")
Back to Journals » Neuropsychiatric Disease and Treatment » Volume 12
Is the Dissociative Experiences Scale able to identify detachment and compartmentalization symptoms? Factor structure of the Dissociative Experiences Scale in a large sample of psychiatric and nonpsychiatric subjects
Authors Mazzotti E , Farina B, Imperatori C, Mansutti F, Prunetti E, Speranza AM, Barbaranelli C
Received 26 January 2016
Accepted for publication 9 March 2016
Published 3 June 2016 Volume 2016:12 Pages 1295—1302
DOI https://doi.org/10.2147/NDT.S105110
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Roger Pinder
Eva Mazzotti,1 Benedetto Farina,2 Claudio Imperatori,2 Federica Mansutti,3,4 Elena Prunetti,3,4 Anna Maria Speranza,5 Claudio Barbaranelli1
1Department of Psychology, Faculty of Medicine and Psychology, Sapienza University of Rome, Rome, Italy; 2Department of Human Sciences, European University of Rome, Rome, Italy; 3Associazione di Psicologia Cognitiva e Scuola di Psicoterapia Cognitiva, Rome, Italy; 4Casa di Cura Villa Margherita, Arcugagno (Vi) Italy, 5Department of Dynamic and Clinical Psychology, Sapienza University, Rome, Italy
Background: In this study, we explored the ability of the Dissociative Experiences Scale (DES) to catch detachment and compartmentalization symptoms.
Participants and methods: The DES factor structure was evaluated in 768 psychiatric patients (546 women and 222 men) and in 2,403 subjects enrolled in nonpsychiatric settings (1,857 women and 546 men). All participants were administered the Italian version of DES. Twenty senior psychiatric experts in the treatment of dissociative symptoms independently assessed the DES items and categorized each of them as follows: “C” for compartmentalization, “D” for detachment, and “NC” for noncongruence with either C or D.
Results: Confirmatory factor analysis supported the three-factor structure of DES in both clinical and nonclinical samples and its invariance across the two groups. Moreover, factor analyses results overlapped with those from the expert classification procedure.
Conclusion: Our results showed that DES can be used as a valid instrument for clinicians to assess the frequency of different types of dissociative experiences including detachment and compartmentalization.
Keywords: Dissociative Experiences Scale, confirmatory factor analysis, detachment, compartmentalization, validity
A Letter to the Editor has been received and published for this article.
Introduction
According to the fifth edition of the Diagnostic and Statistical Manual of Mental Disorders (DSM-5) the term “dissociation” is used to identify the “disruption of/and or discontinuity in the normal integration of consciousness, memory, identity, emotion, perception, body representation, motor control, and behavior.”1 Moreover, DSM-5 states that “dissociative symptoms can potentially disrupt every area of psychological functioning.”1 Despite this definition, there is still no agreement on many aspects of dissociation, such as conceptualization, interpretation, and categorization, of dissociative experiences and symptoms.2–4
The existence of different forms of dissociative experiences has been suggested from normal dissociative experiences, such as absorption/imaginative symptoms, to pathological dissociative experiences, such as depersonalization/derealization phenomena and dissociative amnesia.3–5 Furthermore, it has been proposed to distinguish dissociative pathological phenomena into the following two main categories with different definitions, mechanisms, and treatment implications: detachment and compartmentalization.5,6 Detachment is defined by the subjective experience of “an altered state of consciousness, characterized by a sense of separation (or detachment) from certain aspects of everyday experience, be it the body (as in out-of-body experiences), the sense of self (as in depersonalization), or the external world (as in derealization).”5 Compartmentalization is characterized by a partial or complete failure: “in the ability to deliberately control processes or actions that would normally be amenable to such control”.5 This definition refers to “conditions characterized by an inability to bring normally accessible information into conscious awareness (eg, dissociative amnesia), which can also be regarded as a control problem”.5
The Dissociative Experiences Scale (DES)7 is one of the most common instruments used to investigate different kind of dissociative symptoms in both clinical and nonclinical samples.8 It consist of 28 items that assess the frequency and severity of a wide range of dissociative experiences using an eleven-point visual analog scale (0%–100%).
Although the DES showed excellent convergent validity with other dissociative experiences questionnaires and excellent predictive validity with dissociative disorders,8 factor analyses have detected conflicting results. Even though a three-factor structure (ie, absorption, amnesia, and depersonalization–derealization dimensions) has been consistently documented,9–12 other studies also reported one-factor,13–15 two-factor,16–18 four-factor,19–22 and seven-factor models.23
Although the Italian version of the DES is widely used, to the best of our knowledge, no study has investigated the detachment and compartmentalization dimensions of the DES in a large sample of psychiatric and nonpsychiatric individuals. Fabbri et al,15 comparing the fit of the one-factor, two-factor, and three-factor models in 364 nonpsychiatric adults, reported a better fit for the one-factor model. A one-factor solution has been also reported by Mazzotti and Cirrincione in 330 Italian undergraduate students.13 Recently, Garofalo et al17 obtained a two-factor model in a sample of 122 inmates and 198 community participants. Although the authors suggested that these two factors may reflect the detachment and compartmentalization phenomena, the DES items were not categorized in detachment and compartmentalization dissociative experiences.
Therefore, the aims of this study were to investigate 1) the ability of the DES to catch detachment and compartmentalization dissociative experiences, 2) the generalizability of the factorial solution across a large sample of psychiatric and nonpsychiatric subjects, and 3) the psychometric properties of the Italian version of the DES.
Participants and methods
Participants
The participants were 780 Italian patients who were referred for treatment of psychiatric disorders (546 women and 222 men; mean age: 39.2±13.91 years) and 2,303 subjects enrolled in nonpsychiatric settings (1,857 women and 546 men; mean age: 30.3±14.17 years). The psychiatric sample comprised 1) 212 outpatients from six public mental health centers in Rome, Italy, and 2) 568 inpatients from a mental health care clinic in Vicenza, Italy. Patients were consecutively referred to the centers, in nonemergency situations, between 2007 and 2010. The patients’ response rate was 98.7%.
The nonpsychiatric sample was obtained by administering the DES to 1) undergraduate students (N=1,358) enrolled at the School of Psychology, Chieti University, Italy; 2) consecutive sample of adults self-referred to a dermatology outpatient clinic in Rome, Italy (N=491; response rate, 88.8%); 3) women seen at outpatient gynecological health care centers in Rome, Italy (N=145; response rate, 72.5%); 4) cancer patients and their caregivers, attending chemotherapy treatment in a Clinic Cancer Center in Rome (N=122 and N=145; response rate, 91.8% and 96.7%, respectively); and 5) airline company employees (N=42; response rate, 72.4%). For the nonpsychiatric sample, we chose to collect data from different settings in order to avoid sampling bias (ie, focus on a specific group, such as undergraduate students).
Inclusion criteria were age ≥18 years and Italian speaking. Exclusion criteria were the inability to complete the assessment for whatever reason (ie, insufficient time/willingness) and/or the refusal to provide informed consent. Study participants contributed voluntarily and anonymously after providing informed consent. No compensation was provided for completing the assessments. Written informed consent was obtained from all participants after providing complete information about the purpose of the study. Data collection was performed at each site under the guidelines approved by the respective medical ethics committee to guarantee anonymity and privacy, utilizing unique coded identifiers. The research was approved by the ethics review boards of Sapienza University and the European University of Rome.
Procedure
All participants were administered the Italian versions of the DES13 and a checklist assessing demographic (ie, sex and age) and clinical characteristics (ie, patient-reported condition and time elapsed since diagnosis/symptoms). Psychiatric patients were diagnosed using the structured clinical interview for DSM-IV Axis I and Axis II disorders (SCID-I and SCID-II).24,25 Only in this group, SCID-D was used only when the DES score was >25. Demographic and clinical data of psychiatric and nonpsychiatric sample are listed in Table 1.26
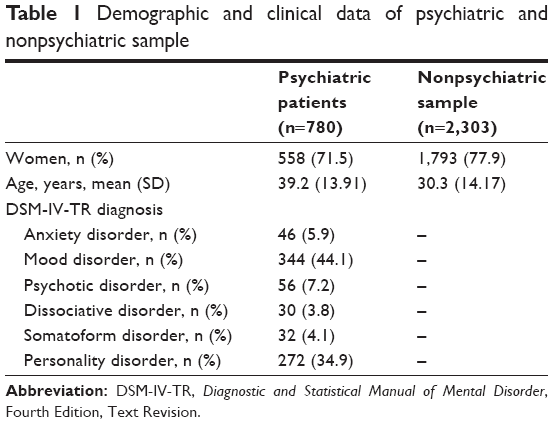 | Table 1 Demographic and clinical data of psychiatric and nonpsychiatric sample |
The DES is a 28-item, self-administered inventory to measure the frequency of dissociative experiences.7 To answer the DES questions, subjects indicate the percentage of time (given in 10% increments ranging from 0 to 100) they had the experience described.
The Italian version of the DES,13 which was translated in 1996 for the first time,15 was used in this study. Good psychometric properties were reported in the Italian validation, such as good internal consistency (Cronbach’s α =0.90).13
DES items are thought to reflect three dissociative experiences: 1) absorption experiments (“Some people find that when they are watching television or a movie they become so absorbed in the story that they are unaware of other events happening around them” [translation “Alcune persone, mentre guardano la televisione o un film, sono così assorbiti dalla storia che stanno guardando, da non rendersi conto di ciò che sta accadendo intorno a loro”]); 2) amnesia experiences (“Some people find that they have no memory for some important events in their lives” [translation “Alcune persone scoprono di non avere alcun ricordo di eventi importanti della propria vita”]); and 3) depersonalization–derealization experiences (“Some people have the experience of feeling that their body does not seem to belong to them” [translation “Ad alcune persone capita di avere la sensazione che il proprio corpo non appartenga loro”]).
A subset of eight items of the DES, the so-called DES-T, is considered especially as sensitive to identify pathological dissociation.27 The DES-T total score is calculated by averaging items 3, 5, 7, 8, 12, 13, 22, and 27 of DES (“Some people have the experience of finding themselves in a place and have no idea how they got there” [translation “Ad alcune persone capita di trovarsi in un posto e di non avere alcuna idea di come vi siano arrivati”]). A cutoff score of 15 is widely used to identify patients with pathological dissociation.28,29
DES items classification by experts
The expert judgment method gathers the opinions of a group of 20 experts with the aim of producing an accurate, unbiased estimate. All experts were selected for their expertise with dissociative patients, ie, >20 years of clinical work with dissociative patients in their curriculum vitae. A detailed email with the central aim of the study (ie, the ability of the DES to catch detachment and compartmentalization dissociative experiences) was sent by the senior author (BF) to 25 experts in the field of dissociative disorders. Two of them refused to participate, and three of them did not respond.
The expert judgment method is a structured technique involving a multistep procedure: 1) providing a written definition of compartmentalization and detachment, in accordance with Holmes et al, and a response form;5 2) assessment by 20 senior psychiatric experts individually the DES items and categorization of each of them as follows: “C” for compartmentalization, “D” for detachment, and “NC” for noncongruence with either C or D; and 3) finally, collection and analyses of the expert’s personal estimate.
Statistical analysis
The frequency distribution of the responses to the DES individual items was studied for skewness and kurtosis. Reliability in terms of internal consistency of the DES dimensions was examined by calculating Cronbach’s α.
A confirmatory factor analysis (CFA), the three-factor model according to the expert judgment, was performed. In particular, this model was examined in a large sample of psychiatric and nonpsychiatric subjects.
The weighted least squares means and variance adjusted (WLS-MV) method for estimating parameters in a skewed distribution (included in the MPLUS 7.11 software) was utilized to conduct CFA.30 WLS-MV provides “weighted least square parameter estimates using a diagonal weight matrix with standard errors and mean and variance adjusted chi-square test statistic that use a full weight matrix.”30 Factor solutions were evaluated by means of goodness-of-fit indices available in MPLUS. Values <0.08 for standardized root-mean-squared residual and <0.05 for root-mean square error approximation (RMSEA) are deemed to be adequate.31 Three different sets of CFAs were performed on all samples (total, psychiatric sample, and nonpsychiatric sample).
Independent (unpaired) samples t-tests were used to analyze the differences between groups. Spearman’s rho coefficients were reported as measures of associations among DES-T and DES factors’ questionnaires.
All statistical analyses were performed using STATA, Version 11.0 (StataCorp LP, College Station, TX, USA) and the MPLUS 6.11 software.
Results
Preliminary descriptive analyses and DES items classification
All the DES items presented a highly nonnormal distribution, with skewness ranging from 0.05 to 5.08 (2.07±6.79) and kurtosis ranging from −0.70 to 30.18 (5.22±6.79). This phenomenon appeared in both samples but was particularly relevant in the nonpsychiatric sample, where the item distribution showed higher positive skewness. Accordingly, in all items except three (items 15, 18, and 24), nonpsychiatric subjects obtained statistically significant lower scores.
Classification of DES items and percentage of experts’ agreement are listed in Table 2. For compartmentalization dissociative experiences, a percentage of agreement ≥85 was reported for nine DES items (eg, “Found new things among belongings but not remembering buying them”). For detachment dissociative experiences, a percentage of agreement ≥85 was reported for seven DES items (eg, “Felt body was not one’s own”).
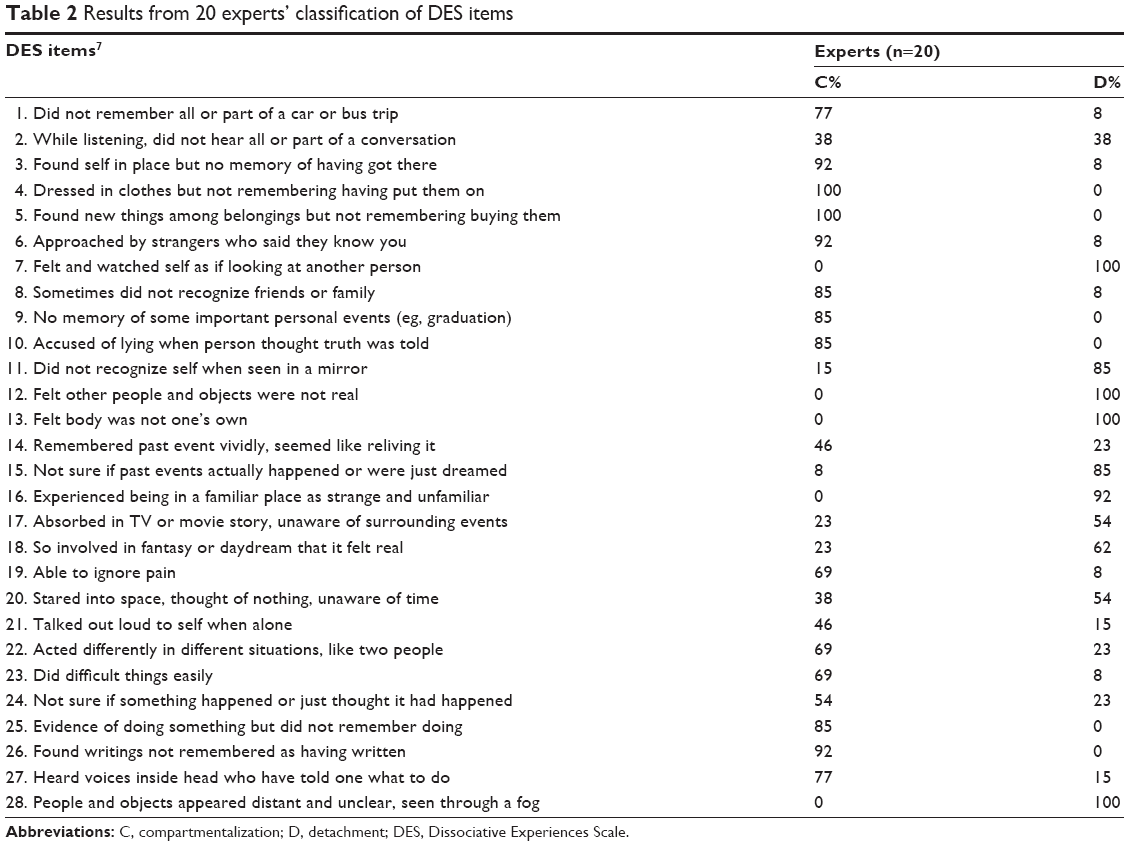 | Table 2 Results from 20 experts’ classification of DES items |
CFA
As reported in Table 3, the three-factor solution can be supported from fit indices in any sample considered (total, psychiatric patients, and nonpsychiatric subjects). RMSEA and standardized root-mean-squared residual showed excellent fit, being far beyond the suggested cutoff of 0.06 and 0.08, respectively, while comparative fit index (CFI) and Tucker–Lewis index (TLI) showed only a marginal fit. One possible answer comes from what was recently outlined by David Kenny,32 who noted that TLI and CFI values: are related with the average size of the correlations in the data (eg, TLI will not be very high when the average correlation between variables is not high). He also noted that “a reasonable rule of thumb is to examine the RMSEA for the null model and make sure that is no smaller than 0.158. If the RMSEA for the null model is less than 0.158, an incremental measure of fit may not be that informative”.32
 | Table 3 Fit indices of the three-factor solution |
In the samples and subsamples considered in Table 3, RMSEA of the null model ranged from 0.08 to 0.10, with an average of 0.09. According to Kenny’s suggestion, then the TLI and CFI results must be considered with caution, as they are substantially noninformative of the model’s fit.
Factor loadings’ estimates of the items in the various samples are reported in Table 4. The first for the first factor scale (which we called “nonpathological absorption”) included items 1, 2, 10, and 14–26; the second factor scale (compartmentalization) included items 3–6, 8, and 9; the third factor scale (detachment) included items 7, 11–13, 27, and 28.
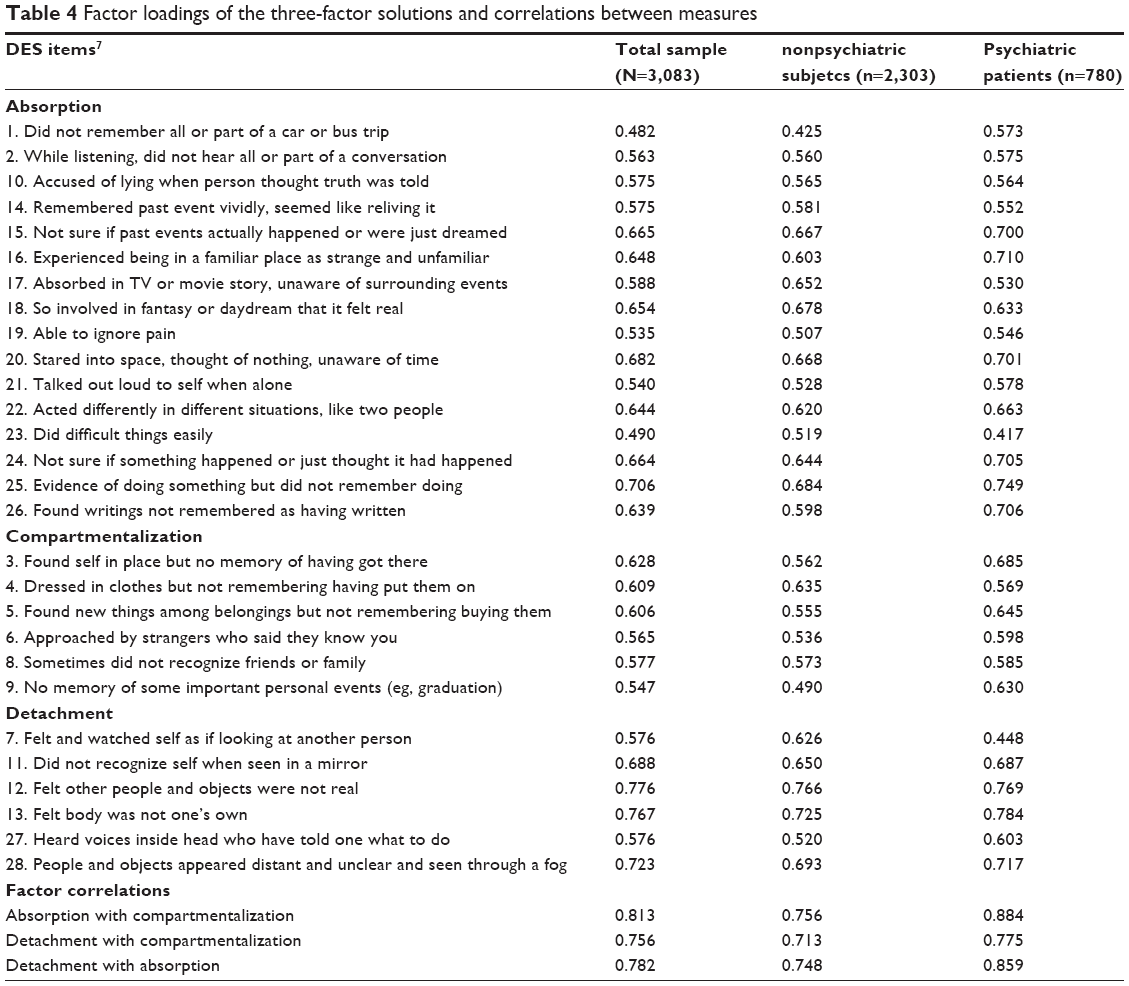 | Table 4 Factor loadings of the three-factor solutions and correlations between measures |
Factor reliability
Computed using Cronbach’s α, reliability for the nonpathological absorption factor was 0.90. Reliability for the “compartmentalization” factor was 0.74. Finally, the reliability for the “detachment” factor was 0.84. The item-total corrected correlation coefficients ranged from 0.67 to 0.80.
Table 5 shows the DES-total score and the compartmentalization, detachment, and nonpathological DES-subscales’ scores, along with mean and SD in each categories. When compared to nonpsychiatric subjects, psychiatric patients reported higher compartmentalization (11.02±14.26 vs 6.58±9.03; t1,003.08=8.15, P<0.001), detachment (17.48±19.78 vs 7.46±12.40; t998.5=13.32, P<0.001), and absorption dissociative experiences (24.35±18.16 vs 20.34±14.78; t1,153.56=5.58, P<0.001). Furthermore, patients with dissociative disorders reported higher compartmentalization (19.17±13.30 vs 9.08±13.16; t506=4.07, P<0.001), detachment (34.58±24.43 vs 12.80±16.19; t30.62=4.82, P<0.001), and absorption dissociative experiences (35.65±24.43 vs 19.81±15.61; t506=5.42, P<0.001) than patients with other Axis I disorders. Finally, patients with borderline personality disorder reported higher compartmentalization (15.93±16.84 vs 10.54±13.19; t269.98=2.96, P<0.01), detachment (27.63±22.99 vs 18.94±20.11; t265.22=3.32, P<0.001), and absorption dissociative experiences (35.47±21.04 vs 25.66±17.41; t268.93=4.21, P<0.001) than patients with other personality disorders.
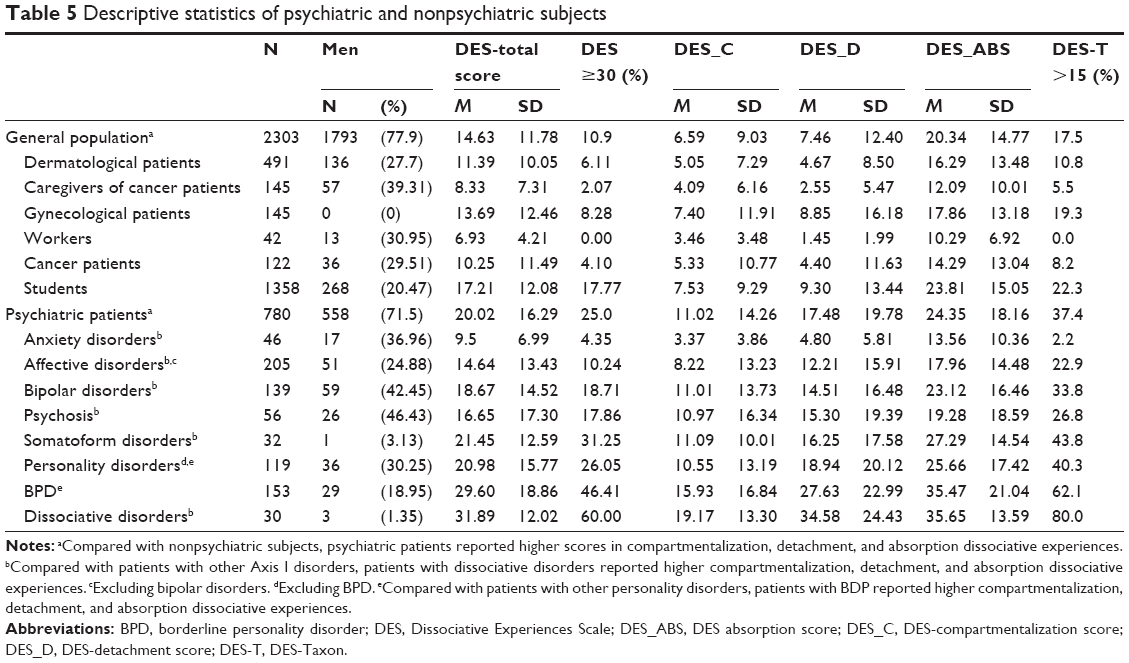 | Table 5 Descriptive statistics of psychiatric and nonpsychiatric subjects |
The correlations (Spearman’s rho) between the DES-T score and detachment and compartmentalization were 0.86 (P<0.001) and 0.70 (P<0.001), respectively. The correlations (Spearman’s rho) between the DES-total score and detachment and compartmentalization were 0.74 (P<0.001) and 0.73 (P<0.001), respectively. Other correlations are reported in Table 4.
Discussion
Our results were consistent with previous data9–12 and supported the three-factor structure of the DES, in both clinical and nonclinical samples. Furthermore, our findings showed that two of these DES factors adequately reflected detachment and compartmentalization dissociative experiences. In our study, the factor analysis results overlap with those from the expert classification procedure: six of nine items (items 3, 4, 5, 6, 8, and 9; eg, “Found new things among belongings, but not remembering buying them”) for compartmentalization factor and five of seven items (items 7, 11, 12, 13, and 28; eg, “Felt and watched self as if looking at another person”)for detachment factor. Furthermore, twelve items with a percentage of experts agreement <85 have been also caught by CFA as nonpathological absorption.
Factor analyses and expert classification are consistent with recent theoretical approaches and previous suggestions that dissociative experience can be divided into pathological and nonpathological experiences and that pathological dissociation can be classified into detachment and compartmentalization symptoms.5,6 Moreover, positive correlation exists between pathological dissociation as measured by DES-T, regardless of psychiatric diagnosis, and detachment and compartmentalization dimensions.
Consistent with previous data,5,8,33,34 in our patients’ sample, the DES-compartmentalization and DES-detachment mean scores showed differences between diagnostic groups. For example, in agreement with Zanarini et al,34 patients with borderline personality disorder reported higher dissociative experiences (both pathological and nonpathological symptoms) than patients with other personality disorders. Furthermore, in-line with previous data,8 our findings showed that, although dissociative experiences are widely represented in all diagnostic categories, they are higher in patients with dissociative disorders. All these results lead us to consider DES as a useful clinical tool to distinguish between the different forms of dissociation.
The two forms could appear together, but it is possible that their pathogenic mechanism could be different even if overlapped and/or intertwined.5,35–37 Moreover, as stated by Brown,6 different forms of dissociative problems require different types of treatment and the “one-size-fits-all” approach implied by the unitary model of dissociation could be clinically misleading. Detachment symptoms usually benefit from grounding techniques, modulation of arousal, and prevention of detachment triggers;5,38 at the same time, compartmentalization phenomena require more complex treatment based on integration of functions and contents (ie, parts of personalities, body representation, and control).38,39
There are some limitations in generalizing the results. First, no other dissociative experiences questionnaires were used. Second, test–retest stability was not investigated. Third, psychiatric evaluation of nonpsychiatric sample was not performed. Finally, the expert opinions were shaped a priori, and this may have influenced their categorization. On the other hand, to our knowledge, this is the first study to examine the factor structure of the DES in both large psychiatric and nonpsychiatric sample, taking into account compartmentalization and detachment dissociative experiences.
Conclusion
Our results showed that DES could be a valid tool for clinicians to assess the frequency of several types of dissociative experiences, such as nonpathological dissociation and pathological dissociations, such as detachment and compartmentalization in both clinical and nonclinical settings. It provides clinicians with additional information about dissociative experiences as well as important treatment indicators.
Disclosure
The authors report no conflicts of interest in this work.
References
American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders – DSM-5. 5th ed. Arlington, TX: American Psychiatric Publishing; 2013. | ||
Cardena E, Bowman ES. Defining (structural) dissociation: a debate. J Trauma Dissociation. 2011;12(4):413–415. | ||
Spiegel D, Loewenstein RJ, Lewis-Fernandez R, et al. Dissociative disorders in DSM-5. Depress Anxiety. 2011;28(12):E17–E45. | ||
Nijenhuis ER, Van der Hart O. Dissociation in trauma: a new definition and comparison with previous formulations. J Trauma Dissociation. 2011;12(4):416–445. | ||
Holmes EA, Brown RJ, Mansell W, et al. Are there two qualitatively distinct forms of dissociation? A review and some clinical implications. Clin Psychol Rev. 2005;25(1):1–23. | ||
Brown RJ. Different types of “dissociation” have different psychological mechanisms. J Trauma Dissociation. 2006;7(4):7–28. | ||
Bernstein EM, Putnam FW. Development, reliability, and validity of a dissociation scale. J Nerv Ment Dis. 1986;174(12):727–735. | ||
van Ijzendoorn MH, Schuengel C. The measurement of dissociation in normal and clinical populations: meta-analytic validation of the Dissociative Experiences Scale (DES). Clin Psychol Rev. 1996;16(5):365–382. | ||
Carlson EB, Putnam FW, Ross CA, et al. Validity of the Dissociative Experiences Scale in screening for multiple personality disorder: a multicenter study. Am J Psychiatry. 1993;150(7):1030–1036. | ||
Ross CA, Joshi S, Currie R. Dissociative experiences in the general population: a factor analysis. Hosp Community Psychiatry. 1991;42(3):297–301. | ||
Ruiz MA, Poythress NG, Lilienfeld SO, Douglas KS. Factor structure and correlates of the dissociative experiences scale in a large offender sample. Assessment. 2008;15(4):511–521. | ||
Stockdale GD, Gridley BE, Balogh DW, Holtgraves T. Confirmatory factor analysis of single- and multiple-factor competing models of the dissociative experiences scale in a nonclinical sample. Assessment. 2002;9(1):94–106. | ||
Mazzotti E, Cirrincione R. La Dissociative Experiences Scale, esperienze dissociative in un campione di studenti italiani. [The Dissociative Experiences Scale, dissociative experiences in a sample of Italian students]. Giornale Italiano di Psicologia. 2001;(1):179–192. Italian. | ||
Bernstein IH, Ellason JW, Ross CA, Vanderlinden J. On the Dimensionalities of the Dissociative Experiences Scale (DES) and the Dissociation Questionnaire (DIS-Q). J Trauma Dissociation. 2001;2(3):101–120. | ||
Fabbri A, Bertin I, Cristante F, Colombo G. Un contributo alla standardizzazione della Dissociative Experiences Scale (DES) di Bernstein e Putnam. [A contribution to the standardization of the Dissociative Experiences Scale (DES) Bernstein and Putnam]. Boll Psicol Appl. 1996;219:39–46. Italian. | ||
Larøi F, Billieux J, Defeldre AC, Ceschi G, Van der Linden M. Factorial structure and psychometric properties of the French adaptation of the Dissociative Experiences Scale (DES) in non-clinical participants. Eur Rev Appl Psychol. 2013;63(4):203–208. | ||
Garofalo C, Velotti P, Zavatti GC, et al. On the factor structure of the Dissociative Experiences Scale: contribution with an Italian version of the DES-II. Psychiatr Psychol Klin. 2015;15(1):4–12. | ||
Olsen SA, Clapp JD, Parra GR, Gayle Beck J. Factor structure of the Dissociative Experiences Scale: an examination across sexual assault status. J Psychopathol Behav Assess. 2013;35(3):394–403. | ||
Espirito Santo H, Abreu JL. Portuguese validation of the Dissociative Experiences Scale (DES). J Trauma Dissociation. 2009;10(1):69–82. | ||
Amdur RL, Liberzon I. Dimensionality of dissociation in subjects with PTSD. Dissociation. 1996;9(2):118–124. | ||
Dunn GE, Ryan JJ, Paolo AM. A principal components analysis of the Dissociative Experiences Scale in a substance abuse population. J Clin Psychol. 1994;50(6):936–940. | ||
Ray WJ, Faith M. Dissociative experiences in a college age population: follow-up with 1190 subjects. Pers Indiv Differ. 1995;18(2):223–230. | ||
Ray WJ, June K, Turaj K, Lundy R. Dissociative experiences in a college age population: a factor analytic study of two dissociation scales. Pers Indiv Differ. 1992;13(4):417–424. | ||
First MB, Spitzer RL, Gibbon M, Williams JBW. Structured Clinical Interview for DSM-IV Axis I Disorders-Patient Version (SCID-I/P). New York: New York Psychiatric Institute, Biometrics Research Department; 1996. | ||
First MB, Gibbon M, Spitzer RL, Williams JBW, Benjamin LS. Structured Clinical Interview for DSM-IV Axis II Personality Disorders, (SCID-II). Washington, DC: American Psychiatric Press, Inc.; 1997. | ||
Steinberg M. Interviewer’s Guide to the Structured Clinical Interview for DSM-IV Dissociative Disorders (SCID-D). Washington, D.C.: American Psychiatric Press; 1994. | ||
Waller NG, Putnam FW, Carlson EB. Types of dissociation and dissociative types: a taxometric analysis of dissociative experiences. Psychol Methods. 1996;1(3):300–321. | ||
Ogawa JR, Sroufe LA, Weinfield NS, Carlson EA, Egeland B. Development and the fragmented self: longitudinal study of dissociative symptomatology in a nonclinical sample. Dev Psychopathol. 1997;9(4):855–879. | ||
Modestin J, Erni T. Testing the dissociative taxon. Psychiatry Res. 2004;126(1):77–82. | ||
Muthén B, Muthén L. Mplus User’s Guide. Sixth Edition. Los Angeles, CA; 2010. | ||
Kline RB. Principles and Practice of Structural Equation Modeling. 2nd Edition ed. New York: The Guilford Press; 2005. | ||
David A Kenny. Measuring Model Fit. [webpage on the Internet]. 2015. Available from: http://davidakenny.net/cm/fit.htm. Accessed 27 April 2016. | ||
Simeon D, Knutselska M, Nelson D, Guralnik O, Schmeidler J. Examination of the pathological dissociation taxon in depersonalization disorder. J Nerv Ment Dis. 2003;191(11):738–744. | ||
Zanarini MC, Ruser TF, Frankenburg FR, Hennen J, Gunderson JG. Risk factors associated with the dissociative experiences of borderline patients. J Nerv Ment Dis. 2000;188(1):26–30. | ||
Farina B, Liotti G. Does a dissociative psychopathological dimension exist? A review on dissociative processes and symptoms in developmental trauma spectrum disorders. Clin Neuropsychiatry. 2013;10(1):11–18. | ||
Schore AN. Attachment trauma and the developing of right brain: origin of pathological dissociation. In: Dell P, O’Neil JA, eds. Dissociation and Dissociative Disorders: DSM-V and Beyond. New York: Routledge; 2009:107–141. | ||
Lanius RA, Vermetten E, Loewenstein RJ, et al. Emotion modulation in PTSD: clinical and neurobiological evidence for a dissociative subtype. Am J Psychiatry. 2010;167(6):640–647. | ||
Ogden P, Minton K, Pain C. Trauma and the Body. New York: Norton; 2006. | ||
Van der Hart O, Nijenhuis E, Steele K. The Haunted Self: Structural Dissociation and the Treatment of Chronic Traumatization. New York, London: Norton; 2006. |
 © 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2016 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.