")
Back to Journals » Infection and Drug Resistance » Volume 16
Is Halving Maintenance of Voriconazole Safe and Efficient in Patients Suffering from Invasive Fungal Infections with Serious Hepatic Dysfunction?
Authors Cai X, Li W, Yang J, Wu G, Song J, Gong X, Liu D, He Y
Received 13 October 2022
Accepted for publication 28 December 2022
Published 5 January 2023 Volume 2023:16 Pages 1—8
DOI https://doi.org/10.2147/IDR.S390026
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Prof. Dr. Héctor Mora-Montes
Xuezhou Cai,1,2,* Wei Li,1,* Jian Yang,1,3,* Guangjie Wu,1 Jianxin Song,4 Xuepeng Gong,1 Dong Liu,1 Yan He1
1Department of Pharmacy, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China; 2Department of Pharmacy, Xianning Central Hospital, Hubei University of Science and Technology, Xianning, People’s Republic of China; 3Department of Pharmacy, General Hospital of Central Theater Command of Chinese People’s Liberation Army, Wuhan, People’s Republic of China; 4Department of Infectious Diseases, Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, People’s Republic of China
*These authors contributed equally to this work
Correspondence: Yan He; Dong Liu, Email [email protected]; [email protected]
Background: There is a wide debate about the efficacy and safety of voriconazole in patients with impaired hepatic function at Child-Pugh C level.
Objective: The purpose of this study was to investigate the safety and efficacy between the two groups treated with different dosages of voriconazole (400mg/day vs 200mg/day) in the treatment of invasive fungal infections (IFIs) in patients with hepatic dysfunction.
Methods: A retrospective study enrolling patients with hepatic dysfunction receiving intravenous voriconazole for IFIs from January 1st, 2017, to December 30th, 2021 was conducted. Patients were enrolled in the 400mg per day dose group and 200mg per day dose group. In patients with the same degree of hepatic impairment, factors affecting prognosis were screened and differences in steady-state blood trough concentrations (Cmin) of voriconazole, positive G/GM tests and adverse effects (AEs) were compared between the two groups described above.
Results: In total, 308 patients with IFIs were enrolled. For Child-Pugh C class, patients receiving the halved maintenance dose had a lower Cmin and AEs rate but higher recovered rate compared to those receiving maintenance dose, and significant predictors of recovery were dosage (OR, 5.131; 95% CI, 1.599– 16.464; p = 0.006) and diabetes (OR, 0.111; 95% CI, 0.020– 0.597; p = 0.010). For patients of Child-Pugh A & B class, chronic liver disease (OR, 0.334; 95% CI, 0.159– 0.704; p = 0.004) was a prognosis-related factor.
Conclusion: Halving maintenance dose ensure the efficacy and safety of voriconazole in patients suffering from invasive fungal infections with serious hepatic dysfunction.
Keywords: hepatic dysfunction, invasive fungal infections, voriconazole, through concentration, Child-Pugh
Introduction
Patients with hepatic dysfunction are prone to develop IFIs and result in high mortality rate due to immunodeficiency.1 Voriconazole is a first-line antifungal agent in the treatment of invasive aspergillosis and is widely used in high-risk populations.2 The recommended dose of intravenous voriconazole for adults is 400 mg/12 hours on the first day, followed by 200 mg/12 hours, maintaining a Cmin range of 1.0–5.5 mg/L to ensure efficacy and reduce AEs.3,4 As voriconazole is mainly metabolised by liver, the ability of patients with impaired hepatic function to metabolise voriconazole is reduced. At the same time, impaired protein synthesis results in a reduced proportion of the drug in bound form in the blood, ultimately leading to increased drug exposure in these patients.5 That is why the maintenance dose is halved after the standard load dose being required in the instructions for patients with mild to moderate hepatic cirrhosis (Child-Pugh A&B). Nevertheless, clinical data were controversial for patients of Child-Pugh C.6 This study was conducted to explore the impacts of halving maintenance of dosage on the efficacy and safety of voriconazole comparing to maintenance of dosage, and patients of Child-Pugh C are our priority. Meanwhile, very few studies have addressed the factors affecting the prognosis of this group of patients. This retrospective study identified factors associated with the prognosis of patients with different hepatic functions.
Materials and Methods
Patients
This retrospective study recruited patients with hepatic insufficiency admitted to our infection unit between 1 January 2017 and 30 December 2021. The full course of the experiment is shown in Figure 1. Patients over 18 years old who were treated with intravenous voriconazole (400 mg/day or 200 mg/day) for IFIs lasting more than 72 hours with a documented Child-Pugh scores within 24 hours of starting voriconazole were enrolled. Patients who were pregnant, using voriconazole as prophylaxis, using CYP2C19 inhibitors or inducers (eg sodium valproate and rifampicin), having had their voriconazole dosage adjusted or with incomplete medical data were excluded. Patients who died within 5 days after admission were also excluded from the study population as the stable voriconazole concentrations could not be obtained.
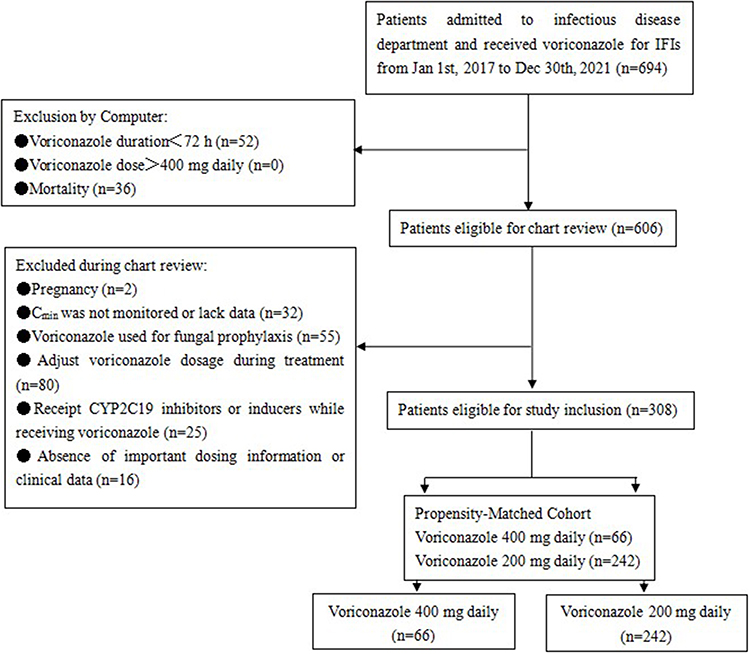 |
Figure 1 Eligibility screening. |
Study Design
The ethics committee of Tongji Hospital, Tongji Medical College, Huazhong University of Science and Technology approved the retrospective cohort study and agreed that patient consent to review their medical records was not required. The authors declare that the procedures followed were in accordance with the regulations of the responsible Clinical Research Ethics Committee and in accordance with those of the World Medical Association and the Helsinki Declaration.
According to the dose regimens, patients were allocated to two groups. In the maintenance dose group, patients received the recommended dosing regimen of 400 mg of loading dose intravenously every 12 hours on day 1, followed by 400 mg daily (200 mg intravenously every 12 hours). In the halved maintenance dose group, patients received the same loading dose, but a halved maintenance dose of 200 mg daily. Hepatoprotective agents such as glutathione, ademetionine 1,4-butanedisulfonate were used during the treatment. Patients with hepatitis B were treated with entecavir or tenofovir.
Treatment success was defined as IFI patients treated with voriconazole, the clinical manifestations included gradual recovery of body temperature, white blood cells and C-reactive protein, relief and disappearance of symptoms and signs at the corresponding infected sites, improvement of imaging and negative culture. Patient was deemed to have failed treatment without significant improvement in signs and symptoms, or once the use of antifungal medication escalated during the course of treatment.
The first detectable Cmin of voriconazole was included in the study. Child-Pugh score using data detected at the beginning of voriconazole treatment were performed for all patients. A patient who discontinued voriconazole treatment was considered to have had an adverse reaction associated with voriconazole only if the electronic medical record system recorded it.
The revised 2020 EORTC/MSG criteria was adopted as the diagnostic criteria for IFIs.7 IFI diagnostic criteria: (1) Proven diagnosis: the patient obtained histological or microbiological evidence of fungal infection through aseptic culture of specimens in biopsy or autopsy tissues or normal parts; (2) Probable/Clinical diagnosis: the patient with risk factors of fungal infection and has evidence of special imaging changes of infection in corresponding parts or two important clinical features (symptoms or signs of respiratory tract infection have worsened recently, respiratory secretions examination or imaging indicates infection; symptoms or signs of peritonitis, abnormal biochemical or routine examination of abdominal puncture fluid samples; urinary tract irritation symptoms such as frequency, urgency, and pain, abnormal biochemical examination of urine and abnormal number of urine sediment cells). At least one microbiological examination is positive at the same time (direct microscopic examination or cytological examination of airway secretions shows positive mycelium/spore or fungal culture; two consecutive urine cultures without urinary catheter show positive yeast, and the urine culture yeast obtained by direct catheterization is positive; direct microscopic examination/cytological examination of drainage fluid from drainage tubes such as chest, abdomen, pelvic cavity and ventricle shows positive mycelium/spore or fungal culture; blood samples G or GM test was positive for two consecutive times; (3) Possible diagnosis: there are risk factors of fungal infection, at least one microbiological test is positive, or there is evidence of special imaging changes of corresponding site infection, or two important clinical features.
Blood Sampling and Analytical Assays
A steady-state Cmin was determined as stated method.1,8 High-performance liquid chromatography (HPLC) assays were used to measure voriconazole plasma concentrations. Liver-related biochemical indexes were measured by automatic biochemical detector Olympus AU 5000.
Data Collection
All of the clinical data was collected from electronic medical record system by an information-gathering team of trained, permanent staff using standard form.
Statistical Analysis
Continuous variables were presented as the mean and standard deviation. Categorical variables were reported as frequencies and percentages. Pearson’s chi-squared test or Fisher’s exact test were used for categorical variables. Continuous variables were compared by T-test or the Wald test. Multivariable analyses of factors associated with prognosis were performed using forward, stepwise, and binary logistic regression. A two-sided p value of <0.05 was considered statistically significant. Statistical analysis was performed using SPSS 24.0 (IBM SPSS Inc.).
Result
Univariate Analysis of Characteristics and Clinical Data
A total of 308 patients were considered eligible for inclusion: 96 (31.17%) were proven diagnosed with IFIs, 98 (31.82%) were probable diagnosed and 114 (37.01%) were possible diagnosed. As summarized in Table 1, 155 fungal strains isolated from 155 (50.32%) patients were confirmed by psychophysiology. Candida (56, 36.13%) and aspergillus (99, 63.87%) were isolated from samples of sputum culture/alveolar lavage, urine, ascites and drainage.
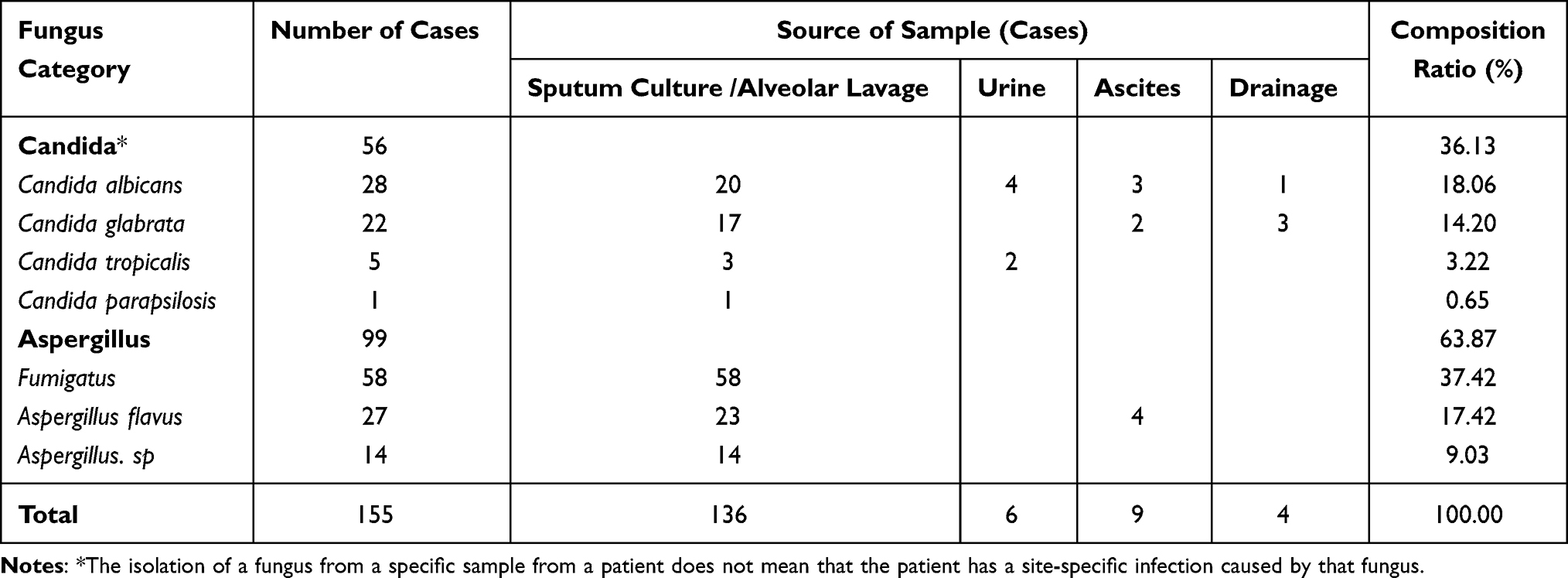 |
Table 1 Distribution, Composition Ratio and Source of 155 Isolated Fungi |
Of these patients, 242 (78.57%) received halved maintenance doses, and 66 (21.43%) received maintenance doses. The patient’s demographic and clinical data are listed in Table 2. The two groups were well matched with respect to demographics and complications.
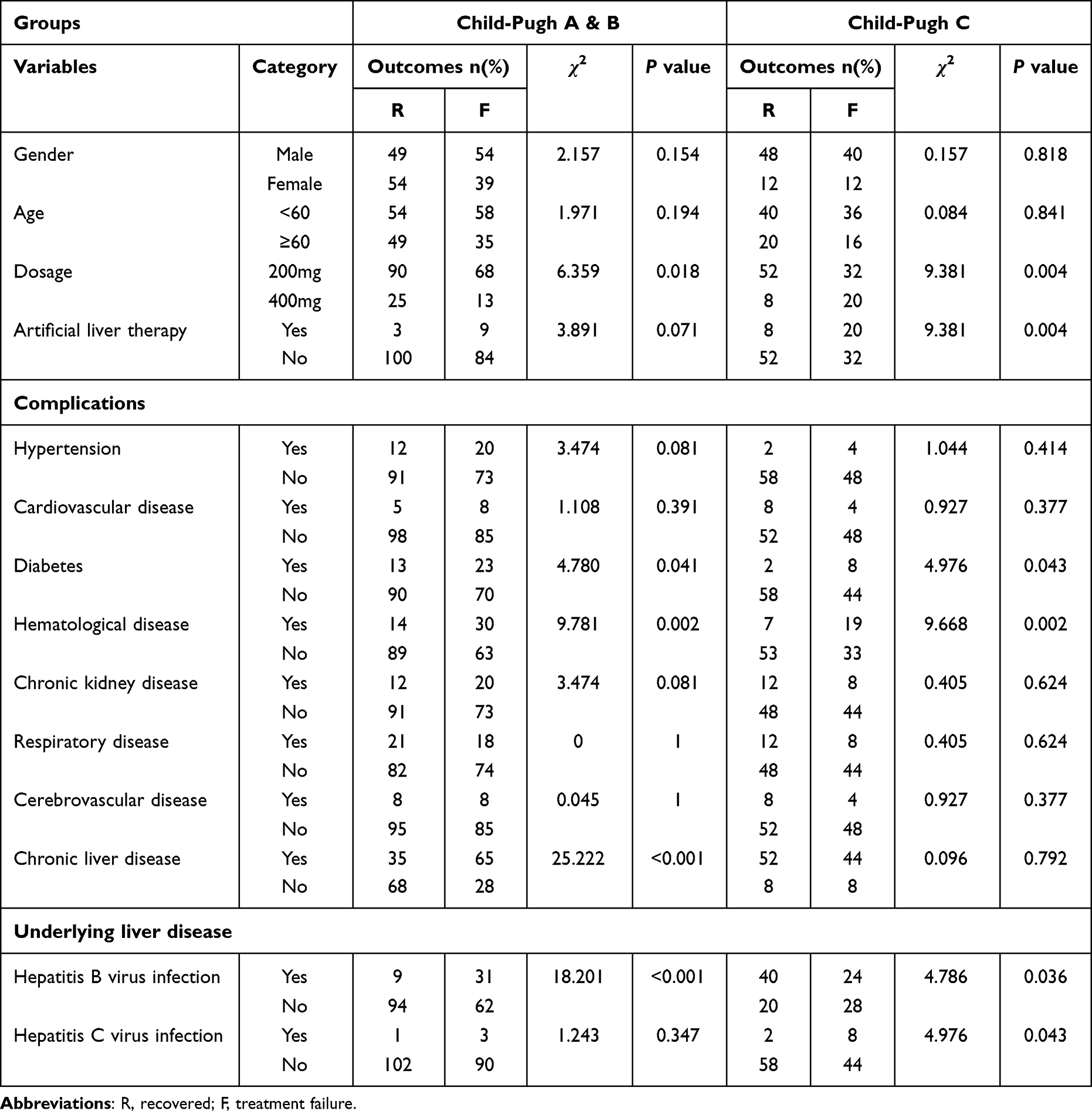 |
Table 2 Patient’s Demographic and Clinical Data |
196 and 112 patients were assigned to Child-Pugh A&B group and Child-Pugh C group respectively, corresponding to mild & moderate liver damage and severe liver damage, on the basis of Child-Pugh scores. The recovered rates were 58.67% and 53.57% for Child-Pugh A&B group and Child-Pugh C group respectively. Gender and age had no effect on recovered rates in either group. In the Child-Pugh A & B group, patients receiving a dose of 400 mg/day had a higher recovered rate than those receiving a dose of 200 mg/day (65.79% vs 56.96%, p = 0.018), while in Child-Pugh Group C, the opposite was true (p = 0.004). Artificial liver support was effective for patients with severe hepatic impairment (p = 0.004), but did not affect the prognosis of patients with mild or moderate hepatic impairment (p = 0.071). In both groups representing different liver function states, suffering from diabetes (Child-Pugh A&B, p = 0.041 and Child-Pugh C, p = 0.043) or hematologic diseases (Child-Pugh A&B, p = 0.002 and Child-Pugh C, p = 0.002) was associated with poor prognosis. Nevertheless, complicating chronic liver disease was associated with the prognosis of patients with mild to moderate liver injury (p < 0.001), but did not affect the prognosis of patients with severe liver injury (p = 0.792). Details are presented in Table 2.
Multivariate Analysis
By multivariate analysis correction of confounders, dosage (OR 5.131, 95% CI (1.599–16.464), p = 0.006) and diabetes (OR 0.111, 95% CI (0.020, 0.597), p = 0.010) were shown to be associated with the recovered rate in Child-Pugh C group, and suffering from chronic liver disease (OR 0.334, 95% CI (0.159, 0.704), p = 0.004) mean to lower recovered rate for patients in Child-Pugh A&B group (Table 3).
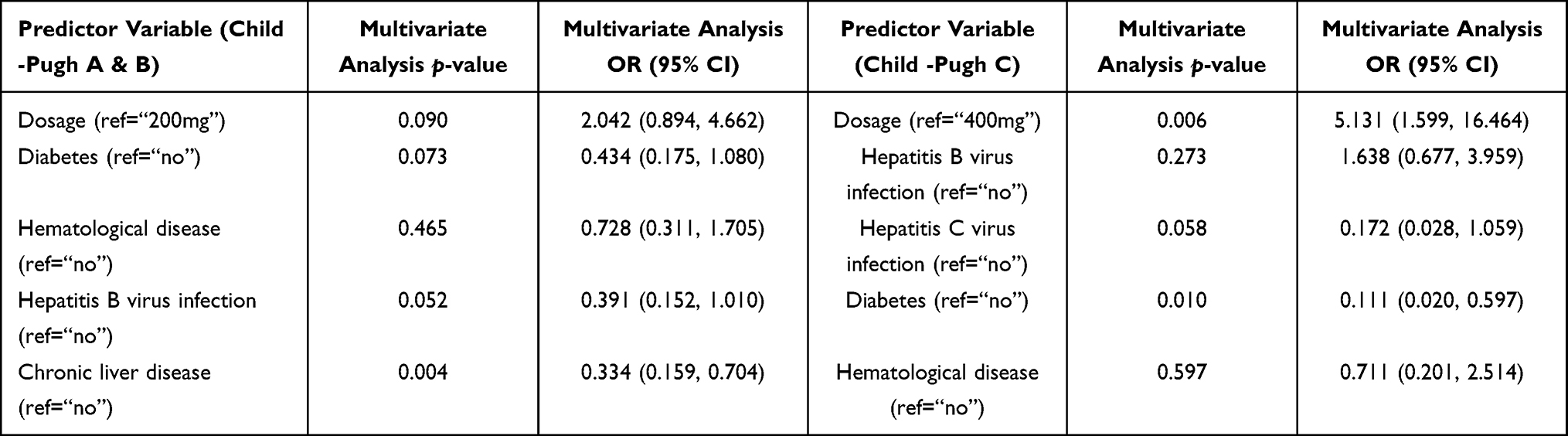 |
Table 3 Multivariable Analyses of the Association Between Potential Predictor Variables and Recovery Rate Among Different Child-Pugh Class Patients Receiving Voriconazole |
Voriconazole Cmin and Efficacy of Antifungal Treatment
Table 4 describes Patient’s clinical outcomes of different Child-Pugh class. Trough concentrations of voriconazole showed significant individual differences regardless of whether the recommended dose was maintained (242 patients, mean±SD (2.80±3.20 μg/mL)) or halved (122 patients, mean±SD (2.73±1.60 μg/mL)). The average trough concentration of voriconazole between this two groups showed no difference (p = 0.967). Interestingly, after stratifying the patients according to liver function, the mean concentration of voriconazole in patients with the same liver function showed differences according to the dose (Child-Pugh A&B, p = 0.012; Child-Pugh C, p = 0.009).
 |
Table 4 Patient’s Clinical Outcomes of Different Child-Pugh Class |
For patients in Child-Pugh classes A & B class, higher dosages were associated with lower positive rate of G/GM test (p = 0.001). But for patients in Child-Pugh classes C class, the situation seems to be the opposite (p = 0.097). The most common voriconazole-related AEs were neurological disturbance.9–11 Up to 10% of patients suffered from AEs including encephalopathy (n = 6), tremor (n = 4), dizziness (n = 4), consciousness disturbance (n = 5), hallucination (n = 3), etc. For patients in Child-Pugh groups A and B, the difference in the incidence of AEs between dose groups was not significant (15/158 vs 2/38, P = 0.534), while for patients with severe liver injury, the odds of AEs were significantly lower for those on a reduced half dose of voriconazole compared to the regular dose group (5/84 vs 10/28, P = 0.000).
Discussion
Patients with hepatic dysfunction are susceptible to IFIs, which increased year by year according to Infectious Diseases Society of America (IDSA).2 At present, major antifungal agents include triazoles, echinocandins and polyenes. As a broad-spectrum triazole antifungal agent, voriconazole has the activity of anti-aspergillosis and anti-candida resistant to fluconazole.12,13 Nevertheless, voriconazole is metabolized in liver, and patients with hepatic dysfunction are vulnerable to overexposure and adverse reactions. Meanwhile, experience in using voriconazole in patients with severe hepatic dysfunction (Child-Pugh C) is still scarce. Although existing studies have assessed the safety of regimens with halved maintenance dose of voriconazole in patients with serious hepatic impairment, the level of evidence is poor. For these patients, the pros and cons should be fully weighed and voriconazole as a treatment drug should be carefully selected. In the meantime, close monitoring of the patient’s liver function, as well as voriconazole trough concentrations, is imperative to ensure the security. That is why we further validated the safety and efficacy of halved voriconazole dosage in patients of Child-Pugh C.
Due to the decreased metabolic ability of voriconazole in patients with hepatic dysfunction, increased voriconazole exposure may be accompanied by an increase in AEs, so the voriconazole maintenance dose should be halved in these patients.14 This study reinforces the view by revealing that higher dosages (400 mg per day) were associated with an increased treatment failure (p = 0.006) and higher incidence of adverse events (p = 0.000) in patients with serious liver function impairment.
We discovered that in Child-Pugh C patients, halving the dose resulted in lower Cmin and a higher recovery rate, with a lower incidence of adverse reactions. This may be due to the reduced ability to metabolize voriconazole in patients who develop severe hepatic dysfunction, resulting in saturated voriconazole metabolism at half the maintenance dose. As found by Gao and Wang, higher doses would only lead to increased exposure and thus metabolic burden or higher incidence of adverse effects.1,15 In addition, we found that in patients of Child-Pugh A & B, the halved dose group had a more positive pre-discharge G/GM test than the maintenance dose group, which could be interpreted as a failure to meet serum concentrations. However, for patient of Child-Pugh C, the situation was reversed for causes to be identified. We found that the antibiotic escalation occurred only in the half maintenance dose group and the failure to achieve the plasma concentration was the possible cause.
Artificial liver therapy is a therapeutic apheresis that creates an opportunity for hepatocyte regeneration and recovery of liver function by exchanging toxic and nutrient substances between in vivo and in vitro. Patients receiving plasma exchange often receive voriconazole for IFIs, and the effect of artificial liver therapy on voriconazole plasma concentrations is also of concern.16–18 Whether the contribution of artificial liver therapy to the plasma concentration of a medicine is clinically significant depends on two pharmacokinetic parameters of the medicine, namely distribution volume (Vd) and fraction of protein binding (PB).19,20 It is generally acknowledged that drugs with Vd < 0.2 L/kg and PB > 80% are considered to be easily removed during plasma replacement.20 While voriconazole had a Vd value of 4.5 L/kg and PB of 58%.21 In a case report of a patient with fungal pneumonia requiring plasma exchange who was given voriconazole 2.5 hours prior to the start of plasma exchange, the effect of plasma exchange on drug concentrations was not significant.21 This is the explanation for not including artificial liver treatment as an exclusion criterion in this study. Furthermore, artificial liver treatment can eliminate excessive inflammatory response thus regulating the patient’s inflammatory status and improving liver function.22 While the patient’s inflammatory status and liver function can affect the metabolism of voriconazole, the magnitude of this effect needs to be further examined.
The concentration of anti-microbial drugs is variable due to severe hepatic impairment, and dose adjustment is necessary at this stage.23,24 The description requires that the maintenance dose of voriconazole be halved in patients in groups A&B, motivated by concerns about the high exposure and more adverse reactions associated with the maintenance dose. In our study, for groups A&B, there was no advantage of this regimen over the original dose in terms of patient recovery rates and incidence of adverse reactions (no impact on recovery rates and incidence of adverse reactions). Notably, for group C this regimen demonstrated an advantage (higher recovery rate and fewer adverse reactions). This indicates the urgency of dose reduction for patients with severe hepatic impairment, and how appropriate a dose reduction needs the comparison of more dosing regimens, such as one-third of the maintenance dose.25 Diabetes, hematological disease and chronic liver disease reflect the immune status indirectly, which are the risk factors of liver dysfunction, it is easy to understand that independent correlate with recovery rate.
A limitation of this study was the introduction of patients diagnosed with possible fungal infections, which made up a large proportion of the sample size. Although we had an infection specialist on our team who was responsible for keeping the correctness of the final diagnosis, it was inevitable that there would be false-positive patients. Thus, the inclusion of patients with a possible diagnosis in the study may have inflated the eventual recovery rate of patients by introducing patients with false-positive infections.
Conclusions
In this study, Child Pugh C patients receiving the halved maintenance dose had a lower Cmin and AEs rate but higher recovered rate compared to those receiving maintenance dose. Therefore, the halved maintenance regimen of voriconazole for patients with mild to moderate hepatic failure may also be appropriate for Child-Pugh C patients to decrease the risk of AEs, reduce treatment failure and promote liver function recovery, but further clinical trials are needed.
Disclosure
The authors report no conflicts of interest in this work.
References
1. Wang T, Yan M, Tang D, et al. Therapeutic drug monitoring and safety of voriconazole therapy in patients with Child–Pugh class B and C cirrhosis: a multicenter study. Int J Infect Dis. 2018;72:49–54. doi:10.1016/j.ijid.2018.05.009
2. Patterson TF, Thompson GR III, Denning DW, et al. Practice guidelines for the diagnosis and management of aspergillosis: 2016 update by the infectious diseases society of America. Clin Infect Dis. 2016;63:e1–e60. doi:10.1093/cid/ciw326
3. Ashbee HR, Barnes RA, Johnson EM, et al. Therapeutic drug monitoring (TDM) of antifungal agents: guidelines from the British society for medical mycology. J Antimicrob Chemother. 2014;69:1162–1176. doi:10.1093/jac/dkt508
4. Driscoll TA, Yu LC, Frangoul H, et al. Comparison of pharmacokinetics and safety of voriconazole intravenous-to-oral switch in immunocompromised children and healthy adults. Antimicrob Agents Chemother. 2011;55(12):5770–5779. doi:10.1128/AAC.00531-11
5. Alffenaar J-W, Devos T, Uges DA, et al. High voriconazole trough levels in relation to hepatic function: how to adjust the dosage? Br J Clin Pharmacol. 2009;67:262. doi:10.1111/j.1365-2125.2008.03315.x
6. Zhao Y, Hou J, Xiao Y, et al. Predictors of voriconazole trough concentrations in patients with Child–Pugh Class C cirrhosis: a prospective study. Antibiotics. 2021;10:1130.
7. Donnelly JP, Chen SC, Kauffman CA, et al. Revision and update of the consensus definitions of invasive fungal disease from the European organization for research and treatment of cancer and the mycoses study group education and research consortium. Clin Infect Dis. 2020;71:1367–1376. doi:10.1093/cid/ciz1008
8. Li Z-W, Peng F-H, Yan M, et al. Impact of CYP2C19 genotype and liver function on voriconazole pharmacokinetics in renal transplant recipients. Ther Drug Monit. 2017;39:422. doi:10.1097/FTD.0000000000000425
9. Jin H, Wang T, Falcione BA, et al. Trough concentration of voriconazole and its relationship with efficacy and safety: a systematic review and meta-analysis. J Antimicrob Chemother. 2016;71:1772–1785. doi:10.1093/jac/dkw045
10. Luong M-L, Al-Dabbagh M, Groll AH, et al. Utility of voriconazole therapeutic drug monitoring: a meta-analysis. J Antimicrob Chemother. 2016;71:1786–1799. doi:10.1093/jac/dkw099
11. Tan K, Brayshaw N, Tomaszewski K, et al. Investigation of the potential relationships between plasma voriconazole concentrations and visual adverse events or liver function test abnormalities. J Clin Pharmacol. 2006;46(2):235–243. doi:10.1177/0091270005283837
12. Bajaj JS, O’Leary JG, Tandon P, et al. Nosocomial infections are frequent and negatively impact outcomes in hospitalized patients with cirrhosis. Am J Gastroenterol. 2019;114:1091. doi:10.14309/ajg.0000000000000280
13. Zhang Y, Wang Y, Zhang J, et al. The application of voriconazole in 76 patients with cirrhosis at Child-Pugh C stage complicated by invasive fungal infection. Zhonghua Gan Zang Bing Za Zhi. 2021;29:137–142. doi:10.3760/cma.j.cn501113-20190813-00302
14. Johnson H, Han K, Capitano B, et al. Voriconazole pharmacokinetics in liver transplant recipients. Antimicrob Agents Chemother. 2010;54:852–859. doi:10.1128/AAC.00429-09
15. Gao J, Zhang Q, Wu Y, et al. Improving survival of acute-on-chronic liver failure patients complicated with invasive pulmonary aspergillosis. Sci Rep. 2018;8:1–8. doi:10.1038/s41598-017-17765-5
16. Brecher ME. Plasma exchange: why we do what we do. J Clin Apher. 2002;17:207–211. doi:10.1002/jca.10041
17. Guillevin L. Synchronization of plasma exchange and adjuvant treatments. Transfus Sci. 1998;19:27–33. doi:10.1016/S0955-3886(98)00006-X
18. Smith JW, Weinstein R, For the AABB Hemapheresis Committee. Therapeutic apheresis: a summary of current indication categories endorsed by the AABB and the American society for apheresis. Transfusion. 2003;43(6):820–822. doi:10.1046/j.1537-2995.2003.00397.x
19. Fauvelle F, Petitjean O, Tod M, et al. Clinical pharmacokinetics during plasma exchange. Therapie. 2000;55(2):269–275.
20. Kintzel PE, Eastlund T, Calis KA. Extracorporeal removal of antimicrobials during plasmapheresis. J Clin Apher. 2003;18(4):194–205. doi:10.1002/jca.10074
21. Spriet I, Brüggemann RJ, Annaert P, et al. Pharmacokinetic profile of voriconazole in a critically ill patient on therapeutic plasma exchange. Ther Drug Monit. 2013;35:141–143. doi:10.1097/FTD.0b013e31827d76b0
22. Liang Z, Yu M, Liu Z, et al. Inflammation affects liver function and the metabolism of voriconazole to voriconazole-N-oxide in adult and elderly patients. Front Pharmacol. 2022;13:835871. doi:10.3389/fphar.2022.835871
23. Jager NG, van Hest RM, Lipman J, et al. Therapeutic drug monitoring of anti-infective agents in critically ill patients. Expert Rev Clin Pharmacol. 2016;9:961–979. doi:10.1586/17512433.2016.1172209
24. Roberts JA, Lipman J. Pharmacokinetic issues for antibiotics in the critically ill patient. Crit Care Med. 2009;37:840–851. doi:10.1097/CCM.0b013e3181961bff
25. Yamada T, Imai S, Koshizuka Y, et al. Necessity for a significant maintenance dosage reduction of voriconazole in patients with severe liver cirrhosis (Child-Pugh class C). Biol Pharm Bull. 2018. doi:10.1248/bpb.b18-00164
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The full terms of this license are available at https://www.dovepress.com/terms.php and incorporate the Creative Commons Attribution - Non Commercial (unported, v3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted without any further permission from Dove Medical Press Limited, provided the work is properly attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.