Back to Journals » Clinical Ophthalmology » Volume 17
IRIS® Registry (Intelligent Research In Sight) Analysis of the Incidence of Monovision in Cataract Patients with Bilateral Monofocal Intraocular Lens Implantation
Authors Bafna S, Gu X ![]() , Fevrier H, Merchea M
, Fevrier H, Merchea M
Received 23 June 2023
Accepted for publication 6 October 2023
Published 19 October 2023 Volume 2023:17 Pages 3123—3129
DOI https://doi.org/10.2147/OPTH.S424195
Checked for plagiarism Yes
Review by Single anonymous peer review
Peer reviewer comments 3
Editor who approved publication: Dr Scott Fraser
Shamik Bafna,1 Xiaolin Gu,2 Helene Fevrier,3 Mohinder Merchea2
1Cleveland Eye Clinic, Brecksville, OH, USA; 2Alcon Vision LLC, Fort Worth, TX, USA; 3Verana Health, San Francisco, CA, USA
Correspondence: Shamik Bafna, Cleveland Eye Clinic, 7001 S Edgerton Road, Brecksville, OH, 44141, USA, Tel +1 216-287-2060, Email [email protected]
Purpose: To determine the incidence of pseudophakic monovision among patients bilaterally implanted with monofocal intraocular lenses (IOLs) and to characterize the distribution of myopic offsets achieved.
Patients and Methods: This retrospective database study included data on patients receiving care from ophthalmologists who contributed to the Academy IRIS® (Intelligent Research In Sight) Registry. Anonymized data were collected, including patient age, ethnicity, procedure data (CPT code, date, laterality), and postoperative manifest refractive spherical equivalent (MRSE) in both eyes implanted with monofocal or monofocal toric IOLs. No data regarding IOL manufacturer, model, or power were collected. One primary outcome measure was the percentage of patients achieving monovision (defined as emmetropia within ± 0.25 diopters [D] in one eye and a myopic offset of ≥ 0.50 D in the fellow eye) among all patients receiving bilateral monofocal IOLs at the time of cataract surgery between January 1, 2016, and September 1, 2019, with at least 90 days of follow-up. Other primary outcomes included the distribution and frequency of myopic offsets (anisometropia) between eyes.
Results: Of the 16,765 people receiving bilateral monofocal IOLs within the study period, 4796 (28.6%) achieved emmetropia in at least one eye, as defined by an MRSE within ± 0.25 D. The incidence of monovision among these patients was 34.2% (1638/4796). One-quarter (24.7%; 405/1638) of patients who achieved monovision had a myopic offset between 0.50 and 0.74 D, with more than one-third (35.2%; 576/1638) falling within 0.75– 1.24 D and 18.0% within 1.25– 1.74 D. A myopic offset ≥ 1.75 D was observed in 22.1% (362/1638) of patients who achieved monovision.
Conclusion: Pseudophakic monovision for presbyopia correction was achieved in ~34% of patients in the IRIS Registry bilaterally implanted with monofocal IOLs, with myopic offsets typically ranging from 0.5 to 1.24 D.
Keywords: presbyopia, monovision, monofocal IOLs, myopic offset, diopter correction
Introduction
Presbyopia, an age-related loss of accommodation resulting in reduction of near vision, is estimated to affect about 1.8 billion people worldwide,1 with up to 50% having little to no correction.1,2 Uncorrected presbyopia diminishes both productivity3,4 and quality of life,5 both of which are improved with presbyopia correction.4,5 Uncorrected presbyopia in people aged <65 years has been estimated to reduce annual global productivity by more than US $25 billion, whereas this amount could be reduced to US $1.4 billion by correction of presbyopia.3
Options for presbyopia correction include spectacles, contact lenses, surgical procedures and pharmaceutical agents. One approach to presbyopia correction is monovision, in which one eye is corrected for distance vision and the contralateral eye is corrected for near vision using a myopic offset. Examples include monofocal contact lenses,6 corneal refractive surgeries,7 and pseudophakic monofocal intraocular lenses (IOLs).6,8,9 An alternative approach is to restore multifocal vision to each eye, using, for example, bi-, tri-, and multifocal spectacles6 and bi- and multi-focal contact lenses.10 Alternatively, presbyopia can be corrected using multifocal refractive procedures that create a corneal multifocality to increase depth of focus with or without a corneal inlay;7,11–13 multifocal, accommodating, and extended depth of focus (EDOF) IOLs;14,15 and scleral expansion procedures.12,16 Presbyopia can also be corrected by treatment with drugs, most of which are miotics that rely on the pupillary pinhole effect or are intended to restore crystalline lens flexibility.17
While advances in IOL technology have provided innovative means of correcting presbyopia with multifocal techniques, pseudophakic monovision remains a common solution to this high-prevalence problem. Since first reported in 1984,18 studies have examined outcomes associated with pseudophakic monovision, in which one eye is targeted for emmetropia and the contralateral eye is targeted for modest myopia, thereby providing intermediate and/or near visual acuity (VA). Traditional monovision uses a myopic offset in the range of 1.75 to 3 D to produce equivalent distance and near VA outcomes compared with multifocal IOLs to increase spectacle independence,9,19,20 but significantly reduces stereopsis.9 Modified and mini-monovision have smaller myopic offsets and have worse near VA outcomes but better stereoacuity and binocular intermediate VA than traditional monovision.9 Spectacle independence with monovision has been found to decrease over time, with one study reporting that 44% of patients were spectacle independent at 1 year, whereas only 22% were spectacle independent at 5 years.21
Despite the large number of options for presbyopia correction at the time of cataract surgery, surprisingly little is known regarding the frequency of pseudophakic monovision in large-scale, real-world settings. The present study describes the incidence of monovision achieved among patients included in the IRIS® Registry (Intelligent Research In Sight) database of the American Academy of Ophthalmology (Academy) who underwent cataract surgery and received bilateral monofocal or monofocal toric IOLs. The distribution and frequency of myopic offsets (anisometropia) among these monovision patients were evaluated.
Methods
This was an analysis of existing, anonymized data drawn from the IRIS Registry. The IRIS Registry is an ongoing database of real-world data extracted from the electronic health records (EHRs) of 440 million encounters between 74 million unique patients and over 15,000 ophthalmologists and the clinicians working in their practices between January 1, 2013, and April 1, 2022.22 The database search and resulting data set were provided by Verana Health (San Francisco, CA, USA), the vendor designated by the American Academy of Ophthalmology. The study was conducted in accordance with the Declaration of Helsinki. An Institutional Review Board waiver is not applicable to the study because (i) the research and analysis was conducted on anonymized data in accordance with the deidentification standard promulgated under 45 CFR § 164.514 and (ii) no research was conducted on human subjects.
Data were drawn from the EHRs of adults aged ≥45 years with bilateral age-related cataract, as defined by International Classification of Diseases, Tenth Revision (ICD-10) diagnosis codes developed by the World Health Organization (Supplementary Table 1). Patients with other ICD-10 diagnosis codes were excluded (Supplementary Table 2). All included patients underwent bilateral cataract extraction with implantation of bilateral monofocal (including monofocal toric) IOLs, as defined by Current Procedural Terminology (CPT) codes maintained by the American Medical Association (Supplementary Table 3) between January 1, 2016, and September 1, 2019, with the maximum interval between fellow-eye surgery of ≤365 days. Other eligibility criteria included specification of laterality of both procedure codes, a minimum of two pre-operative visits before first-eye surgery and 90 days of follow-up after second-eye surgery with postoperative refractive data available for both eyes; one eye with postoperative spherical equivalent (SE) between +0.25 D and −0.25D inclusive; the fellow eye with a postoperative SE of ≤0.5 D; a difference in SE between the two eyes of ≥0.5 D; and the absence of disallowed CPT codes (Supplementary Table 4).
Data collected included age, gender, race/ethnicity, procedure data (CPT code, date, laterality), and postoperative manifest refractive SE (MRSE) in both eyes. No data regarding IOL manufacturer, model, or power were collected.
The primary outcome of this analysis was the incidence of monovision (defined as final refractive emmetropia (SE ± 0.25 D) in one eye and myopic offset or inter-eye difference in SE, of ≥0.5 D) among patients with bilateral monofocal IOL implantation. Secondary outcomes included the distribution and frequency of inter-eye myopic offsets among monovision patients. All outcomes were analyzed using descriptive statistics only. No formal power/sample size analysis was conducted a priori. The final sample size consisted of all patients in the IRIS Registry database meeting the eligibility criteria of this study. All descriptive statistical analyses were performed using RStudio 1.2.5033 statistical software.
Results
This analysis identified 16,765 patients who underwent bilateral cataract surgery with bilateral monofocal IOL implantation within the study timeframe, with all required data available for both eyes (Figure 1). The demographic characteristics of these patients are shown in Table 1.
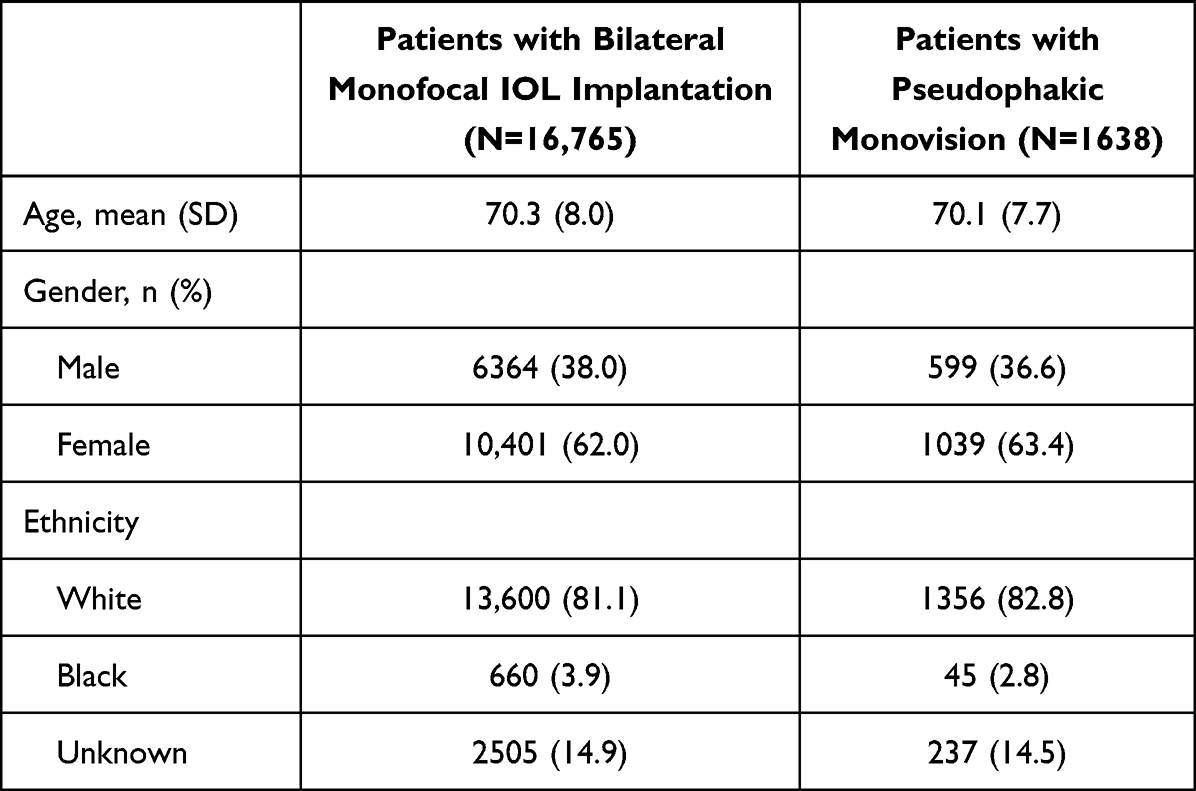 |
Table 1 Demographic Characteristics of All Patients Receiving Bilateral Monofocal Intraocular Lens Implantation and the Subgroup Achieving Pseudophakic Monovision |
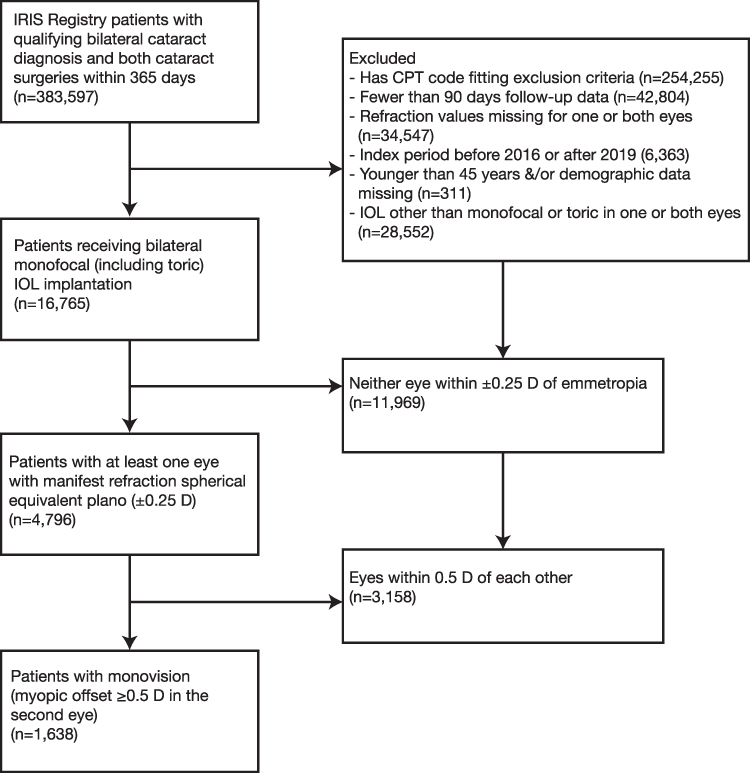 |
Figure 1 Study design: retrospective descriptive analysis of the IRIS clinical registry database. |
Of the 16,765 individuals receiving bilateral monofocal IOLs during the study period, 4796 (28.6%) achieved emmetropia in at least one eye, as defined by a refractive SE within ± 0.25 D. Moreover, 1638 patients achieved monovision with myopic offset ≥0.50 D in the second eye; the demographic characteristics of this latter subset are also presented in Table 1 and are similar to those in the larger group. The incidence of monovision (one eye within ± 0.25 D of emmetropia and the fellow eye with myopic offset of ≥0.5 D) among these patients was 34.2% (1638/4796).
Figure 2 shows the distribution of myopic offsets among the 1638 patients with monovision. There was a myopic offset between 0.50–0.75 D for 24.7% (405/1638) of patients, 0.75–1.24 D for 35.2% (576/1638), and 1.25–1.74 D for 18.0% (295/1638). A myopic offset ≥1.75 D was observed in 22.1% (362/1638) of monovision patients.
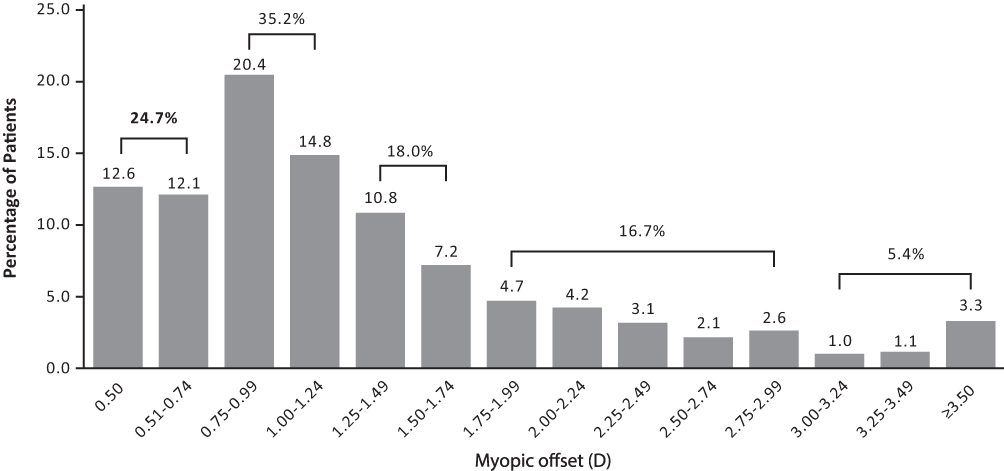 |
Figure 2 Frequency and distribution of myopic offsets among 1638 patients with pseudophakic monovision. |
Discussion
This analysis describes the achievement of pseudophakic monovision for presbyopia correction after bilateral cataract surgery using data from the IRIS Registry. Monovision (one eye with SE within ± 0.25 D of emmetropia and the fellow eye with a ≥ 0.5 D myopic offset) was achieved in ~34% of patients received bilateral monofocal IOL implantation.
These real-world findings from US cataract surgeons participating in the IRIS Registry are similar to other reports of pseudophakic monovision utilization, showing that monovision is still a common approach to manage presbyopia at the time of cataract surgery. Prior to the development of modern presbyopia-correcting IOLs, pseudophakic monovision was common, with 86% of surgeons in a 2003 survey of the American Society of Cataract and Refractive Surgery utilizing this technique.23 A more recent 2017 survey of more than 1900 delegates of the European Society of Cataract and Refractive Surgery found that surgeons utilized monovision or mini-monovision for presbyopia correction in 43% of cataract procedures, whereas presbyopia-correcting IOLs were used in only 6% of procedures.24 These findings were consistent with a 2019 survey of the ASCRS, in which 27% of cataract procedures involved use of pseudophakic monovision and only 10% utilized presbyopia-correcting IOLs.25 The use of presbyopia-correcting IOLs has increased in recent years, as shown in a 2022 survey of the ASCRS, which reported that 17% of cataract procedures involved use of presbyopia-correcting IOLs, whereas 22% utilized pseudophakic monovision IOLs.26
Presbyopia-correcting IOL technology has advanced markedly over the past ten years. Compared with former generations of presbyopia-correcting IOLs, modern diffractive bifocal, trifocal, and EDOF IOLs have shown beneficial effects on spectacle independence and patient satisfaction.15,27–29 Monovision with monofocal IOLs, which can provide some level of presbyopia correction, has limitations, however, with some patients showing low tolerance due to reduced binocularity and stereopsis, especially with traditional monovision, and relatively low and unsustainable spectacle independence.30–34 The relatively high usage of monovision with monofocal IOLs in the present study and the relatively low adoption rate of presbyopia-correcting IOLs throughout the study period were somewhat surprising. The possible reasons include cost, as most patients must bear the added cost of premium IOLs over standard monofocal IOLs and the visual phenomena associated with diffractive IOLs, which can include glare, halos, and starbursts, as well as decreased contrast sensitivity.15,20,35 Novel non-diffractive EDOF IOLs, which have been found to provide an extended range of vision, accompanied by a lower incidence of visual phenomena, as compared with diffractive EDOFs, may help increase the adoption of presbyopia-correcting IOLs.36–38
The target postoperative refraction and the preoperative intent to achieve monovision were not analyzed in the current EHR dataset due to lack of data availability. The present study defined monovision in refractive terms, rather than functionally, as an emmetropic eye and a myopic offset in the contralateral eye. The myopic offsets in near eyes ranged from 0.5 D to 10.125 D, with the majority (59.9%) falling between 0.50 D and 1.24 D, but only about one-fifth (22.1%) being ≥1.75 D. Offsets >3.0 D may, however, be associated with inaccurate IOL power calculations, because surgeons rarely target anisometropia >2.5D.9 The myopic offsets observed in the present study were consistent with those reported in other studies, with a trend for smaller degrees of anisometropia to preserve stereopsis and minimize aniseikonia in recent years. Early studies evaluated myopic offsets of ≥2.0 D,21,23,39–41 later studies explored the range of 1.5–2.0 D,42,43 and more recent studies have evaluated offsets of 0.75–1.75 D.44–49 These latter offsets were initially referred to as mini-monovision to distinguish them from the higher offsets used earlier. At present, however, offsets <1.0 D are considered mini-monovision.
Although this study was unable to analyze preoperative monovision intent and target postoperative refraction, this study found that 34% of the patients achieved monovision, as defined by at least one eye achieving emmetropia (postoperative MRSE within ± 0.25D) and a myopic offset ≥0.50 D in the contralateral eye. Of these patients, 35.2% and 24.7% had myopic offsets of 0.75 D–1.24 D and.0.5 D–0.74 D, respectively, a distribution consistent with current trends of modified or mini-monovision with monofocal IOLs.
The strengths of this study include its use of data from the IRIS Registry, reflecting the real-world practice of over 12,000 US ophthalmologists. The limitations include the incomplete participation of United States ophthalmology practices and hospital systems in the IRIS Registry. This observational dataset is subject to errors in EHR documentation, missing data, and miscoded diagnoses or procedures. Additionally, there is limited availability of data on preoperative planning including target postoperative refractions as well as binocular VAs at distance, intermediate, and near, which are not routinely tested in most patients.
Conclusions
In summary, this analysis of real-world data from the IRIS Registry database demonstrates that pseudophakic monovision was achieved for presbyopia correction in ~34% of eyes bilaterally implanted with monofocal IOLs, with 59.9% of myopic offsets in the range of 0.5–1.24 D.
Acknowledgments
Editorial support was provided by BelMed Professional Resources, with funding from Alcon.
Disclosure
Dr Shamik Bafna is a key opinion leader for Alcon, Zeiss, and BVI, outside the submitted work. Mrs Helene Fevrier is an employee of Verana Health which was contracted to perform these analyses. Dr Xiaolin Gu and Dr Mohinder Merchea are employees of Alcon Vision, LLC. The authors report no other conflicts of interest in this work.
References
1. Fricke TR, Tahhan N, Resnikoff S, et al. Global prevalence of presbyopia and vision impairment from uncorrected presbyopia: systematic review, meta-analysis, and modelling. Ophthalmology. 2018;125(10):1492–1499. doi:10.1016/j.ophtha.2018.04.013
2. Holden BA, Fricke TR, Ho SM, et al. Global vision impairment due to uncorrected presbyopia. Arch Ophthalmol. 2008;126(12):1731–1739. doi:10.1001/archopht.126.12.1731
3. Frick KD, Joy SM, Wilson DA, Naidoo KS, Holden BA. The global burden of potential productivity loss from uncorrected presbyopia. Ophthalmology. 2015;122(8):1706–1710. doi:10.1016/j.ophtha.2015.04.014
4. Reddy PA, Congdon N, MacKenzie G, et al. Effect of providing near glasses on productivity among rural Indian tea workers with presbyopia (PROSPER): a randomised trial. Lancet Glob Health. 2018;6(9):e1019–e1027. doi:10.1016/S2214-109X(18)30329-2
5. Goertz AD, Stewart WC, Burns WR, Stewart JA, Nelson LA. Review of the impact of presbyopia on quality of life in the developing and developed world. Acta Ophthalmol. 2014;92(6):497–500. doi:10.1111/aos.12308
6. Wolffsohn JS, Davies LN. Presbyopia: effectiveness of correction strategies. Prog Retin Eye Res. 2019;68:124–143. doi:10.1016/j.preteyeres.2018.09.004
7. Stival LR, Figueiredo MN, Santhiago MR. Presbyopic excimer laser ablation: a review. J Refract Surg. 2018;34(10):698–710. doi:10.3928/1081597X-20180726-02
8. Mahrous A, Ciralsky JB, Lai EC. Revisiting monovision for presbyopia. Curr Opin Ophthalmol. 2018;29(4):313–317.
9. Labiris G, Toli A, Perente A, Ntonti P, Kozobolis VP. A systematic review of pseudophakic monovision for presbyopia correction. Int J Ophthalmol. 2017;10(6):992–1000. doi:10.18240/ijo.2017.06.24
10. Remon L, Perez-Merino P, Macedo-de-Araujo RJ, Amorim-de-Sousa AI, Gonzalez-Meijome JM. Bifocal and multifocal contact lenses for presbyopia and myopia control. J Ophthalmol. 2020;2020:8067657. doi:10.1155/2020/8067657
11. Shetty R, Brar S, Sharma M, Dadachanji Z, Lalgudi VG. PresbyLASIK: a review of PresbyMAX, Supracor, and laser blended vision: principles, planning, and outcomes. Indian J Ophthalmol. 2020;68(12):2723–2731. doi:10.4103/ijo.IJO_32_20
12. Bilbao-Calabuig R, Llovet-Osuna F. Non-lens-based surgical techniques for presbyopia correction. Arch Soc Esp Oftalmol. 2017;92(9):426–435. doi:10.1016/j.oftal.2017.04.005
13. Arlt E, Krall E, Moussa S, Grabner G, Dexl A. Implantable inlay devices for presbyopia: the evidence to date. Clin Ophthalmol. 2015;9:129–137. doi:10.2147/OPTH.S57056
14. Bilbao-Calabuig R, Gonzalez-Lopez F, Llovet-Rausell A, Ortega-Usobiaga J, Tejerina Fernandez V, Llovet-Osuna F. Lens-based surgical correction of presbyopia. Where are we in 2020? Arch Soc Esp Oftalmol. 2021;96(2):74–88. doi:10.1016/j.oftal.2020.07.012
15. Sieburth R, Chen M. Intraocular lens correction of presbyopia. Taiwan J Ophthalmol. 2019;9(1):4–17. doi:10.4103/tjo.tjo_136_18
16. Hipsley A, Hall B, Rocha KM. Scleral surgery for the treatment of presbyopia: where are we today? Eye Vis. 2018;5(1):4. doi:10.1186/s40662-018-0098-x
17. Montes-Mico R, Charman WN. Pharmacological strategies for presbyopia correction. J Refract Surg. 2019;35(12):803–814. doi:10.3928/1081597X-20191010-04
18. Boerner CF, Thrasher BH. Results of monovision correction in bilateral pseudophakes. J Am Intraocul Implant Soc. 1984;10(1):49–50. doi:10.1016/S0146-2776(84)80077-4
19. Kelava L, Baric H, Busic M, Cima I, Trkulja V. Monovision versus multifocality for presbyopia: systematic review and meta-analysis of randomized controlled trials. Adv Ther. 2017;34(8):1815–1839. doi:10.1007/s12325-017-0579-7
20. Greenstein S, Pineda R. The quest for spectacle Independence: a comparison of multifocal intraocular lens implants and pseudophakic monovision for patients with presbyopia. Semin Ophthalmol. 2017;32(1):111–115. doi:10.1080/08820538.2016.1228400
21. Ito M, Shimizu K, Iida Y, Amano R. Five-year clinical study of patients with pseudophakic monovision. J Cataract Refract Surg. 2012;38(8):1440–1445. doi:10.1016/j.jcrs.2012.03.031
22. American Academy of Ophthalmology. IRIS Registry Data Analysis. Available from: https://www.aao.org/iris-registry/data-analysis/requirements.
23. Xiao J, Jiang C, Zhang M. Pseudophakic monovision is an important surgical approach to being spectacle-free. Indian J Ophthalmol. 2011;59(6):481–485. doi:10.4103/0301-4738.86318
24. European Society for Cataract and Refractive Surgery. Clinical Trends Survey 2017; 2017. Available from: https://www.eurotimes.org/wp-content/uploads/2018/11/Clinical_Survey_Supplement-2017Results-12pp-final.pdf.
25. American Society of Cataract and Refractive Surgery. Clinical Survey 2019; 2019. Available from: https://supplements.eyeworld.org/eyeworld-supplements/ascrs-clinical-survey-2019.
26. American Society of Cataract and Refractive Surgery. Highlights from the 2022 ASCRS Clinical Survey. Available from: https://supplements.eyeworld.org/i/1483249-ascrs-clinical-survey-2022/0?.
27. Maxwell WA, Waycaster CR, D’Souza AO, Meissner BL, Hileman K. A United States cost-benefit comparison of an apodized, diffractive, presbyopia-correcting, multifocal intraocular lens and a conventional monofocal lens. J Cataract Refract Surg. 2008;34(11):1855–1861. doi:10.1016/j.jcrs.2008.07.024
28. Song X, Liu X, Wang W, et al. Visual outcome and optical quality after implantation of zonal refractive multifocal and extended-range-of-vision IOLs: a prospective comparison. J Cataract Refract Surg. 2020;46(4):540–548. doi:10.1097/j.jcrs.0000000000000088
29. Zvornicanin J, Zvornicanin E. Premium intraocular lenses: the past, present and future. J Curr Ophthalmol. 2018;30(4):287–296. doi:10.1016/j.joco.2018.04.003
30. Son HS, Kim SH, Auffarth GU, Choi CY. Prospective comparative study of tolerance to refractive errors after implantation of extended depth of focus and monofocal intraocular lenses with identical aspheric platform in Korean population. BMC Ophthalmol. 2019;19(1):187. doi:10.1186/s12886-019-1193-z
31. Rodov L, Reitblat O, Levy A, Assia EI, Kleinmann G. Visual outcomes and patient satisfaction for trifocal, extended depth of focus and monofocal intraocular lenses. J Refract Surg. 2019;35(7):434–440. doi:10.3928/1081597X-20190618-01
32. Pedrotti E, Chierego C, Talli PM, et al. Extended depth of focus versus monofocal IOLs: objective and subjective visual outcomes. J Refract Surg. 2020;36(4):213–222. doi:10.3928/1081597X-20200212-01
33. Reinhard T, Maier P, Bohringer D, et al. Comparison of two depth of focus intraocular lenses with a monofocal lens: a multi-centre randomized trial. Graefes Arch Clin Exp Ophthalmol. 2021;259(2):431–442. doi:10.1007/s00417-020-04868-5
34. Pedrotti E, Neri E, Bonacci E, et al. Extended depth of focus versus monofocal IOLs in patients with high myopia: objective and subjective visual outcomes. J Refract Surg. 2022;38(3):158–166. doi:10.3928/1081597X-20211220-01
35. de Vries NE, Nuijts RM. Multifocal intraocular lenses in cataract surgery: literature review of benefits and side effects. J Cataract Refract Surg. 2013;39(2):268–278. doi:10.1016/j.jcrs.2012.12.002
36. Bala C, Poyales F, Guarro M, et al. Multicountry clinical outcomes of a new nondiffractive presbyopia-correcting IOL. J Cataract Refract Surg. 2022;48(2):136–143. doi:10.1097/j.jcrs.0000000000000712
37. McCabe C, Berdahl J, Reiser H, et al. Clinical outcomes in a U.S. registration study of a new EDOF intraocular lens with a nondiffractive design. J Cataract Refract Surg. 2022;48(11):1297–1304. doi:10.1097/j.jcrs.0000000000000978
38. Guarro M, Sararols L, Londoño GJ, et al. Visual disturbances produced after the implantation of 3 EDOF intraocular lenses vs 1 monofocal intraocular lens. J Cataract Refract Surg. 2022;48(12):1354–1359. doi:10.1097/j.jcrs.0000000000000988
39. Lubinski W, Cholewa M, Podboraczynska-Jodko K. Conventional pseudophakic monovision--visual function, patient satisfaction and complications. Klin Oczna. 2013;115(3):189–193.
40. Ito M, Shimizu K, Amano R, Handa T. Assessment of visual performance in pseudophakic monovision. J Cataract Refract Surg. 2009;35(4):710–714. doi:10.1016/j.jcrs.2008.12.019
41. Greenbaum S. Monovision pseudophakia. J Cataract Refract Surg. 2002;28(8):1439–1443. doi:10.1016/S0886-3350(02)01218-X
42. Hayashi K, Yoshida M, Manabe S, Hayashi H. Optimal amount of anisometropia for pseudophakic monovision. J Refract Surg. 2011;27(5):332–338. doi:10.3928/1081597X-20100817-01
43. Marques FF, Sato RM, Chiacchio BB, Marques DM, Barreiro J, Caetano RL. Evaluation of visual performance and patient satisfaction with pseudophakic monovision technique. Arq Bras Oftalmol. 2009;72(2):164–168. doi:10.1590/S0004-27492009000200006
44. Abdelrazek Hafez T, Helaly HA. Spectacle Independence and patient satisfaction with pseudophakic mini-monovision using aberration-free intraocular lens. Clin Ophthalmol. 2019;13:2111–2117. doi:10.2147/OPTH.S215229
45. Turnbull AMJ, Hill WE, Barrett GD. Accuracy of intraocular lens power calculation methods when targeting low myopia in monovision. J Cataract Refract Surg. 2020;46(6):862–866. doi:10.1097/j.jcrs.0000000000000187
46. Zhang F, Sugar A, Arbisser L, Jacobsen G, Artico J. Crossed versus conventional pseudophakic monovision: patient satisfaction, visual function, and spectacle Independence. J Cataract Refract Surg. 2015;41(9):1845–1854. doi:10.1016/j.jcrs.2015.10.013
47. Naeser K, Hjortdal JO, Harris WF. Pseudophakic monovision: optimal distribution of refractions. Acta Ophthalmol. 2014;92(3):270–275. doi:10.1111/aos.12148
48. Goldberg DG, Goldberg MH, Shah R, Meagher JN, Ailani H. Pseudophakic mini-monovision: high patient satisfaction, reduced spectacle dependence, and low cost. BMC Ophthalmol. 2018;18(2):293. doi:10.1186/s12886-018-0963-3
49. Hayashi K, Ogawa S, Manabe S, Yoshimura K. Binocular visual function of modified pseudophakic monovision. Am J Ophthalmol. 2015;159(2):232–240. doi:10.1016/j.ajo.2014.10.023
 © 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.
© 2023 The Author(s). This work is published and licensed by Dove Medical Press Limited. The
full terms of this license are available at https://www.dovepress.com/terms
and incorporate the Creative Commons Attribution
- Non Commercial (unported, 3.0) License.
By accessing the work you hereby accept the Terms. Non-commercial uses of the work are permitted
without any further permission from Dove Medical Press Limited, provided the work is properly
attributed. For permission for commercial use of this work, please see paragraphs 4.2 and 5 of our Terms.