Back to Journals » International Journal of General Medicine » Volume 16
Knowledge, Attitude and Practice of Patients with Gestational Diabetes Mellitus Regarding Gestational Diabetes Mellitus: A Cross-Sectional Study
Authors Tan J, Chen L, Wu Y, Zhu X, Fei H ![]()
Received 30 May 2023
Accepted for publication 15 September 2023
Published 26 September 2023 Volume 2023:16 Pages 4365—4376
DOI https://doi.org/10.2147/IJGM.S423565
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Jie Tan,1 Lumeng Chen,2 Yingying Wu,2 Xuhong Zhu,3 Huali Fei4
1Department of Nutrition, Hangzhou Women’s Hospital, Hangzhou, People’s Republic of China; 2Department of Outpatient, Hangzhou Women’s Hospital, Hangzhou, People’s Republic of China; 3Department of Ministry of Women’s Health, Hangzhou Women’s Hospital, Hangzhou, People’s Republic of China; 4Department of Reproduction and Family Planning, Hangzhou Women’s Hospital, Hangzhou, People’s Republic of China
Correspondence: Lumeng Chen, Department of Outpatient, Hangzhou Women’s Hospital, Hangzhou, People’s Republic of China, Tel +86-18258170364, Email [email protected]
Introduction: Self-monitoring of blood glucose levels and changes in diet and lifestyle play important roles in the management of gestational diabetes mellitus (GDM).
Methods: This cross-sectional study enrolled patients with GDM at Hangzhou Women’s Hospital, China, between September 1, 2022, and October 26, 2022. A questionnaire was designed that included the following dimensions: demographic/clinical information, knowledge, attitude and practice. Correlations between knowledge, attitude and practice scores were evaluated using Spearman correlation analysis. Factors associated with practice score ≥ 14/16 were identified using multivariate logistic regression.
Results: The analysis included 499 women with GDM and a mean age of 31.22± 3.89 years. The average knowledge, attitude and practice score were 11.55± 3.04, 34.23± 4.06 and 10.7± 2.87 points, respectively. Knowledge score was positively correlated with attitude score (r=0.318, P< 0.001) and practice score (r=0.351, P< 0.001); attitude and practice scores were also positively correlated (r=0.209, P< 0.001). Multivariate analysis identified higher knowledge score (odds ratio [OR], 1.138; 95% confidence interval [95% CI], 1.042– 1.244; P=0.004) and higher attitude score (OR, 1.137; 95% CI, 1.060– 1.219; P< 0.001) as independently associated with good practice (ie, practice score ≥ 14 points).
Conclusion: The results provide important insights into the knowledge, attitudes and practices of women with GDM in China regarding GDM and its management. These findings may facilitate the development and implementation of education and training programs to improve the self-management of GDM by women in China.
Keywords: diabetes mellitus, gestational, blood glucose self-monitoring, health-related behavior, diet modification, surveys and questionnaires
Introduction
Abnormal glucose tolerance that has an onset or is first recognized during pregnancy is known as gestational diabetes mellitus (GDM).1 Although the precise diagnostic definition of GDM varies somewhat between different organizations and countries, GDM is usually recognized at 24–28 weeks of gestation as an elevated blood glucose level and/or an abnormal result in an oral glucose tolerance test (OGTT).1 The standardized prevalence of GDM is 14% worldwide and varies between geographic regions from 7.1% in North America to 27.6% in the Middle East and North Africa,2 while the pooled prevalence in 24 European countries was 10.9%.3 The pooled prevalence of GDM in mainland China was reported to be 14.8% but was as high as 26.7% in older pregnant women.4 Furthermore, GDM prevalence varied between different regions of China, with the highest prevalence of 24.2% in Tongzhou, Beijing.5 Risk factors for GDM include advanced maternal age, overweight/obesity, family history of type 2 diabetes mellitus (T2DM) and a previous (first) pregnancy without GDM that was complicated by hypertensive disorders, perinatal mortality, maternal obesity or fetal macrosomia.4,6,7 GDM is associated with adverse outcomes such as increased risks of maternal pre-eclampsia/eclampsia, maternal cardiovascular disease, maternal T2DM, fetal macrosomia, preterm delivery, caesarian section, birth trauma, infant born large for gestational age, infant respiratory distress syndrome, cardiac malformations in neonate, and admission of neonate to intensive care unit.6,8,9 GDM is also associated with an elevated long-term risk of obesity, T2DM and cardiovascular disease in children.6 Thus, it is important that GDM is diagnosed and treated in a timely manner.
The management of GDM requires a multidisciplinary approach and includes both non-pharmacologic and pharmacologic interventions.10 The majority of patients with GDM can be managed with daily self-monitoring of fasting and postprandial blood glucose levels, dietary modifications and monitoring of nutrition, exercise and physical activity, maternal weight gain management, and other lifestyle modifications,11 and programs to facilitate the implementation of these interventions have been set up in China.12,13 In addition, up to 30% of patients with GDM require pharmacotherapy with insulin or oral hypoglycemic agents such as metformin or glibenclamide.11 The above management strategies place a great deal of responsibility on the patient since they require self-monitoring of blood glucose (SMBG), dietary and lifestyle modifications to limit weight gain, and in some cases the self-administration of drugs such as subcutaneous injection of insulin. Adherence to the recommended management strategy is essential for the maximum benefits to be obtained. Despite the abundance of published studies discussing self-efficacy in women with GDM, the number of implemented measures that could significantly improve self-management practice is still limited.14,15 Moreover, modifiable risk factors for GDM differ according to region and lifestyle,3,5 suggesting the need to discuss specific barriers for adherence to nutrition- and exercise-based interventions among women in Asia.
Identifying barriers that reduce adherence to healthy behaviors is important because this can facilitate the design and implementation of interventions to improve the self-management of GDM. Knowledge, attitude and practice (KAP) surveys provide useful information regarding baseline knowledge, attitudes, beliefs, misconceptions and behaviors towards a health-related topic.16 Furthermore, the data provided by KAP surveys can facilitate the development and implementation of education/training programs to overcome issues and barriers that hinder the management of patients with a health problem.16 Therefore, this study aims to evaluate the knowledge, attitudes and practices of GDM management among patients with GDM.
Materials and Methods
Study Design and Subjects
This cross-sectional study enrolled patients with GDM at Hangzhou Women’s Hospital, Hangzhou, China, between September 1, 2022, and October 26, 2022. The inclusion criteria were as follows: 1) aged >18 years-old; 2) received OGTT screening during the second trimester (at 24–28 weeks of gestation) and was diagnosed with GDM: fasting, 1 hr after oral glucose and 2 hr after oral glucose with blood glucose thresholds of 5.1, 10.0 and 8.5 mmol/L, respectively;10 3) treated in the Nutritional Clinic and 4) fully understood the study objective and provided informed consent for participation. The exclusion criteria were as follows: 1) hypertension, renal disease, cardiac disease or other severe complications and 2) multiple pregnancies. This study was approved by the Ethics Committee of Hangzhou Women’s Hospital (ethics approval number: 2022K0807), and all participants provided informed written consent.
Design and Distribution of the Questionnaire
The questionnaire was designed according to a questionnaire validated in a previous study.17 The first draft of the questionnaire was modified by one expert in the management of GDM, and the finalized questionnaire was administered to 20 patients with GDM as a pretest. Analysis of the pretest results indicated that the questionnaire had good-to-excellent reliability (a Cronbach’s α value of 0.890, suggesting good internal consistency). Analysis of all the data also indicated that the questionnaire had good-to-excellent reliability (a Cronbach’s α value of 0.837). The result of the confirmatory factor is shown in Supplementary Figure 1 ((CFI = 0.813 (>0.800); IFI = 0.815 (>0.800); RMSEA = 0.057 (<0.080); CMIN/DF = 2.625 (> 1: 1–3 excellent, 3–5 good)), indicating that the questionnaire has good reliability and validity.
The final version of the questionnaire was in Chinese and consisted of four dimensions: demographic/clinical information, knowledge, attitude and practice (Supplemental Material). The demographic/clinical characteristics collected by the questionnaire included age, body mass index (BMI), education level, occupation, gravidity, parity, method of conception, family history of T2DM, history of macrosomia, history of polycystic ovary syndrome (POS) and gestational week. The knowledge dimension consisted of 18 questions (K1–K18), each of which was scored either 1 point for a correct answer (for multiple response questions, 1 point was awarded only if all the correct responses were selected) or 0 points for an incorrect answer or selecting “unclear.” The total score for the knowledge dimension ranged from 0 to 18 points. The attitude dimension consisted of eight questions (A1–A8), which were scored using a 5-point Likert scale (“strongly agree” = 5 points, “strongly disagree” = 1 point). “Strongly agree” and “agree” were considered positive responses, while “neutral”, “disagree” and “strongly disagree” were considered negative responses. The total score for the attitude dimension ranged from 8 to 40 points. The practice dimension consisted of 10 questions (P1–P10). Six items in the practice dimension (P1–P5 and P7) were scored on a scale of 0–2 (“often” = 2 points, “occasionally” = 1 point and “never” = 0 points), and the remaining four items (P6, P8–P10) were each scored 1 point for “yes” and 0 points for “no.” The total score for the practice dimension ranged from 0 to 16 points. The SoJump platform provided by WeChat messenger (Tencent, Shenzhen, China) was used to prepare the online questionnaire; all eligible individuals, willing to participate, were asked to scan QR code and fill in the questionnaire after receiving the explanation and signing the informed consent form.
Statistical Analysis
The SPSS 26.0 software (IBM Corp., Armonk, NY, USA) was used for statistical analysis. Continuous variables were tested for a normal distribution using the Kolmogorov–Smirnov test. Normally distributed continuous variables are presented as the mean ± standard deviation (SD) and were compared between groups using Student’s t-test (two groups) or analysis of variance (three or more groups). Non-normally distributed continuous variables are described as median (range) and were compared between groups using the Mann–Whitney U-test (two groups) or Kruskal–Wallis test (three or more groups). Correlations between continuous variables were evaluated using Spearman correlation analysis. Categorical variables are expressed as n (%). Practices were categorized according to the 87.5% scores, with a score of 14 points or above considered to indicate “good practice.” Factors associated with good practice were identified using univariate and multivariate logistic regression analyses. Variables with P < 0.05 in the univariate analysis were included in the multivariate analysis. Odds ratios (ORs) and 95% confidence intervals (95% CIs) were calculated. A two-sided P-value of less than 0.05 was considered statistically significant.
Results
Demographic and Clinical Characteristics of the Study Participants
A total of 502 questionnaires were collected, and 3 were excluded due to logical errors. The final analysis included completed questionnaires from 499 women with GDM. The demographic and clinical characteristics of the study participants are summarized in Table 1. The mean gestational week of participants was 28.74±4.34. With a mean age of 31.22±3.89 years, nearly half of the respondents (232/499, 46.9%) were aged ≤30 years-old, with only 60 participants (12.02%) aged ≥36 years-old. Most of the respondents (323/499 64.73%) had a BMI of 18.5–23.9 kg/m2, although a quarter of the participants had a BMI ≥24 kg/m2. The vast majority of women (443/499, 88.78%) were educated at junior college level or higher. Approximately half the respondents (245/499, 49.10%) had a gravidity of 1, and the majority (306/499, 61.32%) had a parity of 0. Most of the participants (475/499, 95.19%) had conceived naturally, and the majority of the women did not have POS (451/499, 90.38%), a family history of T2DM (390/499, 78.16%), or a history of macrosomia (487/499, 97.60%).
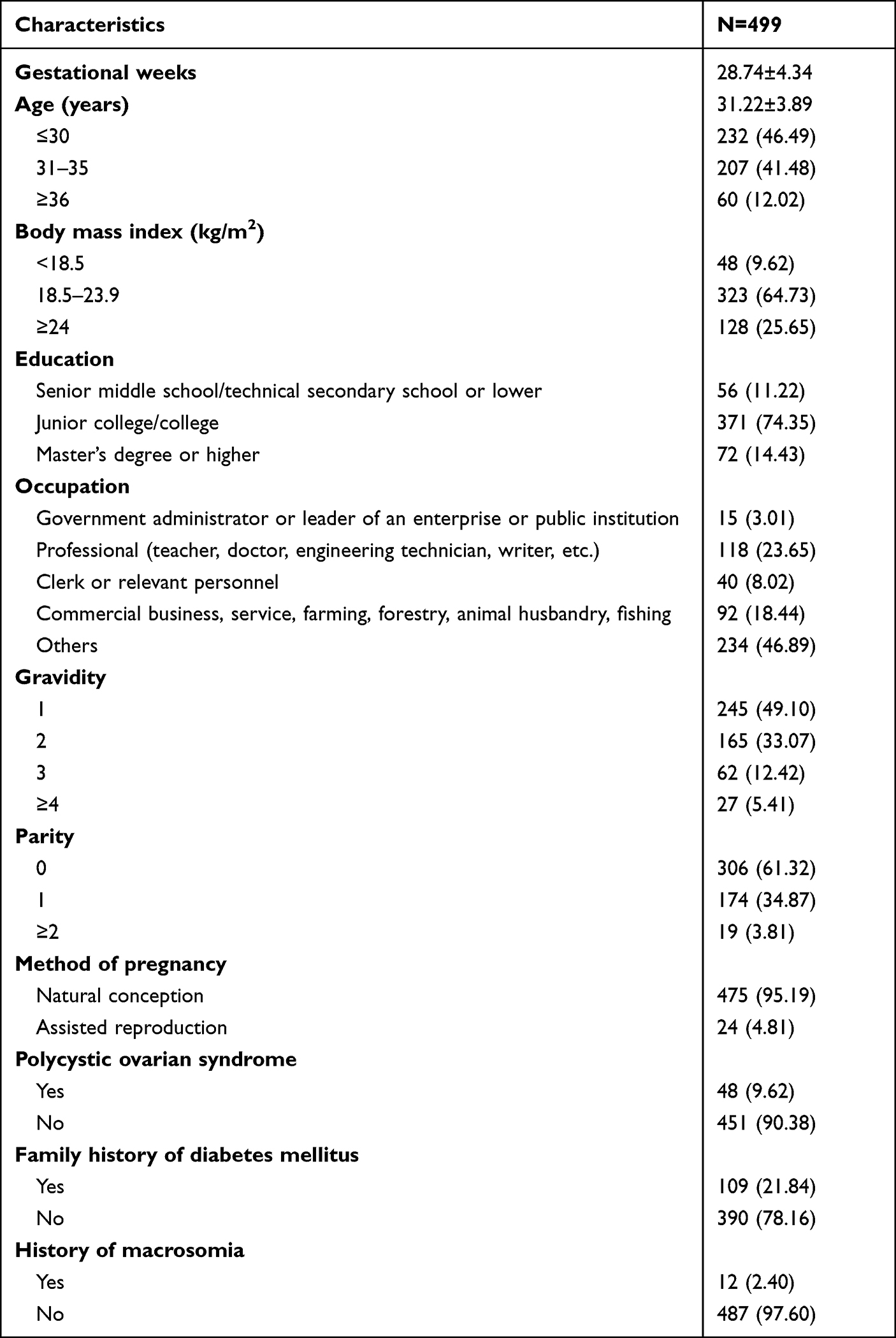 |
Table 1 Demographic/Clinical Characteristics of the Women with Gestational Diabetes Mellitus |
Knowledge Score
The mean knowledge score was 11.55 ± 3.04 points (possible range, 0–18 points), suggesting that the surveyed women had a moderate level of knowledge about GDM (Table 2). The proportion of respondents giving correct answers to each of the 18 questions in the knowledge dimension ranged from 15.03% to 99.60% (Table 3). Seven of the 18 questions (items K9–K11, K14, K15, K17 and K18) were answered correctly by more than 90% of the respondents, one question was answered correctly by more than 75% of the respondents (item K2), while further four questions (items K3, K4, K12 and K13) were answered correctly by more than 60% of respondents. However, only 36.67% of the study participants knew the correct definition of GDM (item K1), and only 15.03% of the women could identify factors associated with an increased risk of GDM (item K5). Furthermore, less than 35% of the participants were aware of the maternal, fetal and neonatal effects of maternal hyperglycemia (items K16–K8). Additionally, only 26.25% of the women were aware of the importance of controlling daily total nutritional intake (item K16).
 |
Table 2 Questionnaire Scores Stratified According to the Demographic/Clinical Characteristics of the Women with Gestational Diabetes Mellitus |
 |
Table 3 Rates of Correct Answers to Questions in the Knowledge Dimension |
The knowledge score did not differ significantly between groups stratified according to age, occupation, gravidity, parity, method of conception, history of POS, family history of T2DM or history of macrosomia (Table 2). However, the knowledge score was significantly higher in women with a lower BMI (P = 0.043) or higher education level (P < 0.001).
Attitude Score
The average attitude score was 34.23 ± 4.06 (possible range, 8–40 points), indicating that the surveyed women had a strongly positive attitude toward the management of GDM. The distributions of the responses to the eight questions in the attitude dimension are summarized in Figure 1. The vast majority of respondents (>90%) strongly agreed or agreed with 6 of the 8 statements in the attitude dimension (items A1, A2, A4–A6 and A8; Figure 1), and 83.17% of the women gave a positive response to item A3. Approximately half of the participants strongly agreed or agreed that insulin therapy and other drug therapy for GDM are difficult to accept (item A7).
 |
Figure 1 Responses to items in the attitude dimension. |
Attitude score was significantly higher in respondents with a lower BMI (P = 0.030) or higher education level (P < 0.001), and differences were also observed according to occupation (P < 0.001; Table 2). However, attitude score was not influenced by age, gravidity, parity, method of conception, history of POS, family history of T2DM or history of macrosomia (Table 2).
Practice Scores
The practice score for the respondents averaged 10.7 ± 2.87 points (possible range, 0–16 points). Notably, approximately two-thirds of the women reported often eating a low-glucose, low-fat and low-oil diet (P4) and often restricting dietary intake in accordance with the recommendations of doctors/dieticians (P5), and less than 4% of the respondents reported never doing these things (Figure 2). However, SMBG (P1), recording of weight and diet (P2) and exercise (P3) were performed regularly by less than half of the respondents, and more than a quarter of the participants (26.65%) stated that they never performed SMBG on a regular basis (Figure 2). Furthermore, only 33.47% of the participants often actively sought information regarding GDM and its management (P7). More than a quarter of women with GDM (29.46%) kept candy available in case of hypoglycemia during exercise (P6), and 37.68% of the respondents stated that they would ask community medical services for help in SMBG (P8). However, the majority of women with GDM (92.18%) indicated that they would see a doctor immediately if their blood glucose level was not well controlled (P9), and 99.40% of the respondents received regular prenatal examinations (P10). The practice score was comparable between groups stratified according to the various baseline characteristics (Table 2).
 |
Figure 2 Responses to items in the practice dimension. |
Correlations Between the Knowledge, Attitude and Practice Scores
Spearman correlation analysis (Table 4) revealed that the knowledge score was significantly positively correlated with the attitude score (r = 0.318, P < 0.001) and practice score (r = 0.351, P < 0.001). There was also a positive correlation between the attitude and practice scores (r = 0.209, P < 0.001).
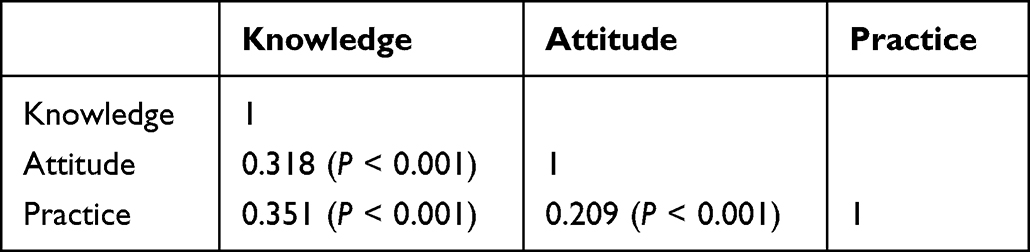 |
Table 4 Spearman Correlations Between Knowledge, Attitude and Practice Scores |
Logistic Regression Analysis of Factors Associated with Good Practice
Univariate logistic regression analysis indicated that knowledge score (P < 0.001) and attitude score (P < 0.001) were significantly associated with good practice (Table 4). The multivariate analysis identified higher knowledge score (OR, 1.138; 95% CI, 1.042–1.244; P = 0.004) and higher attitude score (OR, 1.137; 95% CI, 1.060–1.219; P < 0.001) as independently associated with good practice (Table 5).
 |
Table 5 Logistic Regression Analysis of Factors Associated with Good Practice |
Discussion
Important findings of this study were that women with GDM in China had moderate knowledge, good attitudes and moderate levels of practice with regard to GDM and its management. Furthermore, the knowledge, attitude and practice scores were significantly positively correlated with each other. Additionally, the knowledge score and attitude score were independently associated with the practice score. To our knowledge, this is the first survey evaluating the knowledge, attitudes and practices of women with GDM in China regarding the management of their condition. Our findings provide new insights that may help to inform the development and implementation of targeted interventions to improve the self-management of GDM by pregnant women.
Previous research has indicated that women, including those who are pregnant, have a low awareness of GDM, its causes (including obesity), and the importance of lifestyle modifications (including eating a healthy diet and regular exercise) to minimize the risk of developing GDM.15–18 The present study focused specifically on women with GDM, who might be expected to have a greater awareness of GDM and its management than women without this disorder. Overall, the respondents in this study had a moderate level of knowledge, which agrees well with a previous survey of pregnant women with GDM in Malaysia.17 The finding that around 85% of women did not know the main risk factors for GDM are consistent with previous reports discussing women of reproductive age in Poland18 and Nigeria19 as well as in pregnant women in Nigeria20 and Australia.21 The above observations suggest that insufficient knowledge might increase the risk of GDM complications and educational programs are needed to raise awareness of modifiable risk factors and by nutrition- and exercise-based interventions to encourage appropriate lifestyle modifications.22–24
The model of education discussed in the study by Staynova et al25 implies the distribution of the booklet with information about SMBG, nutritional management and lifestyle modification. In this study, all participants received similar printed educational materials after the initial diagnosis of GDM; however, less than 40% of the participants were aware of some GDM risks, in particular the effects of maternal hyperglycemia on the mother, fetus and neonate (items K6–K8). It suggests that contents of the existing education on GDM should be modified, possibly including earlier opportunities for learning, prior to conception or during pregnancy, as discussed by Gastrich et al.26
Another interesting observation of this study was that the knowledge score was significantly higher for women with a higher level of education or a lower BMI. Our results regarding education level agree well with published data,27,28 although not all studies have observed an association between GDM awareness and level of education.29 In contrast, previous reports have tended to find that a higher BMI was either associated with better knowledge of GDM18 or was without significant influence.30 It is possible that the women in the present study who had a lower BMI were those who made greater efforts to control their weight because they were more aware of the risks of overweight/obesity to the mother and fetus. Given the knowledge gaps identified by our survey, we suggest that the implementation of educational interventions during early pregnancy may help women with GDM to better understand the nature of their condition, the risks associated with it and the importance of adhering to self-management strategies to reduce the risks.
The respondents in this study had a strongly positive attitude toward GDM and its management, with education level, BMI (both of which also influenced the knowledge score) and occupation influencing attitude to some degree. Most of the surveyed women (>83%) strongly agreed or agreed with each of the statements in items A1–6, whereas around half of the participants strongly agreed or agreed that insulin therapy and other drug therapy for GDM are difficult to accept (item A7). Previous studies have reported that pregnant women in Nigeria,20 Spain31 and Samoa32 had positive attitudes toward eating a healthy diet or preventing GDM, which would be consistent with our results.
Our findings highlight some deficiencies in the practices of women with GDM surveyed in this study, despite their positive attitudes towards preventing and managing GDM. In particular, despite restricting dietary intake in accordance with the recommendations of doctors/dieticians, less than half of participants participated in exercise, and more than a quarter of the participants did not perform SMBG on a regular basis. It is interesting to note that in the previous study, comparing the women with GDM and those with pre-existing diabetes, women in GDM group reported adhering to dietary restrictions more often, suggesting that this part of lifestyle management is successfully covered by in-hospital education.33 At the same time, exercising and especially regular SMBG need to be explained in more detail and additional support should be proposed to those women who might need it. In this study, practice scores did not depend on baseline characteristics but rather were associated with knowledge and attitude, implying that interventions to enhance knowledge and attitude might lead to improvements in practice. In addition to that, digital health interventions such as smartphone apps, SMS messaging and websites have been shown to enhance glycemic control in pregnant women with GDM.34 Thus, additional studies are merited to explore the effects of interventions such as these on the knowledge, attitudes and practices of women with GDM and on their glycemic control.
This study has some limitations. First, the sample size was not very large, so it is possible that the analysis had insufficient statistical power to detect some real differences between groups. Second, this was a single-center study, so the generalizability of the findings remains unknown. Third, although the KAP questionnaire was designed based on a previously described tool, it may have limitations regarding its ability to evaluate perceptions of GDM. Fourth, this study did not assess whether education/training programs would enhance questionnaire scores or glycemic control.
Conclusions
In conclusion, results of this study provide important insights into the knowledge, attitudes and practices of women with GDM in China regarding GDM and its management. We anticipate that these findings and those of other surveys14,15,35 will facilitate the development and implementation of education and training programs to improve the self-management of GDM by women in China.
Abbreviations
GDM, gestational diabetes mellitus; OGTT, oral glucose tolerance test; T2DM, type 2 diabetes mellitus; KAP, Knowledge, attitude and practice; BMI, body mass index; POS, polycystic ovary syndrome; K1–K18, knowledge dimension consisted of 18 questions; SD, standard deviation.
Data Sharing Statement
All data generated or analysed during this study are included in this published article.
Ethics Approval and Informed Consent
This work has been carried out in accordance with the Declaration of Helsinki (2000) of the World Medical Association. This study was approved by the Ethics Committee of Hangzhou Women’s Hospital (ethics approval number: 2022K0807), and all participants provided informed written consent.
Acknowledgments
The authors thank all the women who kindly agreed to participate in this study.
Author Contributions
JT, YW and LC carried out the studies, participated in collecting data and drafted the manuscript. JT and YW performed the statistical analysis and participated in its design. XZ and HF participated in acquisition, analysis or interpretation of data and draft the manuscript. All authors read and approved the final manuscript. All authors made substantial contributions to conception and design, acquisition of data or analysis and interpretation of data; took part in drafting the article or revising it critically for important intellectual content; agreed to submit to the current journal; gave final approval for the version to be published; and agreed to be accountable for all aspects of the work.
Funding
This study was funded as a Hangzhou Special Science and Technology Project for the Supporting of the Development of Biomedical and Health Industry (Research on Digital Diagnosis and Treatment Platform of Perinatal Nutrition and Intelligent Application of Key Technologies; grant no. 2021WJCY332).
Disclosure
The authors declare that they have no competing interests.
References
1. Sweeting A, Wong J, Murphy HR, Ross GP. A clinical update on gestational diabetes mellitus. Endocr Rev. 2022;43(5):763–793. doi:10.1210/endrev/bnac003
2. Wang H, Li N, Chivese T, et al. IDF diabetes atlas: estimation of global and regional gestational diabetes mellitus prevalence for 2021 by international association of diabetes in pregnancy study group’s Criteria. Diabetes Res Clin Pract. 2022;183:109050. doi:10.1016/j.diabres.2021.109050
3. Paulo MS, Abdo NM, Bettencourt-Silva R, Al-Rifai RH. Gestational diabetes mellitus in Europe: a systematic review and meta-analysis of prevalence studies. Front Endocrinol. 2021;12:691033. doi:10.3389/fendo.2021.691033
4. Gao C, Sun X, Lu L, Liu F, Yuan J. Prevalence of gestational diabetes mellitus in mainland China: a systematic review and meta-analysis. J Diabetes Investig. 2019;10(1):154–162. doi:10.1111/jdi.12854
5. Juan J, Yang H. Prevalence, prevention, and lifestyle intervention of gestational diabetes mellitus in China. Int J Environ Res Public Health. 2020;17(24):9517. doi:10.3390/ijerph17249517
6. Plows JF, Stanley JL, Baker PN, Reynolds CM, Vickers MH. The pathophysiology of gestational diabetes mellitus. Int J Mol Sci. 2018;19(11):3342. doi:10.3390/ijms19113342
7. Yoles I, Sheiner E, Wainstock T. First pregnancy risk factors and future gestational diabetes mellitus. Arch Gynecol Obstet. 2021;304(4):929–934. doi:10.1007/s00404-021-06024-8
8. Ye W, Luo C, Huang J, Li C, Liu Z, Liu F. Gestational diabetes mellitus and adverse pregnancy outcomes: systematic review and meta-analysis. BMJ. 2022;377:e067946. doi:10.1136/bmj-2021-067946
9. Billionnet C, Mitanchez D, Weill A, et al. Gestational diabetes and adverse perinatal outcomes from 716,152 births in France in 2012. Diabetologia. 2017;60(4):636–644. doi:10.1007/s00125-017-4206-6
10. Zhang M, Zhou Y, Zhong J, Wang K, Ding Y, Li L. Current guidelines on the management of gestational diabetes mellitus: a content analysis and appraisal. BMC Pregnancy Childbirth. 2019;19(1):200. doi:10.1186/s12884-019-2343-2
11. Lende M, Rijhsinghani A. Gestational diabetes: overview with emphasis on medical management. Int J Environ Res Public Health. 2020;17(24):9573. doi:10.3390/ijerph17249573
12. Liao N, Luo J, Zhou X, Qin J. 妊娠期糖尿病一日门诊干预效果观察 [Therapeutic effect of one-day outpatient on gestational diabetes mellitus patients]. J Cent South Univ Med Sci. 2017;42(8):966–972. Chinese. doi:10.11817/j.issn.1672-7347.2017.08.015
13. Tang Q, Yang Z. Maternal and infant specialist nursing on improvement of knowledge, attitude, blood sugar and delivery outcome in patients with gestational diabetes mellitus. Investig Clin. 2020;61(3):1521–1528.
14. Al Hashmi I. Gestational diabetes and determinants of adherence to healthy behaviors. Minerva Obstet Gynecol. 2022;74(2):146–154. doi:10.23736/S2724-606X.21.04754-7
15. Karavasileiadou S, Almegwely W, Alanazi A, Alyami H, Chatzimichailidou S. Self-management and self-efficacy of women with gestational diabetes mellitus: a systematic review. Glob Health Action. 2022;15(1):2087298. doi:10.1080/16549716.2022.2087298
16. Andrade C, Menon V, Ameen S, Kumar Praharaj S. Designing and conducting knowledge, attitude, and practice surveys in psychiatry: practical guidance. Indian J Psychol Med. 2020;42(5):478–481. doi:10.1177/0253717620946111
17. Hussain Z, Yusoff ZM, Sulaiman SA. Evaluation of knowledge regarding gestational diabetes mellitus and its association with glycaemic level: a Malaysian study. Prim Care Diabetes. 2015;9(3):184–190. doi:10.1016/j.pcd.2014.07.007
18. Lis-Kuberka J, Orczyk-Pawiłowicz M. Polish women have moderate knowledge of gestational diabetes mellitus and breastfeeding benefits. Int J Environ Res Public Health. 2021;18(19):10409. doi:10.3390/ijerph181910409
19. Ogu RN, Maduka O, Agala V, et al. Gestational diabetes mellitus knowledge among women of reproductive age in Southern Nigeria: implications for diabetes education. Int Q Community Health Educ. 2020;40(3):177–183. doi:10.1177/0272684X19876526
20. Offomiyor FA, Rehal S. Exploring the knowledge, attitude, and practices of healthy pregnant women towards gestational diabetes mellitus in Nigeria. Qual Health Res. 2023;33(1–2):39–52. doi:10.1177/10497323221139105
21. Poth M, Carolan M. Pregnant women’s knowledge about the prevention of gestational diabetes mellitus: a qualitative study. Br J Midwifery. 2013;21:692–700. doi:10.12968/bjom.2013.21.10.692
22. Melero V, García de la Torre N, Assaf-Balut C, et al. Effect of a Mediterranean diet-based nutritional intervention on the risk of developing gestational diabetes mellitus and other maternal-fetal adverse events in Hispanic women residents in Spain. Nutrients. 2020;12(11):3505. doi:10.3390/nu12113505
23. Davenport MH, Ruchat SM, Poitras VJ, et al. Prenatal exercise for the prevention of gestational diabetes mellitus and hypertensive disorders of pregnancy: a systematic review and meta-analysis. Br J Sports Med. 2018;52(21):1367–1375. doi:10.1136/bjsports-2018-099355
24. Sayakhot P, Carolan-Olah M, Steele C. Use of a web-based educational intervention to improve knowledge of healthy diet and lifestyle in women with gestational diabetes mellitus compared to standard clinic-based education. BMC Pregnancy Childbirth. 2016;16(1):208. doi:10.1186/s12884-016-0996-7
25. Staynova R, Vasileva E, Stankova T, Yanachkova V. The impact of a printed educational booklet on disease awareness in women with gestational diabetes. Eur J Public Health. 2021;31(Supplement_3):
26. Gastrich MD, Peck S, Janevic T, Bachmann G, Lotwala N, Siyam A. Gestational diabetes mellitus: an educational opportunity. J Diabetes Nurs. 2013;17(6):220–224.
27. Gomez Gonzalez de Langarica A, Hediger H, Kaeppeli BM, Keller-Senn A. Evaluation of knowledge about gestational diabetes mellitus among postpartum women and its connection with women’s sociodemographic and clinical characteristics: a quantitative cross-sectional study. Midwifery. 2022;111:103367. doi:10.1016/j.midw.2022.103367
28. Byakwaga E, Sekikubo M, Nakimuli A. Level of and factors associated with awareness of gestational diabetes mellitus among pregnant women attending antenatal care at Kawempe National Referral Hospital: a cross sectional study. BMC Pregnancy Childbirth. 2021;21(1):467. doi:10.1186/s12884-021-03927-x
29. Elmekresh A. Gestational diabetes awareness in women of childbearing age in Sharjah. Glob J Obes Diabetes Metab Syndr. 2017;4(2):51–53. doi:10.17352/2455-8583.000023
30. Abualsaud RM, Baghdadi ES, Bukhari AA, Katib HA. Awareness of gestational diabetes mellitus among females in Jeddah, Saudi Arabia - A cross-sectional study. Fam Med Prim Care Rev. 2022;11(7):3442–3448. doi:10.4103/jfmpc.jfmpc_2485_21
31. Rhoads-Baeza M, Reis J. An exploratory mixed method assessment of low income, pregnant Hispanic women’s understanding of gestational diabetes and dietary change. Health Educ J. 2012;71:80–89. doi:10.1177/0017896910386287
32. Price LA, Lock LJ, Archer LE, Ahmed Z. Awareness of gestational diabetes and its risk factors among pregnant women in Samoa. Hawaii J Med Public Health. 2017;76(2):48–54.
33. Staynova R, Gueorguiev S, Petkova-Gueorguieva E, Petleshkova P. A comparative study on diabetes self-management in pregnant women with gestational diabetes and pre-existing diabetes. Biomed Res. 2018;29(18):3526–3531. doi:10.4066/biomedicalresearch.29-18-1044
34. Leblalta B, Kebaili H, Sim R, Lee S. Digital health interventions for gestational diabetes mellitus: a systematic review and meta-analysis of randomised controlled trials. PLOS Digit Health. 2022;1:e0000015. doi:10.1371/journal.pdig.0000015
35. Carolan-Olah M, Vasilevski V. Development and validation of the ‘Knowledge of Gestational Diabetes (GDM)’ questionnaire among a sample of women with GDM in Australia. Patient Educ Couns. 2021;104(8):2112–2118. doi:10.1016/j.pec.2021.01.029
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluating Patient and Provider Preferences for a Once-Weekly Basal Insulin in Adults with Type 2 Diabetes

Kerr D, Rajpura JR, Namvar T
Patient Preference and Adherence 2024, 18:411-424
Published Date: 14 February 2024