Back to Journals » Advances in Medical Education and Practice » Volume 13
“Keep It Simple”—Co-Creation of a Tailored Newborn Resuscitation Course for Midwifery Students
Authors Ljungblad LW ![]() , Skovdahl K, McCormack B
, Skovdahl K, McCormack B ![]() , Dahl B
, Dahl B ![]()
Received 2 November 2021
Accepted for publication 23 December 2021
Published 18 January 2022 Volume 2022:13 Pages 81—93
DOI https://doi.org/10.2147/AMEP.S346991
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Prof. Dr. Balakrishnan Nair
Linda Wike Ljungblad,1 Kirsti Skovdahl,2 Brendan McCormack,2,3 Bente Dahl1
1Centre for Women’s, Family and Child Health, Faculty of Health and Social Sciences, University of South-Eastern Norway, Kongsberg, Norway; 2Faculty of Health and Social Sciences, University of South-Eastern Norway, Kongsberg, Norway; 3Centre for Person-Centred Practice Research, School of Health Sciences, Queen Margaret University, Edinburgh, UK
Correspondence: Linda Wike Ljungblad
Centre for Women’s, Family and Child Health, Faculty of Health and Social Sciences, University of South-Eastern Norway, P.O. Box 235, Kongsberg, N-3603, Norway
Tel +47 93458429
Email [email protected]
Purpose: To develop a tailored newborn resuscitation course for midwifery students.
Patients and Methods: A qualitative study using an explorative, abductive approach was applied. Co-creation through workshops was facilitated to develop a tailored newborn resuscitation course for midwifery students. Four workshops with midwifery students and midwives were conducted from May to October 2020. Twenty participants attended one workshop of their choice. Five out of Norway’s six midwifery education programmes participated, and included midwives from across Norway. All workshops were held digitally via the Zoom platform. A seven-step framework analysis method was applied to analyse the workshop data.
Results: We identified four themes: 1) practice guidance, 2) technical skills 3) non-technical skills 4) innovative methods.
Conclusion: Findings emphasize the importance of practice guidance, technical skills, non-technical skills and innovative methods to facilitate the learning process. However, these skills cannot be acquired without the context to facilitate them, and thus a supportive culture is essential to sustain newborn resuscitation expertise as a midwife/midwifery student. We found that midwives expressed the same need to learn, train and prepare themselves for newborn resuscitation as midwifery students. The importance of facilitating the learning of newborn resuscitation with low-dose, high-frequency training in a supportive culture thus matters to both midwifery students and expert midwives.
Keywords: co-creation, course, framework analysis, midwifery students, midwives, newborn resuscitation, PARIHS framework
Introduction
Newborn resuscitation is largely defined as a set of interventions initiated after delivery to help newborn babies start breathing.1 The complexity of handling newborn resuscitation is particularly pertinent to midwifery, as midwives perform the most deliveries globally.2 Approximately 10% of all newborn babies need some assistance with the natural transition to breathing after birth,3 and recent evidence suggests that this might be as high as 20%.4 It is therefore essential that midwives are able to respond appropriately, and to maintain their newborn resuscitation skills. Moreover, to ensure that midwives handle newborn resuscitation appropriately, midwifery students must learn these skills before becoming registered midwives.5
However, newborn resuscitation has historically been a challenge for midwives. In 1987, the American Academy for Pediatrics (AAP) implemented a newborn resuscitation programme (NRP) that has been continuously improved.6 Two decades ago, a new paradigm in teaching newborn resuscitation was recommended, due to the lack of fidelity of the newborn manikin traditionally used.7 While this goal has been addressed in recent years, calls remain for a cultural change around what constitutes the essential components of newborn resuscitation.8 Moreover, midwifery studies from around the world report other challenges associated with performing newborn resuscitation: among these are a lack of knowledge and skills, organizational constraints and inadequate teamwork.9,10 Additional studies highlight an urgent need to strengthen simulation-based training for effective newborn resuscitation, and for formal education in order to increase midwives’ competency in this area.11,12
In a previous study, we found that midwives described newborn resuscitation as frightening, complex and challenging;2 we thus identified the importance of tailoring a course for midwifery students to prepare them for newborn resuscitation through their own contextual understandings. This tailored newborn resuscitation course emphasizes a supportive culture and simplified guidelines for performing newborn resuscitation.5
Further, although effective ventilation is the most critical step in newborn resuscitation13 and indeed has been described as a cornerstone in newborn resuscitation,14 ineffective ventilation is often the reason for unsuccessful resuscitation.15 Due to midwives’ infrequent exposure to newborn resuscitation in clinical training, professional development programmes are needed to improve their skills in this area.16 In the current study, therefore, we focused on midwifery students’ process of learning about and preparing for newborn resuscitation; we then developed a prospective course through co-creation with midwifery students and midwives, which might be transferrable to similar settings.
Maternity services in Norway operate from the perspective that all pregnant women are healthy or without complicating factors during their pregnancies. Healthy women are selected into categories in delivery with a midwife in charge. Any pathologies in pregnancy that require medical treatment are seen by an obstetrician in addition to the midwife. Norwegian midwives are registered with an additional authorization after being registered as nurses, and are solely responsible for all normal deliveries. This responsibility is split between actively supporting a mother’s safe delivery of her baby and her baby’s need of newborn resuscitation.
Norwegian midwives assess all newborn babies for Apgar scores at 1, 5 and 10 minutes following birth.17 When newborn babies do not breathe within one minute, immediate assistance is required. As midwives are present at most deliveries, they are tasked with providing newborn babies sufficient assistance at the correct time to naturally transition to breathing. This transition also needs “some seconds”, and it is challenging to measure precisely when the situation is no longer normal: this can be described as tacit knowledge based on years of midwifery experience and practice. The midwifery role and midwives’ tacit knowledge in newborn resuscitation is essential for their ability to conduct correct assessments and initiate newborn resuscitation at the correct time. In addition, there is a need to consider contextual factors that impact on the gaining and sustaining of these skills, like the culture created at each maternity ward.18
There is limited research on how midwifery students learn to perform newborn resuscitation. However, three Australian studies describe midwifery students’ experiences of simulation exercises for newborn resuscitation.19–21 While midwifery students reported improved knowledge, confidence and skills in newborn resuscitation after these exercises,20,21 their anxiety levels stayed static, even though they were better prepared.19 Simulation training as a method of learning has been emphasized as suitable for small groups, in which everyone has an active role in debriefing and reflecting on the clarity of communication and situational awareness.21 Notably, for it to be effective, this training needs to be repeated over a longer period of time.20 Additionally, role understanding is highlighted as essential in midwifery to ensure correct priorities and responsibilities.20 Students have limited opportunity to practise newborn resuscitation in clinical practice; as such, there is a need to improve support in midwifery education to manage such complex situations.22 Moreover, research suggests that the current approach to improving midwifery students’ understanding and developing their cognitive skills needs to be changed.23
Despite decades of multiple simulation training programmes, midwives still report a need to improve skills and knowledge to be prepared for newborn resuscitation.24 Although courses have been developed and published, no consensus has been reached about how best to prepare midwifery students for the complexity of newborn resuscitation. We therefore designed this study to develop a tailored newborn resuscitation course for midwifery students.
Materials and Methods
Aim
The aim of this study was to develop a tailored newborn resuscitation course for midwifery students.
Design
A qualitative study with an explorative design and an abductive approach was applied.
Theoretical Underpinning
Changing practice and implementing new ideas in midwifery education is complex with respect to both macro and micro aspects. Conceptual frameworks have been developed to help promote the implementation of research into practice,25 as the latter can be “complex, messy and demanding”.26 In this study, the Promoting Action on Research Implementation in Health Services (PARIHS) framework was used to design, plan and facilitate the workshops. This framework is multidimensional and consists of three core structures derived from research on practice development and quality improvement: evidence, context and facilitation. Successful implementation occurs when the evidence matches the context (ie, professional consensus and patient needs). Moreover, to change the culture, leadership that includes internal and external facilitators of change is needed.25 The PARIHS framework has been further developed and validated, especially through “the meaning of context” to promote evidence-based practice.27 The PARIHS framework, as a theory of change, informed our decisions when drawing on the empirical evidence base, contextualizing that evidence base and utilizing local experience and expertise. These components are recognized as part of the evidence constructed in the PARIHS framework. Co-creation in the workshops was facilitated to develop a tailored newborn resuscitation course for midwifery students.28 We discussed the design of the course with the participants; we also discussed how it might work in their specific contexts. We worked iteratively throughout the entire process using the lenses of evidence, context and facilitation.
Recruitment and Participants
Recruiting midwives and midwifery students to participate in the workshops was a two-step-process. In total, 8 midwives and 12 midwifery students contacted the first author, LWL, to participate in 1 of the 4 workshops. Students from five of Norway’s six midwifery programmes participated, as did midwives from across Norway. Table 1 provides details of the characteristics of the workshop participants. Two workshops were comprised of a mix of registered midwives, and two workshops consisted of midwifery student participants.
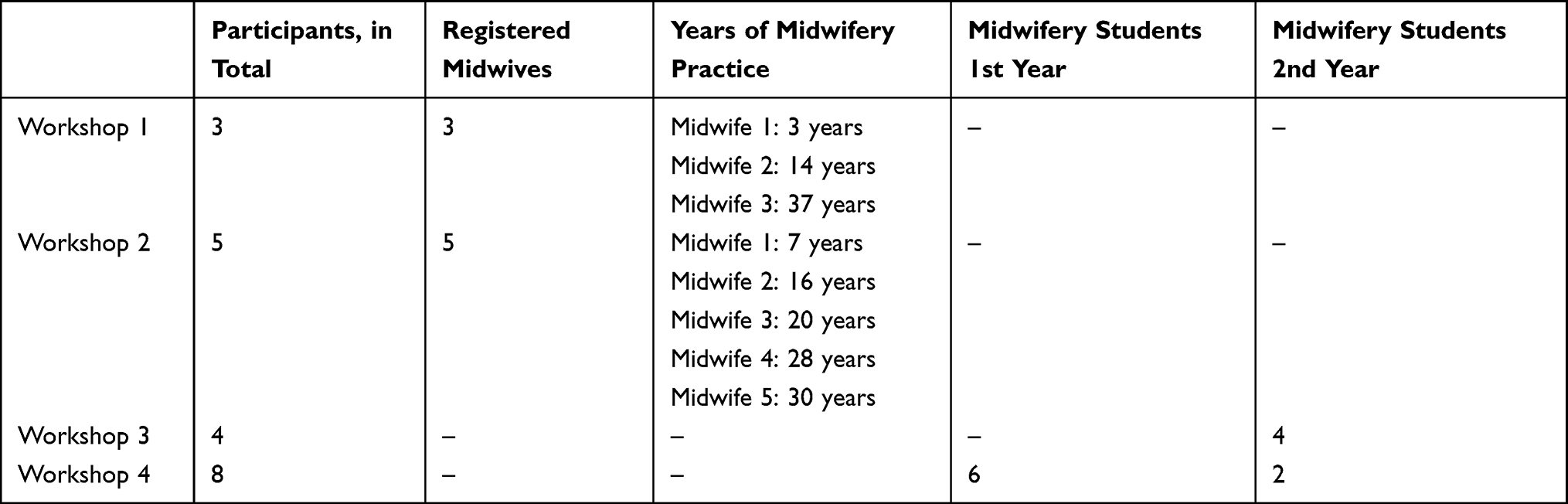 |
Table 1 Characteristics of the Workshop Participants |
Midwives
A convenience sampling method was applied. We recruited midwives for participation from a previous study we conducted that focused on midwives’ experiences of newborn resuscitation.2 Sixteen midwives from the prior study were contacted and asked if they would be interested in participating digitally in the co-creation of a newborn resuscitation course. Eight midwives attended either of the two workshops that were scheduled at dates and times convenient for participants.
Midwifery Students
Midwifery students were recruited from most of the midwifery programmes in Norway to ensure a wide distribution in our sample. They received information about the study via Facebook (a midwifery forum) and Canvas (the universities’ digital platform for midwifery education). They were willing to give their perspectives on the prospective content of a newborn resuscitation course for midwifery students.
Data Collection
Four digital workshops were conducted from May to October 2020 via the Zoom platform due to COVID-19 restrictions. The workshops lasted from 70 to 111 minutes. LWL facilitated all workshops, of which a co-researcher attended two. LWL emphasized the value of participating in the development of this newborn resuscitation course. The aim was to create a safe, respectful and non-judgemental atmosphere, by emphasizing expert competence and valuing all participants’ ideas, perspectives and experiences.
All participants briefly introduced themselves, and they were encouraged to talk freely and to interrupt when they had ideas to share. We used several creative tools in the workshops to stimulate participant engagement. For example, we focused on the top section of the existing guidelines by holding up an empty gold frame. This frame symbolized the “golden minute”, to help participants visualize the importance of a midwifery focus when encountering non-breathing newborn babies at birth. The participants were asked to describe and discuss what this focus should consist of. Next, a video clip from the British Broadcasting Corporation (BBC) production Call the Midwife29 was used to illustrate what a period of 60 seconds feels like in a resuscitation situation. Participants then made a word cloud online with words they would use to describe and characterize newborn resuscitation. After this introduction, participants were encouraged to discuss how to tailor a newborn resuscitation course for midwifery students. A poem describing newborn resuscitation from outside the discipline of midwifery was read aloud to stimulate further discussion.30
We chose to conduct workshops to build on each other’s experiences and ideas in a co-creation process. To ensure that all participants’ voices were heard, follow-up questions were asked to give each participant the opportunity to contribute. The workshops were both audio- and video-recorded through Zoom. Three-hundred and fifty-one minutes of workshop-material was transcribed verbatim, resulting in 143 pages of data for analysis.
The themes that emerged from the analyses were then translated into a prospective newborn resuscitation course for midwifery students. The outline for this course was sent by e-mail to all participants for review, and we asked for their feedback: all participants who answered agreed to the course outline.
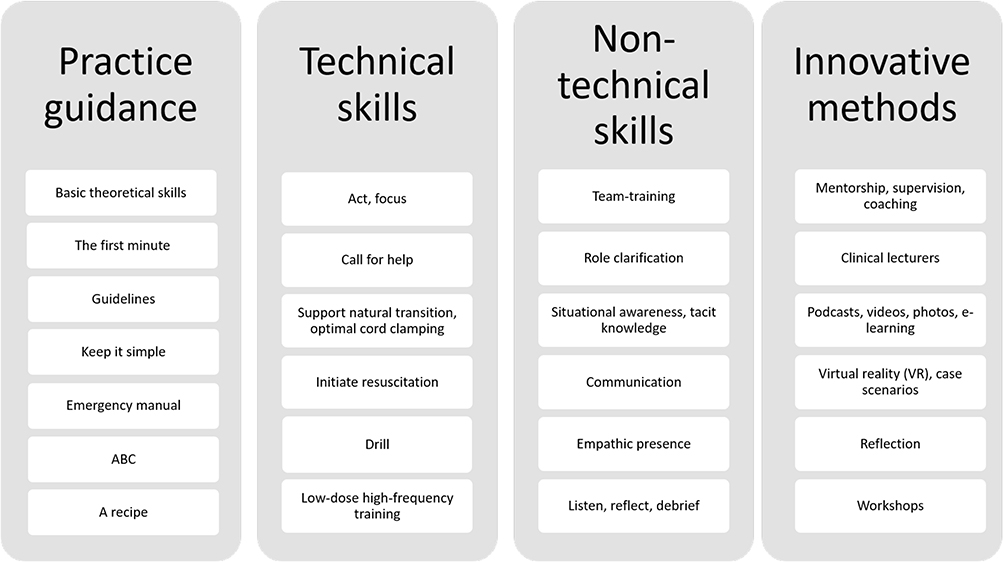 |
Figure 1 Themes regarding the development of a midwifery newborn resuscitation course. |
Ethical Considerations
The study was conducted in accordance with the Helsinki Declaration.31 Approval for this study was given by the Regional Ethics Committee, and the Norwegian Centre for Research Data. Coreq checklist was applied. All participants received written information about the study, including assurances of anonymity and confidentiality, with the opportunity to withdraw from the study at any time without explanation. This information was sent by e-mail to all participants before participating in the workshops. All participants also received an e-mail with an invitation to the digital workshops and agreed to participate by entering the digital workshop room at the scheduled time. Audio- and video-recordings from each workshop were accepted by the participants and field notes were written. Data were stored on a safe server at our university, accessed only by the first author. Lists of participants and codes were kept separately in a locked drawer. To further ensure confidentiality, the quotations selected for this article do not expose any participants’ identity.
Data Analysis
Data analysis was informed by a seven-stage model of framework analysis,32,33 detailed below.
Stage 1: Transcription. LWL transcribed each workshop verbatim and anonymized all participants before starting the analysis. Double spacing and large margins were created for later coding, impressions and analytical comments.
Stage 2: Familiarization with the data. LWL transcribed and re-listened to all workshop recordings, and thus familiarized herself with the empirical material as a whole. LWL also read and read the notes, comments and impressions she had written. The other researchers read the transcribed material or attended the workshops.
Stage 3: Coding. This stage was informed by the constructs from the overarching PARIHS framework. The transcriptions were read line by line and marked with codes describing what participants found important eg, values, behaviours, incidents or structures within newborn resuscitation. We coded all data for further comparison with the entire data set. The coding was done with pen, paper, a yellow highlighter and sticky notes of varying colours.
Stage 4: Developing a working analytical framework. After coding the transcripts, the labels were compared and grouped together into categories. The researchers met weekly (digitally) to work on the development of this analytical framework. It was an iterative process, and several codes and different approaches were tried out to help us visualize the framework.
Stage 5: Applying the analytical framework. Each code was used as an index for easy identification in the transcripts. We structured and organized the data to make it accessible for further analysis.
Stage 6: Charting data into the framework matrix. A large amount of data were entered into the framework matrix. A vital step in the analysis process was to summarize and reduce the data. Whole segments of data relating to different categories from each workshop transcript were first entered into the matrix before they were reduced, but they retained their original meaning. Illustrative quotations were also noted.
Stage 7: Interpreting the data. LWL wrote notes before, during and after the workshops to make sure that impressions, thoughts and early understandings of the data were noted. In this final stage, we revisited these notes after working on the matrix, and found a general similarity to our initial understanding of the data. Gradually, however, differences between the data emerged, and four clear themes were identified in response to our study aim.
Results
We identified four themes that emerged regarding the development of a tailored newborn resuscitation course for midwifery students: 1) practice guidance, 2) technical skills, 3) non-technical skills, and 4) innovative methods. These themes are illustrated in Figure 1, and form the framework for learning newborn resuscitation.
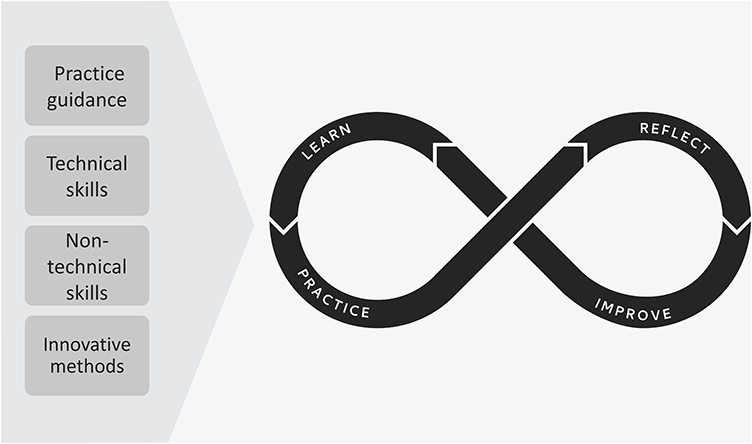 |
Figure 2 Midwifery newborn resuscitation course. |
Practice Guidance
Participants emphasized the importance of basic theoretical skills in the first minute of newborn resuscitation, also describing it as “the most frightening minute”. A midwifery student in Workshop 3 described newborn resuscitation as a “make-it-or-break-it experience”, which she experienced as traumatic. After the experience, she was uncertain as to whether she wanted to continue training to be a midwife; it had occurred early in her placement, and she had felt unsupported during it. Another midwife concurred:
I believe that everyone is scared when initiating newborn resuscitation, but it helps me when I have gained the knowledge I need to be able to act to resolve situations … It is frightening every time I do not know what to do … It is still the same feeling even after decades of experience … I feel a lump in my stomach, but then my mind focuses and it’s as if my brain is going through a tunnel. (Midwife, Workshop 1)
Other participants agreed with this statement, and noted that they felt unprepared to handle these situations because of a lack of training and infrequent clinical emergencies. In each workshop, the complexity of the existing guidelines were discussed. Participants described the national guidelines in newborn resuscitation as overly complex, containing too much text, difficult to understand and hard to follow in emergency situations. An experienced midwife described this as follows:
I believe that is because it’s too complex … I find that the guidelines are too complex even though I have had 35 years of midwifery practice … To make it simple enough is what is most difficult … focusing on the top section of the guidelines … Surrounding factors also matter. (Midwife, Workshop 1)
Additionally, midwives discussed the challenge of being responsible for the mother and the baby simultaneously, and how this was complicated by the overly complex guidelines. They thus recommended simplified, clear guidelines—such as a checklist or “recipe”—to tell them exactly what to do and when. Indeed, “keep it simple” was repeatedly mentioned among the participants. They suggested that the emergency manual be written like a “recipe” or as an “ABC” specifying the three most important elements, which one person could then read aloud in a resuscitation situation. As this midwife described:
To simplify the three most important elements … Experience, recognition and awareness are complicated to learn … Even after 20 years I question whether I did everything correctly … but I know what to do … Three elements, like an ABC for students. Then experience will come later. (Midwife, Workshop 2)
Technical Skills
Technical skills were highlighted as a priority. Participants noted that all students and midwives need this basic knowledge before advancing their skills and integrating non-technical skills into the complexity of newborn resuscitation situations:
Learning by doing … hands on … It might be a secure start if the teacher enters the room after the students have practised for a while … It is about feeling secure, and being allowed to fail. (Midwifery student, Workshop 4)
Keeping a clear focus on ventilation in newborn resuscitation was described as essential, as well as being familiar with all equipment. Moreover, most participants cited calling for help and initiating resuscitation by stimulation and ventilation as supporting newborns’ transition to breathing. Optimal cord-clamping was mentioned as another important measure to continue to provide newborn babies with already pre-warmed oxygenated blood. Participants also discussed that resuscitations could often be avoided if the cord was kept intact:
It’s important to teach midwifery students that as long as the placenta and the cord are intact, there is no need to panic, because the “life-vest”, the umbilical cord, is still attached to the newborn baby and we must support this normal phenomenon. Warm, oxygen-rich whole blood is still finding its way from the placenta into the newborn baby. (Midwife, Workshop 2)
Technical equipment was pointed to as important for supporting the natural transition to breathing and simultaneously initiate resuscitation. A drill to “practise, practise, and practise” systematically was mentioned as the only way to gain and sustain skills in newborn resuscitation. Regular simulation training and practical training were requested, as many midwives reported having simulation training only once per year. Short sessions, repeated frequently and preferably mandatory, were recommended. As this midwifery student explained:
‘Training has to be frequent … regular and frequent … Instead of training for two hours, it should be repeated until one becomes skilled and feels safe and secure’. (Midwifery Student, Workshop 3)
Low-dose high-frequency training was suggested by the participants as a solution to becoming skilled in newborn resuscitation. Another midwifery student highlighted the following goal:
The goal must be to train as much as necessary until one can act automatically when required … just acting without stopping and thinking … I believe it is the frequency of the training that gives the feeling of safety and security. (Midwifery student, Workshop 4)
Non-Technical Skills
Team-training was suggested as a solution for all professions to get to know each other for better cooperation. Role clarification was discussed as essential for successful resuscitation. Several midwives described having unclear roles, and often experiencing conflicts of values in situations where the mother and newborn baby were separated after delivery because the equipment for resuscitation was placed in another room.
Participants discussed how all midwives will experience newborn resuscitation at some point in their career. They pointed out that although tacit knowledge and midwifery experience are often forgotten in a busy ward, they are important to teach midwifery students. Here, situational awareness and embodying the essential principles of resuscitation were seen as essential to learn—but challenging to teach. One midwife described this as follows:
You cannot transfer 10 years of midwifery knowledge and 3 to 4 resuscitations into a student … This is my intuitive understanding, where I save my thousands of impressions and do not have to analyse but immediately recognize similar situations … I value my knowledge gained through years of experience as pure gold, calling it my “emergency tool-box” … We can give students tools for building their experience … and help them dare to be humble and ask for help … This is the content of tacit midwifery knowledge. (Midwife, Workshop 2)
Participants considered communication as a bridge among all professionals on the birth team. They were clear about the need for training in effective communication, and claimed it was “the root of everything”. They emphasized the importance of being skilled in non-verbal communication, as well, such as facial expressions or glances. As one midwife noted:
I just nodded my head and my colleagues responded with a smile to confirm that everything was okay’. (Midwife, Workshop 1)
Relatedly, the midwives emphasized that “chaos control” was important for students to learn as part of non-verbal communication. Some midwives described how tranquillity could quickly turn to chaos. Further, participants noted and discussed the impact of their empathic presence on the emergency team. Moreover, feeling safe in the team was emphasized as important:
We all quickly become part of a culture, good or bad. It is our responsibility to be aware and include students in a positive environment … to support each other to become good at what we do … to become part of our winning team. (Midwife, Workshop 2)
“Listening and reflection groups” were suggested as a way to help midwives reflect on their own and other’s actions. One midwife described this as follows:
No matter how much education we embed in the students, it does not change the fact that the maternity ward is an acute ward and midwives will encounter difficult situations as part of the job. We need to reflect together in systematic debriefing sessions. You cannot be a midwife by only approaching the positive aspects. (Midwife, Workshop 2)
To facilitate reflection and discussion, self-selected small groups were preferred—especially for debriefing. As this midwifery student stated:
It has to be a safe learning environment, preferably in small groups … with somebody you feel safe with … and somebody who focuses on the fact that it is not a test, but a training session … But we are kind of tested all the time in our practical placement. (Midwifery student, Workshop 3)
Innovative Methods
Participants highlighted the importance of mentorship and supervision in developing midwifery students’ confidence and preparation regarding newborn resuscitation. The participants discussed various creative and innovative methods for learning newborn resuscitation. Midwifery students requested engagement from clinical lecturers, as they could bring their clinical experience into their teaching about newborn resuscitation. The students described newborn transition as the most difficult topic to learn, because of the advanced physiology of cardiopulmonary circulation. They requested more lectures about this, as they highlighted the importance of this understanding.
Podcasts were mentioned as effective tools for learning this physiology, because they could be listened to repeatedly. Videos, photos and e-learning about how to assess newborn babies were pointed to as other useful learning tools. Virtual reality (VR) and case scenarios were also described as beneficial, as they emphasized students’ active role in their own learning.
We use VR and it is fantastic. You get your nose out from the books … It is an excellent way of learning, but it has to be related to existing routines … It would be interesting to try newborn resuscitation in VR … It should be more widely used in midwifery training. I am very happy with it and positively surprised. (Midwifery student, Workshop 4)
Supervision and coaching were reported as the most effective way of learning newborn resuscitation, especially with reflection as the focus. Here, reflection on one’s own learning was described as visualizing what each midwife or student needed to enhance practice. One way of facilitating reflection was to create workshops that include first- and second-year students and help them reflect upon their own learning and be creative within a safe culture. As one student described,
Workshops with first and second year students for sharing recent experiences about being new into midwifery could be useful … It would have been good to share my experiences with somebody at a similar level of education. (Midwifery student, Workshop 3)
Summarized and Interpreted Results
The very first results is presented in Figure 1 are recognized as essential components. The midwifery newborn resuscitation course illustrated in Figure 2 is based on participants’ discussions and co-creation in the workshops. New knowledge, practise and reflection are important in order to both improve and maintain skills in newborn resuscitation. Participants in our study were clear about keeping it simple, and we were guided by their advice and feedback when developing our course (Figure 2). The eternity symbol demonstrates the importance of continual training, and that all midwives need to practise newborn resuscitation skills as a lifelong learning process.
Discussion
From the results of this study, we discerned the importance of 1) practice guidance, 2) technical skills, 3) non-technical skills and 4) innovative methods in the co-creation and tailoring of a newborn resuscitation course for midwifery students. These themes relate to the process of learning technical and non-technical skills, as well as how midwifery students are being supported and supervised in practice. The themes further relate to developing a culture that enables these students to continue practising their newborn resuscitation skills’ as lifelong learning, even once they become midwives.
To understand midwifery students’ learning process, which is essential to helping them prepare for newborn resuscitation, we drew on34 andragogic model. The authors describe six assumptions developed for adult learning, illustrated in Table 2. They define learning as a process, emphasizing that individualization, responsibility of learning and timing are important factors in the gaining of knowledge.34 Especially pertinent to our study is students’ need to know, readiness to learn and how they move from one developmental stage to the next; Figure 2 describes how the newborn resuscitation course can spark a newborn resuscitation course lifelong learning process for midwifery students. This is what the eternity symbol in Figure 2 is intended to represent: new questions will be raised that demand new answers, which in turn require further learning and development, sparking new questions, and so the cycle continues. The curiosity appears when midwifery students bring their theoretical knowledge into their clinical practice.
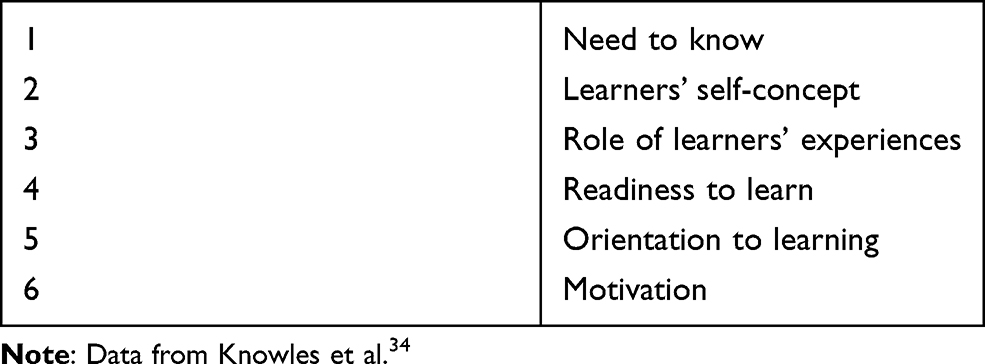 |
Table 2 The Andragogical Model |
Learn
To learn newborn resuscitation, workshop participants were clear that it must be made as simple as possible. Indeed, as previously stated, “keep it simple” was a common refrain among participants. A key consideration therefore in tailoring our course was to make it simple enough both to follow and to help students understand the complexity of newborn resuscitation (see Figure 2). This course was tailored to the individual via a stepwise approach to learning. In this process, midwifery students defined their “need to know” and take responsibility for their own learning in accordance with the andragogical model.34 This relates to workshop participants’ requests for tools upon which to build their experience: that they requested new approaches to learning highlights their sense of responsibility for their own learning. In the workshops, midwifery students explained that, following their first clinical practice, they were motivated to learn skills in newborn resuscitation because they had first-hand knowledge of what was at stake. Here, personal motivation was highlighted by most participants as essential, since it was clear that all midwives would eventually deliver a newborn baby in need of resuscitation. This finding is important, as motivation must be present if the learning process is to start, according to the andragogical model:34 in other words, midwifery students will master newborn resuscitation skills once they are ready to learn them. We understand this as students’ need to understand why they need to know this information before they develop the motivation to learn it. Following the andragogical model, it all starts with a “why”, which must be answered individually by each midwifery student to tailor their own learning process—much like pressing a “start button”.
Practice
Our findings indicate that midwifery students did not feel ready to perform newborn resuscitation upon graduation. This suggests that the integration of new methods into current midwifery programmes may help midwifery students learn and prepare for newborn resuscitation. Moreover, we found that, here, innovation may be important: in our course, each student learns the necessary skills through a variety of innovative methods that prepare them to handle newborn resuscitation. This learning process demonstrates the importance of individual methods for learning and each student being responsible for their own learning process, according to the andragogical model.34
An important issue in preparing midwifery students for newborn resuscitation is to help them understand the complexity of newborn resuscitation. However, developing this kind of professional understanding is challenging when one has not yet entered the profession, as students must be clear as to why the understanding is necessary.34 Moreover, students reported a disconnect between their training in basic skills and the lack of sustained practice (under the guidance of a mentor). Without this latter, the students described it as a challenge to adapt their basic skills knowledge to their daily work. To facilitate this translation of theoretical knowledge into everyday clinical practice, midwifery students must be provided specific tools for learning. By integrating these innovative methods for learning newborn resuscitation in our course, we add new perspectives into the existing simulation training.
Participants described non-technical skills as challenging in newborn resuscitation, and requested that these be part of the tailored course—especially those related to communication. They wanted more training in communication to prepare themselves, and described instances in which poor communication between team members had led to negative outcomes for the newborn baby. Gaining competence in communication and teamwork has also been reported as challenging in previous research.10 The significant correlation between technical and non-technical scores in training underlines the need for resuscitation education programmes to extend beyond training in technical skills.16 In our study, participants emphasized this through their focus on non-verbal communication: for example, the use of a “nod or a look” to confirm to colleagues whether or not the baby was breathing.
Innovative methods for learning newborn resuscitation is one of the themes that emerged in this study. In the workshops, discussions arose about how different people both gain new knowledge and build on prior knowledge in newborn resuscitation. Additionally, it was emphasized that newborn resuscitation skills need to be continuously improved.35 For decades, these skills have been practised through simulation training; however, simulation creates realistic contexts, evidence suggests that it can never be a substitute for real clinical midwifery experience.36 These authors additionally suggest the development of strategies to help midwifery students reflect on their practice, which relates to our tailoring a course specifically for midwifery students (Figure 2). All students learn differently, and some need more time and repetition than others, which is supported by individualization in the andragogical model. Indeed, participants emphasized different methods for learning as being important, as these would provide them with tools to enhance their own learning. We argue that one size does not fit all, and this study adds new knowledge for learning and understanding the complexity of newborn resuscitation for midwifery students.
One innovative method that emerged from the workshops relates to the use of VR. VR was considered to be beneficial by participants in this study, and research highlights its risk-free potential in clinical skills training.37 Workshop participants recommended increasing the use of VR in midwifery education and newborn resuscitation training. Another innovative learning method that participants cited as beneficial were podcasts. Podcasts were seen as easy to use and could be repeatedly accessed whenever needed. In addition to VR and podcasts, low-dose, high-frequency training was considered to be one of the most important factors in preparing midwives for undertaking newborn resuscitation. Indeed, prior research argues that regular training of practical delivery room understanding should be mandatory.38 In our study, participants stated that this kind of training was not mandatory in any of their hospitals, and the frequency of the training they did have varied widely. None of the participants mentioned that they trained too frequently, however, and in fact they requested more frequent training to feel prepared and to maintain their skills.
Reflect
One important finding is the participants’ emphasis on the (over)complexity of existing guidelines in newborn resuscitation, and their suggestion that innovative methods be used to create an “ABC” approach. Similarly, Wrammert et al39 found positive impacts of clarifying guidelines and responsibilities. Another study suggests that the perceived complexity may also be due to a lack of competency and skills among midwives.10 Indeed, participants in our study described newborn resuscitation as “one of the most frightening situations a midwife will experience”. This statement underpins the importance of meeting their requested need for increased knowledge and skills. Some participants expressed that they were practically prepared for newborn resuscitation, but not for the culture of the practice.
As noted earlier, international evidence supports the need for formal education to increase midwives’ competency in newborn resuscitation,12 and participants in our study concurred with this. They noted that, alongside the teaching of ventilation skills, the contextual factors that impact everyday practice must also be included in any newborn resuscitation course (Figure 2). Moreover, they stated that these contextual factors must be further developed in small debriefing and reflection groups. While they mentioned that practical guidance was important—and indeed they requested more of this—they emphasized that it is not enough in itself to prepare them for practice. Moreover, many of the experienced midwives voiced that, while they had been trained in newborn resuscitation, they were unable to perform it. As such, they stated, something in the culture must change. Whilst practice guidelines may be visible (as posters) in clinical settings, they felt newborn resuscitation should be embedded in a supportive culture where the midwives felt safe, confident and trusted to be able to work together as a team.
In the workshops, participants discussed how best to prepare midwifery students for the reality of meeting newborn resuscitation in different contexts in practice. They noted that, although simulation training with mannequins has been used for decades, it may no longer meet students’ learning needs. Instead, the focus must be on helping midwifery students connect their theoretical education with clinical practice. This relates to the findings of this study with regards to practice guidance. Both midwifery students and midwives emphasized the complexity of translating theory into practice, and the need for reflection and mentorship to develop this ability. As some participants explained, even though they may be trained to handle newborn resuscitation, they still need to be supported and empowered as midwives when they are enacting that practice. Therefore, the complexity of newborn resuscitation requires more than just offering simulation training: we need to look into the context, culture and guidelines to fully understand newborn resuscitation and midwives’ learning needs in this area.
Improve
This article offers new insights into tailoring newborn resuscitation course courses to midwifery students; moreover, it shows how a course like this may spark a lifelong learning process, which students will carry into and throughout their midwifery practice. In the andragogical model, Knowles et al34 describe “moving from one developmental stage to the next”; in our study, we understand this as the improvement of one’s own knowledge and practice. In Figure 2, we illustrate this through the “circle of eternity”, showing how midwifery students advance from basic skills and continue developing in a never-ending process.
We know that there are challenges in preparing midwifery students for newborn resuscitation, even when simulation training is frequently offered. Some of these challenges are linked to poor mannequins or lack of fidelity, relying exclusively on simulation and even the transferability of evidence into practice; nevertheless, we continue to prepare midwifery students using similar methods.7 With a solid evidence base, our paper identifies the need to change the methods we use to train midwifery students for newborn resuscitation. Participants in our study explicitly requested a course tailored to midwives, as existing models prepare other professionals for their tasks in newborn resuscitation.6
Halamek et al8 have detailed the need for a cultural change regarding what are viewed as the essential components of newborn resuscitation. Here, we add that there is also a need for a different approach concerning how we prepare midwifery students for this practice. Midwives are the bridge between obstetricians and paediatricians, and can therefore play an important role in the development of a new, simplified approach to learning newborn resuscitation.
Strengths and Limitations
A strength in our research team was the contribution and variety of inside and outside perspectives on newborn resuscitation, forming a solid knowledge base ensured by our clinical and theoretical backgrounds. Our research group consisted of two professors within nursing, one professor within midwifery and a PhD candidate within midwifery. Two researchers have been clinical midwives, and have experience with newborn resuscitation.
We were surprised that conducting workshops digitally turned out to be a strength rather than a limitation in this study. The digital workshops contributed to dynamic, equal participation and fruitful discussions, as everyone had their cameras turned on. The facilitator ensured that every voice was heard; moreover, the engaged dialogue among participants from across Norway (unknown to each other before the workshop) meant the researchers’ voices were not prioritized over the participants’ in this co-creation, thereby minimizing our interpretations. Although the workshops were originally planned to be held physically, COVID-19 restrictions necessitated that they be conducted digitally. We consider this a strength, as it enabled a wider sample of participants to attend, from all over Norway. This sample gave us a broader perspective on the topic than initially planned.40
Another strength of this study was that the data were collected from both the expert midwives and the students for whom the course was tailored. Their strong interest in participating demonstrates their motivation to learn more about this topic. (However, this might also be a considered a limitation, as their interest could represent selection bias.) We found the recruited sample appropriate for developing a tailored newborn resuscitation course for midwifery students. We also found that this course sparked a learning process that promised to continue beyond just the course, which represents another strength.
As user involvement is a strength and important in creating a course, this study was centred on workshops in co-creation with the stakeholders who will be the end-users of this course, as well as their facilitators and supervisors. We asked them how newborn resuscitation skills can best be learned. In these workshops with midwifery students and midwives, we collaborated to identify key factors in order to tailor a newborn resuscitation course for midwifery students. Existing courses for midwifery students in newborn resuscitation are not reported to include user-involvement, which reflects an important knowledge gap. Based on the theoretical framework of the PARIHS framework, we emphasize user involvement, co-creation and all participants’ expert competence in this study.
The core constructs of the PARIHS framework are based on evidence, context and facilitation, which have shaped this study through all its stages. The evidence was collected from two prior studies to form a solid base for further development of the newborn resuscitation course. The context was broad and flexible, as methods for collecting data in workshops were based on creative elements. In each workshops, the facilitation of discussion was attended to, in an effort to create engagement and a safe environment in which participants could freely discuss. Further evaluation and implementation is planned. As such, the theoretical constructs are important in creating a solid foundation for this study.
Conclusion
The results of this study emphasize the importance of practice guidance, technical skills, non-technical skills and innovative methods when tailoring a newborn resuscitation course for midwifery students. Although these skills cannot be learned without a context to facilitate these skills, a supportive culture is essential in performing newborn resuscitation—both for midwifery students and midwives. This learning is a lifelong process, starting when one is a midwifery student and continuing onwards, throughout one’s professional career as a midwife.
Although this paper focuses on how to prepare midwifery students for newborn resuscitation, we were surprised to find that midwifery students and experienced midwives alike expressed the same need to learn, train and prepare themselves for newborn resuscitation. The importance of facilitating lifelong learning in newborn resuscitation with low-dose, high-frequent training in a safe culture matters equally to both midwifery students and expert midwives.
Acknowledgments
We would like to thank each of the midwifery students and midwives who helped develop the tailored newborn resuscitation course for midwifery students.
Disclosure
The authors declare no conflict of interests.
References
1. American Academy of Pediatrics and American Heart Association. Textbook of Neonatal Resuscitation (NRP).
2. Ljungblad SK, Dahl B, Dahl B, Dahl B. Balancing life and death during the golden minute - midwives’ experiences of performing newborn resuscitation. J Multidiscip Healthc. 2020;13:943–952. doi:10.2147/jmdh.S268959
3. Wyllie J, Bruinenberg J, Roehr CC, Rudiger M, Trevisanuto D, Urlesberger B. European resuscitation council guidelines for resuscitation 2015: section 7. Resuscitation and support of transition of babies at birth. Resuscitation. 2015;95:249–263. doi:10.1016/j.resuscitation.2015.07.029
4. Williams J, Ebert L, Duff J. Neonatal resuscitation training for midwives in Australia: a discussion of current practice. Women Birth. 2020;33:e505–e510. doi:10.1016/j.wombi.2020.01.002
5. Ljungblad SK, McCormack B, Dahl B, Dahl B. An exploration of midwives’ perceptions of newborn resuscitation programmes for midwifery students. Midwifery. 2021;100:103021. doi:10.1016/j.midw.2021.103021
6. Sawyer T, Umoren RA, Gray MM. Neonatal resuscitation: advances in training and practice. Adv Med Educ Pract. 2017;8:11–19. doi:10.2147/amep.S109099
7. Halamek LP, Kaegi DM, Gaba DM, et al. Time for a new paradigm in pediatric medical education: teaching neonatal resuscitation in a simulated delivery room environment. Pediatrics. 2000;106(4):E45. doi:10.1542/peds.106.4.e45
8. Halamek LP. Simulation and debriefing in neonatology 2016: mission incomplete. Semin Perinatol. 2016;40(7):489–493. doi:10.1053/j.semperi.2016.08.010
9. Ljungblad LW, Sandvik SO, Lyberg A. The impact of skilled birth attendants trained on newborn resuscitation in Tanzania: a literature review. Int J Afri Nurs Sci. 2019;11:100168. doi:10.1016/j.ijans.2019.100168
10. Kassab M, Alnuaimi K, Mohammad K, Creedy D, Hamadneh S. Midwives’ experiences, education, and support needs regarding basic newborn resuscitation in Jordan. Clin Nurs Res. 2016;25(3):291–309. doi:10.1177/1054773815619388
11. Mileder LP, Urlesberger B, Szyld EG, Roehr CC, Schmolzer GM. Simulation-based neonatal and infant resuscitation teaching: a systematic review of randomized controlled trials. Klin Padiatr. 2014;226(5):259–267. doi:10.1055/s-0034-1372621
12. Khriesat W, Kassab M, Hamadneh S, Mohammad K, Hamadneh J, Khader YS. Infant resuscitation practices of midwives in a developing country. Adv Neonatal Care. 2017;17(5):400–406. doi:10.1097/anc.0000000000000418
13. Foglia EE, Te Pas AB. Effective ventilation: the most critical intervention for successful delivery room resuscitation. Semin Fetal Neonatal Med. 2018;23(5):340–346. doi:10.1016/j.siny.2018.04.001
14. Perlman JM, Wyllie J, Kattwinkel J, et al. Part 7: neonatal resuscitation: 2015 international consensus on cardiopulmonary resuscitation and emergency cardiovascular care science with treatment recommendations. Circulation. 2015;132(16_suppl_1Suppl 1):S204–S241. doi:10.1161/CIR.0000000000000276
15. Perlman JM, Risser R. Cardiopulmonary resuscitation in the delivery room: associated clinical events. Arch Pediatr Adolesc Med. 1995;149(1):20–25. doi:10.1001/archpedi.1995.02170130022005
16. De Bernardo G, Sordino D, Cavallin F, et al. Performances of low level hospital health caregivers after a neonatal resuscitation course. Ital J Pediatr. 2016;42(1):100. doi:10.1186/s13052-016-0313-0
17. Apgar V. A proposal for a new method of evaluation of the newborn infant. Curr Res Anesth Analg. 1953;32:260–267. doi:10.1213/00000539-195301000-00041
18. McCormack B, McCance T. Person-centred nursing: theory, models and methods. 2010:194.
19. Bull A, Sweet L. Midwifery students receiving the newborn at birth: a pilot study of the impact of structured training in neonatal resuscitation. Nurse Educ Pract. 2015;15:387–392. doi:10.1016/j.nepr.2015.03.002
20. Carolan-Olah M, Kruger G, Brown V, Lawton F, Mazzarino M. Development and evaluation of a simulation exercise to prepare midwifery students for neonatal resuscitation. Nurse Educ Today. 2016;36:375–380. doi:10.1016/j.nedt.2015.09.009
21. Carolan-Olah M, Kruger G, Brown V, Lawton F, Mazzarino M, Vasilevski V. Communicating out loud: midwifery students’ experiences of a simulation exercise for neonatal resuscitation. Nurse Educ Pract. 2018;29:8–14. doi:10.1016/j.nepr.2017.10.027
22. Forster EM, Donovan H. Enhancing bereavement support skills using simulated neonatal resuscitation. Int J Palliat Nurs. 2016;22(10):500–507. doi:10.12968/ijpn.2016.22.10.500
23. Lake S, McInnes RJ. Exploring cognitive skill development in midwifery education. Nurse Educ Pract. 2012;12(5):264–268. doi:10.1016/j.nepr.2012.04.015
24. Alhassan A, Fuseini AG, Osman W, Basour Adam A. Knowledge and experience of neonatal resuscitation among midwives in tamale. Nurs Res Pract. 2019;2019:3652608. doi:10.1155/2019/3652608
25. Kitson A, Harvey G, McCormack B. Enabling the implementation of evidence based practice: a conceptual framework. Qual Health Care. 1998;7(3):149–158. doi:10.1136/qshc.7.3.149
26. Rycroft-Malone J, Kitson A, Harvey G, et al. Ingredients for change: revisiting a conceptual framework. Qual Saf Health Care. 2002;11(2):174–180. doi:10.1136/qhc.11.2.174
27. McCormack B, Kitson A, Harvey G, Rycroft‐Malone J, Titchen A, Seers K. Getting evidence into practice: the meaning of `context. J Adv Nurs. 2002;38(1):94–104. doi:10.1046/j.1365-2648.2002.02150.x
28. Rycroft-Malone J. The PARIHS framework—a framework for guiding the implementation of evidence-based practice. J Nurs Care Qual. 2004;19(4):297. doi:10.1097/00001786-200410000-00002
29. Thomas H. Call the Midwife: Series Eight; Christmas Special. BBC production; 2019.
30. Skaug T. Jordmordiktet. [The Midwifery Poem]. Available from: https://www.facebook.com/watch?v=175042373730213. Accessed May 5, 2020. Norwegian.
31. General Assembly of the World Medical Association. Declaration of Helsinki ethical principles for medical research involving human subjects. Am Coll Dent. 2014;81(3):14–18.
32. Gale NK, Heath G, Cameron E, Rashid S, Redwood S, Gale NK. Using the framework method for the analysis of qualitative data in multi-disciplinary health research. BMC Med Res Methodol. 2013;13(1):117. doi:10.1186/1471-2288-13-117
33. Ritchie J, Lewis J. Qualitative Research Practice: A Guide for Social Science Students and Researchers. Sage Publications; 2003.
34. Knowles MS, Holton E, Swanson RA. The Adult Learner: The Definitive Classic in Adult Education and Human Resource Development.
35. Enweronu-Laryea C, Dickson KE, Moxon SG, et al. Basic newborn care and neonatal resuscitation: a multi-country analysis of health system bottlenecks and potential solutions. BMC Pregnancy Childbirth. 2015;15(Suppl 2):S4. doi:10.1186/1471-2393-15-s2-s4
36. McKenna L, Bogossian F, Hall H, Brady S, Fox-Young S, Cooper S. Is simulation a substitute for real life clinical experience in midwifery? A qualitative examination of perceptions of educational leaders. Nurse Educ Today. 2011;31(7):682–686. doi:10.1016/j.nedt.2011.02.014
37. Williams J, Jones D, Walker R. Consideration of using virtual reality for teaching neonatal resuscitation to midwifery students. Nurse Educ Pract. 2018;31:126–129. doi:10.1016/j.nepr.2018.05.016
38. Marshall S, Lang AM, Perez M, Saugstad OD. Delivery room handling of the newborn. J Perinatal Med. 2019;48:1. doi:10.1515/jpm-2019-0304
39. Wrammert J, Sapkota S, Baral K, Kc A, Malqvist M, Larsson M. Teamwork among midwives during neonatal resuscitation at a maternity hospital in Nepal. Women Birth. 2017;30(3):262–269. doi:10.1016/j.wombi.2017.02.002
40. Creswell JW, Poth CN. Qualitative inquiry & research design: choosing among five approaches. In: Qualitative Inquiry and Research Design.
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.