluchestan province in south-east of Iran. BMC Med Educ. 2021;21(1):49. doi:10.1186/s12909-020-02374-0
23. Tomas Petrović A, Pavlović N, Stilinović N, et al. Self-medication perceptions and practice of medical and pharmacy students in Serbia. IJERPH. 2022;19(3):1193. doi:10.3390/ijerph19031193
24. Daanish AF, Mushkani EA. Influence of medical education on medicine use and self-medication among medical students: a cross-sectional study from Kabul. DHPS. 2022;14:79–85. doi:10.2147/DHPS.S360072
25. Niwandinda F, Lukyamuzi EJ, Ainebyona C, Ssebunya VN, Murungi G, Atukunda EC. Patterns and practices of self-medication among students enrolled at Mbarara University of Science and Technology in Uganda. Integr Pharm Res Pract. 2020;9:41–48. doi:10.2147/IPRP.S237940
26. Ikwara AE, Atwijukiire H. Self-medication and medication storage practices among Lira University students in Lira city, Northern Uganda. Front Public Health. 2023;11:1259279. doi:10.3389/fpubh.2023.1259279
27. Nakato G, Adongo PR, Iramiot JS, Epuitai J. Practices and drivers of self-medication with antibiotics among undergraduate medical students in Eastern Uganda: a cross-sectional study. Fadare JO, ed. PLoS One. 2023;18(12):e0293685. doi:10.1371/journal.pone.0293685
28. Narayana G, Suchitra M, Sunanda G, Ramaiah J, Kumar B, Veerabhadrappa K. Knowledge, attitude, and practice toward cervical cancer among women attending Obstetrics and Gynecology Department: a cross-sectional, hospital-based survey in South India. Indian J Cancer. 2017;54(2):481. doi:10.4103/ijc.IJC_251_17
29. Bekele KM, Abay AM, Mengistu KA, et al. Knowledge, attitude, and practice on over-the-counter drugs among pharmacy and medical students: a facility-based cross-sectional study. IPRP. 2020;9:135–146. doi:10.2147/IPRP.S266786
30. Abay SM, Amelo W. Assessment of Self-Medication Practices Among Médical, Pharmacy, Health Science Students in Gondar University, Ethiopia. J Young Pharm. 2010;2(3):306–310. doi:10.4103/0975-1483.66798
31. Kumar N, Kanchan T, Unnikrishnan B, et al. Perceptions and practices of self-medication among medical students in coastal south India. Al Naggar RA, ed. PLoS One. 2013;8(8):e72247. doi:10.1371/journal.pone.0072247
32. Jamshed SQ, Wong PS, Yi HC, Yun GS, Khan MU, Ahmad A. Self-medication practices among female students of higher educational institutions in Selangor, Malaysia: a quantitative insight. J Pharm Bioallied Sci. 2016;8(3):217–222. doi:10.4103/0975-7406.172662
33. Helal RM, Abou-ElWafa HS. Self-medication in university students from the City of Mansoura, Egypt. J Environ Public Health. 2017;2017:9145193. doi:10.1155/2017/9145193
34. Mulder LTC, Busch M, Kristoffersen AE, Hök Nordberg J, Van Der Werf ET. Prevalence and predictive factors of complementary medicine use during the first wave of the COVID-19 pandemic of 2020 in the Netherlands. BMC Complement Med Ther. 2022;22(1):43. doi:10.1186/s12906-022-03528-x
35. Gaviria-Mendoza A, Mejía-Mazo DA, Duarte-Blandón C, et al. Self-medication and the ‘infodemic’ during mandatory preventive isolation due to the COVID-19 pandemic. Therap Adv Drug Safety. 2022;13:204209862210723. doi:10.1177/20420986221072376
36. Mannasaheb BA, Al-Yamani MJ, Alajlan SA, et al. Knowledge, attitude, practices and viewpoints of undergraduate university students towards self-medication: an institution-based study in Riyadh. IJERPH. 2021;18(16):8545. doi:10.3390/ijerph18168545
37. Al-Qahtani AM, Shaikh IA, Shaikh MAK, Mannasaheb BA, Prevalence A-QFS. Perception, and practice, and attitudes towards self-medication among undergraduate medical students of Najran University, Saudi Arabia: a cross-sectional study. RMHP. 2022;15:257–276. doi:10.2147/RMHP.S346998
38. Naseef H, Joza’ D, Awawdeh A, et al. Evaluation of self-medication with antibiotics in primary care clinics in Palestine. Patient Prefer Adherence. 2022;16:2877–2892. doi:10.2147/PPA.S384671
39. Nakakande J, Taremwa IM, Nanyingi M, Mugambe S. The utility of internet-enabled antibiotic self-medication and its associated factors among patients attending private clinics in kawempe division in Kampala capital city, Uganda: community-based cross-sectional study. Drug Healthc Patient Saf. 2023;15:85–91. doi:10.2147/DHPS.S405072
40. Muratovic S, Curcic J, Milosevic N. Use and misuse of antibiotics among students in Serbian province Vojvodina. European Journal of Public Health. 2016;26(suppl_1). doi:10.1093/eurpub/ckw174.236
41. Haque M, Rahman NAA, McKimm J, et al. Self-medication of antibiotics: investigating practice among university students at the Malaysian National Defence University. IDR. 2019;12:1333–1351. doi:10.2147/IDR.S203364
42. Jackson M, Namuwenge Okure G, Namusisi M, Mukanga D. Over-the-counter suboptimal dispensing of antibiotics in Uganda. JMDH. 2013;303. doi:10.2147/JMDH.S49075
43. Kassa T, Gedif T, Andualem T, Aferu T. Antibiotics self-medication practices among health care professionals in selected public hospitals of Addis Ababa, Ethiopia. Heliyon. 2022;8(1):e08825. doi:10.1016/j.heliyon.2022.e08825
44. Lei X, Jiang H, Liu C, Ferrier A, Mugavin J. Self-medication practice and associated factors among residents in Wuhan, China. IJERPH. 2018;15(1):68. doi:10.3390/ijerph15010068
45. Gama ASM, Secoli SR. Self-medication among nursing students in the state of Amazonas - Brazil. Rev Gaucha Enferm. 2017;38(1). doi:10.1590/1983-1447.2017.01.65111
46. Tuyishimire J, Okoya F, Adebayo AY, Humura F, Lucero-Prisno DE. Assessment of self-medication practices with antibiotics among undergraduate university students in Rwanda. Pan Afr Med J. 2019;33. doi:10.11604/pamj.2019.33.307.18139
47. Behzadifar M, Behzadifar M, Aryankhesal A, et al. Prevalence of self-medication in university students: systematic review and meta-analysis. EMHJ. 2020;30(846–857):846–857.
48. Subashini N, Udayanga L. Demographic, socio-economic and other associated risk factors for self-medication behaviour among university students of Sri Lanka: a cross sectional study. BMC Public Health. 2020;20(1):613. doi:10.1186/s12889-020-08622-8
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.