Back to Journals » Risk Management and Healthcare Policy » Volume 16
Is Co-Occurrence of Frailty and Multimorbidity Associated with Increased Risk of Catastrophic Health Expenditure? A Prospective Cohort Analysis in China
Authors Li H ![]() , Chen J
, Chen J ![]() , Su D, Xu X, He R
, Su D, Xu X, He R
Received 19 December 2022
Accepted for publication 11 February 2023
Published 8 March 2023 Volume 2023:16 Pages 357—368
DOI https://doi.org/10.2147/RMHP.S402025
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 2
Editor who approved publication: Dr Jongwha Chang
Haomiao Li,1 Jiangyun Chen,2 Dai Su,3 Xiwu Xu,4 Ruibo He1,5
1School of Political Science and Public Administration, Wuhan University, Wuhan, Hubei, People’s Republic of China; 2Institute of Health Management, Southern Medical University, Guangzhou, Guangdong, People’s Republic of China; 3Department of Health Management and Policy, School of Public Health, Capital Medical University, Beijing, People’s Republic of China; 4School of Economics and Management, Beijing Jiaotong University, Beijing, People’s Republic of China; 5College of Finance and Public Administration, Hubei University of Economics, Wuhan, Hubei, People’s Republic of China
Correspondence: Ruibo He, School of Political Science and Public Administration, Wuhan University, Wuhan, Hubei, 430072, People’s Republic of China, Email [email protected]
Purpose: The coexistence of multimorbidity and frailty is more likely to increase the risk of physical limitations, mortality and other adverse health outcomes in older adults than their individual occurrence. However, whether and how this coexistence is associated with catastrophic health expenditure (CHE) has not been well assessed. This study aimed to evaluate the independent and coexisting effects of frailty and multimorbidity on CHE.
Participants and Methods: A total of 4838 participants obtained from the China Health and Retirement Longitudinal Study (CHARLS) without CHE at baseline (2011) were included in the analytical sample. Marginal structural model (MSM) and time-varying Cox regression model were used to assess the independent and co-occurring impact of frailty and multimorbidity on CHE, respectively.
Results: Suffering from single chronic disease (HR, 1.26; 95% CI, 1.13– 1.40; P < 0.001), multimorbidity (HR, 1.80; 95% CI, 1.63– 1.99; P < 0.001) and frailty (HR, 1.32; 95% CI, 1.21– 1.45; P < 0.001) were associated with a higher risk of CHE. Frailty co-occurring with a single chronic disease (HR, 1.28; 95% CI, 1.03– 1.60; P = 0.027) or multimorbidity (HR, 1.91; 95% CI, 1.56– 2.32; P < 0.001), and multimorbidity co-occurring with frailty also increased CHE risk (HR, 1.32; 95% CI, 1.17– 1.48; P < 0.001) compared with single frailty or multimorbidity status.
Conclusion: Preventing, postponing, or reducing frailty, and enhancing standard management of chronic diseases are essential in reducing healthcare costs and preventing families from poverty. More efficient interventions for frailty and multimorbidity are urgently required.
Keywords: frailty, multimorbidity, catastrophic health expenditure, co-occurrence
Introduction
China is one of the world’s most rapidly ageing countries, with more people aged 65 and over than in any other country. In 2019, the Chinese population constituted 18% of the world’s population, with 164.5 million citizens aged 65 and above, and 26 million aged 80 or above.1,2 This will continue to exacerbate the burden borne by the management of chronic non-communicable diseases, physical frailty, neurodegenerative diseases, cardiovascular diseases and so on.3 This grim reality could increase the risk of households’ catastrophic health expenditure (CHE). CHE is an important index for measuring health equity, and reducing its risk in families is the original intention of medical system designs in various countries. CHE is critical to proactively addressing population ageing, promoting health equity, and making more targeted policy recommendations.
Frailty and multimorbidity are two risk factors for CHE among the older populations. Frailty describes a state of overall decline in physical, mental, or cognitive functions between unhealthy and non-serious impairment. Frailty is a predictor of mortality, falls, worsening disability, diseases (dementia, cardiovascular events, etc.), and is significantly associated with a decreased quality of life.4,5 According to the impact of frailty on clinically adverse outcomes, it is easy to predict that frailty is associated with increased healthcare costs in older populations.6,7 Some previous cross-sectional studies have found that frailty is positively associated with increased healthcare use, and can predict subsequent high healthcare costs.8–10 Jin et al examined the association between frailty and healthcare expenditure among Chinese older adults, and found that frailty was associated with higher odds of incurring outpatient, inpatient, and self-treatment expenditure.11 Fan et al found that prefrail or frail adults were associated with higher odds for CHE through a prospective cohort analysis12 in one of the first studies to explore the association between frailty and CHE in China. However, the study period was relatively short (2011–2013). The ageing situation, disease spectrum, and socioeconomic status of older adults have changed dramatically during the past years.
With an ageing population and high levels of risk factors for non-communicable diseases, the prevalence of multimorbidity in China has increased rapidly. According to Hu’s systematic review, the prevalence of multimorbidity in older adults (60+) ranged from 6.4% to 76.5% in China.13 A recent study using a nationally representative sample of older Chinese people also presented a 42.2% prevalence of multimorbidity. Multimorbidity is associated with a high economic burden for older populations (both themselves and their households). Significant positive relationships between multimorbidity and healthcare use, total and out-of-pocket (OOP) healthcare costs were found in several previous studies, many of which found that use or costs significantly increased with each additional condition.14–16 An epidemiological study demonstrated that older adults with multimorbidity experienced a higher probability of incurring CHE than those without it.17 In Zhao’s study, which was the first study from China that used panel survey data, physical multimorbidity was found to be associated with a significantly increased likelihood of CHE, which persisted even among the higher socioeconomic groups and across all health insurance programmes.18 Fu et al also found that multimorbidity affects about two-thirds of Chinese patients with diabetes and can lead to CHE for their families across all health insurance types irrespective of socioeconomic status in China.19
Based on recent studies, both frailty and multimorbidity are increasingly prevalent along with the growth of an ageing population. The attention received by both conditions is derived from their strong association with disability, hospitalisation, economic burden, and mortality.20 Frailty and multimorbidity represent two different clinical conditions. According to Vetrano’s review, the prevalence of multimorbidity in frail individuals and frailty in multimorbid individuals was 72% and 16%, respectively. This suggested that most frail individuals are also multimorbid, but fewer multimorbid ones also present frailty, although the causal association between the two is not conclusive.21 Some longitudinal studies suggest a bidirectional association between multimorbidity and frailty.22–24
To date, it is unclear whether and how co-occurrence of frailty and multimorbidity affects CHE among middle-aged and older adults, especially in China. Some studies have assessed the impact one of the issues on CHE, with another issue adjusted as a confounding or subgroup analysis. For example, in Fan et al’s study, frailty was associated with increased risk of CHE after multimorbidity and many other covariates were controlled.25 Jing et al investigated the effect of co-occurrence of frailty on CHE among single empty-nest older adults with multimorbidity in China, and demonstrated that there is a positive effect of co-occurrence of frailty on CHE among them, and that this effect varies by economic status.26
The coexistence of multimorbidity and frailty was found to more likely increase the risk of physical limitations, mortality, and other adverse health outcomes in older adults than multimorbidity or frailty status individually.27,28 Nevertheless, longitudinal assessments are scarce, and investigation of independent and combined effects of frailty and multimorbidity on CHE are urgently required. Therefore, through cohort analysis based on nationally representative data, this study aimed to evaluate independent and co-occurring effects of frailty and multimorbidity on CHE. We proposed two hypotheses: (1) both frailty and multimorbidity can independently predict CHE; (2) co-occurrence of frailty and multimorbidity will increase the risk of CHE, compared with those who suffer from only one condition.
Materials and Methods
Participants
Data for this study were obtained from the China Health and Retirement Longitudinal Study (CHARLS), conducted in 2011, 2013, 2015 and 2018. CHARLS is a representative database for geriatrics research in China, with a high quality of micro-level database on middle-aged and older adults. The sampling details and variables have been described minutely in previous studies.29 We included data from participants who were not lost to follow-up over the four waves and aged 45 years and older in wave 2011. We excluded participants who had missing values of dependent or independent variables. Then participants not suffering from CHE at baseline were considered for the analysis.
Variables
Exposure – Frailty and Multimorbidity
Frailty status was measured by the Rookwood’s Cumulative Deficit Frailty Index (FI). The deficits used for calculating FI were selected according to the following inclusions: (1) a minimum of 30 total deficits; (2) associated with adverse health outcomes; (3) increase in prevalence with age at least into the tenth decade; (4) prevalence of at least 1% in the population; (5) does not saturate.30 A total of 34 deficits were selected to calculate FI, with binary variables coded as 0 or 1 and some ordered categorical variables coded as 0, 0.5, and 1 (details in Supplementary Table S1).31 FI was calculated by summing the number of deficits reported by the participants and dividing it by the total number of answered possible deficits. An FI ranged from 0 to 1 was then generated, with higher FI indicating more serious status of frailty. Participants were classified as not frail (FI <0.25), or frail (FI ≥0.25).30 Additionally, participants with missing items of frailty-related deficits exceeding seven (20% out of 34 items) were excluded from our analysis.
Multimorbidity is defined as the presence of two or more physical chronic non-communicable diseases.32 We used 11 self-reported diagnosed non-communicable chronic diseases to measure multimorbidity (hypertension, diabetes, dyslipidaemia, heart disease, stroke, cancer, chronic lung disease, digestive disease, liver disease, kidney disease, and arthritis). We enumerated the number of non-communicable diseases for each participant to identify those with multimorbidity.
Outcome – Catastrophic Health Expenditure (CHE)
CHE at the household level was calculated by integrating individuals’ and their spouses’ OOP. We defined a household as incurring CHE when OOP spending on health equalled or exceeded 40% of a household’s capacity to pay, defined as the total consumption expenditure of the household minus the food-based household spending.18,33 This expenditure level was the denominator and the numerator was the sum of participants’ and their spouses’ OOP spending for outpatient and inpatient care in the past year. We defined a binary variable, which indicated whether the participant’s household had CHE or not.
Covariates
Covariates in this study included participants’ demographic characteristics (age, gender, marital status), socioeconomic background (hukou status, level of education, rural/urban residence, public health insurance coverage, household per capita consumption and current work status, and health behaviours (alcohol intake, smoking status). Hukou status is obtained from the registration system based on place of birth and lineage, and is a special identifier in China. Hukou status differentiates opportunity structures for Chinese population by giving priority to urban hukou holders in many spheres, including education, job opportunities, housing, health insurance, and other social services and provisions.34 The grouping details for the covariates are presented in Table 1.
 |
Table 1 Baseline Characteristics of the Sample |
Statistical Analysis
In description analysis of the participants’ baseline characteristics within different exposure groups (“None”, “Single chronic disease”, “Multimorbidity”, “Frailty”, “Frailty and single chronic disease”, “Frailty and multimorbidity”), “number” (percentage) and “mean ± standard deviation” (SD) were used for describing binary or categorical variables and continuous variables, respectively. The statistical differences were tested by ordinal chi-square tests for the categorical variables and Kruskal–Wallis one-way analysis for the numerical variables which were abnormally distributed.
Cox proportional hazard models were employed to calculate relative risk of CHE with survey waves as the timescale. Participants classified as CHE at baseline were excluded from the analysis, and those who remained without CHE were treated as censored data.
When analysing independent effects, we treated one condition (frailty or multimorbidity) as exposure, with another one as time-varying confounder, which is associated with both the exposure and outcome. Then, we performed marginal structural model (MSM) via inverse probability of treatment weighting (IPTW) to mitigate time-varying confounders and overcome immortal time bias. The stabilised weights for MSM were calculated based on IPTW by multiplying the treatment and censoring weights, which were then pooled into the marginal structural model to calculate the associations between frailty or multimorbidity and CHE.
When analysing the co-occurrence effect, we treated frailty and multimorbidity as time-varying exposures to avoid immortal time bias. The analysis strategy is presented in Supplementary Table S2. Hazard ratios (HRs) with 95% confidence intervals (CIs) were calculated through MSM and time-varying Cox regression, respectively.
Sampling and non-response weight were not considered in this study because many studies that employed CHARLS data suggested that results of regression analyses with and without weighting were similar.35 P values were two-tailed, where statistical significance was set at an alpha level of 0.05. Data were analysed using R version 3.6.3 (R Foundation for Statistical Computing, Vienna, Austria).
Sensitivity Analysis
To validate the results, we performed two sensitivity analyses. First, considering the heavy economic burden brought by cancer, we excluded participants suffering from cancer and repeated the above analysis. Second, multiple imputations were conducted to impute the missing covariate values based on five replications and a chained equation approach, to avoid statistical test performance reduction and bias due to direct exclusion of missing values. Additionally, to evaluate the potential effect of unmeasured confounding in the association between co-occurrence (of multimorbidity and frailty) and CHE, E-value analysis was performed using the methodology developed by VanderWeele and Ding.36,37 E-value is an alternative approach to sensitivity analyses for unmeasured confounding in our study that avoids making assumptions that, in turn, require subjective assignment of inputs for some formulas.
Heterogeneity Analysis
There are significant variances between rural and urban area in China in terms of economic level, proportion of older people and ageing process, family structures, and healthcare resources. Therefore, we further explored the variance of the impact of frailty and multimorbidity on CHE for rural and urban participants separately.
Results
Descriptive Analysis
We identified 6117 participants without missing outcomes and exposure variables, and who had completed all the four waves of surveys. The prevalence of CHE in participants with different co-occurrence of frailty and multimorbidity status are shown in Table 2. It shows that the prevalence of CHE in participants with co-occurrence of frailty and multimorbidity was higher than all the other groups, which ranged from 32.7% to 40.95%; participants without any conditions had the lowest prevalence of CHE.
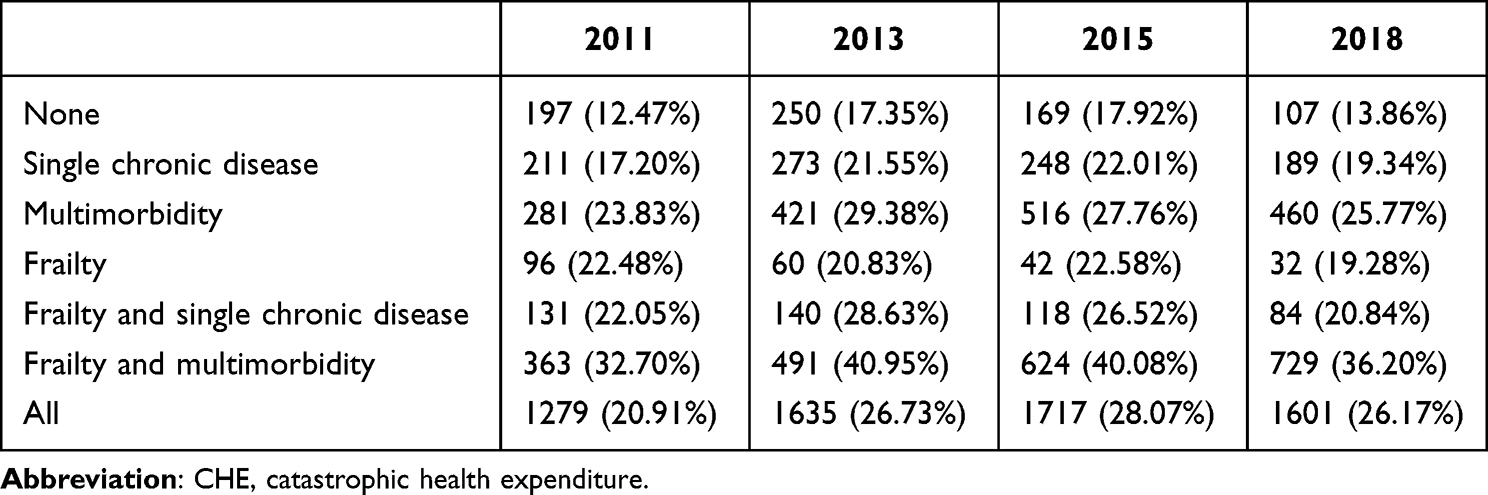 |
Table 2 Prevalence of CHE Across 4 Survey Waves (N=6117) |
A total of 4838 participants without CHE at baseline were included in the following analytical sample. Table 1 presents the baseline characteristics of the sample according to co-occurrence of frailty and multimorbidity status. The prevalence of multimorbidity without frailty and frailty without chronic diseases was 18.56% and 6.84%, respectively. The prevalence of frailty co-occurring with multimorbidity was 15.44%, which was higher than that of frailty co-occurring with a single chronic disease. The age of participants without frailty and multimorbidity was lower than the other groups. Females were more likely to suffer from the co-occurrence of frailty and multimorbidity. All the variances between different exposure groups were statistically significant.
Independent Effect of Multimorbidity and Frailty on CHE
After adjusting for time-varying exposure (multimorbidity status) and confounders (frailty status), both suffering from a single chronic disease (adjusted HR, 1.26; 95% CI, 1.13–1.40; P < 0.001) and multimorbidity (adjusted HR, 1.80; 95% CI, 1.63–1.99; P < 0.001) were associated with a higher risk of CHE. After adjusting for multimorbidity status as a time-varying confounder, frailty (adjusted HR, 1.32; 95% CI, 1.21–1.45; P < 0.001) was also associated with a higher risk of CHE. Details are presented in Table 3.
 |
Table 3 Independent Impact of Multimorbidity and Frailty on CHE Based on Marginal Structural Model |
Effect of Co-Occurrence of Multimorbidity and Frailty on CHE
We classified the participants into six groups according to the co-occurrence of frailty and chronic diseases. Based on time-varying Cox regression (Table 4), we found that compared to those suffering neither from frailty nor chronic diseases, single chronic disease (adjusted HR, 1.23; 95% CI, 1.08–1.39; P = 0.001), multimorbidity (adjusted HR, 1.60; 95% CI, 1.42–1.81; P < 0.001), co-occurrence of frailty and single chronic disease (adjusted HR, 1.42; 95% CI, 1.21–1.67; P < 0.001), and co-occurrence of frailty and multimorbidity (adjusted HR, 2.11; 95% CI, 1.86–2.38; P < 0.001) were significantly associated with increased CHE risk, whereas only suffering from frailty did not increase CHE risk.
 |
Table 4 Impact of Combined Status of Multimorbidity and Frailty on CHE Based on Time-Varying Cox Regression Analysis |
Compared to participants only suffering from frailty but not any chronic disease, both frailty co-occurring with a single chronic disease (adjusted HR, 1.28; 95% CI, 1.03–1.60; P = 0.027) and with multimorbidity (adjusted HR, 1.91; 95% CI, 1.56–2.32; P < 0.001) were associated with increased CHE risk. Similarly, frailty co-occurring with multimorbidity also increased CHE risk compared with those with multimorbidity but not frailty (adjusted HR, 1.32; 95% CI, 1.17–1.48; P < 0.001).
Sensitivity Analysis
We additionally analysed participants not suffering from cancer and data with multiple imputation as two sensitivity analyses (presented in Table 5). The results were consistent with our main analysis, which validated our conclusions. E-value analysis was further conducted to assess the robustness of the impact of co-occurrence of frailty and multimorbidity on CHE in the MSM and time-varying Cox regression models. The E-values were greater than the estimated confounders for CHE (presented in Supplementary Table S3); therefore, it is unlikely that a potential unmeasured confounder could have a considerably greater effect on CHE than these known risk factors.
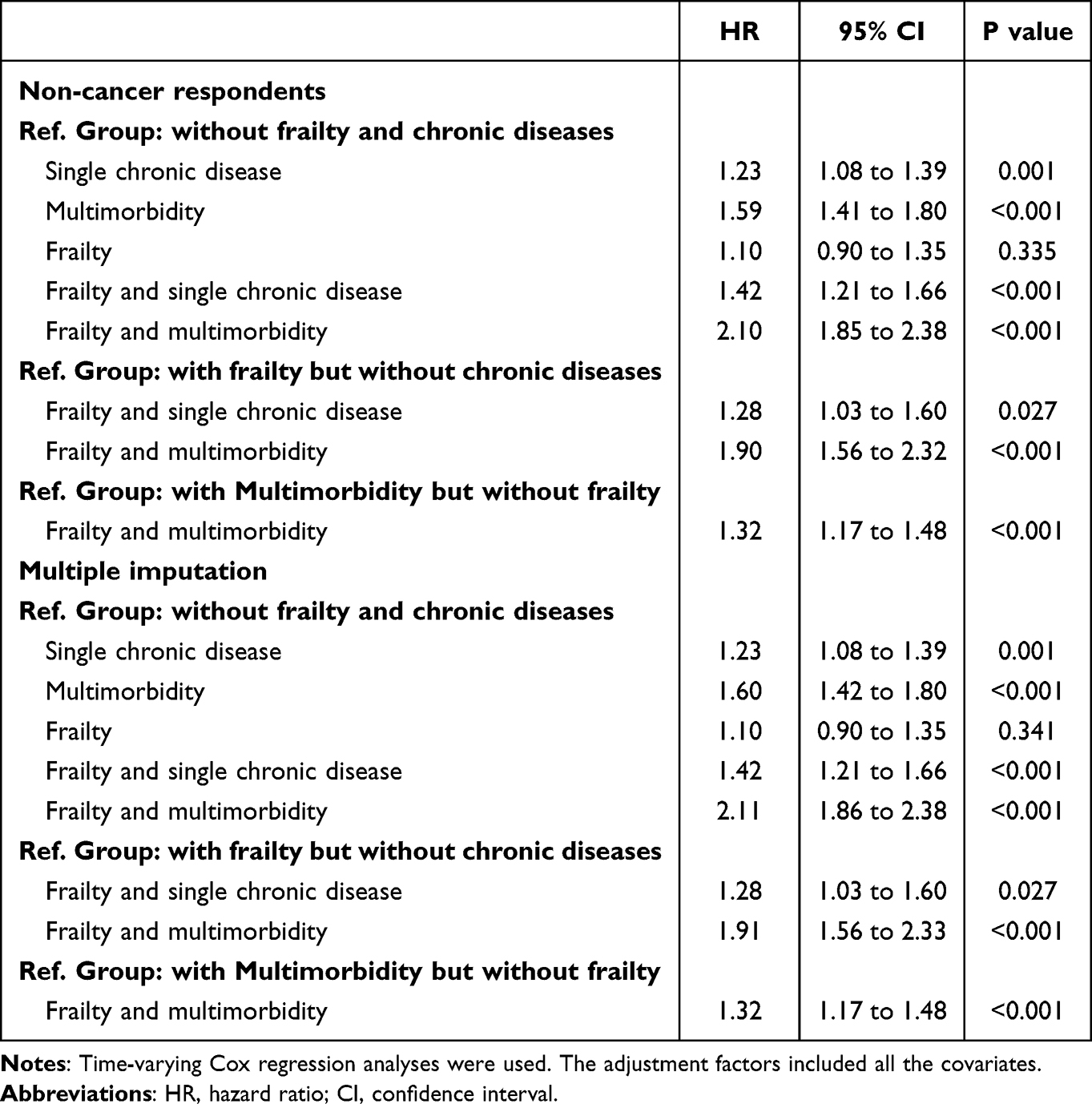 |
Table 5 Sensitivity Analysis |
Heterogeneity Between Rural and Urban Areas
We compared the effect of co-occurrence of frailty and multimorbidity on CHE between urban and rural areas (Table 6). Notably, compared with participants without frailty and chronic diseases, frailty co-occurring with multimorbidity was significantly associated with increased CHE risk in both rural and urban areas; nevertheless, the impact of single chronic diseases and frailty co-occurring with single chronic diseases was only significant in rural areas. Additionally, frailty co-occurring with a single chronic disease or multimorbidity was significantly associated with increased CHE risk only in rural areas compared with those with frailty but without chronic diseases; it was also only significant for the effect of multimorbidity’s co-occurrence with frailty in rural areas compared to those with multimorbidity without frailty.
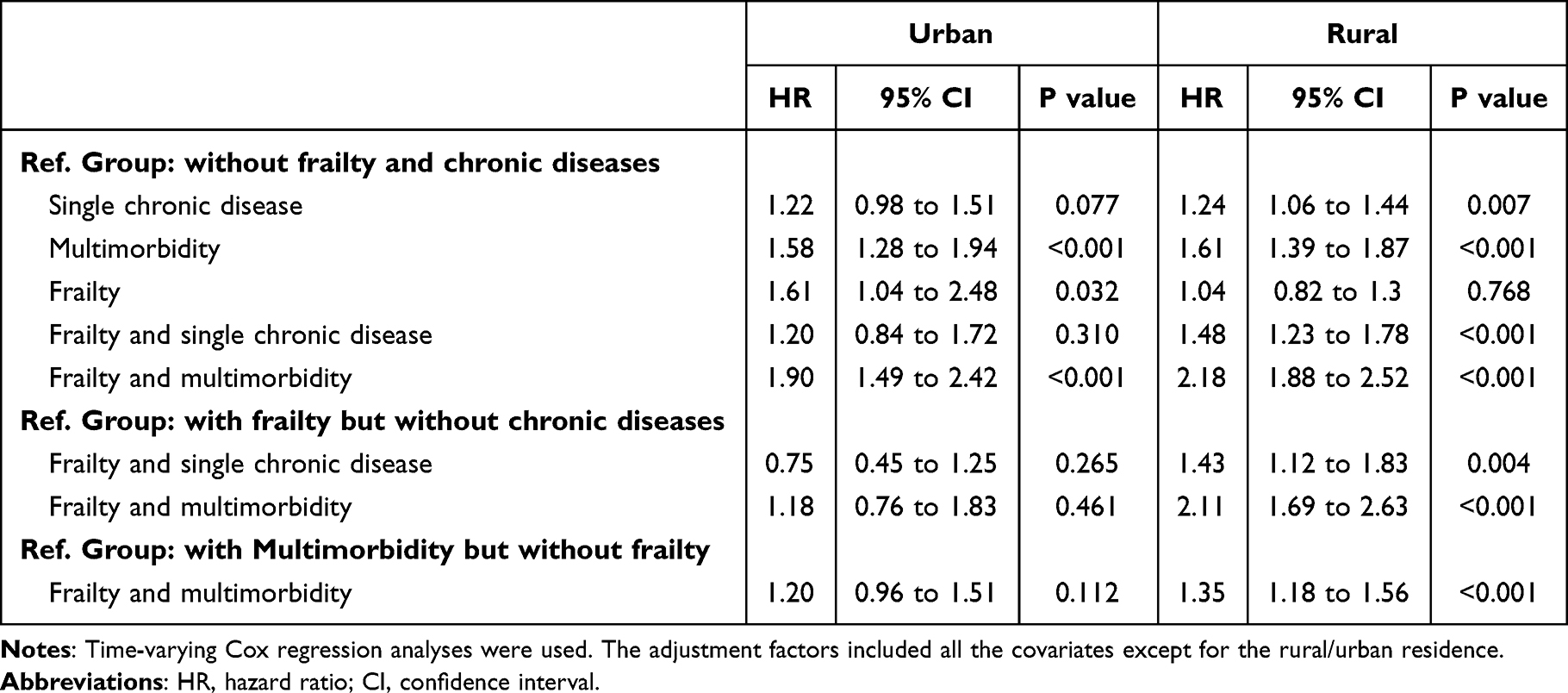 |
Table 6 Heterogeneity Between Rural and Urban Areas |
Discussion
To the best of our knowledge, this is the first study to use cohort analysis to evaluate the impact of co-occurrence of frailty and multimorbidity on CHE in China based on a nationally representative database among middle-aged and older adults. This study proved that both frailty and multimorbidity can independently predict increased CHE risk. More importantly, both frailty co-occurring with single or multiple chronic diseases and multimorbidity co-occurring with frailty increases CHE risk compared with frailty or multimorbidity’s individual status; but these effects are only significant in rural areas. However, co-occurrence of frailty and multimorbidity increases CHE risk in both rural and urban areas compared with the most robust participants (without frailty and chronic diseases).
Frailty and multimorbidity have been shown to be associated with older people’s risk of disability, hospitalisation, and mortality, as well as escalating health-related costs.38,39 The coexistence of multimorbidity and frailty was found to be more likely to increase the risk of adverse health outcomes in older adults than multimorbidity or frailty alone;28 therefore, both frailty co-occurring with chronic diseases and morbidity co-occurring with frailty may bring about great economic burden and increase CHE risk. Many older adults suffering from chronic diseases or multimorbidity have to enrol in long-term medication and regular examination. Additionally, chronic diseases often have complications, or acute episodes. Multimorbidity may be thought of as the accumulation of biological abnormalities deemed as clinically relevant and that define overt disease diagnoses.7,40 These situations release more demand for medical services, and bring great economic burdens for their families. Therefore, the increased risk of CHE was observed in all subgroups with a single chronic disease or multimorbidity compared to the robust group. Moreover, symptoms related to chronic diseases might have a relevant role in the onset or worsening of frailty status,40,41 which could also explain why CHE risk is higher in frailty co-occurring with a single chronic disease or multimorbidity than in frailty alone. For those with multimorbidity, co-occurrence of frailty may accelerate disease progression, affect disease prognosis, or cause acute onset of chronic diseases.42–44 Therefore, multimorbidity co-occurring with frailty also increases CHE risk.
Notably, frailty was observed to independently predict CHE risk after multimorbidity was controlled; however, frailty alone is not significantly associated with increased CHE risk compared with those without chronic disease and frailty. First, it may be caused by different reference groups and analysis models. Second, frailty stems from the progressive accumulation of biological deficits that pile up with time as an expression of ageing. It can be considered as a global and transversal measure for capturing both clinical and subclinical impairments.7,41 That means, frailty does not mean disease, and the mechanism between frailty, disease, healthcare utilisation, and medical economic burden is complex, and requires further prospective analysis in the future. Noticeably, frailty is characterised as systemic, dynamic, and reversible.4,12 Thus, certain intervention measures can be taken to prevent early occurrence of frailty, control its progress, or promote recovery to potentially lead to cost savings. This can provide policy makers with clear evidence of the requirement for certain interventions to prevent and control frailty. This also indicates that the coexistence of frailty and chronic disease is more harmful for older adults.
The heterogeneity of impact of co-occurrence of frailty and multimorbidity on CHE was observed in this study, with rural participants more likely to experience CHE. This may be because rural participants, with lower capacity to pay than urban participants, represent a large sample of lower socioeconomic levels, and the economic risks of frailty co-occurring with chronic diseases or multimorbidity co-occurring with frailty are too great for rural families with similar medical costs. Based on previous studies, we found that there are differences between urban and rural areas in terms of basic health status,45 and resources that can be accessed for medical services,46 which could cause differences in the impact of co-occurrence of frailty and multimorbidity between urban and rural areas. It is essential to balance the urban and rural economies, promote rural revitalisation, and establish a national social security network to maintain efficiency and equity.47
Policy Implications
According to the global Strategy for Healthy Aging, the core objective of healthy ageing is to improve the quality of life of older adults, shorten the survival period with disease, and extend healthy life expectancy.48 Both frailty and multimorbidity have been proved to be associated with worse quality of life,37,49 and as shown in this study, their coexistence causes catastrophic economic burden for families. Thus, prevention of frailty and multimorbidity, intensive management of older adults suffering from frailty and multimorbidity, and policy intervention should be enhanced to promote healthy ageing. China is experiencing an ageing population which could magnify the frailty and multimorbidity epidemic and will require significant adjustments to the countrywide management strategy. First, China has established a multi-tiered and widely covered medical security system, and has made significant achievements in reducing the economic burden of disease, releasing the demand for medical services and improving health.50 However, in the future, preferential policy towards the older population with frailty and multimorbidity, and promotion of fairness needs to be further strengthened. Second, China has invested a lot of resources to integrate basic public health services into primary healthcare (such as strengthening the management of hypertension and diabetes populations) and carrying out many health management projects for the elderly (such as routine physical examination).51 In the future, continuous attention to multimorbid populations and accurate screening of frailty need to be strengthened. Finally, China’s “Active Response to Population Aging Strategy” and “Healthy China Strategy” emphasise co-construction and sharing, and active initiative of the older population.52 Combined with previous effective interventions on multimorbidity and frailty in the older population, we should encourage older adults to enhance self-management of chronic diseases. Additionally, a good social atmosphere should strengthen publicity and education for the older population in urban and rural communities.
Limitations
This study has several limitations. First, it acknowledges the existence of recall bias, because information was self-reported. For example, indexes associated with physical function and mental health were the main constituent elements of frailty. However, a self-rated levels may differ from that of reality. Second, participants who died before 2018 had not been included our analysis. Given that frailty and multimorbidity are associated with mortality, excluding them may have introduced a survival bias. Third, indirect medical economic burden was not assessed in this study. Fourth, the causal effect and bidirectional association between frailty and multimorbidity, and which affects CHE more could not be assessed in this study. Finally, the FI covers numerous indicators. During the interview process, many indicators were observed missing among the participants, which led to sample loss.
Conclusion
Co-occurrence of frailty and multimorbidity is associated with a high risk of CHE. Preventing, postponing, or reducing frailty, and enhancing standard management of chronic diseases are essential in reducing healthcare costs and preventing families from poverty. More efficient interventions for frailty and multimorbidity are urgently required.
Data Sharing Statement
All the original data could be obtained from the official website of CHARLS (http://charls.pku.edu.cn/). The identified analysis dataset is available to other researchers and others upon request by emailing the corresponding author ([email protected]).
Ethics Approval and Consent to Participate
The Biomedical Ethics Review Committee of Peking University approved CHARLS, and all participants were required to provide written informed consent. The ethical approval number was IRB00001052-11015. As the data were accessible to the public, review and approval was not required for this research by the authors’ institutional review board or ethics committee.
Author Contributions
All authors made a significant contribution to the work reported, whether that is in the conception, study design, execution, acquisition of data, analysis and interpretation, or in all these areas; took part in drafting, revising or critically reviewing the article; gave final approval of the version to be published; have agreed on the journal to which the article has been submitted; and agree to be accountable for all aspects of the work.
Funding
This work was supported by the National Natural Science Foundation of China (71734003; 72104073).
Disclosure
The authors report no conflicts of interest in this work.
References
1. Lancet T. Ageing in China: a ticking bomb. Lancet. 2016;388(10056):2058. doi:10.1016/S0140-6736(16)32058-X
2. Fang EF, Xie C, Schenkel JA, et al. A research agenda for ageing in China in the 21st century (2nd edition): focusing on basic and translational research, long-term care, policy and social networks. Ageing Res Rev. 2020;64:101174. doi:10.1016/j.arr.2020.101174
3. Prince MJ, Wu F, Guo Y, et al. The burden of disease in older people and implications for health policy and practice. Lancet. 2015;385(9967):549–562. doi:10.1016/S0140-6736(14)61347-7
4. Dent E, Martin FC, Bergman H, et al. Management of frailty: opportunities, challenges, and future directions. Lancet. 2019;394(10206):1376–1386. doi:10.1016/S0140-6736(19)31785-4
5. Fan J, Yu C, Guo Y, et al. Frailty index and all-cause and cause-specific mortality in Chinese adults: a prospective cohort study. Lancet Public Health. 2020;5(12):e650–e660. doi:10.1016/S2468-2667(20)30113-4
6. Hoogendijk EO, Afilalo J, Ensrud KE, et al. Frailty: implications for clinical practice and public health. Lancet. 2019;394(10206):1365–1375. doi:10.1016/S0140-6736(19)31786-6
7. Clegg A, Young J, Iliffe S, Rikkert MO, Rockwood K. Frailty in elderly people. Lancet. 2013;381(9868):752–762. doi:10.1016/S0140-6736(12)62167-9
8. Bock JO, Konig HH, Brenner H, et al. Associations of frailty with health care costs--results of the ESTHER cohort study. Bmc Health Serv Res. 2016;16:128. doi:10.1186/s12913-016-1360-3
9. Fried LP, Ferrucci L, Darer J, Williamson JD, Anderson G. Untangling the concepts of disability, frailty, and comorbidity: implications for improved targeting and care. J Gerontol A Biol Sci Med Sci. 2004;59(3):255–263. doi:10.1093/gerona/59.3.M255
10. Butler A, Gallagher D, Gillespie P, et al. Frailty: a costly phenomenon in caring for elders with cognitive impairment. Int J Geriatr Psychiatry. 2016;31(2):161–168. doi:10.1002/gps.4306
11. Jin HY, Liu X, Xue QL, Chen S, Wu C. The association between frailty and healthcare expenditure among Chinese older adults. J Am Med Dir Assoc. 2020;21(6):780–785. doi:10.1016/j.jamda.2020.03.008
12. Fan L, Hou XY, Liu Y, et al. Catastrophic health expenditure associated with frailty in community-dwelling Chinese older adults: a prospective cohort analysis. Front Public Health. 2021;9:718910. doi:10.3389/fpubh.2021.718910
13. Hu X, Huang J, Lv Y, Li G, Peng X. Status of prevalence study on multimorbidity of chronic disease in China: systematic review. Geriatr Gerontol Int. 2015;15(1):1–10. doi:10.1111/ggi.12340
14. Glynn LG, Valderas JM, Healy P, et al. The prevalence of multimorbidity in primary care and its effect on health care utilization and cost. Fam Pract. 2011;28(5):516–523. doi:10.1093/fampra/cmr013
15. Lehnert T, Heider D, Leicht H, et al. Review: health care utilization and costs of elderly persons with multiple chronic conditions. Med Care Res Rev. 2011;68(4):387–420. doi:10.1177/1077558711399580
16. Lee JT, Hamid F, Pati S, Atun R, Millett C. Impact of noncommunicable disease multimorbidity on healthcare utilisation and out-of-pocket expenditures in middle-income countries: cross sectional analysis. PLoS One. 2015;10(7):e127199.
17. Wang Z, Li X, Chen M. Catastrophic health expenditures and its inequality in elderly households with chronic disease patients in China. Int J Equity Health. 2015;14(1):8. doi:10.1186/s12939-015-0134-6
18. Zhao Y, Atun R, Oldenburg B, et al. Physical multimorbidity, health service use, and catastrophic health expenditure by socioeconomic groups in China: an analysis of population-based panel data. Lancet Glob Health. 2020;8(6):e840–e849. doi:10.1016/S2214-109X(20)30127-3
19. Fu Y, Chen M, Si L. Multimorbidity and catastrophic health expenditure among patients with diabetes in China: a nationwide population-based study. BMJ Glob Health. 2022;7(2):e007714. doi:10.1136/bmjgh-2021-007714
20. Villacampa-Fernandez P, Navarro-Pardo E, Tarin JJ, Cano A. Frailty and multimorbidity: two related yet different concepts. Maturitas. 2017;95:31–35. doi:10.1016/j.maturitas.2016.10.008
21. Vetrano DL, Palmer K, Marengoni A, et al. Frailty and multimorbidity: a systematic review and meta-analysis. J Gerontol A Biol Sci Med Sci. 2019;74(5):659–666. doi:10.1093/gerona/gly110
22. Hajek A, Brettschneider C, Posselt T, et al. Predictors of frailty in old age - results of a longitudinal study. J Nutr Health Aging. 2016;20(9):952–957. doi:10.1007/s12603-015-0634-5
23. Zheng Z, Guan S, Ding H, et al. Prevalence and incidence of frailty in community-dwelling older people: Beijing longitudinal study of aging II. J Am Geriatr Soc. 2016;64(6):1281–1286. doi:10.1111/jgs.14135
24. Guaraldi G, Brothers TD, Zona S, et al. A frailty index predicts survival and incident multimorbidity independent of markers of HIV disease severity. AIDS. 2015;29(13):1633–1641. doi:10.1097/QAD.0000000000000753
25. Hanlon P, Nicholl BI, Jani BD, et al. Frailty and pre-frailty in middle-aged and older adults and its association with multimorbidity and mortality: a prospective analysis of 493 737 UK Biobank participants. Lancet Public Health. 2018;3(7):e323–e332. doi:10.1016/S2468-2667(18)30091-4
26. Jing Z, Li J, Fu PP, et al. Catastrophic health expenditure among single empty-nest elderly with multimorbidity in rural Shandong, China: the effect of co-occurrence of frailty. Int J Equity Health. 2021;20(1):23. doi:10.1186/s12939-020-01362-6
27. Woo J, Leung J, Fan L. Multi-morbidity, dependency, and frailty singly or in combination have different impact on health outcomes. Age. 2014;36(2):923–931. doi:10.1007/s11357-013-9590-3
28. Aarts S, Patel KV, Garcia ME, et al. Co-presence of multimorbidity and disability with frailty: an examination of heterogeneity in the frail older population. J Frailty Aging. 2015;4(3):131–138. doi:10.14283/jfa.2015.45
29. Zhao Y, Hu Y, Smith JP, Strauss J, Yang G. Cohort profile: the China Health and Retirement Longitudinal Study (CHARLS). Int J Epidemiol. 2014;43(1):61–68. doi:10.1093/ije/dys203
30. Rockwood K, Song X, MacKnight C, et al. A global clinical measure of fitness and frailty in elderly people. CMAJ. 2005;173(5):489–495. doi:10.1503/cmaj.050051
31. Kojima G, Iliffe S, Walters K. Smoking as a predictor of frailty: a systematic review. BMC Geriatr. 2015;15:131. doi:10.1186/s12877-015-0134-9
32. Barnett K, Mercer SW, Norbury M, et al. Epidemiology of multimorbidity and implications for health care, research, and medical education: a cross-sectional study. Lancet. 2012;380(9836):37–43. doi:10.1016/S0140-6736(12)60240-2
33. Si Y, Zhou Z, Su M, et al. Catastrophic healthcare expenditure and its inequality for households with hypertension: evidence from the rural areas of Shaanxi Province in China. Int J Equity Health. 2017;16(1):27. doi:10.1186/s12939-016-0506-6
34. Song Q, Smith JP. Hukou system, mechanisms, and health stratification across the life course in rural and urban China. Health Place. 2019;58:102150. doi:10.1016/j.healthplace.2019.102150
35. Yao SS, Cao GY, Han L, et al. Prevalence and patterns of multimorbidity in a nationally representative sample of older Chinese: results from the China health and retirement longitudinal study. J Gerontol A Biol Sci Med Sci. 2020;75(10):1974–1980. doi:10.1093/gerona/glz185
36. VanderWeele TJ, Ding P. Sensitivity analysis in observational research: introducing the E-value. Ann Intern Med. 2017;167(4):268–274. doi:10.7326/M16-2607
37. Haneuse S, VanderWeele TJ, Arterburn D. Using the E-value to assess the potential effect of unmeasured confounding in observational studies. JAMA. 2019;321(6):602–603. doi:10.1001/jama.2018.21554
38. Vetrano DL, Rizzuto D, Calderon-Larranaga A, et al. Trajectories of functional decline in older adults with neuropsychiatric and cardiovascular multimorbidity: a Swedish cohort study. PLoS Med. 2018;15(3):e1002503. doi:10.1371/journal.pmed.1002503
39. Marengoni A, Angleman S, Melis R, et al. Aging with multimorbidity: a systematic review of the literature. Ageing Res Rev. 2011;10(4):430–439. doi:10.1016/j.arr.2011.03.003
40. Fabbri E, Zoli M, Gonzalez-Freire M, et al. Aging and multimorbidity: new tasks, priorities, and frontiers for integrated gerontological and clinical research. J Am Med Dir Assoc. 2015;16(8):640–647. doi:10.1016/j.jamda.2015.03.013
41. Morley JE, Vellas B, van Kan GA, et al. Frailty consensus: a call to action. J Am Med Dir Assoc. 2013;14(6):392–397. doi:10.1016/j.jamda.2013.03.022
42. Onder G, Vetrano DL, Marengoni A, et al. Accounting for frailty when treating chronic diseases. Eur J Intern Med. 2018;56:49–52. doi:10.1016/j.ejim.2018.02.021
43. Shah S, Goldberg DS, Kaplan DE, et al. Patient frailty is independently associated with the risk of hospitalization for acute-on-chronic liver failure. Liver Transpl. 2021;27(1):16–26. doi:10.1002/lt.25896
44. Zazzara MB, Vetrano DL, Carfi A, Onder G. Frailty and chronic disease. Panminerva Med. 2019;61(4):486–492. doi:10.23736/S0031-0808.19.03731-5
45. Jiang J, Wang P. Health status in a transitional society: urban-rural disparities from a dynamic perspective in China. Popul Health Metr. 2018;16(1):22. doi:10.1186/s12963-018-0179-z
46. Wang W, Zhang Y, Lin B, et al. The urban-rural disparity in the status and risk factors of health literacy: a cross-sectional survey in central China. Int J Environ Res Public Health. 2020;17(11):1729.
47. Fu XZ, Sun QW, Sun CQ, Xu F, He JJ. Urban-rural differences in catastrophic health expenditure among households with chronic non-communicable disease patients: evidence from China family panel studies. BMC Public Health. 2021;21(1):874. doi:10.1186/s12889-021-10887-6
48. Rudnicka E, Napierala P, Podfigurna A, et al. The World Health Organization (WHO) approach to healthy ageing. Maturitas. 2020;139:6–11. doi:10.1016/j.maturitas.2020.05.018
49. Makovski TT, Schmitz S, Zeegers MP, Stranges S, van den Akker M. Multimorbidity and quality of life: systematic literature review and meta-analysis. Ageing Res Rev. 2019;53:100903. doi:10.1016/j.arr.2019.04.005
50. Tao W, Zeng Z, Dang H, et al. Towards universal health coverage: lessons from 10 years of healthcare reform in China. BMJ Glob Health. 2020;5(3):e2086.
51. Wang L, Wang Z, Ma Q, Fang G, Yang J. The development and reform of public health in China from 1949 to 2019. Global Health. 2019;15(1):45. doi:10.1186/s12992-019-0486-6
52. Tan X, Zhang Y, Shao H. Healthy China 2030, a breakthrough for improving health. Glob Health Promot. 2019;26(4):96–99. doi:10.1177/1757975917743533
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
Recommended articles
Evaluation of Joint Effect of Frailty and Sleep Health on Cardiometabolic Multimorbidity in Aging Population
Pan X, Tian A, Tan J, Miao Y, Zhang Q
Nature and Science of Sleep 2025, 17:2051-2064
Published Date: 2 September 2025