")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 19
It Goes Beyond Anxiety: Experiences of Family Members and Caregivers of Epilepsy Care and Support
Authors Musekwa OP , Makhado L
Received 19 July 2023
Accepted for publication 4 October 2023
Published 7 December 2023 Volume 2023:19 Pages 2757—2764
DOI https://doi.org/10.2147/NDT.S430337
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Ofhani Prudance Musekwa,1 Lufuno Makhado2
1Department of Psychology, University of Venda, Thohoyandou, Limpopo, South Africa; 2Department of Public Health, University of Venda, Thohoyandou, Limpopo, South Africa
Correspondence: Ofhani Prudance Musekwa, Department of Psychology, University of Venda, Private Bag X5050, Thohoyandou, Limpopo, South Africa, Tel +27 015 962 8828, Email [email protected]
Purpose: To investigate the knowledge of epilepsy care and the support given by professionals to assist family members and caregivers in providing good care to People Living with Epilepsy (PLWE).
Patients and Methods: In this case study, fifteen participants participated. Of these, eleven were parents, and four were siblings. Twelve of the participants were primary caregivers, and three were secondary caregivers. Data were collected via in-person semi-structured interviews and analysed via thematic analysis.
Results: From the study, two themes emerged: Participant experiences regarding epilepsy practices and knowledge regarding epilepsy. From these two themes, four subthemes emerged: Epileptic seizure practice and treatment, as well as epilepsy knowledge and counselling and support.
Conclusion: This study revealed that although family members and caregivers are essential in patient care, they need more support and care from health providers. The much-needed care and support would assist in alleviating some pressures on epilepsy patient care and increase care standards and quality of life for families and PLWE.
Keywords: epilepsy care, epilepsy support, family members, caregivers, PLWE
Introduction
Family members play a vital role in healthcare, complementing the efforts of health professionals.1 The dynamic interaction among the patient, healthcare professional, family member, and caregiver can significantly impact the patient’s well-being. Family members and caregivers are crucial in patient healthcare decision-making, providing general care, supporting, and addressing the patient’s challenges.1 Therefore, it is imperative to comprehend their experiences, support them, and ensure they are adequately prepared to provide care. By understanding their unique perspectives and challenges, healthcare providers can offer tailored assistance, resources, and education to empower them in their caregiving roles. This collaborative approach enhances the overall quality of patient care while recognizing family members’ and caregivers’ essential contributions and needs.
Research indicates that family members and caregivers face many intricate challenges when caring for People Living with Epilepsy (PLWE). These challenges encompass various aspects, such as the unpredictable nature of seizures, the management of treatment regimens, the presence of stigma, the emotional toll of anxiety and depression, and the wide-ranging psychosocial impacts. Furthermore, primary caregivers often must grapple with the adjustment of dedicating substantial time and attention to patient care.2–6
Understanding and acknowledging these unique challenges is of utmost importance to develop effective programs and interventions that cater specifically to the needs of family members and caregivers. By recognizing the multifaceted nature of these difficulties, healthcare professionals and policymakers can work towards implementing targeted initiatives that address each aspect comprehensively. These efforts may include providing education and support on seizure management, offering strategies to cope with stigma and psychological well-being, and creating networks or support groups where caregivers can share experiences and gain emotional support.
Furthermore, ensuring that these programs and interventions are tailored to the individual needs and circumstances of family members and caregivers is crucial. This requires considering factors such as cultural beliefs, socioeconomic status, geographic location, and access to healthcare resources. By developing comprehensive and personalized approaches, healthcare providers can effectively support and empower family members and caregivers as they navigate the challenges of caring for PLWE. Ultimately, recognising and understanding these challenges will pave the way for more targeted and impactful interventions that improve the overall well-being of PLWE and their caregivers. While the importance of family members and caregivers in epilepsy management is increasingly recognized, a notable dearth of studies specifically focuses on their individual care and support experiences. In South Africa, several studies have been conducted on aspects such as the self-management experiences of people living with epilepsy, caregiver burden, and caregivers’ experiences with medication.7–10 However, a gap exists in understanding the lived experiences of family members and caregivers, particularly in rural areas of South Africa. This gap in knowledge hinders the development of comprehensive strategies and interventions that can effectively address the specific needs of family members and caregivers.
To bridge this gap, this paper explores the care and support experiences of family members and caregivers of people with epilepsy. By delving into these experiences, researchers can gain valuable insights and a deeper understanding of family members’ and caregivers’ unique challenges and requirements. This exploration will expand the existing knowledge base, helping researchers and healthcare professionals develop tailored strategies and interventions that address the specific needs of family members and caregivers. Ultimately, by shedding light on their experiences, this research aims to enhance the support provided to this critical group of individuals and improve overall epilepsy care and management.
Materials and Methods
This current study was the second phase of an explanatory sequential study conducted in rural Limpopo and Mpumalanga provinces in South Africa. These two provinces are located about 409 km away from each other. In Limpopo and Mpumalanga, there has been an increase in access to basic services as these provinces have a number of secluded rural settlements. More schools and clinics are being built near the villages, but hospitals are still reserved for the bigger towns. Limpopo has the fifth largest populationin South Africa, with an overall population of 400,000.11 In addition, Mpumalanga comprises 4.4 million people, 50.7% of, whom are female and 49.3% male. Although most of the population migrated from outside the country to Mpumalanga, over 100,000 migrants are from Limpopo province. The poverty headcount is at 7.8%, and most houses are reported to have access to basic needs.11
A qualitative case study method was employed to answer the objective: What were the family members’ and caregivers’ experiences of epilepsy care and support?
Population
The population of this study included 519 family members and caregivers from Limpopo and Mpumalanga provinces who participated in the quantitative stage of the study. This had both males and females, siblings to PLWE, parents, primary and secondary caregivers. Primary caregivers were the prominent persons within the family who cared for the patient, and the secondary caregivers cared for patients occasionally or were present when the patient needed care. In addition, only individuals above eighteen participated in the study.
Sampling & Inclusion Criteria
From the population, twenty participants were purposefully selected and recruited to participate in the study (ten from each province). However, during data collection, convenience sampling was applied concerning siblings found present during the time arranged for the interview. This included both males and females above the age of eighteen. Only participants who were parents or siblings of PLWE were included in the study.
Data Collection
Before data collection, individuals who participated in the study agreed to participate and signed a consent form. Data were collected physically (face-to-face) in Mpumalanga and telephonically in Limpopo. Telephonic interviews were used due to the financial restraints of the study. Telephonic interviews have been accredited by Rahman12, who argued that when compared to face-to-face interviews, they can yield accurate results. All selected individuals agreed to participate in the study as they were already familiar with it. However, two Mpumalanga participants were unavailable for the data collection appointments (including rescheduled dates) and resigned from participation. In Limpopo, one selected participant was not found because they gave their phone to a relative who lived in a different village.
Data were collected within three weeks by two trained research assistants who participated in the data collection as field note-takers or interview conductors. In Mpumalanga, data was collected within the participants’ homes. Both face-to-face interviews and telephone interviews were administered for 25–35 minutes. Data were collected via in-depth semi-structured interviews. The data collection tool was divided into two sections; section A was socio-demographic data, and section B included questions on participants’ experiences of epilepsy care and support. In Mpumalanga, data saturation was reached by participant three. In Limpopo, saturation was reached by participant six. However, the researchers interviewed three more participants in each province to ascertain saturation. In total, fifteen participants were included in the study. Raw data was analysed by the researcher using thematic analysis and co-coded by an independent researcher. From this analysis, two themes emerged, from which four subthemes came.
Results
Socio-Demographic Characteristics
The participants from this study were drawn from both Mpumalanga and Limpopo provinces. However, most participants came from Mpumalanga province (9), as illustrated in Table 1. The study comprised more females (10) than males (5). From these, the majority were parents to the patients (11) and had no formal education or only studied as far as their primary education (11). In addition to this, most participants were Christian faith believers (12).
 |
Table 1 Socio-Demographic Information |
From this study, two themes and four subthemes emanated, as illustrated in Figure 1. The two themes that emerged were experiences regarding epilepsy practices and Inadequate counselling and information sharing. From these themes, sub-themes, including epileptic seizure practice and epilepsy treatment, epilepsy source of knowledge and inadequate counselling and information sharing emerged. This study revealed discrepancies regarding proper techniques and sound knowledge concerning epilepsy care for PLWE.
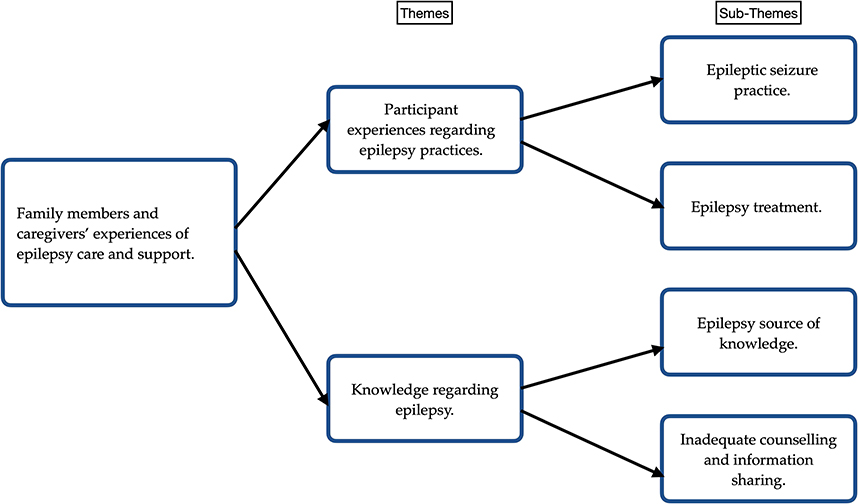 |
Figure 1 Study findings themes and subthemes. |
Theme 1: Participant Experiences Regarding Epilepsy Practices
Although challenging, participants expressed continued care for epileptic patients according to their needs. Some participants reported caring for an epileptic patient during a seizure as an emotional experience. In addition, some family members reported that they do not know what to do during a seizure.
…even now, it’s hard for me because when the seizure comes, he just dies for that certain moment. It is so painful to see him in such a condition. (Participant 7, F, MP)
… my mother knows almost everything about it because she is always around… (Participant 9, M, MP)
Sub-Theme 1: Epileptic Seizure Practice
This study shows that most participants were generally concerned about the patients not biting themselves, controlled room temperature, or having the jerking movements physically harming them. During a seizure, eight participants reported physically restraining the patient to stop the seizure or keep them from harming themselves. Two participants said they ensured the patient was in a cool temperature environment, and five participants placed something in the mouth. In the occurrence of a seizure, participants generally showed poor seizure care practices.
I normally hold him down, press him down and put him in a cool place. (Participant 1, F, LP)
I hold them for a while, 10 seconds, then they sleep for an hour. When they wake up, they are better. (Participant 8, M, LP)
I used to put a cloth, and now I put a spoon in their mouth… (Participant 11, F, MP)
Sub-Theme 2: Epilepsy Treatment
Although one participant reported using Christian methods (which, according to them, worked), most participants reported that their treatment preferences are Western medicine instead of traditional methods of treating epilepsy. These participants expressed their preferences as follows:
… seemed like he was getting worse day by day, and when we prayed, he was okay. (Participant 10, F, MP)
We tried traditional medication, we didn’t see a difference, but when he drinks Western ones, we see a difference. (Participant 15, F, MP)
I prefer Western medication because he gets better when he uses the treatment, which reduces seizures. (Participant 1, F, LP)
However, some participants expressed a challenge regarding attaining proper medication from local clinics (primary health care facilities). Participants showed that sometimes they must buy medication from their private funds because medication would run out or be ineffective.
…It is difficult because when we go to the clinic to take their regular dosage, sometimes they just say they don’t have medication. What are we supposed to do? (Participant 12, F, LP)
… I don’t give him medication from the clinic anymore. It doesn’t work. I take them to a doctor who will prescribe medication we will get from the pharmacy because that works for him. I’m even getting tired and broke because this medication costs much money, and he cannot continue without it. (Participant 13, F, LP)
His medication is not always available at a clinic. Sometimes we don’t get them [the medication]. (Participant 6, M, MP)
…we always get our medication at the hospital in another town… (Participant 8, M, LP)
Theme 2: Knowledge Regarding Epilepsy
When asked about epilepsy knowledge and support, two subthemes were found within this study: epilepsy source of knowledge and inadequate counselling and information sharing. Participants in this study generally expressed that they do know about epilepsy. However, they also shared that although highly needed, there is no counselling given to them and no intentional knowledge or information sharing about epilepsy.
Sub-Theme 1: Epilepsy Source of Knowledge
Participants showed they were not adequately equipped or educated about epilepsy, and there is no continued knowledge sharing with caregivers and family members. Almost all the participants explained that they first learned about or were made aware of epilepsy through a personal encounter with a seizure and learned about epilepsy through the patient. On the other hand, one participant had prior knowledge due to a history of epilepsy within the family, another participant first learned about epilepsy from the radio, and one participant never disclosed how they came to know about epilepsy. However, eleven participants showed they formally learned about epilepsy from a nurse after diagnosis at the clinic/hospital. In addition, five participants stated that they were never trained in epilepsy management or given any formal education about epilepsy.
… even my brother once suffered from it. It’s just that he didn’t suffer for a long period. (Participant 3, F, LP)
… no one has ever explained epilepsy to me. I don’t know what causes it, and all that information. His grandparents never had it. How did it get to him? (Participant 6, M, MP)
I got it at the clinic. A doctor told me that it is epilepsy and I must take care and keep an eye on him because if he can fall while he is alone, he can have a stroke. (Participant 14, F, MP)
No one has ever told me about this disease, and it was my first time witnessing it. (Participant 4, F, LP)
This other day on the radio, I heard them talking about it. (Participant 10, F, MP)
Sub-Theme 2: Inadequate Counselling and Information Sharing
The participants in this study showed that healthcare workers never provided any form of counselling and support for family members and caregivers. Twelve showed that the counselling sessions merely entailed diagnosis, caution towards treatment adherence, and seizure first aid. Furthermore, it was reported that there must be information sheets or follow-up counselling sessions when family members collect their medication. In contrast, four participants stated that home-based carers often talk to them in detail (as a form of counselling) about epilepsy during their monthly visits.
We have never received any pamphlets on epilepsy… we were just told that we must make sure the patient doesn’t bite their tongue and must not go near the fire (Participant 1, F, LP)
We have never been counselled,… no one has ever spoken to my family about epilepsy (Participant 8, M, LP)
They just told us we are supposed to give him medication (Participant 5, M, MP)
When we go to collect treatment, they just ask how the patient is doing and if they are coping. (Participant 12, F, LP)
Home-based carers used to come and give us health talks on epilepsy. When they come, they speak to anyone who is there at the house. (Participant 4, F, LP)
Home base carers visit us at home to advise us on how to treat the patient and also give health talks which cover counselling because they give us guidance and encourage us to keep caring for our brother (Participant 15, F, MP)
Discussion
The outcomes of this study suggest that seizure exposure is associated with knowledge and awareness of epilepsy. This implies that if these family members and caregivers have never cared for an epileptic patient, they may not understand what epilepsy is. This is reinforced by Musekwa et al13, who conducted a study on community members’ knowledge and understanding of epilepsy. The findings demonstrated Insufficient knowledge and moderate awareness. Furthermore, there is a clear and obvious failure to discern between epilepsy awareness and knowledge. This was illustrated when participants expressed that they first knew about epilepsy from the patient, although they were formally told about it at the clinics. In addition, participants in this study did not seem to be equipped appropriately in first aid management of a seizure. These behaviours explain why most family members and caregivers felt unprepared to handle a seizure,14 with most participants only resolving to inappropriate first aid procedures (such as physical restraint) as a kind of seizure care. It shows that family members and caregivers must be equipped to care for epileptic patients correctly.15–17 However, even with the different methods of seizure practices, most patients mentioned that Western methods (in terms of medication and treatment) were the best methods of epilepsy management.
The challenge of treatment attainment poses a significant obstacle for individuals seeking effective care.18–20 The study participants reported difficulties accessing medication and sometimes experienced its ineffectiveness. Despite these challenges, a majority of participants expressed a preference for Western treatment options over faith-based treatments.
The study suggests that the irregularities in management methods stem from a need for more training, information, and psychological support. To ensure the survival and well-being of patients, it is crucial to address these gaps by making training and information dissemination mandatory.21–23 Participants highlighted that healthcare workers occasionally shared insights on epilepsy. Still, a more intentional effort is needed to empower families and caregivers of epileptic patients with proper knowledge.
The study’s findings underscore the importance of professional healthcare providers actively educating and continuously sharing information about epilepsy. This is crucial to equip families and caregivers with the necessary knowledge and understanding to support individuals with epilepsy effectively. By providing ongoing education and information, healthcare providers can empower these stakeholders and contribute to improved outcomes for PLWE.
Limitations
The study’s data collection methods may have posed a limitation because to collect data and telephonic interviews may have weakened or limited the wealth of information that would have been brought forth. Telephonic interviews are impersonal, mainly because the researchers had already formed a rapport with the participants. The familiarity between researchers and participants may have influenced study biases during data collection.
Conclusion
The involvement of family members is crucial for enhancing the overall well-being and quality of life of individuals living with epilepsy. However, the participants in this study revealed a need for sufficient training and support in their role as caregivers. Moreover, they expressed significant challenges related to treatment, which could potentially affect their ability to adhere to epilepsy treatment plans. Therefore, these family members must receive proper education and training on epilepsy care from healthcare providers to ensure that they can provide adequate support. Irrespective of their geographic location or socioeconomic status, family members and caregivers need to stay updated with the latest knowledge and information about epilepsy. They can develop the skills and understanding required to effectively assist PLWE by acquiring the necessary education and training. This education should cover various aspects of epilepsy management, including medication adherence, recognizing and responding to seizures, and providing emotional support. Ensuring that family members and caregivers are well-informed and equipped will contribute to a higher standard of care for individuals with epilepsy.
Abbreviation
PLWE, People Living With Epilepsy.
Ethics Approval and Informed Consent
The study was conducted following the Declaration of Helsinki and approved by the Human and Clinical Trial Research Ethics Committee of the University of Venda (SHS/20/PSYCH/12/2710, approved 30 October 2020).
Consent for Publication
Authors consent that the details disclosed in this study can be published as is. Participants’ informed consent included the publication of anonymized responses.
Acknowledgments
The authors would like to acknowledge all study participants and support researchers who have offered support throughout the project. The authors would also like to acknowledge Prof A Maphula for supervising the research study.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis, and interpretation, or in all these areas; took part in drafting, revising, or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This research was funded by GladAfrica Foundation Trust and NIHSS-SAHUDA doctoral scholarship (project number: SDS20/1189). The work reported herein was made possible through funding by the South African Medical Research Council through its Division of Research Capacity Development under the SAMRC Researcher Development Award from funding received from the South African National Treasury (SAMRC/RCD/RDA23/24). The content hereof is the authors’ sole responsibility and does not necessarily represent the official views of the SAMRC or the funders.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Slowther AM. The role of the family in patient care. Clin Ethics. 2006;1(4):191–193. doi:10.1258/147775006779151148
2. Ostendorf AP, Gedela S. Effect of epilepsy on families, communities, and society. In: Seminars in Pediatric Neurology. WB Saunders; 2017:340–347.
3. Lee SA, Han SH, Cho YJ, et al. Factors associated with stigma and depressive symptoms in family members of patients with epilepsy. Epilepsy Behav. 2020;110:107129. doi:10.1016/j.yebeh.2020.107129
4. Berg AT, Kaiser K, Dixon‐Salazar T, et al. Seizure burden in severe early‐life epilepsy: perspectives from parents. Epilepsia Open. 2019;4(2):293–301. doi:10.1002/epi4.12319
5. England MJ, Liverman CT, Schultz AM, Strawbridge LM. Epilepsy across the spectrum: promoting health and understanding.: a summary of the Institute of Medicine report. Epilepsy Behav. 2012;25(2):266–276. doi:10.1016/j.yebeh.2012.06.016
6. Smith G, Wagner JL, Edwards JC. Epilepsy Update, Part 2. Am J Nurs. 2015;115(6):34–44. doi:10.1097/01.NAJ.0000466314.46508.00
7. Muchada IF, Wilmshurst JM, Laing N, Davies EH, Fieggen K. A qualitative study exploring caregivers’ experiences, perspectives, and expectations for precision medicine in epilepsy in South Africa. Epilepsy Behav. 2021;117:107873. doi:10.1016/j.yebeh.2021.107873
8. Miller WR, Von Gaudecker J, Tanner A, Buelow JM. Epilepsy self-management during a pandemic: experiences of people with epilepsy. Epilepsy Behav. 2020;111:107238. doi:10.1016/j.yebeh.2020.107238
9. Sabo UA, Buttner P, Scher G. Impact of caregiver burden on health-related quality of life and family functioning of carers of children with epilepsy at the charlotte maxeke johannesburg academic hospital, South Africa. South Af J Child Health. 2020;14(2):66–70. doi:10.7196/SAJCH.2020.v14i2.1603
10. Keikelame MJ, Swartz L. ‘Whom will I give him to? The difficulty is mine’: psychosocial difficulties experienced by care givers of patients with epilepsy in Cape Town, South Africa. J Health Psychol. 2016;21(11):2550–2561. doi:10.1177/1359105315581065
11. Statistics South Africa (StatsSA), Statssa.gov.za. Media Release Mpumalanga Community Survey 2016 results; 2016. Available from: https://www.statssa.gov.za/?p=8150.
12. Rahman RB. Comparison of telephone and in-person interviews for data collection in qualitative human research; 2023.
13. Musekwa OP, Makhado L, Maphula A. Public perception of epilepsy in rural Limpopo and Mpumalanga provinces: a quantitative study on knowledge, awareness, and attitudes. Challenges. 2022;13(2):65. doi:10.3390/challe13020065
14. Musekwa OP, Makhado L, Maphula A. Caregivers’ and Family Members’ Knowledge Attitudes and Practices (KAP) towards epilepsy in rural Limpopo and Mpumalanga, South Africa. Int J Environ Res Public Health. 2023;20(6):5222. doi:10.3390/ijerph20065222
15. O’Hara KA. First aid for seizures: the importance of education and appropriate response. J Child Neurol. 2007;22(5_suppl):30S–7S. doi:10.1177/0883073807303066
16. Kissani N, Moro M, Arib S. Knowledge, attitude and traditional practices towards epilepsy among relatives of PWE (patients with epilepsy) in Marrakesh, Morocco. Epilepsy Behav. 2020;111:107257. doi:10.1016/j.yebeh.2020.107257
17. Dessalegen HM, Gedlu E, Moges A. Knowledge, attitude and practices of parents and guardians of children with epilepsy at pediatric neurology clinic in a tertiary hospital in Ethiopia. Ethiop Med J. 2021;59:3.
18. Nicholas A. Unlocking the hidden burden of epilepsy in Africa: understanding the challenges and harnessing opportunities for improved care. Health Sci Rep. 2023;6(4):e1220. doi:10.1002/hsr2.1220
19. Chabangu Q, Maputle MS, Lebese RT. Management of epilepsy through indigenous traditional and Western approaches in Africa: a systematic review. Health SA Gesondheid. 2022;27:1–8.
20. Mmbando BP, Bhwana DK, Massawe IS, et al. Community knowledge, attitudes, and practices regarding epilepsy in Mahenge, Tanzania: a socio-anthropological study in an onchocerciasis-endemic area with a high prevalence of epilepsy. Epilepsy Behav. 2022;128:108568. doi:10.1016/j.yebeh.2022.108568
21. Shafer PO, Gilchrist B, Miller W, et al. Improving self-efficacy in seizure first aid: developing a seizure first aid certification program in the United States. Epilepsy Behav. 2022;129:108624. doi:10.1016/j.yebeh.2022.108624
22. Higgins A, Downes C, Varley J, Doherty CP, Begley C, Elliott N. Supporting and empowering people with epilepsy: contribution of the Epilepsy Specialist Nurses (SENsE study). Seizure. 2019;71:42–49. doi:10.1016/j.seizure.2019.06.008
23. Yu Z, Shao Q, Hou K, Wang Y, Sun X. The experiences of caregivers of children with epilepsy: a meta-synthesis of qualitative research studies. Front Psychiatry. 2022;13:987892. doi:10.3389/fpsyt.2022.987892
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.