Back to Journals » Nature and Science of Sleep » Volume 17

Is Sham Acupuncture Equally Effective for Primary Insomnia? A Bayesian Network Meta-Analysis
Authors Wang Y, Wu M ![]() , Zhang J, Li X, Yu D, Su Y, Wei X, Zhu L
, Zhang J, Li X, Yu D, Su Y, Wei X, Zhu L ![]()
Received 24 May 2025
Accepted for publication 26 July 2025
Published 29 August 2025 Volume 2025:17 Pages 1997—2012
DOI https://doi.org/10.2147/NSS.S541797
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Ahmed BaHammam
Yuting Wang,1 Minmin Wu,2 Jiongliang Zhang,1 Xinyue Li,1 Donghui Yu,1 Yumeng Su,1 Xiangyu Wei,1 Luwen Zhu2,3
1Second Clinical Medical College, Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, People’s Republic of China; 2Rehabilitation Center, The Second Affiliated Hospital of Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, People’s Republic of China; 3Heilongjiang Provincial Key Laboratory of Brain Function and Neurorehabilitation, Heilongjiang University of Chinese Medicine, Harbin, Heilongjiang, People’s Republic of China
Correspondence: Luwen Zhu, Heilongjiang University of Chinese Medicine, 24 Heping Road, Xiangfang District, Harbin, Heilongjiang, 150000, People’s Republic of China, Email [email protected]
Purpose: To compare the efficacy differences between acupuncture and sham acupuncture in adult primary insomnia through Bayesian network meta-analysis, analyze the impact of different types of sham acupuncture on efficacy, and explore the basis for the control setting.
Methods: A literature search of seven databases, including PubMed and Embase, until April 23, 2025, included randomized controlled trials (RCTs) comparing AT with noninvasive sham acupuncture (NISA), superficial acupuncture (SA), and non-acupuncture therapy (NAT) for treating PI in adults. The statistical analyses were conducted using R (version 4.4.1) and Stata (version 15.1). The protocol was registered with the International Prospective Register of Systematic Reviews (CRD420251012912).
Results: This meta-analysis incorporated 33 RCTs encompassing 3004 participants, with most studies originating from China. The results showed that at the treatment endpoint and after 4 weeks, AT significantly improved subjective sleep quality (Pittsburgh Sleep Quality Index, PSQI) compared to SA and NISA, exceeding the minimum clinically important difference (MCID: 2.5 points). Specifically, at the endpoint, AT vs SA (MD: − 3.66; 95% CI: − 4.48 to − 2.84) and AT vs NISA (MD: − 4.35; 95% CI: − 5.67 to − 3) were significant, while differences among SA, NISA, and NAT were not. Based on the surface under the cumulative rank curve (SUCRA), AT ranked first (99.9%), followed by SA (47.8%), NAT (31.9%), and NISA (20.4%). No significant differences were found between AT, NISA, and SA regarding objective sleep parameters.
Conclusion: AT significantly improved subjective sleep quality in patients with PI, though its impact on objective sleep measures was limited. When designing RCTs of acupuncture for PI, NISA is recommended as the sham acupuncture control. However, due to geographical limitations, the study results may be difficult to generalize. Future research should focus on monitoring objective sleep parameters and conducting international, multicenter RCTs involving diverse cultural populations.
Keywords: primary insomnia, sham acupuncture, acupuncture therapy, Bayesian network meta-analysis, randomized controlled trial
A Letter to the Editor has been published for this article.
A Response to Letter by Dr Zhao has been published for this article.
Graphical Abstract:

Introduction
Insomnia is a clinical syndrome characterized by dissatisfaction with the duration or quality of sleep, usually accompanied by at least three months of difficulty falling asleep and sleep maintenance disorders. It is characterized by frequent awakening or difficulty falling asleep again after awakening and triggers daytime dysfunction such as daytime sleepiness or hyperarousal.1 Many factors can affect sleep, including psychological factors, such as anxiety and depression, and unhealthy lifestyle habits, such as caffeine or nicotine abuse.2–4 Primary insomnia (PI) is a type of insomnia that is not attributable to other identifiable medical, psychiatric, or psychological conditions5,6 and is not only strongly associated with a wide range of physical illnesses and psychiatric problems (especially depressive disorders) but also significantly increases the public health burden, while simultaneously leading to lower work productivity, higher absenteeism, and an increase in transportation accidents.4,7,8 Clinical data indicate that insomnia is an independent risk factor for suicide.9 Conventional treatments for insomnia include both pharmacological and non-pharmacological treatments. Although medication is effective in the short term, it is not recommended for long-term use due to its various adverse effects.10 Contrastingly, acupuncture, a time-honored and safe non-pharmacological therapy used in China for more over 4000 years, has been used since early times to treat sleep problems. As the international interest in acupuncture research continues to grow, evidence-based research on acupuncture is also evolving. Randomized controlled trials (RCTs), the first level of evidence in evidence-based medicine, are regarded as the “gold standard” for evaluating the efficacy of clinical interventions and, therefore, a large number of RCTs have recently investigated the treatment of insomnia with acupuncture.
However, some recently published international acupuncture research articles have concluded that there is no significant difference in efficacy between acupuncture and sham-acupuncture controls.11 One study concluded that the efficacy of acupuncture was equivalent to a placebo effect,12 which has prevented universal recognition of the efficacy of acupuncture. This phenomenon may be explained by the need for inert sham acupuncture controls in RCTs to exclude non-specific efficacy, such as the placebo effect, and thus to more clearly assess the net effect of acupuncture.13 However, some researchers have suggested that sham acupuncture is not completely inert and that the control group may have some physiological and psychological responses14,15 which may lead to false-negative results in RCTs with sham acupuncture controls.13 Therefore, the use of sham acupuncture controls in the design on acupuncture RCTs remains controversial.
Additionally, the choice of sham needling method for control use is a major challenge. Currently, the two commonly used main methods of sham needling are noninvasive sham acupuncture (NISA) and superficial acupuncture (SA). NISA primarily employs nested sliding blunt-tip needles, the most widely recognized of which are the Streitberger16 and Park17 devices, while SA is performed by slightly piercing the surface of the skin to avoid eliciting the “Deqi” sensation (also known as minimal acupuncture). Therefore, identifying the differences between NISA and SA to determine which method is more appropriate as a sham acupuncture control is important for optimizing the design of future acupuncture studies.
Based on the above, this study aimed to quantitatively assess both subjective sleep quality and objective sleep indicators in patients with PI via Bayesian network meta-analysis (NMA) and to investigate the rationale for including sham acupuncture controls in acupuncture research. Furthermore, by comparing the therapeutic effects of NISA and SA, we aimed to determine the most suitable sham acupuncture method, providing a scientific basis and comprehensive reference for designing future trials.
Methods
This NMA complies with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) statement18,19 and the Cochrane Collaboration Handbook,20 (Supplementary Table S1). The protocol for this study was registered with the International Prospective Register of Systematic Reviews (CRD420251012912).
Data Sources and Search Strategy
Two independent reviewers (YT-W and JL-Z) searched PubMed, the Cochrane Central Register of Controlled Trials, Web of Science, Embase, China Biomedical Literature Service System (SinoMed), China National Knowledge Infrastructure (CNKI), and Wanfang databases from inception to December 26, 2024, and updated the search on April 23, 2025.
The search strategy incorporated a combination of MeSH terms and free words, with searches appropriately tailored to each database. To ensure comprehensiveness and minimize publication bias, we also searched the gray literature through ProQuest Dissertations & Theses Global, conference proceedings, and preprint servers (eg, bioRxiv, medRxiv). Additionally, we manually screened the references of the included studies and related reviews to prevent the omission of relevant literature.
Retrieve keywords: (“Sleep Initiation and Maintenance Disorders”[MeSH Terms] OR (“Sleep Initiation and Maintenance Disorders” OR “agrypnia” OR “awakening early” OR “Chronic Insomnia” OR “Disorders of Initiating and Maintaining Sleep” OR “Early Awakening” OR “hyposomnia*” OR “insomnia disorder*” OR “insomnia*” OR “insomnia chronic” OR “insomnia primary” OR “insomnia psychophysiological” OR “insomnia rebound” OR “insomnia transient” OR “Nonorganic Insomnia” OR “Primary Insomnia” OR “Psychophysiological Insomnia” OR “Rebound Insomnia” OR “sleep initiation and maintenance disorder*” OR “sleep initiation dysfunction*” OR “Sleeplessness” OR “Transient Insomnia”)) AND (“Acupuncture”[MeSH Terms] OR (“Acupuncture” OR “Pharmacopuncture” OR “acupuncture therapy”)) AND (“Randomized Controlled Trial”[Publication Type] OR ((“Randomized Controlled Trial” OR “controlled clinical trial” OR “randomized” OR “randomised” OR “placebo” OR “randomly” OR “trial” OR “groups”) NOT “animals”)). The detailed search strategies are presented in Supplementary Table S2.
Eligibility Criteria
This study developed the inclusion and exclusion criteria based on the PICOS framework.
Inclusion criteria:
1) Adults (>18 years) diagnosed with insomnia according to the Diagnostic and Statistical Manual of Mental Disorders (DSM)-3-R21 DSM-4,22 DSM-4-TR,23 DSM-5,24 International Classification of Sleep Disorders (ICSD)-3,1 Chinese Classification of Mental Disorders (CCMD)-3,25 or other standardized criteria;
(2) The interventions included were limited to acupuncture;
(3) The control group received NISA, SA, or non-acupuncture therapy (NAT), with NISA consisting mainly of the use of sham acupuncture devices, such as the Streitberger device or the Park device, and NAT consisting mainly of waiting lists or usual care;
(4) Outcome indicators included at least one of the following:
- Subjective sleep quality, assessed using the Pittsburgh Sleep Quality Index (PSQI);26
- Objective sleep parameters, including total sleep time (TST), sleep efficiency (SE), and wake-after-sleep-onset (WASO) measured using polysomnography (PSG) or actigraphy;
(5) To reduce bias, improve internal validity, enhance comparability between studies, and ensure the validity of the combined analysis, we included only RCTs published in Chinese or English.
Exclusion criteria:
- Participants with secondary insomnia (ie, insomnia due to mental or physical comorbidities or due to substances such as drugs or alcohol), eg, insomnia caused by disorders such as major depressive disorder, major anxiety disorder, obstructive sleep apnea, and restless legs syndrome;
- Use of methods other than NISA or SA as sham acupuncture controls (eg, transcutaneous laser or transcutaneous electrical stimulation);
- Assessed the effects of acupuncture therapy (AT) in combination with other treatments not applied to the control group;
- Continuous use of sedative-hypnotic drugs during the study period;
- Clinical trials that were in the registration phase of the trial protocol and not yet formally started.
Risk of Bias (ROB) Assessment
The Cochrane Collaboration tool version 220 was used to assess ROB in the included RCTs. This tool evaluates ROB in six domains: randomization process, deviations from the intended interventions, missing outcome data, outcome measurement, selective reporting of results, and overall bias. Each domain was rated as having a low, unclear or moderate, or high ROB. Two investigators (YT-W and JL-Z) performed the ROB assessment. A third investigator (MM-W) was consulted if conflicts arose regarding the assessments.
Study Selection and Data Extraction
All the retrieval results were exported to EndNote 21, where a combination of automated and manual methods was employed to identify duplicate entries within the search results. Duplicate records were removed, and the titles and abstracts were reviewed to exclude studies that did not meet the inclusion criteria. Full texts were searched and reviewed to determine the final included studies. Two investigators (YT-W and JL-Z) performed the screening process. Any conflicts were resolved through discussion with a third investigator (MM-W). Eligible studies were subjected to standardized data extraction using an Excel spreadsheet. The extracted information included (1) first author; (2) publication year; (3) country; (4) sample size; (5) demographic characteristics (age, sex, duration of disease); (6) intervention protocols including timing, frequency, and dosage; (7) diagnostic criteria; (8) follow-up; (9) outcome indicators; and (10) details of acupuncture intervention. Data were independently extracted by two researchers (YT-W and JL-Z). The consistency of the extraction results was evaluated using Cohen’s kappa (κ). A κ value greater than 0.7 indicates good consistency, and deemed the data reliable for inclusion. Any conflicts were addressed through discussion with a third investigator (MM-W). If the data were ambiguous, the authors were contacted via email.
Data Synthesis and Statistical Analysis
A statistical model based on a Bayesian framework was developed using the JAGS software (gemtc 0.8–2 and rjags 4–10 packages) in R (4.4.1; RStudio, Boston, MA, USA). To determine the effect size, mean difference (MD), and 95% credible interval (CI) were calculated for the continuous data. Given the clinical heterogeneity (such as different durations and frequencies of acupuncture treatments and the location of the acupuncture site) of the included trials, all NMAs were conducted using a random-effects model.27 Four Markov chains were set up for each result, each running 50,000 iterations, with 20,000 iterations discarded as the burn-in period.28 Surface under the cumulative rank curve (SUCRA) was employed to estimate the relative ranks of the different interventions for each relevant result.29 A higher SUCRA value corresponds to a higher rank in the intervention.29 Additionally, the deviance information criterion (DIC) was employed to compare the consistency and inconsistency models. A difference of less than 5 points in DIC indicated satisfactory consistency; therefore, the consistency model was selected.30 Subjective sleep outcomes (treatment endpoints and follow-up) were examined using a Network Meta-regression analysis (NMR) to determine whether any other factors could have altered the treatment effect. The NMR covariates included the year of publication, sample size, and number of treatment sessions. The NMR results are presented as regression coefficients (beta) with corresponding 95% CI. If a covariate’s 95% CI excludes zero, then there is >95% probability that the covariate exerts a statistically significant influence on the outcome measures.27 Transitivity was evaluated using descriptive statistics from the studies and population baselines. Heterogeneity was assessed using the I² test, where an I² value of less than 50% was considered acceptable level of heterogeneity, and the robustness of the results was tested by excluding studies with a high ROB for sensitivity analyses. Funnel plots and Egger’s tests were used to assess the publication bias. Network plots for NMA, funnel plots, and SUCRA line plots were produced using Stata (version 15.1; StataCorp, College Station, Texas, USA).
Quality of Evidence Assessment
The quality of evidence for effect estimates was assessed using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework.31,32 First, the ROB, inconsistency, indirectness, and publication bias of the direct estimates were assessed. Subsequently, the certainty of evidence for the indirect estimate was evaluated by considering the lowest ratings of the two direct comparisons that formed the most dominant first-order loop and intransitivity. The certainty of evidence for the NMA estimates was assessed by choosing the highest between direct and indirect ratings and examining incoherence and imprecision. The certainty of the evidence was judged as high, moderate, low, or very low for each outcome comparison.
Results
Results of Study Selection
Of the initially identified 6786 articles, 1986 were excluded as duplicates, three were marked as ineligible by EndNote, and 4754 were excluded based on unsuitable titles and abstracts. A full-text search was performed on the remaining 43 articles, of which 10 did not meet the inclusion criteria: 5 had non-compliant interventions, 3 had a non-compliant trial design, and 2 were unable to obtain the required data (Supplementary Table S3). The secondary search identified no additional articles that met the inclusion criteria. Ultimately, 33 RCTs were included.33–65 Figure 1 presents the PRISMA flowchart.
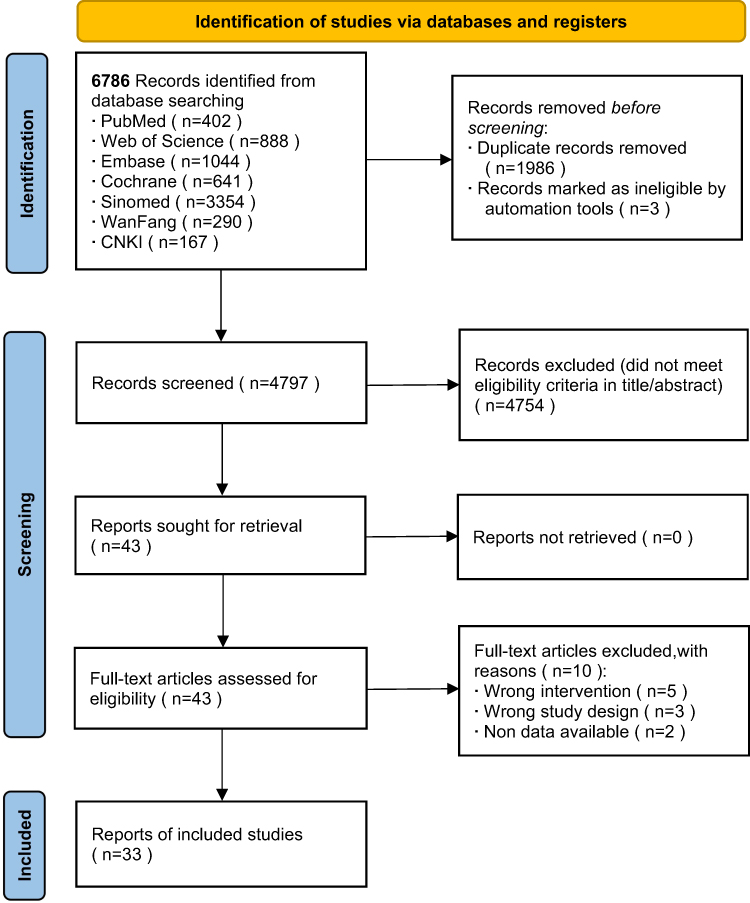 |
Figure 1 PRISMA flowchart for the study selection. Notes: PRISMA figure adapted from Hutton B, Salanti G, Caldwell DM, Chaimani A, Schmid CH, Cameron C, Ioannidis JP, Straus S, Thorlund K, Jansen JP, Mulrow C, Catalá-López F, Gøtzsche PC, Dickersin K, Boutron I, Altman DG, Moher D. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015 Jun 2;162(11):777–84.18 |
Basic Information
Thirty-three RCTs33–65 involving 3004 patients were included and published between 2009 and 2024, with the vast majority conducted in China and only one in Korea.41 Regarding the control group settings, 9 studies compared AT with NISA,34–36,40,43,48,51,52,59 22 studies compared AT with SA,33,37–39,42,44–47,49,50,53–58,61–64 1 three-armed study compared AT, NISA, and NAT,41 and 1 study compared AT and NAT.60 Regarding acupuncture methods, 13 studies utilized electroacupuncture33,34,41,44,46–49,53,60,61,63,65 and 20 studies employed manual acupuncture.35–40,42,43,45,50–52,54–59,62 In terms of outcome indicators, 31, 7, 5, and 4 studies assessed subjective sleep quality using the PSQI,33–35,37–47,49–65 TST using PSG or actigraphy,34,36,37,45,48,64,65 objectively evaluated SE,34,36,45,48,65 and objective assessments of WASO,34,45,48,65 respectively. Regarding the time point, 31 studies provided PSQI scores at the end of treatment,33–35,37–47,49–65 and 12 studies provided PSQI scores at four-week follow-up.35,41–43,49–51,53,54,57,59,62 Detailed demographic and intervention data are shown in Supplementary Tables S4 and S5.
ROB Assessment
Four studies (12.1%) did not report specific random sequence generation methods; therefore, they were considered a high ROB in randomization. Since 2 studies (6.1%) had a control group receiving usual care, it was impossible to blind the participants. Therefore, they were considered to have the same concerns regarding intervention allocation. Seven studies (21.2%) did not report the blinding of outcome assessors and data analysts, and were therefore considered to have some concerns regarding the measurement of outcomes (Figure 2). According to the ROB assessment, 20 (60.6%), 9 (27.3%), and 4 (12.1%) studies exhibited low, moderate, and high ROB, respectively (Supplementary Figure S1).
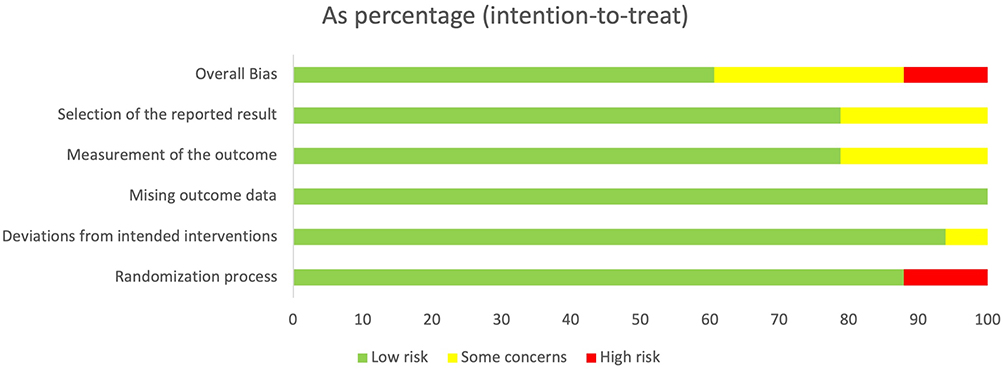 |
Figure 2 Risk of bias assessment. Notes: ROB figure adapted from Higgins JP, Altman DG, Gøtzsche PC, Jüni P, Moher D, Oxman AD, Savovic J, Schulz KF, Weeks L, Sterne JA; Cochrane Bias Methods Group; Cochrane Statistical Methods Group. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011 Oct 18;343:d5928.20 |
Network Meta-Analysis
Subjective Sleep Quality
At the end of treatment, 31 studies assessed subjective sleep quality using the PSQI (Figure 3A). Figure 3B presents the main results of the NMA. Compared with SA (MD: −3.66; 95% CI: −4.48, −2.84) and NISA (MD: −4.35; 95% CI: −5.67, −3), AT significantly improved the subjective sleep quality of patients with PI, and the results were clinically significant. The difference between SA and NAT was not significant (MD, −0.42; 95% CI, −3.19, 2.33), as was the difference between NISA and NAT (MD, 0.27; 95% CI, −2.52, 3.01). When comparing SA with NISA, SA (MD: −0.69; 95% CI: −2.24, to 0.89) showed no significant difference between the two groups. The funnel plot and Egger’s test yielded p = 0.63, indicating no evidence of publication bias (Supplementary Figure S2). The SUCRA plot showed that AT was ranked first (99.9%), followed by SA (47.8%), NAT (31.9%), and NISA (20.4%) (Figure 4). In the sensitivity analysis, the exclusion of four studies35,49,54,60 with a high risk of bias had no significant impact on the results (Supplementary Table S6).
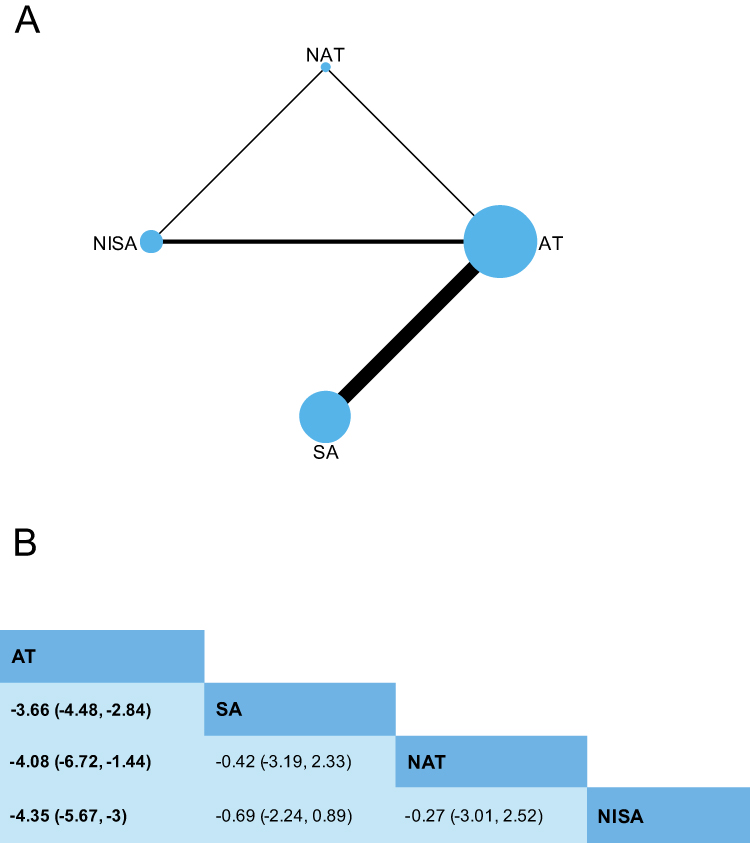 |
Figure 3 Network plot and league table for PSQI at treatment endpoint. (A) Network plot for PSQI at treatment endpoint. Node (circle) sizes indicate the number of studies, and edge (line) widths represent the number of direct comparisons. (B) League table for PSQI at treatment endpoint. Estimates are presented as mean difference (MD) and 95% credible intervals (CI). Comparisons between treatments should be read from left to right. The estimate of intervention effectiveness is located at the intersection of the column-defining intervention and the row-defining intervention. Significant results are presented in bold. Abbreviations: AT, Acupuncture Therapy; SA, Superficial Acupuncture; NISA, Non-Invasive Sham Acupuncture; NAT, Non-acupuncture Therapy. |
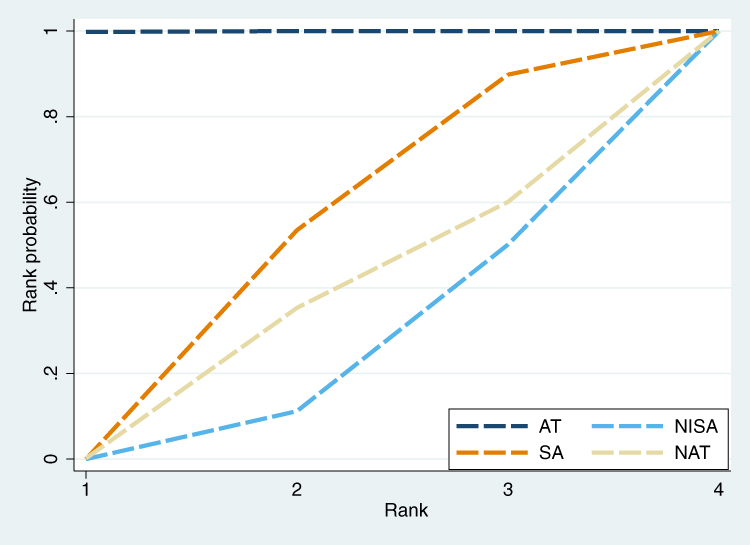 |
Figure 4 SUCRA plot for PSQI at treatment endpoint. SUCRA is a numeric presentation of the overall ranking and presents a single number associated with each treatment. SUCRA values range from 0 to 1. The higher the SUCRA value, and the closer to 1, the higher the likelihood that a therapy is in the top rank or one of the top ranks; the closer to 0 the SUCRA value, the more likely that a therapy is in the bottom rank, or one of the bottom ranks. Abbreviations: AT, Acupuncture Therapy; SA, Superficial Acupuncture; NISA, Non-Invasive Sham Acupuncture; NAT, Non-acupuncture Therapy. |
At the four-week follow-up, 12 studies assessed subjective sleep quality (Supplementary Figure S3A). The results presented in Supplementary Figure S3B demonstrate that AT exhibits a significant and clinically meaningful correlation with improved subjective sleep quality when compared to SA (MD: −4.21; 95% CI: −6.14, −2.3) and NISA (MD: −5.44; 95% CI: −7.63, −3.15). Compared with NAT, there were no significant differences in SA (MD: −0.75; 95% CI: −5.64, 4.14) and NISA (MD: 0.45; 95% CI: −4.08, 4.95). Compared with NISA, SA (MD: −1.22; 95% CI: −4.13, 1.78) showed no significant difference. The p-value of the Egger’s test was 0.012, and the funnel plot displayed slight asymmetry, indicating possible publication bias (Supplementary Figure S4). According to the SUCRA plot, AT was the highest (99.4%), followed by SA (48%), NAT (32.6%), and finally NISA (20%) (Supplementary Figure S5). In the sensitivity analysis, after excluding 3 studies35,49,54 with a high risk of bias, the results of AT vs NAT changed from (MD: −4.96; 95% CI (−9.46, −0.45) to (MD: −4.97; 95% CI (−10.42, 0.48), with no significant changes in the remaining results (Supplementary Table S7).
Objective Sleep Parameters
TST
Compared with subjective sleep quality, fewer studies have assessed objective sleep parameters. Seven studies evaluated TST at the treatment endpoint (Supplementary Figure S6A). Supplementary Figure S6B shows the main results of the NMA, which indicated that AT did not significantly prolong the TST in patients with PI comparedwith NISA (MD: 31.03; 95% CI: −7.61, 70.99) and SA (MD: 24.38; 95% CI: −14.27, 58.9). There was no significant difference between NISA and SA (MD: 6.62; 95% CI: −43.93, 63.01). The funnel plot and Egger’s test yielded a p = 0.91, indicating no evidence of publication bias (Supplementary Figure S7). The SUCRA plot showed that AT ranked first (93.4%), followed by SA (35.3%), and NISA (21.3%) (Supplementary Figure S8).
SE
At the treatment endpoint, 5 studies assessed SE (Supplementary Figure S9A). Supplementary Figure S9B shows the main results of the NMA, which indicated that AT did not significantly improve SE in patients with PI compared to NISA (MD: 0.38; 95% CI: −14.22, 15.05) and SA (MD: 4.44; 95% CI: −3.42, 12.98). Compared with NISA, SA (MD: 4.06; 95% CI: −12.44, 21.09) showed no significant difference. The Egger’s test found p = 0.013, and the funnel plot displayed slight asymmetry, indicating possible publication bias (Supplementary Figure S10). The SUCRA plot showed that AT ranked first (91.6%), followed by NISA (43%), and finally SA (15.4%) (Supplementary Figure S11).
WASO
Four studies assessed WASO at the treatment endpoint (Supplementary Figure S12A). Supplementary Figure S12B shows the main results of the NMA, which indicated that AT did not significantly shorten the wake-after-sleep-onset in patients with PI compared with NISA (MD, −4.9; 95% CI (−54.49, 43.07) and SA (MD, −37.2; 95% CI, −90.36, 13.84). Compared with SA, NISA (MD: −32.04; 95% CI: −103.28, 39.07) showed no significant difference. The funnel plot and Egger’s test yielded a p = 0.13, indicating no evidence of publication bias (Supplementary Figure S13). The SUCRA plot showed that AT ranked first (79.2%), followed by NISA (61.3%) and SA (9.6%) (Supplementary Figure S14).
Consistency, Heterogeneity, and Transitivity Assessment
For overall consistency, the DIC was used to compare the consistency and inconsistency models. The changes in all existing closed-loop models were less than 5 points, indicating favorable overall consistency based on the DIC. For local consistency, the node-splitting method was employed to test the results, and no local inconsistencies were found (p > 0.05). The overall level of heterogeneity was tested using the I² test, and the results indicated that the overall level of heterogeneity was low (I² < 50%). In the meta-regression analysis, the covariates (publication year, sample size, and number of treatment sessions) did not significantly affect the results (Supplementary Tables S8 and S9). Furthermore, according to descriptive statistical data, the included trials had acceptable transitivity.
Quality of Evidence Assessment
At the treatment endpoint, the quality of direct evidence for subjective sleep quality measured using the GRADE criteria ranged from “high” to “low”. The primary reasons for downgrading were the presence of bias risk, imprecision, or both. The quality of the indirect evidence for subjective sleep quality estimated by the NMA was “moderate” or “low”, with the primary reason for further downgrading being imprecision in the NMA effect estimates (Supplementary Table S10). The quality of direct evidence for objective sleep parameters (TST and WASO) measured using the grade was rated as “moderate”, with the downgrade primarily due to imprecision. The quality of indirect evidence for TST and WASO estimated by the NMA was “moderate” or “low”, with the primary reason for further downgrading being imprecision in the NMA effect estimates (Supplementary Tables S11 and S12). The quality of direct evidence for SE in objective sleep parameters was rated as “low”, primarily because of imprecision and publication bias. The quality of the indirect evidence for SE from the NMA was rated as “very low”, primarily because of the imprecision in the NMA effect estimates (Supplementary Table S13). At the four-week follow-up, the quality of direct evidence for subjective sleep quality measured using the GRADE criteria was rated as “moderate” to “very low”, with downgrading primarily due to risks of bias, publication bias, and imprecision. The quality of the indirect evidence for subjective sleep quality estimated by the NMA was rated as “very low”, with the primary reason for further downgradation being the imprecision in the NMA effect estimates (Supplementary Table S14).
Discussion
This study used PI as an example and employed Bayesian NMA to systematically evaluate the effects of two sham acupuncture methods, NISA and SA, on subjective and objective sleep indicators during AT. Although several high-quality systematic reviews and meta-analyses have examined the efficacy of acupuncture for PI,66–70 this study revealed the potential impact of sham acupuncture method selection on treatment outcomes, providing important insights for acupuncture trial design and evidence-based guidance for future trial protocols.
Although acupuncture has a long history of empirical application, early studies often lacked rigorous, objective assessment methods, such as polysomnography (PSG), functional magnetic resonance imaging (fMRI), and multi-omics analysis. In recent years, these technologies have allowed researchers to explore the mechanisms underlying acupuncture treatment for insomnia in greater depth. For instance, Yukai Wang et al used PSG to determine that acupuncture enhances non-rapid eye movement (NREM)-3 stage and rapid eye movement (REM) sleep in insomnia patients, thereby improving deep sleep.65 Research by Xuke Han et al71 confirmed that acupuncture reduces the excessive release of cortisol and corticotropin-releasing hormone (CRH) by inhibiting the hyperactive hypothalamic-pituitary-adrenal (HPA) axis. They also found that HPA axis inhibition is associated with enhanced deep sleep.72,73 Gihyun Lee et al discovered that acupuncture regulates the electrophysiological activity of the locus coeruleus (LC) in a rat model of insomnia. The LC is the main site of norepinephrine (NE) secretion in the brain,74 and Oxana Eschenko et al have shown that LC-NE neurons are active during wakefulness and quiescent during sleep, especially REM sleep.75,76 Zhaoyi Chen et al further used fMRI to reveal that acupuncture may improve patients’ sleep by regulating LC functional activity.64 These findings collectively suggest that acupuncture may exert its specific therapeutic effects through a multi-target regulatory mechanism.
The current NMA indicated that AT outperformed SA and NISA at the treatment endpoint and four-week follow-up, demonstrating its superiority in enhancing subjective sleep quality in patients with PI. This finding aligns with existing meta-analyses on acupuncture for PI that support the superiority of acupuncture over sham acupuncture in enhancing subjective sleep quality.66,67,70 The NMR results showed that covariates (publication year, sample size, and total number of treatments) did not significantly affect the results. First, this implies that between 2009 and 2024, the difference in efficacy between acupuncture and sham acupuncture remained stable, unaffected by the standardization of acupuncture procedures or updates to diagnostic criteria. Second, small-sample RCTs did not systematically overestimate the efficacy of acupuncture. Third, the efficacy remained stable across the number of treatment sessions within the clinically applicable range, despite the fact that the number of treatment sessions included in our study ranged from 6 to 24. Sensitivity analysis, which excluded studies with a high risk of bias, showed no significant differences in outcomes at the treatment endpoint. However, at the four-week follow-up, the AT versus NAT results changed, though the overall level of heterogeneity did not significantly change. One possible reason for this phenomenon is that, after excluding three studies through sensitivity analysis, only nine studies that reported follow-up results remained, and only one study compared AT with NAT. This reduction in sample size may have compromised the statistical power and affected the results.77 Furthermore, follow-up results are at risk of publication bias, and studies with a high risk of bias are more likely to publish positive results.78,79 Thus, excluding such studies reduces bias and may yield results closer to the actual situation. After sensitivity analysis, the main results (AT vs SA, AT vs NISA, and SA vs NISA) remained robust, and we consider the follow-up results to be reliable.
For objective sleep parameters, the therapeutic effects of AT were not statistically significant compared to NISA and SA. This discrepancy between subjective and objective assessment results has also been observed in previous studies.67,80 However, the finding that acupuncture did not significantly improve objective sleep parameters in PI patients should be interpreted with caution. The reasons are as follows: First, while 33 studies assessed subjective sleep quality, only four to seven studies reported objective sleep parameters. The limited sample size could potentially influence the outcomes.77 Second, after reviewing the original studies, it was found that the AT group showed improvements in objective sleep parameters at the treatment endpoint compared to baseline. However, these improvements were not statistically significant when compared to the SA and NISA groups. This may be related to the potential nonspecific effects of sham acupuncture, which may be amplified when sample sizes are insufficient.81 Third, PSG measurements require a laboratory environment. However, changes in the patient’s sleeping environment can interfere with natural sleep patterns and affect the results. Additionally, insomnia patients often experience sleep state misperceptions. Subjective scales cannot quantify sleep status as well as objective indicators can. This cognitive confusion and time delay may also lead to differences between subjective and objective indicators.80,82 It is worth emphasizing that the PSQI is a widely validated self-assessment scale with high validity. It assesses sleep from seven dimensions: sleep quality, sleep latency, sleep duration, habitual sleep efficiency, sleep disturbance, use of sleeping medication, and daytime dysfunction. The total score is 21, and the MCID is 2.5.26,83 The NMA results demonstrated that AT was significantly superior to SA (MD: −3.66; 95% CI: −4.48, −2.84) and NISA (MD: −4.35; 95% CI: −5.67, −3.00) at the endpoint, with a high quality of evidence. At the four-week follow-up, AT was significantly superior to SA (MD: −4.21; 95% CI: −6.14, −2.30) and NISA (MD: −5.44; 95% CI: −7.63, −3.15), though the quality of evidence was low to moderate. These findings demonstrate clinically significant differences, indicating that acupuncture effectively improves sleep quality, reduces hypnotic drug use, and alleviates daytime functional impairments. High-quality evidence at the endpoint strongly supports this conclusion. Jia Xing et al’s research has shown that acupuncture is as effective as cognitive behavioral therapy (CBT) in improving sleep quality and mood. Additionally, acupuncture improves daytime functioning more quickly.84 The four-week follow-up results confirmed acupuncture’s short- and medium-term efficacy, but other studies have shown that acupuncture remains significantly effective at 40 weeks.51 Furthermore, acupuncture can reduce hypnotic drug use, making it economically viable.85
Acupuncture treatment includes specific (physiological) and nonspecific (psychological) therapeutic effects. A sham acupuncture control group was set up to distinguish between the two effects.86 However, if the trial demonstrates that both acupuncture and sham acupuncture are significantly more effective than standard care, such as non-acupuncture NAT, then it suggests that sham acupuncture may produce significant specific effects. This would render it unsuitable as a control group.87 The NMA results revealed that there was no significant difference between sham acupuncture controls (NISA and SA) and NAT in improving subjective sleep quality. This indicates that these two types of sham acupuncture are feasible as control groups. However, it should be noted that only two studies involved NAT, and only subjective sleep quality was assessed without comparative results from objective indicators. Therefore, this conclusion should be interpreted with caution.
The present NMA also showed that there were no statistically significant differences in subjective sleep quality and objective sleep indicators between SA and NISA, consistent with Chenyong Liu et al’s meta-analysis results.67 However, this study used Bayesian NMA to perform a unique SUCRA ranking of SA and NISA, quantifying differences between them and making the comparison more intuitive. A higher SUCRA value indicates a stronger therapeutic effect and lower suitability as a sham acupuncture control.29 The results showed that NISA ranked higher in the SUCRA of SE and WASO (evidence quality was low to very low). Meanwhile, SA ranked higher in the SUCRA of TST, PSQI at endpoint, and PSQI at follow-up (evidence quality was moderate to very low). Notably, in the SUCRA for endpoint PSQI, NISA ranked lowest (even lower than NAT, with moderate evidence quality). Based on the results of the SUCRA and evidence quality assessments, NISA ranked lower than SA overall. Therefore, it is speculated that NISA may be the preferred sham acupuncture method in studies targeting PI. The main difference between SA and NISA lies in whether the skin is pierced. For SA, even if only 1–2 mm is pierced, it may produce a specific therapeutic effect.88,89 In addition, superficial acupuncture technique is a therapeutic acupuncture technique used according to the patient’s constitution or the nature of the disease. For example, floating needles, acupoint patches, and intradermal needles stimulate the skin surface to achieve therapeutic purposes. In contrast, NISA does not pierce the skin, providing minimal stimulation to the body and producing a weaker therapeutic effect. Furthermore, the Park and Streitberger devices ensure good blinding of patients by making the control and the experimental groups appear identical, which makes it difficult to break the blind.16,17 Previous studies have demonstrated that NISA is an effective single-blind control method.90 However, when using SA, patients can observe the circumstances of needle insertion, which may cause doubt about the treatment’s effectiveness and trigger a nocebo effect (adverse reactions caused by negative expectations about the treatment). This may affect the results.91 Therefore, when designing experiments involving diseases with superficial lesions, SA may not be a suitable sham acupuncture control because it may underestimate the efficacy of acupuncture.87 In studies requiring horizontal or oblique needling, NISA may be inapplicable due to operational limitations. SA is more suitable for use on areas that patients cannot directly observe, such as the head, neck, and back. Alternatively, patients can wear blindfolds to block their vision during treatment.
Although this NMA yielded positive results, the significant geographical concentration of the included studies suggests that these results may not apply to non-Chinese populations. Of the 33 original studies, 32 (97%) were conducted in China and only one (3%) was conducted in South Korea. This uneven geographical distribution severely limits the global applicability and external validity of the results. Karst et al pointed out in their comparative analysis of cross-cultural acupuncture trials that cultural background profoundly influences the assessment of treatment efficacy through three mechanisms: patient expectations, medical environment, and doctor attitude.92 First, Eastern and Western patients have different expectations and cultural perceptions. Chinese patients generally believe that the “sensation of Deqi” is a prerequisite for therapeutic efficacy, making them more likely to recognize the ineffectiveness of sham acupuncture. Western patients, on the other hand, may be unfamiliar with acupuncture, leading them to trust sham acupuncture more as the number of treatment sessions increases. For example, a multicenter trial by Garcia et al revealed that acupuncture was significantly more effective than sham acupuncture and standard care at the Chinese center. In contrast, at the American center, only sham acupuncture was more effective than standard care, and there was no difference between acupuncture and standard care.93 Second, the medical environment and operating procedures vary. The high prevalence of acupuncture in primary healthcare in China (community hospital coverage rate >80%)94 has prompted physicians to master more proficient “Deqi” induction techniques, which may amplify the therapeutic effects. In contrast, Western acupuncturists have less standardized practices, leading to deviations in efficacy assessments. Additionally, differences in needle types, insertion depths, and acupoint selection across regions exacerbate clinical heterogeneity. Third, acupuncturists have different attitudes towards sham acupuncture. Acupuncture treatment has a long history in China, and Chinese acupuncturists are very familiar with acupuncture techniques. Consequently, they may experience greater frustration when performing sham acupuncture, which could negatively impact the efficacy of treatment by transferring these emotions to patients. However, Western acupuncturists may perform sham acupuncture in a more neutral manner.93
Limitations
The limitations of this study are mainly as follows. The first limitation is geographic limitation. The majority of studies are from China. This fundamental constraint significantly compromises the global generalizability and external validity of the findings. The second limitation concerns the risk of bias. Four studies (12.1% of the included studies) were rated as having a high risk of bias due to inadequate reporting of randomization methods. Furthermore, potential publication bias may exist in the follow-up results. Although sensitivity analyses and meta-regression were performed to test the robustness of the primary results, the interpretation of the findings (especially those from subjective sleep quality assessments) should remain cautious, with full consideration of these potential biases. The third limitation involves the inadequate coverage and depth of objective sleep measures. While 30 studies assessed subjective sleep quality, only four to seven studies provided objective sleep parameters obtained through PSG or similar devices. This paucity of objective data diminishes the comprehensiveness of our results. More importantly, most PSG-based studies failed to report essential sleep architecture parameters, including N1%, N2%, N3%/slow-wave sleep, and REM sleep duration, thereby precluding a thorough evaluation of sleep health. The fourth limitation relates to the insufficient follow-up duration. Constrained by the original data, the analysis of subjective sleep quality was limited to the 4-week follow-up period, which only confirmed the short-to-medium term effects of acupuncture. The absence of longer-term (eg, ≥12 weeks) follow-up data precludes definitive conclusions about the sustained efficacy of both acupuncture and sham acupuncture. In view of these limitations, the following recommendations are proposed for future RCTs: (1) Implement multicenter trials involving diverse cultural populations to enhance external validity and enable more comprehensive efficacy analyses; (2) Strengthen objective sleep assessment by expanding the use of PSG and systematically reporting sleep architecture parameters (N1, N2, N3 stages, and REM duration) to address potential subjective reporting biases and establish gold-standard evidence; (3) Extend follow-up periods to facilitate a robust evaluation of long-term treatment sustainability; (4) Develop advanced sham acupuncture controls using automated or innovative technologies (eg, virtual reality-simulated acupuncture) to create truly “zero-stimulation” controls, thereby eliminating potential therapeutic effects from sham procedures and improving methodological rigor; (5) Conduct head-to-head comparative effectiveness research pitting acupuncture against standard insomnia treatments (eg, CBT) to clarify its evidence-based positioning and promote appropriate integration into modern healthcare systems.
Conclusions
This NMA indicates that acupuncture is significantly more effective than sham acupuncture in improving subjective sleep quality in patients with PI. However, its effects on objective sleep parameters require further investigation. When designing RCTs of acupuncture for PI, it is recommended that NISA be used as the sham acupuncture control group.
Data Sharing Statement
The datasets generated and analyzed during the present study are available from the corresponding author on reasonable request.
Author Contributions
All authors made significant contributions to this work, from study conception and design to data acquisition, analysis, and interpretation. Each participated in drafting and revising the manuscript, approved the final version for publication, and agreed on the submission to this journal. All authors take full responsibility for the content of this article. The individual contributions of the authors, based on the CRediT taxonomy, are as follows: Yuting Wang: Writing - original draft, Formal analysis, Data curation, Conceptualization, Writing-review & editing. Minmin Wu: Validation, Supervision, Methodology, Writing-review & editing. Jiongliang Zhang: Data curation, Methodology, Supervision, Writing-review & editing. Xinyue Li: Methodology, Supervision, Software, Writing-review & editing. Donghui Yu: Methodology, Supervision, Software, Writing-review & editing. Yumeng Su: Data curation, Formal analysis, Writing-review & editing. Xiangyu Wei: Data curation, Formal analysis, Writing-review & editing. Luwen Zhu: Supervision, Project administration, Resources, Writing-review & editing.
Funding
This work was supported by the National Natural Science Foundation of China (82174477) and Heilongiiang Key R&D Program [2022ZX06C241].
Disclosure
The authors have no relevant financial or non-financial interests to disclose.
References
1. Sateia MJ. International classification of sleep disorders-third edition: highlights and modifications. Chest. 2014;146(5):1387–1394. doi:10.1378/chest.14-0970
2. Clark I, Landolt HP. Coffee, caffeine, and sleep: a systematic review of epidemiological studies and randomized controlled trials. Sleep Med Rev. 2017;31:70–78. doi:10.1016/j.smrv.2016.01.006
3. Jaehne A, Unbehaun T, Feige B, Lutz UC, Batra A, Riemann D. How smoking affects sleep: a polysomnographical analysis. Sleep Med. 2012;13(10):1286–1292. doi:10.1016/j.sleep.2012.06.026
4. Roth T. Insomnia: definition, prevalence, etiology, and consequences. J Clin Sleep Med. 2007;3(5 Suppl):S7–10. doi:10.5664/jcsm.26929
5. Thorpy MJ. Classification of Sleep Disorders. Neurotherapeutics. 2012;9(4):687–701. doi:10.1007/s13311-012-0145-6
6. Buysse DJ. Insomnia. JAMA. 2013;309(7):706–716. doi:10.1001/jama.2013.193
7. Daley M, Morin CM, LeBlanc M, Grégoire JP, Savard J, Baillargeon L. Insomnia and its relationship to health-care utilization, work absenteeism, productivity and accidents. Sleep Med. 2009;10(4):427–438. doi:10.1016/j.sleep.2008.04.005
8. Bolge SC, Doan JF, Kannan H, Baran RW. Association of insomnia with quality of life, work productivity, and activity impairment. Qual Life Res. 2009;18(4):415–422. doi:10.1007/s11136-009-9462-6
9. Lin HT, Lai CH, Perng HJ, et al. Insomnia as an independent predictor of suicide attempts: a nationwide population-based retrospective cohort study. BMC Psychiatry. 2018;18(1):117. doi:10.1186/s12888-018-1702-2
10. De Crescenzo F, D’Alò GL, Ostinelli EG, et al. Comparative effects of pharmacological interventions for the acute and long-term management of insomnia disorder in adults: a systematic review and network meta-analysis. Lancet. 2022;400(10347):170–184. doi:10.1016/s0140-6736(22)00878-9
11. Madsen MV, Gøtzsche PC, Hróbjartsson A. Acupuncture treatment for pain: systematic review of randomised clinical trials with acupuncture, placebo acupuncture, and no acupuncture groups. BMJ. 2009;338:a3115. doi:10.1136/bmj.a3115
12. Solomon S. Acupuncture for Headache. It’s Still All Placebo. Headache. 2017;57(1):143–146. doi:10.1111/head.12975
13. Lundeberg T, Lund I, Näslund J, Thomas M. The Emperors sham - wrong assumption that sham needling is sham. Acupunct Med. 2008;26(4):239–242. doi:10.1136/aim.26.4.239
14. Lee YS, Chae Y. Powerful effects of placebo needles. Acupunct Med. 2018;36(3):197–198. doi:10.1136/acupmed-2017-011516
15. Napadow V, Dhond R, Park K, et al. Time-variant fMRI activity in the brainstem and higher structures in response to acupuncture. Neuroimage. 2009;47(1):289–301. doi:10.1016/j.neuroimage.2009.03.060
16. Streitberger K, Kleinhenz J. Introducing a placebo needle into acupuncture research. Lancet. 1998;352(9125):364–365. doi:10.1016/s0140-6736(97)10471-8
17. Park J, White A, Stevinson C, Ernst E, James M. Validating a new non-penetrating sham acupuncture device: two randomised controlled trials. Acupunct Med. 2002;20(4):168–174. doi:10.1136/aim.20.4.168
18. Hutton B, Salanti G, Caldwell DM, et al. The PRISMA extension statement for reporting of systematic reviews incorporating network meta-analyses of health care interventions: checklist and explanations. Ann Intern Med. 2015;162(11):777–784. doi:10.7326/m14-2385
19. Moher D, Hopewell S, Schulz KF, et al. CONSORT 2010 explanation and elaboration: updated guidelines for reporting parallel group randomised trials. BMJ. 2010;340:c869. doi:10.1136/bmj.c869
20. Higgins JP, Altman DG, Gøtzsche PC, et al. The Cochrane Collaboration’s tool for assessing risk of bias in randomised trials. BMJ. 2011;343:d5928. doi:10.1136/bmj.d5928
21. Cooper AM, Michels R. Diagnostic and statistical manual of mental disorders, 3rd ed. revised (DSM-III-R). Am J Psychiatry. 1988;145(10):1300–1301. doi:10.1176/ajp.145.10.1300
22. Bell CC. DSM-IV: diagnostic and statistical manual of mental disorders. JAMA. 1994;272(10):828–829. doi:10.1001/jama.1994.03520100096046
23. Segal DL. Diagnostic and statistical manual of mental disorders (DSM-IV-TR). Corsini Encycl Psychol. 2010;2010:1–3.
24. American Psychiatric Association. Diagnostic and Statistical Manual of Mental Disorders: DSM-5. American Psychiatric Association; 2013.
25. Chen Y-F. Chines Classification of Mental Disorders (CCMD-3): towards Integration in International Classification. Psychopathology. 2002;35(2–3):171–175. doi:10.1159/000065140
26. Backhaus J, Junghanns K, Broocks A, Riemann D, Hohagen F. Test-retest reliability and validity of the Pittsburgh Sleep Quality Index in primary insomnia. J Psychosom Res. 2002;53(3):737–740. doi:10.1016/s0022-3999(02)00330-6
27. Efthimiou O, Debray TP, van Valkenhoef G, et al. GetReal in network meta-analysis: a review of the methodology. Res Synth Methods. 2016;7(3):236–263. doi:10.1002/jrsm.1195
28. Brooks SP, Gelman A. General methods for monitoring convergence of iterative simulations. J Comput Graph Stat. 1998;7(4):434–455. doi:10.1080/10618600.1998.10474787
29. Veroniki AA, Straus SE, Fyraridis A, Tricco AC. The rank-heat plot is a novel way to present the results from a network meta-analysis including multiple outcomes. J Clin Epidemiol. 2016;76:193–199. doi:10.1016/j.jclinepi.2016.02.016
30. Dempster AP. The direct use of likelihood for significance testing. Stat Comput. 1997;7(4):247–252. doi:10.1023/A:1018598421607
31. Puhan MA, Schünemann HJ, Murad MH, et al. A GRADE Working Group approach for rating the quality of treatment effect estimates from network meta-analysis. BMJ. 2014;349:g5630. doi:10.1136/bmj.g5630
32. Brignardello-Petersen R, Bonner A, Alexander PE, et al. Advances in the GRADE approach to rate the certainty in estimates from a network meta-analysis. J Clin Epidemiol. 2018;93:36–44. doi:10.1016/j.jclinepi.2017.10.005
33. Xi HQ, Wu WZ, Liu CY, Wang XQ, Li JH. Effect of Tongdu Tiaoshen needling in treatment of chronic insomnia by regulating the hypothalamic-pituitary-adrenal axis. Acupuncture Res. 2020;45(7):552–556. doi:10.13702/j.1000-0607.190791
34. Yeung WF, Chung KF, Zhang SP, Yap TG, Law ACK. Electroacupuncture for primary insomnia: a randomized controlled trial. Sleep. 2009;32(8):1039–1047. doi:10.1093/sleep/32.8.1039
35. Bo D, Zeqin C, Jie MA. Clinical curative observation of applying acupuncture at Yintang (EX-HN3), Baihui (Du20) and Dazhui (Du14) with periosteal puncture method in the treatment of primary insomnia. J Sichuan Tradit Chin Med. 2018;36:176–178.
36. Yin X, Gou M, Xu J, et al. Efficacy and safety of acupuncture treatment on primary insomnia: a randomized controlled trial. Sleep Med. 2017;37:
37. Ma Y, Pang R, Teng R, Song J, Shi Y, Wu X. Effect of scalp acupuncture on sleep quality in patients with chronic insomnia. J Changchun Univ Chin Med. 2022;38(12):2023119740. doi:10.13463/j.cnki.cczyy.2022.12.014
38. Lai C-H. Clinical research on the treatment of paradoxical insomnia with acupuncture for regulating the mind and inducing sleep. Inner Mongolia J Tradit Chin Med. 2024;43(4):2024314461. doi:10.16040/j.cnki.cn15-1101.2024.04.063
39. Zhang F, Tang Q, Guo J, et al. Effects of “Old Ten Needles” acupoints group on sleep quality and excessive arousal in patients with chronic insomnia. J Tradit Chin Med. 2019;60(8):671–674. doi:10.13288/j.11-2166/r.2019.08.010
40. Zhao FY, Xu H, Hong YF, et al. Attention network function of insomniacs improved by manual acupuncture: evidence from attention network task. World J Acupunct Moxibustion. 2019;29(2):91–96. doi:10.1016/j.wjam.2019.05.006
41. Lee B, Kim B-K, Kim H-J, et al. Efficacy and safety of electroacupuncture for insomnia disorder: a multicenter, randomized, assessor-blinded, controlled trial. Nat Sci Sleep. 2020;12:1145–1159. doi:10.2147/nss.S281231
42. Li H-Q, Zou Y-H, Guo J, Wei J, Cao K-G. 30 cases of primary insomnia treated by ‘Zhou’s method of regulating the spirit and acupuncture’. Glob Tradit Chin Med. 2017;10(7):2017522119. doi:10.3969/j.issn.1674-749.2017.07.033
43. Zhang L, Tang Y, Hui R, et al. The effects of active acupuncture and placebo acupuncture on insomnia patients: a randomized controlled trial. Psychol Health Med. 2020;25(10):
44. Li J-H, Wu W-Z, Liu C-Y, et al. Effect of Tiaoshen needling on plasma melatonin and cortisol in patients with chronic insomnia. Acupuncture Res. 2021;46(8):690–694. doi:10.13702/j.1000-0607.201009
45. Jiang TF, Chen ZY, Liu J, et al. Acupuncture modulates emotional network resting-state functional connectivity in patients with insomnia disorder: a randomized controlled trial and fMRI study. BMC Complement Med Ther. 2024;24(1):311. doi:10.1186/s12906-024-04612-0
46. Wang XQ, Qin S, Wu WZ, et al. Effect of electroacupuncture on serum melatonin and dopamine in aged insomnia. Chin Acupunct Moxibustion. 2021;41(5):
47. Xi H-Q, Wu W-Z, Liu C-Y, et al. Effect of acupuncture at Tiaoshen acupoints on hyperarousal state in chronic insomnia. Acupuncture Res. 2021;41(3):263–267. doi:10.13703/j.0255-2930.20200303-k0004
48. Yeung WF, Yu BY, Yuen JW, et al. Semi-individualized acupuncture for insomnia disorder and oxidative stress: a randomized, double-blind, sham-controlled trial. Nat Sci Sleep. 2021;13:1195–1207. doi:10.2147/nss.S318874
49. Zhao Y, Wu W, Wang X, Xu Y, Jiang Y, Liu C. To observe the effect of tiaoshen acupuncture on hyperarousal in patients with chronic insomnia. Modern Tradit Chin Med Mater Med-World Sci Technol. 2021;23(07):2538–2543. doi:10.11842/wst.20200704001
50. Huo Y-S, Chen Z-Y, Yin X-J, et al. Tiaoshen acupuncture for primary insomnia: a pilot randomized controlled trial. Chin Acupunct Moxibustion. 2023;43(9):1008–1013. doi:10.13703/j.0255-2930.20221120-0001
51. Zhang L, Deng Y, Hui R, et al. The effects of acupuncture on clinical efficacy and steady-state visual evoked potentials in insomnia patients with emotional disorders: a randomized single-blind sham-controlled trial. Front Neurol. 2023;13. doi:10.3389/fneur.2022.1053642
52. Zhao FY, Zhang ZY, Xia XJ, et al. Memory response to manual acupuncture in chronic insomniacs: evidence from event-related potentials. J Acupunct Tuina Sci. 2018;16(6):382–388. doi:10.1007/s11726-018-1078-3
53. Wu WZ, Zhao YN, Liu CY, et al. Effects of electroacupuncture on sleep quality, daytime fatigue and serum cortisol in chronic insomnia. China J Tradit Chin Med Pharm. 2021;36(9):2021544137.
54. Jing G, Chu-Ying T, Lin-Peng W. Effect of tiaoshen acupuncture therapy on sleep quality and hyperarousal state in primary insomnia. J Clin Acupuncture Moxibust. 2017;10(7):882–885.
55. Zhangxiao S, Tongfei J, Xuejiao Y, Liying Z, Jing G. A study on central mechanism of tiaoshen acupuncture treatment for early awakening insomnia based on fMRI Low-frequency amplitude ratio analysis. J Clin Acupuncture Moxibust. 2024. doi:10.19917/j.cnki.1005-0779.024147
56. Cui YX, Ao YT, Sun JQ. Metabonomics study on acupuncture improving primary insomnia. Clin J Tradit Chin Med. 2021;33(8):2021512126. doi:10.16448/j.cjtcm.2021.0847
57. Guo J, Hu J, Zhang F, et al. Clinical study of the effect of acupuncture with the method of regulating the spirit on the rate of heart rate variability in primary insomnia. Glob Tradit Chin Med. 2019;12(12):2020368089. doi:10.3969/j.issn.1674-1749.2019.12.024
58. Zhang X, Zhang Y, Liu L, Guo J, Zhang F. Acupuncture for regulating hyperarousal state in chronic insomnia with deficiency of heart and spleen: a clinical trial study. Beijing J Tradit Chinese Med. 2024;43(7):2024434082. doi:10.16025/j.1674-1307.2024.07.007
59. Zhang LX, Hui R, Tang Y, et al. Effects of acupuncture on insomnia with depression. China J Tradit Chin Med Pharm. 2020;35(8):2020707159.
60. Xu S, Sun Y, Wang S, Wu J, Yin P. Clinical observation on the treatment of primary insomnia mainly by electroacupuncture on Baihui Shenting. J Sichuan Tradit Chin Med. 2014;32(5):2014516312.
61. Xu X, Wang X, Wu W, et al. Effects of electroacupuncture on sleep quality and serum melatonin in elderly insomnia patients. Shanghai J Acupuncture Moxibustion. 2022;41(1):2022158412. doi:10.13460/j.issn.1005-0957.2022.01.0001
62. Zhu L, Chen K, Jiang T, Chen Z, Wang G, Guo J. Clinical study of spirit-regulating acupuncture improving sleep latency and hyperarousal of patients with CID. J Clin Acupuncture Moxibust. 2024;40(9):2024488395. doi:10.19917/j.cnki.1005-0779.024167
63. Liu C, Zhao Y, Qin S, Wang X, Jiang Y, Wu W. Randomized controlled trial of acupuncture for anxiety and depression in patients with chronic insomnia. Ann Transl Med. 2021;9(18):1426. doi:10.21037/atm-21-3845
64. Chen Z, Jiang T, Yin X, Li B, Tan Z, Guo J. The increased functional connectivity between the locus coeruleus and supramarginal gyrus in insomnia disorder with acupuncture modulation. Front Neurosci. 2023;17:1131916. doi:10.3389/fnins.2023.1131916
65. Wang YK, Li T, Ha LJ, et al. Effectiveness and cerebral responses of multi-points acupuncture for primary insomnia: a preliminary randomized clinical trial and fMRI study. BMC Complement Med Ther. 2020;20(1):254. doi:10.1186/s12906-020-02969-6
66. Kim SA, Lee SH, Kim JH, et al. Efficacy of acupuncture for insomnia: a systematic review and meta-analysis. Am J Chin Med. 2021;49(5):1135–1150. doi:10.1142/s0192415x21500543
67. Liu C, Xi H, Wu W, et al. Placebo effect of acupuncture on insomnia: a systematic review and meta-analysis. Ann Palliat Med. 2020;9(1):19–29. doi:10.21037/apm.2019.11.15
68. Cheuk DK, Yeung WF, Chung KF, Wong V. Acupuncture for insomnia. Cochrane Database Syst Rev. 2012;2012(9):Cd005472. doi:10.1002/14651858.CD005472.pub3
69. Zhao FY, Fu QQ, Kennedy GA, et al. Can acupuncture improve objective sleep indices in patients with primary insomnia? A systematic review and meta-analysis. Sleep Med. 2021;80:244–259. doi:10.1016/j.sleep.2021.01.053
70. Zhang J, He Y, Huang X, Liu Y, Yu H. The effects of acupuncture versus sham/placebo acupuncture for insomnia: a systematic review and meta-analysis of randomized controlled trials. Complement Ther Clin Pract. 2020;41:101253. doi:10.1016/j.ctcp.2020.101253
71. Han X, Gao Y, Yin X, et al. The mechanism of electroacupuncture for depression on basic research: a systematic review. Chin Med. 2021;16(1):10. doi:10.1186/s13020-020-00421-y
72. Buckley TM, Schatzberg AF. On the interactions of the hypothalamic-pituitary-adrenal (HPA) axis and sleep: normal HPA axis activity and circadian rhythm, exemplary sleep disorders. J Clin Endocrinol Metab. 2005;90(5):3106–3114. doi:10.1210/jc.2004-1056
73. Saleh-Ghadimi S, Dehghan P, Sarmadi B, Maleki P. Improvement of sleep by resistant dextrin prebiotic in type 2 diabetic women coincides with attenuation of metabolic endotoxemia: involvement of gut-brain axis. J Sci Food Agric. 2022;102(12):5229–5237. doi:10.1002/jsfa.11876
74. Lee G, Kim W. The modulatory effect of acupuncture on the activity of locus coeruleus neuronal cells: a review. Evid Based Complement Alternat Med. 2017;2017:9785345. doi:10.1155/2017/9785345
75. Eschenko O, Magri C, Panzeri S, Sara SJ. Noradrenergic neurons of the locus coeruleus are phase locked to cortical up-down states during sleep. Cereb Cortex. 2012;22(2):426–435. doi:10.1093/cercor/bhr121
76. Eschenko O, Sara SJ. Learning-dependent, transient increase of activity in noradrenergic neurons of locus coeruleus during slow wave sleep in the rat: brain stem-cortex interplay for memory consolidation? Cereb Cortex. 2008;18(11):2596–2603. doi:10.1093/cercor/bhn020
77. Slavin R, Smith D. The relationship between sample sizes and effect sizes in systematic reviews in education. Educ Eval Policy Anal. 2009;31(4):500–506. doi:10.3102/0162373709352369
78. Ioannidis JP. Why most published research findings are false. PLoS Med. 2005;2(8):e124. doi:10.1371/journal.pmed.0020124
79. Kicinski M, Springate DA, Kontopantelis E. Publication bias in meta-analyses from the Cochrane database of systematic reviews. Stat Med. 2015;34(20):2781–2793. doi:10.1002/sim.6525
80. Bianchi MT, Williams KL, McKinney S, Ellenbogen JM. The subjective-objective mismatch in sleep perception among those with insomnia and sleep apnea. J Sleep Res. 2013;22(5):557–568. doi:10.1111/jsr.12046
81. Linde K, Niemann K, Meissner K. Are sham acupuncture interventions more effective than (other) placebos? A re-analysis of data from the Cochrane review on placebo effects. Forsch Komplementmed. 2010;17(5):259–264. doi:10.1159/000320374
82. Lauderdale DS, Chen JH, Kurina LM, Waite LJ, Thisted RA. Sleep duration and health among older adults: associations vary by how sleep is measured. J Epidemiol Community Health. 2016;70(4):361–366. doi:10.1136/jech-2015-206109
83. Qin Z, Zhu Y, Shi DD, Chen R, Li S, Wu J. The gap between statistical and clinical significance: time to pay attention to clinical relevance in patient-reported outcome measures of insomnia. BMC Med Res Methodol. 2024;24(1):177. doi:10.1186/s12874-024-02297-0
84. Xing J, Wu X, Liu H, et al. Effects of electroacupuncture therapy and cognitive behavioral therapy in chronic insomnia: a randomized controlled study. Evid Based Complement Alternat Med. 2020;2020:5630130. doi:10.1155/2020/5630130
85. Ruan JW, Zheng PY. Therapeutic analysis on the acupuncture for drug-dependence insomnia. Chin J Rehab Med. 2002;17(3):167–168.
86. Kim TH, Lee MS, Lee H. Sham Acupuncture Is Not Just a Placebo. J Acupunct Meridian Stud. 2022;15(6):333–335. doi:10.51507/j.jams.2022.15.6.333
87. Lund I, Lundeberg T. Are minimal, superficial or sham acupuncture procedures acceptable as inert placebo controls? Acupunct Med. 2006;24(1):13–15. doi:10.1136/aim.24.1.13
88. MacPherson H, Green G, Nevado A, et al. Brain imaging of acupuncture: comparing superficial with deep needling. Neurosci Lett. 2008;434(1):144–149. doi:10.1016/j.neulet.2008.01.058
89. Huang H-Y, Cai Y-Y, Zhang Q-S, Huang Y-P, Fu Z-H. Blinding effect of sham Fu’s subcutaneous needling in a healthy population. World J Acupunct Moxibustion. 2024;34(4):312–317. doi:10.1016/j.wjam.2024.09.010
90. Kennedy S, Baxter GD, Kerr DP, Bradbury I, Park J, McDonough SM. Acupuncture for acute non-specific low back pain: a pilot randomised non-penetrating sham controlled trial. Complement Ther Med. 2008;16(3):139–146. doi:10.1016/j.ctim.2007.03.001
91. Colloca L. The Nocebo Effect. Annu Rev Pharmacol Toxicol. 2024;64:171–190. doi:10.1146/annurev-pharmtox-022723-112425
92. Karst M, Li C. Acupuncture-A question of culture. JAMA Network Open. 2019;2(12):e1916929. doi:10.1001/jamanetworkopen.2019.16929
93. Garcia MK, Meng Z, Rosenthal DI, et al. Effect of true and sham acupuncture on radiation-induced xerostomia among patients with head and neck cancer: a randomized clinical trial. JAMA Network Open. 2019;2(12):e1916910. doi:10.1001/jamanetworkopen.2019.16910
94. Pan X, Dib HH, Wang X, Zhang H. Service utilization in community health centers in China: a comparison analysis with local hospitals. BMC Health Serv Res. 2006;6:93. doi:10.1186/1472-6963-6-93
 © 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2025 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 4.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.