Back to Journals » Journal of Multidisciplinary Healthcare » Volume 15
Is the Hospital Value-Based Purchasing Program Associated with Reduced Hospital Readmissions?
Authors Beauvais B ![]() , Whitaker Z
, Whitaker Z ![]() , Kim F, Anderson B
, Kim F, Anderson B
Received 3 February 2022
Accepted for publication 19 April 2022
Published 12 May 2022 Volume 2022:15 Pages 1089—1099
DOI https://doi.org/10.2147/JMDH.S358733
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Scott Fraser
Bradley Beauvais,1 Zachary Whitaker,2 Forest Kim,2 Benjamin Anderson3
1Texas State University, San Marcos, TX, USA; 2Baylor University, Waco, TX, USA; 3Colorado Hospital Association, Greenwood Village, CO, USA
Correspondence: Bradley Beauvais, Tel +210 627-1078, Email [email protected]
Introduction: Hospital readmissions have been associated with adverse outcomes and elevated financial costs to patients, families, and hospitals across the United States. Historically, nearly 20% of all Medicare discharges had a readmission within 30 days. In an effort to address this issue, the Affordable Care Act (ACA) established the Hospital Readmission Reduction Program (HRRP) in 2012 to positively influence readmissions associated with acute myocardial infarction, chronic obstructive pulmonary disease, heart failure, pneumonia, coronary artery bypass graft surgery, and total hip and/or knee arthroplasty. However, as recently as 2018, there were still 3.8 million 30-day all-cause adult hospital readmissions, with a 14% readmission rate and an average readmission cost of $15,200. The ACA also produced the Hospital Value-Based Purchasing (HVBP) program with the stated intent to (1) reduce mortality and complications, (2) reduce healthcare-associated infections, (3) increase patient safety, (4) improve the patient experience, and (5) increase efficiency and reduce costs. Given the costs and quality implications of an average readmission, it is logical to believe that HVBP eligible hospitals are simultaneously seeking to meet the goals of both programs. However, to date, no studies have examined if that is the case. Thus, in this study, we seek to determine if HVBP eligible hospitals are associated with a reduction in the core set of HRRP readmission rates better than the facilities that are not eligible for the HVBP program.
Methods: Hospital-level data from calendar year 2019 for 3,276 short-term acute care hospitals in the United States were evaluated using multivariate regression analysis to examine the readmission rate performance between 2,719 HVBP eligible hospitals and 557 ineligible hospitals.
Results: Our six separate multivariable linear regressions revealed a statistically significant and positive association between HVBP participation and readmission rates after controlling for numerous organizational, clinical complexity, and environmental factors. In each case, the magnitude of the positive directional association is moderate, ranging from and increase of +0.19% (pneumonia readmissions) to as high as +0.37% (all cause readmissions) for HVBP eligible hospitals. When considered in the context of the average number of discharges in our data set (x- = 9570), a third of a percent increase from the average 15.56% all cause readmissions to 16.08% in HVBP eligible hospitals equates to 50 additional readmissions annually (9570 × 15.56% = 1,489 vs 9570 × 16.08% = 1,539). At an average cost of $15,200 per readmission, which equates to an average additional cost to the average HVBP eligible hospital in excess of $760,000.
Discussion: The fact that there is a positive association between HVBP participating hospitals and readmissions at all, and that the same effect appears to be persistent across all dependent measures is concerning. One would logically expect hospitals that are focused on quality-based care to thoroughly care for individuals in order for them to not be readmitted to the hospital. The results provided do not necessarily prove that either program is not working. But they also do not confirm that the HVBP and HRRP programs are working together and accomplishing what they were originally designed to do: improve patient care and lower health-care costs.
Keywords: hospitals, value-based care, HVBP, readmissions, HRRP
Introduction
In the United States, health care is a $4 trillion industry (2020) and currently accounts for 17.7% of US Gross Domestic Product (GDP), and nearly a third of this cost (32.8%) is directly attributable to hospital care.5 The trajectory of health-care cost inflation shows little sign of slowing down as the health-care share of GDP is expected to rise to 19.7% by 2028.6 A significant portion of the expense incurred within the US healthcare system can be attributed to hospital readmission.1,2 In addition, over $52.4 billion is spent annually to care for patients that were readmitted to the hospital within 30 days for a previously treated condition.7,8 As recently as 2018, there were 3.8 million 30-day all-cause adult hospital readmissions, with a 14% readmission rate and an average readmission cost of $15,200.3
The 111th United States Congress and President Barack Obama sought to address these issues with the passage of the Patient Protection and Affordable Care Act.9 One outcome of the ACA was the advancement of a series of pay-for-performance (P4P) initiatives, which aim to reward hospitals that provide a higher quality of care through monetary incentives. The Centers for Medicare and Medicaid Services (CMS) led the way in designing P4P programs, including, among other programs, both the Hospital Value-Based Purchasing (HVBP) program and the Hospital Readmission Reduction Program.10
The purpose of HVBP is to incentivize hospitals to deliver high quality, versus merely high volume, care.11 The HVBP is specifically designed to improve the quality and experience of care for hospital patients.9 It does this by encouraging hospitals to improve the quality, efficiency, patient experience and safety of care that Medicare beneficiaries receive during acute care inpatient stays.9 HVBP eligible hospitals are assessed by a set of key metrics that determine the quality of care they provide, which result in reimbursements that are directly related to their quality-of-care ratings.12 The HVBP program contains four domains that are scored individually. These domains are (1) clinical outcomes, (2) safety, (3) person and community engagement, and (4) efficiency and cost reduction.
Some hospitals are excluded from the HVBP program annually. Exclusion reasons include hospitals that are subject to payment reductions under the Hospital Inpatient Quality Reporting (IQR) Program, hospitals that were cited for three or more deficiencies during the performance period that pose immediate jeopardy to the health or safety of patients, hospitals with an approved extraordinary circumstance exception (ECE), and hospitals located in the state of Maryland.13
The amount of financial benefit eligible hospitals receive is determined by the combination of Total Performance Score (TPS), however the HVBP program is budget neutral. This means that the entire 2% reduction must be paid back to participating hospitals. The highest-performing hospitals can earn back bonuses greater than the payment reduction, while others may receive minimal payment increases or not earn a bonus payment at all.11 In 2019, CMS paid out more than $1.9 billion to roughly 2,700 hospitals in the United States.14
In contrast to the HVBP program, which covers a broad spectrum of hospital performance, the HRRP program is more focused on reducing the number of readmissions for previously treated hospital conditions – specifically hip/knee replacement, chronic obstructive pulmonary disease (COPD), acute myocardial infarction (AMI), heart failure, pneumonia, and coronary artery bypass graft (CABG) surgery. Through the HRRP Program, the Centers for Medicare & Medicaid Services penalizes hospitals for “excess” readmissions when compared to “expected” levels of readmissions. According to the American Hospital Association, since the program began on Oct. 1, 2012, hospitals have prevented nearly 600,000 readmissions, but have also experienced nearly $2.5 billion in financial penalties.15
CMS’ intent with introduction and proliferation of these two value-based programs is clearly focused on improving patient outcomes. However, questions remain regarding whether there is a positive association between the two programs. It is logical to assume quality focused hospital leadership would seek to improve all aspects of care, but some have voiced concern if the different incentive structures and competing measures might be counterproductive.16
Some studies discuss problems with HVBP or identify the performance of hospitals within the program on various outcome measures (eg, mortality); however, to our knowledge, no comparison to hospitals that are not in the program has yet been made on the topic of readmissions, perhaps because it is presumed that eligible hospitals are logically operating at a higher level of performance.17–19
Literature Review
Based on 2013 Medicare Cost Report data, for every patient discharge, the median hospital lost $82; however, forty-five percent of hospitals were profitable, with 2.5% earning more than $2475 per adjusted discharge.20 In more recent years, hospital median operating margins have hovered around 2.4% (2019) and have dropped to a razor thin 0.5% in FY 2020.21 Thus, hospitals which participate in a volume-focused prospective payment reimbursement structure may be inclined to discharge patients from the hospital as quickly as possible in an effort to constrain costs and maintain profitability. With this in mind, it is reasonable to presume that quality of care may be compromised in some instances.22
It has been shown that there is a positive effect of financial incentives on performance.23 This is why pay-for-performance (P4P) programs were introduced into the health-care industry in recent years. Clearly, the primary goal of HVBP is to incentivize care providers to deliver high value, not just high volume, health care.12 Instead of rewarding the quantity of services rendered, HVBP rewards hospitals based on the quality of care provided to patients that are part of Medicare.9 In order to gauge the quality-of-care hospitals are providing, they use outcome measures such as mortality and complications, health care-associated infections, patient safety, patient experience, process, efficiency and cost reduction.24 Many of these measures continue to evolve. For example, assessing the patient experience has required modification of the questions to assess the quality of care provided at the hospital. Historically, the questions patients were being asked had more to do with a hotel stay than with a health-care institution.25 Although P4P programs make sense theoretically, many have questioned if it works in the health-care industry. Recent studies assess if the HVBP is measuring quality of care appropriately.17–19 However, these studies only look at how accurate the Total Performance Score (TPS) is in assessing quality of care in hospitals and none of the studies in question examined if hospitals participating in HVBP provide better quality care than those who do not. Some have also argued that many of the published studies evaluating the impact of P4P programs suffer from methodological weaknesses that make it hard to determine whether the HVBP intervention had an effect above and beyond other changes. Damberg, Sorbero, Lovejoy, Martsolf, and Raaen (2014) assessed hospital characteristics with how they were ranked in accordance to HVBP.26 The authors found that most of the variation among HVBP scores was attributed to profit status, geographic region, and the number of Comprehensive Primary Care reported measures. Another study observed how HVBP could affect the business model of the hospital. It was determined that HVBP was associated with superior hospital performance; however, the researchers seem to agree that the research contained some methodological challenges.17 Thus, these prior authors encountered difficulty determining if HVBP is the causal factor of the study’s positive observations, or if there were other factors involved.26
Figueroa, et al. evaluated the performance of 4,267 acute care hospitals, of which 2919 were currently participating in the HVBP program and 1,348 hospitals were ineligible and used as controls.27 The mortality rates were measured among all of the hospitals and then compared to determine if the eligible hospitals were associated with a lower 30-day risk adjusted mortality for acute myocardial infarction, heart failure, and pneumonia. The findings concluded that the evidence to suggest that HVBP led to a lower mortality rate is lacking. They also suggest, similar to other studies mentioned previously, that there are some holes in this specific pay for performance program.27
Another study conducted by Ryan et al also examined the HVBP program to assess if participating hospitals were associated with lower mortality rates.19 They evaluated the performance of the hospital in respect to mortality rate and other clinical processes and patient experience quality measures over the first four years that the HVBP program was in existence. They determined that HVBP was not associated with significant reductions of mortality rate and that even in respect to the measures of clinical process or patient experience, HVBP participating hospitals showed no significant improvement.19 Lastly, Werner and Bradlow (2006) concluded that hospital performance measures do not predict significant differences in hospital risk-adjusted mortality rate. Additionally, these authors suggest that further studies should be developed to determine other measures that are more associated with patient outcomes.28
Therefore, based primarily on the Figueroa, et al. and Ryan, et al. studies, we endeavor to extend their research and examine if HVBP eligible hospitals are associated with lower overall readmission rates.19,27 In our view, examining the difference in quality of care between eligible and non-eligible hospitals is important to determine if eligible hospitals are actively reducing readmissions to meet the goals of the HVBP program. Logically, one would presume that they do, but this premise has yet to be tested. Given some of these exclusion criteria previously noted (i.e., hospitals that are subject to payment reductions under the IQR program and hospitals that were cited for three or more deficiencies during the performance period that pose immediate jeopardy to the health or safety of patients), there is a logical basis to hypothesize that HVBP eligible hospitals are associated with lower overall hospital readmissions.
Methods
Data and Sample
Data from 3,276 hospitals were gathered from the Definitive Health care data set (defhc.com) from calendar year 2019. Definitive Health care compiled the data for this study, drawing from numerous public data sources including the Healthcare Cost Report Information System (HCRIS), Hospital Compare, the United States Census Bureau, the Centers for Medicare and Medicaid Services (CMS) Hospital Compare, the CMS Hospital Value-Based Purchasing (HVBP) program, the CMS Hospital Readmission Reduction Program (HRRP), and several others.
Measures – Dependent Variables
The dependent variables for this study are the standard set of Hospital Readmission Reduction Program (HRRP) variables – each of which is used to examine a different aspect of health-care service delivery. The variables include 30-day readmission rates for all cause hospital wide sources, hip/knee replacement, chronic obstructive pulmonary disease (COPD), acute myocardial infarction (heart attack), heart failure, and pneumonia. An insuffiient number of hospitals reported results for coronary artery bypass graft (CABG) surgery readmissions (n = 981). For this reason, we removed this dependent variable from the final analysis. The readmission rate indicates how many patients had to be readmitted back into a hospital within 30 days after they were originally discharged. Hospitals maintain lower readmission rates when they have appropriately resolved the patient’s health-care needs without further intervention.29–35
Measures – Independent Variable
The independent variable of interest is a dichotomous variable indicating whether the hospital is eligible for the HVBP program, or if they are not eligible for the HVBP program. In our dataset, this variable was coded as 1 = eligible, 0 = not eligible.
Measures – Control Variables
Numerous control variables are included in the study to account for the confounding variation in hospital readmissions associated with various individual hospital characteristics, including hospital ownership type (for profit vs not-for-profit), number of staffed beds as a proxy for size, teaching status, case mix index, average length of stay, outpatient service mix, urban or rural location, government operated or not, annual number of discharges as a proxy for level of utilization, hospital system membership, local hospital market concentration (as measured via the Herfindahl–Hirschman Index), occupancy rate, American Hospital Association geographic region, and Hospital Compare Score as a proxy for patient perceptions of care.
Dichotomous variables were coded as follows: system membership: 1 = part of a hospital system, 0 = not part of a hospital system; teaching: 1 = teaching hospital, 0 = not a teaching hospital; hospital compare score: 1 = score of 5, 0 = 4 or less; for-profit ownership: 1 = for profit, 0 = non-for-profit; government owned: 1 = government owned, 0 = not; and for the hospital city location: 1 = urban, 0 = rural based on US Census Bureau criteria. For the outpatient service mix, the inpatient and outpatient revenues were summed and used as the denominator and the outpatient revenue was used as the numerator to solve for the outpatient service mix as a proportion. Lastly, each hospital was assigned a geographic region in accordance with the American Hospital Association (1–9). The supportive sources to support inclusion of the control variables used in this study can be found in the Appendix.
Analysis
Six separate multivariable linear regressions were conducted for each response (dependent) variable using IBM SPSS Statistics package 27. Sample sizes for each model varied due to missing values associated with the dependent variable. Hospitals that lacked data for the dependent variable were removed for the analysis . In each of the analyses performed, the hypothesized relationship between HVBP participation and HRRP outcomes was rejected at an α = 0.05. Model fit was assessed using adjusted R2.
Results
Table 1 displays the overall descriptive statistics pertaining to the entire set of variables included in the study. The average readmission rates for each dependent variable were, for all causes: 15.56%, hip/knee replacement: 4.01%, chronic obstructive pulmonary disease: 19.67%, heart attack: 16.11%, heart failure: 21.96%, and pneumonia: 16.74%. Of the hospitals in our sample, 83% are participating in the HVBP program. 81% of hospitals are a part of a health system; whereas, only 5% of hospitals are ACGME accredited as teaching hospitals. A majority of the care services provided by the hospitals were outpatient services, as the service mix percentage is 54.74%. As far as the hospital compare rating goes, only 11% of the study sample received the maximum score of 5 on the survey. Approximately 24% of the hospitals in the data set are for-profit hospitals and about 15% of the hospitals in the data set are government operated. Most (69%) hospitals are located in urban areas. All hospitals across our sample had an average CMI of 1.63. The average number of annual discharges was 9,570 and the average number of staffed beds was 189. The average occupancy rate was 48.84% and the average length of stay was 4.48 days.
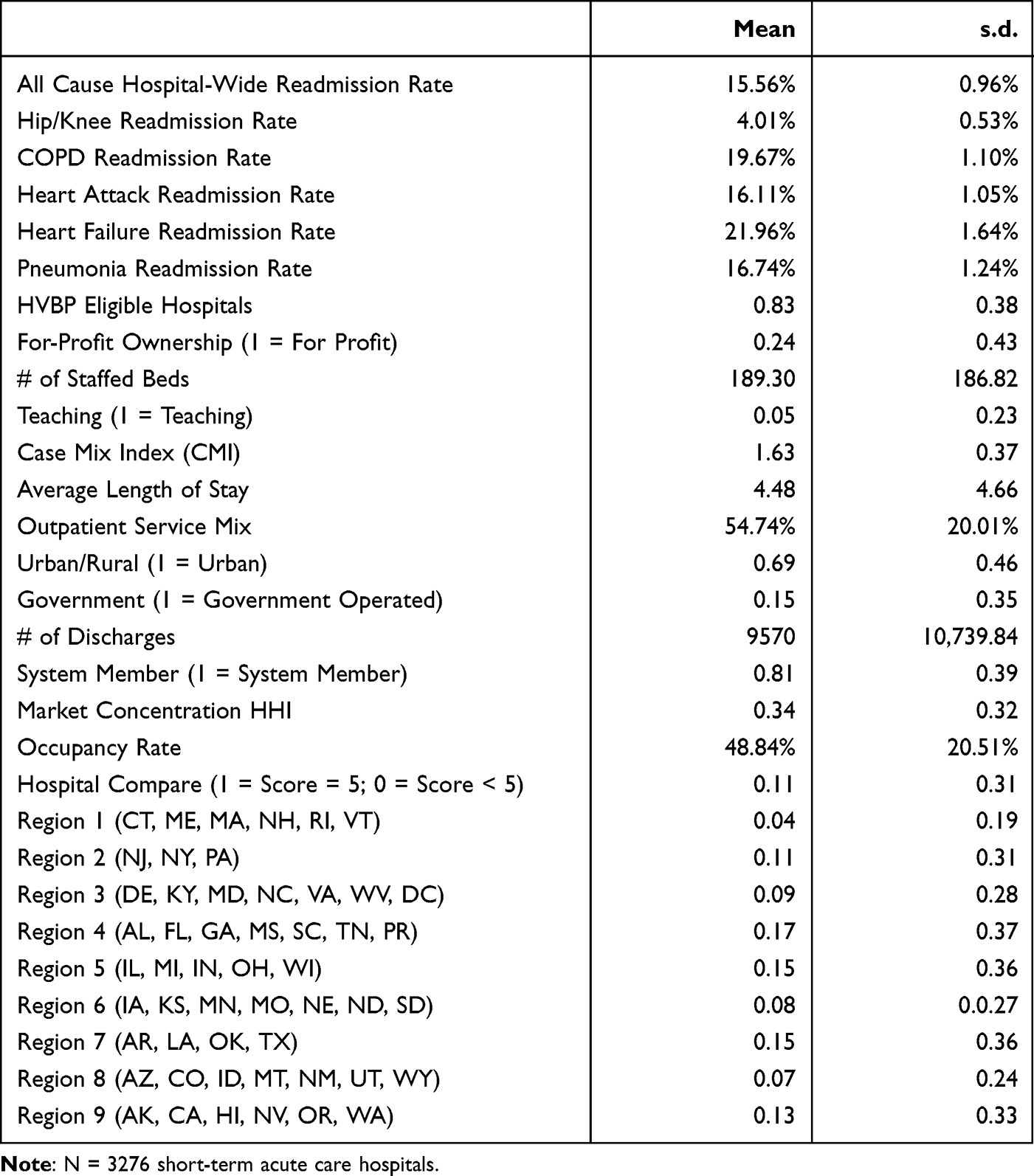 |
Table 1 Overall Descriptive Statistics |
Table 2 provides clarity pertaining to the differences between the HVBP participating and non-participating hospitals. Among other differences, on average, HBVP participating hospitals have a higher number of beds (213 vs 74), a higher number of discharges (10,841 vs 3,119), and maintain a lower average length of stay (4.31 vs 5.35). On some factors, there is little difference between the two groups, particularly with respect to case mix index (1.63 vs 1.62) and outpatient service mix (55.1% vs 53.04%).
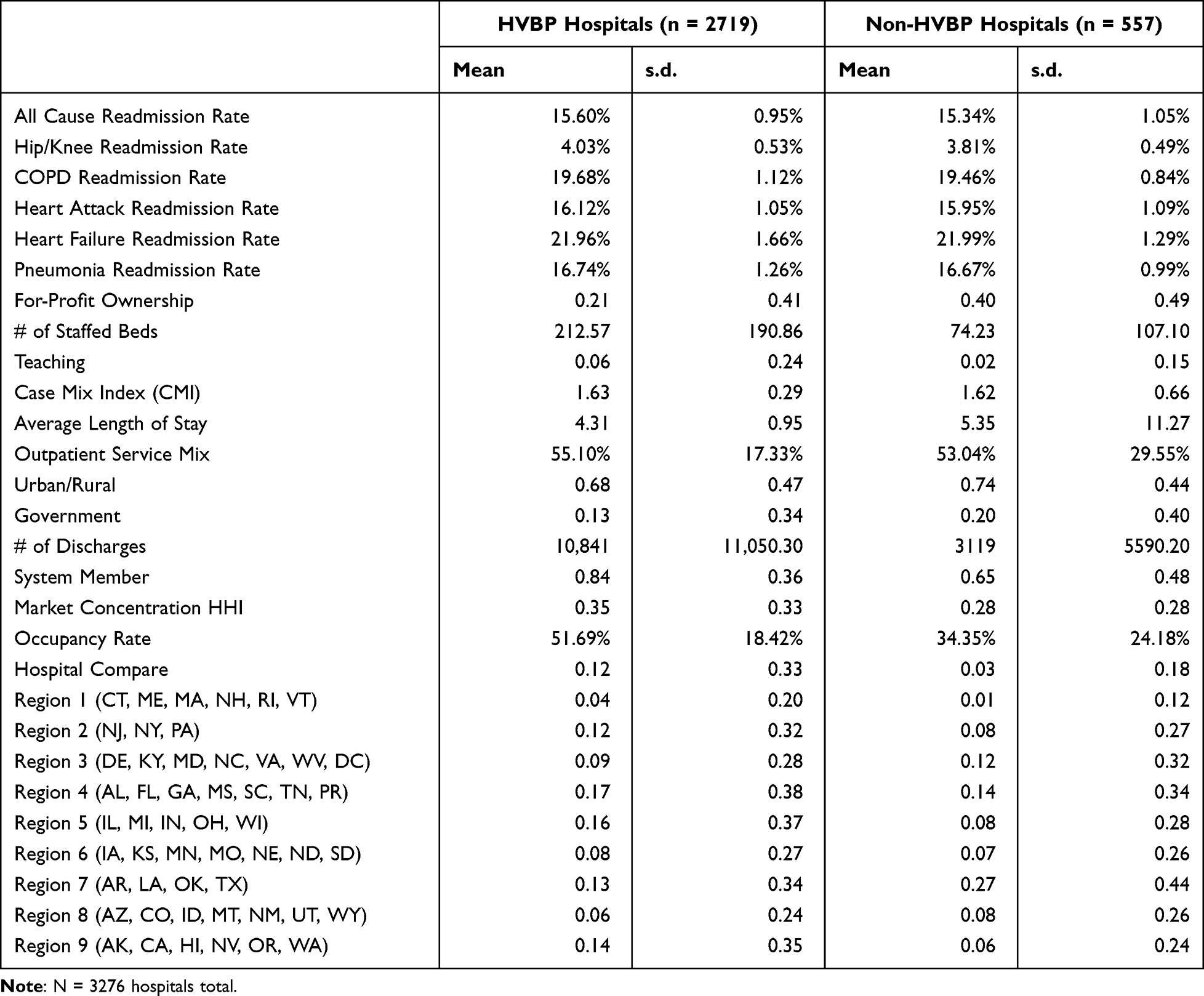 |
Table 2 Comparative Descriptive Statistics |
Table 3 shows the results of the regression analysis for each dependent variable. The analysis across all six dependent variables indicated models with moderate adjusted R2 values. The highest value was found in the “All Cause Hospital Wide Readmission Rate” at 24.7%. The remaining analyses demonstrated R2 values ranging from 10.0% (COPD) to 18.3% (Heart Failure). Our six separate multivariable linear regressions revealed a statistically significant and positive association between HVBP participation and readmission rates after controlling for numerous organizational and environmental factors. In each case, the magnitude of the directional association is moderate, ranging from a low 0.19% (pneumonia readmissions) to a high of 0.37% (all cause readmissions).
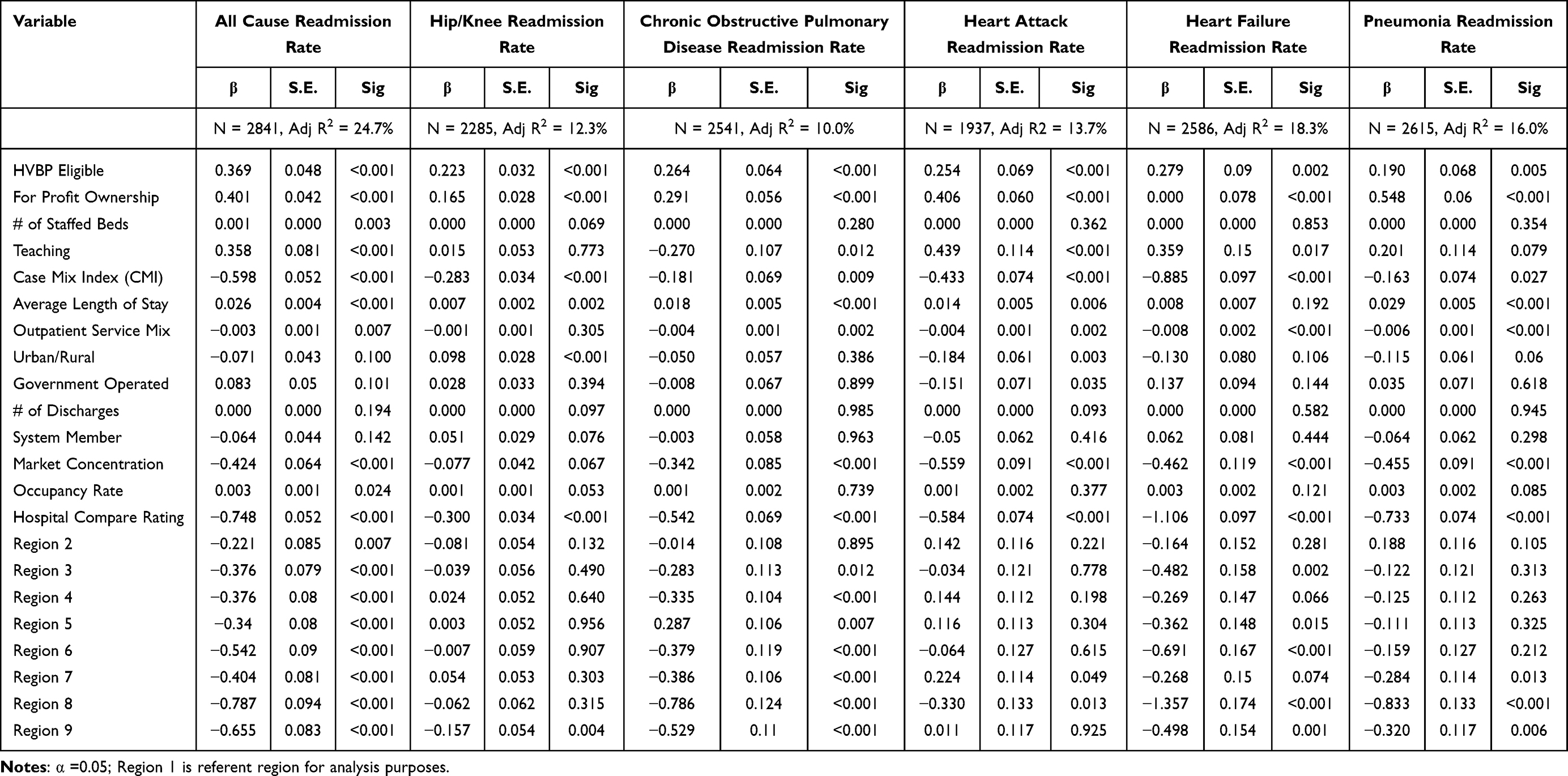 |
Table 3 Multiple Regression of All Readmission Rate Dependent Variables |
Additional interesting secondary findings were noted in the study results. Notably, for profit facilities and the average length of stay were both significantly and positively associated with readmission rates across all six dependent measures. Conversely, case mix index, outpatient service mix, market concentration, and the hospital compare score were all negatively associated with readmission rates – again, consistently observed across all six regression models.
Discussion
A hospital readmission, for any reason, is disruptive to all parties involved in the health-care delivery process: patients, families, caregivers, and the health-care system. Readmissions put patients at additional risk of hospital-acquired infections or complications and are a significant source of family stress. They are also a source of significant frustration to medical staff and may be very costly to the health-care system. Although some readmissions cannot be avoided as a result of the progression of chronic conditions, some may result from poor quality of care or inadequate transitional care.36 Therefore, while readmission rates would never be expected to be zero, there should always be an interest and concern pertaining to the reason for readmission and the variation in readmission rates across the broad spectrum of conditions we evaluated in this study.
Several researchers have independently examined the HVBP and HRRP programs to assess their association with improved quality, cost, patient satisfaction, hospital financial performance, and others. Some have assessed whether or not HVBP participating hospitals are associated with reduced mortality rates in comparison to ineligible hospitals.19,27 However, to the best of our knowledge, this study is the first to evaluate the association between these two value-based purchasing initiatives legislated through the Affordable Care Act.
Our findings reflect a significant and positive association between HVBP participating hospitals and every measure of hospital readmission in the HRRP program after controlling for numerous organizational and contextual factors. These results run contrary to our initial hypothesis. We conjecture a number of factors are contributory to this outcome. It is possible that hospital leaders are prioritizing their efforts on one set of measures over the other or are unable to maintain sufficient oversight over such a wide range of outcome measures simultaneously. Some have also expressed concern with the use of monetary enticements in the health-care industry and have indicated financial incentives are generally effective at improving targeted process of care, but may not necessarily improve patient outcomes.37,38
However, there is also ample evidence indicating improving the quality of care, including hospital readmissions, is inherently associated with improved financial performance.39,40 In a time when hospitals are struggling with the financial and capacity issues of the COVID-19 pandemic, the results of our study represent one additional unwelcome burden. In 2020, hospitals were projected to lose an estimated $323 billion, leaving nearly half of America’s hospitals and health systems with negative operating margins by the end of the year.41 So, while the magnitude of our results observed on our independent variables of interest could be considered relatively small, when considered in the context of the average number of discharges in our data set (x = 9,570), a third of a percent increase from the average 15.56% all cause readmissions to 16.08% in HVBP participating hospitals equates to 50 additional readmissions annually (9,570 × 15.56% = 1,489 vs 9,570 × 16.08% = 1,539). At an average cost of $15,200 per readmission, which equates to an average additional cost to the hospital in excess of $760,000.3,4
Lastly, the fact that there is a positive association between HVBP participating hospitals and readmissions at all, and that the same effect appears to be persistent across all dependent measures, is perhaps most concerning. This is troubling because one would expect hospitals that are focused on quality-based care to thoroughly care for individuals in order for them to not be readmitted to the hospital. The results provided do not necessarily prove that the program is not working. But they also do not confirm that the HVBP and HRRP programs are working together and accomplishing what they were fundamentally designed to do: improve patient care and lower health-care costs.
Limitations and Future Research
This study has some limitations. First, there may be other influences on readmissions that we did not control for in our study. This is apparent in our relatively low R2 values in each of our regression equations. Although we controlled for case mix index in our study, one significant factor which may be an important variable to consider in future research is the individual patient condition at point of admission and discharge. Clearly, this would require a more detailed and comprehensive dataset of patient-level data than we currently have access to, but we believe it would add substantive depth and quality to the study.
Second, we acknowledge that our current study does not include specifics pertaining to the demographics or socio-economics of the local patient population. Although we have included proxies for these factors in our study (ie, region, urban/rural, teaching/non-teaching, etc.), none of these are precise measures of these important factors. We logic that once a patient leaves a hospital, the hospital has little influence to ensure patient follows discharge instructions and care plan and conjecture that hospitals located in more impoverished areas do worse in the HRRP program than hospitals located in more affluent areas.
Third, this study uses a single cross-section of a data, thus we are not able to assess strengthening or weakening of impact over time. It is also possible, if not likely, that hospitals currently excluded from the program for one of the reasons previously noted, may have been eligible and participated in the past. Clearly, this is an area for additional research, as is further investigation into the component measures that comprise the HVBP score and their influence on hospital readmissions. At this point, we are only considering participation in the program or not as our independent variable of interest, however a logical next step is to examine each of the component HVBP elements to see how improvement or decline in each area might influence hospital readmissions. Earlier researchers have found that individuals who are being observed perform better at the same task than those who are not.42 One could presume that organizations, like individuals, will improve performance in areas of work that are being directly observed and incentivized. Thus, it is reasonable to assume that hospitals with published quality metrics are more likely to demonstrate higher quality scores on these measures than their counterparts whose quality metrics are not published.43
Lastly, an additional limitation of our study is the nature of the HRRP program as a measure of hospital quality performance. Some have questioned the program based on the measures used to define success – specifically, and exclusively, inpatient hospitalizations.44 Thus, observation stays, emergency department visits, or even the hastened death of a discharged patient may not be adequately accounted for in the program. These additional care settings may be worth considering for inclusion in future research efforts.
Conclusions and Practice Implications
There is an old proverb that says, “If you chase two rabbits, you will not catch either one”. The teachable lesson is that in trying to achieve two things at once, neither effort will be fruitful. In recent years, there has been an increased interest in the cost and quality of care provided at the hospital level. However, despite passage of the Affordable Care Act and the broad efforts of programs such as the HVBP and HRRP, the health-care industry continues to struggle with the implications of hospital readmissions. Based on our analysis, we question if these two programs are operating in concert, and further wonder if the sheer number of HVBP and HRRP measures are creating competing incentives for hospital leaders. If true, this has meaningful implications for patients, payers, policy-makers, and providers alike.
Ethics Statement
This research project was reviewed by the Texas State University Research Integrity and Compliance (RIC) under IRB Determination Request No. FWA00000191, on January 27th, 2022. According to the provisions in 45 CFR § 46.102 pertaining to “human subject” research, the RIC determined this study exclusively involves the examination of data originally collected and created by Definitive Healthcare, which provides data that is anonymous and publicly available. Therefore, the RIC concluded this research does not use human subjects and is not regulated by the provisions in 45 CFR § 46.102 and therefore an IRB review of the study was not required.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Jencks SF, Williams MV, Coleman EA. Rehospitalizations among patients in the Medicare fee-for-service program. N Engl J Med. 2009;360(14):1418–1428. doi:10.1056/NEJMsa0803563
2. McIlvennan CK, Eapen ZJ, Allen LA. Hospital readmissions reduction program. Circulation. 2015;131(20):1796–1803. doi:10.1161/CIRCULATIONAHA.114.010270
3. Weiss AJ, Jiang HJ. Overview of clinical conditions with frequent and costly hospital readmissions by payer, 2018: statistical brief# 278. 2021.
4. Bailey MK, Weiss AJ, Barrett ML, Jiang HJ. Characteristics of 30-day all-cause hospital readmissions, 2010–2016: statistical Brief# 248; 2019. Available from: https://www.hcup-us.ahrq.gov/reports/statbriefs/sb248-Hospital-Readmissions-2010-2016.jsp.
5. Keehan SP, Cuckler GA, Poisal JA, et al. National health expenditure projections, 2019–28: expected rebound in prices drives rising spending growth: national health expenditure projections for the period 2019–2028. Health Aff. 2020;39(4):704–714. doi:10.1377/hlthaff.2020.00094
6. Hartman M, Martin AB, Benson J, Catlin A; National Health Expenditure Accounts Team. National health care spending in 2018: growth driven by accelerations in medicare and private insurance spending: US health care spending increased 4.6 percent to reach $3.6 trillion in 2018, a faster growth rate than that of 4.2 percent in 2017 but the same rate as in 2016. Health Aff. 2020;39(1):8–17. doi:10.1377/hlthaff.2019.01451
7. Nuckols TK, Keeler E, Morton S, et al. Economic evaluation of quality improvement interventions designed to prevent hospital readmission: a systematic review and meta-analysis. JAMA Intern Med. 2017;177(7):975–985. doi:10.1001/jamainternmed.2017.1136
8. Fingar K, Washington R. Trends in hospital readmissions for four high-volume conditions, 2009–2013: statistical brief# 196. 2016.
9. Patient Protection & Affordable Care Act. Patient protection and affordable care act. Public Law. 2010;111(48):759–762.
10. James J. Pay-for-performance. Health Aff. 2012;34(8):1–6.
11. American Hospital Association. Hospital value based purchasing; 2021a. Available from: https://www.aha.org/hospital-value-based-purchasing/home.
12. Blumenthal D, Jena AB. Hospital value‐based purchasing. J Hosp Med. 2013;8(5):271–277.
13. Gugliuzza M, Bryant B. Where’s my report? Everything you want to know about the FY 2022 hospital VBP program percentage payment summary report [presentation transcript]. Hospital Value Based Purchasing Program; 2021. Available from: https://www.qualityreportingcenter.com/en/inpatient-quality-reporting-programs/hospital-inpatient-quality-reporting-iqr-program/2021-events/vbp12121/.
14. Morse S. CMS will pay $1.9 billion to hospitals in value-based payments for inpatient care; 2019. Available from: https://www.healthcarefinancenews.com/news/cms-will-pay-19-billion-hospitals-value-based-payments-inpatient-care.
15. American Hospital Association. Hospital value based purchasing; 2021b. Available from: https://www.aha.org/hospital-readmission-reduction-program/home.
16. Kahn CN, Ault T, Potetz L, Walke T, Chambers JH, Burch S. Assessing Medicare’s hospital pay-for-performance programs and whether they are achieving their goals. Health Aff. 2015;34(8):1281–1288. doi:10.1377/hlthaff.2015.0158
17. Borah BJ, Rock MG, Wood DL, Roellinger DL, Johnson MG, Naessens JM. Association between value-based purchasing score and hospital characteristics. BMC Health Serv Res. 2012;12(1):1–12. doi:10.1186/1472-6963-12-464
18. Ramirez AG, Tracci MC, Stukenborg GJ, Turrentine FE, Kozower BD, Jones RS. Physician-owned surgical hospitals outperform other hospitals in medicare value-based purchasing program. J Am Coll Surg. 2016;223(4):559–567. doi:10.1016/j.jamcollsurg.2016.07.014
19. Ryan AM, Krinsky S, Maurer KA, Dimick JB. Changes in hospital quality associated with hospital value-based purchasing. N Engl J Med. 2017;376(24):2358–2366. doi:10.1056/NEJMsa1613412
20. Bai G, Anderson GF. A more detailed understanding of factors associated with hospital profitability. Health Aff. 2016;35(5):889–897. doi:10.1377/hlthaff.2015.1193
21. Hospital Financial Management Association. NFP hospital profitability plummeted in 2020 despite expense mitigation strategies, Moody’s reports; 2021. Available from: https://www.hfma.org/topics/financial-sustainability/article/nfp-hospital-profitability-plummeted-in-2020-despite-expense-mit.html.
22. Miller HD. From volume to value: better ways to pay for health care. Health Aff. 2009;28(5):1418–1428. doi:10.1377/hlthaff.28.5.1418
23. Garbers Y, Konradt U. The effect of financial incentives on performance: a quantitative review of individual and team‐based financial incentives. J Occup Organ Psychol. 2014;87(1):102–137. doi:10.1111/joop.12039
24. Centers for Medicare and Medicaid Services. Hospital value based purchasing program; 2021. Available from: https://www.cms.gov/Medicare/Quality-Initiatives-Patient-Assessment-Instruments/HospitalQualityInits/Hospital-Value-Based-Purchasing-.
25. Mazurenko O, Collum T, Ferdinand A, Menachemi N. Predictors of hospital patient satisfaction as measured by HCAHPS: a systematic review. J Health Care Manag. 2017;62(4):272–283.
26. Damberg CL, Sorbero ME, Lovejoy SL, Martsolf GR, Raaen L, Mandel D. Measuring success in health care value-based purchasing programs: findings from an environmental scan, literature review, and expert panel discussions. Rand Health Quart. 2014;4(3):240.
27. Figueroa JF, Tsugawa Y, Zheng J, Orav EJ, Jha AK. Association between the value-based purchasing pay for performance program and patient mortality in US hospitals: observational study. BMJ. 2016;2016:353.
28. Werner RM, Bradlow ET. Relationship between Medicare’s hospital compare performance measures and mortality rates. JAMA. 2006;296(22):2694–2702. doi:10.1001/jama.296.22.2694
29. Haas B, Gomez D, Hemmila MR, Nathens AB. Prevention of complications and successful rescue of patients with serious complications: characteristics of high-performing trauma centers. J Trauma Acute Care Surg. 2011;70(3):575–582. doi:10.1097/TA.0b013e31820e75a9
30. Benbassat J, Taragin M. Hospital readmissions as a measure of quality of health care: advantages and limitations. Arch Intern Med. 2000;160(8):1074–1081. doi:10.1001/archinte.160.8.1074
31. Chee TT, Ryan AM, Wasfy JH, Borden WB. Current state of value-based purchasing programs. Circulation. 2016;133(22):2197–2205. doi:10.1161/CIRCULATIONAHA.115.010268
32. Das A, Norton EC, Miller DC, Ryan AM, Birkmeyer JD, Chen LM. Adding a spending metric to Medicare’s value-based purchasing program rewarded low- quality hospitals. Health Aff. 2016;35(5):898–906. doi:10.1377/hlthaff.2015.1190
33. Krumholz HM, Wang K, Lin Z, et al. Hospital-readmission risk—isolating hospital effects from patient effects. N Engl J Med. 2017;377(11):1055–1064. doi:10.1056/NEJMsa1702321
34. Morley C, Unwin M, Peterson GM, Stankovich J, Kinsman L. Emergency department crowding: a systematic review of causes, consequences and solutions. PLoS One. 2018;13(8):e0203316. doi:10.1371/journal.pone.0203316
35. Shen Y, Lee LH. Improving the wait time to consultation at the emergency department. BMJ Open Qual. 2018;7(1):e000131. doi:10.1136/bmjoq-2017-000131
36. Rifkin W. 30-day hospital readmission rate - a flawed but important metric [White Paper], MCG; 2021. Available from: https://info.mcg.com/white-paper-30-day-readmission-rate.html.
37. Flodgren G, Eccles MP, Shepperd S, Scott A, Parmelli E, Beyer FR. An overview of reviews evaluating the effectiveness of financial incentives in changing health care professional behaviours and patient outcomes. Cochrane Database Syst Rev. 2011;(7). doi:10.1002/14651858.CD009255
38. Doran T, Maurer KA, Ryan AM. Impact of provider incentives on quality and value of health care. Annu Rev Public Health. 2017;38:449–465. doi:10.1146/annurev-publhealth-032315-021457
39. Akinleye DD, McNutt LA, Lazariu V, McLaughlin CC. Correlation between hospital finances and quality and safety of patient care. PLoS One. 2019;14(8):e0219124. doi:10.1371/journal.pone.0219124
40. Beauvais B, Richter JP, Kim FS, et al. Does patient safety pay? Evaluating the association between surgical care improvement project performance and hospital profitability. J Health Care Manag. 2019;64(3):142–154.
41. American Hospital Association. Hospitals face continued financial challenges one year into the COVID-19 pandemic; 2021c. Available from: https://www.aha.org/system/files/media/file/2021/03/hospitals-face-continued-financial-challenges-one-year-into-covid-19-pandemic-fact-sheet.pdf.
42. McCambridge J, Witton J, Elbourne DR. Systematic review of the Hawthorne effect: new concepts are needed to study research participation effects. J Clin Epidemiol. 2014;67(3):267–277. doi:10.1016/j.jclinepi.2013.08.015
43. Hibbard JH, Stockard J, Tusler M. Does publicizing hospital performance stimulate quality improvement efforts? Health Aff. 2003;22(2):84–94. doi:10.1377/hlthaff.22.2.84
44. Wadhera RK, Yeh RW, Maddox KEJ. The hospital readmissions reduction program—time for a reboot. N Engl J Med. 2019;380(24):2289. doi:10.1056/NEJMp1901225
 © 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2022 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.