Back to Journals » International Journal of General Medicine » Volume 14
Key Issues Surrounding Appropriate Antibiotic Use for Prevention of Surgical Site Infections in Low- and Middle-Income Countries: A Narrative Review and the Implications
Authors Mwita JC, Ogunleye O, Olalekan A ![]() , Kalungia AC
, Kalungia AC ![]() , Kurdi A
, Kurdi A ![]() , Saleem Z
, Saleem Z ![]() , Sneddon J, Godman B
, Sneddon J, Godman B
Received 1 December 2020
Accepted for publication 7 January 2021
Published 18 February 2021 Volume 2021:14 Pages 515—530
DOI https://doi.org/10.2147/IJGM.S253216
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Julius C Mwita,1 Olayinka O Ogunleye,2,3 Adesola Olalekan,4,5 Aubrey C Kalungia,6 Amanj Kurdi,7,8 Zikria Saleem,9 Jacqueline Sneddon,10 Brian Godman7,11,12
1Department of Internal Medicine, Faculty of Medicine, University of Botswana, Gaborone, Botswana; 2Department of Pharmacology, Therapeutics and Toxicology, Lagos State University College of Medicine, Lagos, Nigeria; 3Department of Medicine, Lagos State University Teaching Hospital, Lagos, Nigeria; 4Department of Medical Laboratory Science, University of Lagos, Lagos, Nigeria; 5Centre for Genomics of Non-Diseases and Personalized Healthcare (CGNPH), University of Lagos, Lagos, Nigeria; 6Department of Pharmacy, University of Zambia, Lusaka, Zambia; 7Strathclyde Institute of Pharmacy and Biomedical Sciences, Strathclyde University, Glasgow, UK; 8Department of Pharmacology, College of Pharmacy, Hawler Medical University, Erbil, Iraq; 9Department of Pharmacy Practice, Faculty of Pharmacy, The University of Lahore, Lahore, Pakistan; 10Healthcare Improvement Scotland, Glasgow, UK; 11School of Pharmacy, Sefako Makgatho Health Sciences University, Pretoria, South Africa; 12School of Pharmaceutical Sciences, Universiti Sains Malaysia, Penang, Malaysia
Correspondence: Brian Godman
Strathclyde Institute of Pharmacy and Biomedical Sciences, University of Strathclyde, Glasgow, UK
Tel +44 141 548 3825
Email [email protected]
Background: There is a concern with the growing use of antimicrobials across countries increasing antimicrobial resistance (AMR) rates. A key area within hospitals is their use for the prevention of surgical site infections (SSI) with concerns with timing of the first dose, which can appreciably impact on effectiveness, as well as duration with extended prophylaxis common among low- and middle-income countries (LMICs). This is a concern as extended duration increases utilization rates and AMR as well as adverse events. Consequently, there is a need to document issues of timing and duration of surgical antibiotic prophylaxis (SAP) among LMICs together with potential ways forward to address current concerns.
Methods: Narrative review of timings and duration of SAP among LMICs combined with publications documenting successful approaches to improve SAP to provide future direction to all key stakeholder groups.
Results: There were documented concerns with the timing of the first dose of antibiotics, with appropriate timing as low as 6.7% in Egypt, although as high as 81.9% in Turkey. There was also an extensive duration of SAP, ranging from long duration times in all patients in a study in Nigeria with a mean of 8.7 days and 97% of patients in Egypt to 42.9% of patients in Pakistan and 35% in Turkey. Successful interventions to improve SAP typically involved multiple approaches including education of all key stakeholder groups, monitoring of usage against agreed guidelines,as well as quality targets. Multiple approaches typically improved timing and duration as well as reduced costs. For instance, in one study appropriateness increased from 30.1% to 91.4%, prolonged duration reduced to 5.7% of patients, and mean costs of antibiotics decreased 11-fold.
Conclusion: There are considerable concerns with the timing and duration of SAP among LMICs. Multiple interventions among LMICs can address this providing future directions.
Keywords: surgical site infections, antibiotic prophylaxis, timing of prophylaxis, duration of prophylaxis, LMICs, quality indicators
Introduction
Globally, utilization of antibiotics rose by 39% between 2000 and 2015, which has been driven mainly by increasing consumption in lower- and middle-income (LMIC) countries.1–3 This is a concern as rising rates will increase antimicrobial resistance (AMR), increasing morbidity, mortality, and costs.4–7
One of the key areas to reduce inappropriate prescribing of antibiotics in hospitals surrounds their use in preventing surgical site infections (SSIs).8 SSIs are categorized as infections related to a given operative procedure that occurs at or near the surgical incision within 30 days of the procedure or longer if a prosthesis is implanted, and affects either the incision or deep tissue at the operation site or any part of the surrounding anatomy such as pertinent organs or spaces.9–11 They are currently the most common infectious complications seen among hospitalized patients in developing countries,12,13 and are among the most common and costly causes of hospital acquired infections (HAIs), especially in LMICs.14–22 SSIs can also account for appreciable antibiotic use in hospitals.23–26 Costs associated with SSIs are enhanced by associated increases in the length of hospital stay, which is in addition to increasing morbidity and mortality.15,–27–29 Published studies suggest consolidated incidence figures for SSIs for Nigeria and across Africa at between 14.5–14.8% of all operations,12,30 with rates typically higher in LMICs vs high-income countries.13,–30–35 Consequently, there is an urgent need to improve their prevention in LMICs.
Recognized measures to reduce SSIs include surgical hand preparation, antiseptic preparation, coated sutures, wound protector devices, and negative-pressure wound dressings.18,–29,–36–38 In addition, improving the quality of surgery through increased education as well as the development and monitoring of pertinent quality indicators (QIs).39–41 Measures also include administering antimicrobial prophylaxis, which is seen as the single most effective intervention to reduce SSI rates.42 The selection of antibiotics for SSIs is often based on the risk of wound infection according to the wound classification, ie, clean, clean–contaminated, contaminated, or dirty–infected, the normal floral distribution of the site to be operated on, and local antibiotic resistance patterns.14,43,44 Broad-spectrum antibiotics are often preferred to narrow spectrum antibiotics, and cephalosporins are commonly used.27,–45–47 For instance, cefazolin is commonly recommended for the gastroenterological, genitourinary tract, and hepatobiliary surgeries.48 Ideally, administration of the first antibiotic dose should be within 60 minutes of the first incision, longer for vancomycin and the fluoroquinolones, with a second dose administered for long procedures.18,–42,–49–51 Vicentini et al8 found that adequate antibiotic choices and length of administration were associated with significantly reduced risks of SSIs. Overall, published studies have shown that the risk of SSIs is almost 5-times higher when antibiotics are administered more than 120 minutes prior to the first incision and almost doubled when antibiotics are administered after the first incision.52 Extending prophylaxis beyond 1 day also does not appear to improve patient outcomes, whilst at the same time increasing the chances of acute kidney injury, Clostridium difficile infections, AMR, and costs.13,–42,–53–56
We are aware that there can be poor compliance to current guidelines when available to prevent SSIs across LMICs and wider.45,–57–62 This is in addition to the lack of antibiotic guidelines generally in some hospitals.63 For instance, Madubueze et al59 found that compliance with surgical antibiotic prophylaxis (SAP) protocols among orthopedic surgeons in Nigeria was only 30.3% of situations. Reasons for poor compliance to guidelines included following old practices (25%), concerns that the hospitals were not sufficiently clean (27.3%), and proper aseptic techniques were not being followed (27.3%).59 Other reasons for poor compliance include overcrowding in hospitals, resistance to change among physicians, poor knowledge regarding antibiotics among physicians, and concerns with malnutrition in some patients.45,50,64 Patient expectations may also play an important factor in decision-making.50,65
Principal areas of concern with current SAP approaches across countries including LMICs include timing of administration as well as prolonged use post-surgery.23,45,66,67 Consequently, we believe there is a need to document issues regarding the current timing of administration and the duration of antibiotic administration for SAP among LMICs as well as debate potential ways forward to improve this. This is because reducing the length of post-operative administration will reduce the extent of broad-spectrum antibiotic use for SAP, which in turn should reduce AMR as well as adverse events. Improved SAP can be part of the agreed National Action Plans as countries move to reduce their AMR rates.68–70 This was the objective behind this review article.
Materials and Methods
We have chosen LMICs as they typically have the highest rates of AMR with concerns with antibiotic prescribing common across countries and sectors.68,–71–73 We are also aware of the challenges involved with implementing quality improvement programs among hospitals in LMICs to improve future antibiotic prescribing, which include manpower and resource issues as well as physician resistance as part of any antibiotic stewardship program(ASP).74,75 ASPs are important as they can appreciably improve antibiotic use in hospitals and reduce costs.74,76 These challenges with improving the appropriate use of antibiotics in hospitals are exacerbated by variable knowledge regarding antibiotics, AMR, and ASPs among clinicians in LMICs.73,–77–85 Consequently, we will look to build upon successful approaches to improve SAP instigated among LMICs to give guidance on potential ways forward to address concerns where these continue to exist.50,86
The first step will be to document timings and the duration of antibiotic administration for SAP among a range of LMICs before documenting interventions that have been successful with improving SAP among LMICs. This will involve a narrative review of the published literature. The findings will be combined with the extensive experience of the senior-level co-authors to provide future guidance on potential ways to enhance SAP among LMICs including lessons generally from a range of former Soviet Union Republics that have variably instigated initiatives to reduce inappropriate prescribing of antibiotics. We have chosen former Soviet Union Republics as they typically have less Gross Domestic Product (GDP) per capita than among higher income Western European countries,87 ie, more akin to LMICs.
We did not undertake a systematic review since we were aware that there had been a number of reviews surrounding the use of antibiotic prophylaxis as well as other potential interventions to reduce SSIs.29,–50,–52,–86,–88–93 In addition, our aim was to provide possible guidance for key stakeholder groups within LMICs based on our experiences for potential debate. We have successfully used this approach across LMICs to stimulate debate in different key disease areas and topics.68,–94–97
The interventions that have been undertaken and proposed will be broken down into the 4Es where pertinent, namely Education, Engineering, Economics, and Enforcement,98,99 to enhance understanding and comparisons given the range of potential interventions that could be instigated. Education includes developing guidelines or formularies, with adherence to well-constructed guidelines increasingly seen as indicating good quality care.25,–100–103 Activities within hospitals to enhance the rational use of medicines are typically co-ordinated by Drug and Therapeutic Committees (DTCs).104–106 Antimicrobial stewardship groups may be part of DTCs; alternatively, separate groups working in the hospital as part of infection, prevention, and control groups.107,108 In addition, the development and dissemination of the WHO AWaRe list of antibiotics to improve future antibiotic prescribing and dispensing.109,110 Engineering includes organizational or managerial interventions such as instigating and monitoring prescribing targets and quality targets.99,100 Quality targets could include the percentage of antibiotics prescribed according to agreed guidance, the percentage of antibiotics prescribed within a specified time and for an agreed length to prevent SSIs, as well as monitoring drug and therapeutic committee (DTC) activities against agreed performance indicators.59,102,111 Economics includes financial incentives to hospitals, physicians, pharmacists, or patients, ie, providing financial incentives to hospitals to improve patient safety and not pay for preventable errors, to physicians for attaining agreed prescribing targets, and fining pharmacists for illegally dispensing an antibiotic without a prescription.99,100,112,113 Enforcement includes regulations by law.99 Examples include laws banning the dispensing of antibiotics in pharmacies without a prescription as well as national policies outlining the existence of DTCs in hospitals as currently seen in South Africa.105,114
Results
Timing and Duration of Administration for SAP Among LMICs
Table 1 documents a range of timings and duration of administration for SAP among LMICs across continents. Ideally, administration of the first antibiotic dose should be within 60 minutes of the first incision and only for 1 day. However, wide variations were seen with only a limited number of patients across a range of LMICs generally receiving SAP within this time (Table 1). Documented rates for staying within agreed timings of the first incision ranged from as low as 6.7% of patients in Egypt, up to 81.9% in Turkey.
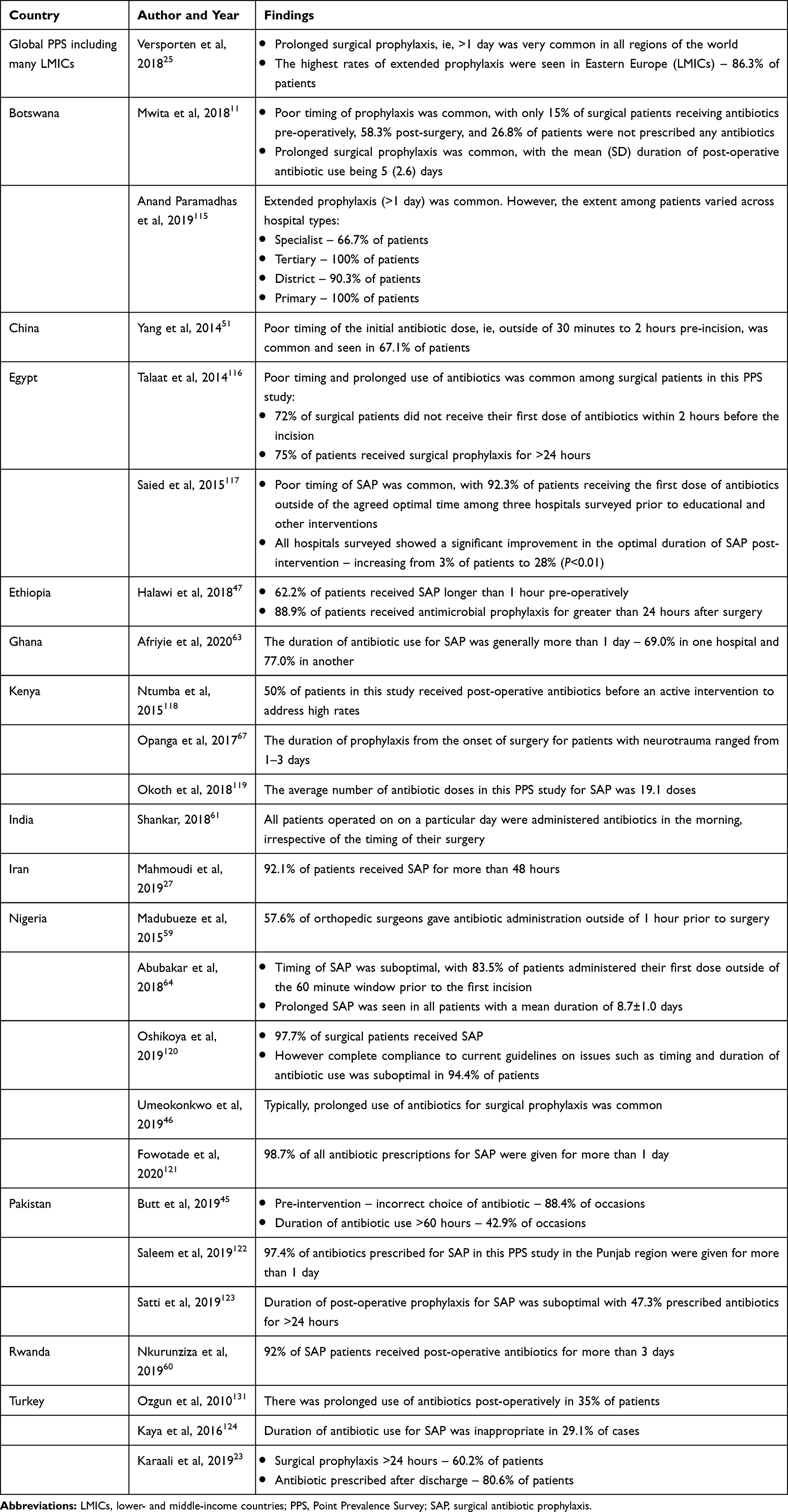 |
Table 1 Published Rates Regarding Inappropriate Timing and Length of Administration of Antibiotics for SAP Among LMICs |
There were similar concerns regarding the extent of prophylactic antibiotics given for longer than 1 day across LMICs. Rates of extended prophylaxis ranged from all patients in Nigeria in the study by Abubakar et al (2018) with a mean of 8.7 days, to 97% of patients in Egypt and Pakistan (Saied et al 2015 and Saleem et al 2019, respectively), and 86.3% among surgical patients in Eastern Europe (part of the Global PPS study). Extended prophylaxis was seen in 42.9% of patients in Pakistan (Butt et al 2019) and 35% in Turkey (Ozgun et al 2020) (Table 1).
Interventions to Enhance Adherence to SAPs Among Countries
A number of interventions have been instigated across many LMICs to improve SAP broken down into Education, Engineering, Economics, and Enforcement where pertinent and by year to provide guidance.
Interventions principally centred around educational inputs. In addition, monitoring subsequent prescribing against agreed guidance (QIs) and providing feedback to help improve subsequent SAP (Engineering – Table 2). Multiple interventions resulted in appreciable improvements in SAP across LMICs. For instance, Bozkurt et al (2014) found that multiple interventions improved the duration of prophylaxis from 10.3% to 59.4% of cases, Saied et al (2015) that optimal timing of the first dose can be appreciably improved (6.7% to 38.7%), and Brink et al (2017) that the choice of antibiotic, consistent with agreed guidelines, can be improved to 95.9% of patients (Table 2).
 |  |  |
Table 2 Summary of Published Studies Across Countries Documenting the Impact of Interventions on Subsequent Timing and Length of Antibiotic Administration Among a Range of LMICs |
However, we are aware there are cases where interventions have not always been effective. In their study, Ozgun et al131 instigated a number of measures including analyzing key concerns regarding SAP with individual surgical teams, as well as educational meetings with all key stakeholders during which concerns including timing and duration of antibiotic use were discussed. However, compliance to agreed guidelines actually decreased post-intervention, and the number of patients receiving prolonged SAP was higher after the intervention than before, increasing from 34% of patients (Table 1) to 52%, which was statistically significant (P<0.01), with surgeons comfortable at the time with prolonged administration.131
Discussion and Recommendations
We have shown that there can be considerable concerns regarding the current use of SAP among LMICs to reduce SSIs. These include concerns with both the timing and duration of administration of antibiotics (Table 1). Both need to be addressed to enhance the effectiveness of appropriate SAP to prevent SSIs, reduce the extent of any adverse events including Clostridium difficile infections and AMR, as well as reduce costs.8,–52–55
Encouragingly, typically multifaceted interventions appear to be successful in addressing concerns with timing and duration of antibiotic prophylaxis providing direction to others (Table 2). This mirrors the successful impact of multiple interventions instigated by health authorities and others in different disease areas and situations, including antibiotics as well as medicines for acid-related stomach disorders, depression, hypertension, and hypercholesterolemia, to improve their prescribing.132–140 There have been limited changes in physician prescribing behavior in the absence of such interventions.141–143 In addition, we are aware that multiple demand-side measures in former Soviet Union Republics have improved appropriate use of antibiotics. In Azerbaijan, initiatives including Education, Economics, and Enforcement resulted in antibiotic utilization decreasing by 47% between 2011 and 2015.144 In Slovenia, multiple activities including all the 4Es also resulted in antibiotic utilization falling by 31% between 1999 to 2012,137 with multiple activities in the Republic of Srpska including all the 4Es resulting in a decreasing trend in antibiotic consumption in recent years, with utilization rates comparable or lower than those seen in neighboring countries.145 This contrasts with Poland, where limited activities among the authorities and other groups between 2007 and 2016 resulted in Poland continuing to have one of the highest rates of antibiotic consumption across Europe.146 However, we are aware of situations where multiple interventions have not improved SAP.131
Potential future activities to improve SAP center around the development of antimicrobial stewardship activities including ASPs which can be part of DTCs within countries and hospitals if not already instigated to address concerns and misconceptions (Table 3). This may include the need for additional educational activities surrounding antibiotics and concerns with hygiene, AMR, and SAP if pertinent, along with the development of any local guidelines and QIs. The outputs from subsequent monitoring of SAP post-intervention, including changes in any agreed QIs, can be used to develop and instigate additional pertinent interventions. This is because we have seen that multiple activities including Education, Engineering, and Enforcement can have a significant impact on both the timing and duration of antibiotic use as part of SAP, impacting on future prevalence and morbidity of SSIs as well as costs (Table 2).
 |
Table 3 Potential Strategies to Improve SAP Within Hospitals in LMICs |
More studies are needed though to assess the cost-effectiveness of different interventions as opposed to studies that principally measure individual cost components before and after interventions to provide future guidance (Table 3). In addition, any QI developed needs to be robust, appropriate, measurable, and improve future care, building on examples in other situations as well as suggestions from the WHO and others.25,–61,–147–149
We are aware that Health Technology Assessment (HTA) units are less developed in LMICs vs high-income countries and there can be concerns with implementing the findings of HTA analyses.150,151 However, this is starting to change in some countries, with suggestions for a more integrative approach.152,153 This is important as the outputs from HTA units can help hospitals and governments prioritize resources and personnel, with the situation becoming even more imperative post the current COVID-19 and its consequences.97 This is important to enhance the rational use of SAP in LMICs. However, HTA as a strategy to curb AMR requires appropriate legislative and institutional frameworks, as well as human and financial resources, to translate any findings into effective implementation and monitoring of health interventions.154 In addition, physicians, nurses, and pharmacists must confidently trust any STGs produced to enhance their acceptability and success in curbing AMR.155,156 This, complemented by enhancing healthcare worker’s knowledge regarding antibiotic use, AMR, and ASPs within hospitals through targeted educational interventions, can improve the rational use of antibiotics.
We are aware of some limitations with this paper. These include the fact that we did not undertake a systematic review for the reasons discussed. We have, though, contextualized the findings to provide direction to key stakeholder groups to improve SAP in LMICs based on the considerable experience of the co-authors. We believe these recommendations are robust based on their experience and knowledge across LMICs.
Conclusion
We believe this is the first review study to combine a narrative review of the timings and duration of antibiotic use for SAP among LMICs as well as approaches that have been successful in addressing current concerns with SAP to provide future direction. We have shown that there are considerable concerns with current SAP among LMICs, including timing and duration, which is important given rising antimicrobial consumption rates and AMR among LMICs. However, multiple interventions can appreciably improve the situation and reduce costs. As a result, there are multiple activities that all key stakeholder groups can undertake to improve future SAP where important issues have been identified, and we will be monitoring this.
Author Contributions
All authors contributed to the design and development of the paper through their extensive activities to improve the use of antibiotics within hospitals and wider. All authors critically evaluated the first and subsequent drafts and approved the final version before submission.
Funding
There was no funding for this paper.
Disclosure
The authors have no relevant conflicts of interest to declare.
References
1. Klein EY, Milkowska-Shibata M, Tseng KK, et al. Assessment of WHO antibiotic consumption and access targets in 76 countries, 2000–15: an analysis of pharmaceutical sales data. Lancet Infect Dis. 2020;21:107–115. doi:10.1016/S1473-3099(20)30332-7
2. Klein EY, Van Boeckel TP, Martinez EM, et al. Global increase and geographic convergence in antibiotic consumption between 2000 and 2015. Proc Natl Acad Sci U S A. 2018;115(15):E3463–e70. doi:10.1073/pnas.1717295115
3. Schellack N, Benjamin D, Brink A, et al. A situational analysis of current antimicrobial governance, regulation, and utilization in South Africa. Int J Infect Dis. 2017;64:100–106. doi:10.1016/j.ijid.2017.09.002
4. Bell BG, Schellevis F, Stobberingh E, Goossens H, Pringle M. A systematic review and meta-analysis of the effects of antibiotic consumption on antibiotic resistance. BMC Infect Dis. 2014;14:13. doi:10.1186/1471-2334-14-13
5. Cassini A, Hogberg LD, Plachouras D, et al. Attributable deaths and disability-adjusted life-years caused by infections with antibiotic-resistant bacteria in the EU and the European Economic Area in 2015: a population-level modelling analysis. Lancet Infect Dis. 2019;19(1):56–66. doi:10.1016/S1473-3099(18)30605-4
6. Godman B, Fadare J, Kibuule D, et al. Initiatives across countries to reduce antibiotic utilisation and resistance patterns: impact and implications. In: Arora G, Sajid A, Kalia VC, editors. Drug Resistance in Bacteria, Fungi, Malaria, and Cancer. Cham: Springer International Publishing; 2017:539–576.
7. Hofer U. The cost of antimicrobial resistance. Nat Rev Microbiol. 2019;17(1):3. doi:10.1038/s41579-018-0125-x
8. Vicentini C, Politano G, Corcione S, et al. Surgical antimicrobial prophylaxis prescribing practices and impact on infection risk: results from a multicenter surveillance study in Italy (2012–2017). Am J Infect Control. 2019;47(12):1426–1430. doi:10.1016/j.ajic.2019.07.013
9. Weber WP, Marti WR, Zwahlen M, et al. The timing of surgical antimicrobial prophylaxis. Ann Surg. 2008;247(6):918–926. doi:10.1097/SLA.0b013e31816c3fec
10. Young PY, Khadaroo RG. Surgical site infections. Surg Clin North Am. 2014;94(6):1245–1264. doi:10.1016/j.suc.2014.08.008
11. Mwita JC, Souda S, Magafu M, Massele A, Godman B, Mwandri M. Prophylactic antibiotics to prevent surgical site infections in Botswana: findings and implications. Hosp Pract. 2018;46(3):97–102. doi:10.1080/21548331.2018.1450605
12. Ngaroua JE, Benet T, Djibrilla Y, Djibrilla Y. [Incidence of surgical site infections in sub-Saharan Africa: systematic review and meta-analysis]. Pan Afr Med J. 2016;24:171. French. doi:10.11604/pamj.2016.24.171.9754
13. Saito H, Inoue K, Ditai J, Weeks AD. Pattern of peri-operative antibiotic use among surgical patients in a regional referral and teaching hospital in Uganda. Surg Infect (Larchmt). 2020;21(6):540–546. doi:10.1089/sur.2019.176
14. Anderson DJ, Podgorny K, Berrios-Torres SI, et al. Strategies to prevent surgical site infections in acute care hospitals: 2014 update. Infect Control Hosp Epidemiol. 2014;35(6):605–627. doi:10.1086/676022
15. Zimlichman E, Henderson D, Tamir O, et al. Health care-associated infections: a meta-analysis of costs and financial impact on the US health care system. JAMA Intern Med. 2013;173(22):2039–2046. doi:10.1001/jamainternmed.2013.9763
16. Korol E, Johnston K, Waser N, et al. A systematic review of risk factors associated with surgical site infections among surgical patients. PLoS One. 2013;8(12):e83743. doi:10.1371/journal.pone.0083743
17. Goyal R, Pal H, Sandhu S, Kumar A, Kosey S, Mehra N. Surveillance method for surgical site infection. Indian J Pharm Pract. 2015;8:54–60. doi:10.5530/ijopp.8.2.2
18. Najjar PA, Smink DS. Prophylactic antibiotics and prevention of surgical site infections. Surg Clin North Am. 2015;95(2):269–283. doi:10.1016/j.suc.2014.11.006
19. Saleem Z, Hassali MA, Godman B, Hashmi FK, Saleem F. A multicenter point prevalence survey of healthcare-associated infections in Pakistan: findings and implications. Am J Infect Control. 2019;47(4):421–424. doi:10.1016/j.ajic.2018.09.025
20. Labi AK, Obeng-Nkrumah N, Owusu E, et al. Multi-centre point-prevalence survey of hospital-acquired infections in Ghana. J Hosp Infect. 2019;101(1):60–68. doi:10.1016/j.jhin.2018.04.019
21. Abubakar U. Antibiotic use among hospitalized patients in northern Nigeria: a multicenter point-prevalence survey. BMC Infect Dis. 2020;20(1):86. doi:10.1186/s12879-020-4815-4
22. Abubakar U. Point-prevalence survey of hospital acquired infections in three acute care hospitals in Northern Nigeria. Antimicrob Resist Infect Control. 2020;9(1):63. doi:10.1186/s13756-020-00722-9
23. Karaali C, Emiroglu M, Atalay S, et al. A new antibiotic stewardship program approach is effective on inappropriate surgical prophylaxis and discharge prescription. J Infect Dev Ctries. 2019;13(11):961–967. doi:10.3855/jidc.11734
24. Saleem Z, Hassali MA, Godman B, et al. Point prevalence surveys of antimicrobial use: a systematic review and the implications. Expert Rev Anti Infect Ther. 2020;18:897–910. doi:10.1080/14787210.2020.1767593
25. Versporten A, Zarb P, Caniaux I, et al. Antimicrobial consumption and resistance in adult hospital inpatients in 53 countries: results of an internet-based global point prevalence survey. Lancet Global Health. 2018;6(6):e619–e29. doi:10.1016/S2214-109X(18)30186-4
26. Al Matar M, Enani M, Binsaleh G, et al. Point prevalence survey of antibiotic use in 26 Saudi hospitals in 2016. J Infect Public Health. 2019;12(1):77–82. doi:10.1016/j.jiph.2018.09.003
27. Mahmoudi L, Ghouchani M, Mahi-Birjand M, Bananzadeh A, Akbari A. Optimizing compliance with surgical antimicrobial prophylaxis guidelines in patients undergoing gastrointestinal surgery at a referral teaching hospital in southern Iran: clinical and economic impact. Infect Drug Resist. 2019;12:2437–2444. doi:10.2147/IDR.S212728
28. de Lissovoy G, Fraeman K, Hutchins V, Murphy D, Song D, Vaughn BB. Surgical site infection: incidence and impact on hospital utilization and treatment costs. Am J Infect Control. 2009;37(5):387–397. doi:10.1016/j.ajic.2008.12.010
29. De Simone B, Sartelli M, Coccolini F, et al. Intraoperative surgical site infection control and prevention: a position paper and future addendum to WSES intra-abdominal infections guidelines. World J Emerg Surg. 2020;15(1):10. doi:10.1186/s13017-020-0288-4
30. Olowo-Okere A, Ibrahim YKE, Olayinka BO, Ehinmidu JO. Epidemiology of surgical site infections in Nigeria: a systematic review and meta-analysis. Niger Postgrad Med J. 2019;26(3):143–151. doi:10.4103/npmj.npmj_72_19
31. Allegranzi B, Bagheri Nejad S, Combescure C, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet. 2011;377(9761):228–241. doi:10.1016/S0140-6736(10)61458-4
32. Mawalla B, Mshana SE, Chalya PL, Imirzalioglu C, Mahalu W. Predictors of surgical site infections among patients undergoing major surgery at Bugando Medical Centre in Northwestern Tanzania. BMC Surg. 2011;11. doi:10.1186/1471-2482-11-21
33. Rickard J, Beilman G, Forrester J, et al. Surgical infections in low- and middle-income countries: a global assessment of the burden and management needs. Surg Infect (Larchmt). 2020;21(6):478–494. doi:10.1089/sur.2019.142
34. Olowo-Okere A, Ibrahim YKE, Sani AS, Olayinka BO. Occurrence of surgical site infections at a tertiary healthcare facility in Abuja, Nigeria: a prospective observational study. Med Sci. 2018;6(3):60. doi:10.3390/medsci6030060
35. Maleknejad A, Dastyar N, Badakhsh M, et al. Surgical site infections in Eastern Mediterranean region: a systematic review and meta-analysis. Infect Dis. 2019;51(10):719–729. doi:10.1080/23744235.2019.1642513
36. Ling ML, Apisarnthanarak A, Abbas A, et al. APSIC guidelines for the prevention of surgical site infections. Antimicrob Resist Infect Control. 2019;8(1):174. doi:10.1186/s13756-019-0638-8
37. Rojas-Gutierrez E, Vilar-Compte D. An overview of surgical site infection in low- and middle-income countries: the role of recent guidelines, limitations, and possible solutions. Curr Treat Options Infect Dis. 2019;11(3):300–316. doi:10.1007/s40506-019-00198-1
38. Loftus MJ, Guitart C, Tartari E, et al. Hand hygiene in low- and middle-income countries. Int J Infect Dis. 2019;86:25–30. doi:10.1016/j.ijid.2019.06.002
39. Ng-Kamstra JS, Arya S, Greenberg SLM, et al. Perioperative mortality rates in low-income and middle-income countries: a systematic review and meta-analysis. BMJ Global Health. 2018;3(3):e000810. doi:10.1136/bmjgh-2018-000810
40. Roa L, Citron I, Ramos JA, et al. Cross-sectional study of surgical quality with a novel evidence-based tool for low-resource settings. BMJ Open Qual. 2020;9(1):e000880. doi:10.1136/bmjoq-2019-000880
41. Saluja S, Mukhopadhyay S, Amundson JR, et al. Quality of essential surgical care in low- and middle-income countries: a systematic review of the literature. Int J Qual Health Care. 2019;31(3):166–172. doi:10.1093/intqhc/mzy141
42. Bull AL, Worth LJ, Spelman T, Richards MJ. Antibiotic prescribing practices for prevention of surgical site infections in Australia: increased uptake of national guidelines after surveillance and reporting and impact on infection rates. Surg Infect (Larchmt). 2017;18(7):834–840. doi:10.1089/sur.2017.119
43. Varley AJ, Sule J, Absalom AR. Principles of antibiotic therapy. Critical Care Pain. 2009;9(6):184–188. doi:10.1093/bjaceaccp/mkp035
44. Culver DH, Horan TC, Gaynes RP, et al. Surgical wound infection rates by wound class, operative procedure, and patient risk index. National nosocomial infections surveillance system. Am J Med. 1991;91(3):152s–7s. doi:10.1016/0002-9343(91)90361-Z
45. Butt SZ, Ahmad M, Saeed H, Saleem Z, Javaid Z. Post-surgical antibiotic prophylaxis: impact of pharmacist’s educational intervention on appropriate use of antibiotics. J Infect Public Health. 2019;12(6):854–860. doi:10.1016/j.jiph.2019.05.015
46. Umeokonkwo CD, Madubueze UC, Onah CK, et al. Point prevalence survey of antimicrobial prescription in a tertiary hospital in South East Nigeria: a call for improved antibiotic stewardship. J Global Antimicrob Resist. 2019;17:291–295. doi:10.1016/j.jgar.2019.01.013
47. Halawi E, Assefa T, Hussen S. Pattern of antibiotics use, incidence and predictors of surgical site infections in a Tertiary Care Teaching Hospital. BMC Res Notes. 2018;11(1):538. doi:10.1186/s13104-018-3643-8
48. Bratzler DW, Dellinger EP, Olsen KM, et al. Clinical practice guidelines for antimicrobial prophylaxis in surgery. Surg Infect (Larchmt). 2013;14(1):73–156. doi:10.1089/sur.2013.9999
49. Malhotra NR, Piazza M, Demoor R, et al. Impact of reduced preincision antibiotic infusion time on surgical site infection rates: a retrospective cohort study. Ann Surg. 2020;271(4):774–780. doi:10.1097/SLA.0000000000003030
50. Cooper L, Sneddon J, Afriyie DK, et al. Supporting global antimicrobial stewardship: antibiotic prophylaxis for the prevention of surgical site infection in low- and middle-income countries (LMICs): a scoping review and meta-analysis. JAC-AMR. 2020;2(3). doi:10.1093/jacamr/dlaa070.
51. Yang Z, Zhao P, Wang J, et al. DRUGS system enhancing adherence of Chinese surgeons to antibiotic use guidelines during perioperative period. PLoS One. 2014;9(8):e102226. doi:10.1371/journal.pone.0102226
52. de Jonge SW, Gans SL, Atema JJ, Solomkin JS, Dellinger PE, Boermeester MA. Timing of preoperative antibiotic prophylaxis in 54,552 patients and the risk of surgical site infection: a systematic review and meta-analysis. Medicine. 2017;96(29):e6903. doi:10.1097/MD.0000000000006903
53. Branch-Elliman W, O’Brien W, Strymish J, Itani K, Wyatt C, Gupta K. Association of duration and type of surgical prophylaxis with antimicrobial-associated adverse events. JAMA Surg. 2019;154(7):590–598. doi:10.1001/jamasurg.2019.0569
54. Harbarth S, Samore MH, Lichtenberg D, Carmeli Y. Prolonged antibiotic prophylaxis after cardiovascular surgery and its effect on surgical site infections and antimicrobial resistance. Circulation. 2000;101(25):2916–2921. doi:10.1161/01.cir.101.25.2916
55. Hawn MT, Knowlton LM. Balancing the risks and benefits of surgical prophylaxis: timing and duration do matter. JAMA Surg. 2019;154(7):598–599. doi:10.1001/jamasurg.2019.0570
56. Langerman A, Thisted R, Hohmann S, Howell M. Antibiotic and duration of perioperative prophylaxis predicts surgical site infection in head and neck surgery. Otolaryngol Head Neck Surg. 2016;154(6):1054–1063. doi:10.1177/0194599816634303
57. Musmar SM, Ba’ba H, Owais A. Adherence to guidelines of antibiotic prophylactic use in surgery: a prospective cohort study in North West Bank, Palestine. BMC Surg. 2014;14:69. doi:10.1186/1471-2482-14-69
58. Alemkere G, Hawryluk GWJ. Antibiotic usage in surgical prophylaxis: a prospective observational study in the surgical ward of Nekemte referral hospital. PLoS One. 2018;13(9):e0203523. doi:10.1371/journal.pone.0203523
59. Madubueze CC, Umaru H, Alada A. Attitudes of Nigerian orthopaedic surgeons to the use of prophylactic antibiotics. Int Orthop. 2015;39(11):2161–2165. doi:10.1007/s00264-015-2822-7
60. Nkurunziza T, Kateera F, Sonderman K, et al. Prevalence and predictors of surgical-site infection after caesarean section at a rural district hospital in Rwanda. Br J Surg. 2019;106(2):e121–e8. doi:10.1002/bjs.11060
61. Shankar R. Implementation of the WHO Surgical Safety Checklist at a teaching hospital in India and evaluation of the effects on perioperative complications. Int J Health Plann Manage. 2018;33(4):836–846. doi:10.1002/hpm.2533
62. Alahmadi YM, Alharbi RH, Aljabri AK, Alofi FS, Alshaalani OA, Alssdi BH. Adherence to the guidelines for surgical antimicrobial prophylaxis in a Saudi tertiary care hospital. J Taibah Univ Med Sci. 2020;15(2):136–141. doi:10.1016/j.jtumed.2020.01.005
63. Afriyie DK, Sefah IA, Sneddon J, et al. Antimicrobial Point Prevalence Surveys in two Ghanaian hospitals: opportunities for antimicrobial stewardship. JAC AMR. 2020;1–9.
64. Abubakar U, Syed Sulaiman SA, Adesiyun AG. Utilization of surgical antibiotic prophylaxis for obstetrics and gynaecology surgeries in Northern Nigeria. Int J Clin Pharm. 2018;40(5):1037–1043. doi:10.1007/s11096-018-0702-0
65. Aiken AM, Wanyoro AK, Mwangi J, Juma F, Mugoya IK, Scott JA. Changing use of surgical antibiotic prophylaxis in Thika Hospital, Kenya: a quality improvement intervention with an interrupted time series design. PLoS One. 2013;8(11):e78942. doi:10.1371/journal.pone.0078942
66. Friedman ND, Styles K, Gray AM, Low J, Athan E. Compliance with surgical antibiotic prophylaxis at an Australian teaching hospital. Am J Infect Control. 2013;41(1):71–74. doi:10.1016/j.ajic.2012.02.012
67. Opanga SA, Mwang’ombe NJ, Okalebo FA, Godman B, Oluka M, Kuria KAM. Determinants of the effectiveness of antimicrobial prophylaxis among neurotrauma patients at a referral hospital in Kenya: findings and implications. Infect Dis Preve Med. 2017;5:169.
68. Godman B, Haque M, McKimm J, et al. Ongoing strategies to improve the management of upper respiratory tract infections and reduce inappropriate antibiotic use particularly among lower and middle-income countries: findings and implications for the future. Curr Med Res Opin. 2020;36(2):301–327. doi:10.1080/03007995.2019.1700947
69. Saleem Z, Hassali MA, Hashmi FK. Pakistan’s national action plan for antimicrobial resistance: translating ideas into reality. Lancet Infect Dis. 2018;18(10):1066–1067. doi:10.1016/S1473-3099(18)30516-4
70. Ghana Ministry of Health, Ministry of Food and Agriculture, Ministry of Environment, Science, Technology and Innovation, Ministry of Fisheries and Aquaculture Development. Ghana national action plan for antimicrobial use and resistance; 2017–2021. Available from: http://www.moh.gov.gh/wp-content/uploads/2018/04/NAP_FINAL_PDF_A4_19.03.2018-SIGNED-1.pdf.
71. Ayukekbong JA, Ntemgwa M, Atabe AN. The threat of antimicrobial resistance in developing countries: causes and control strategies. Antimicrob Resist Infect Control. 2017;6(1):47. doi:10.1186/s13756-017-0208-x
72. Kalungia A, Godman B. Implications of non-prescription antibiotic sales in China. Lancet Infect Dis. 2019;19(12):1272–1273. doi:10.1016/S1473-3099(19)30408-6
73. Akpan MR, Isemin NU, Udoh AE, Ashiru-Oredope D. Implementation of antimicrobial stewardship programmes in African countries: a systematic literature review. J Global Antimicrob Resist. 2020;22:317–324. doi:10.1016/j.jgar.2020.03.009
74. Cox JA, Vlieghe E, Mendelson M, et al. Antibiotic stewardship in low- and middle-income countries: the same but different? Clin Microbiol Infect. 2017;23(11):812–818. doi:10.1016/j.cmi.2017.07.010
75. Charani E, Smith I, Skodvin B, et al. Investigating the cultural and contextual determinants of antimicrobial stewardship programmes across low-, middle- and high-income countries-A qualitative study. PLoS One. 2019;14(1):e0209847. doi:10.1371/journal.pone.0209847
76. Nathwani D, Varghese D, Stephens J, Ansari W, Martin S, Charbonneau C. Value of hospital antimicrobial stewardship programs [ASPs]: a systematic review. Antimicrob Resist Infect Control. 2019;8:35. doi:10.1186/s13756-019-0471-0
77. Fadare JO, Ogunleye O, Iliyasu G, et al. Status of antimicrobial stewardship programmes in Nigerian tertiary healthcare facilities: findings and implications. J Global Antimicrob Resist. 2019;17:132–136. doi:10.1016/j.jgar.2018.11.025
78. Engler D, Meyer JC, Schellack N, Kurdi A, Godman B. Compliance with South Africa’s antimicrobial resistance national strategy framework: are we there yet? J Chemother. 2021;33(1):21–31. doi:10.1080/1120009X.2020.1789389
79. Kalungia AC, Mwambula H, Munkombwe D, et al. Antimicrobial stewardship knowledge and perception among physicians and pharmacists at leading tertiary teaching hospitals in Zambia: implications for future policy and practice. J Chemother. 2019;31(7–8):378–387. doi:10.1080/1120009X.2019.1622293
80. Babatola AO, Fadare JO, Olatunya OS, et al. Addressing antimicrobial resistance in Nigerian hospitals: exploring physicians prescribing behavior, knowledge and perception of antimicrobial resistance and stewardship programs. Expert Rev Anti Infect Ther. 2020;1–10. Doi:10.1080/14787210.2021.1829474
81. Firouzabadi D, Mahmoudi L. Knowledge, attitude, and practice of health care workers towards antibiotic resistance and antimicrobial stewardship programmes: a cross-sectional study. J Eval Clin Pract. 2020;26(1):190–196. doi:10.1111/jep.13177
82. Saleem Z, Hassali MA, Hashmi FK, Godman B, Ahmed Z. Snapshot of antimicrobial stewardship programs in the hospitals of Pakistan: findings and implications. Heliyon. 2019;5(7):e02159. doi:10.1016/j.heliyon.2019.e02159
83. Labi AK, Obeng-Nkrumah N, Bjerrum S, et al. Physicians’ knowledge, attitudes, and perceptions concerning antibiotic resistance: a survey in a Ghanaian tertiary care hospital. BMC Health Serv Res. 2018;18(1):126. doi:10.1186/s12913-018-2899-y
84. Singh S, Charani E, Wattal C, Arora A, Jenkins A, Nathwani D. The state of education and training for antimicrobial stewardship programs in indian hospitals-a qualitative and quantitative assessment. Antibiotics. 2019;8(1):11. doi:10.3390/antibiotics8010011
85. Hayat K, Rosenthal M, Gillani AH, et al. Perspective of key healthcare professionals on antimicrobial resistance and stewardship programs: a multicenter cross-sectional study from Pakistan. Front Pharmacol. 2020;10:1520. doi:10.3389/fphar.2019.01520
86. Ariyo P, Zayed B, Riese V, et al. Implementation strategies to reduce surgical site infections: a systematic review. Infect Control Hosp Epidemiol. 2019;40(3):287–300. doi:10.1017/ice.2018.355
87. World Bank. GDP per capita; 2020. Available from: https://data.worldbank.org/indicator/NY.GDP.PCAP.CD.
88. Haque M, McKimm J, Godman B, Abu Bakar M, Sartelli M. Initiatives to reduce postoperative surgical site infections of the head and neck cancer surgery with a special emphasis on developing countries. Expert Rev Anticancer Ther. 2019;19(1):81–92. doi:10.1080/14737140.2019.1544497
89. Franco LM, Cota GF, Pinto TS, Ercole FF. Preoperative bathing of the surgical site with chlorhexidine for infection prevention: systematic review with meta-analysis. Am J Infect Control. 2017;45(4):343–349. doi:10.1016/j.ajic.2016.12.003
90. Shi D, Yao Y, Yu W. Comparison of preoperative hair removal methods for the reduction of surgical site infections: a meta-analysis. J Clin Nurs. 2017;26(19–20):2907–2914. doi:10.1111/jocn.13661
91. Yao R, Tan T, Tee JW, Street J. Prophylaxis of surgical site infection in adult spine surgery: a systematic review. J Clin Neurosci. 2018;52:5–25. doi:10.1016/j.jocn.2018.03.023
92. Schreiber PW, Sax H, Wolfensberger A, Clack L, Kuster SP. The preventable proportion of healthcare-associated infections 2005–2016: systematic review and meta-analysis. Infect Control Hosp Epidemiol. 2018;39(11):1277–1295. doi:10.1017/ice.2018.183
93. Boonchan T, Wilasrusmee C, McEvoy M, Attia J, Thakkinstian A. Network meta-analysis of antibiotic prophylaxis for prevention of surgical-site infection after groin hernia surgery. Br J Surg. 2017;104(2):e106–e17. doi:10.1002/bjs.10441
94. Godman B, Basu D, Pillay Y, et al. Review of ongoing activities and challenges to improve the care of patients with type 2 diabetes across Africa and the implications for the future. Front Pharmacol. 2020;11:108. doi:10.3389/fphar.2020.00108
95. Godman B, Grobler C, Van-De-Lisle M, et al. Pharmacotherapeutic interventions for bipolar disorder type II: addressing multiple symptoms and approaches with a particular emphasis on strategies in lower and middle-income countries. Expert Opin Pharmacother. 2019;20(18):2237–2255. doi:10.1080/14656566.2019.1684473
96. Godman B, McCabe H, Leong T et al. Fixed dose drug combinations - are they pharmacoeconomically sound? Findings and implications especially for lower- and middle-income countries. Expert Rev Pharmacoecon Outcomes Res. 2020;20(1):1–26. doi:10.1080/14737167.2020.1734456
97. Ogunleye OO, Basu D, Mueller D, et al. Response to the Novel Corona virus (COVID-19) pandemic across Africa: successes, challenges, and implications for the future. Front Pharmacol. 2020;11:1205.
98. Wettermark B, Godman B, Jacobsson B, Haaijer-Ruskamp FM. Soft regulations in pharmaceutical policy making: an overview of current approaches and their consequences. Appl Health Econ Health Policy. 2009;7(3):137–147. doi:10.1007/BF03256147
99. Godman B. Health authority activities to enhance the quality and efficiency of medicine use and their impact. Adv Human Biol. 2021;11:11–16.
100. Godman B, Wettermark B, van Woerkom M, et al. Multiple policies to enhance prescribing efficiency for established medicines in Europe with a particular focus on demand-side measures: findings and future implications. Front Pharmacol. 2014;5:106. doi:10.3389/fphar.2014.00106
101. Niaz Q, Godman B, Massele A, et al. Validity of World Health Organisation prescribing indicators in Namibia’s primary healthcare: findings and implications. Int J Qual Health Care. 2019;31(5):338–345. doi:10.1093/intqhc/mzy172
102. Nakwatumbah S, Kibuule D, Godman B, et al. Compliance to guidelines for the prescribing of antibiotics in acute infections at Namibia’s national referral hospital: a pilot study and the implications. Expert Rev Anti Infect Ther. 2017;15(7):713–721. doi:10.1080/14787210.2017.1320220
103. Niaz Q, Godman B, Campbell S, Kibuule D. Compliance to prescribing guidelines among public health care facilities in Namibia; findings and implications. Int J Clin Pharm. 2020;42(4):1227–1236. doi:10.1007/s11096-020-01056-7
104. Hoffmann M. The right drug, but from whose perspective? A framework for analysing the structure and activities of drug and therapeutics committees. Eur J Clin Pharmacol. 2013;69(Suppl 1):79–87. doi:10.1007/s00228-013-1491-y
105. Matlala M, Gous AGS, Meyer JC, Godman B. Formulary management activities and practice implications among public sector hospital pharmaceutical and therapeutics committees in a South African Province. Front Pharmacol. 2020;11:1267. doi:10.3389/fphar.2020.01267
106. Matlala M, Gous AG, Godman B, Meyer JC. Structure and activities of pharmacy and therapeutics committees among public hospitals in South Africa; findings and implications. Expert Rev Clin Pharmacol. 2017;10(11):1273–1280. doi:10.1080/17512433.2017.1364625
107. Mpinda-Joseph P, Anand Paramadhas BD, Reyes G, et al. Healthcare-associated infections including neonatal bloodstream infections in a leading tertiary hospital in Botswana. Hosp Pract. 2019;47(4):203–210. doi:10.1080/21548331.2019.1650608
108. Lee MH, Lee GA, Lee SH, Park YH. Effectiveness and core components of infection prevention and control programmes in long-term care facilities: a systematic review. J Hosp Infect. 2019;102(4):377–393. doi:10.1016/j.jhin.2019.02.008
109. Sharland M, Gandra S, Huttner B, et al. Encouraging AWaRe-ness and discouraging inappropriate antibiotic use-the new 2019 Essential Medicines List becomes a global antibiotic stewardship tool. Lancet Infect Dis. 2019;19(12):1278–1280. doi:10.1016/S1473-3099(19)30532-8
110. Saleem Z, Hassali MA, Godman B, et al. Sale of WHO AWaRe groups antibiotics without a prescription in Pakistan: a simulated client study. J Pharm Policy Pract. 2020;13(1):26. doi:10.1186/s40545-020-00233-3
111. Mashaba TP, Matlala M, Godman B, Meyer JC. Implementation and monitoring of decisions by pharmacy and therapeutics committees in South African public sector hospitals. Expert Rev Clin Pharmacol. 2019;12(2):159–168. doi:10.1080/17512433.2018.1545572
112. Brooks J. US Medicare will stop paying for preventable errors. CMAJ. 2007;177(8):841–842. doi:10.1503/cmaj.071347
113. Alrasheedy AA, Alsalloum MA, Almuqbil FA, et al. The impact of law enforcement on dispensing antibiotics without prescription: a multi-methods study from Saudi Arabia. Expert Rev Anti Infect Ther. 2020;18(1):87–97. doi:10.1080/14787210.2020.1705156
114. Jacobs TG, Robertson J, van den Ham HA, Iwamoto K, Bak Pedersen H, Mantel-Teeuwisse AK. Assessing the impact of law enforcement to reduce over-the-counter (OTC) sales of antibiotics in low- and middle-income countries; a systematic literature review. BMC Health Serv Res. 2019;19(1):536. doi:10.1186/s12913-019-4359-8
115. Anand Paramadhas BD, Tiroyakgosi C, Mpinda-Joseph P, et al. Point prevalence study of antimicrobial use among hospitals across Botswana; findings and implications. Expert Rev Anti Infect Ther. 2019;17(7):535–546. doi:10.1080/14787210.2019.1629288
116. Talaat M, Saied T, Kandeel A, et al. A point prevalence survey of antibiotic use in 18 hospitals in Egypt. Antibiotics. 2014;3(3):450–460. doi:10.3390/antibiotics3030450
117. Saied T, Hafez SF, Kandeel A, et al. Antimicrobial stewardship to optimize the use of antimicrobials for surgical prophylaxis in Egypt: a multicenter pilot intervention study. Am J Infect Control. 2015;43(11):e67–e71. doi:10.1016/j.ajic.2015.07.004
118. Ntumba P, Mwangi C, Barasa J, Aiken A, Kubilay Z, Allegranzi B. Multimodal approach for surgical site infection prevention – results from a pilot site in Kenya. Antimicrob Resist Infect Control. 2015;4(1):P87. doi:10.1186/2047-2994-4-S1-P87
119. Okoth C, Opanga S, Okalebo F, Oluka M, Baker Kurdi A, Godman B. Point prevalence survey of antibiotic use and resistance at a referral hospital in Kenya: findings and implications. Hosp Pract. 2018;46(3):128–136. doi:10.1080/21548331.2018.1464872
120. Oshikoya KA, Ogunyinka IA, Adamaigbo C, Olowo-Okere A. Surgical antimicrobial prophylaxis and its dose appropriateness among paediatric patients in a Nigerian teaching hospital. J Chemother. 2019;31(6):329–342. doi:10.1080/1120009X.2019.1615725
121. Fowotade A, Fasuyi T, Aigbovo O, et al. Point prevalence survey of antimicrobial prescribing in a Nigerian hospital: findings and implications on antimicrobial resistance. West Afr J Med. 2020;37(3):216–220.
122. Saleem Z, Hassali MA, Versporten A, et al. A multicenter point prevalence survey of antibiotic use in Punjab, Pakistan: findings and implications. Expert Rev Anti Infect Ther. 2019;17(4):285–293. doi:10.1080/14787210.2019.1581063
123. Satti MZ, Hamza M, Sajid Z, et al. Compliance rate of surgical antimicrobial prophylaxis and its association with knowledge of guidelines among surgical residents in a tertiary care public hospital of a developing country. Cureus. 2019;11(5):e4776.
124. Kaya S, Aktas S, Senbayrak S, et al. An evaluation of surgical prophylaxis procedures in Turkey: a multi-center point prevalence study. Eurasian J Med. 2016;48(1):24–28. doi:10.5152/eurasianjmed.2015.15222
125. Gomez MI, Acosta-Gnass SI, Mosqueda-Barboza L, Basualdo JA. Reduction in surgical antibiotic prophylaxis expenditure and the rate of surgical site infection by means of a protocol that controls the use of prophylaxis. Infect Control Hosp Epidemiol. 2006;27(12):1358–1365. doi:10.1017/S0195941700075305
126. Bozkurt F, Kaya S, Tekin R, et al. Analysis of antimicrobial consumption and cost in a teaching hospital. J Infect Public Health. 2014;7(2):161–169. doi:10.1016/j.jiph.2013.09.007
127. Kim RY, Kwakye G, Kwok AC, et al. Sustainability and long-term effectiveness of the WHO surgical safety checklist combined with pulse oximetry in a resource-limited setting: two-year update from Moldova. JAMA Surg. 2015;150(5):473–479. doi:10.1001/jamasurg.2014.3848
128. Brink AJ, Messina AP, Feldman C, Richards GA, van den Bergh D. From guidelines to practice: a pharmacist-driven prospective audit and feedback improvement model for peri-operative antibiotic prophylaxis in 34 South African hospitals. J Antimicrob Chemother. 2017;72(4):1227–1234. doi:10.1093/jac/dkw523
129. Allegranzi B, Aiken AM, Zeynep Kubilay N, et al. A multimodal infection control and patient safety intervention to reduce surgical site infections in Africa: a multicentre, before-after, cohort study. Lancet Infect Dis. 2018;18(5):507–515. doi:10.1016/S1473-3099(18)30107-5
130. Abubakar U, Syed Sulaiman SA, Adesiyun AG, Lo TS. Impact of pharmacist-led antibiotic stewardship interventions on compliance with surgical antibiotic prophylaxis in obstetric and gynecologic surgeries in Nigeria. PLoS One. 2019;14(3):e0213395. doi:10.1371/journal.pone.0213395
131. Ozgun H, Ertugrul BM, Soyder A, Ozturk B, Aydemir M. Peri-operative antibiotic prophylaxis: adherence to guidelines and effects of educational intervention. Int J Surg. 2010;8(2):159–163. doi:10.1016/j.ijsu.2009.12.005
132. Godman B, Shrank W, Andersen M, et al. Comparing policies to enhance prescribing efficiency in Europe through increasing generic utilization: changes seen and global implications. Expert Rev Pharmacoecon Outcomes Res. 2010;10(6):707–722. doi:10.1586/erp.10.72
133. Godman B, Wettermark B, Miranda J, Bennie M, Martin A, Malmstrom RE. Influence of multiple initiatives in Sweden to enhance ARB prescribing efficiency following generic losartan; findings and implications for other countries. Int J Clin Pract. 2013;67(9):853–862. doi:10.1111/ijcp.12130
134. Martin A, Godman B, Miranda J, et al. Measures to improve angiotensin receptor blocker prescribing efficiency in the UK: findings and implications. J Comp Eff Res. 2014;3(1):41–51. doi:10.2217/cer.13.83
135. Leporowski A, Godman B, Kurdi A, et al. Ongoing activities to optimize the quality and efficiency of lipid-lowering agents in the Scottish national health service: influence and implications. Expert Rev Pharmacoecon Outcomes Res. 2018;18(6):655–666. doi:10.1080/14737167.2018.1501558
136. Godman B, Kurdi A, McCabe H, et al. Ongoing initiatives within the Scottish National Health Service to affect the prescribing of selective serotonin reuptake inhibitors and their influence. J Comp Eff Res. 2019;8(7):535–547. doi:10.2217/cer-2018-0132
137. Furst J, Cizman M, Mrak J, et al. The influence of a sustained multifaceted approach to improve antibiotic prescribing in Slovenia during the past decade: findings and implications. Expert Rev Anti Infect Ther. 2015;13(2):279–289. doi:10.1586/14787210.2015.990381
138. Molstad S, Lofmark S, Carlin K, et al. Lessons learnt during 20 years of the Swedish strategic programme against antibiotic resistance. Bull World Health Organ. 2017;95(11):764–773. doi:10.2471/BLT.16.184374
139. Bao L, Peng R, Wang Y, et al. Significant reduction of antibiotic consumption and patients’ costs after an action plan in China, 2010–2014. PLoS One. 2015;10(3):e0118868. doi:10.1371/journal.pone.0118868
140. Godman B, Bishop I, Finlayson AE, Campbell S, Kwon HY, Bennie M. Reforms and initiatives in Scotland in recent years to encourage the prescribing of generic drugs, their influence and implications for other countries. Expert Rev Pharmacoecon Outcomes Res. 2013;13(4):469–482. doi:10.1586/14737167.2013.820956
141. Godman B, Petzold M, Bennett K, et al. Can authorities appreciably enhance the prescribing of oral generic risperidone to conserve resources? Findings from across Europe and their implications. BMC Med. 2014;12:98. doi:10.1186/1741-7015-12-98
142. Bennie M, Bishop I, Godman B, et al. Are prescribing initiatives readily transferable across classes: the case of generic losartan in Scotland? Qual Prim Care. 2013;21(1):7–15.
143. Kim Y, Kwon H-Y, Godman B, Moorkens E, Simoens S, Bae S. Uptake of biosimilar infliximab in the UK, France, Japan, and Korea: budget savings or market expansion across countries? Front Pharmacol. 2020;11:970. doi:10.3389/fphar.2020.00970
144. Abilova V, Kurdi A, Godman B. Ongoing initiatives in Azerbaijan to improve the use of antibiotics; findings and implications. Expert Rev Anti Infect Ther. 2018;16(1):77–84. doi:10.1080/14787210.2018.1417835
145. Bojanic L, Markovic-Pekovic V, Skrbic R, et al. Recent initiatives in the Republic of Srpska to enhance appropriate use of antibiotics in ambulatory care; their influence and implications. Front Pharmacol. 2018;9:442. doi:10.3389/fphar.2018.00442
146. Wojkowska-Mach J, Godman B, Glassman A, et al. Antibiotic consumption and antimicrobial resistance in Poland; findings and implications. Antimicrob Resist Infect Control. 2018;7(1):136. doi:10.1186/s13756-018-0428-8
147. Campbell SM, Godman B, Diogene E, et al. Quality indicators as a tool in improving the introduction of new medicines. Basic Clin Pharmacol Toxicol. 2015;116(2):146–157. doi:10.1111/bcpt.12295
148. Robertson J, Iwamoto K, Hoxha I, et al. Antimicrobial medicines consumption in Eastern Europe and Central Asia – an updated cross-national study and assessment of quantitative metrics for policy action. Front Pharmacol. 2019;9:1156. doi:10.3389/fphar.2018.01156
149. Le Maréchal M, Tebano G, Monnier AA, et al. Quality indicators assessing antibiotic use in the outpatient setting: a systematic review followed by an international multidisciplinary consensus procedure. J Antimicrob Chemother. 2018;73(suppl_6):vi40–vi9. doi:10.1093/jac/dky117
150. Ghassemi S, Dehnavieh R. Applying the results of Health Technology Assessment reports in developing countries, the pale face of coin. Technol Health Care. 2016;24(5):781–782. doi:10.3233/THC-161233
151. Oortwijn W, van Oosterhout S, Kapiriri L. Application of evidence-informed deliberative processes in health technology assessment in low- and middle-income countries. Int J Technol Assess Health Care. 2020;1–5.
152. Dehnavieh R, Noori Hekmat S, Ghasemi S, Mirshekari N. The vulnerable aspects of application of “Health Technology Assessment”. Int J Technol Assess Health Care. 2015;31(3):197–198. doi:10.1017/S0266462315000288
153. Oortwijn W, Determann D, Schiffers K, Tan SS, van der Tuin J. Towards integrated health technology assessment for improving decision making in selected countries. Value Health. 2017;20(8):1121–1130. doi:10.1016/j.jval.2017.03.011
154. WHO. Key elements for establishing a national system of HTA; 2020. Available from: https://www.who.int/health-technology-assessment/about/SYSTEMHTA/en/.
155. Gustafsson LL, Wettermark B, Godman B, et al. The ‘wise list’- a comprehensive concept to select, communicate and achieve adherence to recommendations of essential drugs in ambulatory care in Stockholm. Basic Clin Pharmacol Toxicol. 2011;108(4):224–233. doi:10.1111/j.1742-7843.2011.00682.x
156. Eriksen J, Gustafsson LL, Ateva K, et al. High adherence to the ‘Wise List’ treatment recommendations in Stockholm: a 15-year retrospective review of a multifaceted approach promoting rational use of medicines. BMJ Open. 2017;7(4):e014345. doi:10.1136/bmjopen-2016-014345
157. Bjorkhem-Bergman L, Andersen-Karlsson E, Laing R, et al. Interface management of pharmacotherapy. Joint hospital and primary care drug recommendations. Eur J Clin Pharmacol. 2013;69(Suppl 1):73–78. doi:10.1007/s00228-013-1497-5
158. Yoon CH, Ritchie SR, Duffy EJ, et al. Impact of a smartphone app on prescriber adherence to antibiotic guidelines in adult patients with community acquired pneumonia or urinary tract infections. PLoS One. 2019;14(1):e0211157. doi:10.1371/journal.pone.0211157
159. Campbell SM, Kontopantelis E, Hannon K, Burke M, Barber A, Lester HE. Framework and indicator testing protocol for developing and piloting quality indicators for the UK quality and outcomes framework. BMC Fam Pract. 2011;12:85. doi:10.1186/1471-2296-12-85
160. Lorencatto F, Charani E, Sevdalis N, Tarrant C, Davey P. Driving sustainable change in antimicrobial prescribing practice: how can social and behavioural sciences help? J Antimicrob Chemother. 2018;73(10):2613–2624. doi:10.1093/jac/dky222
161. McGinn D, Godman B, Lonsdale J, Way R, Wettermark B, Haycox A. Initiatives to enhance the quality and efficiency of statin and PPI prescribing in the UK: impact and implications. Expert Rev Pharmacoecon Outcomes Res. 2010;10(1):73–85. doi:10.1586/erp.09.73
162. Schellack N, Bronkhorst E, Coetzee R, et al. SASOCP position statement on the pharmacist’s role in antibiotic stewardship 2018. South Afr J Infect Dis. 2018;33(1):28–35. doi:10.4102/sajid.v33i1.24
163. Chigome AK, Matlala M, Godman B, Meyer JC. Availability and use of therapeutic interchange policies in managing antimicrobial shortages among South African public sector hospitals; findings and implications. Antibiotics. 2019;9(1):4. doi:10.3390/antibiotics9010004
 © 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2021 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.