")
Back to Journals » Journal of Multidisciplinary Healthcare » Volume 17
Knowledge and Practice of Healthcare Professionals in the Medical Care of Asthma Adult Patients in Jordan with a Particular Reference to Adherence to GINA Recommendations
Authors Al-hamaden RA, Abed A , Khader HA, Hasoun L , Al-Dulaimi AH, Alsayed AR
Received 6 October 2023
Accepted for publication 15 January 2024
Published 26 January 2024 Volume 2024:17 Pages 391—404
DOI https://doi.org/10.2147/JMDH.S433149
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Rana Ahmad Al-hamaden,1 Anas Abed,2 Heba A Khader,3 Luai Hasoun,1 Abdullah Hatem Al-Dulaimi,4 Ahmad R Alsayed1
1Department of Clinical Pharmacy and Therapeutics, Faculty of Pharmacy, Applied Science Private University, Amman, Jordan; 2Pharmacological and Diagnostic Research Centre, Faculty of Pharmacy, Al-Ahliyya Amman University, Amman, Jordan; 3Department of Clinical Pharmacy and Pharmacy Practice, Faculty of Pharmaceutical Sciences, The Hashemite University, Zarqa, Jordan; 4Ibn Sina Teaching Hospital, Mosul, Iraq
Correspondence: Ahmad R Alsayed, Department of Clinical Pharmacy and Therapeutics, Faculty of Pharmacy, Applied Science Private University, Amman, Jordan, Tel +962786770778, Email [email protected]; [email protected]
Purpose: This study aimed to evaluate Jordanian healthcare professionals’ knowledge, skills, and experience in dealing with and treating adult asthmatic patients and assess healthcare professionals’ compliance with the Global Initiative for Asthma (GINA) guideline recommendations for asthma treatment and management in Jordan.
Patients and Methods: A cross-sectional survey was conducted in Jordan between May and June 2023. This study included physicians, pharmacists, and nurses working in clinical settings and directly interacting with asthma patients in Jordan’s private and governmental healthcare facilities who were eligible to participate in this research. Three primary sections of an online survey were constructed using Google Forms and included demographic data, a diagnosis and management of the illness, and a list of worldwide medical references for asthma.
Results: A total of 300 healthcare professionals, including pharmacists (103), nurses (87), Doctor of Pharmacy (28), and physicians (82), took part in this research. The survey respondents’ general knowledge of the nature and symptoms of asthma is quite high, exceeding 84% and 86%, respectively. The survey also showed a high degree of awareness of asthma diagnosis. It was also revealed that around one-quarter of participants consistently reported the severity of asthma. The most frequent factor influencing the decision to take controller or maintenance medicines is symptom severity (reported from 86% of participants). The GINA guidelines were selected as the asthma information source by almost half of the participants. Finally, 47% of participants were aware of the GINA’s 2019 adjustments of the recommendations.
Conclusion: This study showed that Jordanian healthcare professionals understand the nature, symptoms, and diagnoses of asthma disease. However, many of the survey participants lack adherence, awareness, and understanding of the GINA recommendations about asthma management. More research is required to assess the adherence to the evidence-based recommendations and evaluate the impact of training courses.
Keywords: adherence, asthma, GINA, healthcare, practitioners
Introduction
Asthma is a prevalent, controllable condition that places a high financial and social cost on society. Asthma is characterized by respiratory symptoms such as wheezing, shortness of breath, chest tightness, coughing, and fluctuating expiratory airflow restriction.1 Asthma is a widespread chronic noninfectious illness that affects adults and children, causes considerable morbidity and death, and requires continuing therapeutic therapy.1 The number of confirmed cases of asthma has grown in Jordan during the last ten years.2–4
The Global Initiative for Asthma (GINA) Scientific Committee was established in 2002 and comprises volunteers dedicated to the importance of adult and pediatric asthma research. The committee issues new recommendations practically almost every year while meeting every two years with the American Thoracic Society (ATS) and the European Respiratory Society (ERS) to examine the most recent discoveries in asthma research.1,5 By collaborating with medical experts and public health officials worldwide, GINA seeks to raise awareness of asthma, its symptoms, causes, and means of prevention and management. The most significant shift in asthma management in the past 30 years was made when GINA issued its recent guidelines in 2019 that updated how mild asthma is treated.6,7 As a result, monotherapy with short-acting beta2-agonists (SABA) is no longer recommended as the first treatment line for mild asthma according to the 2019 GINA guidelines since it raises the risk of life-threatening asthma-related complications. Therefore, to reduce this risk, all asthmatic individuals should get combination treatment with long-acting beta-agonists (LABA) and inhaled corticosteroids (ICS) when needed for mild asthma or routinely every day for moderate or severe asthma.5,7 Moreover, low-dose budesonide-formoterol or beclomethasone-formoterol is recommended as a first-line treatment as a reliever and controller medication. When SABA is administered, low-dose ICS should also be utilized.1,5,7,8
Thus, sufficient knowledge and awareness among physicians and other healthcare providers are required to manage asthma and limit its exacerbation, directly influencing lower death rates and economic costs.2
This study aimed to ascertain the knowledge and how healthcare professionals in Jordan manage adult asthmatic patients according to the global medical resources, focusing on adherence to the GINA 2019–2022 recommendations. To achieve this aim, the main objectives of this study were to evaluate Jordanian healthcare professionals’ knowledge, skills, and experience in dealing with and treating adult asthmatic patients and to assess the compliance level of healthcare professionals with GINA guidelines for asthma treatment and management in Jordan.
Materials and Methods
Study Design and Participants
In order to evaluate the knowledge and practice of Jordanian healthcare professionals in treating adult asthma, this cross-sectional study was carried out between May and June 2023 in Jordan using an online survey. Physicians, pharmacists, and nurses who work in clinical settings and interact with asthma patients were eligible to participate in this study. In contrast, all individuals who were not in the medical field or not dealing with asthma patients were excluded. The study participants’ knowledge and behavior were evaluated using knowledge questions based on the GINA recommendations.
The Research Ethics Board of Applied Science Private University, Amman in Jordan (2023-PHA-26), provided ethical approval for this study. This study complies with the Declaration of Helsinki.
Survey Development and Administration
The questionnaire was created utilizing earlier research, with few alterations.2,9 A preliminary version of the survey in English was written using variables taken from the literature before it was distributed to participants. Following a validation procedure by five experts, subject matter experts gave their valuable advice and feedback on the final version of the survey, which had its content confirmed. These steps include thoroughly examining the survey items for clarity, relevance, and appropriateness by the experts, followed by iterative discussions and revisions to refine the instrument.
As a quick and easy replacement for outdated data-gathering techniques, the survey was created using Google Forms. Web-based surveys can reduce the time needed to gather data from replies, saving researchers money and effort and guaranteeing respondents’ privacy.
The study invites a suitable sample of eligible people to take part. Healthcare practitioners were encouraged to participate through face-to-face interviews and social media channels like Facebook and WhatsApp. In the beginning, every participant in this research consented to participate.
Afterward, a self-administered online survey, delivered anonymously to all participants and containing a summary of the study, inclusion criteria, and informed consent, was undertaken to decrease the chance of bias and protect participant’s anonymity throughout the procedure.
The survey included questions about the participants knowledge of recommended treatments, diagnostic criteria, and management strategies outlined in the GINA guideline.
Data Collection
The approved version of the questionnaire consists of three main parts. The first part focuses on demographic information, including age, gender, years of work experience, specialization, place of employment, and the weekly average number of asthma patients encountered.
The second part gathers data on the awareness of asthma among study participants. It has been divided into three sections. The first section is about the knowledge about the nature of asthma disease; it consists of only one question about the type of disease. The second section is about the knowledge of the symptoms and diagnosis of asthma disease; it consists of eight questions, including its symptoms, diagnosis, classifying the asthma patient status, and the aim of the treatment to be obtained by healthcare professionals. The third and latest section about participants’ understanding of asthma treatment and medication regimens included five questions about treatment and medication plans.
The third part of the questionnaire consists of two questions; the first is about international medical references for asthma, and the second is about healthcare professionals’ awareness and knowledge of the changes and updates that occurred in 2019 by GINA.
Statistical Analysis
The data from the online survey was first downloaded to Excel heat-spread software (Microsoft Corporation, Redmond, WA, USA) and then imported into IBM Statistical Package for Social Science (SPSS). SPSS version 26 (IBM Corporation, New York, NY, USA) was used to analyze the data. The continuous variables are expressed as Mean ± standard deviation (SD), and the categorical variables are expressed as frequencies (percentages).
Results
Demographical Characteristics of the Study Participants
The characteristics of the study participants are listed in Table 1. This research included 300 individuals with an average age of 31.4 years. Females comprised more than half of the participants; n = 173,57.7%. Pharmacists, nurses, physicians, and Doctors of Pharmacy were the survey participants’, with the following frequencies for each specialty: 34.3%, 29.0%, 27.3%, and 9.3%, respectively. More than one-quarter of the participants, n = 82,28.0%, have between one and five years of job experience. Additionally, 19.0% of the participants worked in community pharmacies, 17.7% at private hospitals, and 23.3% in settings other than those specified such as private medical centers. Finally, 1 to 4 asthma cases are examined by 45.8% of participants per week.
 |
Table 1 Participants’ Demographical Characteristics (N = 300) |
Awareness of Asthma Among Study Participants
The second section of the questionnaire was designed to estimate the participants’ knowledge of the asthma condition. In terms of knowledge of the illness’s nature, symptoms, and diagnosis, this section compiles data from the participants.
Knowledge About the Nature of Asthma Disease
Overall, the participants’ understanding of the nature of the condition is relatively high, according to the data shown in Table 2. A correct answer to the questions concerning the nature of asthma was given by more than 84% of participants, demonstrating that the majority of participants had appropriate awareness of the disease’s nature.
 |
Table 2 Knowledge of the Study Participants’ About the Nature of Asthma Disease |
Knowledge About the Symptoms and Diagnosis of Asthma Disease
Most of the participants had appropriate knowledge about asthma symptoms. Most participants showed a high frequency of more than 86% for giving the right answer to the questions regarding asthma symptoms. It was also noticed that difficulty breathing received the highest frequency of the reported answers as asthma symptoms (Table 3).
 |
Table 3 Knowledge of the Study Participants’ About the Symptoms and Diagnosis of Asthma |
The information regarding the asthma diagnosis is represented in Table 3. The majority of participants answered yes to all of the triggers stated in the second question concerning asthma triggers, with temperature changes being the least frequent trigger; n=191 (63.7%). It also revealed that a majority of participants approximately 65.7%, 57.0%53.0%, and 47.3% believe that a spirometer, chest radiography, peak flow meter, and arterial blood gases, respectively, are very crucial tools for diagnosing asthma patients, and 42.7%, 40.3%, 33.0%, and 30.0% believe that arterial blood gas, peak flow meter, chest radiography, and spirometer respectively, are can be used in diagnosing asthma patients but not very essential. The majority of participants, as indicated in question 4, believed that cyanosis, a fast heartbeat (tachycardia), and worsening of the typical everyday symptoms were indicators or symptoms of an asthma attack, with the frequency being 79.3%, 84.7%, and 81.3%, respectively.
The capacity of the medical expert to assess the severity of the illness is one of the crucial variables that influence how any illness is treated. As a result, the purpose of the question in Figure 1 was to ascertain how frequently the research participants classified their patients’ asthma as mild, moderate, or severe. According to the findings, only 25.7% of healthcare professionals who participated in this study always identified illness severity and classified asthma patients as mild, moderate, and severe asthma disease in their diagnosis. On the other hand, the vast majority of the participants 33.0% sometimes identified illness severity and classified asthma patients as mild, moderate, and severe asthma disease in their diagnosis.
 |
Figure 1 Knowledge of the study participants about the classification of disease severity, n=300. |
The research participants’ goals when treating mild, moderate, and severe asthma are shown in Figure 2. The healthcare professionals ranked symptoms control over exacerbation reduction as the most important aim when dealing with their asthma patients, so we noticed that in patients with mild asthma, the percentage was (43.7% vs 23.3%), and in moderate asthma was (39.3% vs 36.7%). Additionally, a greater proportion of healthcare professionals ranked exacerbation reduction as their main treatment goal in patients with severe asthma in percent 35.0%.
 |
Figure 2 Participants’ expected outcomes when treating asthma disease, n=300. |
Participants’ Understanding of the Treatment and Medication Regimens for Asthma
Each participant was asked a number of questions to assess their level of knowledge on asthma therapy Table 4. More than half of the participants believed that all of the previously described criteria should be taken into account when recommending controller or maintenance drugs. Furthermore, of all the characteristics indicated in Question 1, the frequency of symptom intensity was the highest 86.0%. At Question 2, the participants asked about the medication considered as the first line for stable asthma, the most common first-line therapy for stable asthma is inhaled albuterol 81.7%, whereas Cromolyn 19.7% is the least common. While question 3 was about if it was possible to treat mild asthma patients with SABA (short-acting beta-agonist) therapy as albuterol alone without other medications, (n = 185), 61.7% of participants responded in the affirmative.
 |
Table 4 Participants’ Knowledge About the Treatment of Asthma Disease |
The questionnaire discovered that 43.3% of participants selected inhaled SABA (short-acting beta-agonist) alone, such as salbutamol or albuterol, as the first line of therapy for adult patients with mild asthma. Contrarily, the ICS/LABA (long-acting beta-agonist) fixed-dose combination without inhaled SABA (short-acting beta-agonist)is the less popular option for patients with mild asthma, with a frequency of 2.3%, also revealed that the least popular treatment for adult patients with moderate asthma was an ICS/LABA (long-acting beta-agonist) fixed-dose combination without inhaled SABA with a frequency of 11.0%, while the highest percentage of participants 26.0% chose Low-dose maintenance ICS with inhaled SABA (short-acting beta-agonist) therapy as the first-line treatment for adult patients with moderate asthma (Figure 3).
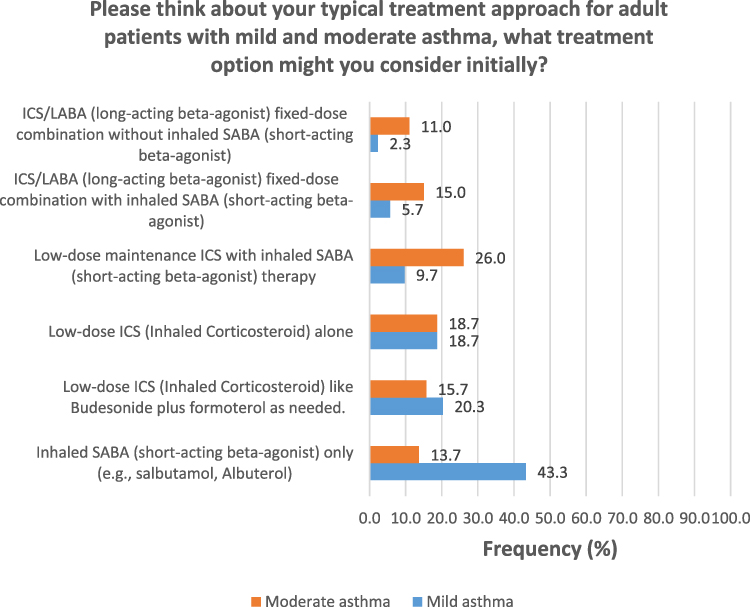 |
Figure 3 Participants’ knowledge about mild and moderate asthma treatment. |
International Medical References for Asthma
The third part of the questionnaire was about the asthma medical references that are used by healthcare professionals. The participants answered the reference that was considered the most frequently used reference is medical websites and mobile applications, with a frequency rate of 53.0% immediately followed by GINA with a frequency rate of 47.7%, while the Canadian Thoracic Society (CTS), which has a frequency rate of 28.0% is the least commonly used reference by participants as mentioned in Table 5.
 |
Table 5 References Used for Asthma According to the Study Participants |
Since one of the key purposes of this study is to assess the medical professionals’ adherence to GINA recommendations for asthma treatment and management, the last question was about the awareness and knowledge of the changes and updates that occurred in 2019 by GINA. The results showed only 47.3% of healthcare professionals knew about the updates and modifications made by GINA in 2019 (Figure 4).
 |
Figure 4 Participants’ level of knowledge about GINA’s improvements and updates. |
Discussion
The main goal of the current study was to determine how healthcare providers in Jordan manage adult asthmatic patients according to international medical resources, emphasizing adherence to GINA recommendations. This study showed that there is a lack of adherence, awareness, and understanding of the GINA guidelines and recommendations about asthma management, despite around half of the participants reported using the GINA as a medical reference for asthma disease, but this is not entirely consistent with their answers to treatment and medication plan section in the questionnaire.
Inflammation of the airways and respiratory symptoms are the hallmarks of asthma, a chronic disorder expected to afflict more than 300 million people worldwide of all ages.10 Half of patients with asthma have ineffective asthma control despite extensive asthma management programs and accessible therapies.11
Conversing with patients and healthcare professionals about asthma treatment and control is crucial to enhancing outcomes.1 Therefore, asthma recommendations do promote team decision-making.1 The partnership between healthcare professionals (Physicians, pharmacists, and nurses who work in clinical settings and interact with asthma patients) and patients with asthma must be developed to induce effective management; this aims to enable patients to take control of their condition, discuss and agree on treatment goals, develop an individualized written care plan, and self-manage their asthma with the guidance of healthcare professionals.8 Therefore, this study aimed to determine how Jordanian healthcare providers treat adult patients with asthma and manage the illness through their treatment plans and international medical resources, emphasizing compliance with GINA guidelines.
According to our research, the pharmacist specialty had 34.3%, Which was the highest percentage among the participants when asked about their specialization in the medical field; this shows the vital role of the pharmacist, and as stated in a recent study that explains the role of the pharmacist and its importance in treating and controlling the disease, by improving patient health outcomes and saving healthcare costs by detecting and preventing treatment-related problems in a variety of diseases.8 According to our research, most participants were aware of the nature of the conditions. In that regard, a recent study by Said et al in Egypt found that hospital pharmacists were much more knowledgeable about asthma than community pharmacists and pharmacists with more experience; it also showed that one-quarter of the pharmacists had adequate asthma knowledge.12 Additionally, the findings of a new investigation in Jordan (2021) showed that the general level of asthma knowledge was sufficient and that more than 78% of physicians exhibit an adequate awareness of asthma.2
Additionally, Amorha et al’s data from 2020 in a Nigerian State showed that most community pharmacists (87.6%) were aware that the main signs of asthma include persistent chest tightness, wheezing, and coughing.13 Likewise, according to Adeniyi et al research from 2017, only 61% of the study respondents in West Nigeria were familiar with the symptoms of an asthma attack.14 This finding was similar to ours, which showed that the participants thoroughly understood asthma symptoms.
Several studies have focused on the importance of different environmental exposure characteristics (chemicals, drugs, smoking, diet, pollution, viruses, allergens, microbiome changes) as triggers of asthma disease and its exacerbation.8,15–20 The current research’s findings showed that most participants agreed with all of the triggers listed in the question about asthma triggers. A recent study in Saudi Arabia found that almost half of the research participants understood the triggers connected to asthma.21
Along with the study’s findings, more than half of the participants thought diagnostic instruments such as spirometer, chest radiography, peak flow meter, and arterial blood gases were essential for diagnosing asthma. The result of Adeniyi et al (2017) in South-West Nigeria found that the percentage of physicians using diagnostic tools peak flow meter (97%), spirometer (95%), and chest radiography (61%) to diagnose asthma.14 Furthermore, only 17.2% of doctors indicated that they were aware that spirometers were available at their primary care facilities, according to a 2014 study by Almutawa et al in Kuwait.22 Despite the critical role peak flow meters play in acute asthma, Assiri et al’s study from 2021 in Abha, Saudi Arabia, found that only 41% of doctors had access to this diagnostic device.23
Furthermore, the findings indicated that only 25% of the participants in the present study consistently documented the severity of their patients’ disease. Simultaneously, 33% occasionally engaged in the aforementioned behavior, despite being the most prevalent group. According to a recent study by Chapman et al, most physicians categorize their patients’ illnesses into three levels of severity: mild, moderate, or severe. The research findings indicate that less than 5% of clinicians classify illnesses frequently, while less than 1% never engage in such categorization.9
Optimizing symptom control, lowering the likelihood of asthma flare-ups, and avoiding side effects from treatment are the key objectives of asthma treatment. In our research, symptom management (43.7%) is prioritized for patients with mild asthma, while reducing exacerbations (23.3%) is the lowest priority. Furthermore, regarding moderate asthma, 39.3% and 36.7% of respondents aimed to manage symptoms and reduce exacerbations, respectively. Asthma control (33.7%) and exacerbation reduction (35.0%) were among the top goals for treating severe asthma. These findings are consistent with the study by Chapman et al in 2021. When prescribing daily maintenance medicine, doctors in all four of the study’s participating nations (Canada, Australia, China, and the Philippines) ranked symptom severity higher than exacerbation risk as the most crucial consideration. Moreover, they misrepresented that, except for Canada, most doctors ranked preventing symptoms higher than lowering the risk of exacerbations as their primary treatment objective for patients with mild and moderate asthma. On the other hand, more doctors in Australia, Canada, and the Philippines prioritized exacerbation reduction over symptom management as their top treatment objective for patients with severe asthma.9
Numerous therapeutic problems are brought on by the diverse nature of asthma and different phenotypes.24 Thus, a patient’s medical characteristics and pharmaceutical response play a key role in determining their individualized asthma therapy.25 Our research revealed that more than half of participants thought controller or maintenance medication recommendations depended on many parameters. The frequency of symptom intensity was also the greatest (86.0%) of all the mentioned characteristics.
This study revealed that 43.3% of participants chose to treat adult patients with mild asthma with an inhaled SABA alone, such as salbutamol (albuterol). This indicates that they were not aware on the major change happened with 2019 edition og GINA. On the other hand, with a frequency of just 2.3%, the ICS/LABA fixed-dose combination without inhaled SABA is the less common choice for individuals with mild asthma. This result is in line with the findings of a study by Chapman et al, which found that for patients with mild asthma, doctors in Australia, Canada, China, and the Philippines indicated that SABA by itself was the most commonly prescribed medication (31.9–66.5%). They also stated that the daily low-dose ICS with SABA is the second option in those nations (13.7–22.3%), whereas the daily low-dose ICS without SABA is the second option in China (18.1%).9
Additionally, the results of the participant’s answers highlighted that an ICS/LABA fixed-dose combination without inhaled SABA with a frequency of 11.0% was the least preferred treatment for adult patients with moderate asthma. In contrast, the highest proportion of respondents (26.0) selected low-dose maintenance ICS with inhaled SABA treatment as the initial course of treatment for those patients. Previous research indicated that most physicians (77%) favored ICS for treating mild asthma. On the other hand, about 74% of physicians preferred ICS/LABA to treat moderate asthma.26 The results of the participant’s answers are not compatible with GINA recommendations; the controller and reliever treatment in Track 1 is as-needed low-dose ICS-formoterol, and Track 2 is low-dose maintenance ICS and as-needed SABA as a reliever in mild asthma. For moderate asthma, the controller and reliever treatment in Track 1 is low-dose maintenance ICS-formoterol and as needed, low-dose ICS-formoterol as a reliever. And Track 2 is low-dose maintenance ICS-LABA and as-needed SABA as a reliever.1
In the current study, inhaled albuterol was the most popular first-line treatment for stable asthma (81.7%), while Cromolyn was considerably the least popular (19.7%). This result is consistent with Maselli and Peters (2018) research that found that albuterol was the most commonly utilized bronchodilator for treating acute asthma.27 Its popularity comes from its ability to act quickly, its half-life of 4–6 hours, and its low cost.
Guidelines for asthma treatment are viewed as a crucial and useful tool for ensuring that all aspects of patient care are based on the latest scientific knowledge, efficient, and secure. These recommendations were created to assist healthcare professionals and patients make the best decisions possible for asthma management by selecting the most effective treatment options for each unique clinical circumstance.28
The most critical finding in our study is that 61.7% of participants answered the possibility of using albuterol (SABA) alone in the treatment of mild asthma; this opposes the recommendation of GINA 2019, which states that
For safety, GINA no longer recommends treatment with short-acting beta2-agonists (SABA) alone. There is strong evidence that SABA-only treatment, although providing short-term relief of asthma symptoms, does not protect patients from severe exacerbations, and that regular or frequent use of SABA increases the risk of exacerbations.
GINA now recommends that all adults and adolescents with asthma receive either symptom-driven (in mild asthma) or daily low-dose ICS-containing controller treatment to reduce their risk of serious.7
The present study discovered that medical websites and mobile applications are the most frequently utilized sources. In contrast, CTS is the less popular source for the treatment and management of asthma illness. Additionally, the following usage patterns were observed when individuals used the GINA as a source of information on asthma: 18.3% of respondents replied “no”, 34.0% said “yes, occasionally”, and 47.7% said, “yes, always”. In light of this, research by Alatawi and Alsayed from 2021 revealed that physicians and nurses strive to learn more about asthma by utilizing books and personal experience, their preferred learning tools.29 Recent research has found a substantial correlation between awareness of asthma recommendations and an elevated level of asthma management.30
The results of this survey indicated that 47.3% of participants were aware of the GINA changes and revisions made in 2019. A further finding revealed that, on average, 63.7% ± 5.7% of physicians confirmed managing asthma according to GINA recommendations.21 Roman-Rodriguez et al also stated that only a low proportion (26%) of physicians followed the asthma guidelines in a prior study conducted in Spain.31 Amorha et al also reported that only 11.2% of community pharmacists successfully implemented the GINA report. The fact that each nation has its own policies and procedures for managing diseases may cause a variance in how well asthma standards are followed across different countries.13
The Ministry of Health in Jordan uses primary healthcare (PHC) institutions to handle non-communicable disorders like asthma. Jordanian PHC clinics encounter various challenges, including a high patient load and an increasing workload for healthcare staff. Therefore, both patients and healthcare professionals must have a thorough understanding of how to treat and manage asthma since doing so will relieve some of the burden on them and decrease the cost and length of treatment.2 This was demonstrated by recent research in Jordan by AL-awaisheh et al, who stated that pharmacists could dramatically raise patients’ ACT scores, QoL ratings, and asthma inhaler technique through a practical teaching intervention.3 Additionally, Alsayed’s (2023) study stated that a partnership with healthcare providers must be established for asthma patients to manage their disease effectively. This will allow the patient to follow the medical professional’s advice for managing their condition. It is also essential to have education from a PharmD, pharmacist, respiratory therapist, and nurse to ensure awareness of the treatment strategy and underline the need to adhere to newly developed respiratory equipment.8 All of these point to the necessity of having access to appropriate care, adhering to medication instructions, having doctor examinations, and educating patients and healthcare professionals to improve asthma management.
Nevertheless, there are certain drawbacks to this study. The ability to demonstrate a correlation between the study variables and the results was restricted due to using a cross-sectional survey research methodology. Furthermore, other limitations include the relatively small sample size and low rate of senior physicians agreeing to participate.
Conclusion
This study showed that Jordanian healthcare professionals understand the nature of asthma, its symptoms, and its diagnoses. However, a substantial number of survey participants lack adherence, awareness, and understanding of the GINA guidelines and recommendations about asthma management, despite almost half of the participants using the GINA as a medical reference for asthma disease, but this is not entirely consistent with their answers to treatment and medication plan section in the questionnaire. The main and effective solution is to hold free training courses in medical centers for Jordanian healthcare professionals to educate and facilitate understanding of the instructions and recommendations issued by GINA.
Adherence to global guidelines, like GINA, is paramount for ensuring optimal asthma management, especially in a healthcare context such as Jordan. To enhance compliance among healthcare professionals, a multifaceted approach is recommended. First and foremost, continuous education and training programs should be implemented to familiarize healthcare providers with the latest GINA recommendations, emphasizing their importance in improving patient outcomes. Additionally, integrating these guidelines into the standard operating procedures of healthcare institutions, accompanied by regular audits, can reinforce adherence. Establishing collaborative networks for knowledge exchange and creating local adaptations of the guidelines that consider Jordan’s specific healthcare landscape and patient demographics can further facilitate implementation. Emphasizing the benefits of guideline adherence in terms of patient well-being and healthcare efficiency is crucial for garnering sustained commitment from healthcare professionals in Jordan.
More research is required to assess the adherence to the evidence-based recommendations and evaluate the impact of training courses.
Acknowledgments
The authors would like to thank the participants in this study and those who validated the questionnaire.
Author Contributions
The corresponding author supervised the research and was involved in all of the research steps. All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Global Initiative for Asthma. Global strategy for asthma management and prevention; 2023. Available from: http://www.gi-nasthma.org.
2. Dahmash EZ. Physicians’ Knowledge and Practices Regarding Asthma in Jordan: a Cross-Sectional Study. Front Public Health. 2021;9:712255. doi:10.3389/fpubh.2021.712255
3. AL-awaisheh R, Alsayed AR, Basheti IA. Assessing the pharmacist’s role in counseling asthmatic adults using the correct inhaler technique and its effect on asthma control, adherence, and quality of life. Patient Preference Adherence. 2023;Volume 17:961–972. doi:10.2147/PPA.S395258
4. Nour A, Alsayed AR, Basheti I. Prevalence of asthma amongst schoolchildren in Jordan and staff readiness to help. MDPI. 2023;183:1.
5. Kommaraju K, Latifi M. Outpatient management of asthma in adults: a snapshot of the 2020 GINA report. Clevel Clin J Med. 2021;88(7):377–380. doi:10.3949/ccjm.88a.20167
6. Abuzakouk M, Jacob S, Ghorab O. Are the Global Initiative for Asthma (GINA) guidelines being correctly used to diagnose severe asthma in the UAE? Cureus. 2020;12(12). doi:10.7759/cureus.12278
7. Global Initiative for Asthma. Global strategy for asthma management and prevention; 2019. Available from: http://www.gi-nasthma.org.
8. Alsayed AR. Illustrating how to use the validated alsayed_v1 tools to improve medical care: a particular reference to the global initiative for asthma 2022 recommendations. Patient Preference Adherence. 2023;Volume 17:1161–1179. doi:10.2147/PPA.S403239
9. Chapman KR, An L, Bosnic-Anticevich S, et al. Asthma patients’ and physicians’ perspectives on the burden and management of asthma. Respir Med. 2021;186:106524. doi:10.1016/j.rmed.2021.106524
10. Holst SS, Sabedin E, Sabedin E, Vermehren C. A shift in asthma treatment according to new guidelines: an evaluation of asthma patients’ attitudes towards treatment change. Int J Environ Res Public Health. 2023;20(4):3453. doi:10.3390/ijerph20043453
11. Gruffydd-Jones K, Hansen K. Working for better asthma control: how can we improve the dialogue between patients and healthcare professionals? Adv Ther. 2020;37(1):1–9. doi:10.1007/s12325-019-01131-0
12. Said ASA, Hussain N, Kharaba Z, Al Haddad AHI, Abdelaty LN, Hussein RRS. Knowledge, attitude, and practice of pharmacists regarding asthma management: a cross-sectional study in Egypt. J Pharm Policy Pract. 2022;15(1):35. doi:10.1186/s40545-022-00432-0
13. Amorha KC, Idoko KE, Okonta MJ, Ukwe CV. Knowledge and practice of the global initiative for asthma report among community pharmacists in a Nigerian State. Pan Afr Med J. 2020;37:83. doi:10.11604/pamj.2020.37.83.18897
14. Adeniyi B, Ilesanmi O, Obaseki D, Desalu O, Betiku B, Erhabor G. Relationship between knowledge and quality of asthma care among physicians in South-West Nigeria. Niger J Clin Pract. 2017;20(5):566. doi:10.4103/1119-3077.206363
15. Alsayed AR, Abed A, Khader HA, et al. Molecular accounting and profiling of human respiratory microbial communities: toward precision medicine by targeting the respiratory microbiome for disease diagnosis and treatment. Int J Mol Sci. 2023;24(4). doi:10.3390/ijms24044086
16. Al-Dulaimi A, Alsayed AR, Maqbali MA, Zihlif M. Investigating the human rhinovirus co-infection in patients with asthma exacerbations and COVID-19. Pharm Pract. 2022;20(2):2665. doi:10.18549/PharmPract.2022.2.2665
17. Alsayed AR, Abed A, Abu-Samak M, Alshammari F, Alshammari B. Etiologies of acute bronchiolitis in children at risk for asthma, with emphasis on the human rhinovirus genotyping protocol. J Clin Med. 2023;12(12):3909. doi:10.3390/jcm12123909
18. Alsayed AR, Abed A, Jarrar YB, et al. Alteration of the respiratory microbiome in hospitalized patients with asthma–COPD overlap during and after an exacerbation. J Clin Med. 2023;12(6):2118. doi:10.3390/jcm12062118
19. Alsayed AR, Al-Dulaimi A, Alkhatib M, Al Maqbali M, Al-Najjar MAA, Al-Rshaidat MM. A comprehensive clinical guide for Pneumocystis jirovecii pneumonia: a missing therapeutic target in HIV-uninfected patients. Expert Rev Resp Med. 2022;16(11–12):1167–1190. doi:10.1080/17476348.2022.2152332
20. Alsayed AR, Talib W, Al-Dulaimi A, Daoud S, Al Maqbali M. The first detection of Pneumocystis jirovecii in asthmatic patients post-COVID-19 in Jordan. Bosn J Bas Med Sci. 2022;22(5):784. doi:10.17305/bjbms.2022.7335
21. Dairi MS. Physicians’ knowledge and practices regarding asthma: a cross-sectional study in Saudi Arabia. Int J Gene Med. 2022;Volume 15:6671–6680. doi:10.2147/IJGM.S369306
22. Almutawa FN, Al-Mutairy G, Al-Arada N, Kamel MI. Perception of primary care physicians about guidelines of bronchial asthma. Alexand J Med. 2019;50(1):17–24. doi:10.1016/j.ajme.2013.05.002
23. Assiri HA, Alkhaldi YM, Alsaleem SA, Alqarni HM. Knowledge, attitude and practices of PHC physicians in Aseer region regarding management of acute asthma. J Family Med Prim Care. 2021;10(5):1882–1889. doi:10.4103/jfmpc.jfmpc_1418_20
24. Alsayed AR, Abu-Samak MS, Alkhatib M. Asthma-COPD Overlap in Clinical Practice (ACO_CP 2023): toward Precision Medicine. J Person Med. 2023;13(4):677. doi:10.3390/jpm13040677
25. Bridgeman MB, Wilken LA. Essential role of pharmacists in asthma care and management. J Pharm Pract. 2021;34(1):149–162. doi:10.1177/0897190020927274
26. Gogtay J, Laouar L, Gaur V. Preference of diagnostic tools, medications, and devices for asthma management: a survey of doctors in Algeria. Perspect Clin Res. 2019;10(2):67–72. doi:10.4103/picr.PICR_63_18
27. Maselli DJ, Peters JI. Medication regimens for managing acute asthma. Respir Care. 2018;63(6):783–796. doi:10.4187/respcare.05953
28. Novembre E, Giovannini M, Barni S, Mori F. From the Global Initiative for Asthma report and asthma guidelines to real-life asthma control: is there room for improvement? Ital J Pediatr. 2022;48(1):110. doi:10.3390/ijms24044086
29. Alatawi A, Alsayed B. Assessment of Asthma Knowledge, Attitudes, and Practice among Health professionals at two hospital settings in Tabuk region, Saudi Arabia. Indian J Med Forensic Med Toxicol. 2021;15:3.
30. Levy ML, Bacharier LB, Bateman E, et al. Key recommendations for primary care from the 2022 Global Initiative for Asthma (GINA) update. NPJ Prim Care Respir Med. 2023;33(1):7. doi:10.1038/s41533-023-00330-1
31. Roman-Rodriguez M, Molina-Paris J, Sanchez AF, et al. Compliance with the clinical guidelines for managing asthma by primary care physicians: an ambispective observational study. Rev Clín Española. 2021;221(4):207–216. doi:10.1016/j.rceng.2019.11.006
 © 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2024 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.