Back to Journals » Nature and Science of Sleep » Volume 17

J-Shaped Association Between Sleep Timing and Suicidal Ideation: A Nationwide Cross-Sectional Study
Received 4 October 2025
Accepted for publication 4 December 2025
Published 19 December 2025 Volume 2025:17 Pages 3155—3165
DOI https://doi.org/10.2147/NSS.S572068
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Marco Veneruso
Jiyu Kang,1 Eurah Goh2
1Department of Medicine, School of Medicine, Kangwon National University, Chuncheon, Kangwon, Republic of Korea; 2Department of Family Medicine, School of Medicine, Kangwon National University, Chuncheon, Kangwon, Republic of Korea
Correspondence: Eurah Goh, Department of Family Medicine, School of Medicine, Kangwon National University, 1 Kangwondeahak-Gil, Chuncheon, Kangwon, 24341, Republic of Korea, Tel +82-10-2321-7097, Fax +82-33-258-2165, Email [email protected]
Purpose: Adolescent suicide has emerged as a global public health concern. Among various risk factors for suicide, sleep—particularly sleep timing—is valuable for its modifiability. However, the relationship between sleep timing and suicidality remains unclear. This study aimed to explore the association between sleep timing and suicidal ideation among Korean adolescents.
Patients and Methods: This cross-sectional study analyzed data from 759,350 adolescents who participated in the Korea Youth Risk Behavior Web-based Survey from 2007 to 2019. Self-reported weekday sleep timing (categorized by “go-to-bed” times from 8 PM to 3 AM) and suicidal ideation were analyzed. Hierarchical multivariable logistic regression was performed to evaluate the association between sleep timing and suicidal ideation, adjusting for potential confounders, including sleep duration, sleep quality, and depressive mood.
Results: Of the 759,350 adolescents, 17.4% reported suicidal ideation. Using 11 PM as the reference, both the early sleep timing (8 PM: OR = 1.54, 95% CI = 1.29– 1.84) and late sleep timing (3 AM: OR = 2.17, 95% CI = 2.09– 2.26) were associated with higher odds of suicidal ideation, demonstrating a J-shaped relationship. This independent association remained after adjusting for sociodemographic factors, sleep duration, sleep quality, and depressive mood. The J-shaped pattern appeared consistently across sex and school level. Age-stratified analyses also showed a consistent J-shaped pattern across all ages, with the nadir shifting slightly later with age (from 10 PM in younger adolescents to midnight in older adolescents).
Conclusion: A J-shaped association between sleep timing and suicidal ideation was observed after controlling for sleep duration, sleep quality, and depressive mood. These findings indicate that sleep timing may serve as a candidate behavioral marker associated with suicidal ideation. Further longitudinal and intervention studies are warranted to confirm temporality and clarify underlying mechanisms.
Keywords: sleep onset time, bedtime, circadian rhythm, suicide, adolescent
Introduction
According to the World Health Organization’s 2020 report, suicide is one of the leading causes of death among adolescents worldwide, making it a major public health concern requiring urgent attention.1,2 In South Korea, suicide has been the primary cause of death among adolescents for over a decade.3,4 Furthermore, the adolescent suicide rate (9.9 per 100,000) significantly exceeds the global average (6.0 per 100,000).4,5 Risk factors for adolescent suicide include sociodemographic factors (such as age, sex, and socioeconomic status),6 biological factors (such as genetic predisposition7 and hormonal dysregulation),8 and health-related behavioral factors (such as smoking,9 alcohol consumption,9 physical inactivity, and sleep behavior).10 Among these factors, sleep has recently gained attention due to its modifiable nature.11
Sleep is known to play a fundamental role in maintaining and optimizing both physical and mental health.11 In adolescents, this role becomes even more critical for mental health, given their intense period of brain development.12 Numerous studies have shown that sleep problems in adolescents—including issues with sleep duration, sleep timing, sleep quality, and sleep disturbances—are related to poor academic performance,12 depression,13 and even suicidal behavior.13 Previous studies on sleep problems and suicidality have primarily focused on sleep duration, finding that both short and long total sleep times may be linked to suicidal ideation and attempts in adolescents.11,13 However, not only sleep duration (“how long”) but also sleep timing (“when”) may be critical for adolescents’ mental health.13,14 Adolescents experience distinct circadian shifts,15,16 which, when combined with early, fixed school start times, often lead to biological dysynchronization.17,18 Such circadian misalignment is associated with impaired cognitive function19 and poorer psychological well-being,11,13,19 including an increased risk of depressive symptoms and suicidal ideation,11,13 independent of sleep duration.
However, research on sleep timing and suicidality is relatively rare.13,19 In particular, there has been a notable lack of studies specifically examining the independent association between sleep timing and adolescent suicidal ideation.13,19 Therefore, this study aimed to address this gap by examining whether sleep timing is independently associated with suicidal ideation among Korean adolescents after adjusting for sociodemographic variables, sleep duration, sleep quality, and depressive mood. Given the limited evidence, we treated the analysis as exploratory and allowed for non-linearity. Using nationally representative survey data, we performed a cross-sectional analysis with weighted multivariable logistic regression models. Furthermore, subgroup analyses were conducted to determine whether the optimal sleep timing associated with the lowest suicidal ideation differed by sex, school level, or age.
Materials and Methods
Study Design and Participants
This study was conducted using data from the 2007–2019 Korea Youth Risk Behavior Web-based Survey (KYRBS), administered by the Korea Centers for Disease Control and Prevention (KCDC). The KYRBS is a nationwide cross-sectional representative survey using a complex sample design, including multistage sampling, stratification, and clustering. The survey aims to assess the health-related risk behaviors among middle and high school students (grades 7–12) and includes more than 100 questions across 15 domains, covering sociodemographic characteristics, health-related risk behaviors, and mental and physical health. The survey questionnaire was developed through expert consultations and pilot testing before implementation, and its validity and reliability have been established as part of the national health statistics quality assurance process. As a large-scale surveillance survey, the KYRBS does not include detailed psychosocial or developmental variables, and residual confounding may remain.
Of the 941,607 students targeted in the 2009–2017 Korea Youth Risk Behavior Web-based Survey (KYRBS), 905,755 completed the survey (response rate, 96.2%). We excluded 2687 participants who reported serious physical illnesses (such as cancer, diabetes, or cardiac disease) or a history of drug abuse. Participants with missing responses to sleep-related items (n = 136,301) or implausible sleep data were further excluded. Implausible cases included those reporting weekday bedtimes before 7 PM or after 4 AM, or those whose calculated sleep duration yielded negative values (n = 7417). The final analytic sample included 759,350 adolescents.
Study Variables
Sleep timing was defined as the usual “go-to-bed” time and was assessed using the question: “What time did you usually go-to-bed during the last weekdays (hh:mm)?” Responses were categorized into hourly intervals: 8 PM (20:00–20:59), 9 PM, 10 PM, 11 PM, 12 AM, 1 AM, 2 AM, and 3 AM. Wake times before 4 AM or after 9 AM and sleep timings between 4 AM and 8 PM were treated as missing; if either value was implausible, both were set to missing. Cases with negative sleep duration were excluded. Analyses used complete cases. Sleep duration was defined as the total time spent sleeping and was calculated using the reported “go-to-bed” and “wake-up” times based on response to this question: “What time did you usually wake up on weekdays over the past week?” The responses were categorized as 4 AM, 5 AM, 6 AM, 7 AM, and 8 AM. Sleep quality was assessed by asking the question: “Do you think your sleep over the past 7 days was sufficient to feel refreshed?” The response options ranged from “1 = sufficient” to “5 = not sufficient at all”. Suicidal ideation (main dependent variable) was assessed by asking the question: “Have you ever considered suicide during the past 12 months?” The responses were either “yes” or “no”.
Sociodemographic variables included sex, age, region (rural, small city, metro city), perceived socioeconomic status (1=very high, 5=very low), and self-estimated academic performance (low, middle, high). Health-related behaviors, including smoking, alcohol consumption, and physical activity, were assessed using the following questions: “Have you ever smoked more than one cigarette?”, “Have you ever consumed more than one glass of alcohol?” and “How many times did you engage in vigorous physical activity during the last 7 days?” respectively. The responses for physical activity ranged from “0 = none” to “5 = over 5 days”. Depressive mood was assessed using a dichotomous (yes/no) response to the question: “During the past 12 months, have you experienced feelings of sadness or hopelessness severe enough to stop performing your usual activities for at least two full weeks?”
Statistical Analysis
Statistical analyses were performed accounting for the complex survey design of the KYRBS, incorporating the provided stratification, clustering, and weighting variables in all procedures. Associations between categorical variables and suicidal ideation were assessed using χ2 tests. Differences in continuous variables across categorical groups were analyzed using independent samples t-tests and one-way analysis of variance. To investigate the independent association of sleep timing with suicidal ideation, a series of hierarchical logistic regression models were constructed by sequentially adding covariates: Model I examined the unadjusted association between sleep timing and suicidal ideation; Model II was adjusted for sociodemographic and health-related behavioral factors; Model III was additionally adjusted for sleep duration; Model IV was additionally adjusted for sleep quality; and Model V was additionally adjusted for depressive mood. Because no established reference sleep timing has been reported in previous literature, we initially analyzed sleep timing without assuming a specific functional form. A J-shaped pattern emerged, and a supplementary piecewise logistic regression (hinge at 11 PM) confirmed a significant slope change (P < 0.05), supporting 11 PM as the inflection point for increased risk. Sensitivity analyses using alternative reference points (10 PM and 12 AM) yielded consistent results, confirming the robustness of the association. Subgroup analyses by sex and school type (middle/high school), as well as analyses stratified by age, were also conducted. Subgroup analyses were exploratory and may increase the risk of type I error due to multiple comparisons. All statistical tests were two-sided, and the level of statistical significance was set at a P-value < 0.05. All statistical analyses were conducted using StataNow 19 SE (StataCorp LLC, College Station, TX).
Ethical Consideration
The KYRBS is a nationally approved survey (approval number 117058) conducted under the ethical oversight of the KDCA Institutional Review Board (IRB). All data were collected anonymously after obtaining informed consent from participants. The present secondary analysis was reviewed by the Kangwon National University IRB and was determined to be exempt from further ethical review in accordance with the Bioethics and Safety Act of Korea (Article 2 and Article 15), which allows exemption for studies using de-identified secondary data.
Results
General Characteristics with and without Suicidal Ideation
Supplementary Table S1 presents the basic characteristics of the participants with and without suicidal ideation. Among the total 759,350 participants, 17.4% (n = 121,062) experienced suicidal ideation. Suicidal ideation was significantly higher among girls, middle school students, residents of metro cities, students with lower socioeconomic status and academic achievement, those who had smoked or consumed alcohol, individuals who did not exercise, and those experiencing depressive mood. Regarding sleep patterns, suicidal ideation was higher among individuals with late or early sleep timing, early wake timing, short sleep duration, and poor sleep quality compared with others.
Sleep Patterns and Sociodemographic Characteristics
Table 1 presents sleep patterns based on sociodemographic factors. The average sleep timing was 12:31 AM, the average wake timing was 6:51 AM, and the average sleep duration was 6 h and 18 min. Girls went to bed later, woke up earlier, and slept less than boys. High school students had a much later bedtime (12:58 AM) than middle school students (12:01 AM), woke up earlier, and had a shorter sleep duration. Residency, socioeconomic status, academic performance, physical activity, smoking, alcohol consumption, and depressive mood were all significantly associated with sleep patterns.
 |
Table 1 Sleep Patterns According to the Sociodemographic Factors |
Association Between Sleep Timing and Suicidal Ideation
Table 2 shows that sleep timing consistently demonstrated an independent association with adolescent suicidal ideation across all models. In Model I (unadjusted), adolescents who went to bed at 8 PM had 1.70 times higher odds of suicidal ideation (95% confidence interval (CI), 1.43–2.02) compared with those sleeping at 11 PM, escalating to 2.08 times higher odds for those with a 3 AM sleep timing (95% CI, 2.00–2.16). After adjusting for sociodemographic and behavioral variables (Model II), the odds of suicidal ideation remained elevated at both extremes of sleep timing: odds ratio (OR) = 1.54 (95% CI, 1.29–1.84) for 8 PM and OR = 2.17 (95% CI, 2.09–2.26) for 3 AM, compared to 11 PM. After adjusting for sleep duration (Model III), the independent association between sleep timing and suicidal ideation persisted, with the lowest OR observed around 11 PM. This independent association remained even after controlling for sleep quality (Model IV) and depressive mood (Model V).
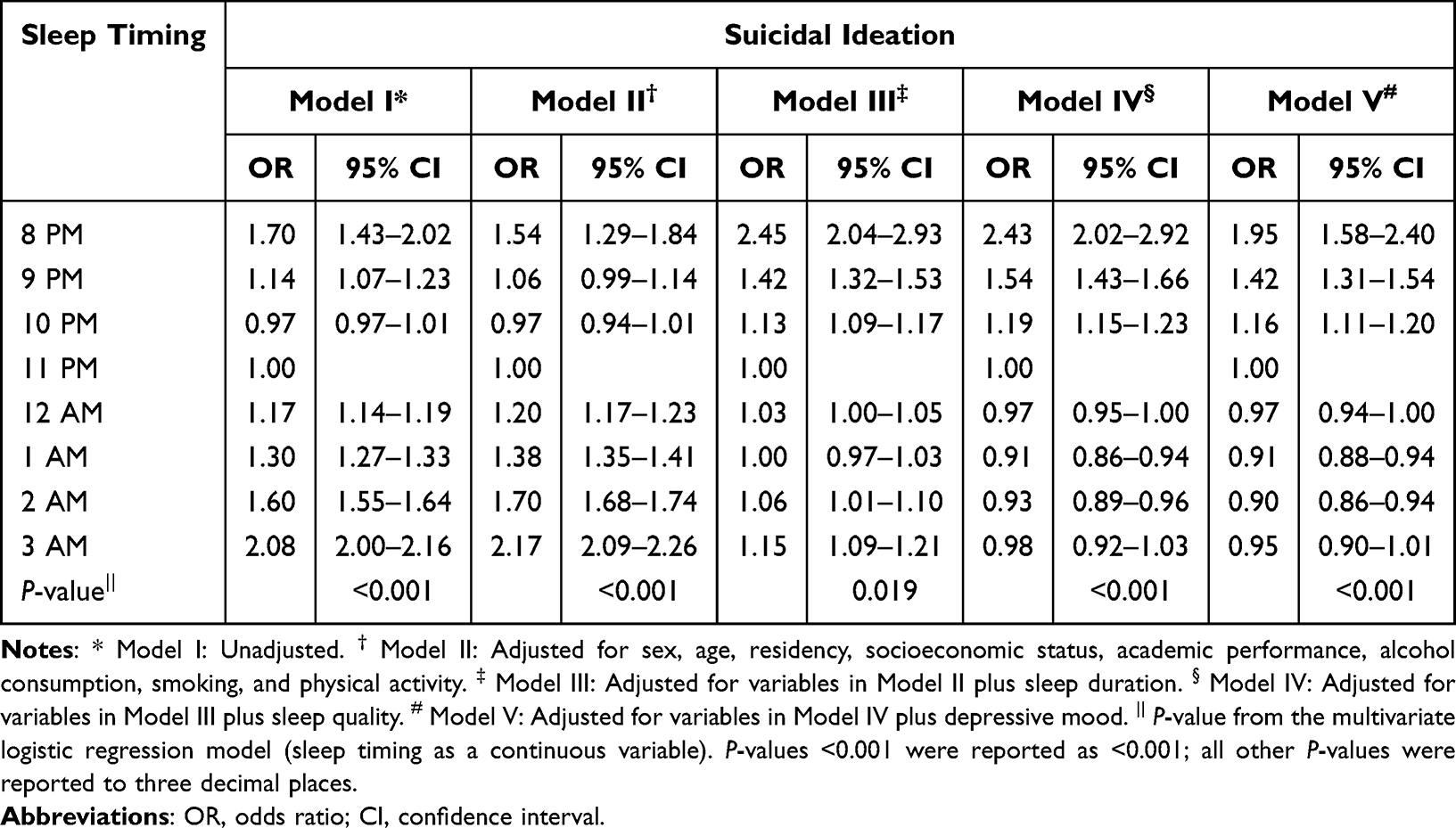 |
Table 2 Association Between Sleep Timing and Suicidal Ideation in the Hierarchical Logistic Regression Models |
Subgroup Analysis by Sex and School Level
Figures 1 and 2 present the association between sleep timing and suicidal ideation based on Model II, stratified by sex (boys vs girls) and school level (middle school vs high school). Following stratification by sex (Figure 1), a distinct J-shaped association between sleep timing and suicidal ideation was observed, with 10 PM as the common nadir for both boys (Figure 1B) and girls (Figure 1A). Sex differences in suicidal ideation risk related to sleep timing were subtle.
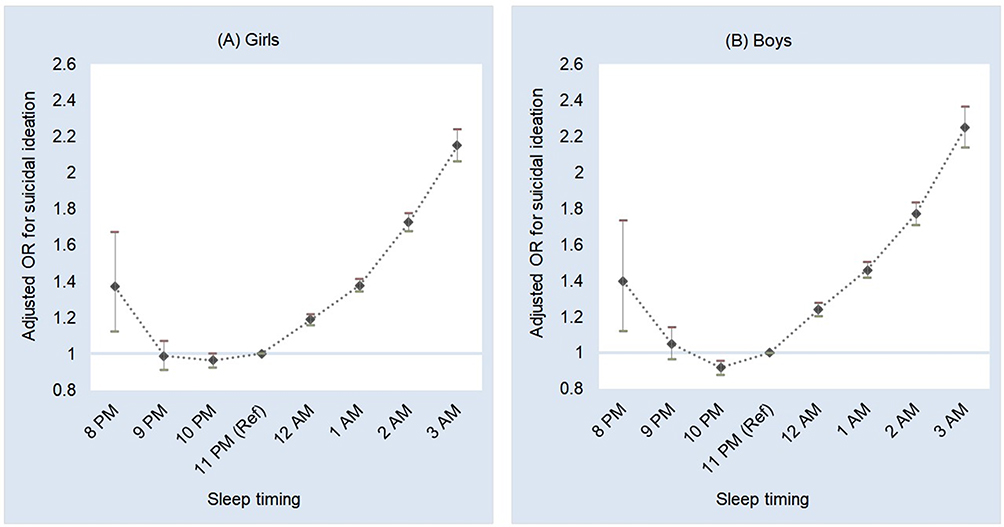 |
Figure 1 Adjusted ORs for suicidal ideation according to sleep timing by sex. Abbreviations: Ref, reference sleep timing; OR, odds ratio; CI, confidence interval. Notes: Both girls (A) and boys (B) showed a J-shaped pattern, with the lowest odds of suicidal ideation around 10 PM and a marked increase at later sleep timing, particularly after 1 AM. ORs and 95% CIs were adjusted for age, residency, socioeconomic status, academic performance, alcohol consumption, smoking, and physical activity. Reference sleep timing= 11 PM. |
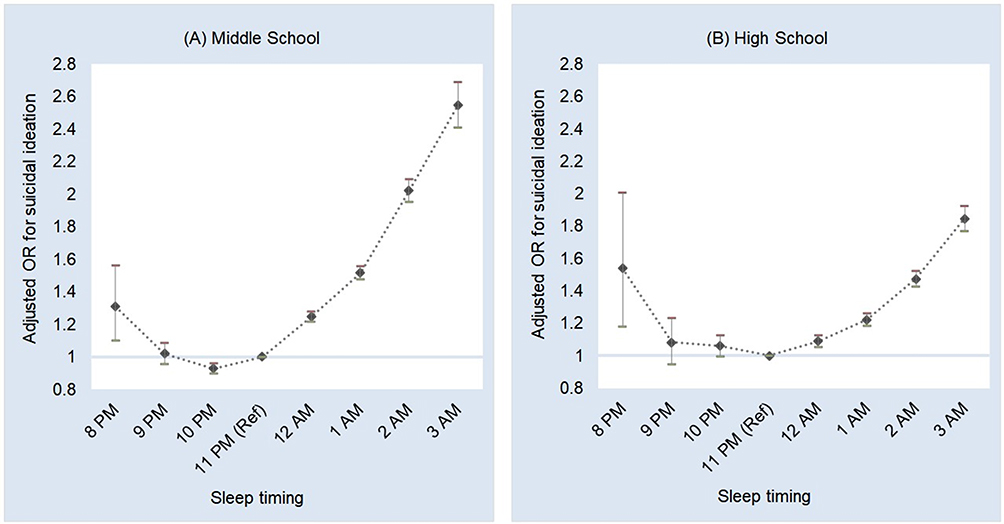 |
Figure 2 Adjusted ORs for suicidal ideation according to sleep timing, by school level. Abbreviations: Ref, reference sleep timing; OR, odds ratio; CI, confidence interval. Notes: Both middle (A) and high (B) school students showed a J-shaped relationship between sleep timing and suicidal ideation. The lowest odds were observed at 10 PM among middle school students and at 11 PM among high school students, with higher odds at both earlier and later sleep timing. ORs and 95% CIs were adjusted for sex, age, residency, socioeconomic status, academic performance, alcohol consumption, smoking, and physical activity. Reference sleep timing = 11 PM. |
When stratified by school level (Figure 2), this J-shaped pattern in suicidal ideation risk according to sleep timing was consistent, although with a different nadir: 10 PM for middle school students (Figure 2A) and 11 PM for high school students (Figure 2B). The risk associated with late sleep timing was more pronounced among middle school students: at 3 AM, the OR was 2.54 (95% CI, 2.41–2.69) among middle schoolers, compared with 1.85 (95% CI, 1.77–1.93) among high schoolers.
Age-Stratified Analysis
Table 3 presents the age-stratified results by 1-year intervals according to Model II. While the J-shaped pattern generally persisted across all age groups, both the nadir of suicidal ideation and the magnitude of the association varied with age. The age-specific nadir of suicidal ideation shifted progressively later, occurring at 10 PM for 12- to 13-year-olds, 11 PM for 14- to 17-year-olds, and 12 AM for 18-year-olds. The OR for suicidal ideation associated with later sleep times increased more markedly in younger adolescents. For example, a 3 AM bedtime was associated with an OR of 4.15 (95% CI, 3.34–5.16) at age 12, compared to 1.60 (95% CI, 1.44–1.77) at age 18.
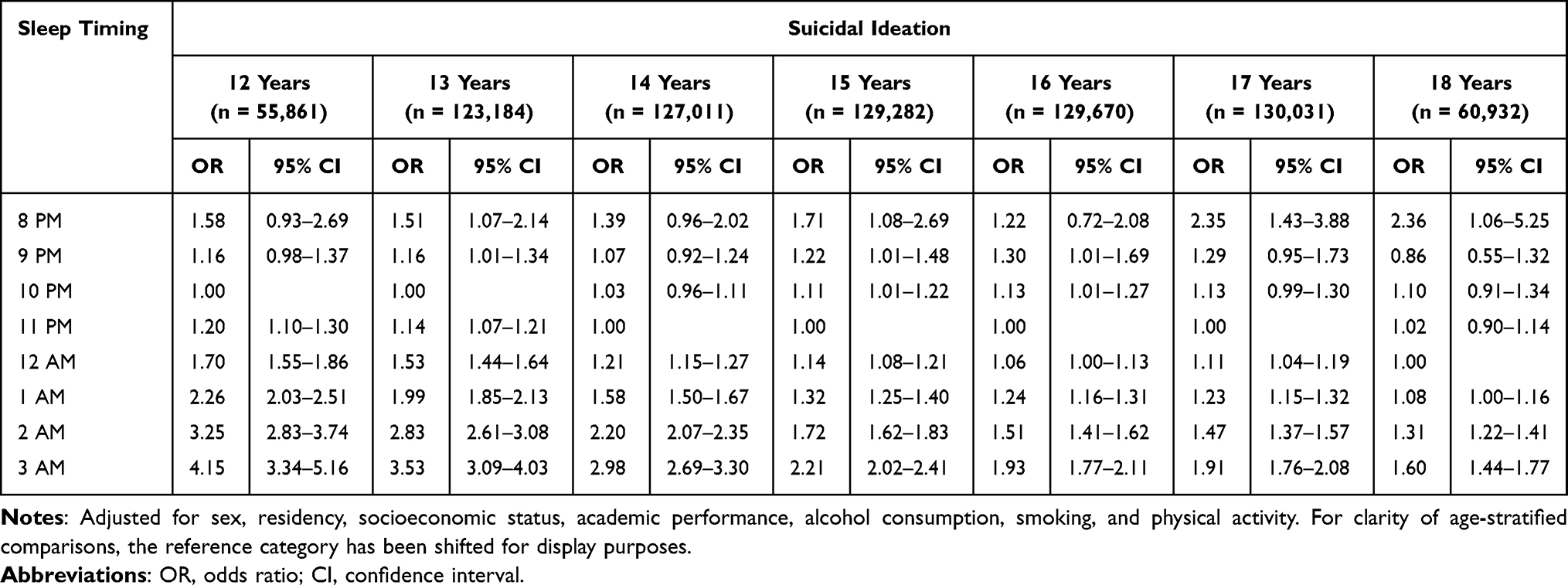 |
Table 3 Age-Stratified Multivariable Logistic Regression of the Association Between Sleep Timing and Suicidal Ideation |
Discussion
This study aimed to examine the association between sleep timing and suicidal ideation among Korean adolescents using a nationally representative sample. Sleep timing was independently associated with suicidal ideation after adjusting for sociodemographic characteristics and health-related behavioral factors. Notably, the independent association between sleep timing and suicidal ideation remained significant even after adjusting for sleep duration, sleep quality, and depressive mood.
Sleep Timing: An Independent Association with Suicidal Ideation
Previous research on sleep has predominantly focused on the relationship between adolescent suicidal ideation and various sleep characteristics—including sleep duration, sleep quality, and disturbances such as insomnia.20,21 However, whether sleep timing is independently associated with suicidal ideation remains a matter of debate.13,19 Due to their fixed early school start times, later sleep timing in adolescents is inevitably associated with shorter sleep duration, whereas earlier sleep timing is associated with longer sleep duration.15,19 Given the inverse correlation between sleep timing and sleep duration, it remains unclear whether the observed effects of sleep timing on mental health are independent or largely mediated by sleep duration.22 Accordingly, Model III, which was adjusted for sleep duration, confirmed that sleep duration was independently associated with suicidal ideation. This suggests that not only sleep duration but also sleep timing may serve as a candidate marker associated with suicidal ideation in adolescents. Similarly, Model IV, which was adjusted for sleep quality, also demonstrated a significant association. Contrary to the traditional hypothesis that inappropriate sleep timing influences suicidal ideation via its effect on sleep quality,20 this result suggests that sleep timing is independently associated with suicidal ideation in adolescents, irrespective of sleep quality.
Traditionally, depressive mood has been considered a mediating factor in suicidal ideation.13 However, in Model V, the association between suicidal ideation and sleep timing remained significant after adjusting for depressive mood, which implies the existence of a hidden pathway between sleep timing and suicidal ideation not mediated by depressive mood.
J-Shaped Relationship Between Sleep Timing and Suicidal Ideation
A key finding of this study was that both excessively early and late bedtimes were associated with increased suicidal ideation among adolescents, revealing a J-shaped association. A similar J-shaped relationship between sleep duration and suicidal ideation has been widely observed, with both short and long sleep durations increasing the risk of suicidal ideation.23–26 Based on this, the National Sleep Foundation recommends 8–10 h of sleep for adolescents.24 However, regarding sleep timing, only late sleep timing has traditionally been considered a risk factor for mental health disorders. Previous studies reported that late sleep timing may be related to adolescent health issues, including depression, anxiety, obesity, poorer academic performance,19 and suicidal ideation.14,25 Research on early sleep timing is scarce, with only a few studies suggesting a possible relationship to behavioral withdrawal or social isolation.19 Based on the hour-by-hour analysis of sleep timing, which was enabled by the large dataset, we found that both early and late sleep timing are associated with increased suicidal ideation across all sexes, school types, and ages.
Plausible Mechanisms Underlying the J-Shaped Association
Late Sleep Timing and Suicidal Ideation
Possible mechanisms that may explain how late bedtime is related to suicidal ideation include: (1) circadian rhythm disruption,17,18 and (2) hypofrontality.27–29
First, adolescence is characterized by a unique circadian rhythm that differs from those of childhood and adulthood.18 Research shows that adolescents have a biological tendency for their sleep-wake cycles to shift later, accompanied by delayed melatonin secretion, reflecting age-related structural changes in circadian rhythms.18 This circadian disruption is further exacerbated in adolescents by social jet lag, often due to academic demands forcing early wake times.17
Second, delayed sleep timing increases the likelihood of wakefulness during the circadian night, leading to frontal lobe hypoactivation (hypofrontality), which in turn heightens vulnerability to suicidal ideation.27,28 This hypofrontality leads to impaired emotional regulation and impulse control, which may contribute to increased suicide risk.28 Adolescents, in particular, are more vulnerable to these effects as their frontal lobes are not yet fully mature.29
Early Sleep Timing and Suicidal Ideation
Possible mechanisms that may explain how early sleep timing is associated with suicidal ideation include: (1) disruption of the circadian rhythm,15,16,18 (2) negative impact on rapid eye movement (REM) sleep,18,30,31 and (3) social isolation and psychological distress.32–34
First, adolescents who go to bed excessively early—before their circadian rhythm is ready for sleep—may experience increased sleep latency and frequent nocturnal awakenings.18 Based on previous research, this may reduce sleep efficiency, causing fatigue, daytime sleepiness, and depressed mood.15,16
Second, early sleep timing that is asynchronous with the biological clock may negatively affect the pattern and structure of REM sleep, which is known to play a vital role in emotional processing.18,30 Previous research suggests that abnormal REM sleep patterns could cause emotional dysregulation, thereby heightening vulnerability to stress and increasing the risk of suicidal ideation.31
Third, although depressive mood was accounted for in our models, residual confounding cannot be excluded. Some adolescents with unrecognized subclinical depression or social withdrawal may exhibit early bedtimes, which could partially explain the observed association between early sleep timing and suicidal ideation.32–34
Age-Specific Optimal Sleep Timing
Age-stratified analysis revealed a consistent J-shaped association across all age groups, though the optimal sleep timing associated with the lowest suicidal ideation differed by age. In younger adolescents (12–13 years), sleeping at 10 PM was associated with the lowest suicidal ideation, whereas in older adolescents (14–17 years), sleeping at 11 PM was associated with the lowest suicidal ideation. These age-related differences likely result from complex interactions among factors, including circadian rhythm shifts,35,36 as well as societal influences such as academic demands,37 peer relationships,38 and smartphone use.39 Particularly, younger adolescents who sleep late exhibited a twofold higher OR (4.15) for suicidal ideation associated with later sleep timing compared to older adolescents. This highlights the need for careful monitoring of sleep timing in younger adolescents, who experience rapid shifts in biological rhythms and habit formation.15,16,40 These findings highlight the necessity of age-specific and practical sleep timing guidelines, rather than relying solely on the conventional advice to “go to bed early”.
Strengths and Limitations
This study has several key strengths. First, using a national representative dataset, the study revealed that sleep timing is independently associated with suicidal ideation among adolescents, regardless of sleep duration, sleep quality, or depressive mood. Second, this is the first study to demonstrate a J-shaped relationship between sleep timing and suicidal ideation. Third, through an hour-by-hour analysis, enabled by a large-scale dataset, we could explore which sleep onset times were most beneficial for mental health at each age.
However, this study has some limitations. First, the use of self-reported data may have introduced biases, such as recall and social desirability biases. Second, owing to its cross-sectional design, it is difficult to establish a causal relationship between sleep timing and suicidal ideation, underscoring the need for future longitudinal studies to confirm this relationship. Third, some important risk factors could not be included in this study, such as relationship risk factors (family or peer conflicts), individual developmental factors (including early childhood experiences), community factors, and broader societal influences that may interact with sleep timing and mental health. Also, cultural factors such as high academic pressure, late-night study habits, and social norms regarding sleep schedules among Korean adolescents may limit the generalizability of our findings to other populations. Future studies incorporating these multi-level contextual factors, ideally through longitudinal and intervention designs, are needed to clarify potential bidirectional pathways and establish temporal ordering.
Conclusion
This study revealed that sleep timing is independently associated with suicidal ideation among adolescents, regardless of sleep duration, sleep quality, or depressive mood. A significant J-shaped relationship was observed, indicating that both early and late sleep timings were associated with higher odds of suicidal ideation. These findings suggest that sleep timing may serve as a candidate behavioral marker associated with adolescent suicidal ideation and highlight the need to extend research attention from sleep duration (“how long”) to also considering sleep timing (“when”). Future longitudinal and intervention studies incorporating psychosocial and developmental risk factors are warranted to clarify causal directions and underlying mechanisms.
Abbreviations
CI, confidence interval; KCDC, Korea Centers for Disease Control and Prevention; KYRBS, Korea Youth Risk Behavior Web-based Survey; OR, odds ratio; REM, rapid eye movement.
Data Sharing Statement
This study analyzed publicly available datasets, which are accessible at https://www.kdca.go.kr/yhs/.
Ethics Approval and Informed Consent
This study used publicly available, de-identified secondary data from the Korea Youth Risk Behavior Survey (KYRBS), conducted annually by the Korea Disease Control and Prevention Agency. The KYRBS is an anonymous, self-administered online survey approved by the Institutional Review Board of the Korea Centers for Disease Control and Prevention (approval number 117058). All participants provided informed consent to participate in the KYRBS, and all data are anonymized prior to public release. According to the Bioethics and Safety Act of Korea (Article 2 and Article 15), research using secondary data that is fully anonymized and contains no identifiable personal information is exempt from IRB review. The present secondary analysis was reviewed by the Kangwon National University IRB and was determined to be exempt from full ethical review.
Acknowledgments
We acknowledge the Korea Disease Control and Prevention Agency for providing access to the Korea Youth Risk Behavior Survey dataset.
Author Contributions
Jiyu Kang contributed to formal analysis, data curation, investigation, validation, visualization, writing – original draft and writing – review & editing. Eurah Goh contributed to conceptualization, methodology, project administration, investigation, validation, visualization, writing – review & editing and supervision. They approved the final version for publication, agreed on the journal of submission, and took responsibility for the integrity and accuracy of the work.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.
Disclosure
The authors declare that they have no competing interests.
References
1. Bertuccio P, Amerio A, Grande E, et al. Global trends in youth suicide from 1990 to 2020: an analysis of data from the WHO mortality database. EClinicalMedicine. 2024;70:102506. doi:10.1016/j.eclinm.2024.102506
2. World Health Organization. Global status report on preventing violence against children 2020. 1st ed. Geneva: World Health Organization; 2020.
3. Kim J, Ko YH, Yoon HK, et al. Study on awareness of suicide and suicide prevention among community youth. J Korean Acad Child Adolesc Psychiatr. 2024;35(3):210–217. doi:10.5765/jkacap.240006
4. Lee Y. Suicide Trends and Responses in Korea. In: Korean Social Trends. Daejeon: Statistics Research Institute, Statistics Korea; 2025.
5. Child and youth mortality data ages 5-24. UNICEF DATA. Available from: https://data.unicef.org/resources/dataset/child-adolescent-and-youth-mortality-rates/.
6. Nock MK, Borges G, Bromet EJ, Cha CB, Kessler RC, Lee S. Suicide and suicidal behavior. Epidemiol Rev. 2008;30(1):133–154. doi:10.1093/epirev/mxn002
7. Colbert SMC, Lepow L, Fennessy B, et al. Distinguishing clinical and genetic risk factors for suicidal ideation and behavior in a diverse hospital population. Transl Psychiatry. 2025;15(1):63. doi:10.1038/s41398-025-03287-6
8. Ho TC, Gifuni AJ, Gotlib IH. Psychobiological risk factors for suicidal thoughts and behaviors in adolescence: a consideration of the role of puberty. Mol Psychiatry. 2022;27(1):606–623. doi:10.1038/s41380-021-01171-5
9. Li X, Chi G, Taylor A, et al. Lifestyle behaviors and suicide-related behaviors in adolescents: cross-sectional study using the 2019 YRBS data. Front Public Health. 2021;9:766972. doi:10.3389/fpubh.2021.766972
10. Pfledderer CD, Burns RD, Brusseau TA. School environment, physical activity, and sleep as predictors of suicidal ideation in adolescents: evidence from a national survey. J Adolesc. 2019;74(1):83–90. doi:10.1016/j.adolescence.2019.05.008
11. Harris LM, Huang X, Linthicum KP, Bryen CP, Ribeiro JD. Sleep disturbances as risk factors for suicidal thoughts and behaviours: a meta-analysis of longitudinal studies. Sci Rep. 2020;10(1):13888. doi:10.1038/s41598-020-70866-6
12. Sung D, Park B, Kim SY, et al. Structural alterations in large-scale brain networks and their relationship with sleep disturbances in the adolescent population. Sci Rep. 2020;10(1):3853. doi:10.1038/s41598-020-60692-1
13. Goldstein TR, Franzen PL. A comprehensive review of the literature on sleep difficulties and suicidality in youth to inform an integrative developmental model and future directions. Curr Sleep Med Rep. 2022;8(1):1–19. doi:10.1007/s40675-022-00222-9
14. Jeong W, Kim YK, Lee HJ, et al. Association of bedtime with both suicidal ideation and suicide planning among Korean adolescents. Int J Environ Res Public Health. 2019;16(20):3817. doi:10.3390/ijerph16203817
15. Gradisar M, Gardner G, Dohnt H. Recent worldwide sleep patterns and problems during adolescence: a review and meta-analysis of age, region, and sleep. Sleep Med. 2011;12(2):110–118. doi:10.1016/j.sleep.2010.11.008
16. Carpenter J, Robillard R, Hickie I. Variations in the sleep–wake cycle from childhood to adulthood: chronobiological perspectives. Chronophysiol Ther. 2015;5:37–49.
17. Carskadon MA. Sleep in adolescents: the perfect storm. Pediatr Clin North Am. 2011;58(3):637–647. doi:10.1016/j.pcl.2011.03.003
18. Crowley SJ, Wolfson AR, Tarokh L, Carskadon MA. An update on adolescent sleep: new evidence informing the perfect storm model. J Adolesc. 2018;67(1):55–65. doi:10.1016/j.adolescence.2018.06.001
19. Dutil C, Podinic I, Sadler CM, et al. Sleep timing and health indicators in children and adolescents: a systematic review. Health Promot Chronic Dis Prev Can. 2022;42(4):150–169. doi:10.24095/hpcdp.42.4.04
20. Goldstein TR, Franzen PL. Sleep difficulties and suicidality in youth: current research and future directions. Curr Opin Psychol. 2020;34:27–31. doi:10.1016/j.copsyc.2019.08.021
21. Lemke T, Hökby S, Carli V, Hadlaczky G. Sleep duration and quality in adolescents: associations with suicidal ideation. J Adolesc. 2025;97(4):1113–1120. doi:10.1002/jad.12473
22. Hasler BP. Chronotype and mental health: timing seems to matter, but how, why, and for whom? World Psychiatry. 2023;22(2):329–330. doi:10.1002/wps.21092
23. Paruthi S, Brooks LJ, D’Ambrosio C, et al. Consensus statement of the American academy of sleep medicine on the recommended amount of sleep for healthy children: methodology and discussion. J Clin Sleep Med. 2016;12(11):1549–1561. doi:10.5664/jcsm.6288
24. Hirshkowitz M, Whiton K, Albert SM, et al. National sleep foundation’s sleep time duration recommendations: methodology and results summary. Sleep Health. 2015;1(1):40–43. doi:10.1016/j.sleh.2014.12.010
25. Kim JH, Park EC, Lee SG, Yoo KB. Associations between time in bed and suicidal thoughts, plans, and attempts in Korean adolescents. BMJ Open. 2015;5(9):e008766. doi:10.1136/bmjopen-2015-008766
26. Guo L, Xu Y, Deng J, et al. Association between sleep duration, suicidal ideation, and suicidal attempts among Chinese adolescents: the moderating role of depressive symptoms. J Affect Disord. 2017;208:355–362. doi:10.1016/j.jad.2016.10.004
27. Perlis ML, Grandner MA, Chakravorty S, Bernert RA, Brown GK, Thase ME. Suicide and sleep: is it a bad thing to be awake when reason sleeps? Sleep Med Rev. 2016;29:101–107. doi:10.1016/j.smrv.2015.10.003
28. Perlis ML, Grandner MA, Brown GK, et al. Nocturnal wakefulness as a previously unrecognized risk factor for suicide. J Clin Psychiatry. 2016;77(06):e726–33. doi:10.4088/JCP.15m10131
29. Blakemore SJ, Burnett S, Dahl RE. The role of puberty in the developing adolescent brain. Hum Brain Mapp. 2010;31(6):926–933. doi:10.1002/hbm.21052
30. Campbell IG, Kraus AM, Burright CS, Feinberg I. Restricting time in bed in early adolescence reduces both NREM and REM sleep but does not increase slow wave EEG. Sleep. 2016;39(9):1663–1670. doi:10.5665/sleep.6088
31. Agargun MY, Cartwright R. REM sleep, dream variables and suicidality in depressed patients. Psychiatry Res. 2003;119(1–2):33–39. doi:10.1016/S0165-1781(03)00111-2
32. Katz SJ, Conway CC, Hammen CL, et al. Childhood social withdrawal, interpersonal impairment, and young adult depression: a mediational model. J Abnorm Child Psychol. 2011;39(8):1227–1238. doi:10.1007/s10802-011-9537-z
33. Luo M. Social isolation, loneliness, and depressive symptoms: a twelve-year population study of temporal dynamics. J Gerontol B Psychol Sci Soc Sci. 2023;78(2):280–290. doi:10.1093/geronb/gbac174
34. Bowker JC, Gurbacki JN, Richard CL, Rubin KH. Anxious-withdrawal and sleep problems during adolescence: the moderating role of peer difficulties. Behav Sci. 2023;13(9):740. doi:10.3390/bs13090740
35. Crowley SJ, Acebo C, Carskadon MA. Sleep, circadian rhythms, and delayed phase in adolescence. Sleep Med. 2007;8(6):602–612. doi:10.1016/j.sleep.2006.12.002
36. Futenma K, Takaesu Y, Komada Y, et al. Delayed sleep–wake phase disorder and its related sleep behaviors in the young generation. Front Psychiatry. 2023;14:1174719. doi:10.3389/fpsyt.2023.1174719
37. Okechukwu FO, Ogba KTU, Nwufo JI, et al. Academic stress and suicidal ideation: moderating roles of coping style and resilience. BMC Psychiatry. 2022;22(1):546. doi:10.1186/s12888-022-04063-2
38. Endo K, Ando S, Shimodera S, et al. Preference for solitude, social isolation, suicidal ideation, and self-harm in adolescents. J Adolesc Health. 2017;61(2):187–191. doi:10.1016/j.jadohealth.2017.02.018
39. Lemola S, Perkinson-Gloor N, Brand S, Dewald-Kaufmann JF, Grob A. Adolescents’ electronic media use at night, sleep disturbance, and depressive symptoms in the smartphone age. J Youth Adolesc. 2015;44(2):405–418. doi:10.1007/s10964-014-0176-x
40. Mantle D, Smits M, Boss M, et al. Efficacy and safety of supplemental melatonin for delayed sleep–wake phase disorder in children: an overview. Sleep Med. 2020;2:100022.
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.