Back to Journals » Patient Preference and Adherence » Volume 20
Knowledge, Attitude, and Practice Toward Long-Term Anticoagulation in Patients with Venous Thromboembolism: A Cross-Sectional Study
Authors Liu Z, Long J, Wang K, Chen J, Liu C, Jian Z
Received 3 February 2026
Accepted for publication 2 May 2026
Published 26 May 2026 Volume 2026:20 600999
DOI https://doi.org/10.2147/PPA.S600999
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Johnny Chen
Zirong Liu,1,* Jinfeng Long,1,* Kai Wang,2 Junliang Chen,2 Canzan Liu,3 Zhaocheng Jian1,2
1School of Medical Imaging, Shandong Second Medical University, Weifang, Shandong, People’s Republic of China; 2Interventional Vascular Surgery Center, Affiliated Hospital of Shandong Second Medical University, Weifang, Shandong, People’s Republic of China; 3Department of Medical Imaging, Yantai Affiliated Hospital of Binzhou Medical University, Yantai, Shandong, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Zhaocheng Jian, Email [email protected]
Background: This study aimed to explore the knowledge, attitude, and practice related to long-term anticoagulation therapy among patients with venous thromboembolism (VTE).
Methods: A cross-sectional study using a convenience sampling approach was conducted at the Interventional Vascular Surgery Center of Affiliated Hospital of Shandong Second Medical University from July 2025 to October 2025. A self-developed questionnaire based on the KAP framework was used for data collection, comprising three dimensions: knowledge (12 items), attitude (7 items), and practice (12 items, of which 5 scored items were used to calculate the practice domain score). Age-stratified subgroup analyses were conducted, and structural equation modeling was performed using AMOS 26.0 with bias-corrected bootstrap resampling to assess direct and indirect effects.
Results: A total of 389 patients with VTE were included, with a mean age of 45.62 years. Male patients accounted for 55.53% of the respondents. The mean scores were 40.87 ± 10.35 (possible range: 12– 60) for knowledge, 24.61 ± 5.32 (possible range: 7– 35) for attitudes, and 19.41 ± 4.15 (possible range: 5– 25) for practices. Based on the predefined 70% threshold, 206 patients (52.96%) met the criterion for adequate knowledge, whereas 183 (47.04%) were below this threshold. In addition, 231 (59.38%) had a positive attitude and 295 (75.84%) had proactive practice. Age-stratified analysis showed significant differences in knowledge, attitude, and practice scores across age groups (P < 0.001, P < 0.001, and P = 0.047, respectively), with patients aged < 45 years showing higher knowledge and attitude scores than older groups. Correlation analysis showed that knowledge was positively correlated with attitude (r = 0.597, P < 0.001), knowledge was positively correlated with practice (r = 0.364, P < 0.001), and attitude was positively correlated with practice (r = 0.487, P < 0.001). Structural equation modeling (SEM) results showed that attitude had a direct effect on practice (β = 0.674, 95% CI: 0.327– 1.068, P = 0.018), while knowledge indirectly affected practice through attitude (β = 0.473, 95% CI: 0.185– 0.783, P = 0.025).
Conclusion: Patients with VTE showed suboptimal knowledge, positive attitudes, and proactive practices towards long-term anticoagulation therapy. To enhance treatment adherence and safety, future clinical strategies should prioritize structured, attitude-oriented educational interventions that not only convey essential knowledge but also address patient concerns and behavioral barriers through individualized, longitudinal support mechanisms.
Keywords: venous thromboembolism, anticoagulants, medication adherence, patient knowledge, health behavior, cross-sectional studies
Background
Venous thromboembolism (VTE), encompassing deep vein thrombosis (DVT) and pulmonary embolism (PE), represents a major cardiovascular disorder with significant global health implications.1 As the third leading cause of cardiovascular mortality worldwide, VTE demonstrates an annual incidence of 1–2 per 1,000 person-years in Western populations and lower yet increasing rates (<1 per 1,000) in Eastern countries.2 Despite Asia’s relatively lower incidence, the substantial population base contributes to a considerable absolute disease burden.3 While PE-related mortality has declined in high-income nations, it remains elevated in lower-income regions, highlighting persistent global healthcare disparities.4 Furthermore, VTE survivors frequently develop long-term complications including post-thrombotic syndrome and chronic thromboembolic pulmonary hypertension, significantly impairing quality of life and increasing healthcare utilization.5
Anticoagulation therapy represents the cornerstone of VTE management, preventing thrombus propagation, embolization, and recurrence.6,7 Without appropriate treatment, recurrence rates increase dramatically, whereas adequate long-term anticoagulation substantially improves patient prognosis. The therapeutic landscape has evolved considerably from traditional warfarin-based regimens. Although effective, warfarin presents significant management challenges due to its narrow therapeutic window, substantial inter-patient dose variability, mandatory INR monitoring, and complex dietary and drug interactions.8,9
The introduction of non-vitamin K antagonist oral anticoagulants (NOACs), including rivaroxaban, apixaban, and dabigatran, has revolutionized VTE management. These agents offer superior pharmacokinetic profiles with fixed dosing, minimal dietary interactions, and eliminate routine coagulation monitoring requirements, substantially improving patient convenience.10,11 Clinical trials and real-world evidence demonstrate comparable efficacy with reduced major bleeding risk compared to warfarin, leading to their recommendation as first-line therapy for most patients with non-cancer-associated VTE.12,13 However, high costs, absence of simple monitoring tools, and inter-drug differences in efficacy and safety profiles—particularly apixaban’s superior safety compared to rivaroxaban and warfarin—limit universal adoption and necessitate individualized treatment approaches.14
Long-term anticoagulation remains crucial for high-recurrence-risk patients, including those with unprovoked VTE, active malignancy, or reduced mobility. Despite therapeutic advances, studies reveal inadequate patient knowledge regarding VTE pathophysiology and anticoagulation therapy,6 with substantial proportions of patients demonstrating suboptimal adherence to prescribed regimens.15 Understanding patient perceptions and treatment adherence patterns is therefore essential for optimizing clinical outcomes.
The knowledge–attitude–practice (KAP) theoretical framework posits that behavioral change occurs through sequential stages: knowledge acquisition, attitude development, and subsequent behavioral modification.16,17 Knowledge alone proves insufficient for behavioral change; it must first influence perceptions, which subsequently shape behaviors.18 KAP surveys have demonstrated utility in chronic disease management, particularly diabetes and hypertension, identifying adherence barriers and guiding targeted interventions.19 However, evidence specifically examining the KAP framework in patients receiving long-term anticoagulation for VTE remains relatively scarce.
This study aims to evaluate knowledge, attitudes, and practices regarding long-term anticoagulation among Chinese patients with DVT or PE history using a structured KAP questionnaire. Specifically, this study addresses the gap in understanding how knowledge, attitude, and practice are interrelated in this population, and whether attitude mediates the relationship between knowledge and practice. We hypothesized that better knowledge would be associated with more positive attitudes, and that more positive attitudes would in turn be associated with better anticoagulation-related practices. The findings may provide insights for developing targeted educational interventions, potentially improving adherence and reducing recurrence and bleeding events, which could contribute to enhanced VTE patient outcomes.
Methods
Study Design and Participants
This cross-sectional study was conducted at the Interventional Vascular Surgery Center of Affiliated Hospital of Shandong Second Medical University from July 2025 to October 2025 using a convenience sampling approach, enrolling adult patients with a confirmed diagnosis of venous thromboembolism (VTE) who had experience with anticoagulant therapy. Eligible participants met the following criteria: (1) age between 18 and 90 years; (2) a documented history of receiving oral anticoagulants (eg., warfarin or non-vitamin K antagonist oral anticoagulants) or parenteral agents such as low-molecular-weight heparin for a continuous duration of at least three months, including both patients currently on therapy and those who had completed their prescribed course; and (3) provision of written informed consent indicating voluntary participation and adequate understanding of the study objectives. Individuals were excluded if they met any of the following conditions: (1) presence of severe hepatic or renal dysfunction; (2) history of acute bleeding disorders or conditions associated with high bleeding risk; (3) known hypersensitivity to any component of anticoagulant medications; (4) current pregnancy or lactation; or (5) any medical, psychiatric, or social condition likely to interfere with adherence to anticoagulation therapy or participation in the study. The study protocol was reviewed and approved by the Institutional Review Board of The Medical Ethics Committee of Affiliated Hospital of Shandong Second Medical University (No. SDSMU-2025-ky-238), and informed consent was obtained from all participants prior to enrollment.
Questionnaire Development and Validation
A self-administered questionnaire was newly developed by the authors to assess patient KAP regarding anticoagulation therapy in the context of VTE. Item generation was informed by existing literature, current anticoagulation management recommendations, and clinical experience from the interventional vascular surgery team, with the aim of capturing both conceptual understanding and behavioral tendencies relevant to long-term anticoagulant use. Before pilot administration, the draft questionnaire was reviewed by clinicians involved in VTE management to ensure clinical relevance and clarity of item content. The instrument was structured into three domains—knowledge, attitude, and practice—each evaluated using a five-point Likert scale. The questionnaire included 12 knowledge items, 7 attitude items, and 12 practice items. Reverse-coded items were included in each section to improve data quality and reduce acquiescence bias. In addition, one attention-check item (item 13 in the knowledge section: “15 × 5 = 85”) was included in the questionnaire to identify inattentive responses; this item was used only for quality control and was not scored as part of the knowledge domain.
The knowledge section consisted of 12 items addressing fundamental concepts such as therapeutic indications, drug types, dosing regimens, side effect recognition, and the risk of recurrence. The attitude section included 7 statements reflecting beliefs about treatment necessity, perceived safety, personal efficacy, and long-term adherence. The practice section comprised 12 items covering self-reported behaviors, treatment-related experiences, and factors affecting adherence. Of these, 5 items (P1, P2, P3, P6, and P7) were scored to calculate the practice domain score and were also used as practice indicators in the SEM, whereas the remaining items (P4, P5, and P8–P12) were descriptive items included for descriptive analysis only. In the SEM and Supplementary Tables, the labels K1–K12 and A1–A7 correspond to the 12 knowledge items and 7 attitude items in the questionnaire, respectively, while P1, P2, P3, P6, and P7 correspond to the scored practice items selected from the 12-item practice section. Among the descriptive items, P4 and P5 assessed patients’ self-reported experience of recurrent thrombosis and bleeding complications during anticoagulation; these items were not included in the practice score or SEM. No specific recall period was defined for these descriptive items in the questionnaire. For scoring purposes, responses ranged from 1 (“strongly disagree”) to 5 (“strongly agree”) for the knowledge and attitude items, and from 1 (“never”) to 5 (“always”) for the scored practice items. Items with reverse polarity were appropriately recoded during analysis. A threshold of 70% of the maximum score in each domain was used to define adequate knowledge, positive attitude, and proactive practice, in line with previous anticoagulation-related KAP research.20
To assess reliability and ensure suitability for the target population, a pilot study was conducted with 40 patients prior to full-scale deployment. Results of the preliminary analysis demonstrated a Cronbach’s alpha coefficient of 0.930, indicating strong internal consistency. Minor revisions were made based on participant feedback to improve item clarity. The final version of the questionnaire was then administered to 389 patients who met inclusion criteria. Reliability analysis of the full dataset yielded a Cronbach’s alpha of 0.938 for the overall scale, confirming a high level of internal consistency across domains. Internal consistency was also assessed separately for each domain. Cronbach’s alpha coefficients were 0.938 for the knowledge domain, 0.801 for the attitude domain, and 0.844 for the practice domain. In addition, corrected item-total correlations were calculated for all scored items to examine item discrimination and potential redundancy. All corrected item-total correlations exceeded 0.30, indicating acceptable internal consistency and item homogeneity (Table 1).
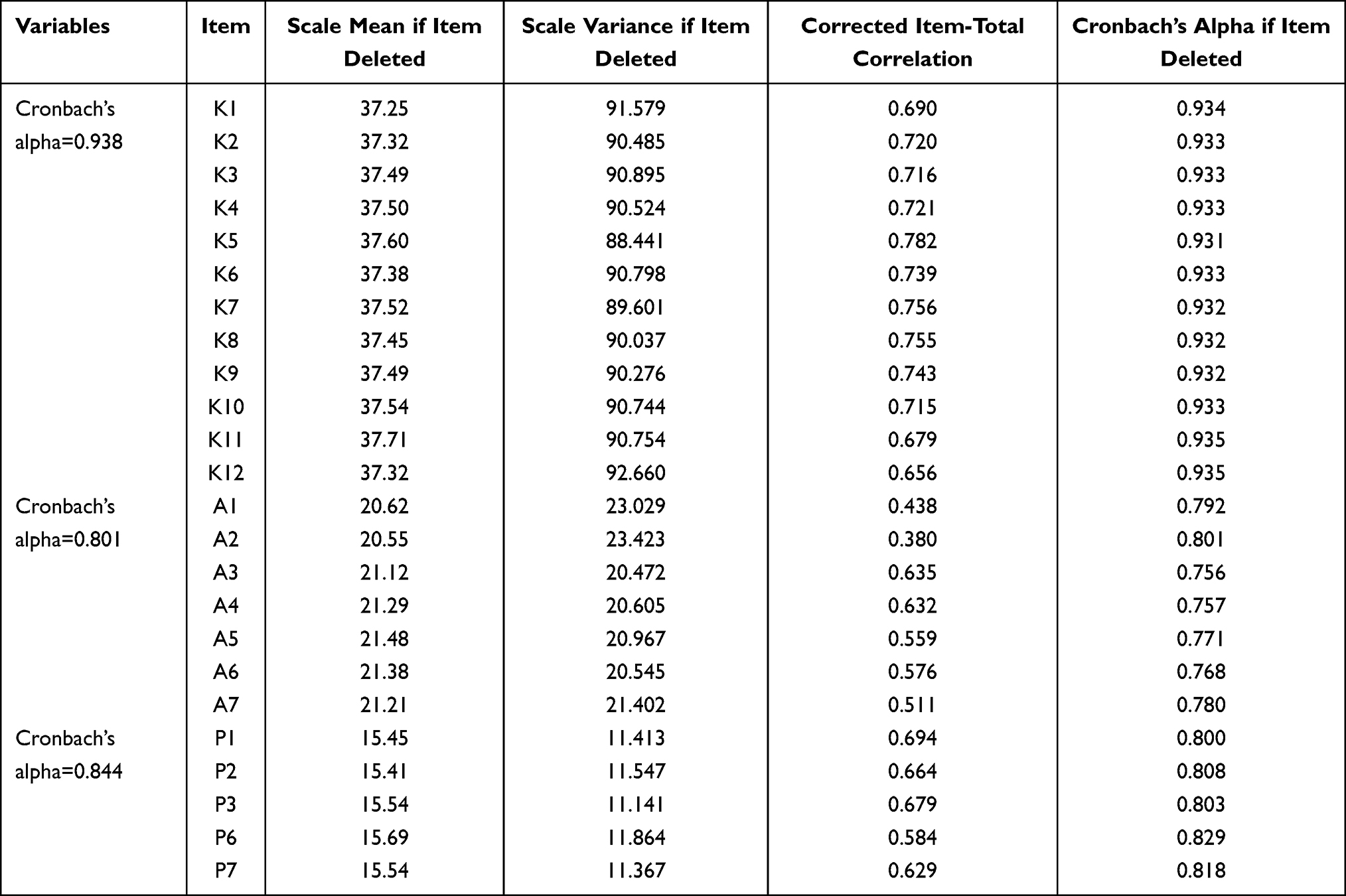 |
Table 1 Item-Total Statistics |
Questionnaire Administration
Data collection was primarily conducted through an online platform, allowing participants to complete the questionnaire electronically using a mobile device or computer. The questionnaire used in this study is provided in the Supplementary Figure 1 For individuals unable to access or navigate the digital system—due to technical limitations, literacy concerns, or personal preference—a paper-based version of the same questionnaire was made available as an alternative. Regardless of the mode of administration, all completed questionnaires were systematically entered into a secure database by trained research personnel. Data were reviewed for completeness and accuracy prior to statistical analysis.
Sample Size Calculation
The sample size for this study was estimated based on the standard formula for cross-sectional surveys, assuming a 95% confidence level, a 5% margin of error, and an expected adequate knowledge rate of 50%.


δ=0.05

The calculated minimum sample size was approximately 384, and considering a possible 20% non-response rate, at least 480 participants were targeted.
Statistical Analysis
All statistical analyses were performed using SPSS version 27.0 (IBM Corp., Armonk, NY, USA) and AMOS version 26.0 (IBM Corp., Armonk, NY, USA). Descriptive statistics were used to summarize demographic characteristics and scores across the domains of knowledge (K), attitude (A), and practice (P). Continuous variables were expressed as means and standard deviations (SD), while categorical variables were reported as frequencies and percentages [n (%)]. Group comparisons of KAP scores across different demographic categories were conducted using non-parametric methods. For group comparison purposes, the marital status variable was dichotomized into “married” and “unmarried” (comprising single, divorced, widowed, and other), to ensure adequate statistical power for the analysis, as the sample sizes in some of the original categories were small. In addition, participants were stratified into three age groups (<45, 45–60, and >60 years), and Kruskal–Wallis H-tests were used to compare knowledge, attitude, and practice scores across age groups. When significant overall differences were observed, post-hoc pairwise comparisons were performed using Dunn’s test with Bonferroni correction. Specifically, the Mann–Whitney U-test was applied for comparisons between two groups, and the Kruskal–Wallis H-test was used for comparisons involving three or more groups, as the data did not meet the assumptions of normality and homogeneity of variance. Correlations among knowledge, attitude, and practice scores were examined using Spearman’s rank correlation coefficient to account for non-normal distributions and ordinal scale properties. To further explore the directional relationships and potential mediating effects among the KAP components, structural equation modeling (SEM) was conducted using AMOS. The SEM included latent variables derived from item-level indicators within each domain. Bias-corrected bootstrap resampling (1,000 samples) was used to formally test the mediating effect of attitude and to estimate standardized direct, indirect, and total effects with their 95% confidence intervals. A mediating effect was considered statistically significant when the bias-corrected 95% confidence interval for the indirect effect did not include zero. Model fit was evaluated using the root mean square error of approximation (RMSEA), comparative fit index (CFI), Tucker–Lewis index (TLI), and incremental fit index (IFI). A two-tailed P-value less than 0.05 was considered statistically significant for all analyses.
Results
Initially, this study collected a total of 392 questionnaires. After quality control, exclusions comprised 2 cases with a response time under 60 seconds and 1 invalid questionnaire. Ultimately, 389 valid questionnaires were included in the analysis, with an effective rate of 99.23%. Although the final sample did not reach the planned target of 480 participants, it exceeded the calculated minimum required sample size of 384.
Demographic and Clinical Characteristics
A total of 389 patients with VTE were included, with a mean age of 45.62 years. Males accounted for 55.53% of respondents. The mean scores were 40.87 ± 10.35 for knowledge, 24.61 ± 5.32 for attitudes, and 19.41 ± 4.15 for practices. Practice scores differed significantly by gender (P = 0.003), with females scoring higher than males. Marital status was associated with knowledge (P = 0.028), with unmarried participants scoring higher. The number of children in the household was associated with knowledge (P = 0.003), attitudes (P = 0.003), and practices (P = 0.014), with childless participants scoring highest. Occupation was related to knowledge (P = 0.003) and practices (P = 0.001): employed participants scored highest in knowledge, while housewives had the highest practice scores. Monthly household income was associated with knowledge (P = 0.018) and attitudes (P = 0.017), with those earning over 10,000 CNY scoring highest. Years since VTE diagnosis were associated with practice (P = 0.001), with participants diagnosed for less than 2 years showing better practice. Current anticoagulant use was also related to practice (P = 0.002), with patients who were currently using anticoagulants scoring higher than those who had completed their prescribed course. Comorbidities were associated with knowledge (P = 0.023) and practices (P < 0.001), and the use of other chronic disease medications was related to lower practice scores (P < 0.001) (Table 2). To further examine age-related differences, participants were stratified into three groups: <45 years (n = 235), 45–60 years (n = 77), and >60 years (n = 77). Significant differences were observed across age groups in knowledge (P < 0.001), attitude (P < 0.001), and practice (P = 0.047) scores. Patients aged <45 years had the highest knowledge (43.66 ± 9.88) and attitude (25.42 ± 5.85) scores, whereas patients aged >60 years had the highest practice score (20.56 ± 3.49) (Table 3). Post-hoc comparisons showed that the <45 years group scored significantly higher than both the 45–60 years and >60 years groups, while no significant difference was observed between the 45–60 years and >60 years groups after Bonferroni correction (Table 4).
 |
Table 2 Baseline Characteristics |
 |
Table 3 Age Stratification Analysis |
 |
Table 4 Post-Hoc Comparisons of Age |
Knowledge, Attitude, and Practice
Based on the predefined 70% threshold, 206 patients (52.96%) met the criterion for adequate knowledge, whereas 183 (47.04%) were below the threshold. Similarly, 231 patients (59.38%) had a positive attitude and 295 (75.84%) had proactive practice. These proportions are summarized in Table 5. Knowledge was generally moderate, but several items showed notable gaps. In particular, many participants were uncertain about alternative therapies to anticoagulant treatment (K11), with 61.44% responding “neutral” or below (29.82% neutral, 24.94% not familiar, 6.68% not familiar at all). Similarly, a considerable proportion were unclear about the types of anticoagulant medications (K5), with 58.36% choosing “neutral” or lower (31.11% neutral, 20.57% not familiar, 6.68% not familiar at all), and about the safe dosage of these medications (K7), where 56.21% responded “neutral” or below (33.16% neutral, 19.02% not familiar, 4.63% not familiar at all). Uncertainty was also common for the duration of anticoagulant therapy (K9, 55.01% neutral or below) and the side effects of anticoagulant therapy (K10, 56.03% neutral or below) (Table 6).
 |
Table 5 Scores Summary of Knowledge, Attitude and Practice |
 |
Table 6 Distribution of Knowledge Dimension Responses |
Overall attitudes were moderately positive, yet several negative perceptions persisted. Notably, 32.9% of participants expressed doubts about their commitment to long-term anticoagulant therapy (A3, 6.43% strongly agree, 12.34% agree, 27.76% neutral), while 40.59% reported anxiety about having to take anticoagulants (A4, 5.4% strongly agree, 17.99% agree, 34.19% neutral). Concerns about potential side effects were also prevalent, with 43.83% indicating worry or uncertainty (A5, 9% strongly agree, 20.57% agree, 33.93% neutral). Additionally, 39.59% felt that treatment costs were burdensome (A6, 8.74% strongly agree, 18.77% agree, 32.13% neutral). Moreover, 24.16% agreed that missing one or two doses would not cause much harm (A7, 5.14% strongly agree, 19.02% agree) (Table 7).
 |
Table 7 Distribution of Attitude Dimension Responses |
Most participants reported relatively good adherence, though lapses and treatment-related barriers were common. About two-thirds consistently took their medication, with 37.02% always and 31.62% often doing so (P1), and 39.59% always and 30.33% often following prescriptions strictly (P2). However, adherence to follow-up visits was slightly lower, with only 37.28% always and 25.19% often attending as advised (P3). Missed doses were frequent, as 31.62% reported rarely and 27.51% never missing doses, meaning over 40% had lapses (P6). Furthermore, 37.53% had discontinued medication without medical advice at least occasionally (P7). In the descriptive items, 27.76% of participants reported having experienced recurrent thrombosis despite regular anticoagulation (P4), and 28.02% reported bleeding complications during anticoagulation (P5). Because these items were self-reported and no specific recall period was defined in the questionnaire, these findings should be interpreted as patient-reported treatment experiences rather than time-specific event rates. Financial burden was notable, with only 21.08% willing to spend more than 1000 CNY monthly on anticoagulants (P11). Regarding barriers, the most cited factors affecting adherence were concerns about side effects (59.9%), cost (54.24%), recurrence risk (53.21%), and treatment duration (53.21%) (P12) (Table 8).
 |
Table 8 Distribution of Practice Dimension Responses |
Correlation Analysis
Correlation analysis showed that knowledge was positively correlated with attitude (r = 0.597, P < 0.001), knowledge was positively correlated with practice (r = 0.364, P < 0.001), and attitude was positively correlated with practice (r = 0.487, P < 0.001) (Table 9).
 |
Table 9 Correlation Analysis |
SEM Analysis
The fit of the SEM model was acceptable (CMIN/DF = 2.979, RMSEA = 0.071, IFI = 0.905, TLI = 0.894, and CFI = 0.905) (Table S1). Bias-corrected bootstrap analysis based on 1,000 resamples showed that attitude had a significant direct effect on practice (β = 0.674, 95% CI: 0.327–1.068, P = 0.018), whereas the indirect effect of knowledge on practice through attitude was statistically significant (β = 0.473, 95% CI: 0.185–0.783, P = 0.025) and the direct effect of knowledge on practice was not significant (β = 0.072, 95% CI: −0.359 to 0.331, P = 0.642). Because the bias-corrected 95% confidence interval for the indirect effect did not include zero, attitude was considered to significantly mediate the relationship between knowledge and practice. The standardized total, direct, and indirect effects estimated by bootstrap are presented in Table 10, and the structural model is shown in Figure 1.
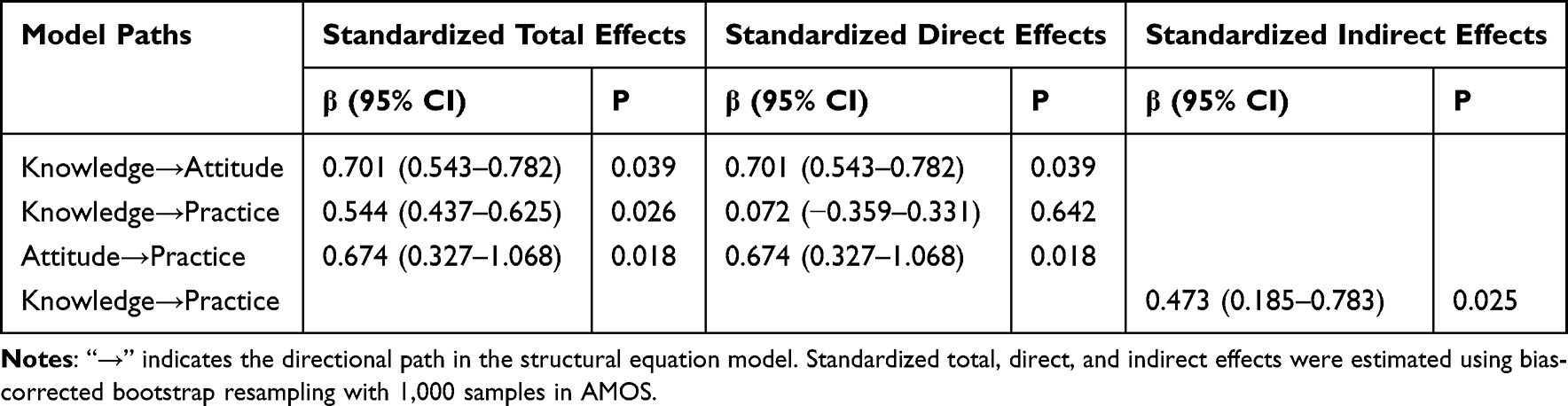 |
Table 10 Bootstrapped Standardized Effects and 95% Bias-Corrected Confidence Intervals for the Structural Model (1,000 Bootstrap Samples) |
 |
Figure 1 SEM of the KAP framework in patients with venous thromboembolism The latent variables “Knowledge,” “Attitude,” and “Practice” were measured using 12, 7, and 5 observed items, respectively; for the practice domain, these 5 observed items corresponded to the scored practice items (P1, P2, P3, P6, and P7) from the 12-item practice section. Standardized factor loadings are shown for each observed variable, and path coefficients illustrate the directional relationships among the latent constructs. Knowledge demonstrated a significant indirect effect on practice mediated through attitude, while attitude exerted a direct influence on practice. |
Discussion
The present findings suggest an imbalanced KAP profile in patients with VTE, characterized by suboptimal knowledge despite generally positive attitudes and relatively proactive practices toward long-term anticoagulation therapy. These findings highlight the need for structured, attitude-oriented educational interventions that not only enhance knowledge but also address patient concerns and motivation, thereby strengthening adherence behaviors and informing the development of scalable, patient-centered anticoagulation management strategies in clinical practice.
The structural equation analysis indicates that the relationship between knowledge and behavioral practice is not straightforward but mediated through patient attitudes. Knowledge appears to influence how patients evaluate the necessity and manageability of treatment, and it is this attitudinal orientation that exerts a more direct impact on whether appropriate practices are adopted. While knowledge may be a necessary foundation, it does not seem to provide sufficient motivational force on its own. This finding is particularly relevant in the context of long-term anticoagulation for VTE. Although VTE-specific studies examining the knowledge–attitude–practice pathway remain limited, previous research has shown that poor patient knowledge about VTE and its therapy is associated with an increased risk of major bleeding and discontinuation of anticoagulation treatment.6 In addition, adherence challenges during anticoagulant therapy have been recognized in real-world clinical practice.15 Our findings extend this anticoagulation-related literature by suggesting that knowledge may not translate directly into better treatment-related practices unless it is accompanied by more positive attitudes toward therapy, such as greater confidence in long-term treatment, lower anxiety, and better acceptance of treatment burden. In our study, many patients expressed uncertainty about key aspects of anticoagulation, such as medication types, dosing, duration, and side effects. Such knowledge gaps may impair the ability to follow treatment correctly, recognize complications, or make informed decisions, thereby heightening the risk of recurrence or bleeding events. The implication is that health education strategies focused exclusively on factual transmission may fall short if they do not also address treatment-related attitudes shaped by trust, past experience, and perceived efficacy. More broadly, this interpretation is also consistent with previous findings in chronic disease management, where knowledge alone often exerts limited behavioral influence unless supported by favorable beliefs and emotional alignment regarding treatment.21
In examining the distribution of knowledge across different thematic areas, a pattern of imbalance becomes apparent. Patients were more familiar with general aspects of disease risk, such as the possibility of recurrence, but demonstrated limited understanding of specific pharmacological principles. There was a particular lack of clarity regarding drug types, dosing schedules, side effect management, and long-term implications of therapy. This discrepancy suggests that while some form of disease-related knowledge may be reaching patients, the content is either too general or inadequately contextualized. Previous studies in chronic illness populations have identified similar gaps between general awareness and actionable understanding, especially when education is not personalized or interactive.22 Under such conditions, individuals may develop surface-level familiarity with terms without acquiring the conceptual depth necessary for informed participation. This may hinder their ability to evaluate conflicting information, interpret symptoms accurately, or make autonomous treatment decisions when clinical guidance is unavailable.
Although patient attitudes toward anticoagulant use were generally positive, closer inspection reveals signs of ambivalence. Many respondents agreed in principle with the importance of taking medication regularly and following medical advice, but at the same time expressed doubts about their own ability to adhere to treatment. Concerns about adverse effects, the burden of long-term therapy, and the cost of medication were commonly reported. These concerns are not uncommon in the context of chronic therapy, especially for asymptomatic conditions. Research in related populations suggests that attitudes significantly influence treatment behavior, particularly when practical burdens are perceived as high.23 In such cases, adherence may be driven more by external obligation than internal conviction, making patients vulnerable to lapses when difficulties arise. Moreover, if patients do not perceive immediate consequences from missing doses, their motivation to maintain consistency may weaken further.
Behavioral indicators presented a complex picture. While many patients reported adherence in general terms, responses also revealed frequent instances of missed doses, self-initiated discontinuation, and recurrence of adverse events such as thrombotic episodes or bleeding complications. These discrepancies raise questions about how patients interpret adherence and how they respond to setbacks during treatment. The relatively high proportions of self-reported recurrent thrombosis and bleeding complications should be interpreted cautiously, as P4 and P5 were descriptive items without a defined recall period and were intended to capture patients’ treatment-related experiences rather than standardized clinical event rates. Notably, a considerable proportion of patients reported behaviors such as missed doses, unsupervised discontinuation, and concerns about the financial burden of long-term therapy. These issues pose substantial clinical risks: irregular or interrupted anticoagulation may predispose patients to recurrence, while continuation without adequate guidance may elevate bleeding risk. Addressing these adherence challenges, alongside economic and psychological barriers, is therefore essential for improving patient safety. Studies in similar chronic conditions have shown that treatment fatigue, cost concerns, and side effect burden interact to undermine adherence, particularly in the absence of sustained clinical support.24 In the Chinese healthcare context, this finding is clinically relevant because the affordability of long-term anticoagulation is shaped not only by drug prices themselves but also by reimbursement arrangements and centralized procurement policies. Previous studies from China and other settings have shown that the cost-effectiveness and accessibility of direct oral anticoagulants vary across agents, and that reducing out-of-pocket costs may help alleviate economic barriers to sustained anticoagulation therapy.25,26
Demographic patterns in the data suggest that age, gender, employment status, and income level may shape how patients experience and manage anticoagulant therapy. In the present study, younger patients (<45 years) showed better knowledge and more positive attitudes than older age groups, whereas the oldest group demonstrated relatively better practice scores. This pattern may reflect the influence of age-related experiential and practical factors on medication-related behavior, beyond knowledge and attitude alone. In the present study, female participants had significantly higher practice scores than male participants (20.14 ± 3.83 vs. 18.82 ± 4.31, P = 0.003), indicating more consistent self-reported anticoagulation-related behaviors. Those with higher income or employment status also demonstrated somewhat greater knowledge and more favorable attitudes, although these advantages did not always extend to behavior. Similar patterns have been observed in population-based studies on chronic kidney disease, where demographic factors were closely linked to knowledge and attitude levels.27 The gap between positive orientation and behavioral follow-through highlights the role of external barriers. Even a patient who understands and values adherence may lack the logistical or financial means to maintain it. This underscores the need for interventions that combine education with structural supports such as subsidized care, flexible appointments, and community-based reinforcement.
Intervention efforts aimed at improving adherence should take these findings into account. A narrowly defined information campaign is unlikely to be effective unless it also addresses attitudinal uncertainty and logistical challenges. In particular, it may be necessary to engage patients in reflective conversations about side effect interpretation, treatment burden, and how they define success. Communication strategies should elicit patient concerns, not merely correct misconceptions. Additionally, periodic reassessment of beliefs and practices can help identify early signs of disengagement. Interventions that combine individualized education with dialogic counseling and system-level support have been shown to improve adherence outcomes in similar contexts.21,28 Structured health education programs, when paired with counseling, have led to measurable improvements in adherence and self-care behaviors across chronic disease populations.23 These integrated approaches are more likely to produce lasting behavioral change than education alone.
This study has several limitations that should be acknowledged. First, the cross-sectional design limits causal inference between knowledge, attitudes, and practices, as temporal or longitudinal dynamics could not be captured; future prospective studies are warranted to validate the observed pathway relationships over time. Although the overall SEM fit was acceptable, the TLI value (0.894) was slightly below the conventional threshold of 0.90, and the model fit should therefore be interpreted with some caution. Second, the sample was drawn from a single center and primarily collected through online questionnaires, which may introduce selection bias and limit the generalizability of findings to populations with lower digital literacy or different healthcare access. In addition, because the study included both patients currently receiving anticoagulants and those who had completed their prescribed course, the attitude and practice scores should be interpreted as reflecting anticoagulation-related perceptions and self-reported behaviors across the treatment experience, rather than only current medication-taking status. Although the final sample size of 389 exceeded the calculated minimum requirement of 384, it did not reach the planned target of 480 participants after accounting for potential non-response. This shortfall may have reduced the precision of some estimates, particularly in subgroup analyses, and should be considered when interpreting the findings. Moreover, multiple subgroup comparisons were conducted across a range of demographic and clinical variables, and no formal correction for type I error inflation was applied to these exploratory analyses; therefore, these associations should be interpreted with caution. Another limitation is that education level, which is an important predictor of health literacy and KAP outcomes, was not collected in the present study because the questionnaire design primarily focused on treatment-related experiences and anticoagulation-specific factors. As a result, its potential influence on knowledge, attitudes, and practices could not be examined and should be considered in future studies. In addition, the study did not differentiate between VTE subtypes (ie., DVT or PE). Given that clinical management, patient concerns, and the required duration of anticoagulation may differ between these conditions, the aggregated analysis may have masked subtype-specific differences in knowledge, attitudes, and practices. Moreover, the type of anticoagulant used (eg., warfarin, NOACs, or low-molecular-weight heparin) was not collected or analyzed separately. This may have limited the interpretation of patient knowledge and practice patterns, as treatment experience and educational needs can vary according to the anticoagulant regimen. Although the study included a relatively diverse sample in terms of demographics and anticoagulant use, regional and institutional factors may still influence patient perceptions and behaviors. Third, self-reported responses are inherently subject to recall and social desirability biases, which may have inflated adherence or attitude scores; however, efforts such as anonymous participation and reverse-coded items were implemented to minimize such effects. In addition, although the present questionnaire demonstrated acceptable internal consistency, it was self-developed rather than based directly on established anticoagulation-specific instruments. Future studies may benefit from further comparison with, or incorporation of, validated tools such as the Oral Anticoagulation Knowledge Test or the Anticoagulation Knowledge Tool for knowledge assessment, and standardized adherence measures such as the Morisky Medication Adherence Scale when appropriate.29,30 In addition, the descriptive items on recurrent thrombosis and bleeding complications (P4 and P5) did not specify a defined recall period, which limits the clinical interpretability of these self-reported proportions. Nevertheless, the questionnaire showed acceptable internal consistency at both the overall and domain levels, and all corrected item-total correlations were above 0.30.
Conclusions
In conclusion, based on the predefined 70% threshold, 206 patients (52.96%) demonstrated adequate knowledge, 231 (59.38%) showed a positive attitude, and 295 (75.84%) exhibited proactive practice. Overall, these findings indicate suboptimal knowledge but relatively positive attitudes and proactive practices among patients with VTE, and further confirm that attitude plays a pivotal mediating role between knowledge and behavioral adherence. To enhance long-term anticoagulation adherence, future interventions should more specifically address the key barriers identified in this study, including treatment cost, concerns about side effects, and uncertainty regarding treatment duration. In the Chinese healthcare setting, more actionable strategies may include clearer medication counseling during follow-up, targeted education on adverse effect recognition and management, improved communication about the expected duration of anticoagulation, and practical support to help patients navigate cost-related treatment decisions within routine care.
Abbreviations
VTE, Venous Thromboembolism; KAP, Knowledge, Attitude, and Practice; DVT, Deep Vein Thrombosis; PE, Pulmonary Embolism; NOACs, Non-Vitamin K Antagonist Oral Anticoagulants; SEM, Structural Equation Modeling; INR, International Normalized Ratio; SPSS, Statistical Package for the Social Sciences; AMOS, Analysis of Moment Structures; RMSEA, Root Mean Square Error of Approximation; CFI, Comparative Fit Index; TLI, Tucker–Lewis Index.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Consent to Participate
The study was approved by the Institutional Review Board of Affiliated Hospital of Shandong Second Medical University (SDSMU-2025-ky-238). All participants were informed about the study protocol and provided written informed consent to participate in the study. I confirm that all methods were performed in accordance with the relevant guidelines. All procedures were performed in accordance with the ethical standards laid down in the 1964 Declaration of Helsinki and its later amendments.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests.
References
1. Klemen ND, Feingold PL, Hashimoto B, et al. Mortality risk associated with venous thromboembolism: a systematic review and Bayesian meta-analysis. Lancet Haematol. 2020;7(8):e583–15. doi:10.1016/S2352-3026(20)30211-8
2. Pastori D, Cormaci VM, Marucci S, et al. A comprehensive review of risk factors for venous thromboembolism: from epidemiology to pathophysiology. Int J Mol Sci. 2023;24(4):3169. doi:10.3390/ijms24043169
3. Zhen K, Tao Y, Xia L, et al. Epidemiology of pulmonary embolism in China, 2021: a nationwide hospital-based study. Lancet Reg Health West Pac. 2025;54:101258. doi:10.1016/j.lanwpc.2024.101258
4. Hagiya H, Harada K, Nishimura Y, et al. Global trends in mortality related to pulmonary embolism: an epidemiological analysis of data from the World Health Organization mortality database from 2001 to 2023. EClinicalMedicine. 2025;86:103389. doi:10.1016/j.eclinm.2025.103389
5. Lutsey PL, Zakai NA. Epidemiology and prevention of venous thromboembolism. Nat Rev Cardiol. 2023;20(4):248–262. doi:10.1038/s41569-022-00787-6
6. Gołąb A, Plicner D, Konieczyńska M, Broniatowska E, Undas A. Poor patients’ knowledge about venous thromboembolism and its therapy is associated with increased risk of major bleeding and discontinuation of anticoagulation: a cohort study. Medicine. 2024;103(28):e38697. doi:10.1097/MD.0000000000038697
7. Kearon C, Kahn SR. Long-term treatment of venous thromboembolism. Blood. 2020;135(5):317–325. doi:10.1182/blood.2019002364
8. Fahmi AM, Elewa H, El Jilany I. Warfarin dosing strategies evolution and its progress in the era of precision medicine, a narrative review. Int J Clin Pharm. 2022;44(3):599–607. doi:10.1007/s11096-022-01386-8
9. Witt DM, Clark NP, Kaatz S, Schnurr T, Ansell JE. Guidance for the practical management of warfarin therapy in the treatment of venous thromboembolism. J Thromb Thrombolysis. 2016;41(1):187–205. doi:10.1007/s11239-015-1319-y
10. Al Mukdad M, Al-Badriyeh D, Elewa HF. Cost-effectiveness evaluations among the direct oral anticoagulants for the prevention and treatment of venous thromboembolism: systematic review. Clin Appl Thromb Hemost. 2019;25:1076029619849103. doi:10.1177/1076029619849103
11. De Caterina R, Chiusolo S. Over 10 years of non-vitamin K antagonist oral anticoagulants: highlights, challenges, and future developments. Eur Heart J Suppl. 2025;27(Suppl 1):i6–i11. doi:10.1093/eurheartjsupp/suae087
12. Kumbhani DJ, Cannon CP, Beavers CJ, et al. ACC expert consensus decision pathway for anticoagulant and antiplatelet therapy in patients with atrial fibrillation or venous thromboembolism undergoing percutaneous coronary intervention or with atherosclerotic cardiovascular disease: a report of the American college of cardiology solution set oversight committee. J Am Coll Cardiol. 2021;77(5):629–658. doi:10.1016/j.jacc.2020.09.011
13. Singh B, Pai P, Kumar H, et al. Expert recommendations on the usage of non-vitamin k antagonist oral anticoagulants (noacs) from India: current perspective and future direction. Cardiol Ther. 2022;11(1):49–79. doi:10.1007/s40119-022-00254-w
14. Bea S, Iyer GS, Kim DH, et al. Oral anticoagulation and risk of adverse clinical outcomes in venous thromboembolism. JAMA Intern Med. 2025;185(7):837–846. doi:10.1001/jamainternmed.2025.1109
15. Talana AS, Huber K, Sorin M, Stalvey C, Davis K, Dietrich E. Patient-level adherence and interventions in an interdisciplinary DOAC clinic. Thromb Res. 2019;179:34–36. doi:10.1016/j.thromres.2019.04.021
16. Abdulazeem HM, Meckawy R, Schwarz S, Novillo-Ortiz D, Klug SJ. Knowledge, attitude, and practice of primary care physicians toward clinical AI-assisted digital health technologies: systematic review and meta-analysis. Int J Med Inform. 2025;201:105945. doi:10.1016/j.ijmedinf.2025.105945
17. Bayked EM, Yimer EM, Gelaw T, Mohammed AS, Mekonen NA. Dietary knowledge, attitude, practice, and associated factors among pregnant mothers in Ethiopia: a systematic review and meta-analysis. Front Public Health. 2024;12:1393764. doi:10.3389/fpubh.2024.1393764
18. Wang J, Chen L, Yu M, He J. Impact of knowledge, attitude, and practice (KAP)-based rehabilitation education on the KAP of patients with intervertebral disc herniation. Ann Palliat Med. 2020;9(2):388–393. doi:10.21037/apm.2020.03.01
19. Chen Q, Liu F, Zhang L, Jin Y, Huang H. Knowledge, attitudes, and practices regarding the prevention of intracerebral hemorrhage among hypertensive patients. Front Cardiovasc Med. 2025;12:1361273. doi:10.3389/fcvm.2025.1361273
20. Li C, Meng Y, Meng X, Song Y. Knowledge, attitude and practice toward oral anticoagulants among patients with atrial fibrillation. Frontiers in Cardiovascular Medicine. 2023:10–2023.
21. Ren L, Li Z, Wu J, Duan L, Gao GJ. Knowledge, attitudes, and practices among elderly chd patients towards self-perceived health abilities. J. Multidiscip. Healthc. 2024;17:1999–2011. doi:10.2147/JMDH.S463043
22. Legese YM, Gebru SB, Gebremariam AG, Tesfay ZA. Knowledge, attitude, and practice towards COVID-19 among chronic disease patients visiting public hospitals. Heliyon. 2023;9(7):e17734. doi:10.1016/j.heliyon.2023.e17734
23. Wang A, Wan J, Zhu L, et al. Frailty and medication adherence among older adult patients with hypertension: a moderated mediation model. Front Public Health. 2023;11:1283416. doi:10.3389/fpubh.2023.1283416
24. Mpinda B, Kabogo CD, Yoko JLM, Tumbo J. Knowledge, attitudes, and practices of chronic disease patients in Bojanala towards COVID-19. S Afr Family Pract. 2023;65(4). doi:10.4102/safp.v65i1.5763
25. Tian S, Zhong H, Yin M, Jiang P, Liu Q. A china-based cost-effectiveness analysis of novel oral anticoagulants versus warfarin in patients with left ventricular thrombosis. Risk Manag Healthc Policy. 2024;17:945–953. doi:10.2147/RMHP.S454463
26. Zhang Q, Wang R, Chen L, Chen W. Effect of China national centralized drug procurement policy on anticoagulation selection and hemorrhage events in patients with AF in Suining. Front Pharmacol. 2024;15:1365142. doi:10.3389/fphar.2024.1365142
27. Kazmi SMK, Dawood T, Arif SM, et al. Assessment of knowledge, attitudes, and practices associated with chronic kidney disease in pakistan. Eur. J. Health Sci. 2023;9(4):40–53. doi:10.47672/ejhs.1696
28. Wang D, Liu Z, Liu Y, et al. Knowledge, attitudes, and practices among patients with diabetes mellitus and hyperuricemia toward disease self-management. Front Public Health. 2024;12:1426259. doi:10.3389/fpubh.2024.1426259
29. Zeolla MM, Brodeur MR, Dominelli A, Haines ST, Allie ND. Development and validation of an instrument to determine patient knowledge: the oral anticoagulation knowledge test. Ann Pharmacother. 2006;40(4):633–638. doi:10.1345/aph.1G562
30. Obamiro KO, Chalmers L, Bereznicki LR. Development and validation of an oral Anticoagulation Knowledge Tool (AKT). PLoS One. 2016;11(6):e0158071. doi:10.1371/journal.pone.0158071
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
New Oral Anticoagulants Open New Horizons for Cancer Patients with Venous Thromboembolism
Wumaier K, Li W, Cui J
Drug Design, Development and Therapy 2022, 16:2497-2507
Published Date: 3 August 2022
Evaluating Strategies for Enhancing Medication Adherence in the Kingdom of Saudi Arabia (KSA): A Cross-Sectional Study
Alhomoud FK, Alwohaibi LW, Aljarrash K, Alhomoud F, Alamer K, Alsultan MM, Alqarni Y, Alotaibi N, Alsaad AK, Alqahtani AD, Alkhnbashi RS
Patient Preference and Adherence 2024, 18:2469-2480
Published Date: 8 December 2024
Perceived Barriers as Key Behavioral Predictors of Medication Adherence in Older Adults with Diabetes in Northern Iran: Insights from the Health Action Process Approach
Dashteban Namaghi A, Bakhtiari A, Ghorbani S, Zeinali A
Patient Preference and Adherence 2026, 20:550698
Published Date: 4 February 2026