Back to Journals » Nutrition and Dietary Supplements » Volume 12
Knowledge and Dietary Practices on Vitamin A and Iron Among Maasai Pregnant Women: A Mixed-Method Study, Ngorongoro, Tanzania
Authors Mshanga N ![]() , Martin H, Petrucka P
, Martin H, Petrucka P
Received 27 May 2020
Accepted for publication 14 August 2020
Published 18 September 2020 Volume 2020:12 Pages 179—188
DOI https://doi.org/10.2147/NDS.S264592
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Chandrika Piyathilake
Naelijwa Mshanga,1 Haikael Martin,1 Pammla Petrucka2
1Department of Food Biotechnology and Nutrition Sciences, The Nelson Mandela African Institution of Science and Technology, Arusha, Tanzania; 2College of Nursing, University of Saskatchewan, Saskatoon, Canada
Correspondence: Naelijwa Mshanga Email [email protected]
Background: Provision of micronutrients knowledge is important during pregnancy as it informs mothers what to eat and avoid, to ensure sufficient micronutrient absorption by the mothers and fetuses. Most studies focus on general nutrition knowledge and dietary practices, but there is minimal known about micronutrient knowledge especially in pastoral societies. Therefore, the aim of this study was to explain the current micronutrient knowledge and dietary practices of pregnant women in this unique pastoral society.
Methods: This is a mixed-method study that involves focus group discussions and questionnaires in assessing the micronutrient knowledge and frequency micronutrients dietary practices of Maasai pregnant women from one week to thirty-six weeks pregnant. Chi-square test and descriptive statistics, such as percentages, frequency distribution and measures of central tendency, were used to assess socio-demographic data, micronutrients knowledge and frequency of micronutrients dietary practices and the comparison between knowledge and dietary practices, while inductive thematic content analysis was used to analyze qualitative data.
Results: In total, 140 questionnaires were completed with a response rate of 100% and 32 participants drawn from this group attended one of four focus group discussions. The study found that most participants had good knowledge of dietary iron, while less than a quarter (24.3%) had good knowledge of vitamin A. Moreover, there was a statistical significance difference (P=0.043) between knowledge and dietary practices. Low dietary micronutrient intake was primarily due to cultural restrictions, prohibition in cultivating and unavailability of micronutrients rich foods in this geographical area.
Conclusion: The majority of the study participants had good knowledge of iron compared to vitamin A; however, they do not translate the knowledge in dietary practices. Therefore, the Government of Tanzania through Ministry of Education and Health should introduce different interventions to increase micronutrients knowledge and practices in pastoral societies.
Keywords: micronutrients, pregnant women, pastoralists, dietary iron, vitamin A, Tanzania
Background
Micronutrients include vitamin and mineral nutrients needed in small amounts for body growth, maintenance, and metabolism.1 The recommended dietary intake (RDI) of few micronutrients increases during pregnancy due to the demands of the growing fetus and elevated metabolic activities of the pregnant woman.2 Adequate intake of micronutrients during pregnancy reduces the risks of low birth weight, neural tube defects, non-communicable diseases (hypertension, cardiovascular disorders, and diabetes) later in life, as well as iron deficiency anemia in mother and baby, maternal miscarriage, stillbirth, and post-partum hemorrhage which could lead to death.3
Micronutrients are found in almost all foods but are especially plentiful in fruits and vegetables.4 Eating adequate fruits and vegetables addresses different micronutrient deficiencies, rather than micronutrient supplementation.5 A Malaysian study found a significant association between intake of fruits and vegetables during pregnancy with an increase of infant birth weight.6 Another study done in Norway showed a significant reduction in preterm delivery among pregnant women who consumed vegetables, fruits, water, and bread rich in fiber compared to pregnant women who consumed starchy and sweetened foods.7 Higher dietary intake of iron and calcium among Tanzanian pregnant women has been significantly related to reduction of preterm delivery, stillbirth, and neonatal mortality.8
Although vitamin A is not a vitamin of interest during pregnancy, the current research decided to study it after different studies reported 100% of vitamin A deficiency to women of reproductive age and pregnant women in this population.9,10 Further, the current study aimed to inform the level of knowledge on maternal vitamin A to the intervention study for an aim of formulating nutrition education and food-basket intervention.10 Most important, the use of plant-based vitamin A foods and nutrition education has been seen to increase serum retinol levels to the vitamin A deficient population without toxicity.10,11
Knowledge of nutrition has a direct link between dietary intake and food choices;12 moreover, nutrition and/or health knowledge can be highly attributed to the level of education and/or cultural beliefs.13,14 A study done by Muthayya et al, reported that, highly educated participants showed increased diversity in their diet compared to their lower educated cohort.15 Micronutrient deficiency in low and middle-income countries (LMIC) often relates to lack of knowledge regarding nutrient intake.3 Furthermore, micronutrient deficiency among pregnant women can be due to cultural beliefs, poor eating habits, and food insecurity.16
The current study was conducted in the rural, remote Maasai communities of Misigyo and Olbalbal in Northern Tanzania. These communities live within the Ngorongoro Conservation Area (NCA), a geographic region with tight restrictions on agricultural cultivation imposed by the Tanzanian government to protect the sensitive ecosystem. Ninety-five percent of residents in NCA are Maasai,17 who are traditionally pastoralists and speak the Maa language.18
Like many cultures, the Maasai have traditional beliefs and taboos that guide pregnant women on what they should, and should not eat during pregnancy.19 One such belief is reducing the portions of maternal diet during the second and third trimesters with the purpose of delivering smaller, lower birth-weight babies, as it is believed that bigger babies increase complications during delivery.9 The complications are being experienced because these pregnant women give birth at home as, it is estimated that 90% of pregnant women attend ANCs; however, only 7% give birth in these clinics.20 Lennox et al (2017) showed these beliefs have a direct impact on dietary behaviors and health of Maasai pregnant women.21
Moreover, food insecurity amongst the Maasai is subject to seasonality and varies in intensity and is somewhat iterative as low milk production leads to overconsumption/reliance on staple foods, such as maize.22 Although pastoralists have a good experiential understanding of the seasonality and nutritive values of many of the local plants,23 this knowledge is heavily focused on animal husbandry applications and past practices, which indirectly contributes to human food supplies.23,24
Therefore, this study quantitatively and qualitatively assessed micronutrient knowledge, frequency of micronutrients dietary intake, and beliefs specifically associated with micronutrient intake among Maasai pregnant women. Micronutrient knowledge studies in pastoral societies are not reflected in the evidence; hence, this study will contribute to a better understanding of the micronutrient knowledge and dietary needs of pregnant women in this unique pastoral society. Findings from this study will potentially aid other researchers to develop a means for micronutrient knowledge translation in pastoral societies.
Methods
Study Area and Design
This study was conducted in NCA, Ngorongoro District located in Northern Tanzania. Ngorongoro District is one of the six districts in Arusha Region, which has a population of 174,278 of which 91,668 are female with 46,750 being women of reproductive age.25 Ngorongoro District has 28 wards, two private hospitals, and each ward has one dispensary which are all Government facilities except three dispensaries. These dispensaries have antenatal clinics (ANC) and they also provide mobile clinics in remote communities, which most pregnant women attend ANC but do not delivery in those clinics. The study was done at Misigyo and Olbalbal wards, which were purposively selected as they are part of Maasai Agri-Health Cooperative program, one of the programs offered by Green Hope Organization. The aim of this program was to develop a model that address both poverty and maternal malnutrition, by involving traditional birth attendants (TBAs) in farming activities (vegetable gardens) for better health and wellbeing of the TBAs and their pregnant clients. The study was conducted specifically at the Olbalbal clinic in Olbalbal ward and Migisyo clinic together with Mobile clinics for the remote villages in Misigyo ward.
The study utilized a mixed methods cross-sectional study design using a questionnaire and focus group discussions to assess current micronutrient knowledge and dietary practices among pregnant Maasai women living in NCA.
Study Population and Selection Criteria
The current study involved Maasai pregnant women from one week to thirty-six weeks who visited ANCs as well as mobile clinics and are residents of Misigyo and Olbalbal wards. Moreover, pregnant women who experienced complications during pregnancy such as; pre-eclampsia and persistent nausea and vomiting were excluded from the study.
Sample Size
Quantitative Method
Sample size was calculated from the standard formula for epidemiological studies [n= [z2*P*(1-P)]/d2]; where n is the total number of the sample, d is the absolute precision (5), CI is the confidence interval (CI= 95%), Z is standard normal distribution (Z=1.96), and P is the proportion of maternal iron deficiency in Tanzania (P= 90%).26 A minimum sample of 138 participants was calculated; thereafter, a total of 150 pregnant women were invited to participate while 140 voluntarily agreed to participate in the questionnaire. Although the study sample size was calculated using the iron deficiency proportion, the sample study was able to achieve a 95% CI of (1.56–0.14) and (0.48–0.14) for the proportion of 0.71 and 0.17 knowledge of iron and Vitamin A, respectively.
Qualitative Method
Thirty-two participants from among those who participated in the questionnaire consented to participate in the FGDs. Participants for FGDs were selected based on their age, gravidity (number of pregnancies), and parity (number of deliveries). Based on gravidity, 15,12 and 5 participants were grouped as gravida 1–3, 4–6 and >7 respectfully while based on parity 5, 17, 7 and 3 participants were grouped as parity 0, 1–3, 4–6 and >7 respectfully. There were four groups each containing eight participants.
Sampling Technique and Study Procedures
Consecutive sampling technique was used where all pregnant women who visited ANCs and mobile clinics were invited to participate in the questionnaire interview. Before the study began, invitations to join the study were made to the churches, ANCs and mobile clinics whereas, all interested participants were informed to visit the clinics for enrollment to the study. The invitations messages comprised of the place where participants will be enrolled, criteria for enrollment such as be a Maasai, pregnant women from 1 week to 36-weeks pregnancy living in Olbalbal and Misigyo ward and the study period. During participant recruitment, measurements, such as last normal menstruation calculations and positive pregnancy test, were used to confirm pregnancy, while fundal height measurement estimated pregnancy age in weeks to fit the inclusion criteria.
Ethics Approval and Consent to Participate
Ethical clearance from the National Institute of Medical Research (NIMR) (NIMR/HQ/R. 8a/Vol. 1X/2708) was obtained and a permit was provided from NCAA (Ngorongoro Conservation Area Authority). This study was conducted in accordance with the declaration of Helsinki. The study was explained by the researcher and translated in Maa by a research assistant to potential participants before consent was sought. All those who willingly accepted to participate signed a written informed consent and for those who could not write, they were requested to press their right thumb in an ink pad and adhere it to the consent form. For participants less than 18 years old, both parents/guardians/husbands signed consent forms and participants (<18 years) signed assent forms were collected before the study began. Furthermore, all participants consented their anonymized responses to be included in the publication.
Data Collection Tools
Quantitative Study
In the quantitative arm of the study, participants were grouped into three categories: participants who can read and write in Swahili (n=20), participants who knew Swahili but do not know how to read and write (n=40), and participants who knew Maa but could not read and write (n= 80). Participants who knew how to read and write in Swahili filled the questionnaires by themselves. Participants who knew Swahili but do not know how to read and write the researcher read the questions and wrote answers for them, while participants who understood Maa but cannot read and write a nurse who knew both Swahili and Maa read and wrote answers for them.
The validated Food and Agriculture Organization (FAO) 2014 (KAP) questionnaire was comprised of multiple choice and open-ended questions translated into Swahili language. The questionnaire was administered by ten trained researchers and two nurses who knew both Swahili and Maa languages. The questionnaire had five parts including socio-demographic information, general micronutrient knowledge, specific knowledge on iron as well as vitamin A, and frequency of dietary intake of micronutrient rich foods. Dietary practices were assessed using a food frequency questionnaire (FFQ) which had the following scale; never, seldom (less than once a month); 1–3 times per month; 1–2 times per week; 3–4 times per week; and daily. The food frequency questionnaire was developed from one food group (fruits and vegetables) which contain ten different options available in Karatu and Ngorongoro District.
Qualitative Study
The researcher provided guiding questions (Appendix 1) and the FGDs were moderated by a nurse who knew both Swahili and Maa language, and an experienced notetaker noted down all the discussions and recorded the conversations at the same time. Participants in all FGDs, chose to use the Maa language and the scripts were later translated to Swahili language; thereafter, the researcher translated the scripts to English. Immediately after each FGD, both the moderator and the notetaker expanded the notes and summarized key issues raised before conducting the next session. The 32 FGD participants were involved for between 55 and 60 minutes in their respective grouping.
Statistical Analysis
Quantitative Data Analysis
Both sections on knowledge of iron and vitamin A had three parts and each part has ten questions. Each respondent was given a score based on the number of correct responses provided in each part. The knowledge score of the population was calculated for each part by dividing the total number of correct responses by the number of respondents who answered the particular question in the respective part. Thereafter the percentage was calculated in each part and categorized as; 75–100% having good knowledge, 74–50% moderate knowledge and 49–0% poor knowledge. These methods were adapted from FAO guidelines for assessing nutrition-related knowledge, attitudes and practices.27
The Statistical Package for Social Science (SPSS™) Version 25 and Graph Pad Prism ™ Version 7 were used to analyze quantitative data. Descriptive statistics, such as percentages, frequency distribution and measures of central tendency, were used to assess socio-demographic data, general micronutrient knowledge, knowledge on dietary iron and vitamin A, symptoms of iron and vitamin A deficiency, as well as consequences of iron deficiency/anemia. Analysis of food frequency questionnaire was performed to understand the dietary intake of pregnant women. Moreover, chi-square test was performed to compare the association between micronutrients knowledge and dietary intake among the study participants. A p-value of below 0.05 confirms an association between two variables.
Qualitative Research Analysis
The recorded voice-note, which was in Maa language, was transcribed and translated into Swahili language by an experienced Maasai research assistant. The researcher (Principal Investigator) analyzed the transcripts using inductive thematic content analysis which involved reading the scripts several times to identify similar as well as differing issues emerging in the scripts and creating short phrases that reflected what had been narrated.28,29 Thereafter, codes were generated from phrases having similar content across all FGDs and sorted into themes. The themes were shared and agreed upon by all co-authors. Verbatim quotes from the scripts were chosen and are presented in the result section together with quantitative data reporting.
Triangulation of quantitative and qualitative data was used to ensure data validation and to provide a clear context in interpretation for results.
Results
Socio-Demographic Characteristics of Respondents
A total of 140 Maasai pregnant women participated in the study. Half (50%) of the participants were within the 25–29 age range and nearly all (97.1%) were married. The majority (69.3%) of the study participants did not have formal education, and more than half of the participants reported mother in laws as their nearest female supporters. Table 1.
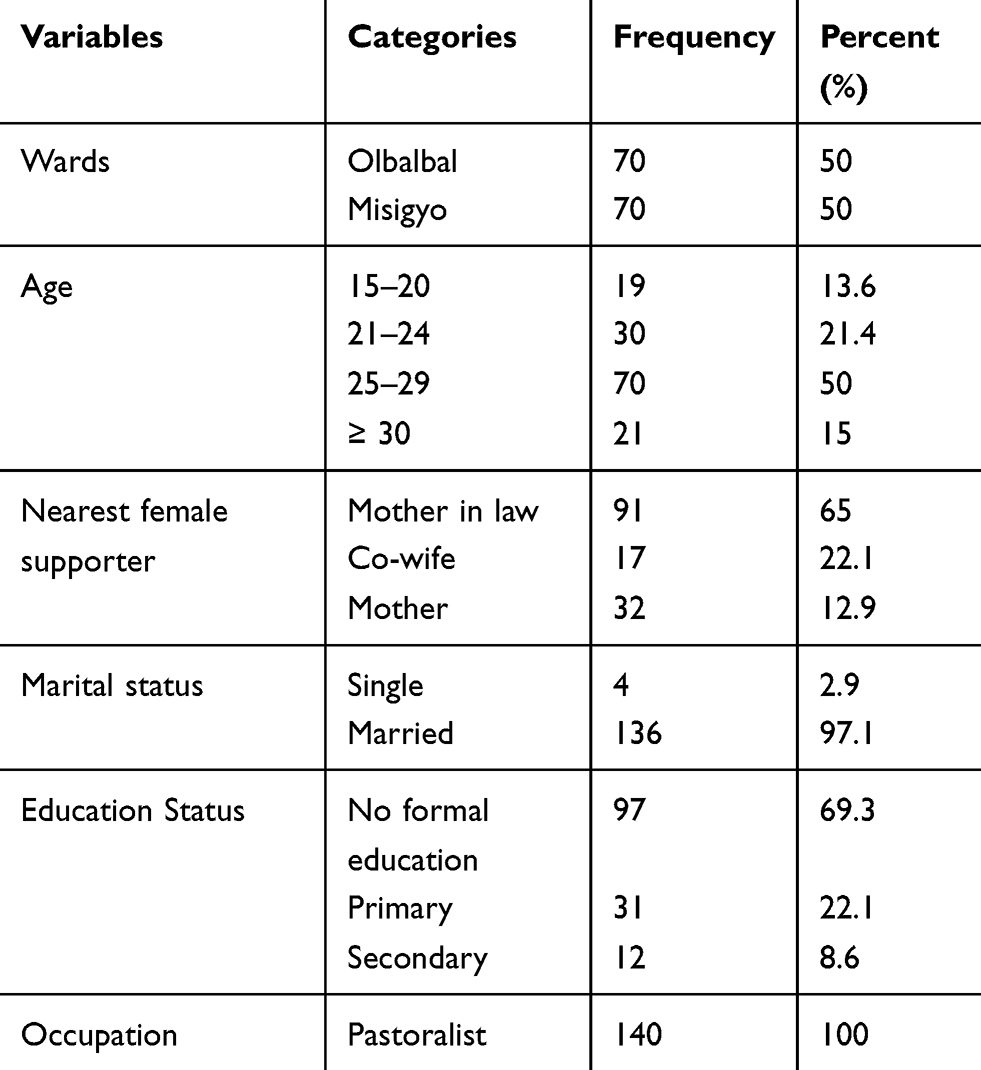 |
Table 1 Socio-Demographic Characteristics of Study Participants (n=140) |
Through focus group discussion, seven themes were generated;
- Vitamin A and C helps in eye visioning;
- Swollen legs and dizziness are symptoms of anemia;
- Failure to push the baby can be caused by low blood count;
- Delivery of low birth weight babies can be caused by food restriction;
- TBAs, nurses and school teachers are our nutrition informants;
- A pregnant woman ate once in a day; and
- Vegetables smell bad.
Nutrition and Health Knowledge
Knowledge versus Belief on Importance of Fruits and Vegetables Consumption During Pregnancy
The majority of pregnant women had good knowledge (86.4%) of the importance of eating fruits and vegetables during pregnancy. Over one-third of participants stated that adequate dietary intake of fruits and vegetables can provide energy to the mother (39.3%), and increase fetal growth (37.9%), whereas a few (5%) indicated that these foods would improve health, produce heat (1.4%), and increase blood volume (5%) during pregnancy.
One FGD participant mentioned that fruits and vegetables are foods that treat anemia although she did not know about vitamins:
“I know that fruits and vegetables treat anemia, but I don’t know what vitamins are, their sources and the role they play in the body” [Misigyo-1st Group-P7].
However, the majority of participants believed that eating vegetables increases blood during pregnancy as stated in the narrative:
“Dietary intake of vegetables increases blood during pregnancy” [Olbalbal-1st and 2nd Groups-Many].
Knowledge versus Belief on Vitamin A and Iron
Most of the participants had good knowledge of iron and iron deficiency anemia but only one-quarter had good knowledge of vitamin A and vitamin A deficiency (Table 2).
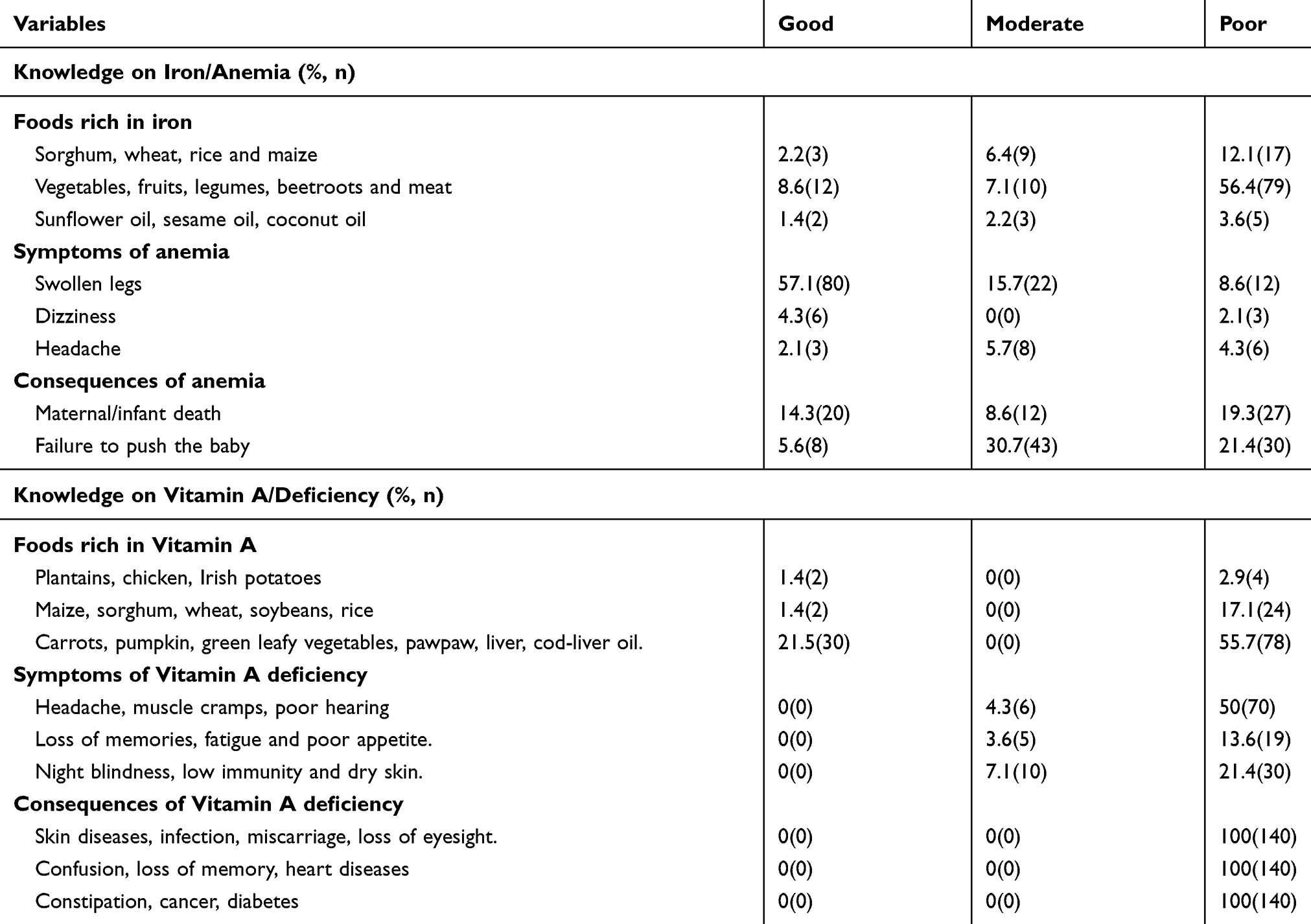 |
Table 2 Micronutrient Knowledge Among Maasai Pregnant Women |
The few participants who knew about vitamin and the effect of vitamin deficiency had attended secondary school. One such FGD participant mentioned that her biology teacher taught her that:
“Vegetables have vitamins such as Vitamin A and C which helps someone to have good eyesight during pregnancy” [Olbalbal-2nd Group-P4].
Knowledge versus Belief on Symptoms and Consequences of Anemia During Pregnancy
More than half (57.1%) of participants said swollen legs is a symptom of anemia and nearly one-third (14.3%) recognized maternal and/or infant death as the worst result of iron deficiency anemia during pregnancy. The FGD participants further described more symptoms and consequences of anemia during pregnancy in stating:
“I came to realize that the swollen legs I had during my last pregnancy was due to low blood count” [Olbalbal & Misigyo-2nd Groups-Many].
Some FGD participants associated failure to push the baby and anemia as stated by one woman:
“Pregnant women can get complications during delivery due to lack of energy to push the baby caused by low blood count” [Olbalbal-1stGroup-P6].
Another participant reiterated that:
“If you have low blood count you can start feeling dizzy, have swollen legs and become weak” [Misigyo-1st Group-P3].
Health Outcomes of Cultural Dietary Restrictions During Pregnancy
The majority of women across all FGDs knew the health outcomes of cultural dietary restrictions. They expressed their different experiences on health outcomes after reduced dietary intake during pregnancy as:
“After food restriction during pregnancy, I deliver(ed) a low birth weight baby with poor health” [Olbalbal-1st Group-P7].
“Due to low dietary intake and food restrictions during my first pregnancy, I failed to push the baby since I had no energy to do so” [Misigyo-2nd Group-P8].
Source of Nutrition Knowledge During Pregnancy
More than half of the participants mentioned traditional birth attendants (56%) while 11.9% of the participants indicated nurses as their primary source of nutrition information. A few participants stated schools (0.7%) and radios/televisions (1.4%) provided them with nutrition and health information.
This pattern was further confirmed during the FGD with the majority of pregnant women mentioning their TBAs as their informants:
“I was advised by a traditional birth attendant on dietary intake during pregnancy” [Olbalbal & Misigyo-1st and2nd Group-Many]
while a few mentioned nurses, and teachers as their primary sources of nutrition information:
“I was advised to take vegetables, beans and fruits by a nurse” [Misigyo-2nd Group-P1]
“I learned about anemia and health issues during pregnancy when I was in school” [Olbalbal-2nd Group-P4]
Dietary Practices During Pregnancy
Foods Mostly Eaten During Pregnancy
Almost half (49.8%) of the pregnant women consumed porridge, while others ate wheat (15%), rice (16.2%), and beans (19.1%). One participant explained her own restricted dietary intake:
“I drink porridge once in a day and do a lot of activities in order to reduce weight” [Misigyo-2nd Group-P3].
One woman stated the reason for reducing weight during pregnancy:
“As a Maasai pregnant woman, I am not allowed to eat beans (legumes), meat, milk, rice in order to cut off weight and have an easy delivery” [Olbalbal-1st Group-P1].
Furthermore, one participant explained what Maasai women eat during pregnancy included:
“Pregnant women drink porridge, water or eat boiled maize without adding anything once in a day to survive” [Misigyo-1st Group-P3].
Dietary Intake of Fruits and Vegetables
More than half (59.5%) of pregnant women reported consuming naturally grown African nightshade (mnavu) as one of the vegetables despite its foul odor; while less than 15% of the participant consumed fruits during pregnancy (Figure 1).
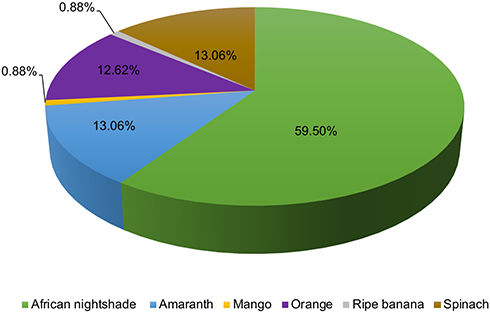 |
Figure 1 Fruits and vegetables consumed 3–4 times per week. More than half of the study participants (59.5%) reported consuming African nightshade “a wild vegetable” while 13.06% of the study population consumed spinach and amaranth 3–4 times a week. Moreover, 12.62% of the participants revealed taking oranges while less than 1% took ripe bananas and mango 3–4 times a week. |
“You have come in a rainy season, that’s why you find us eating wild vegetables (wild African nightshade) as they grow during this season” [Olbalbal&Misigyo-1st Groups-Many]
“I know it is important to take vegetables during pregnancy, but I don’t consume them because they smell bad” [Olbalbal-2nd Group-P5]
Generally, the chi-square test found an association (P=0.043) between nutrition knowledge and dietary practices among the study participants, thus nutrition knowledge of the participants has a direct link with their dietary practices.
Discussion
This study revealed that, overall the participants had good knowledge of micronutrient, although they do not translate this knowledge into dietary practices. The majority of participants had better knowledge on iron compared to Vitamin A, with knowledge of Vitamin A linked to secondary school education. These findings align with the Tanzania secondary school curriculum30 which incorporates numerous nutrition and health topics (ie, digestive system and its functions, food groups, nutrients and nutritional deficiencies (minerals, vitamins, protein, carbohydrate)) while primary school education covers general nutrition (ie, food groups).
In this study, participants demonstrated good knowledge of micronutrient, but they did not consume micronutrient rich foods other than African nightshade during the rainy season, which occurs from March to May each year. Moreover, participants from this pastoral community had knowledge in micronutrients specifically iron; however, those who had secondary education knew Vitamin A as found in green vegetables and fruits having red or orange color which helps in eyesight/improves vision and body immunity. This is a unique finding as most previous studies did not suggest adequate micronutrient knowledge in a pastoral society.9,18,31–33
Furthermore, participants mentioned swollen legs and maternal/infant mortality as the symptoms and consequences of anemia during pregnancy. These findings were in part supported by Klopovich who mentioned swollen legs as one of the symptoms of maternal chronic anemia/iron deficiency anemia.34 Additionally, Spronk et al (2014) revealed that anemia during pregnancy can lead to maternal and fetus mortality.12 Knowing the symptoms and consequences of anemia especially to Maasai pregnant women ensures successfully knowledge transformation and a good starting point for health workers to advice pregnant women to consume iron rich foods and supplements for a healthy pregnancy and future generation.
Most participants chose TBAs (local midwives) as their informants on nutrition/health information, which aligns with a study done in Kenya that reported TBAs to be good advocates of nutrition among pregnant women advising them to take fruits and vegetables in order for them to increase blood and energy.35 Traditional Birth Attendants obtained their knowledge based on experience from older TBAs and informal knowledge acquired through the traditions and practices of the communities where they originated.36 Other studies should be done to study the source of TBA’s traditional nutrition knowledge as, the nutrition knowledge they provide aligns with nutrition sciences.
Poor dietary micronutrient intake in this pastoralist society may be due to cultural dietary restrictions, poor attributes of the foods (ie, bad smell), lack of fresh and/or minimal availability of vegetables and fruits in local markets. Furthermore, all NCA residents are prohibited to cultivate in conservation areas as per Ngorongoro Act of 1957 (Part IV, No 25), due to protection of sensitive nature of ecosystem present in this area.37 Therefore, lack of micronutrients foods, cultural food restriction, and prohibition to cultivate foods in NCA highly affects pregnant women compared to other NCA residents.
Findings from this study are similar to previous studies done in Ngorongoro which found low dietary intake during pregnancy to be associated with cultural restrictions and unavailability of fruits and vegetables.9,21 For those who consumed vegetables, African nightshade “mnavu” was commonly used. African nightshade is a wild vegetable (grows naturally during rainy season) and it is known to have high levels of potassium and iron.38 According to the nutritional content of African nightshade, dietary intake may increase the level of iron and potassium in pregnant women if prepared in a manner that preserves the nutrients.39 More studies should be done to reflect on the cooking practices of vegetables and fruits in regard to the micronutrients lost in order to come up with guidelines on how to prevent micronutrients loss in this community.
Study participants identified the health consequences of food restrictions during pregnancy, such as delivery of low birth weight babies and/or difficulty during childbirth (ie, no strength to push the baby). These consequences are highly associated with low dietary intake. Similarly, a study from Nepal depicted that low consumption of meat, beans, milk, green vegetables, and food taboos can lead to delivering low birth weight babies.40 Lack of strength in pushing the baby during delivery attributed to low dietary intake was contrary to the Lothian study (2009) that reported the lack of strength in pushing the baby is associated with unreleased catecholamine hormone caused by reduced production of oxytocin and endorphins hormones.41 Although there are myths concerning lack of strength in pushing the baby, scientific researches should be done to prove them.
This study had a number of limitations. The first limitation encountered was the communication barrier because the majority could only understand Maa. The need for translation may cause loss of meaning in some cases. This limitation was also expressed by Nes (2010) who found that a different language used during data collection may be understood differently when translated to another language for interpretation and publication.42 The second limitation was seen in the tool used in collecting food frequency. The Food Frequency Questionnaire takes account of foods eaten in a past month period which may be difficult for the participants to remember; therefore, an interviewer used memory probes and cues to improve accuracy of food data collected which may have led to over reporting. Lastly, data collection was done during the rainy season; this timing might have affected results due to differences in food intake (for example, during the rainy season wild vegetables like African nightshade is available for consumption).
Conclusion
The results of the present study show that the majority of participating pregnant Maasai women had good knowledge of iron and poor knowledge of Vitamin A; however, in both instances, they do not translate the knowledge they have into dietary practices. In order to ensure successful micronutrient knowledge attainment, young girls should be encouraged to continue with secondary school education, TBAs, as catalysts for knowledge transfer, should be given more nutrition trainings especially on micronutrients intake during pregnancy. Nutrition and/or health seminars should be provided to all population groups in the pastoral society. In addition, knowledge sensitization on the cost-effectiveness of healthy vegetables and fruits intake should be done to engender positive attitudes among pregnant women, lactating mothers, and other women of reproductive age (15–49). Furthermore, the Government of Tanzania should introduce micronutrient rich food-based interventions in communities living in NCA where there are significant deficits in access to sources of foods rich in micronutrients.
Abbreviations
ANC, antenatal clinics; FGD, focus group discussion; KAP, knowledge, attitude and practice; LMIC, low middle-income countries; NCA, Ngorongoro conservation area; RDI, recommended dietary intake; TBA, traditional birth attendants.
Data Sharing Statement
The datasets generated from the current study are available from the corresponding author on reasonable request.
Acknowledgments
The researchers acknowledge the participants who took part in this study and the health staffs (Nurses, clinicians) as well as Traditional Birth Attendants for their untiring support during the study period.
Author Contributions
All authors made a significant contribution to the conception, study design, acquisition of data, analysis and interpretation; took part in drafting, critically reviewing the article; gave final approval of the version to be published and agree to be accountable for all aspects of the work.
Disclosure
The authors declare that they have no competing interests in this work.
References
1. Miller DD, Welch RM. Food system strategies for preventing micronutrient malnutrition. Food Policy. 2013;42:115–128. doi:10.1016/j.foodpol.2013.06.008
2. Berti C, Biesalski H, Gärtner R, et al. Micronutrients in pregnancy: current knowledge and unresolved questions. Clin Nutr. 2011;30(6):689–701. doi:10.1016/j.clnu.2011.08.004
3. Darnton-Hill I, Mkparu UC. Micronutrients in pregnancy in low-and middle-income countries. Nutrients. 2015;7(3):1744–1768. doi:10.3390/nu7031744
4. Vicente AR, Manganaris GA, Sozzi GO, Crisoto CH. Nutritional Quality of Fruits and Vegetables: Postharvest Handling: A Systems Approach. Florkowski W, Shewfelt EL, Brueckner B, Prussia SE, editors. USA: Elesevier- Academic Press; 2009:57–106.
5. Oguntunde O, Charyeva Z, Cannon M, et al. Factors influencing the use of magnesium sulphate in pre-eclampsia/eclampsia management in health facilities in northern nigeria: a mixed methods study. BMC Pregnancy Child. 2015;15(1):1–8. doi:10.1186/s12884-015-0554-8
6. Loy SL, Marhazlina M, Azwany YN, Hamid JM. Higher intake of fruits and vegetables in pregnancy is associated with birth size. Southeast Asian J Trop Med. 2011;42(Suppl 5):1214–1223.
7. Englund-Ögge L, Brantsæter AL, Sengpiel V, et al. Maternal dietary patterns and preterm delivery: results from large prospective cohort study. BMJ. 2014;348(mar04 3):1446–1464. doi:10.1136/bmj.g1446
8. McMahon SA, Chase RP, Winch PJ, et al. Poverty, partner discord, and divergent accounts; a mixed methods account of births before arrival to health facilities in Morogoro Region, Tanzania. BMC Pregnancy Child. 2016;16(1). doi:10.1186/s12884-016-1058-x
9. Martin H, Petrucka P, Buza J. Determination of vitamins A, C and D status using serum markers and a 24-hour dietary recall among Maasai women of reproductive age. OALibJ. 2014;1(08):1–7. doi:10.4236/oalib.1100893
10. Mshanga N, Martin H, Petrucka P. Food-basket intervention to reduce micronutrient deficiencies among Maasai-pregnant women in Tanzania: a quasi-experimental study. J Hum Nutr Diet. 2019;32(5):625–634. doi:10.1111/jhn.12672
11. Hess SY, Thurnham DI, Hurrell RF. Influence of Provitamin a Carotenoids on Iron, Zinc and Vitamin a Status. Harvest Plus; 2005:1–31.
12. Spronk I, Kullen C, Burdon C, O’Connor H. Relationship between nutrition knowledge and dietary intake. Br J Nutr. 2014;111(10):1713–1726. doi:10.1017/S0007114514000087
13. Klevor MK, Adu-Afarwuah S, Ashorn P, et al. A mixed method study exploring adherence to and acceptability of small quantity lipid-based nutrient supplements (SQ-LNS) among pregnant and lactating women in Ghana and Malawi. BMC Pregnancy Child. 2016;16(1):1–11. doi:10.1186/s12884-016-1039-0
14. Gao H, Stiller CK, Scherbaum V, et al. Dietary intake and food habits of pregnant women residing in urban and rural areas of Deyang City, Sichuan Province, China. Nutrients. 2013;5(Suppl 8):2933–2954. doi:10.3390/nu5082933
15. Muthayya S, Rah JH, Sugimoto JD, Roos FF, Kraemer K, Black RE. The global hidden hunger indices and maps: an advocacy tool for action. PLoS One. 2013;8(6):1–12. doi:10.1371/journal.pone.0067860
16. Torheim LE, Ferguson EL, Penrose K, Arimond M. Women in resource-poor settings are at risk of inadequate intakes of multiple micronutrients. J Nutr. 2010;4(11):2051–2058. doi:10.3945/jn.110.123463
17. Swanson LA. Ngorongoro Conservation Area: Spring of Life. Dissertation Submitted in Fulfillment of Masters of Environmental Studies. USA: University of Pennsylavania; January 2007.
18. Chege PM, Kimiywe JO, Ndungu ZW. Influence of culture on dietary practices of children under five years among Maasai pastoralists in Kajiado, Kenya. Int J Behav Nutr Phy. 2015;12(1):1–6. doi:10.1186/s12966-015-0284-3
19. Martin H, Petrucka P, Buza J. Low macronutrients intake and associated factors among Maasai women of reproductive age in Ngorongoro conservation Area, Tanzania. Am J Res Commun. 2014;2:10–21.
20. Magoma M, Requejo J, Campbell OM, Cousens S, Filippi V. High ANC coverage and low skilled attendance in a rural Tanzanian district: a case for implementing a birth plan intervention. BMC Pregnancy Child. 2010;10(Suppl 13):1–10. doi:10.1186/1471-2393-10-13
21. Lennox J, Petrucka P, Bassendowski S. Eating practices during pregnancy: perceptions of select Maasai women in Northern Tanzania. Glob Health Res Pol. 2017;2:1–9. doi:10.1186/s41256-017-0028-9
22. Fenton C, Hatfield J, McIntyre L. A qualitative pilot study of food insecurity among Maasai women in Tanzania. PAMJ. 2012;12:81.
23. Kilongozi N, Kengera Z, Leshono O. The Utilization of Indigenous Knowledge in Range Management and Forage Plants for Improving Livestock Productivity and Food Security in the Maasai and Barbaig Communities of Kibaha. 2005.
24. Lawson DW, Mulder MB, Ghiselli ME, et al. Ethnicity and Child Health in Northern Tanzania: Maasai Pastoralists are Disadvantaged Compared to Neighboring Ethnic Groups. 2014. doi:10.1371/journal.pone.0110447
25. National Bureau of Statistics. Population and Housing Census. Vol. 177. Tanzania Ministry of Finance; 2012:180
26. Makola D, Ash DM, Tatala SR, Latham MC, Ndossi G, Mehansho H. A micronutrient-fortified beverage prevents iron deficiency, reduces anemia and improves the hemoglobin concentration of pregnant Tanzanian women. J Nutr. 2003;133(5):1339–1346. doi:10.1093/jn/133.5.1339
27. Food and Agriculture Organization (FAO). Guidelines for assessing nutrition-related knowledge, attitude and practices. Prepared by Macías YF & Glasauer P. ISBN 978-92-5-108097-9; 2014. Available from: www.fao.org/docrep/019/i3545e/i3545e00.htm.
28. Kawulich B. Qualitative data analysis techniques. In:
29. Burnard P, Gill P, Stewart K, Treasure E, Chadwick B. Analysing and presenting qualitative data. BDJ. 2008;204(8):429–432. doi:10.1038/sj.bdj.2008.292
30. The United Republic of Tanzania: Ministry of Education and Vocational Training. Biology Syllabus for Secondary Education Form 1–4. 2005:1–157. ISBN 9978-9976-61-303-2.
31. Harika R, Faber M, Samuel F, Kimiywe J, Mulugeta A, Eilander A. Micronutrient status and dietary intake of iron, vitamin a, iodine, folate and zinc in women of reproductive age and pregnant women in Ethiopia, Kenya, Nigeria and South Africa: a systematic review of data from 2005 to 2015. Nutrients. 2017;9(Suppl 10):1–23. doi:10.3390/nu9101096
32. Mayanja M, Rubaire-Akiiki C, Morton J, Young S, Greiner T. Diet diversity in pastoral and agro-pastoral households in Ugandan rangeland ecosystems. Ecol Food Nutr. 2015;54(5):529–545. doi:10.1080/03670244.2015.1041135
33. Keverenge-Ettyang GA, Lichtenbelt WM, Esamai F, Saris W. Maternal nutritional status in pastoral versus farming communities of West Pokot, Kenya: differences in iron and vitamin A status and body composition. Food Nutr Bull. 2006;27(3):228–235. doi:10.1177/156482650602700305
34. Klopovich PM. An overview of anemia in children. Issues Compr Pediatr Nurs. 2009. doi:10.3109/01460868309059842
35. Anono EL, Ochola S, Wawire S, Ogada I, Ndedda C, Kung’u JK. Community perceptions towards the new role of traditional birth attendants as birth companions and nutrition advocates in Kakamega County, Kenya. Matern Child Nutr. 2018;14(Suppl 7):12578–12588. doi:10.1111/mcn.12578
36. World Health Organization. Classifying Health Workers. Geneva: WHO; 2010.
37. Available from: http://tanzanialaws.com/index.php/principal-legislation/ngorongoro-conservation-area-act.
38. Kamga RT, Kouamé C, Atangana AR, Chagomoka T, Ndango R. Nutritional evaluation of five African indigenous vegetables. J Hortic Res. 2013;2(1):99–106. doi:10.2478/johr-2013-0014
39. Maundu PM, Ngugi GW, Kabuye CH. Traditional Food Plants of Kenya. Nairobi, Kenya: National Museums of Kenya; 1999.
40. Sharma SR, Giri S, Timalsina U, et al. Low birth weight at term and it’s determinants in a tertiary hospital of nepal: a case-control study. PLoS One. 2015;10:1–10. doi:10.1371/journal.pone.0123962
41. Lothian JA. Safe, healthy birth: what every pregnant woman needs to know. J Perinat Educ. 2009;18(3):48–54. doi:10.1624/105812409X461225
42. Nes FV, Abma T, Jonsson H, Deeg D. Language differences in qualitative research: is meaning lost in translation? Eur J Ageing. 2010. doi:10.1007/s10433-010-0168-y
 © 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2020 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.