Back to Journals » Journal of Multidisciplinary Healthcare » Volume 19
Knowledge, Attitude, and Practice Regarding Adverse Transfusion Reactions Among Nurses, Physicians, and Transfusion Specialists in China: A Multicenter Cross-Sectional Survey
Authors Hu T, Zhou X, OuYang X, Wang Y, Sun T
Received 23 September 2025
Accepted for publication 4 March 2026
Published 25 March 2026 Volume 2026:19 569692
DOI https://doi.org/10.2147/JMDH.S569692
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Professor Linda Yoder
Tingting Hu,1,* Xueying Zhou,2,* Xu OuYang,2,* Yan Wang,3 Ting Sun1
1Department of Blood Transfusion, Liaoning Cancer Hospital & Institute, Shenyang, People’s Republic of China; 2Blood Transfusion Medicine Department, General Hospital of Northern Theater Command, Shenyang, People’s Republic of China; 3Department of Blood Transfusion, Central Hospital of Yingkou Economic and Technological Development Zone (The People’s Hospital of Yingkou), Yingkou, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Ting Sun, Department of Blood Transfusion, Liaoning Cancer Hospital & Institute, Shenyang, 110042, People’s Republic of China, Tel +8618900917558, Email [email protected]
Introduction: Adverse transfusion reactions (ATRs) can threaten patient safety. Healthcare professionals (HPs) play crucial roles in the prevention and management of ATRs. Although ATRs occur in 0.2– 0.6% of transfusions in China, no study has examined the knowledge, attitude, and practice (KAP) toward them. Therefore, the aim of this study was to investigate the KAP of HPs toward ATRs.
Methods: This multicenter cross-sectional study was conducted between October and December 2023 and included HPs from 146 medical institutions enrolled through WeChat professional groups using convenience sampling. An investigator-developed web-based questionnaire (Cronbach’s α=0.82) was used to collect participants’ demographic characteristics and their KAP towards ATRs. Bloom’s cutoffs were used to categorize KAP dimension scores. Multivariable logistic regression analysis was performed, including the factors statistically significant in the univariable analyses.
Results: The study included 327 (40.93%) nurses, 253 (31.66%) physicians, and 219 (27.41%) transfusion specialists. Among the participants, 598 (74.84%) were females, 238 (29.79%) held a master’s degree or higher, 389 (48.69%) possessed over 10 years of work experience. The knowledge and attitude scores were 11.78± 1.78 (possible range: 0– 14) and 50.43± 4.74 (possible range: 11– 55). The practice scores (possible range: 0– 50) were evaluated for nurses, physicians, and transfusion specialists respectively, and the mean scores were 49.22± 2.79, 47.60± 5.09, and 44.35± 14.13. Multivariate analysis showed that having a master’s degree or above (OR=1.480, 95% CI: 1.079– 2.027, P=0.015) was independently associated with knowledge. The knowledge (OR=1.280, 95% CI: 1.159– 1.423, P=0.001), department (OR=1.731– 1.763, 95% CI: 1.120– 2.696, P< 0.050), and the understanding of ATRs (OR=1.122, 95% CI: 1.035– 1.218, P=0.006) were independently associated with attitude.
Conclusion: The surveyed Chinese healthcare professionals HPs displayed good KAP regarding ATRs. However, specific knowledge gaps were identified, particularly concerning bacterial contamination risks and delayed reactions. While attitudes and self-reported practices were largely positive, targeted educational interventions are recommended to address these identified knowledge deficits and reinforce best practices.
Keywords: knowledge, attitude, practice, healthcare professionals, China, transfusion reaction, cross-sectional study
Introduction
Blood transfusions are relatively common in hospitals worldwide and in China and can be performed to correct blood loss, manage non-hemorrhagic anemia (eg, in patients under chemotherapy), or correct specific medical conditions.1 It is a crucial medical intervention in modern medicine that plays an irreplaceable role.2–4 Although modern transfusions conducted under the strict guidance of blood banks are considered safe, adverse reactions during a transfusion can occur.1,5,6 Most reactions can pose immediate or short-term health threats to the patients and can even be fatal, while others can increase the risk of infection or immune reactions in the long term and can also be fatal.7–11 China has rapidly expanded and formalized its hemovigilance system in recent years, with the Chinese Hemovigilance Network established to systematically monitor transfusion safety and support a national policy on appropriate blood use and adverse reaction reporting.12,13 In China, the overall adverse transfusion reaction (ATR) incidence is 0.2%-0.6%.12–14 Therefore, ensuring transfusion safety and preventing and promptly addressing ATRs are pivotal aspects of enhancing patient treatment outcomes and quality of life.6,15 Given these risks, the competence of healthcare professionals directly influences transfusion outcomes.
Healthcare professionals are the ones who perform transfusions and, therefore, play crucial roles in the prevention and management of ATRs. Their application of specialized knowledge and skills is required in the pre-transfusion assessment, monitoring during transfusion, and post-transfusion observation to identify and manage potential adverse reactions.16 Timely intervention and accurate handling by healthcare professionals are key to avoiding or mitigating adverse reactions. In addition, healthcare professionals are responsible for educating patients and their families about transfusion-related knowledge and enhancing their awareness of transfusion risks, which is an integral component of improving transfusion safety.17
Given the role of healthcare professionals in the management of blood transfusion reactions, it is imperative to understand their awareness and competency in managing ATRs. Knowledge, attitude, and practice (KAP) studies provide quantitative and qualitative data about the gaps, misconceptions, and misunderstandings about a specific subject in a specific population.18,19 KAP studies evaluate what is known (knowledge), what is believed (attitudes), and what is done (practice). KAP studies are often used to design educational activities about a specific subject. Studies in India showed good knowledge and attitudes of physicians toward ATRs but poor practice regarding their reporting,20,21 while another study showed that practice was further complicated by COVID-19.22 A study showed poor KAP toward blood transfusion in nurses in tertiary hospitals in India.23 Although a meta-analysis reported a relatively elevated rate of unnecessary transfusions in China,24 suggesting that improvements are needed in the KAP toward the indications for blood transfusion, no KAP data on ATRs are available.
Recognizing the pivotal role of healthcare professionals in transfusion safety, the aim of this study was to investigate Chinese healthcare professionals’ KAP toward ATRs.
Materials and Methods
Study Design and Participants
This nationwide cross-sectional study was conducted among healthcare professionals from 146 medical institutions across 27 provinces in China between October and December 2023. The inclusion criteria were 1) age between 18 and 80 years and 2) physicians, nurses, and transfusion specialists engaged in clinical work or medical and nursing interns. The exclusion criteria were 1) duplicate questionnaires or 2) incomplete questionnaires. The study was approved by the Medical Ethics Committee of Liaoning Cancer Hospital (KY20231023). Written informed consent was obtained from the study participants before they completed the survey.
Questionnaire
The questionnaire was designed by the investigators based on the relevant literature and guidelines.5,15,24,25 The Chinese guidelines are similar to international ones.24 After designing the questionnaire, feedback from two experts (one specialist in transfusion therapy and one in surgery) was sought and incorporated. The expert review was mainly for the content validity. The modifications were mainly made to reduce the questions on similar topics and to check the questions and answers to make sure they were related to the topic and accurate. A small-scale pilot study was conducted with 67 participants, resulting in a Cronbach’s α of 0.82, indicating acceptable internal consistency.
The final questionnaire was in Chinese and encompassed information collection across four dimensions: 14 questions on basic information, 14 on knowledge, 11 on attitude, and 30 on practice (ie, 10 for nurses, 10 for physicians, and 10 for transfusion specialists). In the knowledge dimension, a correct answer received 1 point, while an unclear or incorrect answer received 0 points. In the attitude and practice dimensions, options were scored from high (5 points) to low (1 point) on a positive-to-negative scale. Supplementary Table S1 presents the classical roles of the healthcare professionals in the transfusion process in China. In summary, physicians evaluate transfusion indications, obtain informed consent, order and assess blood products, oversee the process clinically, and manage or report any transfusion reactions. Nurses execute the transfusion procedure safely, monitor and record the patient’s condition throughout, promptly manage and report adverse reactions, and ensure post-transfusion follow-up and documentation. Transfusion service physicians perform and verify compatibility testing, authorize blood product release, investigate transfusion reactions, and monitor compliance with transfusion standards and documentation. The total score range was 0–14 for knowledge, 11–55 for attitude, and 10–50 for practice. The scores were evaluated based on Bloom’s cutoffs: scores <60% were considered poor, 60–79% were considered moderate, and ≥80% were considered good.26
Questionnaire Distribution and Quality Control
The participants were enrolled through convenience sampling. Distribution of the questionnaires was carried out via official WeChat professional groups or DingTalk professional work groups of the Liaoning Province Society of Blood Transfusion, Society of Clinical Transfusion, Chinese Medical Association, and Blood Alert Network, Chinese Academy of Medical Sciences. The online questionnaire distribution was facilitated through the use of Sojump (https://www.wjx.cn). Participants had the option to either scan the provided QR code using WeChat or follow a provided link to access and complete the questionnaire. The first page was the informed consent form; its signature was mandatory for accessing the questionnaire. All items were mandatory. The research team, composed of three physicians trained as research assistants responsible for questionnaire promotion and distribution, conducted thorough reviews of all submissions. Incomplete questionnaires, those answers using all the same option (eg, all first options), those answered within 45 seconds, and those answered in more than 480 seconds were considered invalid. A given IP address could be used to submit only one questionnaire.
Sample Size Calculation
The sample size was calculated using the formula for cross-sectional studies: α=0.05,  where Z1-α/2=1.96 when α=0.05, the assumed degree of variability of P=0.5 maximizes the required sample size, and δ is an admissible error (which was 5% here). The theoretical sample size was 480, which included an extra 20% to allow for subjects to be lost during the study.
where Z1-α/2=1.96 when α=0.05, the assumed degree of variability of P=0.5 maximizes the required sample size, and δ is an admissible error (which was 5% here). The theoretical sample size was 480, which included an extra 20% to allow for subjects to be lost during the study.
Statistical Analysis
All analyses were performed using R4.3.0. Continuous variables conforming to a normal distribution (according to the Kolmogorov–Smirnov test) were presented as means ± standard deviations (SD) and maximum and minimum values and analyzed using Student’s t-test (two categories) or ANOVA (more than two categories). Continuous variables not conforming to a normal distribution were presented as medians (interquartile ranges) and maximum and minimum values, and analyzed using the Mann–Whitney U-test (two categories) or the Kruskal–Wallis H-test (more than two categories). Categorical data were expressed as n (%) and analyzed using the chi-squared test. The correlations between KAP dimensions were determined using Spearman correlation analysis. Multivariate logistic regression analysis was used to determine the factors independently associated with knowledge and attitude. Univariate variables with P<0.05 were enrolled in the multivariate analysis. The professional titles and years of experience were considered in the analyses in a stratified manner. In the regression analyses, knowledge and attitude were dichotomized based on a cutoff of 70% of the score distribution. Multicollinearity was tested using the variance inflation factor (VIF). VIF=1: There is no correlation between the predictor variable and any of the other independent variables in the model. VIF 1–5: There is moderate correlation among the predictors. This is generally considered acceptable in most contexts. VIF >5: There is a high degree of correlation that may be problematic, leading to unreliable and unstable coefficient estimates. VIF ≥10: This indicates severe multicollinearity, which almost always requires corrective action. Two-sided P-values <0.05 were considered statistically significant.
Results
Characteristics of the Overall Participants
A total of 799 healthcare professionals participated in the study, consisting of 598 (74.84%) females and 201 (25.16%) males, with a mean age of 35.58 ± 8.27 years. The participants included 327 (40.93%) nurses, 253 (31.66%) physicians, and 219 (27.41%) transfusion specialists. Among all participants, 29.79% held a master’s degree or higher, 44.56% had an intermediate professional title, and 48.69% possessed over 10 years of work experience. Most participants (87.48%) performed blood transfusions in their clinical work, and 72.34% had previously encountered ATRs. The knowledge and attitude scores were 11.78 ± 1.78 (possible range: 0–14) and 50.43±4.74 (possible range: 11–55), respectively (Table 1). The practice scores (possible range: 0–50) were evaluated for nurses, physicians, and transfusion specialists respectively. The primary sources of knowledge regarding ATRs were books (91.49%), followed by lectures (73.47%), classroom training (68.71%), and online resources (65.21%) (Supplementary Table S2).
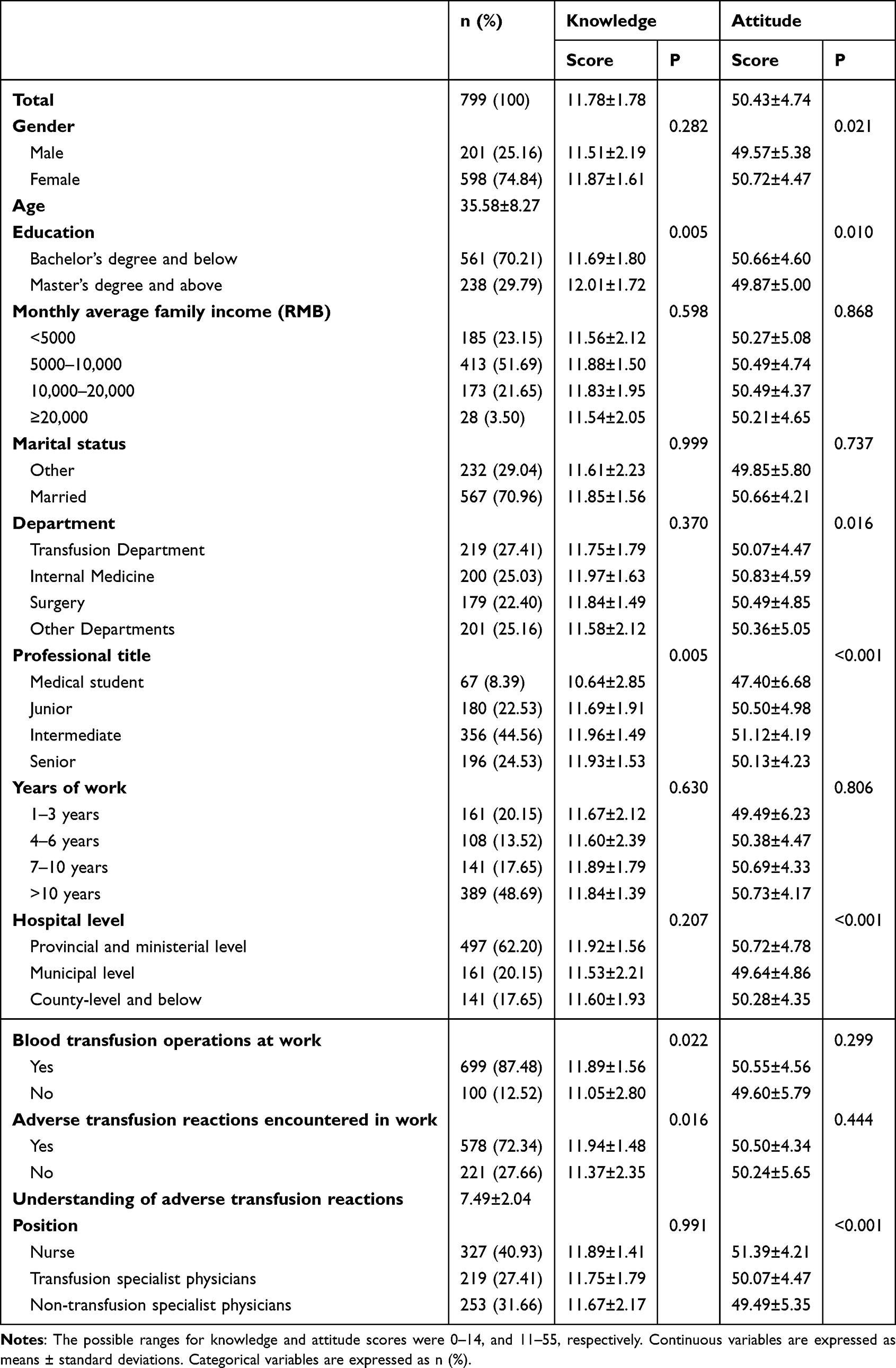 |
Table 1 Characteristics and Knowledge, Attitude of the Participants |
Several knowledge items had notably low correct response rates, aligning with the knowledge gaps identified in the discussion section. The question with the lowest correct rate was K3: “Due to stringent storage and testing regulations for clinical blood use, patients are unlikely to experience ATRs due to bacterial contamination,” with only 33.42% answering correctly. Other items with low to moderate correct rates included K10, concerning delayed hemolytic reactions, with a 34.42% correct rate; K12, regarding the classification of transfusion-transmitted diseases as ATRs, with a 39.30% correct rate; and K13, on the management of mild allergic reactions, with a 71.96% correct rate (Table 2). The attitude item with the lowest score was A2, with only 48.44% of participants agreeing or strongly agreeing with the statement: “I believe that I can prevent patients from experiencing ATRs” (Table 3).
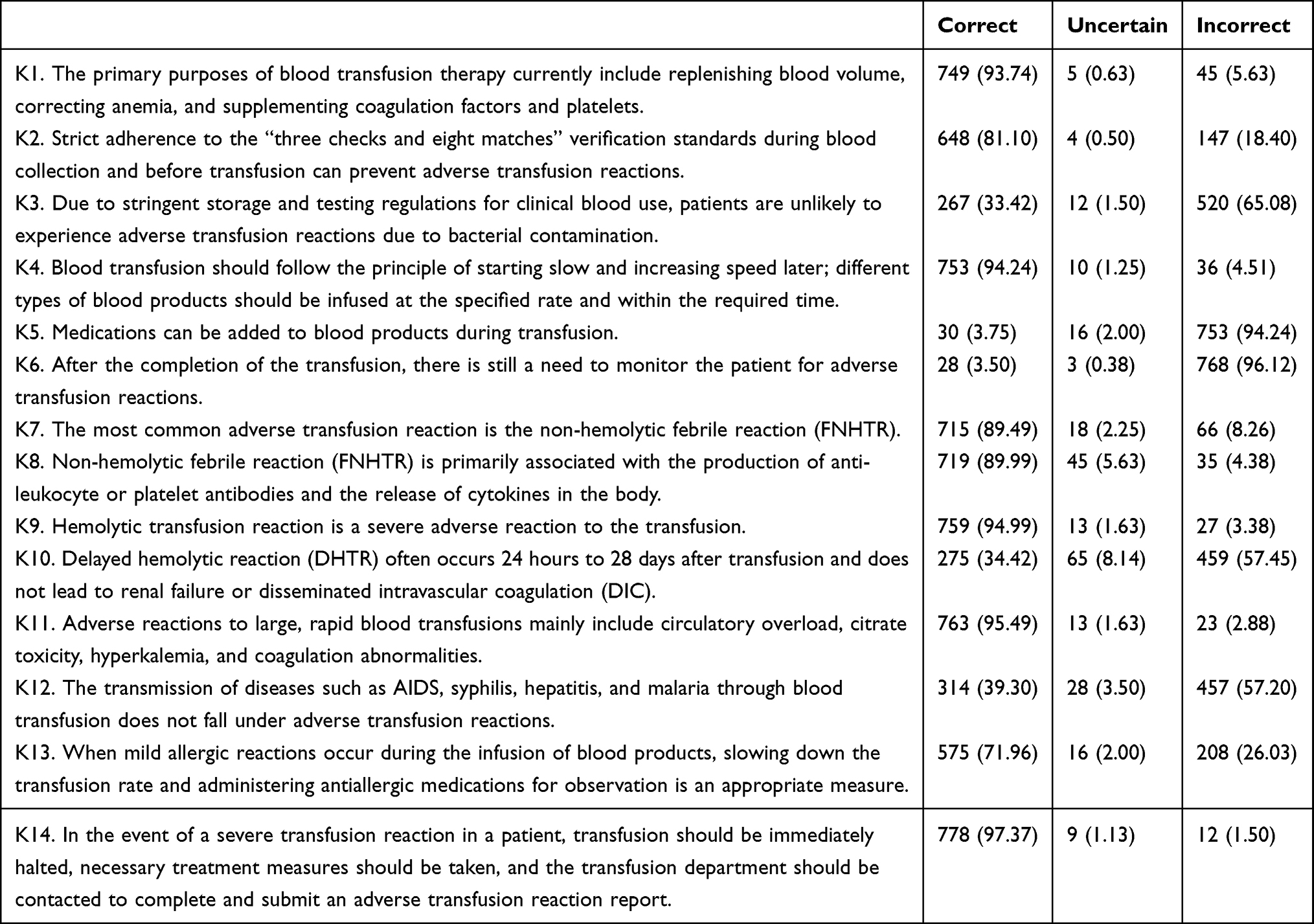 |
Table 2 Knowledge Dimension |
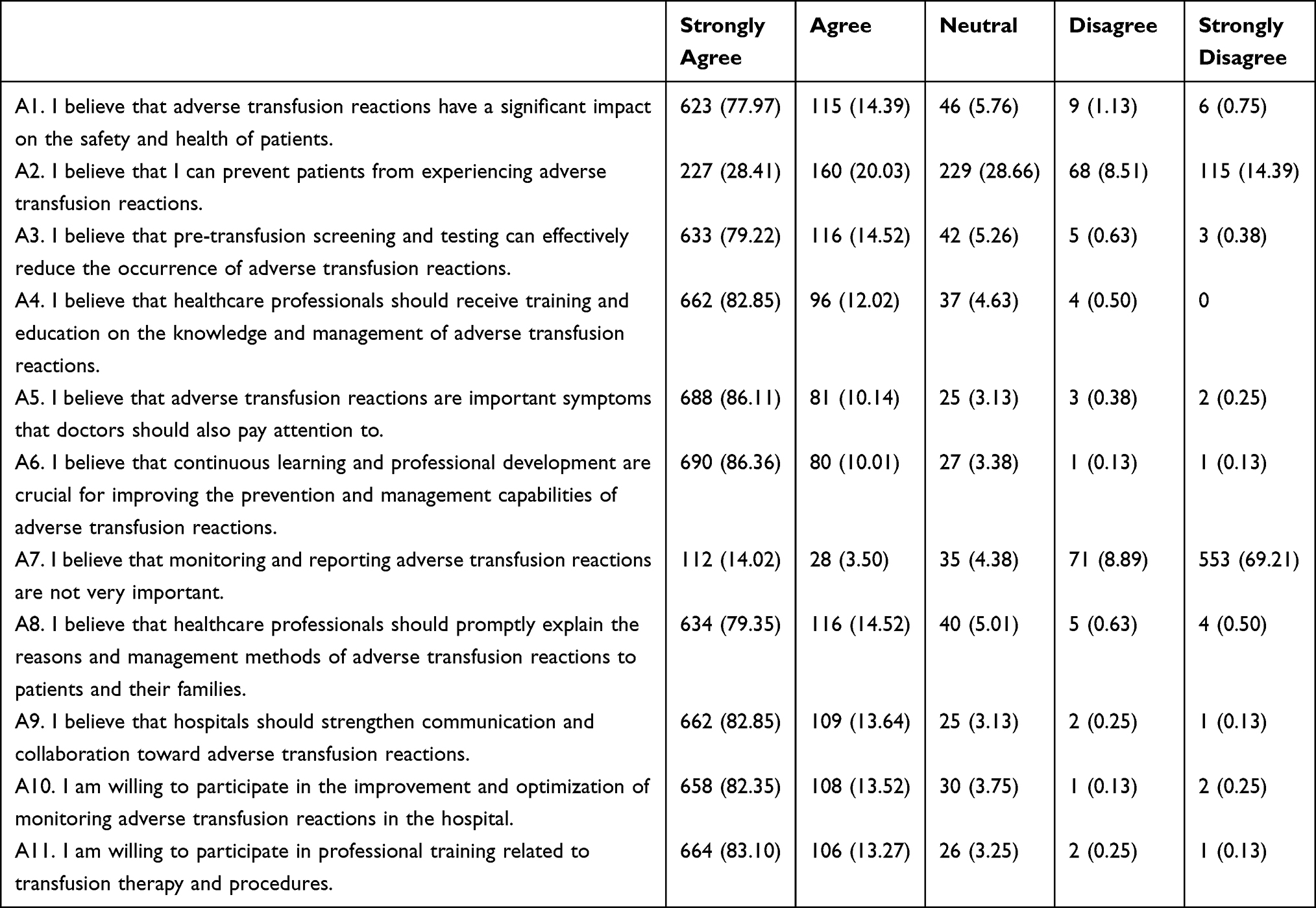 |
Table 3 Attitude Dimension |
Knowledge, Attitude, and Practice (KAP) in Nurses
Of the 327 nurses, the vast majority were female (95.41%), with a mean age of 33.54 ± 7.12 years. Most held a bachelor’s degree or below (96.64%), possessed an intermediate professional title (58.10%), and 48.62% had over 10 years of work experience. The nurses mean knowledge score was 11.89 ± 1.41, the mean attitude score was 51.39 ± 4.21, and the mean practice score was 49.22 ± 2.79 (Supplementary Table S3). The practice item with the lowest score among nurses was Pn3: “Before transfusion, I will provide education to patients or their families on transfusion speed, precautions for transfusion reaction symptoms, etc,” although it still received a high positive response rate of 99.08% (Supplementary Table S4).
Correlation analysis revealed that nurses’ knowledge scores were positively correlated with their attitude (r=0.192, P=0.001) and practice (r=0.120, P=0.030) scores. Furthermore, a strong positive correlation was observed between their attitude and practice scores (r=0.427, P<0.001) (Table 4).
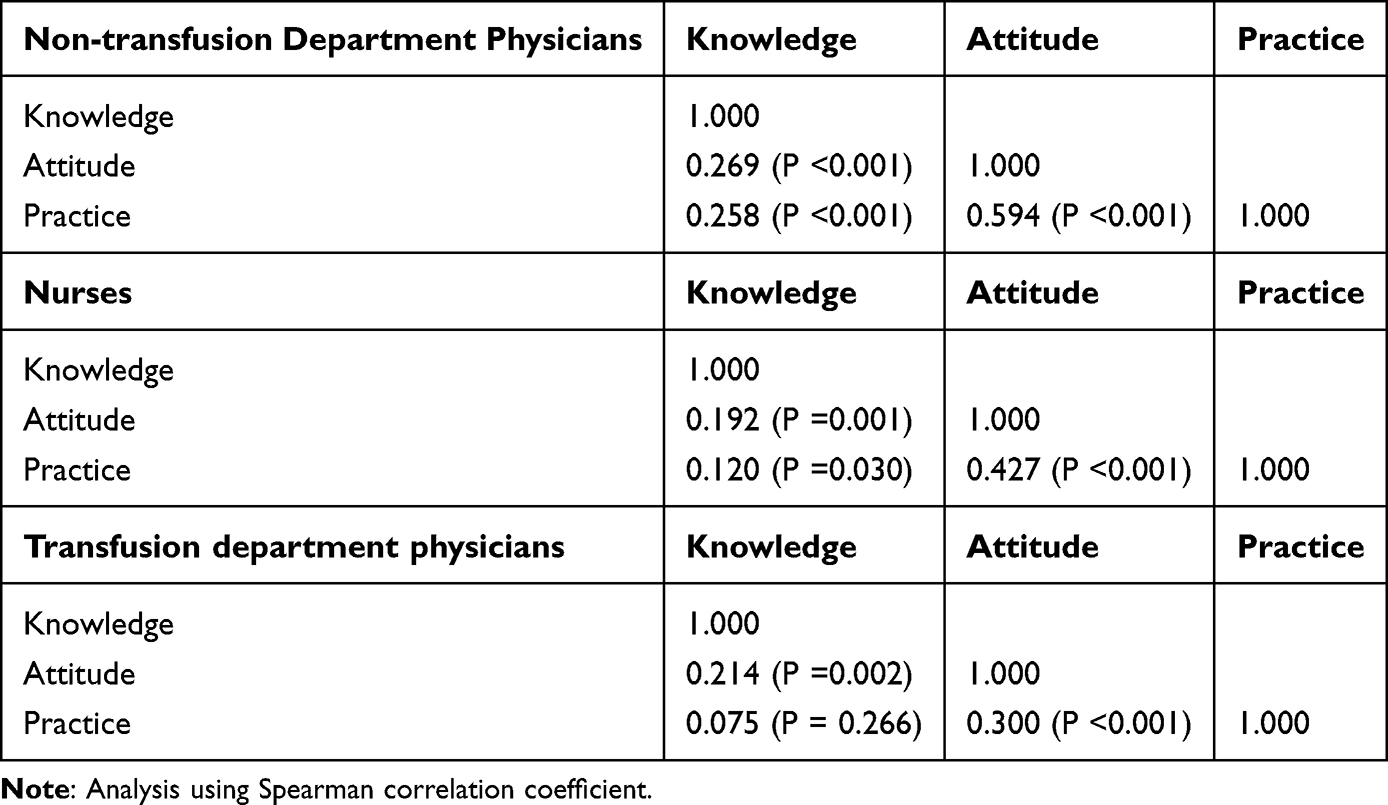 |
Table 4 Correlation Analysis |
Knowledge, Attitude, and Practice (KAP) in Physicians
Th 253 non-transfusion specialist physicians included a slight majority of females (52.96%) and had a mean age of 35.45 ± 8.63 years. Two-thirds of the physicians held a master’s degree or higher (66.80%), 38.34% had a senior professional title, and 40.32% had worked for more than 10 years. For the 253 physicians, the knowledge score was 11.67 ± 2.17, the attitude score was 49.49 ± 5.35, and the practice score was 47.60 ± 5.09 (Supplementary Table S5). The practice item with the lowest score in this group was Pnts2: “I provide clear information to patients or their families before transfusion, explaining the purpose, method, risks, and alternative treatment options,” with a 93.67% proactive response rate (Supplementary Table S6).
Correlation analysis showed that physicians’ knowledge scores were positively correlated with both attitude (r=0.269, P<0.001) and practice (r=0.258, P<0.001). A very strong positive correlation was found between their attitude and practice scores (r=0.594, P<0.001) (Table 4).
Knowledge, Attitude, and Practice (KAP) in Transfusion Specialists
The cohort of 219 transfusion specialists was predominantly female (69.41%), with a mean age of 38.78 ± 8.47 years. The majority held a bachelor’s degree or below (73.52%). The most common professional titles were intermediate (43.84%) and senior (35.16%), and over half of the participants (58.45%) had more than 10 years of work experience. For the transfusion specialists, the mean knowledge score was 11.75 ± 1.79, the mean attitude score was 50.07 ± 4.47, and the mean practice score was 44.35 ± 14.13 (Supplementary Table S7). The practice item with the lowest score was Pts7: “I will conduct post-transfusion efficacy assessments for patients, analyzing vital sign changes and other post-transfusion observations,” with a 92.00% proactive response rate (Supplementary Table S8).
Correlation analysis indicated a positive correlation between knowledge and attitude scores (r=0.214, P=0.002) and between attitude and practice scores (r=0.300, P<0.001). However, no significant correlation was found between knowledge and practice scores (P=0.266) in this group (Table 4).
Multivariable Regression Analysis
Multivariate logistic regression analysis was performed to identify factors independently associated with knowledge and attitude scores across all participants. All VIFs were <2, suggesting minimal collinearity not impeding the analyses. A goodness-of-fit analysis was performed for the regression analysis. For knowledge, the model chi-squared value was 24.054 (P=0.031), while the Hosmer-Lemeshow chi-squared value was 8.788 (P=0.361). For attitude, the model chi-squared was 34.810 (P=0.004), while the Hosmer-Lemeshow chi-squared value was 14.053 (P=0.080). The analysis revealed that holding a master’s degree or higher (OR=1.480, 95% CI: 1.079–2.027, P=0.015) was independently associated with a higher knowledge score (Table 5). Factors independently associated with a more positive attitude score included higher knowledge scores (OR=1.280, 95% CI: 1.159–1.423, P<0.001), working in the surgery department (OR=1.731, 95% CI: 1.120–2.685, P=0.014) or other departments (OR=1.763, 95% CI: 1.157–2.696, P=0.009) compared to the transfusion department, and a greater self-perceived understanding of ATRs (OR=1.122, 95% CI: 1.035–1.218, P=0.006) (Table 6).
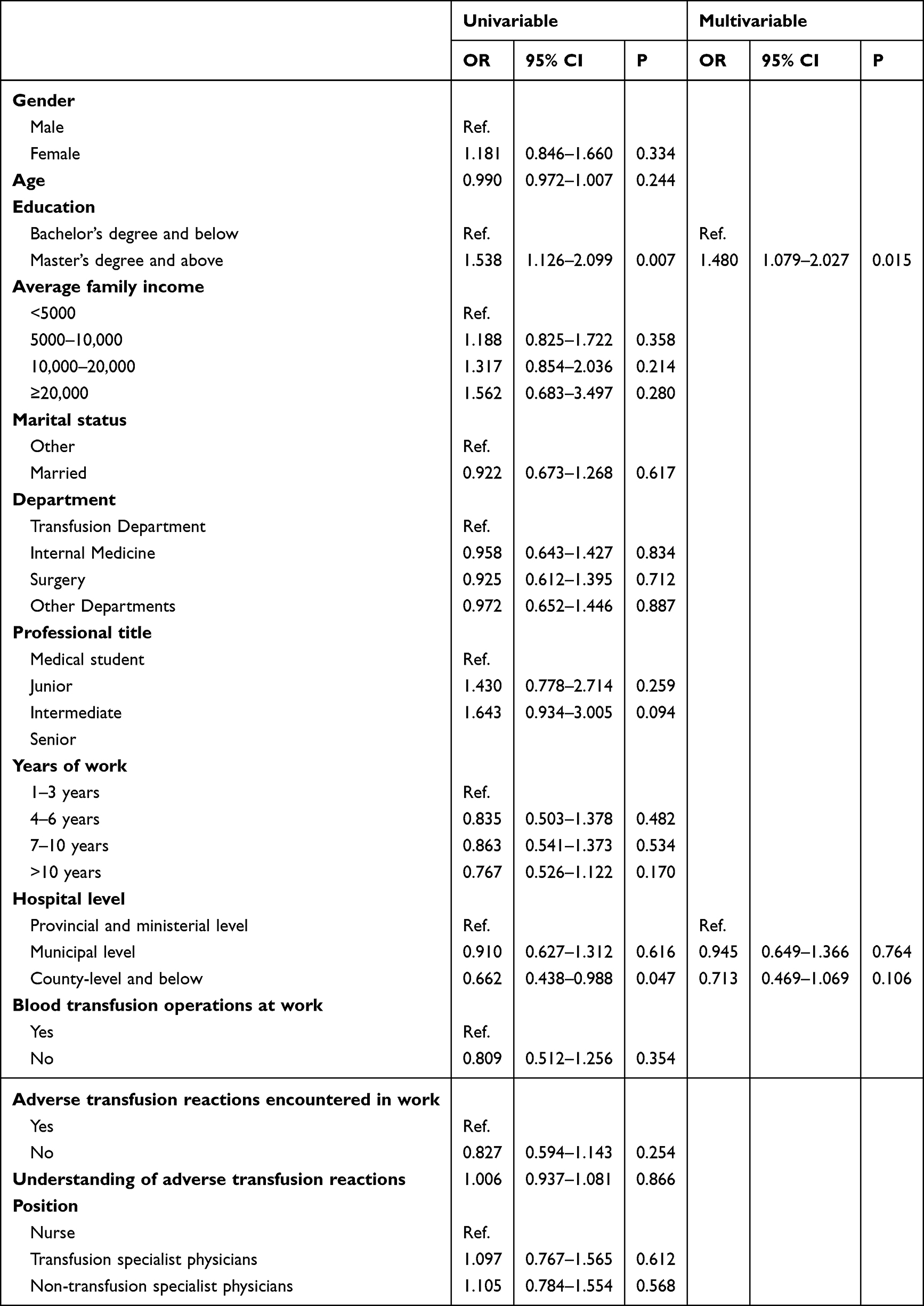 |
Table 5 Multivariable Analysis of Knowledge |
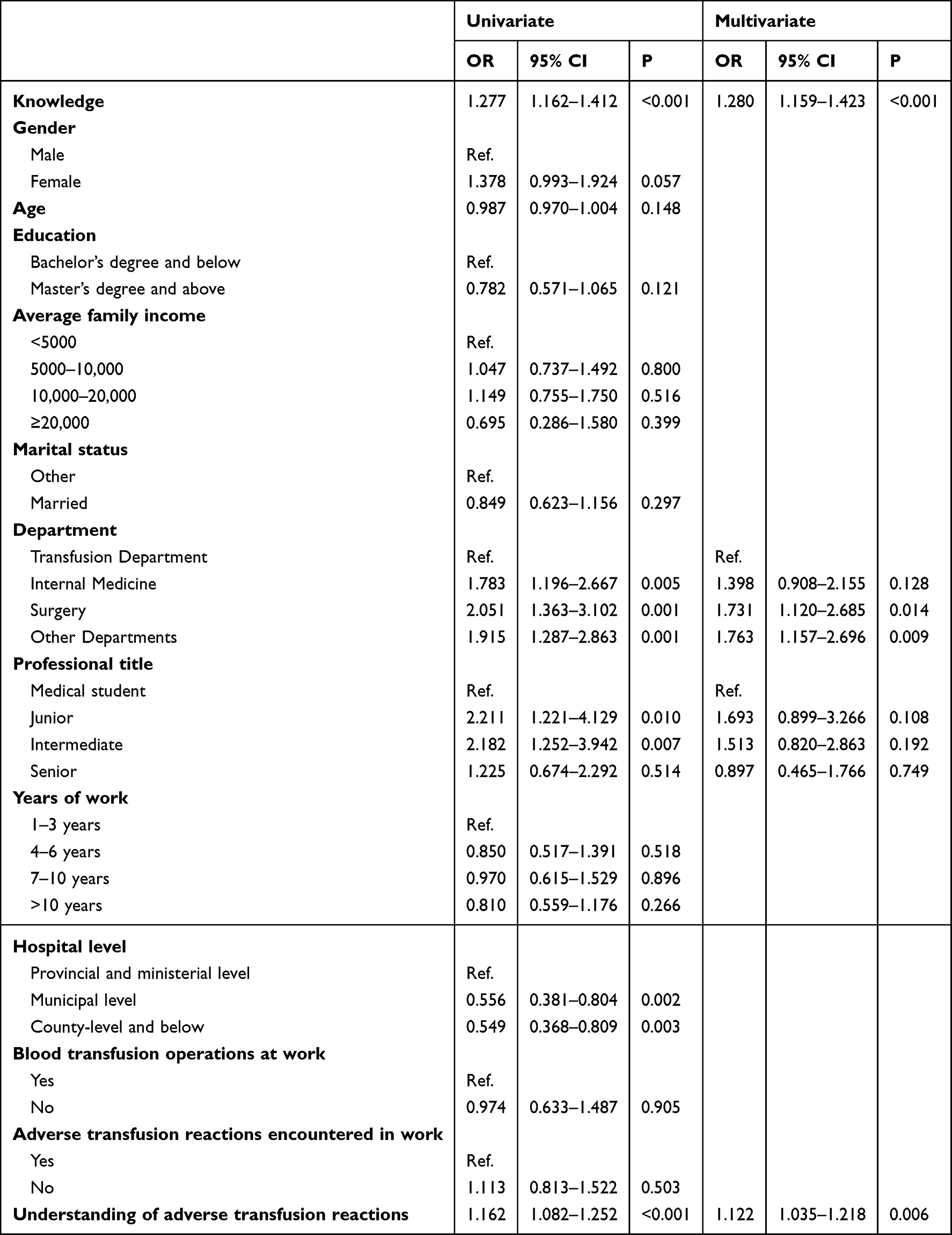 |
Table 6 Multivariate Analysis of Attitude |
Discussion
The results suggest that Chinese nurses, physicians, and transfusion specialists have sufficient knowledge, active attitudes, and practice toward ATRs. Some specific areas of knowledge remain to be improved through educational activities. The results may help identify gaps in KAP and design educational activities to correct them. Improving the KAP of healthcare professionals should translate into improved patient safety when receiving blood transfusions. This study identified key knowledge and attitude items that would warrant education and training to improve the practice of blood transfusion. The training curricula in medical faculties in the study area could be adjusted based on the results of the present study.
No previous study has specifically examined the KAP toward ATRs in China or elsewhere. However, several studies from India exploring hemovigilance and ATRs reporting found that, although the attitude toward ATRs reporting was good, knowledge was variable and practice was moderate at best.20–22,27 Chowdhary et al20 reported that in Kathua (India), healthcare professionals had good knowledge and a positive attitude toward reporting ATRs, but their practice scores were poor. Shivgunde et al27 reported that although healthcare providers in Nashik (India) had a positive attitude toward reporting ATRs, their knowledge was poor, and they almost never reported such reactions. In Nagpur, only 39% of the participants were aware of hemovigilance, 30% were aware of the existence of ATR reporting centers, and 22% were actually reporting events.21 Previous studies in India also reported that only 9–20% of their participants had attended continuous medical education about ATRs.20,27 On the other hand, in the present study, the rate of consulting educational material or attending educational activities about ATRs was high, and almost all participants used more than one method. A study of 247 residents and interns in India reported poor KAP toward safe transfusion practice;28 similar results were reported in Brazil.29 An international study reported poor knowledge of transfusion medicine among residents.30 Previous studies also reported poor knowledge of transfusion medicine, including ATRs, among practicing physicians.31–33 Haspel et al34 proposed a framework for the proper training of physicians in transfusion medicine. In the present study, Chinese nurses, physicians, and transfusion specialists all showed high KAP scores toward ATRs. Discrepancies among studies and the different parts of the world could be related to the work experience of the participants, national guidelines and policies toward transfusion medicine, training curriculum, and the availability and content of continuous medical education.
A study by Mitchell et al in 1989 in Iowa35 reported among faculty members, transfusion medicine medical directors, and transfusion chief technologists, the most common knowledge deficits were related to the selection and use of blood components, transfusion reactions, coagulation, blood products to treat hemostatic problems, and apheresis. In the present study, moderate knowledge scores were observed regarding the possibility of bacterial contamination of blood products, delayed hemolytic reaction, the definition of ATR pertaining to the transmission of blood-borne diseases, and the management of allergic reactions to blood products. Those points should be emphasized in future educational materials and activities.
In the present study, only higher education was independently associated with higher knowledge scores. The finding that working in surgery or other clinical departments was associated with a more positive attitude compared to professionals in the Transfusion Department is noteworthy. This highlights a potential “exposure effect” that may be linked to the nature of professional roles. Although transfusion specialists have the most in-depth technical expertise, healthcare professionals in high-transfusion clinical settings, like surgery, are on the front line, directly witnessing the immediate impact of transfusions and their complications on patients. This routine exposure may foster a greater appreciation for the importance of vigilance and proper management of ATRs, thereby shaping a more proactive attitude compared to those in departments with less transfusion activity. This suggests that familiarity and practical experience are key determinants of professional attitude in this context. The KAP dimensions were generally correlated with each other, as supported by the KAP theory, which states that knowledge is the basis for practice, while attitude is the force driving practice.18,19 In transfusion specialists, knowledge did not correlate to practice, but knowledge correlated to attitude, which correlated to practice. Nevertheless, considering that the KAP scores were all skewed toward the higher ranges, correlation analyses should be taken with caution.
This study has limitations. Although it was open to nurses, physicians, and transfusion specialists across all of China, some provinces were underrepresented. In addition, the relatively short study period probably led to the small sample size (relative to the number of healthcare providers in China). Since the QR code for participation was distributed through social media, it is impossible to determine how many people saw the QR code but did not complete the questionnaire, preventing the calculation of metrics like the response rate. From a statistical perspective, while the total sample size of 799 is robust for overall analysis, the subgroup sizes for nurses (n=327), physicians (n=253), and transfusion specialists (n=219) may limit the power to draw definitive conclusions that are generalizable to each of these distinct professions across the entirety of China. A larger, nationally stratified sample would be necessary to fully represent the heterogeneity within each group of Chinese healthcare workers and strengthen the external validity of the subgroup-specific findings. Because of the different nature of their work, different practice questions had to be designed for nurses, physicians, and transfusion specialists, therefore the practice scores could not be compared among the three professions. The present study was cross-sectional, and the changes in KAP were not evaluated. Nevertheless, the results could eventually be used as a historical baseline to evaluate the effectiveness of an educational intervention. Due to the design of the knowledge items, there is a possibility of overestimating the knowledge scores. Finally, all KAP studies are at risk of social desirability bias. With such bias participants can be tempted to answer what they believe they should think or do instead of what they are really thinking or doing.36,37 Considering that the knowledge scores were high and that the attitude and practice scores were also high, bias is a real possibility. Because participants were recruited from transfusion societies, there may have been an overestimation of the KAP level. Finally, the two experts consulted for questionnaire content validity included one specialist in transfusion therapy and one in surgery. The expert in surgery was consulted because transfusion is a common event in the perioperative period. Nevertheless, the lack of experts from other specialties is a limitation.
Conclusion
The cross-sectional survey results indicate that participating Chinese nurses, physicians, and transfusion specialists self-reported high levels of knowledge, positive attitudes, and appropriate practices regarding ATRs. Despite the high overall scores, specific, critical knowledge gaps related to bacterial contamination, delayed hemolytic reactions, and the classification of transfusion-transmitted diseases were identified. Future training initiatives should address these deficiencies to ensure that positive attitudes reported by healthcare professionals translate into consistently safe and effective transfusion practices. These results could provide valuable evidence to guide the refinement of national transfusion education programs and clinical protocols, supporting the continuous improvement of transfusion safety across healthcare settings in China.
Data Sharing Statement
All data generated or analyzed during this study are included in this published article and its Supplementary Information Files.
Ethics Approval and Consent to Participate
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. The study was approved by the Medical Ethics Committee of Liaoning Cancer Hospital (KY20231023). Written informed consent was obtained from the study participants before they completed the survey.
Funding
There is no funding to report.
Disclosure
The authors declare that they have no competing interests for this work.
References
1. Lotterman S, Sharma S. Blood Transfusion. StatPearls. Treasure Island (FL) ineligible companies. Disclosure: Sandeep Sharma declares no relevant financial relationships with ineligible companies; 2024.
2. Bowman Z, Fei N, Ahn J, et al. Single versus double-unit transfusion: safety and efficacy for patients with hematologic malignancies. Eur J Haematol. 2019;102(5):383–13. doi:10.1111/ejh.13211
3. D’Alessandro A. From omics technologies to personalized transfusion medicine. Expert Rev Proteomics. 2019;16(3):215–225. doi:10.1080/14789450.2019.1571917
4. Yoshida T, Prudent M, D’Alessandro A. Red blood cell storage lesion: causes and potential clinical consequences. Blood Transfus. 2019;17(1):27–52.
5. Carson JL, Guyatt G, Heddle NM, et al. Clinical practice guidelines from the AABB: red blood cell transfusion thresholds and storage. JAMA. 2016;316(19):2025–2035. doi:10.1001/jama.2016.9185
6. Delaney M, Wendel S, Bercovitz RS, et al. Transfusion reactions: prevention, diagnosis, and treatment. Lancet. 2016;388(10061):2825–2836. doi:10.1016/S0140-6736(15)01313-6
7. Negi G, Gaur DS, Kaur R. Blood transfusion safety: a study of adverse reactions at the blood bank of a tertiary care center. Adv Biomed Res. 2015;4(1):237. doi:10.4103/2277-9175.168604
8. Jaworski K, Maslanka K, Kosior DA. Transfusion-related acute lung injury: a dangerous and underdiagnosed noncardiogenic pulmonary edema. Cardiol J. 2013;20(4):337–344. doi:10.5603/CJ.2013.0091
9. Sahu S, Hemlata, Verma A. Adverse events related to blood transfusion. Indian J Anaesth. 2014;58(5):543–551. doi:10.4103/0019-5049.144650
10. Tung JP, Fraser JF, Nataatmadja M, et al. Age of blood and recipient factors determine the severity of transfusion-related acute lung injury (TRALI). Crit Care. 2012;16(1):R19. doi:10.1186/cc11178
11. Simmonds P. The origin of hepatitis C virus. Curr Top Microbiol Immunol. 2013;369:1–15. doi:10.1007/978-3-642-27340-7_1
12. Yin Y, Tian X, Li L, et al. First annual report of Chinese haemovigilance network. Vox Sang. 2021;116(6):718–724. doi:10.1111/vox.13059
13. Tian X, Kong Y, Wang J, He R, Li L, Liu Z. Development of the Chinese Haemovigilance Network and reporting of adverse transfusion reactions from 2018 to 2020. Vox Sang. 2022;117(8):1027–1034. doi:10.1111/vox.13291
14. Chen Q-F, Li P, Wang X-Q. Clinical analysis of 159 times acute transfusion reaction in single center. Blood. 2009;114(22):4196. doi:10.1182/blood.V114.22.4196.4196
15. Soutar R, McSporran W, Tomlinson T, Booth C, Grey S. Guideline on the investigation and management of acute transfusion reactions. Br J Haematol. 2023;201(5):832–844. doi:10.1111/bjh.18789
16. Ackfeld T, Schmutz T, Guechi Y, Le Terrier C. Blood transfusion reactions-a comprehensive review of the literature including a swiss perspective. J Clin Med. 2022;11(10):2859. doi:10.3390/jcm11102859
17. Bielby L, Stevenson L, Wood E. The role of the transfusion nurse in the hospital and blood centre. ISBT Sci Ser. 2011;6(2):270–276. doi:10.1111/j.1751-2824.2011.01537.x
18. Andrade C, Menon V, Ameen S, Kumar Praharaj S. Designing and conducting knowledge, attitude, and practice surveys in psychiatry: practical guidance. Indian J Psychol Med. 2020;42(5):478–481. doi:10.1177/0253717620946111
19. World Health Organization. Advocacy, communication and social mobilization for TB control: a guide to developing knowledge, attitude and practice surveys; 2008. Available from: http://whqlibdoc.who.int/publications/2008/9789241596176_eng.pdf.
20. Chowdhary R, Khajuria V, Sawhney V. Knowledge, attitude, and practice of reporting transfusion reactions in hemovigilance among health-care professionals in a tertiary care teaching hospital of northern India. Natl J Physiol Pharm Pharmacol. 2020;10(11):970–975.
21. Date AP, Date AA, Dashputra AV, Norkar AS. Knowledge attitude and practice of haemovigilance among doctors in tertiary care hospital in Nagpur, Maharashtra, India. Intl J Basic Clin Pharmacol. 2016;5(3):788–793. doi:10.18203/2319-2003.ijbcp20161520
22. Khatiwada B, Chaurasia R, Patidar GK, Pandey HC. Assessment of transfusion practices among doctors during COVID-19 pandemic using questionnaire-based survey. Indian J Hematol Blood Transfus. 2023;39(3):470–477. doi:10.1007/s12288-022-01613-2
23. Panchawagh SJ, Melinkeri S, Panchawagh MJ. Assessment of knowledge and practice of blood transfusion among nurses in a tertiary care hospital in India. Indian J Hematol Blood Transfus. 2020;36(2):393–398. doi:10.1007/s12288-019-01244-0
24. Kong Y, Wang X, Yin Y, et al. Appropriateness of red blood cell use in China in the last thirteen years: a systematic review. Heliyon. 2019;5(3):e01408. doi:10.1016/j.heliyon.2019.e01408
25. Kaliyaperumal K. Guideline for conducting a knowledge, attitude and practice. AECS Illuminat. 2004;4:7–9.
26. Bloom BS. Learning for mastery. Instruction and curriculum. regional education laboratory for the carolinas and virginia, topical papers and reprints, number 1. Eval Comment. 1968;1(2):n2.
27. Shivgunde PP, Besekar SM, Bhojwani KM, Bhojwani DG. Knowledge, attitude and practice of haemovigilance amongst healthcare professionals in Nashik, Maharashtra. India Intl J Basic Clin Pharmacol. 2018;7(5):986–991. doi:10.18203/2319-2003.ijbcp20181647
28. Ray GK, Mukherjee S, Routray SS, et al. Knowledge, attitudes and practices of resident doctors and interns on safe blood transfusion practices: a survey-based study. Hematol Transfus Cell Ther. 2023;45(3):342–349. doi:10.1016/j.htct.2022.06.004
29. Vaena MMV, Alves LA. Assessment of the knowledge and perceptions of Brazilian medical residents on transfusion medicine. Hematol Transfus Cell Ther. 2019;41(1):37–43. doi:10.1016/j.htct.2018.06.002
30. Haspel RL, Lin Y, Mallick R, et al. Internal medicine resident knowledge of transfusion medicine: results from the BEST-TEST international education needs assessment. Transfusion. 2015;55(6):1355–1361. doi:10.1111/trf.12968
31. Gharehbaghian A, Javadzadeh Shahshahani H, Attar M, Rahbari Bonab M, Mehran M, Tabrizi Namini M. Assessment of physicians knowledge in transfusion medicine, Iran, 2007. Transfus Med. 2009;19(3):132–138. doi:10.1111/j.1365-3148.2009.00923.x
32. Milligan C, Higginson I, Smith JE. Emergency department staff knowledge of massive transfusion for trauma: the need for an evidence based protocol. Emerg Med J. 2011;28(10):870–872. doi:10.1136/emj.2009.088138
33. Rock G, Berger R, Pinkerton P, Fernandes B. A pilot study to assess physician knowledge in transfusion medicine. Transfus Med. 2002;12(2):125–128. doi:10.1046/j.1365-3148.2002.00363.x
34. Lin Y, Haspel RL. Transfusion medicine education for non-transfusion medicine physicians: a structured review. Vox Sang. 2017;112(2):97–104. doi:10.1111/vox.12499
35. Mitchell SA, Strauss RG, Albanese MA, Case DE. A survey to identify deficiencies in transfusion medicine education. Acad Med. 1989;64(4):217–219. doi:10.1097/00001888-198904000-00011
36. Bergen N, Labonte R. “Everything Is Perfect, and We Have No Problems”: detecting and limiting social desirability bias in qualitative research. Qual Health Res. 2020;30(5):783–792. doi:10.1177/1049732319889354
37. Latkin CA, Edwards C, Davey-Rothwell MA, Tobin KE. The relationship between social desirability bias and self-reports of health, substance use, and social network factors among urban substance users in Baltimore, Maryland. Addict Behav. 2017;73:133–136. doi:10.1016/j.addbeh.2017.05.005
 © 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2026 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.