")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 13
Knowledge, Attitude, and Practice During the COVID-19 Pandemic: A Review
Authors Puspitasari IM , Yusuf L, Sinuraya RK , Abdulah R , Koyama H
Received 1 June 2020
Accepted for publication 10 July 2020
Published 30 July 2020 Volume 2020:13 Pages 727—733
DOI https://doi.org/10.2147/JMDH.S265527
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Irma Melyani Puspitasari,1,2 Lutfiah Yusuf,1 Rano K Sinuraya,1,2 Rizky Abdulah,1,2 Hiroshi Koyama3
1Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 2Center of Excellence in Higher Education for Pharmaceutical Care Innovation, Universitas Padjadjaran, Sumedang, West Java, Indonesia; 3Department of Public Health, Gunma University Graduate School of Medicine, Maebashi, Gunma, Japan
Correspondence: Irma Melyani Puspitasari
Department of Pharmacology and Clinical Pharmacy, Faculty of Pharmacy, Universitas Padjadjaran, Jl. Bandung Sumedang KM 21, Jatinangor, Sumedang, Sumedang, Indonesia
Tel +62 22 84288888; Ext: 3510
Email [email protected]
Abstract: The World Health Organization declared the novel coronavirus (COVID-19) outbreak a global pandemic on March 11, 2020 due to its rapid spread on a global scale. More than 118,000 cases had been reported in 114 countries, and mortality had reached a total of 4291. Scholars have suggested that the level of panic is correlated with knowledge and attitude among the population. This review presents a summary of knowledge, attitude, and practice during the COVID-19 pandemic among healthcare workers, medical students, and populations in the US, the UK, Italy, Jordan, and China in April 2020. Analysis reveals that the level of the knowledge was positive in general, and optimistic attitudes and good practices are held. Utility of substantial knowledge and positive attitudes and practices hopefully can control the spread of COVID-19.
Keywords: optimism, practice, COVID-19, pandemic
Introduction
Coronaviruses belong to the Coronaviridae family, have a diameter of 65–125 nm, and contain a single strand of RNA with lengths ranging from 26 to 32 kb. Coronaviruses comprise several types, such as alpha, beta, gamma, delta, SARS-CoV, H5N1 influenza A, H1N1 2009, and MERS-CoV.1 At the end of 2019, Wuhan City, the capital city of Hubei province in China, experienced a new coronavirus outbreak that resulted in more than 1800 deaths and more than 70,000 reported cases of infection in the first 50 days since the outbreak.1 The new virus is a member of the beta group of coronaviruses and was named the 2019 novel coronavirus (2019-nCov). Thereafter, the International Committee on Taxonomy of Viruses (ICTV) named the virus SARS-CoV-2 on February 11, 2020 and the disease as COVID-19.2–4
The World Health Organization (WHO) declared the novel coronavirus (COVID-19) outbreak a global pandemic on March 11, 2020.5 COVID-19 spread very quickly with more than 118,000 cases reported in 114 countries and the number of deaths reaching 4291.5 By May 25, 2020, COVID-19 cases reached 5,500,607 with 346,721 deaths.6
The common symptoms of COVID-19 include fever, dry coughing, and fatigue that may lead to serious symptoms, such as difficulty in breathing, chest pain, difficulty in talking, and moving.7 SARS-CoV-2 can spread through human-to-human transmission and indirect contact with contaminated objects.8 SARS-CoV-2 can be transmitted through body fluid droplets from the mouth or nose, which can spread when a person with COVID-19 coughs, sneezes, and talks.7 Droplets typically cannot transverse more than six feet (almost two meters).8 SARS-CoV-2 remains intact and contagious in droplets and can be suspended in the air for up to three hours.8,9 Additionally, contaminated droplets can settle on objects such as plastic, stainless steel, copper, and cardboard.9 A person can become infected if they touch the surface contaminated with SARS-CoV-2 objects and then make contact with mucous membranes such as the eyes, nose, or mouth.8 Therefore, health experts advise frequent hand-washing with soap and water.7
Surveys of knowledge, attitude, and practice (KAP) can collect information on what is known, believed, and done by a specific population.10 Such information is necessary because unclear information and negative attitude toward infectious diseases among the community may lead to distress and panic.11 In this time of crisis, research on KAP is vital for understanding the public’s level of awareness about the knowledge, attitude, and practice toward COVID-19.12 This article aims to shed light in this regard.
Literature Search
A literature search was conducted in April 2020 on PubMed and EBSCO databases using the keywords “knowledge,” “attitude,” “practice,” and “COVID-19”. The search yield a total of 14 articles at initial search on PubMed and one article on EBSCO. Out of the 15 articles, the study excluded three review articles, one non-English article, one non-COVID-19 article, and three articles without abstracts. Thus, the study obtained a total of seven articles for further discussion. Figure 1 presents a flowchart of the literature search.
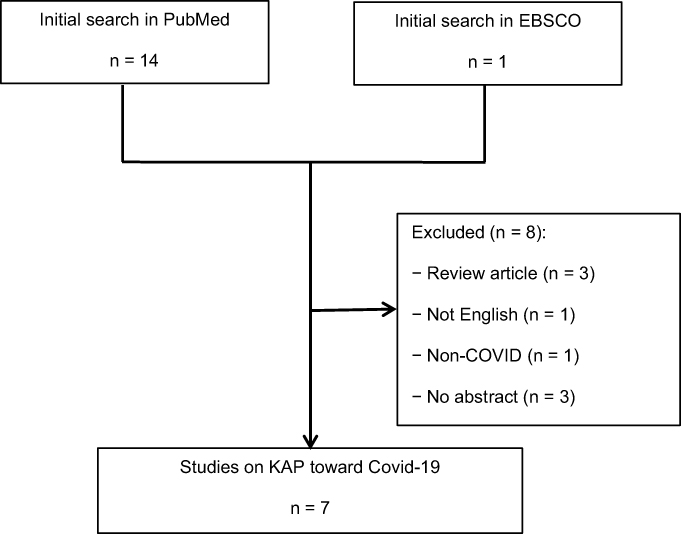 |
Figure 1 Flowchart of literature search. |
Studies on KAP Toward COVID-19
Table 1 presents the seven selected articles on KAP during COVID-19. The articles used questionnaires as instruments with the number of respondents ranging from 240 to 6910 for a total of 17,487. The respondents consisted of health workers, hospital staff, health and non-health students, and sample populations from China, Italy, Iran, Jordan, the US, and the UK.
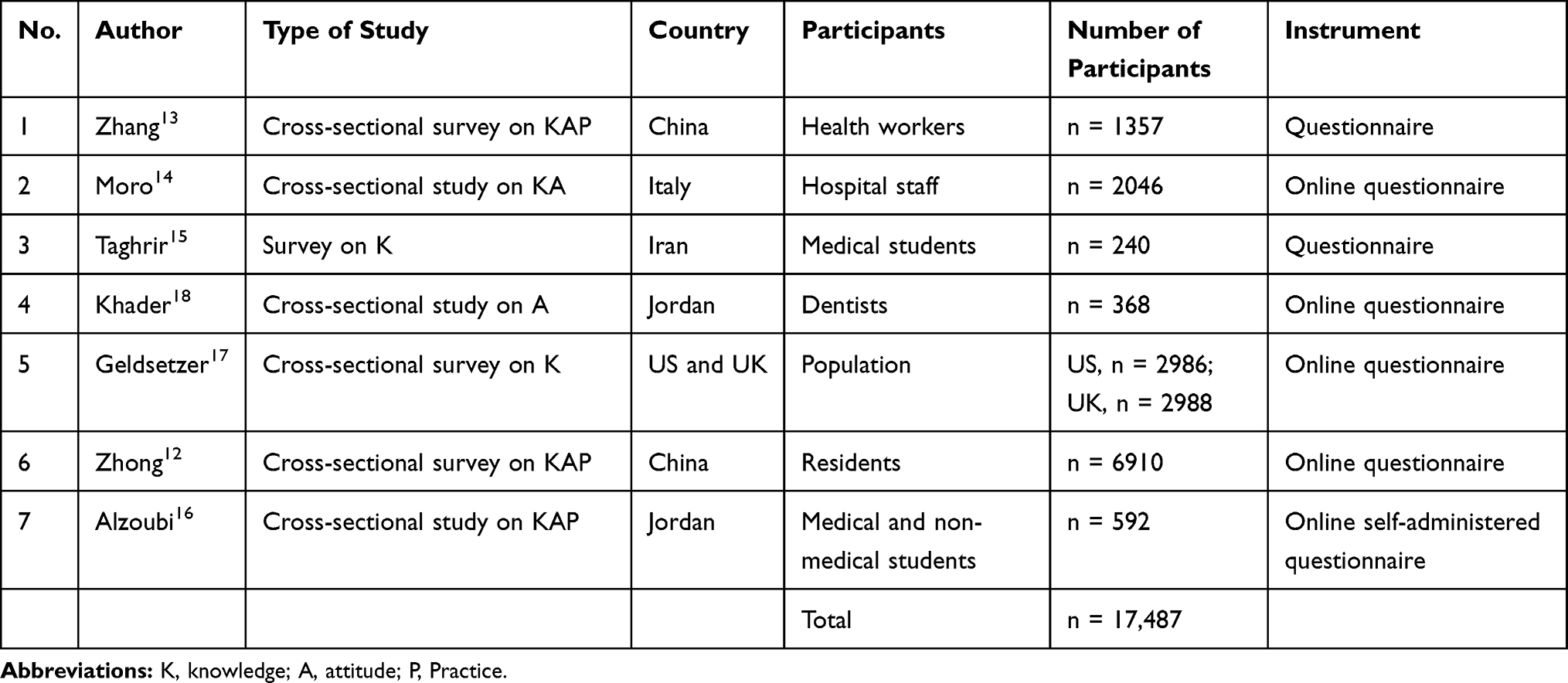 |
Table 1 List of Articles |
Knowledge
Table 2 features six articles on knowledge about COVID-19 among health workers in China, hospital staff in Italy, medical students from Iran and Jordan, and sample populations from the US, the UK, and China. In general, all articles reported considerable levels of knowledge about COVID-19.
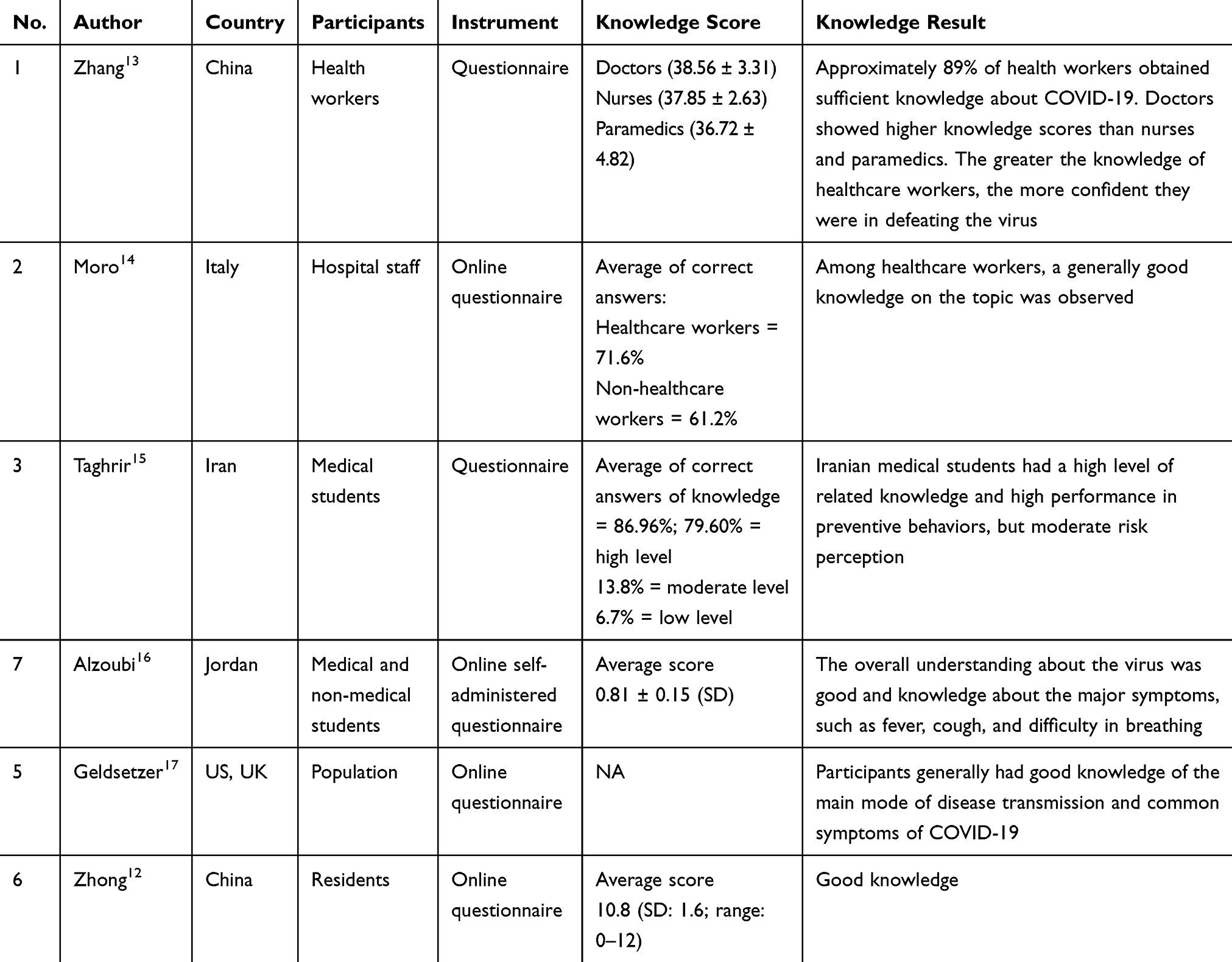 |
Table 2 Knowledge Studies |
A research conducted on 1357 health workers including doctors, nurses, and paramedics in China showed that medical doctors obtained higher knowledge scores compared with nurses and paramedics (doctors = 38.56 ± 3.31; nurses = 37.85 ± 2.63; paramedics = 36.72 ± 4.82).13 Compared with frontline health workers who have direct contact with confirmed and suspected patients, non-frontline workers displayed low levels of confidence to fight the virus (OR = 0.562; 95% CI: 0.376, 0.839).13 In Italy, respondents from 2046 hospital staff showed that, in general, healthcare workers possessed good knowledge.14
A research on medical students from Iran indicated that such students have an average of 96% correct answers with 79.60%, 13.8%, and 6.7% of students holding high, moderate, and low levels of knowledge, respectively.15 In Jordan, medical and non-medical students obtained an average score of 0.81 ± 0.15 (SD), where 90% of the participants had good knowledge of COVID-19 symptoms and more than 80% are aware of the lack of vaccine and treatment for COVID-19. No significant differences were observed regarding knowledge between medical and non-medical students.16 The cited sources of knowledge about COVID-19 are social media (34%), the WHO (19.9%), TV (17.6%), the Internet (13%), the Ministry of Health (10.1%), and colleagues (5.4%).16
Research conducted in the US and the UK revealed considerable knowledge among respondents about the transmission, spread, and symptoms of COVID-19.17 However, a portion of the populations cited misconceptions about the prevention of the disease. Nevertheless, the difference in knowledge and misperception between the US and the UK participants is non-significant.17 Another study in China on 6910 residents argued that the level of knowledge of the residents was positive with a score of 10.8 (SD: 1.6; range: 0–12).12
Attitude Toward COVID-19
Table 3 shows the five articles that discussed attitudes toward COVID-19. The study on health workers in China indicated that knowledge directly influenced attitudes. Approximately 85% of health workers were afraid of being infected while working, whereas 60% experienced anxiety when working in isolation rooms and intensive care units.13 The study on hospital staff from Italy proposes that more than 41% of the respondents avoid crowded places as a precautionary measure. Furthermore, healthcare workers generally were more aware of COVID-19 compared with the public.14
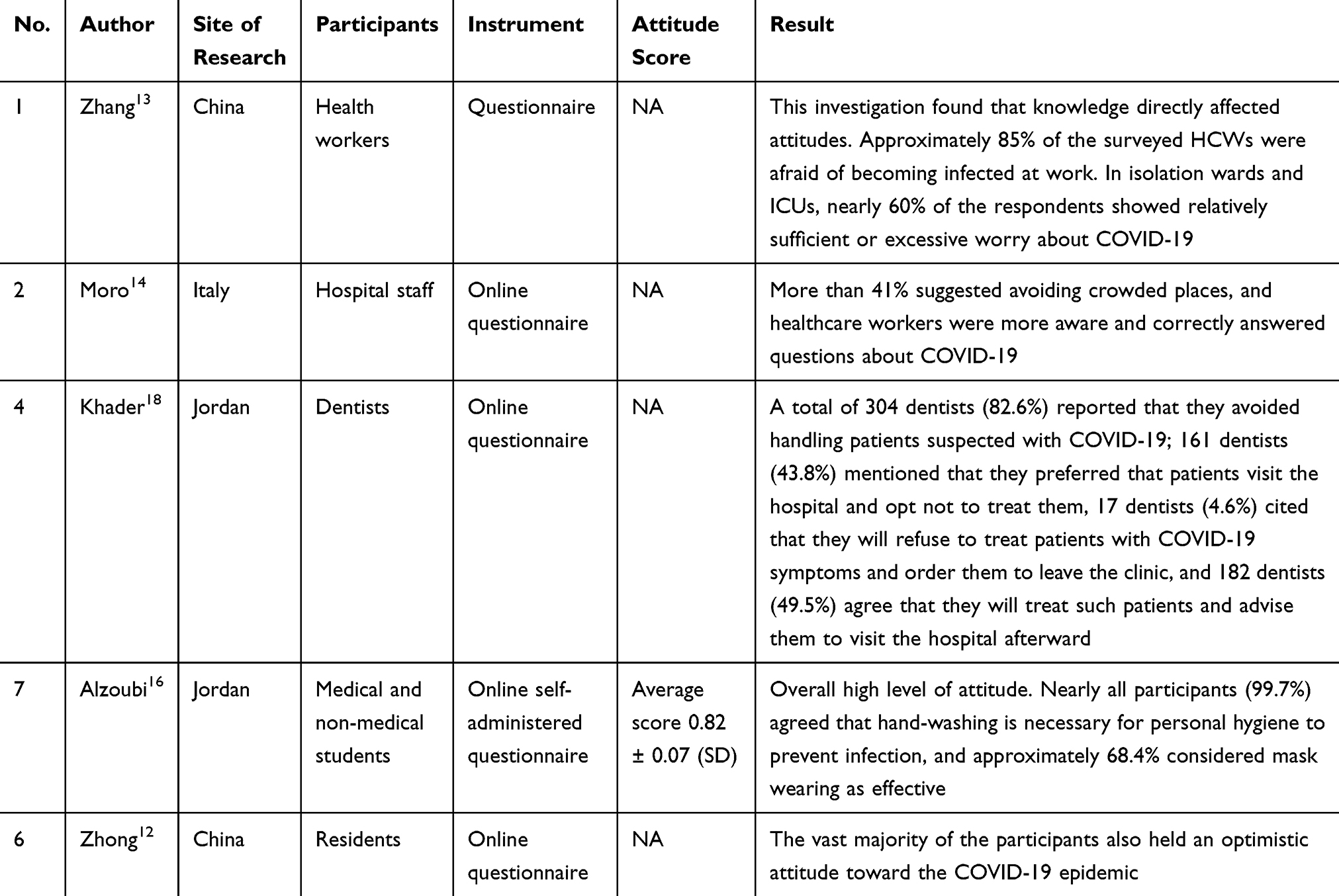 |
Table 3 Attitude Studies |
Furthermore, the research on 368 dentists in Jordan revealed that more than half of the participants (n = 203; 55.2%) deemed that the symptoms of COVID-19 can be resolved over time and thus do not require special treatment.18 A total of 275 dentists (74.7%) agreed that implementing social distancing among patients in the clinic, wearing a mask in the waiting room, and hand-washing before entering the treatment room can prevent the spread of the virus during dentist appointments. However, 80 respondents (21.7%) believe that such measures are not important and do not cause excessive panic.18 A total of 304 dentists (82.6%) reported that they refrain from handling patients that display COVID-19 symptoms, whereas 161 dentists (43.8%) mentioned that they preferred that patients with symptoms visit the hospital instead of their clinics. Furthermore, 17 dentists (4.6%) expressed that they will refuse to treat patients with COVID-19 symptoms and advise them to leave the clinic. In contrast, 182 dentists (49.5%) confirmed that they will treat the patient, but advise them to visit the hospital afterward.18
A study on health and non-health students from Jordan indicated that such students possessed high levels of attitude with an average score of 0.82 ± 0.07 (SD).16 The study showed that nearly all participants (99.7%) agreed that hands should be regularly washed for personal hygiene. In terms of avoidance, approximately 68.4% of the participants expressed that using masks can prevent viral infections, 81.8% and 79.4% agreed that smoking and antibiotics cannot prevent infection, 94.6% cited that they will divulge if they are infected, and 93.6% will visit hospitals if infected.16
The study in China on residents as respondents found that residents in general hold an optimistic attitude toward the COVID-19 pandemic. As many as 90.8% are hopeful that COVID-19 will be successfully controlled, and 97.1% are confident that China will win against the virus.12
Practice Toward COVID-19
Table 4 presents three articles on the practice of COVID-19 conducted in China and Jordan.12,13,16 The study on health workers in China showed that 89.7% of health workers followed correct practices for handling COVID-19 cases.13 In this review, practice is related to work experience, work hours, and other factors.13 The practice of residents toward COVID-19 indicated that Chinese residents avoid crowded places (96.4%) and wore masks when leaving home (98.0%) during the period of the rapid spread of COVID-19.
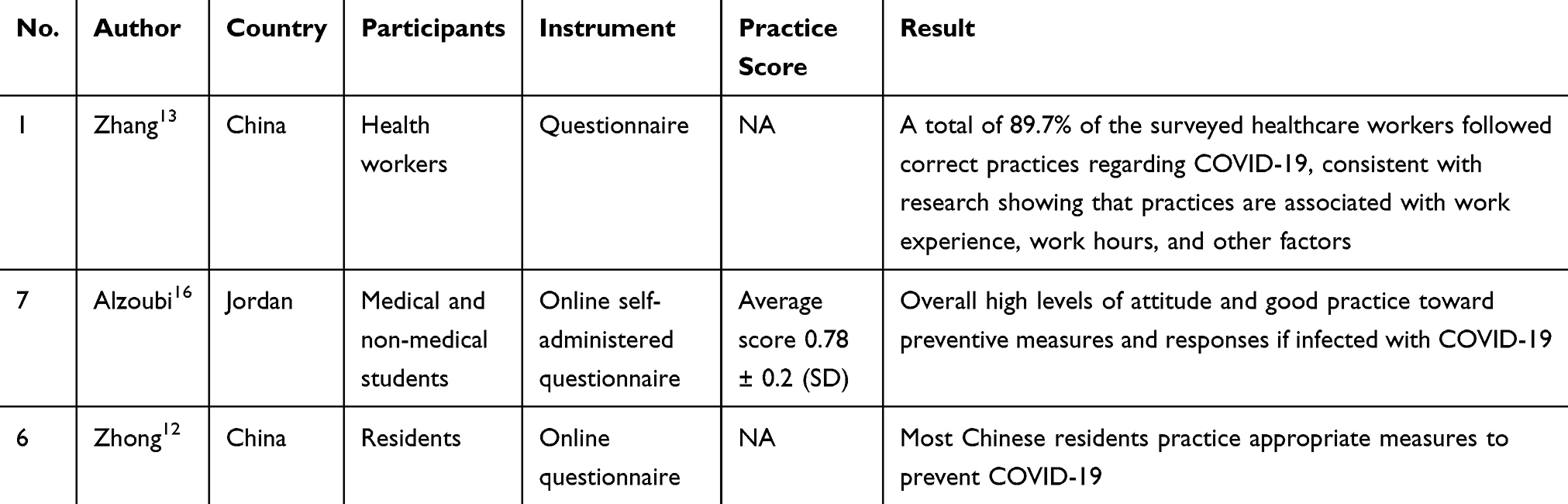 |
Table 4 Studies on Practice |
The Jordan study on health and non-health students obtained an average score of 0.78 ± 0.2 (SD) in terms of practice. In other words, students displayed favorable practices toward COVID-19 prevention, such as hand-washing, refraining from shaking hands, and following the etiquette of coughing and sneezing.16
Importance of Increasing Knowledge About COVID-19
This review study revealed that among seven studies on knowledge, attitude, and practice during pandemics, six studies showed that respondents have good knowledge about COVID-19, five studies found a good and optimistic attitude among respondents, and three studies indicated that respondents have good practices. The findings also indicated that knowledge directly influenced attitudes. Increasing knowledge among communities through health education is important because COVID-19 has been declared a pandemic. As such, the increased knowledge will influence the attitude and practice toward COVID-19.12 KAP is strongly correlated with the incidences of many infectious diseases.19 In the modern society, social media are one of the tools that can be utilized to enhance knowledge among communities. Based on the study in Iran, the students cited that their sources of knowledge about COVID-19 are social media (34%), the WHO (19.9%), TV (17.6%), the Internet (13%), the Ministry of Health (10.1%), and friends (5.4%).16 A global public health campaign strategy to increase knowledge should be conducted to help in controlling the spread of the disease. In this regard, everybody should work together to eradicate this pandemic.
Conclusion
The review summarized seven articles in relation to KAP studies toward COVID-19. Six studies showed that respondents have good knowledge about COVID-19, five studies found a good and optimistic attitude among respondents, and three studies indicated that respondents have good practices and followed such practices related to COVID-19. Good KAP is a tool that can hopefully be used to control the spread of COVID-19.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Shereen MA, Khan S, Kazmi A, Bashir N, Siddique R. COVID-19 infection: origin, transmission, and characteristics of human coronaviruses. J Adv Res. 2020;24:91–98. doi:10.1016/j.jare.2020.03.005
2. Lai -C-C, Shih T-P, Ko W-C, Tang H-J, Hsueh P-R. Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) and coronavirus disease-2019 (COVID-19): the epidemic and the challenges. Int J Antimicrob Agents. 2020;55(3):105924. doi:10.1016/j.ijantimicag.2020.105924
3. World Health Organization. Naming the coronavirus disease (COVID-19) and the virus that causes it. 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/technical-guidance/naming-the-coronavirus-disease-(covid-2019)-and-the-virus-that-causes-it.
4. International Commitee on Taxonomy of Viruses. Naming the 2019 Coronavirus. Available from: https://talk.ictvonline.org.
5. WHO Director-General’s opening remarks at the media briefing on COVID-19-11 March 2020. 2020. Available from: https://www.who.int/dg/speeches/detail/who-director-general-s-opening-remarks-at-the-media-briefing-on-covid-19—11-march-2020.
6. COVID-19 CORONAVIRUS PANDEMIC. 2020. Available from: https://www.worldometers.info/coronavirus/.
7. World Health Organization. Q&A on Coronaviruses (COVID-19). 2020. Available from: https://www.who.int/emergencies/diseases/novel-coronavirus-2019/question-and-answers-hub/q-a-detail/q-a-coronaviruses#:~:text=symptoms.
8. Lotfi M, Hamblin MR, Rezaei N. COVID-19: transmission, prevention, and potential therapeutic opportunities. Clin Chim Acta. 2020;508:254–266. doi:10.1016/j.cca.2020.05.044
9. van Doremalen N, Bushmaker T, Morris DH, et al. Aerosol and surface stability of SARS-CoV-2 as compared with SARS-CoV-1. N Engl J Med. 2020;382(16):1564–1567. doi:10.1056/NEJMc2004973
10. Haq N, Hassali MA, Shafie AA, Saleem F, Farooqui M, Aljadhey H. A cross sectional assessment of knowledge, attitude and practice towards Hepatitis B among healthy population of Quetta, Pakistan. BMC Public Health. 2012;12(1):1. doi:10.1186/1471-2458-12-692
11. Lin Y, Huang L, Nie S, et al. Knowledge, attitudes and practices (KAP) related to the pandemic (H1N1) 2009 among Chinese general population: a telephone survey. BMC Infect Dis. 2011;11(1):128. doi:10.1186/1471-2334-11-128
12. Zhong B, Luo W, Li H, et al. Knowledge, attitudes, and practices towards COVID-19 among Chinese residents during the rapid rise period of the COVID-19 outbreak: a quick online cross-sectional survey. Int J Biol Sci. 2020;16(10):1745–1752. doi:10.7150/ijbs.45221
13. Zhang M, Zhou M, Tang F, et al. Knowledge, attitude and practice regarding COVID-19 among health care workers in Henan, China. J Hosp Infect. 2020;105(2):183–187. doi:10.1016/j.jhin.2020.04.012
14. Moro M, Pietro VG, Capraro M, et al. 2019-novel coronavirus survey: knowledge and attitudes of hospital staff of a large Italian teaching hospital. Acta Biomed. 2020;91(11):29–34. doi:10.23750/abm.v91i3-S.9419
15. Taghrir MH, Borazjani R, Shiraly R. COVID-19 and Iranian medical students; a survey on their related-knowledge, preventive behaviors and risk perception. Arch Iran Med. 2020;23(4):249–254. doi:10.34172/aim.2020.06
16. Alzoubi H, Alnawaiseh N, Lubad MA, Aqel A, Al-Shagahin H. COVID-19 - knowledge, attitude and practice among medical and non-medical university students in Jordan. J Pure Appl Microbiol. 2020;14(1):17–24. doi:10.22207/JPAM.14.1.04
17. Geldsetzer P. Use of rapid online surveys to assess people ’ s perceptions during infectious disease outbreaks: a cross-sectional survey on COVID-19. J Med Internet Res. 2020;22(4):1–19. doi:10.2196/18790
18. Khader Y, Al Nsour M, Al-batayneh OB, et al. Dentists’ awareness, perception, and attitude regarding COVID-19 and infection control: cross-sectional study among jordanian dentists. JMIR PUBLIC Heal Surveill. 2020;6:2. doi:10.2196/18798
19. Pathman A, Aziah B, Zahiruddin W, et al. Knowledge, attitudes, practices and health beliefs toward leptospirosis among urban and rural communities in Northeastern Malaysia. Int J Environ Res Public Health. 2018;15:11. doi:10.3390/ijerph15112425
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.